
Abstract
School-based violence is a current public concern in the United States. One factor that can impact school-based violence that has gained much attention is mental health status. To better inform public perceptions, this study provides new evidence concerning the association between mental health status and acting out violence in school-aged populations. We examined a diverse sample of sixth graders across 14 schools in Texas in 2011-2012 (N = 721) who completed a self-administered survey assessing mental health symptoms and frequency of perpetration and/or receipt of different types of aggressive behaviors. Multinomial regression models tested whether adolescents with mental health symptoms (overall and by symptom types) are more predisposed to be actors only, recipients only, or both, of physical, verbal, and relational aggression. Across aggressive behavior types, symptomatic versus nonsymptomatic adolescents had consistently increased odds of being exclusively a recipient of aggression. When symptomatic adolescents did act out aggression, they participated concurrently as both an actor and recipient. Rarely were symptomatic adolescents more likely to be exclusively an actor of aggression. Moreover, symptomatic versus nonsymptomatic adolescents had five times the odds of being threatened by a weapon including a gun or knife. Compared to those who do not, youth who perceive having a mental health issue had twice the odds of being an actor only of verbal and relational aggression. These findings provide evidence for the need to change how the public associates mental health problems with aggressive behaviors among youth especially following national tragic events. Communities at large may benefit from evidence- and school-based interventions that improve awareness of and tolerance to mental health conditions among youth.
Introduction
Aggressive behaviors between youths such as harassment, victimization, and bullying are a growing concern in the United States. These behaviors are unwanted, intended to harm, and may happen once or repeatedly as in the case of recurrent bullying. Often they occur in peer relationships where an uneven power imbalance exists (Eisenberg & Aalsma, 2005; Gladden, Vivolo-Kantor, Hamburger, & Lumpkin, 2014). Aggressive behaviors can be acted (i.e., perpetrators) or received (i.e., victims) as physical violence, such as kicking or hitting; verbally as in teasing or name-calling; or relationally, such as spreading a rumor or leaving someone out of an activity on purpose (Centers for Disease Control and Prevention [CDC], 2016). Risk factors for acting aggressively include male gender and for receiving aggressive behaviors include those that are members of a sociopolitical minority group or those that are perceived as different from their peers—for example, ethnicity, religion, sexual orientation, gender identity, body size and development, or disability (Borg, 1999; Card & Ernest, 2008; Cook, Williams, Guera, Kim, & Sadek, 2010; Graham, 2006; Nansel et al., 2001; Petersen, 1980; Rivers, 2011; Rose, 2011; Russell & Joyner, 2001).
One factor related to aggressive behaviors between peers that has gained much attention is mental health status. National headlines of tragic incidents such as school shootings (Cowan, 2014; Kamrowski, 2017; Laughland, Luscombe, & Yuhas, 2018) and the suicides of adolescents following extreme bullying (Schweber & Foderaro, 2016; McNamara, 2016) point to two opposing views. On one hand, when school-based violence occurs, a common response heard in the media is to question the mental health of the perpetrator, raising the question of whether youth with mental health issues are more likely to act aggressively towards others. This public perception has increasingly applied to younger ages as evidenced from the “mental health problem at the highest level” political response to school shootings. These responses often ignore other known risk factors of perpetrating violence such as male gender, prior reports of animal abuse or dating violence, and access to firearms; instead, they highlight ongoing cultural stereotypes and misnomers about the relationship between mental illness and violence. This overemphasis on mental illness and underemphasis on other risk factors is a pervasive, common aspect of mental illness stigma. Specifically, the labeling of mental illness, a core component of mental illness stigma (Link & Phelan, 2001), is a salient response to mass school violence in the media, where the perpetrator is characteristically described as having a mental illness that led them to their violent actions. In contrast, media responses to incidents of suicide-related behaviors among youth are oftentimes associated with bullying that target those experiencing mental health problems (Bauman, Toomey, & Walker, 2013; Bhatta, Shakya, & Jefferis, 2014; Hertz, Donato, & Wright, 2013). Following these tragedies, attention is usually placed on the victim’s mental health rather than any interpersonal and cultural intolerance among the perpetrator(s) that potentially led to their suicide. Despite the assertions made in the media, it remains unclear whether school-aged youth with mental health problems are more likely to be actors or recipients of violence, or both.
Previous research suggests that risk of aggressive behaviors may depend on the type of mental health symptoms experienced by youth. Youth with delinquency, hyperactivity, and attention issues are more likely to act out aggression (Ivarsson, Broberg, Arvidsson, & Gillberg, 2005). In contrast, youth with depressive and anxious symptoms are vulnerable to being recipients of peer aggression, in addition to youth who are perceived as different or weak by their peers (Fekkes, Pijpers, Fredriks, Vogels, & Verloove-Vanhorick, 2006; Hodges, Malone, & Perry, 1997; Ivarsson et al., 2005; Olweus, 1994). Youth who simultaneously participate as both actors and recipients score higher on a full range of symptoms including depressive, anxious, hyperactive, and attention issues, suggesting that youth with numerous symptoms are at risk of mutual violence (Fekkes et al., 2006; Ivarsson et al., 2005). Although the direction of mutual violence is ambiguous, youth exposed to violence in the past have increased risk for developing mental health and behavioral problems (Sternberg, Baradaran, Abbott, Lamb, & Guterman, 2006). Together, previous research speaks to the importance of both the type of symptoms and to whether the youth in question acts aggressively, receives aggression from others, or both.
Informed by this prior research, we aim to push our understanding forward by describing the full pattern of relationships that this research suggests may be important. Specifically, we examine whether mental health symptoms overall and by type of symptoms affect the probability of being a recipient only, an actor only, or both an actor and recipient of aggressive behaviors as compared with youths who are neither recipients or actors. Furthermore, we expand what has been learned from previous research by examining different types of aggression including physical, verbal, and relational. Unlike prior research that aggregate types of aggression, our assessment of various domains of aggressive behaviors can provide a more nuanced understanding of aggressive patterns among youth with and without mental health problems. We also test a dose–response relationship between increasing number of symptoms with odds of aggressive behavior outcomes and tap into each youths’ subjective perception of mental health.
As the prevalence of aggressive behaviors, including bullying, is highest and onset of mental health symptoms begins in early adolescence, we conduct our examination in a multi-ethnic sample of sixth graders in Texas, a critical age for investigation (Nansel et al., 2001; Pellegrini et al., 2010). We provide new evidence concerning the life course of school-related violence, asking if the relationship between peer-based aggressive behaviors and a youth’s mental health status is common with early roots. These patterns can inform how school-related violence that comes to national attention during later adolescence may develop, and if extreme examples of school violence are an exception related to other phenomena such as community violence or due to the development of mental health issues. Clarifying the patterns of physical, verbal, and relational aggressive behaviors among youth with mental health problems can inform current public perceptions regarding the relationship between mental health and violence among school-aged youth. Increased knowledge about the profiles of youth who are more likely to act out physical violence and those who are vulnerable to receiving it can inform screening and intervention efforts.
Method
Baseline data from a school-based anti-stigma intervention aimed at changing mental health attitudes were used for analysis. The selection of participants, design, and procedures of the intervention are described in detail elsewhere (Painter et al., 2017). Briefly, 14 school administrators in an urban city in Texas agreed to participate in the study from 2011 to 2012 following our invitation. Using a fully-crossed 2 × 2 × 2 factorial-controlled design, each school’s sixth-grade class was randomly assigned to a mental illness anti-stigma intervention. Both parents/guardians and students gave active assent and consent for participation after receiving information about the study. Students were not included in the study without signed forms. Students and parents/guardians received a modest monetary incentive for returning signed forms and completing the study questionnaires.
Study Sample
The sample for analysis includes 751 sixth graders (60% of those invited) who completed a pretest survey on laptop computers. As the study sample is representative of the classroom aggregate demographic (e.g., race/ethnicity, gender, socioeconomic status), there is little evidence of nonresponse bias. Surveys were offered in English or Spanish, though all students chose the English survey. More than half were female and had a mean age of 11.5 years (Table 1). The sample is ethnically diverse (44% Hispanic/Latino, 23% non-Latino White, 23% non-Latino Black, and 10% other race/ethnic group; 70% preferred using English language at home), as well as socioeconomically— 60% come from a household income of US$40,000 or less, and about 43% had a parent/guardian educational attainment of a high school diploma or less. Youth with incomplete data regarding the assessment of mental health problems and aggressive behaviors were excluded (< 5%). There were no statistically significant differences between the included and excluded participants on these variables. The final sample for these analyses included 729 participants.
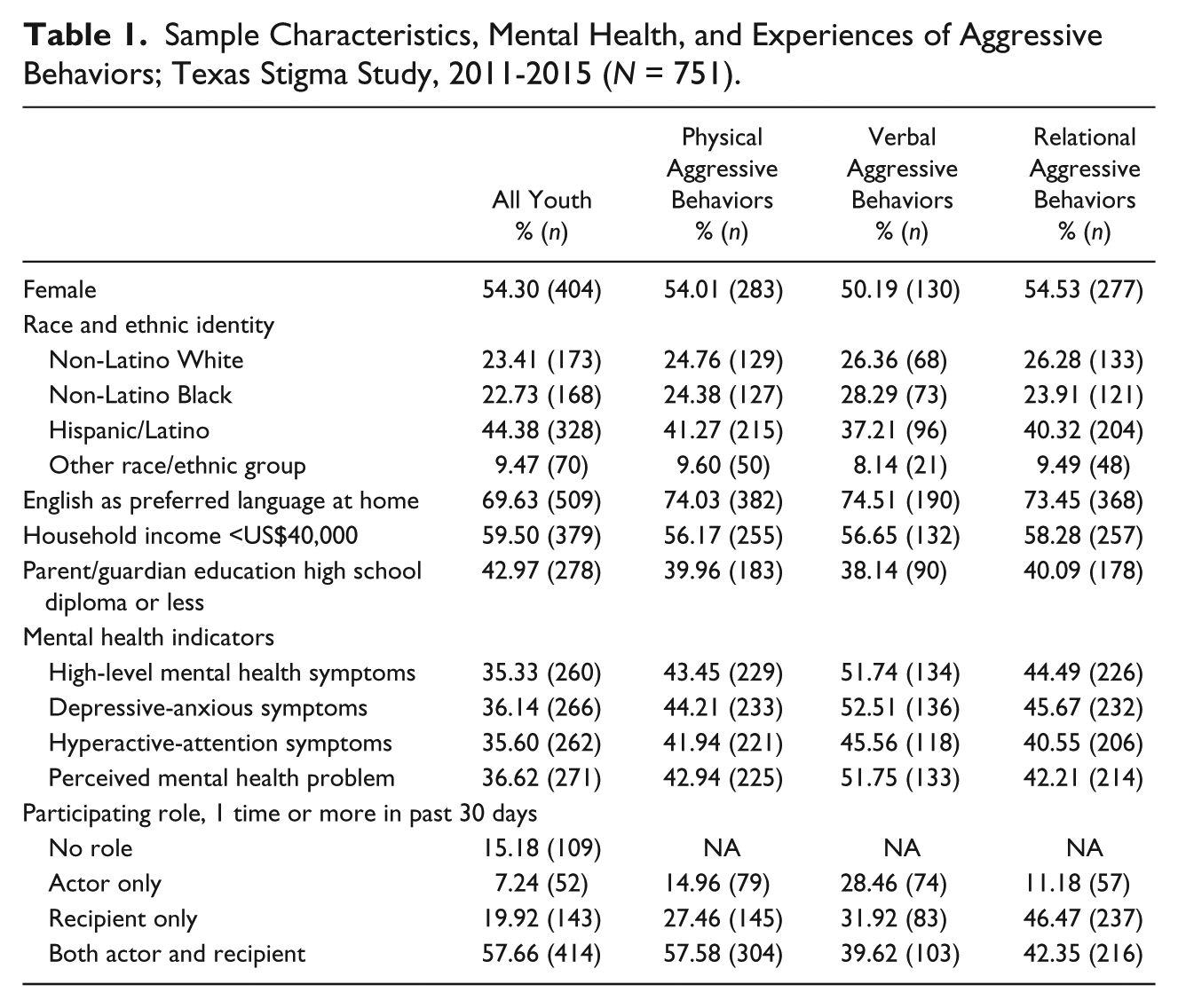
Sample Characteristics, Mental Health, and Experiences of Aggressive Behaviors; Texas Stigma Study, 2011-2015 (N = 751).
Measures
Aggressive behaviors
The 19-item Problem Behavior Frequency Aggression Scale measured the frequency of physical, verbal, and relational aggressive behaviors (Farrell, Kung, White, & Valois, 2000; Orpinas & Frankowski, 2001). Nine items measured acted behaviors such as hitting or picking on another youth and 10 items measured received behaviors such as being called mean names or hit by another youth. Although our data for analysis come from a school-based study, it is possible that the assessments of aggressive behaviors included those outside of the school context. For example, some items include “student” or “kid” in the question such as, “how often did a student ask you to fight?” or “how many times have you hit or slapped another kid?” Other items had an unspecified subject such as “how often have you had someone spread a false rumor about you?” As such, respondents may also have been reporting on aggressive experiences in other aspects of the lives of youth (e.g., community, dating, domestic, or gang violence). Responses to items were coded as “0 times”, “1-2 times”, and “3 or more times”. No differences in item responses were found between the two higher-ordered categories when running analyses. Thus, we dichotomized responses (0 = “0 times,” 1 = “1 or more times”; see Appendix Table A1).
Drawing on the CDC’s guidelines for research in child and adolescent bullying (Gladden et al., 2014) including their definitions of aggressive behavior domains, we constructed acting and receiving scales in the physical, verbal, and relational domains. We examined content validity of the clustered items, labeled the scales, and tested their reliability and correlations (see Appendix Table A2). “Physical” items implied experienced physical contact such as hitting or pushing. The “verbal” items included verbal harassment and threats of physical contact, and “relational” items concerned social exclusion including spreading rumors or intentionally being left out. To assess the participating role in each aggressive behavior type (e.g., physical, verbal, and relational), categorical variables representing participation role were created (0 = “no participation”—base outcome, 1 = “acted only”, 2 = “received only”, 3 = “both acted and received”).
Mental health measures
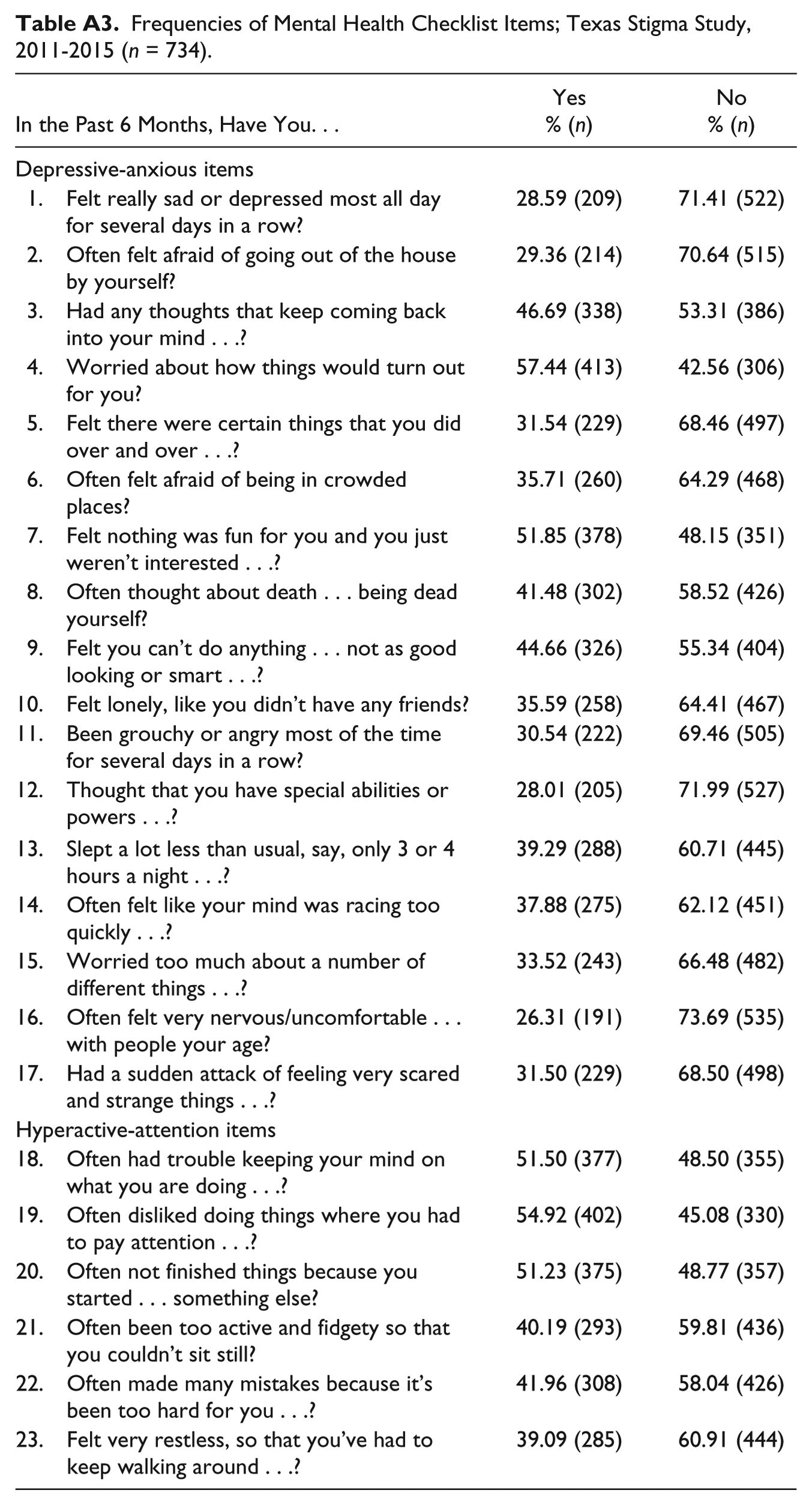
A mental health symptoms checklist provided a compact screen and drew on items from the National Institute of Mental Health Diagnostic Interview Schedule for Children, Version IV (Shaffer, Lucas, Dulcan, & Schwab-Stone, 2000). Items examined attention-hyperactive (e.g., “felt too active or fidgety”), depressive (e.g., “felt really sad or depressed”), and anxious (e.g., “worried too much about a number of different things”) symptoms (see Appendix Table A3). Exploratory factor analysis of youth self-reported symptoms suggested one factor and that using the full 23-item scale fit the data better than reduced scales (α = .87). However, factor analysis of parent reports of symptoms pertaining to their child suggested more than one factor: symptoms of depression and anxiety (α = .83), and symptoms of hyperactivity and attention issues (α = .67). Therefore, to explore patterns of acted and received aggressive behaviors by symptom type, youth self-reported items were summed to create three count variables: (a) all items combined to create a global mental health score; (b) depressive-anxious symptoms only; and (c) hyperactive-attention symptoms only. The top tertile of the global mental health variable was used as a cutoff to identify youth scoring high (1) versus low (0) on the symptom checklist. Similarly, we used the top tertile of depressive-anxious symptoms and hyperactive-attention symptoms as a cutoff to identify youth scoring high (1) versus low (0) on symptoms. Finally, participants were asked if they seemed to have a mental health problem in the past 6 months (0 = “no”, 1 = “yes”) to tap into their subjective perceptions of their mental health.
Covariates
The analyses controlled for gender (female—referent), self-reported race/ethnicity (non-Latino White—referent, Hispanic/Latino, non-Latino Black, and other race/ethnicity group), and family income (0 = “<US$40,000”—referent, 1 = “US$40,000 or more”).
Data Analysis
The association between mental health and aggressive behaviors was examined with multinomial regression models where no involvement in aggressive behaviors was the comparison category. We first examined the crude association between mental health and physical, verbal, and relational aggressive behaviors; then, we controlled for gender, race/ethnicity, and household income. In addition, we tested for potential interactions with all covariates but none were significant.
Controlling for covariates, two models were estimated for each outcome: one included overall mental health (high vs. low symptoms) and perceived problem; the other included type of symptoms (high vs. low depressive-anxious and hyperactive-attention symptoms) and perceived problem. Multinomial models assume that each outcome category is unique, exclusive, and not influenced by other categories (independent of irrelevant alternatives assumption; Long & Freese, 2014). We tested and met this assumption by excluding youth who reported having no role in aggressive behaviors and examining actor only as the base outcome. These results (available upon request) were consistent with the findings presented here. Stata SE 14 was used for all analyses.
Results
Table 1 presents the distribution of sample characteristics for the full sample and by type of aggressive behavior. About a third of youth perceived having a mental health problem in the full sample. Among students with high-level mental health symptoms (n = 258), 58% (n = 150) also perceived having a mental health problem. About 15% had no role in any aggressive behavior, while the most common role was being both an actor and a recipient (58%); the least common role was actor only (7%; Figure 1a); symptomatic youth and those perceiving having a mental health problem saw similar patterns in roles though they had lower prevalence of one-sided acted aggression and greater prevalence of mutual acting and receiving of aggressive behaviors than those without symptoms and a perceived problem (Figure 1b and 1c). For physical and verbal aggressive behaviors, the most common role was being both an actor and recipient (58% and 40%) followed by recipient only (28% and 32%) and actor only (15% and 29%; Table 1). Relational aggressive behaviors saw similar patterns in roles: recipient only was most common (47%) while actor only was the least (11%).
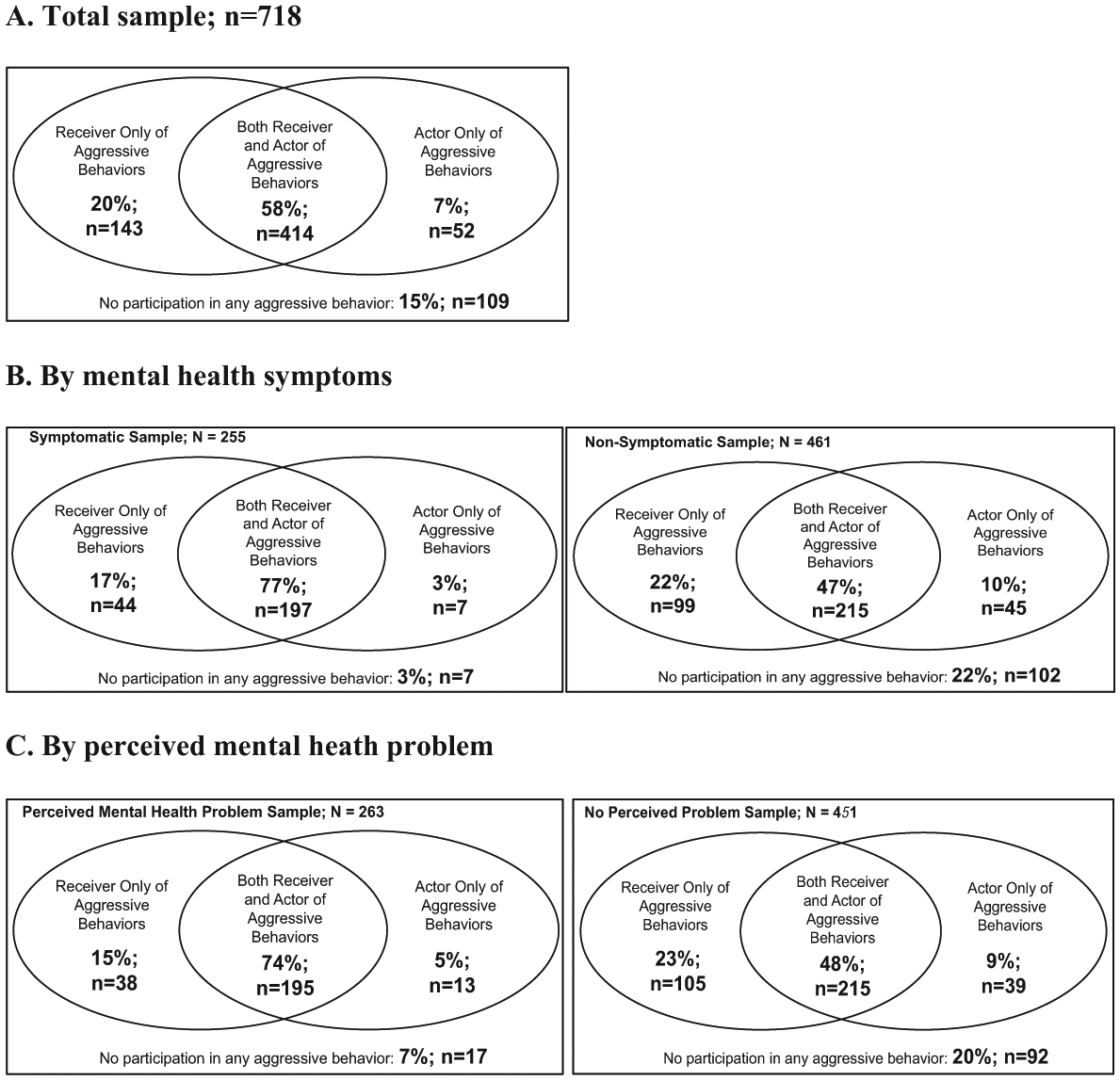
Overlap in aggressive behavior roles at baseline in sixth-grade sample; Texas Stigma Study, 2011-2015: (a) total sample; n = 718; (b) by mental health symptoms; (c) by perceived mental health problem.
Mental Health and Physical Aggressive Behaviors
The results of the multinomial regression models for each aggressive behavior domain (i.e., physical, verbal, and relational) are displayed in Table 2. Model 1A examines the impact of having high levels of mental health symptoms and a perceived mental health problem adjusting for gender, race/ethnicity, and household income. In terms of physical aggression, we found that compared with youth with low-level mental health symptoms, the odds of being a recipient only versus having no role (base outcome) were about three times as great among youths with high mental health symptoms, odds ratio (OR) = 2.9, 95% confidence interval (CI) = [1.6, 5.2]. Strong mental health effects were also seen for the dual role outcome: relative to the base outcome, those with high versus low symptoms were about five times as likely to be both actors and receivers of physical aggressive behaviors than youths without high-level symptoms (OR = 5.3, 95% CI = [3.2, 8.9]). No significant mental health effect was seen for the actor only role. Perceiving oneself to have a mental health problem was associated with greater aggression only among the actor plus recipient group.
Multinomial Regression Models of Actors and Recipients of Each Aggressive Behavior Domain With Mental Health Predictors (OR [95% CI]); Texas Stigma Study, 2011-2015 (n = 611).
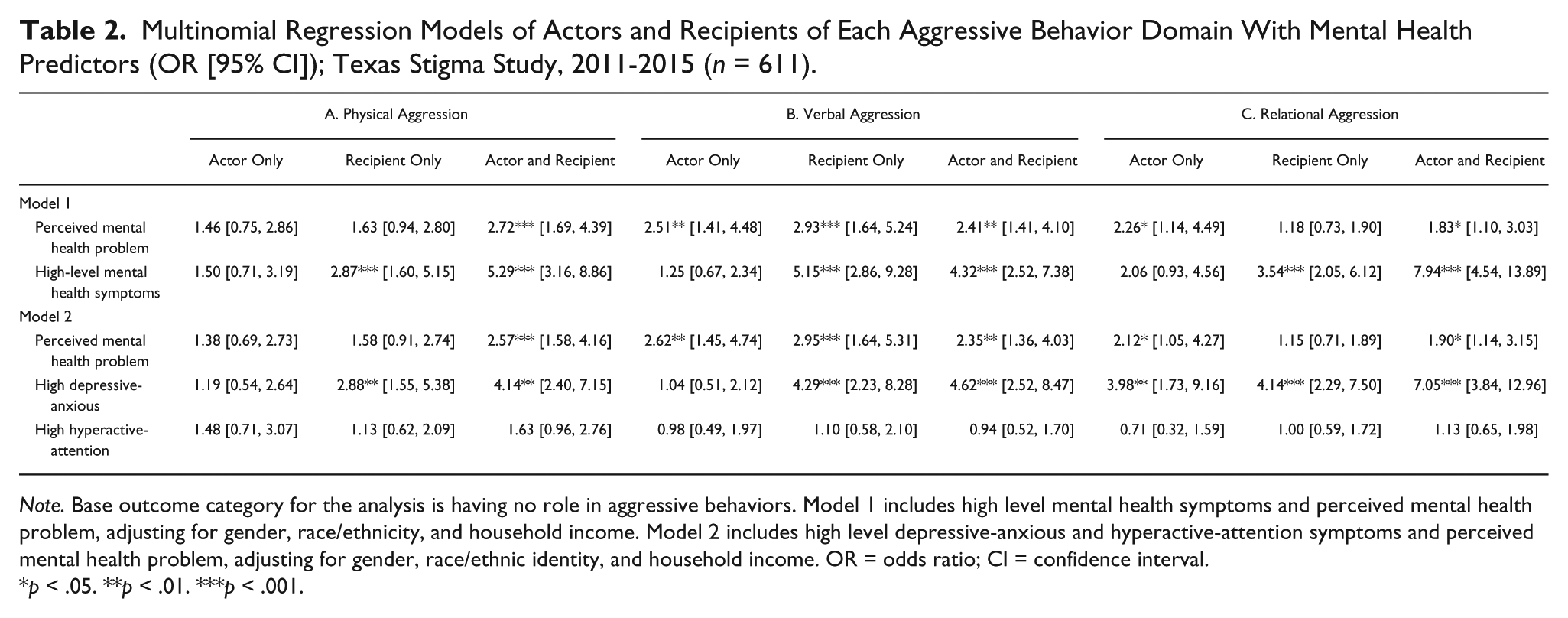
Note. Base outcome category for the analysis is having no role in aggressive behaviors. Model 1 includes high level mental health symptoms and perceived mental health problem, adjusting for gender, race/ethnicity, and household income. Model 2 includes high level depressive-anxious and hyperactive-attention symptoms and perceived mental health problem, adjusting for gender, race/ethnic identity, and household income. OR = odds ratio; CI = confidence interval.
p < .05. **p < .01. ***p < .001.
Model 2A includes type of symptoms and perceived problem. Net of perceived mental health problem and covariates, those with high-level depressive-anxious symptoms had greater odds of being both an actor and recipient of physical aggressive behaviors than those without symptoms (OR = 2.9, 95% CI = [1.6, 5.4]). Relative to the low-symptom group, youth with high-level depressive-anxious symptoms were also three times more likely to be recipients only of physical aggression relative to having no role. No effects were found among those with high-level hyperactive-attention symptoms with respect to physical aggression.
Mental Health and Verbal Aggressive Behaviors
For verbal aggression, the odds of being a recipient only versus having no role were nearly five times as great among youth with high-level mental health symptoms as compared with youth without (Model 1B). Likewise, those with high-level mental health symptoms had four times the odds of being both an actor and recipient relative to the base outcome. There was no association with the actor only role. Perceiving a mental health problem was significantly associated with role participation across the board, including being an actor only (OR = 2.5, 95% CI = [1.4, 4.5]); similar patterns were observed in Model 2B.
With respect to symptom type (Model 2B), youth with depressive-anxious but not hyperactive-attention symptoms had significantly greater odds of being a recipient only compared to those without symptoms. Furthermore, those high on depressive-anxious symptoms (OR = 4.6, 95% CI = [2.5, 8.5]) were significantly more likely to be both actors and recipients of verbal aggression than youths without symptoms.
Using logistic regression, we also examined the role of mental health on the specific items assessing receipt of verbal threats that may lead to physical harm or injury that requires medical attention (results not shown). Youth with high-level mental health symptoms compared with those without had three times the odds of being asked to fight and four times the odds of being threatened to get hit or physically harmed by another student. Finally, while 10% of the entire sample (n = 64) reported being threatened by a weapon (e.g., knife/gun), compared to those with low-level symptoms, the odds of someone receiving threats with a weapon are greater for those with high-level symptoms (OR = 4.9, 95% CI = [2.3, 8.7]).
Mental Health and Relational Aggressive Behaviors
Compared to those without, youth with high-level symptoms had about four times the odds of only receiving relational aggression and eight times the odds of being both an actor and recipient (Model 1C). Youth who perceived having a mental health problem compared with those who did not had twice the odds of being actors only and both actor and recipient (Models 1C and 2C). Youth with high compared to low depressive-anxious symptoms were more likely to participate in all three roles of relational aggression. Those with high hyperactive-attention symptoms compared to those with low levels were not significantly more likely to engage in any role of relational aggression.
Discussion
The current study examined whether youth with mental health problems compared with those without were more or less likely to engage in three types of aggressive behaviors—physical, verbal, or relational—and whether they did so as actors only, recipients only, or as both. Our findings make an important contribution to our understanding of the role that youth with mental health symptoms play in specific types of aggressive behaviors. We find little evidence to suggest that youth with mental health problems, as assessed by self-reported symptoms and perceiving a mental health problem, are more likely than youth without them to engage in aggressive behaviors as actors only; instead, we find that they are much more likely to be recipients only or both recipients and actors. Furthermore, we found that heightened levels of exposure to aggressive behaviors were not limited to just one or two specific mild types of behaviors but were instead consistently elevated across specific instances such as being hit/pushed/shoved, asked to fight, and threatened with a weapon. This finding carries significance for understanding the risk of injury or harm that may require medical attention. This vulnerability can lead to a range of negative consequences including worsening of mental health, impact on treatment and recovery, and academic and social consequences (Arseneault, Bowes, & Shakoor, 2010; Rigby, 1999; Zinner, Conelea, Glew, Woods, & Budman, 2012).
Only 3% of the symptomatic sample had no role at all in aggressive behaviors compared with 22% of the nonsymptomatic sample. This difference is likely due to the increased likelihood of experiencing mutual aggressive behaviors among those who have mental health problems compared with those who do not. That youth with mental health symptoms are much more likely to be an actor and recipient rather than having no role at all in aggressive behaviors is an important finding. This mutuality in aggressive behaviors may point to a lack of social and cultural understanding of mental health issues among preadolescents, and youth with mental health symptoms struggle with both acting and receiving aggressive behaviors with their peers, adding another challenging dimension to their overall health and well-being.
These findings highlight the need to inform youth service providers about the risks of harassment that youth with and without mental health problems may experience and the interpersonal conflicts in which they may be involved. For example, among one-sided actors of aggression toward peers with mental health problems, providers can work on expanding awareness of and tolerance to peers who are perceived as different as a strategy to prevent additional violence. For youth with mental health issues who act out violent behaviors during an interpersonal conflict with a peer, learning nonviolent coping strategies and how to deescalate a potentially violent situation may help reduce mutual aggressive behaviors among those with mental health problems. When youth are being treated for injury related to bullying, clinical providers could screen for concurrent mental health problems (Kim & Kim, 2013).
The primary evidence of significant mental health effects for the actor only role was in verbal threats and relational aggression, but not physical aggression, among youth who perceived having a mental health problem. However, the prevalence of one-sided acted aggression (i.e., actors only) among symptomatic youth and those who perceived themselves to have a mental health problem was low (3% and 7%, respectively). This may in part be due to a true lower prevalence in these groups, or that a lower prevalence exists at this age in development only but may increase as mental health problems further develop in older adolescence. Future research in the area should oversample preadolescents who engage in actor only roles as a way to increase statistical power for detecting mental health effects. Nevertheless, our finding suggests that screening youth for their own subjective feeling of having a mental health issue, and following up with an evaluation and treatment plan, may be important in reducing engagement in verbal and relational aggressive behaviors. However, when youth with high-level symptoms were actors of aggressive behaviors, being an actor almost always co-occurred with being a recipient. These co-occurring roles were pronounced for youth with depressive-anxious symptoms across each type of aggressive behavior; hyperactive-attention problems were not associated with any aggressive behaviors. As our findings show that youth with mental health symptoms compared with those without engage in mutual acting and receiving of aggressive behaviors, interventions or therapies that improve how peers resolve interpersonal conflicts may alleviate aggressive behaviors between them.
Our findings do not replicate prior research that find that youth with hyperactive-attention symptoms are more likely to act out aggression (Ivarsson et al., 2005). The only statistically significant associations for the actor only role that we found were in verbal and relational aggression among youth who perceive having a mental health problem and in relational aggression among those with high levels of depressive-anxious symptoms. The key methodological distinction between our study and previous studies of mental health and aggressive behaviors is that the current study examines unique domains of aggressive behaviors (physical, relational, and verbal) unlike previous studies which conceptualize and aggregate these behaviors as a global construct of bullying (Gini & Pozzoli, 2013). When we combine all aggressive behaviors into a global outcome, we find similar patterns as previously published reports: youth with hyperactive-attention symptoms had increased odds of acting, though statistically insignificant, and youth with depressive-anxious symptoms had increased odds of receiving. Furthermore, our assessment contributes to the understanding of mental health problems and aggressive behaviors by separating the relationships between different symptoms, unique types of aggressive behaviors, and specific participation roles.
Several limitations of the assessment of aggressive behaviors require discussion. First, the current study does not address causality to tell us whether mental health problems lead youth to engage in aggressive behaviors or vice versa. Second, the temporal order in which concurrent aggressive behaviors are acted or received is not captured which could help tease apart the patterns and sequencing of those involved in multiple roles and types of aggressive behaviors. For example, being a mutual actor/receiver of verbal aggression may follow an initial experience of physical assault. Alternatively, participation in mutual acting/receiving verbal aggression may escalate into physical violence. Third, the power dynamics or severity surrounding the aggressive behaviors are unknown. Understanding power differentials between peers may elucidate if any behaviors occurred as self-defense or in defense of a peer. Additional reports from bystanders, school teachers and staff, or parents, including if there was an injury involved, may better capture power dynamics and if severe injury, academic, or disciplinary consequences resulted. Relatedly, prior reports have shown the role of fear in interpersonal violence among youth; thus, understanding presence of fear or coercion between peers, online and offline, may be important (DuPont-Reyes et al., 2014). Although our measure did not assess power differentials, the items were phrased to likely indicate/capture intentions to harm and included an item assessing threats from a weapon such as a gun/knife. If a school shooting occurred, it would have been captured in the assessment of aggressive behaviors, though rare. However, the assessment does not allow us to pick out a reported school shooting in the items specifically. Nevertheless, a school shooting would have been covered by the items in the assessment.
Other limitations merit discussion as well. With respect to the mental health assessment, it appropriately inquired about mental health issues (e.g., depressive, anxious, hyperactive, and attention symptoms) that are commonly experienced in sixth grade (see Appendix Table A3 for a description of each item). Symptoms pertaining to psychotic disorders were not the primary focus of this study. Nevertheless, the mental health assessment did include aspects of psychotic disorders including delusional symptoms (e.g., “special abilities or powers”), disorganized thinking and behaviors, and suicidal thoughts. As such, the mental health assessment captured symptoms of psychotic disorders that correlate with common mental disorders in sixth graders. Other potential confounders such as adverse childhood experiences indicative of threat (e.g., sexual abuse, parental maltreatment) were not assessed; however, we controlled for socioeconomic status, race/ethnicity, and gender, as proxy variables for experienced adversity due to, or related to, poverty/deprivation or being a member of a sociopolitical minority group.
Despite these limitations, the study provides valuable insight into aggressive behaviors in youth with mental health problems in a diverse school-based sample of sixth graders where this area of research is most needed. Using reliable and validated measures of aggressive behaviors in youth recommended for research in bullying, we were able to offer new data of the frequency and participating roles in a range of aggressive incidents. We used validated mental health measures including an objective symptoms checklist, exploring both degree and type of symptoms, and tapping into individual perception of a mental health problem. Finally, our results may be applicable to other school-aged populations in the United States given our socioeconomically and ethnically diverse sample.
Important for the school context, youth with mental health problems are more likely than those without to experience recipient only bullying relative to having no role. Additional evidence in support of our conclusion comes from two vignettes of adolescent characters described as having bipolar and social anxiety disorders, respectively. Participants read these descriptions and responded to a single item corresponding to each character’s potential for being bullied in school. About two thirds of the sample believed that each character was “very” to “somewhat” likely to be bullied in school (results not shown). School-wide interventions that promote anti-bullying of different types of aggressive behaviors and that promote awareness of mental health problems, including the victimization of youth who are “othered,” may benefit all youth. Such interventions could encourage coping strategies to prevent participation in bullying and safety planning to prevent further harm, most especially among youth with mental health problems. Moreover, interventions that increase mental health awareness and promotion may further improve tolerance for youth with mental health problems and prevent their victimization.
Further knowledge in this area will guide intervention and prevention efforts to reduce violence in the school setting including for youth with mental health problems. In terms of public perceptions, our data do not support the idea that youth with mental health problems are more likely to act one-sided physical aggression; in fact, they are more likely to receive it. Perpetrators of aggressive behaviors are not exclusively those who screen positive for mental health problems; similarly, the mental health status of individual youth is not a strong predictor of one-sided perpetration of aggression. Thus, our findings provide evidence for the need to change how the public associates mental health problems with aggressive behaviors among youth especially following national tragic events.
Footnotes
Appendix
Frequencies of Mental Health Checklist Items; Texas Stigma Study, 2011-2015 (n = 734).
| In the Past 6 Months, Have You. . . | Yes |
No |
|---|---|---|
| Depressive-anxious items | ||
| 1. Felt really sad or depressed most all day for several days in a row? | 28.59 (209) | 71.41 (522) |
| 2. Often felt afraid of going out of the house by yourself? | 29.36 (214) | 70.64 (515) |
| 3. Had any thoughts that keep coming back into your mind . . .? | 46.69 (338) | 53.31 (386) |
| 4. Worried about how things would turn out for you? | 57.44 (413) | 42.56 (306) |
| 5. Felt there were certain things that you did over and over . . .? | 31.54 (229) | 68.46 (497) |
| 6. Often felt afraid of being in crowded places? | 35.71 (260) | 64.29 (468) |
| 7. Felt nothing was fun for you and you just weren’t interested . . .? | 51.85 (378) | 48.15 (351) |
| 8. Often thought about death . . . being dead yourself? | 41.48 (302) | 58.52 (426) |
| 9. Felt you can’t do anything . . . not as good looking or smart . . .? | 44.66 (326) | 55.34 (404) |
| 10. Felt lonely, like you didn’t have any friends? | 35.59 (258) | 64.41 (467) |
| 11. Been grouchy or angry most of the time for several days in a row? | 30.54 (222) | 69.46 (505) |
| 12. Thought that you have special abilities or powers . . .? | 28.01 (205) | 71.99 (527) |
| 13. Slept a lot less than usual, say, only 3 or 4 hours a night . . .? | 39.29 (288) | 60.71 (445) |
| 14. Often felt like your mind was racing too quickly . . .? | 37.88 (275) | 62.12 (451) |
| 15. Worried too much about a number of different things . . .? | 33.52 (243) | 66.48 (482) |
| 16. Often felt very nervous/uncomfortable . . . with people your age? | 26.31 (191) | 73.69 (535) |
| 17. Had a sudden attack of feeling very scared and strange things . . .? | 31.50 (229) | 68.50 (498) |
| Hyperactive-attention items | ||
| 18. Often had trouble keeping your mind on what you are doing . . .? | 51.50 (377) | 48.50 (355) |
| 19. Often disliked doing things where you had to pay attention . . .? | 54.92 (402) | 45.08 (330) |
| 20. Often not finished things because you started . . . something else? | 51.23 (375) | 48.77 (357) |
| 21. Often been too active and fidgety so that you couldn’t sit still? | 40.19 (293) | 59.81 (436) |
| 22. Often made many mistakes because it’s been too hard for you . . .? | 41.96 (308) | 58.04 (426) |
| 23. Felt very restless, so that you’ve had to keep walking around . . .? | 39.09 (285) | 60.91 (444) |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by grants R01MH095254 and 5-T32-MH 13043 from the National Institute of Mental Health (NIMH), and by the Latino Research Initiative at The University of Texas at Austin. The content is solely the responsibility of the authors and does not represent the official views of NIMH.