
Abstract
Sexual assault is a major public health concern associated with significant mental health and medical symptoms. Follow-up screening post-sexual assault medical forensic examination (SAMFE) can be one method of determining needs and providing targeted prevention of mental health and medical symptoms among individuals who experienced a recent sexual assault. However, the factors associated with engagement in post-SAMFE follow-up screening have not been identified. The current study examined the association between intimate partner violence victimization and sexual assault–related characteristics and engagement in post-SAMFE follow-up screening. Participants were 193 individuals who received a SAMFE and indicated at the time of SAMFE that they were interested in follow-up by the hospital. It was found that individuals were less likely to engage in follow-up screening if the assault was perpetrated by an intimate partner. These findings suggest that other resources are needed to reach individuals who experience sexual assault perpetrated by an intimate partner due to the unique needs of that population.
Keywords
Sexual assault is a serious public health problem in the United States. Approximately 20% of women and 1.5% of men experience an attempted or completed rape in their lifetime (Smith et al., 2017). Rape is defined as nonconsensual vaginal, oral, or anal penetration. Two factors that are closely associated with post-sexual assault outcomes are type of assault (e.g., intoxicated, forcible; Gilmore et al., 2018; Kaysen et al., 2010; Littleton, Grills-Taquechel, & Axsom, 2009; McCauley, Ruggiero, Resnick, Conoscenti, & Kilpatrick, 2009) and bodily injury sustained during the assault (Campbell, Dworkin, & Cabral, 2009; Dworkin, Menon, Bystrynski, & Allen, 2017). Sexual assault can lead to mental health and medical consequences (Campbell et al., 2009; Dworkin et al., 2017) including, but not limited to, posttraumatic stress disorder, depression, suicidal ideation and behaviors, alcohol and drug use, sexually transmitted infections (STIs), and unintended pregnancy. A post-assault follow-up examination is an ideal time to assess coping, social support resources, as well as reduce and/or treat physical and/or mental health symptoms, yet only 28% to 36% of individuals who experienced a sexual assault complete an in-person follow-up examination post-assault (Ackerman, Sugar, Fine, & Eckert, 2006; Darnell et al., 2015; Holmes, Resnick, & Frampton, 1998). However, the published rates are based on free follow-up clinical services being offered through a grant, which is not the norm. A phone screen conducted by a case manager that provides brief screening for mental health and medical symptoms and provides brief behavioral intervention is one way to reduce barriers to accessing care (e.g., costs, travel, time away from work), and may allow individuals to seek care at their preferred location (e.g., receive behavioral health treatment and/or STI testing from clinics where the individual has an established relationship with the provider) rather than from the hospital where they received a sexual assault medical forensic examination (SAMFE) after the assault. To increase the likelihood of secondary prevention for this at-risk population, it is essential to identify individuals who present for a SAMFE within days of the assault, but do not complete a follow-up screen post-SAMFE to connect to needed care. Accessing follow-up care may help reduce the public health cost burden of sexual assault, which is estimated to be approximately US$95,000 per sexual assault (DeLisi et al., 2010).
Potential barriers to accessing care post-SAMFE can include characteristics of the sexual assault (i.e., relationship of the perpetrator to the victim or injury sustained during the assault), race/ethnicity of the victim, lack of financial resources, logistical barriers (i.e., transportation or inability to manage multiple appointments), and the perception of not having been physically harmed during the assault (Resnick et al., 2000). Rape script theory is central to understanding the impact of sexual assault characteristics on the likelihood to receive services after sexual assault. According to rape script theory, people hold beliefs about the typical context in which rape occurs (Littleton, Axsom, & Grills-Taquechel, 2009; Turchik et al., 2009). Widely held rape scripts that are often influenced by rape myths or false beliefs about rape (Edwards, Turchik, Dardis, Reynolds, & Gidycz, 2011) include that rape occurs in outdoor locations, is perpetrated by strangers rather than by an intimate partner, and involves substantial injury (Turchik et al., 2009). People who experience rape that does not fit with these common rape scripts, such as those who experience sexual assault perpetrated by an intimate partner, may face barriers to receiving related services, while people who have experiences of rape that are more similar to widely held rape scripts may be more likely to seek services (Edwards et al., 2011; Ryan, 2011).
There has been a national focus on increasing access to the SAMFE with the expansion of the SAMFE in the reauthorization of the Violence Against Women and Department of Justice Reauthorization Act (2005). Prior to 2005, only individuals who formally reported to the police were granted a free SAMFE. After 2005, states receiving Violence Against Women Act (VAWA) funds were mandated to provide SAMFE free of charge despite formal reports to the police, thereby allowing free access to a SAMFE for individuals who have barriers to formal reports due to the type of assault (perpetrated by an intimate partner or use of alcohol at the time of the assault). Despite this change over a decade ago, there have been no similar movements to increase services available to individuals after the SAMFE. Therefore, it is necessary to identify assault-related characteristics associated with seeking care post-SAMFE to inform both clinical care and policy. The current research focuses on sexual assault characteristics, including partner type as a predictor of likelihood to complete a post-SAMFE screening.
Characteristics of Sexual Assault
Several characteristics of the sexual assault, including perpetrator relationship to the victim and perpetrator tactics, may influence the likelihood of an individual accessing follow-up care. The type of assault, defined as tactics used by the perpetrator, can include the use of physical force or threats of physical harm, or intoxicated sexual assault when an individual is unable to consent due to voluntary or involuntary intoxication from alcohol and/or drugs. Type of assault is important to consider because the use of drugs or alcohol as tactic for perpetration has been associated with receipt of follow-up care (Ackerman et al., 2006), and according to a recent study, one fourth of individuals attending an emergency department clinic after the assault reported alcohol or drug involvement during the assault (Rossman et al., 2018). Intoxicated sexual assault is a common form of rape (Kilpatrick, Resnick, Ruggiero, Conoscenti, & McCauley, 2007), yet it contradicts widely held rape scripts that suggest assaults must be perpetrated by a stranger and physical force must be used. Similarly, sexual assault perpetrated by an intimate partner does not follow the typical widely held rape script. Finally, individuals who sustained bodily injuries during the sexual assault may be more likely to engage in follow-up care. Not only do injuries match typical rape scripts, they often necessitate some form of follow-up care. Sexual assault–related injuries are associated with increased risk for mental health difficulties (e.g., posttraumatic stress disorder), highlighting the importance of enhanced access to services for this vulnerable population (Campbell et al., 2009; Dworkin et al., 2017).
Rape script theory would posit that people who experienced a sexual assault that occurred within the context of intimate partner violence (IPV), involved intoxication, or did not involve injuries would be less likely to receive follow-up services compared with individuals who experienced sexual assault perpetrated by someone other than a partner, with no intoxication during the assault, and the individual sustained physical or genital injuries during the assault. To understand and improve follow-up services for individuals who experience recent sexual assault, it is important to consider these sexual assault characteristics in relation to post-sexual assault follow-up care.
Post-Sexual Assault Follow-Up Care
It is estimated that 21% to 26% of adults who are sexually assaulted access a SAMFE within days of the sexual assault (Resnick et al., 2000; Zinzow, Resnick, Simone, Danielson, & Kilpatrick, 2012). A range of services following sexual assault is provided in emergency departments that have sexual assault nurse examiner (SANE) programs available in the United States. SANEs are trained to conduct a medical forensic exam, provide testing and/or prophylaxis for STIs, and offer emergency contraception to people seeking emergency services after a sexual assault (Welch & Mason, 2007). After a SAMFE, it is recommended to receive follow-up services in 2 weeks (Centers for Disease Control and Prevention, 2015) for additional testing for STIs, monitor for adherence and toleration of prophylaxis medication, and screen for mental health symptoms. However, only 28% to 36% of people who receive acute services in the emergency department complete the recommended follow-up visits (Ackerman et al., 2006; Darnell et al., 2015; Holmes et al., 1998). Identifying characteristics of sexual assault that are associated with follow-up screening can help to improve engagement in secondary prevention for medical and psychosocial consequences of sexual assault.
Current Study
The current study examined sexual assault characteristics associated with completing a follow-up screen post-SAMFE. To date, no research had examined relationship of perpetrator to the victim and perpetrator tactics in regard to likelihood of completing a follow-up screen. Such research can inform additional strategies needed to connect recent sexual assault victims to needed follow-up care. Consistent with previous research, we hypothesized that individuals who experienced an intoxicated sexual assault, assaults perpetrated by an intimate partner, and involved less injury would be less likely to complete a follow-up screen compared with those whose assault did not include alcohol or drug use. Injury at the time of assault is consistent with widely held rape scripts and predicts receiving medical care following the sexual assault (Zinzow et al., 2012) and attending follow-up exams after a SAMFE (Ackerman et al., 2006). Individual characteristics including age and ethnicity, as well as other assault characteristics including genital injury (defined as abrasions, lacerations, submucosal hemorrhages, contusions, avulsion, and petechiae), bodily injury, weapon use during the assault, and if the assault was perpetrated by an intimate partner were included as covariates in the analyses because of the potential association between those characteristics and completion of a follow-up screen.
Method
Participants
A total of 193 individuals who received a SAMFE within 120 hr of a sexual assault and who indicated at the time of the SAMFE that they were interested in a sexual assault follow-up visit were included in the analyses. There were 41 individuals who were not included in the current study because they indicated that they were not interested in follow-up care (16.7% of the total population of individuals who received a SAMFE). The majority of participants were women (93.8%). Participants were 18 to 62 years old (M = 29.45, SD = 10.37). Participants identified as White (70.5%), Black/African American (24.4%), Hispanic (4.7%), and Asian American (0.5%), largely similar to the state in which the clinic took place (68.5% White, 27.5% Black/African American, 5.5% Hispanic, and 1.6% Asian; U.S. Census Bureau, 2016).
Measures
Assault characteristics
Assault characteristics were identified by the SANEs at the time of the SAMFE. This included if the assault involved intoxication by alcohol or drugs, bodily and genital injury sustained during the assault, if a weapon was used during the assault, and if the assault occurred within the context of IPV. The assault was characterized as IPV if perpetrated by a partner, defined by the state as a "spouse; a former spouse; persons who have a child in common; or a male and female who are cohabitating or formerly have cohabitated" (South Carolina Code of Laws, 2015).
Engagement in follow-up screen
A follow-up clinic providing mental health and medical screening and referral to treatment post-SAMFE attempted to contact all individuals by phone who indicated an interest in receiving a follow-up screen for mental health and medical symptoms. This screen included mental health symptom questionnaires to assess current symptomology and assessment regarding whether the individual received STI testing after the SAMFE. Mental health screening questionnaires included the Alcohol Use Disorders Identification Test–Consumption Questions (AUDIT-C; Bush, Kivlahan, McDonell, Fihn, & Bradley, 1998) to assess for problematic alcohol use, drug use questions, the Patient Health Questionnaire (PHQ-9; Kroenke, Spitzer, & Williams, 2001) to assess depressive symptoms, and the Posttraumatic Stress Disorder Checklist (PCL-5; Weathers et al., 2013) to assess either acute (within 30 days of the assault) or posttraumatic stress (after 30 days of the assault). Participants were labeled as engaged in the follow-up screen if they completed screening questionnaires (either by phone or in person) at least one time after the SAMFE.
Procedures
Adults who presented to the emergency department within 120 hr of sexual assault received a SAMFE by the on-call SANE. Care provided by the SANEs met the standards of care and state guidelines for victim of crime services. Assault characteristics were recorded using standardized state protocol forms, from which the information was abstracted for internal purposes. At the conclusion of the SAMFE, the SANE offered the individual the opportunity to receive a follow-up screen to be completed over the phone or in person. The SANE office staff provided the follow-up clinic with forms completed by individuals who received a SAMFE indicating whether they were interested in follow-up clinic services. The follow-up clinic attempted to contact individuals for a follow-up screen within 1 week of the SAMFE as well as 1, 3, and 6 months after the SAMFE. Individuals were called up to 3 times during each follow-up time period if they did not answer.
If clinical levels of mental health symptoms were reported during the phone screen, brief behavioral interventions including sleep hygiene, in vivo exposure skills, brief behavioral activation, emotion regulation skills, distress tolerance skills, and relapse prevention for alcohol and drug misuse were provided over the phone depending on the symptoms identified. These brief behavioral interventions were provided by a bachelor’s level case manager, a social worker, predoctoral clinical psychology interns, or a psychologist, and all cases were reviewed and supervised by a licensed psychologist. Furthermore, if individuals were exhibiting clinical levels of mental health symptoms (i.e., clinically significant levels of depression, substance use, or acute stress symptoms), they were referred to appropriate behavioral health clinics depending on the symptom presentation. If individuals indicated that they had not yet scheduled or received STI testing post-assault, they were provided with locations to receive this care at low-cost community clinics and/or scheduled at the hospital-affiliated outpatient clinic. As part of the clinic hospital-affiliated outpatient clinic services, transportation was provided for attending appointments if needed to address barriers to accessing treatment.
Results
Descriptive Analyses
A total of 40.9% (n = 79) of individuals who were interested in follow-up care engaged in follow-up screening. Of the entire sample (n = 193), 67.0% of individuals were intoxicated at the time of the assault, 46.8% experienced bodily injury, 26.6% experienced genital injury, 11.5% encountered the use of a weapon during the assault, and 10.9% experienced a sexual assault that was perpetrated by an intimate partner. On average, individuals completed the follow-up screening 18.03 days (SD = 24.05 days) after the SAMFE with number of days after the SAMFE ranging from 0 to 105. A total of 45.6% of individuals completed the screening within 7 days of the SAMFE, 68.4% within 14 days, 74.7% within 21 days. Furthermore, the vast majority of individuals (92.4%) completed the screening within 60 days of the SAMFE.
Regression Analyses
To predict the probability of completing a follow-up screening, a series of univariate regression models were run using a forward selection approach in SPSS 25 (see Table 1). The only variable that was significant, and therefore remained in the model, was IPV (see Table 1). Findings revealed that individuals who were assaulted by an intimate partner were significantly less likely than those with perpetrators who were not an intimate partner to complete follow-up screening (odds ratio [OR] = 0.31, 95% confidence interval [CI] = [0.10, 0.95]). No other main effects were unique predictors of completing follow-up screens.
Results of Logistic Regression Models Predicting Follow-Up Visit.
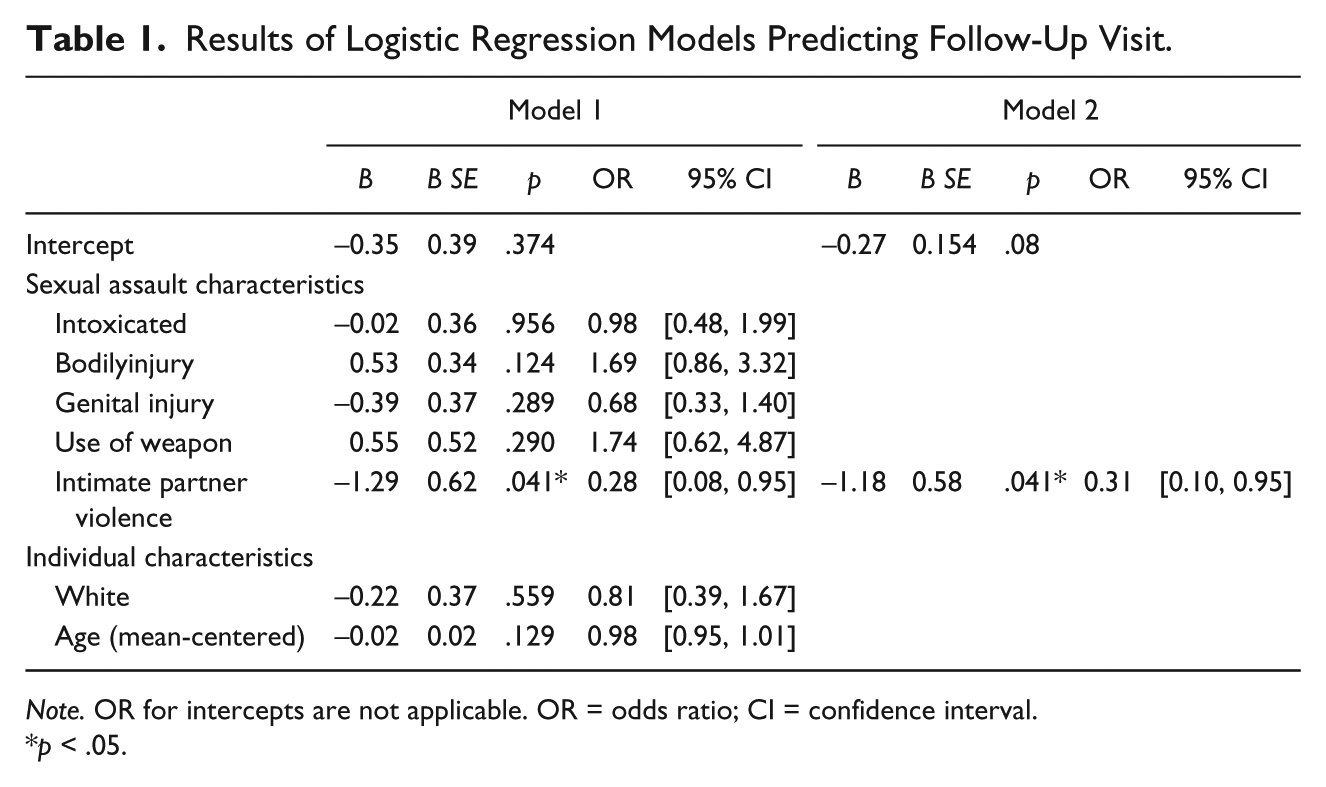
Note. OR for intercepts are not applicable. OR = odds ratio; CI = confidence interval.
p < .05.
Discussion
Due to the high rates of mental health and medical symptoms post-sexual assault, engaging in a follow-up screen post-SAMFE can provide a unique opportunity for secondary prevention efforts. The current study examined the association between assault characteristics and engagement in post-SAMFE follow-up screening. It was found that 40% engaged in a follow-up screen post-SAMFE, a similar proportion of individuals in previous research (28%-36% from Ackerman et al., 2006; Darnell et al., 2015; Holmes et al., 1998), suggesting that providing an initial screening offered over the phone with brief behavioral intervention may be beneficial in real-world settings. The hypotheses were partially supported. It was found that individuals were less likely to engage in a follow-up screen if the assault was perpetrated by an intimate partner. Therefore, a targeted effort to encourage individuals who are assaulted by an intimate partner is needed.
The findings of the current study suggest that individuals who experience sexual assaults that do not follow typical rape scripts—including that the assault is perpetrated by a stranger (Turchik et al., 2009)—are less likely to engage in a follow-up screen. There are already numerous barriers related to stigma associated with attending mental and sexual health care, and if the experience is atypical according to rape scripts, the stigma may be exacerbated. However, current results suggest that if the sexual assault is perpetrated by someone other than an intimate partner, individuals may experience less stigma; therefore, stigma regarding follow-up care may be reduced. Individuals with both IPV and sexual assault victimization have two potential avenues for follow-up services. Therefore, it is crucial to connect these individuals to care due to the potential for help that is available both in the community and through health care systems. Future research should examine perceptions of stigma and other barriers associated with completing a follow-up screen post-SAMFE for individuals who experienced a sexual assault perpetrated by an intimate partner.
It may also be possible that assault characteristics may be associated with more or less distress, as well as more or less concern about STI risk. It is possible that these differences in symptoms and STI concern may mediate the association between assault characteristics and engagement in follow-up care. The current study was unable to examine these associations because data regarding post-SAMFE symptoms and STI concern were only available from individuals who engaged in a follow-up screen. Future work should assess symptoms and STI concern at the time of the SAMFE to examine whether symptoms and STI concern mediate the association between assault characteristics and engagement in a follow-up screen.
Strengths, Limitations, and Future Directions
The results should be interpreted with the following limitations in mind. First, engagement in a follow-up screen was defined by the current study as completion of a mental and sexual health screener to determine the need for follow-up services and to connect to medical or mental health treatment if needed. Only individuals who were interested in a follow-up screen were contacted; therefore, the 41 individuals who were not interested were never contacted. Second, there were a limited number of men who completed a SAMFE; therefore, it was not possible to examine gender differences in follow-up screen completion. Third, this study focused on individuals who attended a SAMFE post-sexual assault and who were interested in follow-up from the hospital-affiliated outpatient clinic. Therefore, we did not have data from individuals who received a SAMFE and were not interested in follow-up, or individuals who experienced sexual assault but did not receive a SAMFE within 120 hr of the assault. Finally, the majority of individuals who experience sexual assault do not attend a SAMFE within days of the sexual assault, and those individuals may be even less likely to engage in follow-up screening than individuals who sought medical treatment immediately after the assault. Finally, future studies can improve on the current design by examining the frequency, severity, and type of IPV victimization to better understand how sexual assault victimization by an intimate partner might influence individuals’ motivations regarding whether or not to seek follow-up care. For example, existing literature suggests that the health care needs of women who experience IPV remain drastically unmet in the United States, particularly among culturally and ethnically diverse populations. More research is needed to increase the likelihood of mental and sexual health follow-up among individuals who do not receive a SAMFE (Calton, Cattaneo, & Gebhard, 2016; Lipsky & Caetano, 2007). It is unclear whether these individuals were not interested in completing a follow-up screen or whether they had significant barriers to answering the calls. More work is needed to determine barriers to accessing a follow-up screen.
The current study had several strengths. One strength was that the assessment used in the emergency department was part of standard clinical care provided within the SAMFE. Therefore, the secondary prevention implications of post-sexual assault mental health symptoms are based on real-world assessments that are already implemented within clinical practice. Another strength of the current study was the availability of follow-up screens to be conducted over the phone free of charge. This may have contributed to the slightly higher engagement rates compared with previous studies. Follow-up screens were available to individuals at no cost to patients due to the availability of grant-funded personnel. Future work could automate follow-up screens so that the service could be provided at no cost to the hospital or the patient. Finally, the interdisciplinary nature of the follow-up clinic team including an infectious disease medical doctor, a psychologist, a social worker, and a case manager as well as collaboration with a local sexual assault advocacy agency allowed for comprehensive services to be provided to individuals who were interested and engaged in post-SAMFE follow-up services.
Conclusion
The findings from the current study suggest that other resources are needed to reach individuals who experience sexual assault within the context of IPV. Targeted prevention for this high-risk group who is less likely to engage in follow-up screening is needed.
Footnotes
Acknowledgements
The authors would like to acknowledge the clinical staff, volunteers on the project, and individuals and community partners who assisted with project coordination which include, but are not limited to, Mollie Selmanoff, Dr. Ryan Byrne, Dr. Tatiana Davidson, Dr. Ally Dir, Dr. Rosaura Orengo-Aguayo, Karen Hughes, People Against Rape, and Dr. Heidi Resnick.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Manuscript preparation was partially supported by a grant from the National Institute on Drug Abuse (K23DA042935 to the first author), the National Institute of Mental Health (T32MH018869), the National Institute on Alcohol Abuse and Alcoholism (K23AA023845 to the last author), and by the South Carolina Clinical & Translation Research (SCTR) Institute, with an academic home at the Medical University of South Carolina NIH–NCATS Grant No. UL1 TR001450. The authors would also like to acknowledge the grant that funded the follow-up clinic that was awarded to the first author: This project is supported by the Federal Formula Grant No. 2015 VA GX 0001, awarded by the Office of Victims of Crime, U.S. Department of Justice through the South Carolina Department of Public Safety. Any points of view or opinions contained within this document are those of the author and do not necessarily represent the official positions or policies of the U.S. Department of Justice.