
Abstract
Differences in child abuse perpetration between individuals with and without mental disorders remain obscure. This study compared the risk difference and further investigated the association between the category of mental disorders and child abuse perpetration. A total of 681,970 adults from the 2002 to 2013 Taiwan National Health Insurance Research Database were analyzed, including 340,985 patients with psychiatric disorders (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] codes 290.x–319.x) and 340,985 sex- and age-matched individuals without psychiatric disorders. Child abuse perpetration (ICD-9-CM N-codes 995.5x and E-code E967) was the outcome variable. Matched analyses indicated that the risk of child abuse among patients with psychiatric disorders (0.25%) was significantly higher than that among those without psychiatric disorders (0.16%; odds ratio [OR] = 1.464, p < .0001). Among the six categories of mental disorders, the prevalence rates of committing child abuse were significantly higher for personality disorders, substance use, and affective disorders (0.56%, 0.45%, and 0.40%, respectively; p < .0001). Compared with anxiety disorders, substance use disorders were significantly associated with higher odds of child abuse perpetration (OR = 2.032, p < .05), especially physical abuse (OR = 2.018, p < .0001). Psychiatric morbidity was associated with higher odds of child abuse, with substance use determined as the major risk category. Screening high-risk families by using the associated factors is crucial.
Introduction
Child abuse is a global public health issue with a potential for long-term impact on victims who did not receive proper interventions. The events of child abuse remain largely hidden and unreported because of fear and stigma and the societal acquiescence of this type of violence (Pinheiro, 2006). Child abuse is broadly defined as any act(s) committed or failure to provide supervision by caregiver(s), resulting in actual or potential harm to a child’s health, development, or dignity, including physical abuse, psychological abuse, sexual abuse, neglect, and exposure to violent environments (Krug, Mercy, Dahlberg, & Zwi, 2002). The prevalence of child abuse varies substantially depending on study definitions, measurements, sample characteristics, and methodologies. A series of meta-analyses has reported that the estimated overall prevalence rates of four types of child abuse, namely, physical abuse, psychological abuse, sexual abuse, and neglect, are 17.7%, 26.7%, 11.8%, and 16.3%, respectively (Stoltenborgh, Bakermans-Kranenburg, Alink, & van Ijzendoorn, 2012; Stoltenborgh, Bakermans-Kranenburg, & van Ijzendoorn, 2013). In Taiwan, the prevalence rate of child maltreatment nearly tripled from 0.15% in 2004% to 0.38% in 2013 (Chen, Yang, & Chou, 2016). Among the types of child maltreatment, violence exposure was the most common, followed by psychological abuse, physical abuse, neglect, and sexual abuse. Furthermore, female victims reported a higher rate of neglect, whereas male victims reported a higher rate of sexual abuse (Chen et al., 2016). The increased incidence might be partially due to the improvement of the child protection system in recognizing the cases or the facilitation of child disclosures. However, a small percentage of child abuse cases are still substantiated by studies or authorities. Therefore, the investigation of potential factors associated with child abuse is imperative in terms of physical and psychological consequences. Because child abuse may physically and mentally affect victims, determining the risk factors for child abuse, particularly for individuals who may potentially commit harmful acts, provides practical implications for modifying policies related to child abuse control and prevention (Feng, Chang, Chang, Fetzer, & Wang, 2015).
With regard to perpetrators, a study indicated that psychiatric or physical morbidity is linked to the incidence of child abuse perpetration because of unstable psychosomatic states. Poverty, low educational achievement, and family breakdown or violence between other family members have been reported as risk factors for parents who abuse their children (Butchart, Phinney Harvey, Kahane, Mian, & Furniss, 2006). Moreover, a study reported a negative relationship between the socioeconomic status of parents and the occurrence of child abuse. Financial problems increased the risk of child abuse (Atta & Youssef, 1998). In addition, studies have indicated that geographical areas and urbanization are related to the occurrence of child abuse (Moritsugu, Vera, Wong, & Duffy, 2015; Weissman, Jogerst, & Dawson, 2003). However, issues regarding patients with psychiatric disorders who commit child abuse have not been adequately discussed. A study reported that a parental history of depression, mania, or schizophrenia doubled or tripled the rate of physical, sexual, or other child abuse. Parental history of antisocial personality disorder also increased the risk of child exposure to physical abuse and any other abuse (Walsh, MacMillan, & Jamieson, 2002). Parents with substance or alcohol abuse have been reported to be a factor associated with child abuse (Famularo, Kinscherff, & Fenton, 1992; Fuller-Thomson & Sawyer, 2014). Nevertheless, the risk caused by nonparental child abuse should be addressed. Furthermore, 12.0% of victims in 2012 were maltreated by a perpetrator who was not the parent of the child. The largest categories in the nonparent group were male relatives and others (U.S. Department of Health and Human Services [DHHS], 2013). More severe brain injury was caused by nonparental child abuse (Scribano, Makoroff, Feldman, & Berger, 2013). Moreover, a study investigating the association between physical morbidity and child abuse indicated that heavy burdens of medical illnesses and impaired physical functions imposed on adults might lead to emotional instability, which increases the risk of child abuse or neglect (Hwang, 2008). Therefore, identifying adults having a high risk of potential child abuse perpetration by using psychiatric and physical morbidities and other factors is crucial.
Previous population-based studies on perpetrators of child abuse have investigated a single type or a few types of mental disorders, or have focused on a small sample size with a limited number of associated factors. A study using a nationally representative sample of participants selected from 48 states in the United States reported that previous experiences of childhood abuse, internalizing disorders, and externalizing disorders contribute to parental abuse (Medley & Sachs-Ericsson, 2009). However, a knowledge gap exists concerning the risk of committing child abuse among patients with mental disorders, particularly prevalent psychiatric categories. Therefore, comparing the risk of child abuse among the comprehensive categories of mental disorders is required. Furthermore, most child abuse studies have used observational data and lack a counterfactual approach, such as inclusion of patients without psychiatric disorders, to increase the strength of inference for child abuse in general populations without limiting it to the parent–child relationship. This study aimed to identify factors that were related to child abuse perpetration. Therefore, on the theoretical basis of psychosomatic vulnerability to properly react to children in patients with unstable mental disorders, the act of child abuse was compared between patients with and without psychiatric disorders. Subsequently, the association between the category of physician-diagnosed mental disorders and the risk of child abuse perpetration was investigated only in patients with psychiatric disorders by using nationally representative data. Sociodemographic factors potentially associated with the act of child abuse were also examined.
Method
Hypothesis and Research Design
This study hypothesized the following:
In addition, the second hypothesis was as follows:
A longitudinal population-based retrospective design was used to examine the two hypotheses by analyzing nationwide data in Taiwan. This study was approved by the Research Ethics Committee at China Medical University Hospital, Taiwan.
Data Source and Study Sample
The National Health Insurance (NHI) program was launched in Taiwan on March 1, 1995. The Taiwan NHI Research Database (NHIRD) is a medical claims database maintained by the Ministry of Health and Welfare and the National Health Research Institutes of Taiwan. The NHIRD represents more than 99.7% of the entire population in Taiwan (Tsai et al., 2012). The database provides medical diagnoses in the format of the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes. In this study, a total of 1,000,000 patients were randomly selected from the 2002 to 2013 Taiwan NHIRD for analysis (longitudinal health insurance database 2005). The sample was created using a systematic sampling method to randomly extract a representative database from the entire NHIRD.
In this retrospective study, a cohort of patients who received a diagnosis of mental disorders on the basis of ICD-9-CM codes (290.x-319.x) was identified from the NHIRD. Patients aged <16 years or those with questionable or inadequate basic data, such as conflicting sex or uncertain birth date, were excluded. To ensure that mental disorder was the antecedent of child abuse, patients who committed child abuse before receiving a mental disorder diagnosis were excluded. Finally, 340,985 adult patients with mental disorders were included. The ICD-9-CM N-codes 995.5x were used to identify the event of all types of child abuse, including 995.5 (child maltreatment syndrome), 995.50 (child abuse, unspecified), 995.51 (child emotional/psychological abuse), 995.52 (child neglect, nutritional), 995.53 (child sexual abuse), 995.54 (child physical abuse), 995.55 (shaken infant syndrome), and 995.59 (other child abuse and neglect). Complementary E-code E967 was used to identify the perpetrator of child abuse. Therefore, this study could retrieve information on adult patients who committed child abuse from the claims data by using both N-codes 995.5x and E-code E967. The commission of the act of child abuse was recorded in the adult actor as a legal proof from the NHIRD. Victims could be the health insurance dependents of perpetrators.
In this study, 340,985 adult patients with mental disorders (case group) were randomly matched according to sex and age with patients without mental disorders (control group) by using the SAS Surveyselect Procedure (SAS Institute, Inc., Cary, NC, USA) to ascertain the comparability of two groups. Consequently, 681,970 individuals were considered eligible for the subsequent analysis. The present study is novel in terms of the identification of both mental disorders and child abuse from the NHIRD.
Variables
Child abuse perpetration (ICD-9-CM N-codes 995.5x and E-code E967) served as the outcome variable defined dichotomously and categorically for the occurrence (yes or no) and type of child abuse, respectively. Child abuse status was further classified into four types, namely, physical abuse, sexual abuse, other abuse, and no child abuse, on the basis of the ICD-9-CM. The N-codes 995.54 and 995.53 were used to define physical abuse (699 cases) and sexual abuse (44 cases), respectively. The remaining types were merged to form the group of other abuse (106 cases) to ascertain reliable statistical estimations. On the basis of the aforementioned literature, the following four major categories of independent variables that may be associated with the occurrence of child abuse were included in this study: mental health, physical health, demographic characteristics, and geographic characteristics. Mental disorders as a major independent variable were defined dichotomously on the basis of ICD-9-CM codes 290.x to 319.x. According to the existing literature and frequency distribution, mental disorders in the cohort design were classified into six categories by using ICD-9-CM, namely, anxiety disorders, affective disorders, schizophrenia, substance use disorders, personality disorders, and other disorders. The first diagnostic code often represents the prominent diagnosis of a mental disorder for a patient. Thus, to ensure a reliable classification, the diagnosis code of a mental disorder that occurred first and continued for at least 3 times in 6 months in a patient was used to determine the category of the mental disorder for that patient. The severity of physical illness was rated using the Charlson comorbidity index (Charlson, Pompei, Ales, & MacKenzie, 1987), and was classified into four ordinal levels on the basis of frequency distribution in this study. Demographic characteristics included sex, age, occupation, and low-income household. Geographic characteristics included region and urbanization level. The urbanization level was measured using a 7-level scale, including highly urbanized town = 1, intermediate urbanized town = 2, booming town = 3, usual town = 4, aged town = 5, agricultural town = 6, and remote town = 7. Demographic variables and geographic variables, except the urbanization level, were defined according to the Registry for Beneficiaries.
Statistical Analysis
Statistical methods used in this study included the chi-square test and logistic regression. The chi-square test was used to examine the observed prevalence rates of child abuse for bivariate associations. Binomial and multinomial logistic regressions were adopted to analyze the dichotomous and categorical outcome variables, respectively. In multivariate analysis, all other covariates were held equal and the odds ratios (ORs) were reported. In addition, this study performed collinearity diagnostics using indices such as variance inflation and tolerance to detect any biasing high interrelation among independent variables. The logistic regression analyses met the data assumptions, including nominal level of measurement, model fit, absence of multicollinearity, and sufficient sample size for maximum likelihood estimates. All tests were two sided and conducted on an alpha value of .05. Data were analyzed using SAS, Version 9.4 (SAS Institute, Inc.).
Results
This study identified a total of 1,391 adults with a record of child abuse perpetration in the NHIRD. Table 1 lists the results of the comparison of the prevalence of child abuse between the case and control groups. The results of the chi-square test revealed that the case group had a significantly higher likelihood of committing child abuse than did the control group (0.25% vs. 0.16%, 849 vs. 542 cases, p < .0001). Furthermore, no significant collinearity was observed.
Child Abuse Perpetration, by Mental Disorders, 2002 to 2013 (Case and Control Groups Randomly Matched by Sex and Age, Chi-Square Test, N = 681,970).
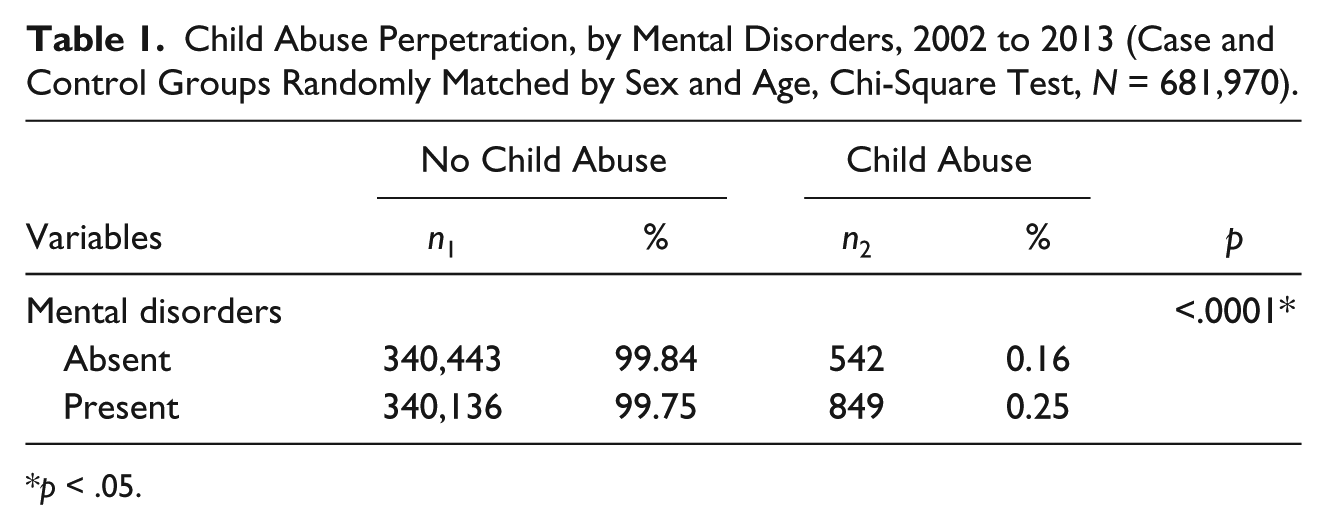
p < .05.
The unadjusted matched logistic regression analysis indicated that seven variables were significantly associated with the act of child abuse (Table 2, all ps < .05). After holding all other covariates constant, seven variables remained significantly associated with child abuse perpetration, namely, mental disorders, severity of physical illness, age, occupation, low-income household, region, and urbanization level (all ps < .05). Compared with the control group, the case group was significantly more likely to commit child abuse (adjusted OR = 1.464, 95% confidence interval [CI] = [1.311, 1.635], p < .0001). In addition, higher odds of child abuse were associated with presence of physical illness burden (Charlson comorbidity index [CCI] = 1, 2, and ⩾3; adjusted OR = 1.333, 2.531, and 2.522, respectively), nonhighest age groups (adjusted OR = 1.935-6.107), labor occupation (adjusted OR = 1.617, 95% CI = [1.410, 1.853]), veterans and religious group members (adjusted OR = 1.561, 95% CI = [1.317, 1.850]), low-income households (adjusted OR = 1.731, 95% CI = [1.166, 2.569]), non-Southern residents (adjusted OR = 1.574-4.699, highest: central region), and residents in Levels 3, 4, 6, and 7 of urbanization (adjusted OR = 1.979, 1.401, 2.268, and 2.702, respectively). Sex was not significantly associated with the occurrence of child abuse.
Association Between Mental Disorders and Child Abuse Perpetration, After Controlling for All Other Characteristics, 2002 to 2013 (Case and Control Groups Randomly Matched by Sex and Age, Binomial Logistic Regression, N = 681,970).
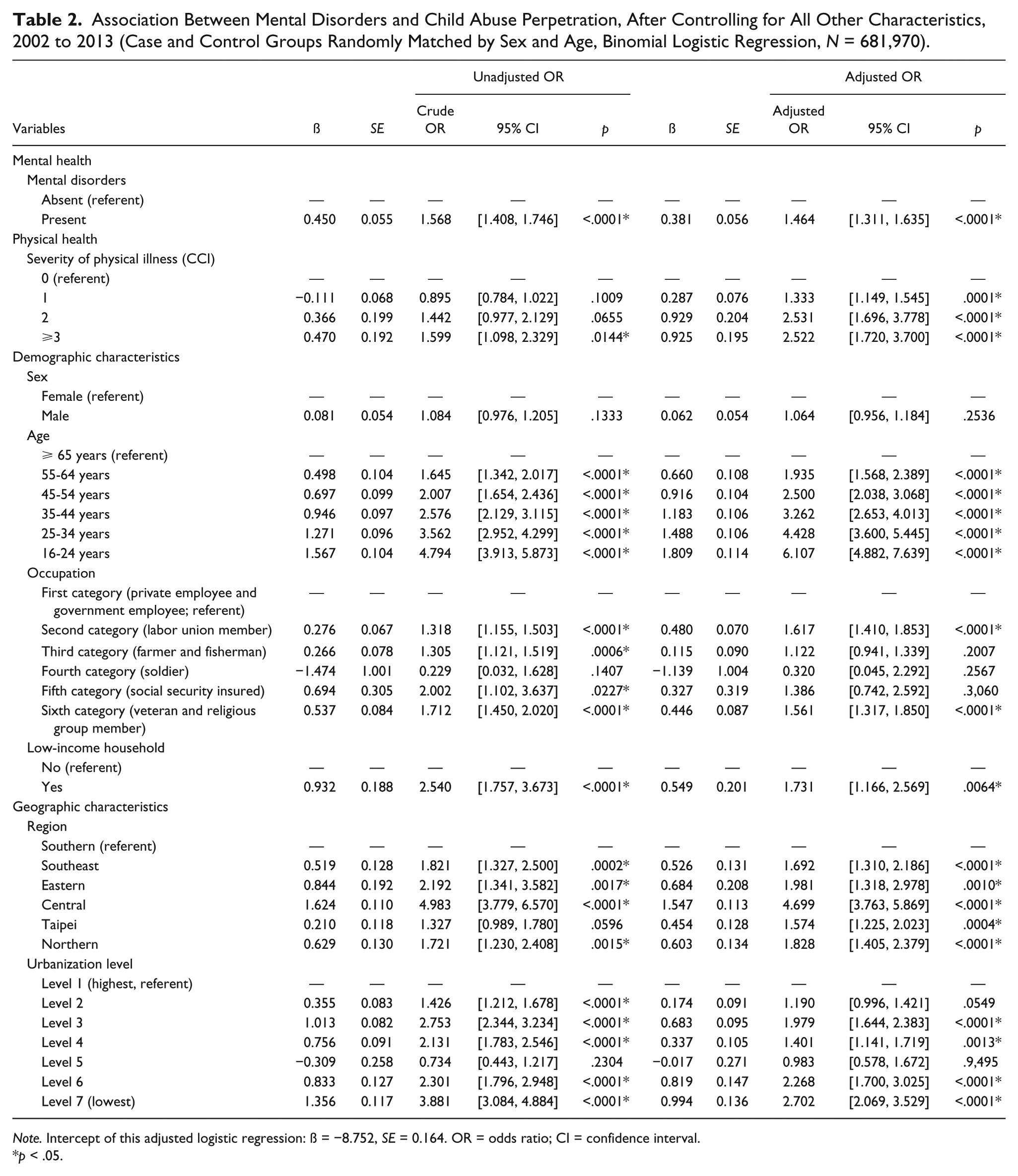
Note. Intercept of this adjusted logistic regression: ß = −8.752, SE = 0.164. OR = odds ratio; CI = confidence interval.
p < .05.
The chi-square test results indicated that among the patients with psychiatric disorders, seven variables were significantly associated with the act of child abuse, namely, category of mental disorders, severity of physical illness, age, occupation, low-income household, region, and urbanization level (Table 3, all ps < .05). Regarding the category of mental disorders, personality disorders, substance use disorders, and affective disorders were associated with a higher prevalence of committing child abuse (0.56%, 0.45%, and 0.40%, respectively). Other characteristics associated with a higher likelihood of child abuse included high severity of physical illness (CCI ⩾ 3, 0.34%), youngest age group (16-24 years, 0.63%), social security insured (0.46%), low-income households (0.66%), residents in the central region (0.58%), and residents in the lowest level of urbanization (Level 7, 0.58%).
Child Abuse Perpetration, by the Category of Mental Disorders and Other Characteristics, 2002 to 2013 (Chi-Square Test, N = 340,985).
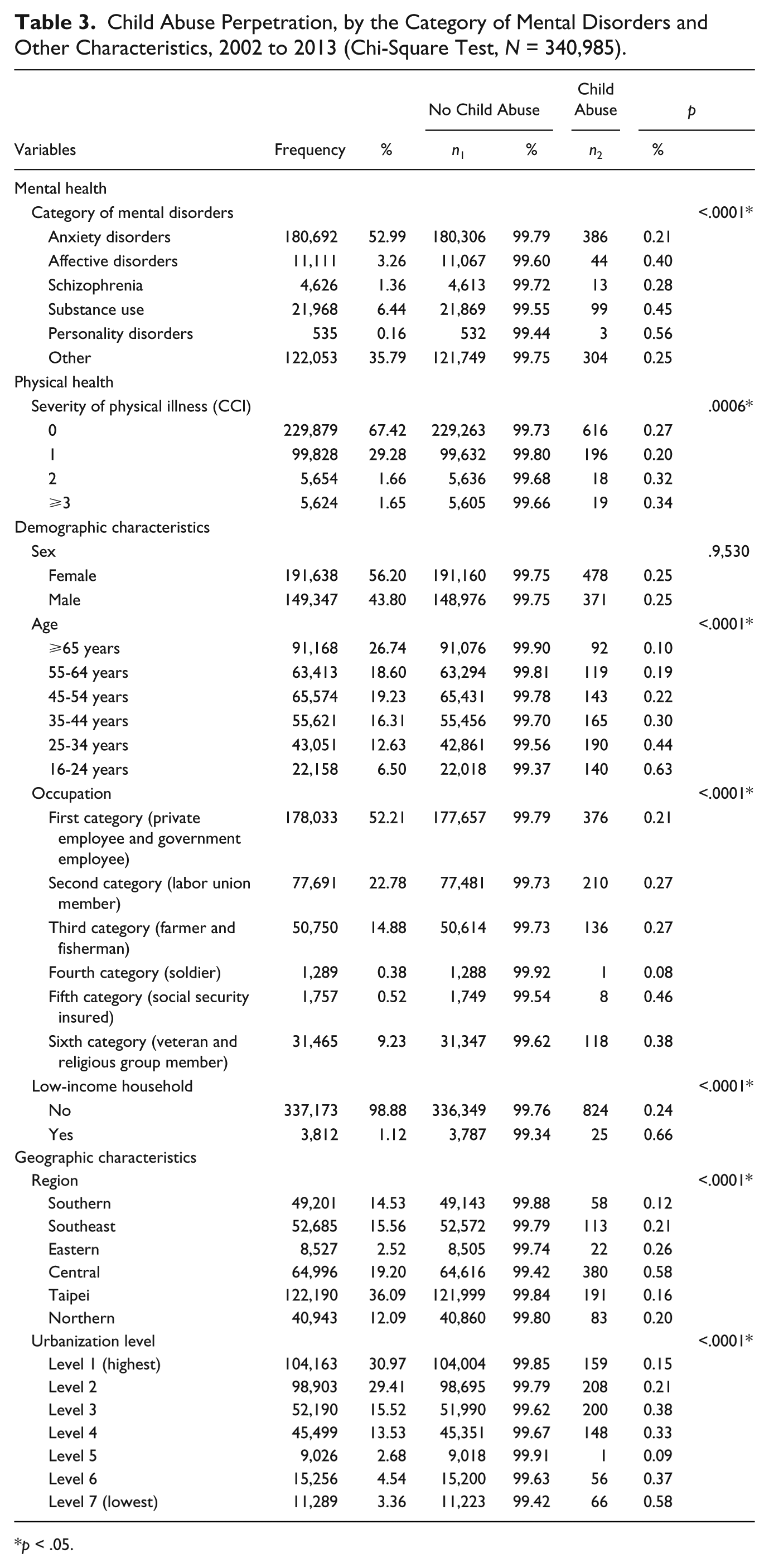
p < .05.
Table 4 lists the logistic regression results for the association between the category of mental disorders and child abuse perpetration. Eight variables were significantly associated with child abuse, namely, category of mental disorders, severity of physical illness, sex, age, occupation, low-income household, region, and urbanization level (all ps < .05). This study used anxiety disorders as a reference group of the outcome variable for all analysis levels. In the unadjusted analysis, affective disorders, substance use disorders, and other mental disorders were associated with higher odds of child abuse (crude ORs = 1.857, 2.115, and 1.166; 95% CIs = [1.359, 2.538], [1.695, 2.639], and [1.003, 1.356], respectively). After controlling for all other factors, the category of mental disorders remained significantly associated with child abuse. The odds of child abuse among the patients with substance use and affective disorders were higher (adjusted ORs = 2.032 and 1.728, CIs = [1.605, 2.571] and [1.262, 2.366], respectively). Other characteristics associated with higher odds of child abuse included CCI = 1, 2, and ⩾3 (adjusted ORs = 1.350, 2.569, 2.367, respectively), nonhighest age groups (adjusted ORs = 2.111-8.176), labor union members (adjusted OR = 1.557, 95% CI = [1.307, 1.856]), veterans and religious group members (adjusted OR = 1.569, 95% CI = [1.267, 1.943]), low-income households (adjusted OR = 1.866, 95% CI = [1.216, 2.862]), non-Southern residents (adjusted OR = 1.660-4.559, highest: central region), and residents in Levels 3, 4, 6, and 7 of urbanization (adjusted ORs = 1.905, 1.506, 2.479, and 2.868, respectively). Sex was not significantly associated with the occurrence of child abuse.
Association Between the Category of Mental Disorders and Act of Child Abuse, After Controlling for All Other Characteristics, 2002 to 2013 (Binomial Logistic Regression, N = 340,985).
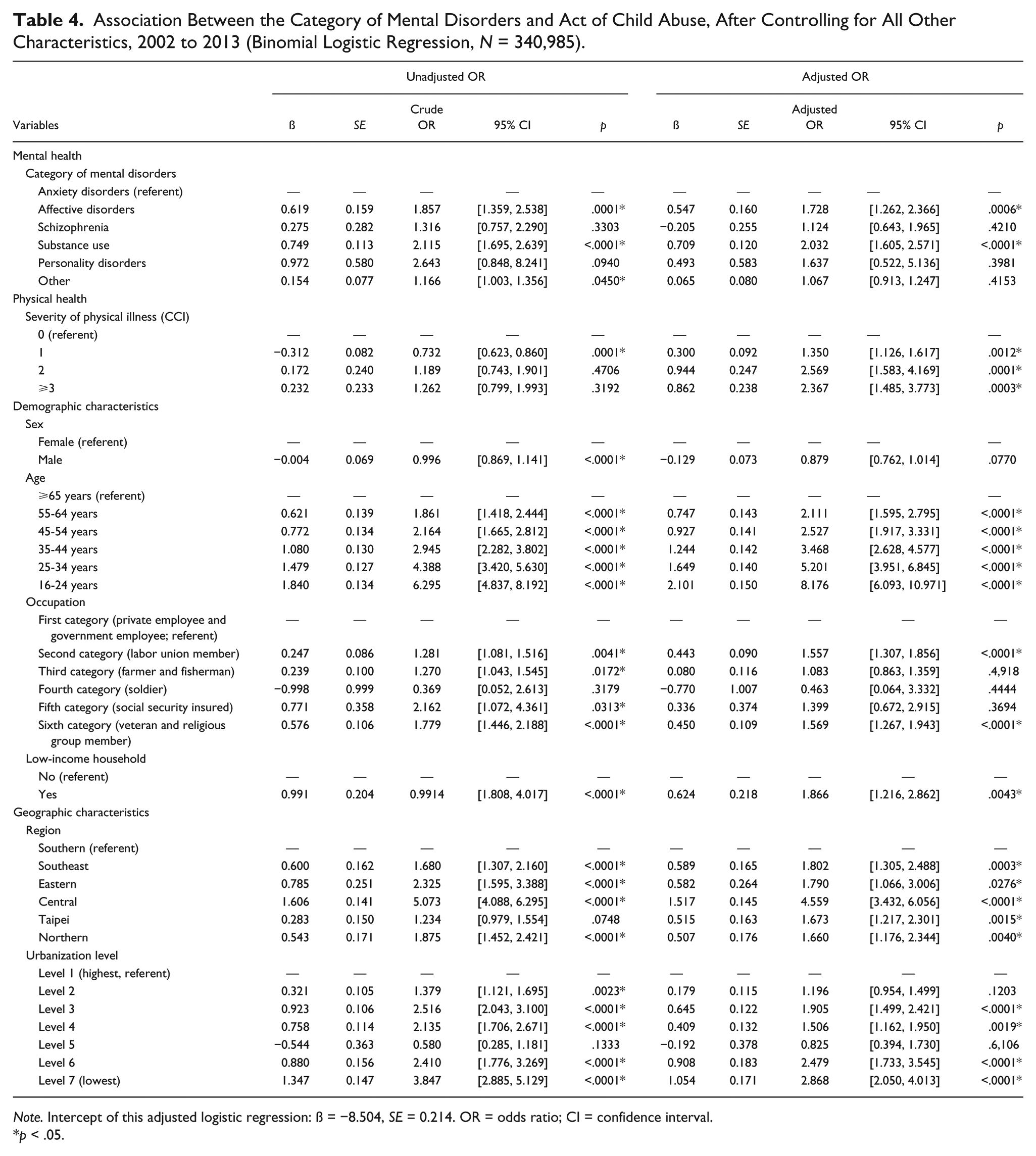
Note. Intercept of this adjusted logistic regression: ß = −8.504, SE = 0.214. OR = odds ratio; CI = confidence interval.
p < .05.
Schizophrenia and personality disorders were merged into the group of other disorders to ensure reliable estimations in the association between the category of mental disorders and type of child abuse. The chi-square test results revealed that the category of mental disorders was significantly associated with the type of child abuse (p < .0001, data not shown in the table). Substance use disorders and affective disorders were associated with a higher prevalence of physical abuse (0.41% and 0.30%, respectively). Other disorders were associated with a higher risk of sexual abuse (0.02%). Moreover, affective disorders were associated with a higher likelihood of other abuse (0.09%). Seven other variables significantly associated with the type of child abuse included severity of physical illness, sex, age, occupation, low-income household, region, and urbanization level (all ps < .05). Among all types of child abuse perpetrated by the patients with mental disorders, physical abuse was the most prevalent (82.33%), followed by other abuse (12.49%) and sexual abuse (5.18%, data not shown).
The results of the adjusted multinomial logistic regression indicated that seven variables were significantly associated with the type of child abuse perpetration (Table 5, all ps < .05). No child abuse was the reference group of the outcome variable in the multinomial logistic regression. Compared with no child abuse, the odds of physical abuse and other abuse both were significantly higher in patients with affective disorders than in patients with anxiety disorders (adjusted ORs = 1.566% and 2.835%, 95% CIs = [1.092, 2.246] and [1.429, 5.624], respectively). The odds of physical abuse were also significantly higher in patients with substance use disorders than in patients with anxiety disorders (adjusted OR = 2.018, 95% CI = [1.574, 2.586]). Other characteristics significantly associated with higher odds of physical abuse included a CCI score ⩾ 1, nonhighest age groups, labor occupation, veteran or religious group membership, low-income households, residing outside the Southeast region, and residing in a location with an urbanization level of 3, 4, 6, or 7 (all adjusted ORs > 1, data not shown). The odds of sexual abuse were significantly associated with residing in a location with an urbanization level of 2, 4, or 7 (all adjusted ORs > 1, data not shown). The odds of other abuse were strongly linked to the following characteristics: female, aged 16 to 54 years, residing in the Southeast region, and residing in a location with an urbanization level of 3 or 4 (all adjusted ORs > 1, data not shown).
Association Between the Category of Mental Disorders and Type of Child Abuse, After Controlling for All Other Characteristics, 2002 to 2013 (Multinomial Logistic Regression, N = 340,985).
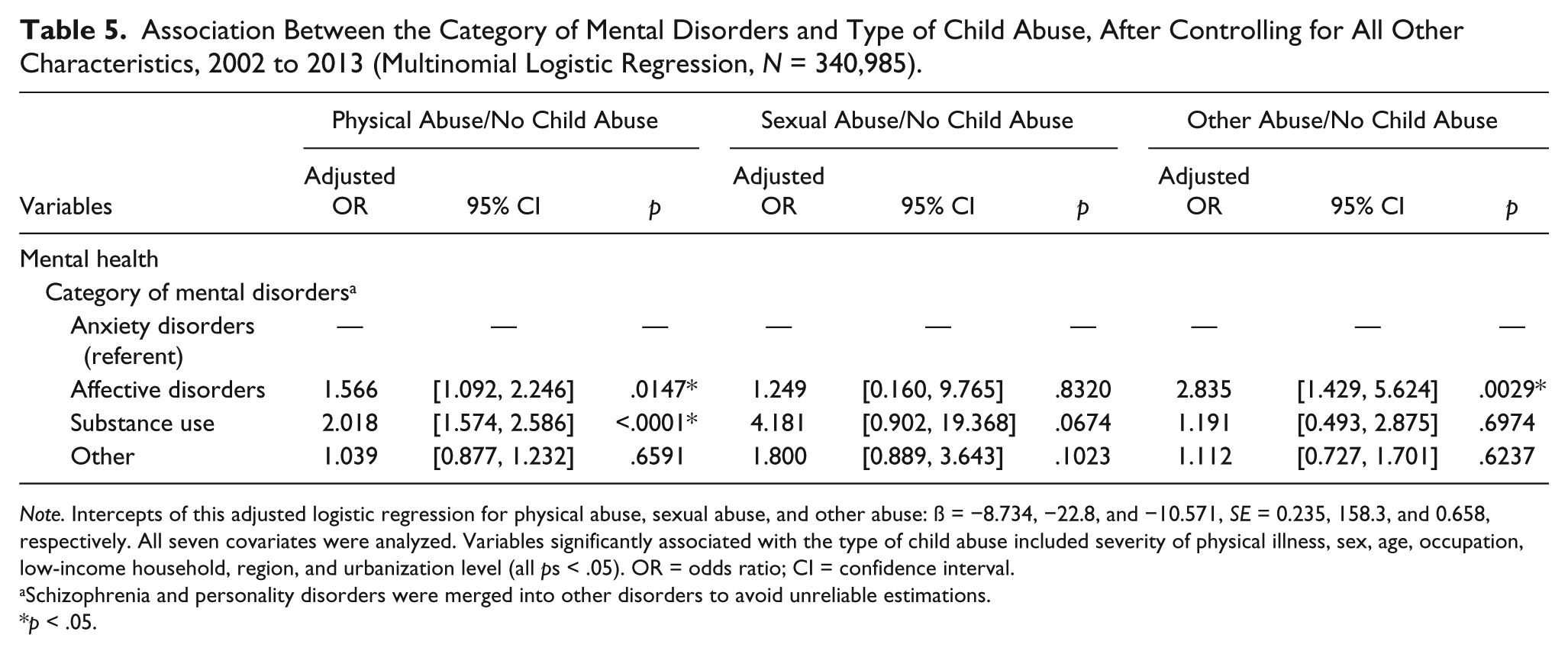
Note. Intercepts of this adjusted logistic regression for physical abuse, sexual abuse, and other abuse: ß = −8.734, −22.8, and −10.571, SE = 0.235, 158.3, and 0.658, respectively. All seven covariates were analyzed. Variables significantly associated with the type of child abuse included severity of physical illness, sex, age, occupation, low-income household, region, and urbanization level (all ps < .05). OR = odds ratio; CI = confidence interval.
Schizophrenia and personality disorders were merged into other disorders to avoid unreliable estimations.
p < .05.
Discussion
Higher Rate of Child Abuse Perpetration Among Patients With Mental Disorders
The findings of this study revealed that the adult patients with mental disorders were associated with an increased risk of child abuse than those without mental disorders (0.25% and 0.16%, respectively; Table 1). This result was similar to those reported in previous studies (Medley & Sachs-Ericsson, 2009; Walsh et al., 2002, 2003). However, to the best of our knowledge, this study is the first to comprehensively investigate the association between mental disorders and child abuse on the basis of a large population-based database with a randomly matched comparison. An adjusted OR of 1.464 represents a robust evidence of higher child abuse risk in patients with mental disorders (Table 2). Furthermore, the association between the category of mental disorders and the type of child abuse was identified. Substance use was linked to physical abuse, whereas affective disorders were related to physical abuse and other abuse (Table 5).
Highest Odds of Child Abuse Perpetration in Patients With Substance Use Disorders
Among the six categories of mental disorders, substance use and affective disorders had higher odds of child abuse. The literature on substance use has indicated a high risk of child abuse among patients of this group (Chaffin, Kelleher, & Hollenberg, 1996; Freisthler, Gruenewald, & Wolf, 2015; Murphy et al., 1991). The current study further confirms the risk through comparing the complete spectrum of mental disorders. Substance use disorder is identified as the highest risk category for child abuse. A study on substance abuse regarded emotional dysregulation as a predictor of child abuse (Ammerman, Kolko, Kirisci, Blackson, & Dawes, 1999); this could be attributable to poor impulse control, decreased frustration tolerance, and inability to cope with negative emotional states induced by substance abuse (Suchman, Decoste, Castiglioni, Legow, & Mayes, 2008).
In addition to substance use disorders, studies have indicated that psychiatric disorders associated with child abuse included depression, mania, schizophrenia, and personality disorders (Walsh et al., 2002). This study found that affective disorders were closely related to high odds of physical and other abuse. Previous studies have revealed that depression may lower the individual threshold of tolerating negative behaviors of children (Dopke, Lundahl, Dunsterville, & Lovejoy, 2003). Furthermore, depressive individuals may experience irritability because of difficulty in regulating their mood and, thus, are likely to respond with rejection to children (Joiner, Coyne, & Blalock, 1999).
Other Predictors of Child Abuse Warranting Attention
Studies have indicated an increased risk of abusive head trauma and other serious harms by nonparental individuals (Kiser et al., 2014; Scribano et al., 2013). Therefore, the prevention policy of child abuse should not be confined to parents, and may be extended to any individual who has close contact with children. Identifying high-risk individuals in domestic violence through medical records mining (Karakurt, Patel, Whiting, & Koyutürk, 2017) and providing treatment programs may be effective to abate the rate of child abuse (Andres-Lemay, Jamieson, & MacMillan, 2005).
Apart from the mental health status, other risk factors of child abuse were also identified, including high severity of physical illness, young age groups, labor occupation, veterans and religious group members, low income, central region, and low urbanization levels (Tables 2 and 4). Overall, these factors were considered as common potential risks of child abuse for individuals with and without psychiatric disorders. The finding of no difference in sex in child abuse is consistent with that of the relevant literature (Stier, Leventhal, Berg, Johnson, & Mezger, 1993; Walsh et al., 2002). However, the finding that female was associated with higher odds of other abuse yields a room for future investigations. The current study identified that young adults were more likely to commit child abuse. This finding is in agreement with that of previous studies and may implicate insufficient understanding of children’s needs and immature responses to children behavior of young adults (Stier et al., 1993). Although veterans and religious group members as an occupational category were evidently associated with child abuse (especially physical abuse), more studies are required to investigate occupational associations. The finding that low income was a risk factor for child abuse is consistent with those of previous studies (Butchart et al., 2006; Knutson, DeGarmo, Koeppl, & Reid, 2005). Region and urbanization level were identified as factors for child abuse in this study. However, the association between geographic characteristics and child abuse remain inconclusive (Moritsugu et al., 2015; Sedlak & Broadhurst, 1996; Weissman et al., 2003) because differences exist among underlying components of geographic characteristics, such as community structure and accessibility to health care, which may require further research. The central region, comprising one metropolitan city (Taichung) and two counties (Changhua and Nantou) located in central Taiwan, presents the highest odds of child abuse. This region is characterized by mountainous terrain, income inequality, and high household out-of-pocket medical expenditures (Chu, Liu, Chen, Tsai, & Chiu, 2005). Therefore, the finding of geographical disparities in the risk of child abuse provides policy implications in child abuse prevention. A prediction model of child abuse is lacking. Future research on factors associated with child abuse may consider the eight independent variables (Tables 2 and 4) in the model for analyzing diverse sample.
The limitations of this study stem from the administrative NHIRD used. First, the child abuse cases were possibly first reported by social workers and physicians and then entered by trained coders using ICD-9-CM N-codes 995.5x and E-code E967. These cases could, thus, be reliably identified as child abuse. However, information on nonsevere cases may not be included in this medical claims database. Therefore, the prevalence rate of child abuse may be underreported. This study could not analyze severity of child abuse in relation to psychiatric disorders. Second, the database does not contain information on children behavior and relationship between the perpetrator and the victim. The lack of such information attenuates the statistical testing power in this study. Nevertheless, child abuse in this study includes all relationship types, yielding a comprehensive investigation. Third, the severity of psychiatric morbidity could not be ascertained from the database, thus limiting further analysis. Fourth, the present study analyzed the sample of the populations in Taiwan. Therefore, the generalizability of the findings to other populations should be cautiously assessed. Finally, because of frequency distributions, other categories of mental disorders (including the dual diagnosis) and the types of child abuse could not be further classified. Future studies should focus on specific categories.
Conclusion
The present study adds to the base of knowledge regarding child abuse. This randomly matched comparison study demonstrated that patients with psychiatric disorders, particularly those with substance use and affective disorders from the cohort, had a higher risk of child abuse perpetration. In addition, other common risk factors for child abuse were identified, including high severity of physical illness, young age group, laborers and veterans, low income, and low urbanization levels. Substance use disorder is the major category of mental disorders associated with the act of child abuse, especially physical abuse. These findings are population based and can be beneficial to the community. Protection policies should center on psychiatrically sensitive prevention measures for child abuse, such as initially identifying families predisposed to child abuse perpetration by using psychiatric and physical morbidities and other risk factors identified by this study. The findings highlight the development of strategies to assist such vulnerable yet high-risk families.
Footnotes
Acknowledgements
The authors are grateful to Taiwan’s National Health Research Institutes for providing the NHIRD. The research team truly thanks Jia-Syun Yu, Min-Yan Lin, and Yu-Hsuan Lin for the assistance during the early stages of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Ministry of Science and Technology, Taiwan (Grant No. NSC 102-2410-H-039-006-SS2 and MOST 105-2410-H-039-008-MY2).