
Abstract
Adult sexual assault (ASA) has been linked to numerous negative psychological and behavioral outcomes. Recent research suggests that postassault adaptation may differ based on how the victim conceptualizes their ASA. For instance, women who label their rape experiences as such (i.e., acknowledged rape victims) report worse mental health symptoms than women who do not (i.e., unacknowledged rape victims). To date, this literature has focused exclusively on heterosexual women. Relative to heterosexuals, sexual minority women (SMW) are at greater risk for sexual assault and report worse postassault outcomes, yet little is known about rape acknowledgment in this at-risk population. Moreover, it is unclear how distal factors, such as childhood sexual abuse (CSA), may influence SMW’s rape acknowledgment following ASA. A total of 205 self-identified lesbian and bisexual women were categorized into four groups (no ASA, ASA that did not involve rape, rape acknowledged, rape unacknowledged) and compared across mental health and drinking outcomes. Roughly, 42% of the sample experienced rape, and of those, 60% were acknowledged rape victims. Results revealed no statistical differences between acknowledged and unacknowledged rape victims in terms of mental health or alcohol use. However, relative to comparison groups, SMW who were acknowledged rape victims reported greater mental health symptoms, and both acknowledged and unacknowledged rape victims reported greater hazardous drinking. Among SMW with rape histories, greater CSA severity increased the probability of acknowledging rape. These findings provide valuable information regarding SMW’s postassault adaptation and can contribute to interventions to assist SMW who experience sexual assault.
Introduction
Adult Sexual Assault (ASA) in Sexual Minority Women (SMW)
Sexual assault refers to a range of unwanted experiences from nonconsensual sexual contact to completed rape. Numerous studies have linked ASA, particularly rape, to deleterious psychological and behavioral outcomes, such as depression, posttraumatic stress disorder, and heavy drinking (Klump, 2006; Miranda, Meyerson, Long, Marx, & Simpson, 2002; Resick, 1993; White House Council on Women and Girls, 2014). Relative to heterosexual women, SMW (i.e., lesbians and bisexuals) are at elevated risk for ASA (Balsam, Beauchaine, Mickey, & Rothblum, 2005; Hequembourg, Livingston, & Parks, 2013; Hughes, McCabe, Wilsnack, West, & Boyd, 2010). For instance, in a national sample, 16% of lesbian and 17% of bisexual women experienced a completed rape during adulthood compared with 8% of heterosexual women (Balsam et al., 2005). In a large-scale review, Rothman, Exner, and Baughman (2011) found rates of ASA in upward of 50% in SMW, with lifetime sexual assault as high as 85%. In general, SMW tend to report higher distress and drinking relative to heterosexual women (Gonzales, Przedworski, & Henning-Smith, 2016; Kerr, Ding, Burke, Ott-Walter, 2015; Reed, Prado, Matsumoto, & Amaro, 2010). These differences are especially notable when it comes to SMW’s adaptation following ASA (Institute of Medicine, 2011; Sigurvinsdottir & Ullman, 2016). Thus, SMW represent an at-risk population, both in terms of assault vulnerability and harmful postassault outcomes. Understanding the factors that influence postassault adaptation in SMW remains a priority in order to improve the longer term functioning in this understudied group.
Rape Acknowledgment
Rape is typically defined as sexual intercourse that is obtained by threat, force, or incapacitation (Abbey, BeShears, Clinton-Sherrod, & McAuslan, 2004). Almost two thirds of rape victims do not label their assault as such, despite reporting experiences consistent with the definition of rape (Kahn, Jackson, Kully, Badger, & Halvorsen, 2003; Layman, Gidycz, & Lynn, 1996; Littleton, Axsom, Grills-Taquechel, 2009; McMullin & White, 2006). This is important because labeling can greatly influence how an individual makes sense of what happened. According to Match-and-Motivation Theory (Peterson & Muehlenhard, 2011), the labeling of rape may depend on the “match” between an individual’s experience and their cognitive representation of rape (e.g., rape scripts) as well as the “motivation” to label (e.g., labeling has greater positive consequences than negative ones). With greater match and motivation, women may be more likely to acknowledge rape after it has happened. Interestingly, acknowledgment also appears to have implications for postassault adaptation. For instance, women who label their rape experiences as such (i.e., acknowledged rape victims) report greater psychological symptoms compared with women who do not (i.e., unacknowledged rape victims; Layman et al., 1996; Littleton et al., 2009; Littleton & Henderson, 2009; McMullin & White, 2006). Conversely, unacknowledged rape victims are at greater risk for hazardous drinking and revictimization compared with acknowledged rape victims (Littleton et al., 2009). Notably, this literature has focused exclusively on the rape experiences of heterosexual women. This is a considerable limitation given that rates of ASA are elevated among SMW (Balsam et al., 2005; Hequembourg, Livingston, & Parks, 2013; Hughes et al., 2010) and SMW report greater postassault distress and heavy drinking (Hequembourg, Livingston, & Parks, 2013; Hughes et al., 2010; Sigurvinsdottir & Ullman, 2016). Examining rape acknowledgment in this population may help to explain some of the mental health and drinking disparities found in SMW compared with heterosexuals. This is of critical importance and has the potential to inform screening and intervention efforts aimed at reducing SMW’s negative postassault outcomes.
Childhood Sexual Abuse (CSA) and Rape Acknowledgment
Few studies have explored the factors that contribute to rape acknowledgment, and of those, the focus has largely been on proximal variables such as assault characteristics (i.e., physical force, resistance at the time of the assault; Cleere & Lynn, 2013; Littleton et al., 2009; McMullin & White, 2006). Less is known about the distal factors that may play a role in women’s labeling of rape. CSA is one such distal variable that may provide insight into this process. Early sexual experiences are thought to influence an individual’s perceptions of sexuality (i.e., sexual scripts or schemas) in ways that might shape or help make sense of subsequent sexual experiences (Gagnon & Simon, 1973), both wanted and unwanted. Consistent with Match-and-Motivation Theory, unwanted sexual experiences in childhood, especially ones that were more severe (e.g., childhood rape), might increase the likelihood of acknowledging rape when also experienced in adulthood because there is greater match in experience and script. To date, only one study has examined CSA as a predictor of women’s rape acknowledgment following ASA. In a sample of heterosexual college women, Wilson and Scarpa (2015) found that, after controlling for dysfunctional personality traits, less severe CSA was associated with a greater likelihood of being an unacknowledged rape victim. The association between CSA severity and acknowledgment status is particularly important given the link between acknowledgment and differential outcomes (e.g., Layman et al., 1996; Littleton et al., 2009; Littleton & Henderson, 2009; McMullin & White, 2006). Relative to heterosexual women, SMW experience CSA at higher rates (CSA prevalence: 44% of lesbians, 48% of bisexual women, 30% of heterosexual women; Balsam et al., 2005) and report more severe CSA (childhood rape: 28% of lesbians, 24% of bisexual women, 17% of heterosexual women; Balsam et al., 2005). CSA is also a well-established predictor for revictimization in adulthood for SMW (Balsam et al., 2005; Hequembourg, Livingston, & Parks, 2013). Therefore, further research is needed to improve our understanding of how CSA severity may influence rape acknowledgment in this vulnerable population.
The Present Study
Despite the referenced literature, which suggests that rape acknowledgment may differentially influence postassault outcomes in heterosexual women, no known studies have examined rape acknowledgment in SMW. This is a significant gap as SMW are more likely to be sexually assaulted and experience poorer postassault adaptation (Balsam et al., 2005; Hughes et al., 2010; Institute of Medicine, 2011; Sigurvinsdottir & Ullman, 2016). Thus, understanding SMW’s rape acknowledgment may provide greater insight into why this understudied group experiences worse outcomes. Based on prior research with heterosexual women (e.g., Layman et al., 1996; Littleton et al., 2009; McMullin & White, 2006), we hypothesized the following:
We were also interested in the distal factors that may predict rape acknowledgment, and thus, we hypothesized the following:
Method
Participants and Procedures
The current study was drawn from a larger study on sexual assault and substance use in sexual minority men and women (Hequembourg, Livingston, & Parks, 2013). Participants were recruited using a modified respondent-driven sampling approach (Heckathorn, 1997) and from advertisements and flyers distributed in a medium-sized city in the northeastern United States. Interested participants were instructed to call and were screened over the phone by trained research staff. Eligibility criteria included being between the ages of 18 and 35 years and self-identifying as gay, lesbian, or bisexual. Transgender men and women were ineligible for the study. As part of the larger study, eligible sexual minority men and women (N = 410) completed an in-person session that involved interviews and self-report questionnaires. Participants were compensated with US$50 for their time. Since women experience ASA at higher rates than men (Elliott, Mok, & Briere, 2004), the current study focused solely on women from the larger study. This included 205 self-identified SMW (98 lesbians and 107 bisexual women). Ethnic composition of female participants was 66% White (n = 135), 21% African American (n = 43), 7% as Multiracial (n = 14), 5% Hispanic (n = 10), and 1% as “Other” (n = 3). The mean age of the sample was 24.47 years (SD = 4.39). On average, participants reported 13.75 years of education (SD = 2.83) and 84% had annual incomes below US$25,000. No demographic differences were found when ASA groups (no ASA, ASA no completed rape, rape acknowledged, rape unacknowledged) were compared (ps = .084-.739)
Measures
Sexual assault
CSA
Six items (adapted from Finkelhor, Hotaling, Lewis, & Smith, 1990; Miller, Downs, & Testa, 1993; current study α = .88) were used to assess unwanted sexual experiences in childhood (before age 14). Items inquired about a range of experiences from sexual exposure (one item; for example, “A person showed his or her genitals to you or you showed your genitals to the other person”), sexual touching (three items; for example, “A person touched your genitals, either with their hands or mouth, or you touched the other person’s genitals, either with your hands or mouth”), and sexual penetration (two items; for example, “A man inserted his penis into your vagina or anus”). Response options for each item were 0 = no or 1 = yes. Responses were then recoded to reflect women’s most severe CSA experience (CSA severity: 0 = no CSA, 1 = sexual exposure, 2 = sexual touching, 3 = sexual penetration).
ASA
The ten item Sexual Experiences Survey–Short Form Victimization (SES-SFV; Koss et al., 2007; current study α = .94) was used to assess unwanted sexual experiences in adulthood (after age 14). The SES-SFV included behavioral-based items measuring unwanted sexual contact (e.g., “Someone fondled, kissed, or rubbed up against the private areas of my body [lips, breast/chest, crotch, or butt] or removed some of my clothes without my consent”), attempted rape (e.g., “Even though it did not happen, a man TRIED to put his penis into my vagina, or someone tried to stick in fingers or objects without my consent”), and completed rape (e.g., “A man put his penis into my vagina, or someone inserted fingers or objects without my consent”). Response options ranged from 0 = 0 times to 3 = 3+ times. A single item at the end of the questionnaire directly asked participants whether they had ever been raped with response options dichotomized (0 = no, 1 = yes). Women’s responses to the behavioral-based questions and the direct rape inquiry were combined to produce four, nonoverlapping groups: (a) women who reported no ASA, (b) women who reported ASA that did not include completed rape, (c) women who endorsed the behavioral-based items related to completed rape and acknowledged they had been raped (i.e., acknowledged rape victims), and (d) women who endorsed the behavioral-based items related to completed rape but did not acknowledge they had been raped (i.e., unacknowledged rape victims). Based on procedures used in the literature (e.g., Koss et al., 2007), group membership was based on the most severe ASA experience reported on the behavioral items. For instance, if a woman reported unwanted sexual contact and an acknowledged rape, she was placed into the “acknowledged rape victim” group.
Mental health and drinking behaviors
Psychological symptoms
The Brief Symptom Inventory (Derogatis & Melisaratos, 1983; 18 items, current study α = .94) was administered to measure psychological distress in the past 12 months. Response options ranged from 0 = not at all to 4 = extremely. Subscales included depressive (α = .90), anxiety (α = .89), and somatization symptoms (α = .82).
Hazardous drinking
The Alcohol Use Disorders Identification Test (Barbor, Higgins-Biddle, Saunders, & Montero, 2001; 10 items, current study α = .88) was administered to identify hazardous patterns of drinking in the past 12 months. Items include questions on alcohol consumption and dependence symptoms. Response options ranged from 0 = never to 4 = daily or almost every day. Total scores were computed, with higher scores indicating more hazardous drinking.
Heavy drinking days
Participants reported on daily alcohol use in the past 6 months via the Timeline Follow-Back interview (TLFB; Sobell & Sobell, 1992). The TLFB is a widely utilized calendar-assisted interview that cues memory to improve recall of drinking behaviors. For the current study, participants were directed through a series of targeted questions by trained research staff to aid them in recalling the past 180 days of drinking (and other behaviors not relevant for the current study). Participant responses were used to compute the total number of heavy episodic drinking days, that is, days where women drank four or more drinks on a single day.
Results
Are There Sexual Identity Differences in Rape Acknowledgment?
In our sample of SMW, 71% (n = 146) endorsed a history of ASA, while 29% (n = 59) did not. Chi-square analyses indicated marginally significant differences in ASA history based on sexual identity, χ2(1, N = 205) = 3.20, p = .073, suggesting a trend for bisexuals to be more likely to report an ASA history than lesbians (44% lesbians vs. 56% bisexuals). Roughly 42% (n = 87) experienced rape during adulthood. Of those with rape histories, 60% (n = 52) were acknowledged victims and 40% (n = 35) were unacknowledged victims. Four groups were identified to reflect ASA and acknowledgment status: (a) no ASA (29%, n = 59), (b) ASA that did not include completed rape (28%, n = 57), (c) acknowledged rape victims (26%, n = 52), and (d) unacknowledged rape victims (17%, n = 35). Chi-square analyses indicated significant sexual identity differences in ASA group membership, χ2(3, N = 203) = 11.42, p = .010. Compared with bisexuals, more lesbians were found in the no ASA (35% lesbians vs. 24% bisexuals) and the ASA that did not include completed rape (33% lesbians vs. 24% bisexuals) groups. Similar percentages were present in the unacknowledged rape group (17% lesbians vs. 18% bisexuals), but there were twice as many bisexuals in the acknowledged rape group than lesbians (16% lesbians vs. 35% bisexuals).
Does Rape Acknowledgment Impact SMW’s Postassault Outcomes?
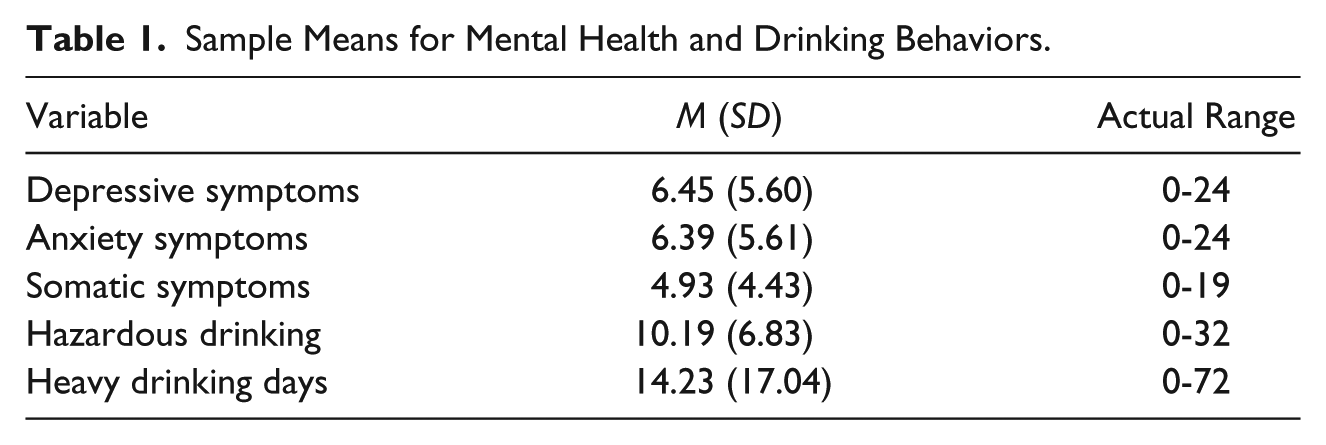
Table 1 provides means, standard deviations, and ranges for mental health and drinking variables for the full sample. We hypothesized that (1a) SMW who were acknowledged rape victims would report greater mental health symptoms relative to unacknowledged victims and comparison groups and (1b) SMW who were unacknowledged rape victims would engage in greater hazardous drinking relative to acknowledged victims and comparison groups. MANCOVA was conducted to examine differences in mental health and drinking behaviors across the four ASA groups after controlling for sexual identity. Results (see Table 2) indicated significant group differences in most study outcomes, F(15, 535) = 2.52, p = .001, Wilks’s λ = .829, partial η2 = .061. For mental health symptoms, differences were found for depressive symptoms, F(3, 198) = 4.15, p = .007, and somatic symptoms, F(3, 198) = 5.67, p = .001, with marginally significant differences noted for anxiety, F(3, 198) = 2.30, p = .079. Acknowledged and unacknowledged rape victims did not differ on depressive (p = .571) or anxiety symptoms (p = .195), but a trend was present for somatic symptoms (p = .066). Acknowledged victims also reported greater depressive, anxiety, and somatic symptoms compared with no ASA (ps < .05) and ASA that did not include completed rape (ps < .05). Unacknowledged victims reported greater depressive symptoms relative to no ASA (p = .042) and ASA that did not include completed rape (p = .048), but no differences were found for anxiety (ps = .380-.527) or somatic symptoms (ps = .152-.181).
Sample Means for Mental Health and Drinking Behaviors.
Group Differences in Mental Health and Drinking Behaviors.
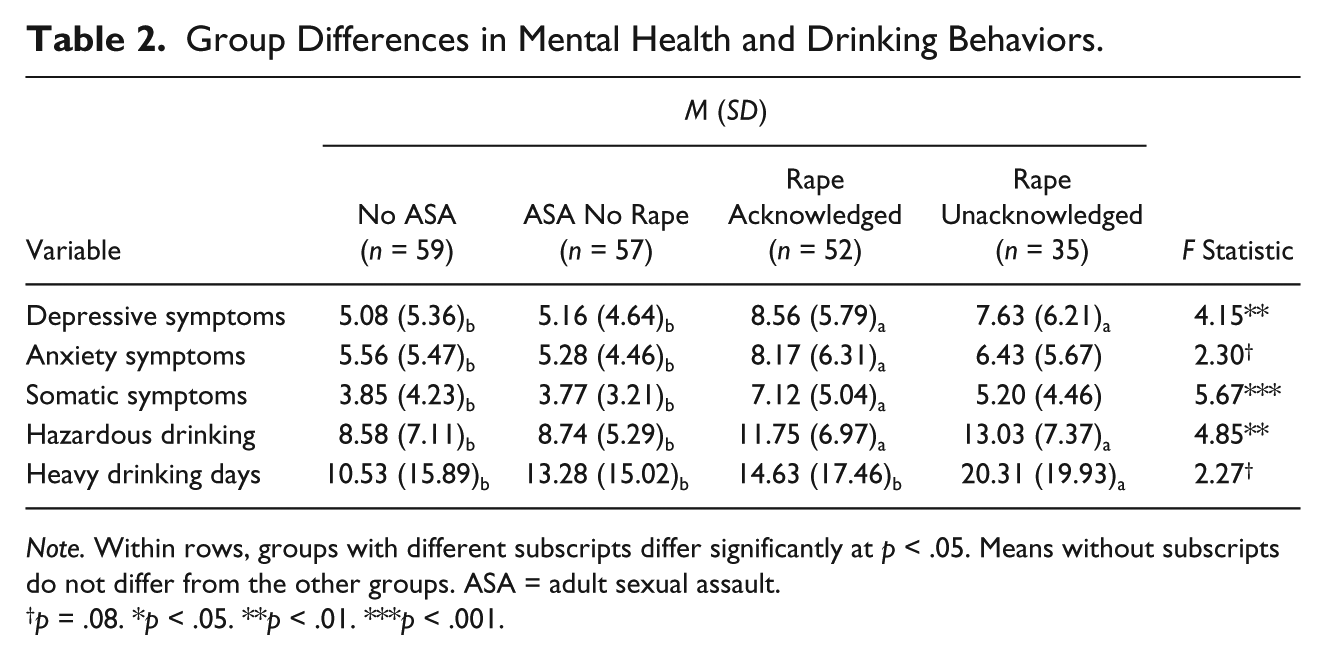
Note. Within rows, groups with different subscripts differ significantly at p < .05. Means without subscripts do not differ from the other groups. ASA = adult sexual assault.
p = .08. *p < .05. **p < .01. ***p < .001.
Results (see Table 2) also indicated significant group differences on hazardous drinking, F(3, 198) = 4.85, p = .003, and a trend for number of heavy drinking days, F(3, 198) = 2.27, p = .082. Acknowledged and unacknowledged rape victims did not statistically differ from one another in hazardous drinking (p = .374). However, acknowledged victims reported significantly higher hazardous drinking scores compared to women with no ASA (p = .017) and ASA that did not include completed rape (p = .025). Similarly, unacknowledged victims reported significantly higher hazardous drinking scores compared to women with no ASA (p = .002) and ASA that did not include completed rape (p = .003). For heavy drinking days, the pattern suggested a trend toward unacknowledged victims reporting more heavy drinking days compared with no ASA (p = .010) and marginally more heavy drinking days than ASA that did not include completed rape (p = .069) and acknowledged rape victims (p = .084). No differences were found in heavy drinking days when acknowledged rape victims were compared with no ASA and ASA that did not include completed rape (ps = .375-.950).
Does CSA Predict SMW’s Rape Acknowledgment Following ASA?
To test whether more severe CSA histories predicted rape acknowledgment, we limited the sample to those who experienced completed rape during adulthood (n = 87). Of this subsample, 63% (n = 55) endorsed a history of CSA, while 37% (n = 32) did not. Of those with CSA histories (n = 57), 8% (n = 7) reported sexual exposure, 20% (n = 17) sexual touching, and 36% (n = 31) sexual penetration as their most severe experience in childhood. Controlling for sexual identity, logistic regression was conducted with CSA severity as a predictor of rape acknowledgment following ASA (0 = unacknowledged status, 1 = acknowledged status). This model was significant, χ2(4, N = 87) = 18.47, p = .001, correctly classified 67% of the rape acknowledgment cases and explained a sizable amount of variance in rape acknowledgment (19% Cox & Snell R2; 26% Nagelkerke R2). Results indicated that sexual identity was not a significant predictor of rape acknowledgment (p = .372), but greater CSA severity increased the probability of acknowledging rape in adulthood (p = .002). That is, the odds of a SMW labeling rape was 7.90 times greater if she experienced more severe sexual abuse in childhood (confidence interval [CI]: [2.21, 28.33]).
Discussion
ASA has been linked to a host of negative psychological and hazardous drinking outcomes (Klump, 2006; Miranda et al., 2002; Resick, 1993; White House Council on Women and Girls, 2014). Research with heterosexual women suggests that postassault adaptation may differ based on how the victim conceptualizes their ASA (Cleere & Lynn, 2013; Littleton et al., 2009; McMullin & White, 2006). SMW are at elevated risk for ASA and experience worse postassault adaptation relative to heterosexuals (Hequembourg, Livingston, & Parks, 2013; Hughes et al., 2010; Sigurvinsdottir & Ullman, 2016), yet little is known about how rape is conceptualized in this at-risk population.
In this study of SMW, we found that 42% of our sample experienced rape during adulthood. Although most research with SMW does not typically break down ASA by severity, the rate of adult rape in our sample was similar to those previously reported (~30%-40%; Balsam et al., 2005; Gilmore et al., 2014). Of the SMW with rape histories, 60% labeled their rape experience as such (i.e., acknowledged rape victims), while 40% did not (i.e., unacknowledged rape victims). To our surprise, rape acknowledgment in this study was much higher than reported in heterosexual samples (~33%; for example, Kahn et al., 2003; Littleton et al., 2009; McMullin & White, 2006). Although our sample size precluded us from examining rape acknowledgment and postassault outcomes separately by sexual identity, we did find over twice as many bisexuals than lesbians in the rape acknowledged group. This was surprising, as we expected that—because bisexual women often partner with men—they would be more similar to heterosexual women than lesbian women in their acknowledgment patterns. Cultural depictions of rape are heteronormative, assuming heterosexuality because the majority of sexual assaults involve male perpetrators and female victims. Therefore, sexual identity has historically been invisible in sexual assault research. However, a growing number of studies have identified higher rates of lifetime sexual assault in SMW (Balsam et al., 2005; Ford & Soto-Marquez, 2016; Hughes et al., 2010), with bisexual women at greater odds of victimization (Lehavot, Molina, & Simoni, 2012). These studies underscore the need to include sexual identity when assessing sexual assault. Furthermore, because these studies rely on behavioral-based questions that do not require women to acknowledge their experiences as sexual assault, we know little about women’s labeling of rape. The current study suggests that bisexual women may be more likely to acknowledge rape than lesbian women. The reasons for this are beyond the scope of the current article and deserve greater attention in future research, but it is possible that bisexual women are more likely to acknowledge rape because they have experienced more sexual trauma over their lifetimes. In addition, bisexual women often partner with men and cultural depictions of rape may better fit with their own experiences, thus providing a script by which they interpret rape in adulthood. This coincides with Peterson and Muehlenhard’s (2011) research, which argues that women’s labeling of rape may depend on the match and motivation to label, with match conceptualized as the link between the individual’s experience of rape and their cognitive representation of rape. Rape scripts, or cognitive representations of what individuals typically think of when referring to rape, include characteristics of perpetrators and victims (Crome & McCabe, 2001). In most cases, these prototypes involve male perpetrators. In the real world, similar to heterosexual victims (e.g., Blayney & Read, 2018), lesbian and bisexual’s ASA tend to involve male perpetrators, ones who are generally known to the victim. In addition, many SMW report that they experience ASA prior to coming out (Hequembourg, Livingston, & Parks, 2013). As theorized, changes in the incident-label match can also occur over time (Peterson & Muehlenhard, 2011). It may be that, over time, discussing life experiences (including sexual assault) with female intimate partners gives SMW a different perspective on unwanted sexual experiences with men during adulthood, although further investigation is greatly needed to clarify why SMW may be more likely to acknowledge rape. Attention to the unique experiences among SMW (e.g., bisexual vs. lesbian) also is warranted.
Contrary to our hypotheses, we found no significant differences in mental health symptoms between SMW who were acknowledged and unacknowledged rape victims. In other words, both groups were high in distress. Although some studies with heterosexual samples have reported similar findings (e.g., Frazier & Seales, 1997; Littleton, Axsom, Breitkopf, & Berenson, 2006), these results run counter to the argument suggested by others that not acknowledging rape may serve a protective function against negative outcomes like distress (Peterson & Muehlenhard, 2011; Wilson & Scarpa, 2015). As expected, acknowledged rape victims reported greater psychological symptoms relative to comparison groups (no ASA, ASA no completed rape). This was also true among unacknowledged rape victims and comparison groups for depression. Rape is a potent psychological stressor and has been linked to poorer mental health outcomes (Classen, Palesh, & Aggarwal, 2005). Our findings suggest that it may be the experience of rape for SMW, rather than how it was conceptualized, that is more reflective of current distress.
Unlike Littleton et al. (2009), we did not find differences between acknowledged and unacknowledged rape victims in terms of hazardous drinking. Within the larger literature, studies have consistently shown that SMW drink at higher rates than heterosexual women (Drabble, Midanik, & Trocki, 2005; Green & Feinstein, 2012; Wilsnack et al., 2008). For our study, it may be that the heavier drinking patterns typical of this population, in combination with smaller group sizes, masked the drinking differences between rape acknowledged and unacknowledged victims that have been found in other studies. However, both acknowledged and unacknowledged victims engaged in greater hazardous drinking relative to comparison groups (no ASA, ASA no completed rape). The higher levels of distress and drinking in both rape groups may be a reflection of self-medication processes through which rape victims in particular are attempting to alleviate psychological distress with alcohol (e.g., Miranda et al., 2002).
Finally, few studies have explored the distal factors that contribute to rape acknowledgment in adulthood. In support of our final hypothesis, we found that more severe CSA increased the likelihood that SMW who experienced rape in adulthood would label it as rape. In fact, SMW with more severe CSA histories were almost 8 times more likely to acknowledge rape following ASA. Given that early sexual experiences are posited to influence an individual’s perceptions of sexuality (Gagnon & Simon, 1973), it makes sense that severe CSA would alter SMW’s understanding of later nonconsensual sex, thus increasing the likelihood that she would apply the label of rape following ASA. This is also consistent with Match-and-Motivation Theory in that nonconsensual sex in childhood could produce a greater match between incident and label when rape is reexperienced in adulthood. Although not examined in the current study, other factors may also influence the association between CSA severity and rape acknowledgment, such as disclosure of early victimization and social support from family or mental health professionals. Our findings, as well as the findings of others (e.g., Wilson & Scarpa, 2015), suggest that continued research into rape acknowledgment, including the role of CSA severity in labeling of later rape experiences, is critical for assisting in the provision of appropriate sexual assault support services for women, particularly for SMW as they experience higher rates of lifetime sexual assault.
Limitations and Future Directions
The current study provides a novel examination of rape acknowledgment in SMW, but—like all studies—it is not without limitations. Our assessment of rape acknowledgment and postassault outcomes involved cross-sectional data, which limits the inferences that can be drawn about the temporal ordering of our variables. To examine ASA group membership, we combined lesbian and bisexual women into one group. Still, our ASA groups were comprised of small sample sizes, which may have affected statistical power when assessing group differences (e.g., acknowledged rape vs. unacknowledged rape comparisons). Future studies can build on this work by incorporating longitudinal designs with larger samples to explore how the process of rape acknowledgment develops over time for lesbian and bisexual women as independent groups. This study did not assess factors that may influence the rape acknowledgment process, such as how CSA experiences were labeled, the gender of the perpetrator(s) involved in CSA or ASA, or whether ASA occurred before coming out. Furthermore, this study did not examine other labels that women may apply to their unwanted sexual experiences (i.e., miscommunication, hook up gone wrong). Qualitative studies are needed to explore the cognitive processes by which SMW make sense of sexual assault. Given that sexual assault occurs at a higher rate among SMW, future studies are needed to compare the experiences of heterosexual and SMW to determine whether and how there are differences in the meaning-making process following ASA. In addition to smaller sample sizes, the rates of heavy drinking in this sample showed variability that may have contributed to the mixed findings in alcohol outcomes (i.e., heavy drinking days vs. hazardous drinking). Finally, in addition to SMW being at elevated risk for sexual assault, the minority stress model posits that this group is also at risk for other social stressors based on their sexual identity, which may influence psychological symptoms (Meyer, 2003). Future work can expand on these findings by examining other social stressors experienced by SMW who are both rape acknowledged and unacknowledged to further understand the high rates of distress in this group.
Clinical Implications and Conclusions
This study adds to the existing literature by exploring rape acknowledgment in SMW’s mental health and drinking behaviors. Our findings revealed high rates of rape acknowledgment, yet surprisingly few differences in postassault outcomes between SMW who were acknowledged and unacknowledged rape victims. However, differences were found when rape acknowledged and unacknowledged victims were compared to women with no ASA or ASA that did not include completed rape. Among SMW with rape histories, more severe CSA increased the odds of rape acknowledgment following ASA. Within treatment settings, our findings highlight the importance of assessing sexual assault using behavioral-based assessment tools, especially among populations that are at elevated risk for sexual assault across the life span, while remaining sensitive to potential asynchrony between women’s responses and their level of acknowledgment about the incident. Regardless of rape acknowledgment status, SMW who experience rape during adulthood appear to be at higher risk for poorer mental health and heavier drinking. These findings can contribute to the development of more culturally informed interventions to assist diverse women who have experienced sexual assault.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by Award No. K01AA016105 (Principal Investigator, A. Hequembourg) from the National Institutes of Health, National Institute on Alcohol Abuse and Alcoholism (NIAAA). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIAAA.