
Abstract
Despite the known consequences associated with children’s exposure to intimate partner violence (IPV), numerous children exposed to IPV never access victim services and/or mental health treatment. Informed by the Child Development-Community Policing Program (CD-CP), the Child Trauma Response Team (CTRT) is designed to provide a coordinated, immediate, trauma-informed, and interdisciplinary response to children, adolescents, and their impacted family members who are exposed to severe IPV. The aim of this study was to explore the feasibility of the CTRT from the perspective of the key stakeholders and to identify what facilitated and/or hindered the collaborative model. Interviews were conducted with all 12 CTRT stakeholders of whom three worked for law enforcement, four worked for the district attorney’s office, four worked for the nonprofit victim service organization, and one worked for the city office funding the pilot. Results indicated that the CTRT program evolved through a cyclical process including (a) implementing and enhancing program services, (b) defining and nurturing partner relationships, and (c) shifting practices among partnering agencies. The results provide concrete tools and practices that were successful in the CTRT pilot implementation. Despite the potential barriers to successful multidisciplinary collaborations, it is critical that we invest in developing and implementing collaborative intervention models in the IPV field. The CTRT model is an innovative model that conducts multidisciplinary coordinated outreach to families experiencing severe IPV to enhance family engagement in services and, when appropriate, in the criminal justice process.
Keywords
Introduction
Children’s exposure to intimate partner violence (IPV) represents a serious public health issue, impacting more than 7 million children a year in the United States (McDonald, Jouriles, Ramisetty-Mikler, Caetano, & Green, 2006). It is estimated that 29% of children in the United States live in families in which IPV has occurred in the past year (McDonald et al., 2006). Researchers have documented the numerous negative effects that seeing, hearing, or attempting to intervene in IPV have on children’s development, mental health, physical health, and adult functioning (Evans, Davies, & DiLillo, 2008; Holt, Buckley, & Whelan, 2008; Hungerford, Wait, Fritz, & Clements, 2012). Children’s exposure to IPV has been linked to deficiencies in cognition, academic achievement, socioeconomic development, and with later adult criminal behavior (Carpenter & Stacks, 2009; Graham-Bermann & Perkins, 2010; Rigterink, Fainsilber, Katz, & Hessler, 2010; Roberts, Gilman, Fitzmaurice, Decker, & Koenen, 2010). Children exposed to IPV also experience disproportionately high levels of child abuse and physical injuries (Hamby, Finkelhor, Turner, & Ormrod, 2010; USDHHS, 2017).
Furthermore, families who experience the most severe forms of IPV often also experience poverty, social disadvantage, and structural racism which create an array of barriers to accessing and engaging in victim services and mental health treatment. Roberts et al. (2010) examined data collected by the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC; Grant, Moore, Shepard, & Kaplan, 2003) and found that Hispanic and Black children had significantly higher risk of witnessing domestic violence as a child than White children and that Black children were at a significantly higher risk for developing post-traumatic stress disorder (PTSD) than White children. However, the researchers also found that among people with PTSD, Black, Hispanic, and Asian individuals were significantly less likely to receive treatment for PTSD than White individuals. Furthermore, in a study conducted by McLaughlin and colleagues (2013) using the National Comorbidity Survey Replication Adolescent Supplement (NCS-A; Kessler et al., 2009), the results found that among adolescents with PTSD, adolescents living in poverty had lower odds of recovery. Therefore, despite the known significant short- and long-term consequences associated with children’s exposure to IPV, the children most vulnerable to these sequelae are often the children least likely to access and engage in victim services and mental health treatment.
Law Enforcement and Community Interventions
The President’s Task Force on 21st Century Policing (2015), aiming to strengthen community policing and trust among law enforcement officers and the communities they serve, recommended that law enforcement agencies engage in multidisciplinary, community team approaches for responding to domestic violence and that communities adopt policies and programs that address the needs of children and youth at risk for violence. Although there are few law enforcement and community partnerships that support children exposed to IPV, this unique partnership has the potential to engage families in increasing their physical and emotional safety while interrupting the potential cascading impact exposure to IPV can have on children.
Law enforcement officers encounter children exposed to IPV on a daily basis and are often the first professionals to interact with the IPV victim and his or her children. According to the National Crime Victimization Survey (Reaves, 2017), 48% of homes with calls to law enforcement for severe IPV include children less than 12 years of age. Therefore, law enforcement officers are in a unique position to provide a gateway to the victim and his or her children to access community services. As Susan J. Ko and colleagues (2008) emphasize, by addressing victims and their children supportively, identifying safe options for the family, and providing victims and their children with trauma-informed community services, first responders can provide a “psychological scaffolding” needed to support families experiencing IPV to “regain hope and reorganize to deal with crises” (p. 399). However, few law enforcement agencies prioritize trauma-informed responses to children who are exposed to IPV and few officers are trained on how to respond to children after a violent incident (Ko et al., 2008; Marans, Hahn, International Association of Chiefs of Police, & Yale University, Child Study Center, 2017).
Community-based organizations, such as victim service organizations and mental health agencies, have an array of trauma-informed programs aimed to increase survivor safety and prevent the development of PTSD. There exists numerous evidence-based mental health interventions, such as Trauma-Focused Cognitive Behavior Therapy (TF-CFT; Cohen, Mannarino, & Deblinger, 2016), Child–Parent Psychotherapy (CPP; Lieberman, 2004), the Child and Family Traumatic Stress Intervention (CF-TSI; Berkowitz, Stover, & Marans, 2011), Kids’ Club (Graham-Bermann, 1992), and Project Support (Jouriles et al., 2001), designed to decrease PTSD symptoms and other serious adverse post-trauma consequences. However, few of these organizations have access to families immediately following severe incidents of IPV. Rather, the majority of victim service and mental health organizations are provided in office settings, by appointment, and require victims to reach out and request support. By partnering the law enforcement agencies that have immediate access to families following severe incidents of IPV with the community-based organizations that are able to provide trauma-informed safety planning and mental health treatment, communities may be able to increase access to and engagement with services by families experiencing IPV.
To date, there are two evaluated interventions, developed by the Yale Child Study Center, that provide coordinated criminal justice and community-based services to children exposed to IPV with the goal of disrupting the resulting negative outcomes associated with such exposure. The CD-CP has been in operation since 1992 and provides a collaborative law enforcement and mental health response for violence-exposed and traumatized children. CD-CP clinicians ride along with patrol officers and respond to situations in which a child is exposed to any form of violence. In addition, the CD-CP reviews cases where children have been exposed to violence and develops and implements response plans. Clinicians involved in the program meet separately to review clinical assessments and treatment needs and provide 24-hr response services in acute situations (Murphy, Rosenheck, Berkowitz, & Marans, 2005).
Murphy and colleagues (2005) conducted an evaluation of the CD-CP program in which they analyzed 2361 child and adolescent clinical records to identify the child and event characteristics associated with the presence of the direct, in-person response at the time of the law enforcement contact. The children and adolescents in the sample experienced and/or witnessed a range of traumatic incidents including accidents, assaults, property crimes, family violence, drug/alcohol offenses, psychiatric crises, fire, sex crimes, conduct problems, maltreatment, and/or IPV. Their analysis yielded two primary results: (a) Hispanic youth were more likely to make use of the program than their Caucasian counterparts and (b) The more severe the incident, the more likely families were to participate in the program (Murphy et al., 2005). However, Murphy and colleagues (2005) found that incidents involving IPV were less likely to result in the presence of the acute response. The researchers noted that IPV is often associated with obstacles to service engagement. Further research, therefore, is needed to understand how a collaborative law enforcement and community response model can support families experiencing IPV.
The second program, The Domestic Violence Home Visit Intervention (DVHVI), is an intervention similar to the CD-CP, but this program focuses exclusively on children’s exposure to IPV. In this intervention, a law enforcement officer and victim service advocate, trained in IPV, trauma, and child development issues, visit families within 2 to 5 days after a violent IPV incident. The goal of the program is to connect families to services and reduce the likelihood that children will develop PTSD. Stover, Poole, and Marans (2009) conducted a cross-sectional evaluation of the DVHVI in which they reviewed 512 cases tracking repeat calls to law enforcement over a period of 12 months. The researchers found that women involved in DVHVI reported more positive feelings toward law enforcement and were more likely to call law enforcement again if they experienced another incident of IPV. The evaluation also found that Hispanic women served by Spanish-speaking advocate–officer teams were the most likely to utilize services and call law enforcement during subsequent incidents (Stover et al., 2009).
Stover, Berkman, Desai, and Marans (2010) conducted a longitudinal evaluation of the DVHVI model with a sample size of 107 women who had experienced IPV (52 treatment and 55 control). Participants were surveyed at 1, 6, and 12 months after the reported incident. The researchers found that women who received DVHVI services were more likely to use court-based services and seek mental health treatment for their children (Stover et al., 2010). Participants from all three of these studies were drawn from one community in New Haven, Connecticut, thereby limiting the generalizability of the results. In addition, while these researchers examined which families engaged in services and how services impacted the likelihood of the families engaging in further criminal justice and mental health services, the studies did not examine how the collaborative model was implemented. Therefore, further research is needed to understand the factors that contribute to the successes and challenges of collaborative criminal justice and community partnerships in addressing the needs of IPV victims and their children.
Multidisciplinary Collaborations
Given the importance of offender accountability and victim safety in IPV interventions, increasing attention has been given to the use of collaborative community responses. Collaboration between law enforcement, prosecutors, judges, parole and probation officers, IPV advocates, health and mental health providers, and child welfare advocates in response to IPV cases is becoming more common. Multidisciplinary collaborations have the potential to initiate system change by aligning agencies that have complementary skills and capacity to coordinate services and systems (Kreger, Brindis, Manuel, & Sassoubre, 2007).
To be successful, collaborators must invest in developing and implementing a shared vision and framework (Kreger et al., 2007). Focus and resources must be provided by all collaborating agencies to recruit staff with the right expertise, knowledge, and approach; provide joint training and team building; support and supervise staff; and monitor and evaluate services provided (Sloper, 2004). Collaborations also require constant clear communication across multiple levels within and across partnering agencies (A. Cameron & Lart, 2003; Sloper, 2004). Co-locating partner agencies increases the opportunities for communication and team building, thereby promoting cross-collaboration, understanding, and information sharing (Sloper, 2004). According to one study, there are seven factors needed for successful interagency collaboration, including (a) commitment, (b) communication, (c) strong leadership from key decision makers, (d) an understanding of the culture of collaborating agencies, (e) engagement in serious preplanning, (f) provision of adequate resources for collaboration, and (g) a minimization of turf issues (Johnson, Zorn, Tam, LaMontagne, & Johnson, 2003).
Although collaborative models to interventions are promising, collaborative work can be difficult to achieve for a number of reasons. Collaborative work requires a negotiation of philosophical differences between agencies, each of which brings different goals, principles, and values to the team (O’Connor, 2007). Collaborations in which there is a lack of clarity regarding roles and responsibilities, lack of consensus between team members, lack of commitment and resources from senior management, poor communication, little information sharing, and lack of trust and understanding among individuals and agencies often fail to achieve their desired outcomes (Johnson et al., 2003; Sloper, 2004). Furthermore, limited funding and staff turnover can make building momentum between partners difficult to achieve.
Despite the potential barriers to successful multidisciplinary collaborations, it is critical that we invest in developing and implementing collaborative intervention models in the field of IPV. Collaborative models can provide an integrative approach in addressing IPV, increasing safety and access to support for victims and their children, holding offenders accountable, and reducing the duplication of effort across agencies.
Description of the Child Trauma Response Team Intervention
The Child Trauma Response Team (CTRT) represents a partnership of The New York City Police Department (NYPD), The New York County District Attorney’s Office (DANY), the Mayor’s Office of Criminal Justice (MOCJ), and Safe Horizon, the nation’s leading crime victims’ organization. The goal of the CTRT is to provide a coordinated, immediate, trauma-informed, and interdisciplinary response to children below the age of 18 years and their impacted family members who are exposed to severe IPV.
The CTRT identifies children who have witnessed serious incidents of IPV and provides a swift interdisciplinary response to children and their caregivers to reduce the immediate and longer-term effects of witnessing such violence. The CTRT team reviews the domestic incident reports (DIRs) filed in the precinct to determine whether an incident of IPV is considered severe. If the domestic violence sergeant indicates on the DIR that a felony assault, misdemeanor assault, or criminal contempt was committed; or if there is a physical injury (such as strangulation); and the opposite party was or is an intimate partner, then the incident is considered a severe incident of IPV. Once a serious incident of IPV is identified and it is known that a child is present in the home, eligible families are contacted and offered a trauma-informed intervention that may include a coordinated home-based outreach by law enforcement and child trauma specialists, victim-centered case management services, and an evidence-based mental health intervention.
The CTRT is designed to perform the following functions: (a) Screen DIRs filed by law enforcement officers at the precinct and referrals made by the district attorney’s office. (b) Identify families with children who have been exposed to severe IPV. (c) Provide a therapeutic acute response to the family within 72 hr of the traumatic event consisting of a joint home visit by the domestic violence Police Officer and a Child Trauma Specialist. (d) Complete a child trauma screening and/or assessment. (e) Educate the caregivers about common reactions to trauma and how their children’s behavior may be linked to the children’s exposure to IPV. (f) Provide safety assessment and risk management planning for the family. (g) Provide the child and impacted family members with evidence-based mental health treatment services. (h) Conduct precinct-based trainings for patrol officers and detectives so they have a basic understanding of trauma symptoms and its impact on children; services available for families through this partnership; and assistance provided for families through evidence-based mental health treatment services. An additional responsibility of the Child Trauma Responders is to assess for child abuse. The Child Trauma Specialists are trained on assessing for co-occurring child abuse and, as mandated reporters, report cases to child welfare when child abuse cues are present. In addition, the child welfare system participates in case review meetings on as-needed basis and the child welfare liaison for the police department attends the quarterly steering committee meetings.
To identify children exposed to severe IPV, (a) the CTRT case manager reviews the domestic incident police reports (DIRs) to identify children who have been exposed to severe IPV, requests the history of IPV incidents in the household from the domestic violence Sergeant, and coordinates outreach attempts with the domestic violence sergeant and law enforcement officers and (b) the domestic violence sergeant and law enforcement officers and/or the District Attorney’s Office screen IPV incidents and coordinate with the CTRT team to facilitate outreach to families. The CTRT Case Manager reviews all IPV incident reports from the precinct daily and conducts outreach calls to each victim, while prioritizing victims of serious misdemeanor or felony offenses. Once a potential family is identified as having experienced severe IPV, the CTRT begins coordinating outreach via phone calls and home visits; additionally, the CTRT conducts daily consultations between program partners to discuss cases and coordinate responses and conducts biweekly case review meetings to further coordinate and discuss follow-up on cases. Once the CTRT team is able to successfully outreach to a family, one of the CTRT team members speaks to the victim (either via an outreach call, an in-person precinct interview, or a coordinated home visit with the Domestic Violence Police Officer or Sergeant). During this initial contact, the Case Manager and/or Child Trauma Specialist engages the victim, assesses the current safety risks of the victim and his or her children, provides brief individual supportive counseling and crisis intervention, provides information on criminal justice and/or social service processes and resources, and provides information about the CTRT program and services. If the victim is willing, the Child Trauma Specialist will discuss the child’s reaction to the IPV incident. During this section of the interaction, the Child Trauma Specialist conducts the Primary Care PTSD screen (the PC-PTSD Screen; R. P. Cameron & Gusman, 2003) to assess for potential indicators that the child may develop PTSD. The PC-PTSD screen consists of four items including the following:
Have had nightmares about it or thought about it when you did not want to?
Tried hard not to think about it or went out of your way to avoid situations that reminded you of it?
Were constantly on guard, watchful, or easily startled?
Felt numb or detached from others, activities, or your surroundings?
The goal of this screen is to engage the caregiver in a brief conversation about reactions their child(ren) may be experiencing following the IPV incident, to validate the caregiver’s experiences and provide psychoeducation on the impact of trauma, to explore concrete coping skills the family can use to manage post-trauma reactions, and to begin to identify and address the family’s immediate needs.
If the victim indicates that his or her child is experiencing at least one of the four screening items, then the Child Trauma Specialist will recommend the completion of a trauma assessment. If the victim is willing to complete a trauma assessment for his or her child, either at that time or by scheduling an additional phone and/or in-person meeting, the Child Trauma Specialist will utilize one of the following three validated trauma assessments: The Young Child PTSD Screen (Scheeringa, 2012), the Pediatric Child Distress Scale (Saylor, Swenson, Reynolds, & Taylor, 1999), or the Child PTSD Symptom Scale (Foa, Johnson, Feeny, & Treadwell, 2001). The goal of the trauma assessment is to further explore how the traumatic event has impacted the child(ren) and assess whether the child is at risk for developing PTSD. If the results of the trauma assessment indicate that the child is at risk for developing PTSD, then the Child Trauma Specialist will explore the possibility of mental health treatment for the child with the caregiver.
The aim of this study was to explore the feasibility of the CTRT, a coordinated, immediate, trauma-focused, and interdisciplinary response to children exposed to IPV. The CTRT model depends on building and maintaining effective interdisciplinary partnerships. Therefore, this study focused on understanding, from the perspective of the key stakeholders, what facilitated and/or hindered the collaborative approach.
Method
This study was initially conducted as part of a program evaluation examining the CTRT as it was piloted in one police precinct in a large, urban environment. Semi-structured interviews were conducted to explore the perceptions, values, and experiences of key administrators piloting the CTRT model. The interviews focused on the successes and challenges of the collaboration between law enforcement, the district attorney office, and the nonprofit organization and explored suggestions for potential replication efforts. The semi-structured interview guide was created by the research team, and reviewed and approved by each participating agency, to understand the following: (a) how the CTRT model was being implemented and the shifts each partnering agency needed to make in the implementation process, (b) how the CTRT partners collaborated in the CTRT model, (c) the strengths and areas for growth in the CTRT partnership, (d) the impact of the CTRT program, and (e) recommendations for replication of the model. Table 1 presents the semi-structured stakeholder interview guide.
Semi-Structured Stakeholder Interview Guide.
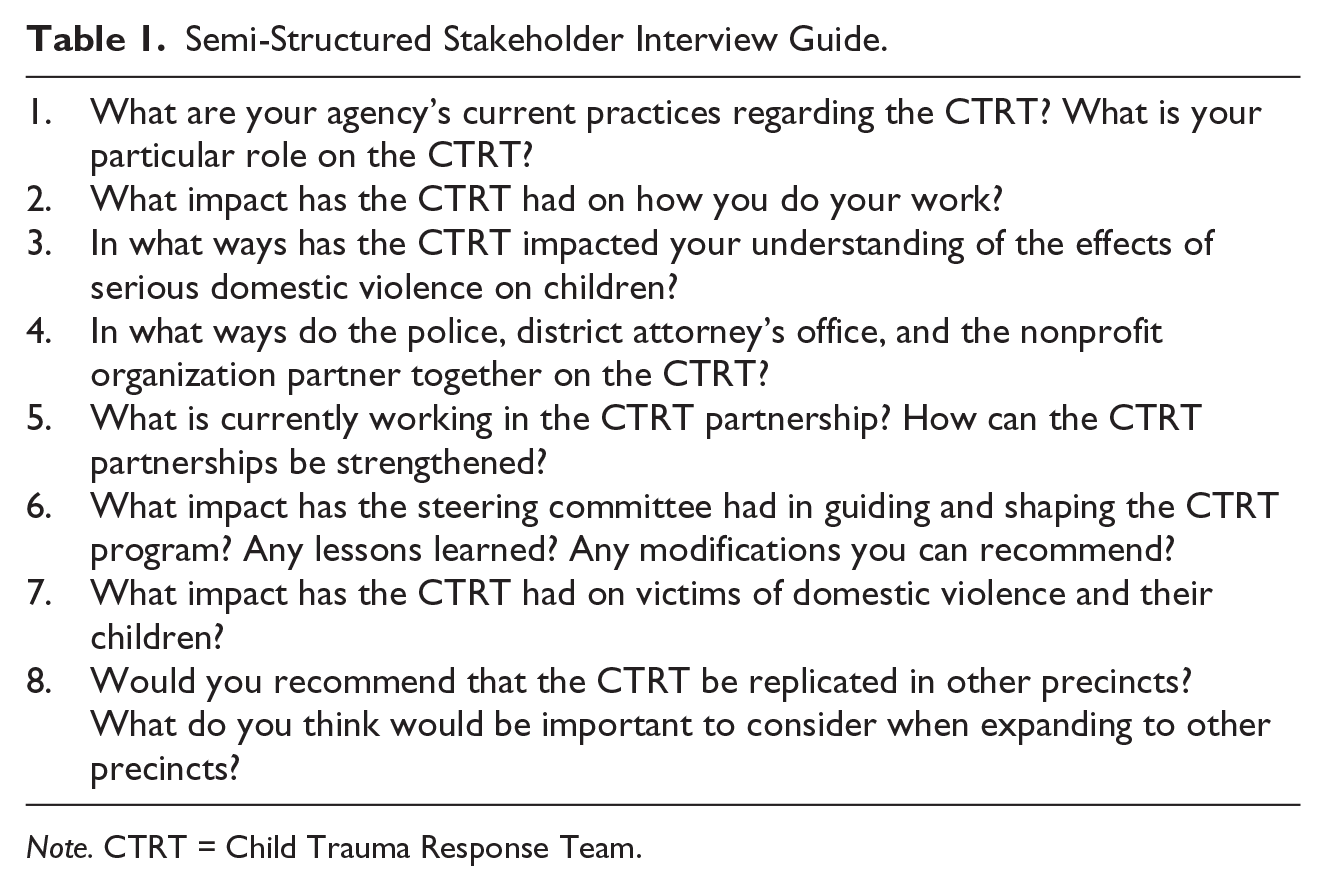
Note. CTRT = Child Trauma Response Team.
Data Collection
All core CTRT stakeholders were invited by the research team to participate in the interviews. In addition, the lead stakeholder from the funding office was invited to participate. All individuals asked to participate in the study agreed to participate. Interviews were conducted with 12 CTRT stakeholders of whom three worked for law enforcement, four worked for the district attorney’s office, four worked for the nonprofit organization, and one worked for the city office funding the pilot demonstration. To preserve the confidentiality of participants, no demographic information was collected.
The interviews occurred between January and April in 2017 and were between 40 and 70 min in length. All interviews took place at each stakeholder’s office and were conducted by two evaluators trained in conducting semi-structured qualitative interviews and experienced in the field of IPV. Consent for participation was obtained by reading a script (approved by each organization) which informed participants of the purpose, objectives, and methodology for the interviews. Participants were informed that while comments provided during the interview would not be personally attributed to the participant in any report or distribution of findings, that due to the small pool of participants, anonymity could not be guaranteed. Once participants provided verbal consent for the interview, participants were then asked to consent for the interview to be audio-recorded. For participants who did not consent to the recording, the interviewer took detailed notes. In total, seven participants (64%) were recorded and four participants (36%) were not recorded. After each interview, the evaluation team transcribed the interviews and transferred all recordings, transcription, and notes into de-identified, password-protected digital files.
Data Analysis
This project was originally completed as part of a process evaluation of the CTRT, and results were intended to provide stakeholders with a better understanding of the strengths and weaknesses of the program implementation and to inform next steps in the program’s expansion. As such, data analysis was conducted using grounded theory, an inductive method that utilizes an iterative process in which themes from the data are used to build a data-driven framework for understanding the phenomenon in question (Charmaz, 2006; Strauss & Corbin, 1998). Grounded theory requires that theories are constructed from data that have been systematically gathered and analyzed while recognizing the subjectivity inherent in qualitative data analysis. According to Strauss and Corbin (1998), “Grounded theories, because they are drawn from data, are likely to offer insight, enhance understanding, and provide a meaningful guide to action” (p. 12).
In accordance with the grounded theory approach, data were systematically reviewed and emerging themes were noted from each interview (open coding). After open coding was completed for all interviews, the interviews were reviewed to analyze relationships and evaluate the overlap of themes (axial coding). Finally, overarching themes within and across each set of codes and categories were identified. These themes were used to develop a model that presents the main factors that contributed to the successes of the CTRT pilot.
Trustworthiness and Credibility
The research team, consisting of two researchers experienced in conducting program evaluation and research in the field of victim services, were tasked by the CTRT to conduct a process evaluation that could be used to guide program implementation. As it is critical for qualitative researchers to focus on achieving trustworthiness and credibility about the subjects’ experiences (Hammersley, 1995), the researchers spent significant time with the CTRT program by attending quarterly Steering Committee meetings, bi-weekly case review meetings at the precinct, and weekly implementation planning meetings. By attending and observing a range of CTRT meetings, the researchers gained familiarity with the program implementation and with the culture of the CTRT team.
When conducting the interviews, the research team wanted the stakeholders to trust the research team to increase transparency and authenticity of the interview. To achieve this, the research team identified ways in which the stakeholders could have say throughout the research process. First, the stakeholders were asked to review and provide feedback on the interview guide. Second, the stakeholders were sent the interview guide prior to the interview to allow the stakeholders time to prepare their responses and to ensure a transparent research process. Third, to encourage honesty in the interview, the researchers explained to the stakeholders that no identifiable data would be released and no demographic questions would be asked. Fourth, each individual stakeholder was asked whether or not he or she was comfortable with the interview being audio-recorded. Fifth, once the results section was written, the stakeholders were each sent a copy of the results and asked to provide feedback. The research team believes that this collaborative process enhanced the credibility of the study.
Results
The CTRT pilot program evolved through a cyclical process including (a) implementing and enhancing program services, (b) defining and nurturing relationships between partners, and (c) shifting practices among partnering agencies (see Figure 1).
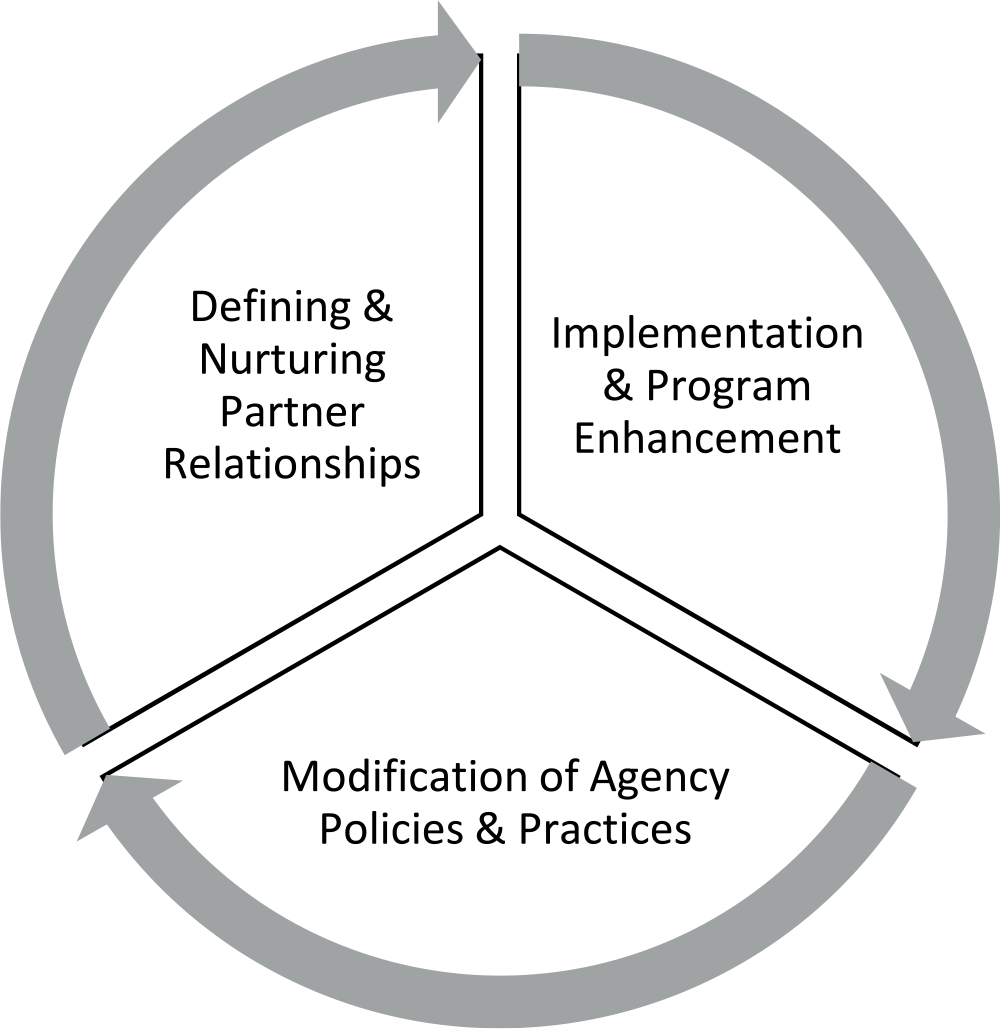
Implementation process of the child trauma response team.
To de-identify the stakeholders interviewed in this study, the following quotes will be identified by the department with PD for the police department, VS for the victim services organization, F for the funding agency, and DA for the district attorney’s office.
Implementation and Program Enhancement
The stakeholder interviews focused on understanding each of the partnering agencies’ practices regarding the CTRT to highlight the key components needed to ensure the program’s success. There were four main components of the model that facilitated the CTRT’s multiagency approach: the (a) co-location of partners, (b) case review meetings, (c) home visits, and (d) Steering Committee meetings.
Co-location of partners
The victim services case manager shared an office in the police precinct with the domestic violence police officers and sergeant. This co-location of law enforcement and victim services created the environment needed for a collaborative team and increased the speed with which the team could respond to severe IPV incidents:
We thought it was a great idea to put them in the same office with Domestic Violence. (1PD) The case manager is mainly at the precinct. . . The sergeant . . . is responsible for making sure that the [domestic violence incident reports] are available as soon as possible because we want to reach the families within 72 hours. (1VS)
Team members agreed that strong leadership in the precinct supporting the co-location was imperative to facilitating a smooth transition and fostering cohesion between the team members:
What’s critical is the leadership from the precinct. (2VS) My Sergeant . . . ensures that [the victim services team] is very welcomed in this precinct and we ensure all our officers make sure they feel that way as well . . . [The victim services team] know most of these cops . . . they feel very welcome and they feel part of the team. And that starts with the leadership in this precinct. . . . We see them [the victim services team] as staff members as well. (2PD)
Case review meetings
Case review meetings were a space carved out for the CTRT team to ensure regular communication on the status of active cases between all partners:
So upstairs is like a machine. They’re constantly working on what we have currently and those meetings are like ok let’s stop and review what we have, what we’re working on in the long term. (2PD)
All stakeholders recognized that case review meetings became more formal over the course of CTRT’s rollout. Out of necessity, early case review meetings were focused on relationship building, discussing CTRT processes, generating a shared understanding of the work, and reaching a consensus around the practical considerations of conducting CTRT activities. One stakeholder explained,
They were more just like kinda program meetings where . . . they would give maybe some update on cases but it wasn’t a formal case review meeting, you know, the Sergeant may do some mini training about, reviewing police report, crime categories, things like that. (2VS)
After laying a foundation, stakeholders ultimately agreed there was a need to impose more structure on the meetings. One stakeholder described how the case review meetings became more structured over time:
Now we know what we’re bringing to the table, ahead of time we know ok this is what we’re going to discuss . . . Whereas before, we were just like let’s just meet and we’ll talk . . . So we’re more prepared ahead of time. So it’s changed, and it’s gotten a lot better. (3PD)
One tool that pushed the case review meetings forward was the creation of a document outlining what information each agency needed to bring to case review meetings:
[There’s] more clarity in what everybody needs to do . . . The outline helped to see what everybody’s contribution was going to be in the meeting, and I think that by just dividing it, it helped everyone be prepared and to have the meeting just focused on the high risk [families]. (1VS)
All stakeholders identified the case review meetings as a critical venue for building and strengthening the partnership:
Strengthen the collaboration, it’s [the case review meetings] to discuss high risk cases, it’s been a good thing to do because you, not one program can carry a high risk case. (1VS) The purpose of those [case review] meetings is for everybody to come together and one address any concerns that we may have regarding a case, and another thing is for everyone to put their input in how we can better the program and to share the information that we have in terms of what we’re seeing, any progress that has been made with any families, any families we’re touching and helping out. You know, to share the success story and to see what we can do to further help these families. (3PD)
Stakeholders stated that case review meetings also created a space to bring up families who may have fallen off the team’s radar:
There was the [male adolescent participant] [the victim service agency] had been dealing with. When she brought it out to the table then it hit me, you know, let’s offer him a chance to join our explorer program . . . So that was an opportunity for, it’s kind of like, the ball was out of my court and then it was brought back to my court and I was able to further assist or come up with a suggestion of what else can we do for this kid. Great he got the therapy, he’s doing better, now what can we do to help him even more? So that’s a good thing—that’s one of the best things about those meetings. (3PD)
Beyond the utilitarian focus of the case review meetings, stakeholders also mentioned that the case review meeting was a place for team members to deepen partners’ understanding of one another’s roles and approaches to the work:
I think that’s really the true venue, um, even beyond some initial training where you really begin to shape each other’s views and responses to these individual cases, um, to kind of bring our different views alive. (3VS)
Home visits
Home visits were a critical piece of the CTRT model as they provided an opportunity for the team to provide coordinated services to children and their caregivers. One stakeholder explained that home visits were important because they gave the CTRT team the opportunity to talk to families in a setting outside of the police precinct:
When they go out they can get a live look at what the situation is at the home and actually speak to the child in a setting where the child’s comfortable. (1PD)
Though there was wide agreement among CTRT members that home visits were an important avenue for reaching families, early in the partnership there was some hesitation on the part of law enforcement related to taking civilians on home visits. One stakeholder noted,
I went on a few visits with [the victim services team] and with the domestic violence unit and obviously, naturally, the officers are like, oh this is a new thing. How does it work? You got [non-police] employees, they’re civilians, a private organization, so there was always this kind of question . . . we went through those challenges and all those and now . . . they work hand-in-hand and they definitely are working collaboratively. They are like one team. (2PD)
Once the team had time to build their relationships and trust, the CTRT worked to implement a home visit model that ensured the police department’s responsibilities were met while also ensuring the victim services staff had the space to engage the victim:
The officers take charge of the initial contact with the prospective client . . . We have a checklist, we have questions we have to ask, and then it’s a segue to CTRT to say they’re here for this, they’re here for the child . . . So it’s good to have that dynamic on the home visit—we take the lead and when we’re done doing what we have to do the introduction to CTRT is done. (1PD)
Home visits are a crucial venue for families to see the police department and the victim services organization working in collaboration:
When we have our staff from [the victim services team] and the Child Trauma Response Team in general, together as one unit, I think the families are a lot more responsive, . . . more inclined to talk to us and to follow up because . . . they feel more comfortable talking to the social service staff as opposed to the officers . . . So when we go to a household, it’s not just an arrest or a report, it’s more than that. It’s actually we wanna hopefully find ways or solutions to the problem in the household to prevent further violence as opposed to just being reactive. (2PD)
Steering committee meetings
All stakeholders expressed their belief in steering committee meetings as an important space for leadership to check in on the functioning of CTRT and troubleshoot as needed:
I am a strong believer in steering committees when you’re rolling out a new project . . . I think it’s important to have all the voices at the table to hear what’s going well, hear what the challenges are, and work on them together. (1F) [The Steering Committee meetings have] been a wonderful place . . . where are we, you know, really sifting through the volume, sifting through who’s engaged, sifting through what we’re doing . . . I also think bringing in actual case examples into every meeting of the steering committee has been helpful. (3VS) I’m a big person in accountability. It [the Steering Committee] holds everybody accountable to what’s happening and what you know, what isn’t happening that needs to happen. (2VS)
Though all stakeholders expressed a strong commitment to the usefulness of Steering Committee meetings, stakeholders noted that attendees at the Steering Committee meetings were, at times, hesitant and guarded:
[Steering Committee members are] being very careful around each other and maybe the trust isn’t quite there yet. (4VS) I wish there wasn’t so much tension. I feel a lot of tension. (1VS) Feels like maybe the wrong people are in the room for the steering committee meeting. The steering committee meetings do not feel like a true reflection of what’s actually happening in the program. Feels like a dog and pony show. (1DA) I would love it if we got to this place with the steering committee where we say look here’s the problem that we’re having can you guys use your considerable influence to help us figure out how to solve it or can you move any of this around for us? (4VS)
Relationship Building
A second theme that emerged in speaking with stakeholders was the critical need to focus on nurturing the partnership between team members. Numerous stakeholders had positive perceptions of the multidisciplinary team relationship:
From the first month to now we’re a lot more engaged, more interactive with each other, we see each other as partners as opposed to being separate entities. (2PD) But now they have a very, very good relationship. They’re always talking after the meeting, so I think that is has, it has strengthened the domestic violence program at the precinct in that they have someone first hand to talk to about cases. (1VS) Where I feel like I have somebody a step away that I can personally speak to and say this is what’s going on, what can we do? So it’s changed a lot . . . We’re just trying to—we all have that victims and those children—that’s our priority at the end of the day. (3PD)
Critical to this partnership was the free exchange of information about cases and supporting all partners in seeing the larger impact of their work:
Sometimes we work in silos . . . You got to get out of that silo . . . The biggest thing is just being able to understand and share information . . . that understanding that things work better when we share information because we can’t do it all. (1PD)
Stakeholders also spoke about the importance of learning about each other’s work, expertise, and resources:
Because we all come from different—we all have different functions and we all bring different attributes or contributions to that case so it’s interesting to see their ideas when they bring them to those meetings. (2PD)
All stakeholders stressed the importance of the multidisciplinary relationship for the success of the CTRT model and emphasized the time and effort needed to foster those relationships:
Developing the relationship . . . is the foundation of it all and starting with those introductions and those meetings and giving the [team] involved a good understanding of why this is important . . . There were a few times when . . . it’s like a little tense. [Developing cross agency relationships] is going to be a challenge and gonna take time and I think that’s been made clear at the steering committee that that is taking some time to develop but I would expect nothing less. And that, that’s sort of a challenge to getting this off the ground, to build those relationships, to make them strong, and that’s where you have to start from and that can take time. (1F) We’ve had some changes in leadership so that has impacted the steering committee because I think that whenever you have, whenever you’re trying to build relationships on an ongoing basis, if the membership is changing it really makes it hard to—because I’m going to do more for you if I feel a loyalty of allegiance to you and/or I’m going to feel comfortable coming to you and calling you if I need something and that can make a difference in the fact that we’re seeing each other on a regular basis. (1VS) I think what I underestimated was the power of relationships. Um, and the time that it takes and the reality of turnover that we face. It’s really the relationships and the partnerships which are going to make or break this project. (3VS)
Shifts in Organizational Practices
Creating and implementing the multidisciplinary CTRT team required all partnering agencies to shift areas of practice. Stakeholders commented on the need for partners to be open to change in the implementation phase, to view the CTRT as a critical component of their work, and to focus on the potential long-term impact of the model:
When the project was introduced I was open minded. I felt that it was needed . . . I also realize that this is the beginning stages and something like this is . . . is something where we’re going to see the benefits in the long run. (3PD)
Stakeholders described how participating in the CTRT model enhanced their focus on children witnessing severe IPV in their daily work:
It kind of opened our eyes a little bit . . . We’ve always went in and you go in sometimes and you’re taking mom and dad . . . kid may go to [child welfare], may go to a family member, and that was it . . . The child was kind of removed from the whole thing . . . We kind of did our job and that’s where we left it . . . We always came back to the adults, but we never came back to the children. So that’s something that’s new. You know, with the program coming in and saying, ‘Hey, wait a minute, let’s go back for the children.’ (1PD) I have to say the Child Trauma Response Team is definitely a success here cause a lot of times we do go into a household and there is a child there and I think in the past we just kind of neglected that . . . But now with the Child Trauma Response Team, I think we’re a lot more responsible and a lot more caring as a department but also providing those services so we’re not just there locking up or arresting their father or mother we’re actually there providing that additional service . . . Because the ultimate victim is the child. (2PD)
Stakeholders also discussed how participation in the CTRT team enhanced their team’s ability to engage with children exposed to severe IPV:
They’re following up and caring for this person—those kids. And they do it passionately . . . And they know them by a first name basis as opposed to—oh that kid from a number street or the building. No, they know him, they know who they are, they know his age, they know what school he attends. So it’s a more personal level I think—that’s the unique thing I think with the CTRT . . . That’s how I feel and it’s good for them because that’s what they want a lot of them—they all want to be there, they all want to feel like they’re doing something that is rewarding. (2PD) So, I think the Child Response Team has worked in terms of having, um, key players . . . really pay much closer attention to the impact of domestic violence on kids . . . To have people put children, kind of, back into the priority zone of. . . of who we should be paying attention to and responding to in domestic violence calls and incidents. (3VS) When I was an officer, and I’m pretty sure this is something that has gone through probably every officer you would speak with, you know, you respond to an incident where the mother assaults the father or the father assaults the mother and there’s children in the home and you’re always wondering . . . what happened to that child—does the child get assaulted? You wonder that, but as a patrol officer you’re on to the next job and like I said it wasn’t until I came to this unit that I had a chance to experience the aftermath of responding to the incident. But now if this program continues we’ll be able to—the officers won’t have that doubt in their mind anymore, now they’ll know ok as long as I document it CTRT is gonna take care of it. Someone’s gonna take care of this—it won’t just be up in the air anymore. (3PD)
Discussion
Children’s exposure to severe IPV impacts their development, physical health, mental health, and adult functioning (Holt et al., 2008). The collaborative CTRT model shows initial promise as a core service for children and their caregivers exposed to severe IPV. Although there are a range of services available to families experiencing IPV, we know that many families experiencing severe abuse never enter the doors of a victim service or mental health organization (McLaughlin et al., 2013; Roberts et al., 2010). Furthermore, for families seeking support after an IPV incident, the focus of services is typically on the adult victim and not on the child exposed to the violence. The CTRT model is an innovative model that conducts coordinated outreach to families experiencing severe IPV to enhance family engagement in services and, when appropriate, in the criminal justice process.
Multidisciplinary collaborations have the potential to initiate system change by aligning agencies that have complementary skills and capacities to coordinate services and systems (Kreger et al., 2007). The multidisciplinary approach to the CTRT model is a critical component to the model’s success. The CTRT pilot program evolved its partnership through the parallel processes of (a) implementing and enhancing program services, (b) defining and nurturing relationships between partners, and (c) shifting practices among partnering agencies.
To build the collaborative partnership, team members identified the importance of co-locating the victim services and law enforcement officers as critical to facilitating the communication of the team members and increasing the speed with which the team could respond to severe IPV incidents. Team members stressed the need for strong leadership in supporting the transition to a co-located model. This finding aligns with the literature that recommends co-locating partners to increase opportunities for communication and team building and thereby promoting cross-collaboration understanding and information sharing (Sloper, 2004).
The stakeholders identified the components critical to the success of the CTRT model, including case review meetings, home visits, and Steering Committee meetings. The biweekly case review meetings were a critical space to ensure regular communication on the status of active cases between all CTRT partners. The home visits, which were conducted collaboratively with the victim services and law enforcement officers, provided a coordinated service to children and their caregivers and an opportunity for families to connect with CTRT services. Finally, the Steering Committee meetings were an important space in the pilot for leadership to check in on the functioning of the CTRT and troubleshoot as needed.
Although the team reported increasing collaboration between partners throughout the pilot, many team members also reported sensing hesitation and mistrust during the Steering Committee Meetings. Researchers have found that collaborations require constant and clear communication across multiple levels within and across partnering agencies (A. Cameron & Lart, 2003; Sloper, 2004). Related to these hesitations, stakeholders pointed out the importance of investing in learning about each other’s work, expertise, and resources and stressed the importance of the team committing to a continual focus on relationships and finding ways to better collaborate with each other.
Despite hesitations, stakeholders commented on their positive perceptions of the multidisciplinary team and the importance of the free exchange of information about cases. Stakeholders emphasized that the success of the CTRT model relied on each agency shifting and aligning their practice model (Kreger et al., 2007) to collaborate across the multidisciplinary team and to heighten each agency’s focus on the children’s exposure to the IPV incident.
Implications and Future Directions
The results of this study suggest that a criminal justice and community-based collaborative intervention designed to support IPV victims and their children is a promising program model warranting future program development and research. Although developing and implementing multiagency collaborative models is challenging, especially when the partners bring different philosophical approaches to the work (O’Connor, 2007), this qualitative feasibility study found that the CTRT model was effectively implemented utilizing a law enforcement, district attorney, and victim services collaboration. Based on these initial findings, local and state criminal justice agencies should consider the feasibility of implementing collaborative models designed to reach children exposed to severe IPV. In developing such models, each jurisdiction must find ways to adapt the model to the needs of their community. Decisions must be made about which partners to include in the model, what crime types will warrant a collaborative team response, and how the program can be implemented with available resources. Jurisdictions looking to develop CTRTs need to focus on how to utilize the team to increase the speed with which the partners access and engage families in services and how to provide and/or modify coordinated responses and services to meet the cultural needs of the community. Furthermore, in developing and nurturing the collaborative relationships, CTRTs must invest time and resources in the partnership, define and clarify roles of each partner, enhance communication and understanding between team members, and develop and implement CTRT protocols for case review meetings, home visits, and steering committee meetings.
There are many areas of further study in identifying how to enhance the collaborative model and in evaluating the impact of the model. Research is needed to explore the implementation of CTRTs across a variety of settings and among diverse communities. Research is also needed to explore how the addition or removal of different stakeholders impacts the functioning and success of the model. For example, how would the inclusion of child welfare partners impact the team’s functioning? In addition, research can further explore the impact of the collaboration on each of the partnering agencies. Did participation in the CTRT model increase partners’ knowledge of child trauma, trust in partnering agencies, and the implementation of collaborative interventions?
It would be also be valuable to explore the impact a family’s engagement with CTRT services has on a range of criminal justice and mental health outcomes. Research is needed to examine whether engagement with the CTRT program decreases child and caregiver’s PTSD symptoms and/or increases the caregiver’s ability to recognize and address PTSD symptoms in his or her child. Research is needed to examine whether participation in the CTRT model increases the families’ knowledge of and access to community and mental health resources, engagement in safety planning activities, and knowledge and utilization of emotional coping skills. Longitudinal studies are needed to understand the impact engaging in the CTRT intervention has on families experiencing IPV.
Limitations
This study is a qualitative exploration designed to inductively broaden conceptual understanding and guide future research. The qualitative questions used were broad and subjective in nature, and only stakeholders from one urban multidisciplinary model were included in the study. Findings must be understood within the context of one multidisciplinary team providing services to children and families in one urban community. An additional limitation to the generalizability of the study is that this model did not include representatives of the child welfare system as full stakeholders in the collaboration.
Another key limitation to the study was that only 64% of the interviews were recorded. Stakeholders were asked permission to record the interviews; however, four stakeholders denied. To address this limitation, the researchers took detailed notes throughout the interview; however, without the audio recording, the data contain credibility concerns. Thus, further research is needed to examine whether the findings could be replicated and to determine whether the findings are generalizable to the greater population of multidisciplinary teams.
Conclusion
Although collaborative models are promising, collaborative work can be difficult to achieve for a number of reasons. Collaborative work requires a negotiation of philosophical differences between agencies, each of which brings different goals, principles, and values to the team (O’Connor, 2007). Despite the potential barriers to successful multidisciplinary collaborations, it is critical that we invest in developing and implementing collaborative intervention models in the field of IPV as these models can provide an integrative approach in addressing IPV, minimizing the duplication of services to families, holding offenders accountable, and advocating on behalf of victims and their children.
Footnotes
Acknowledgements
The Child Trauma Response Team and this research would not have been possible without the hard work and expertise of many people. We would like to thank the following agencies for their support: the Mayor’s Office of Criminal Justice, the Manhattan District Attorney’s Office, the New York City Police Department, and Safe Horizon, Inc.
Authors’ Note
Points of view or opinions contained within this document are those of the author and do not necessarily represent the official position or policies of the New York City Police Department.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Mayor’s Office of Criminal Justice.