
Abstract
Aggressive incidents occur frequently in health care facilities, such as psychiatric care and forensic psychiatric hospitals. Previous research suggests that civil psychiatric inpatients may display more aggression than forensic inpatients. However, there is a lack of research comparing these groups on the incident severity, even though both frequency and severity of aggression influence the impact on staff members. The purpose of this study is to compare the frequency and severity of inpatient aggression caused by forensic and civil psychiatric inpatients in the same Dutch forensic psychiatric hospital. Data on aggressive incidents occurring between January 1, 2014, and December 31, 2017, were gathered from hospital files and analyzed using the Modified Overt Aggression Scale, including sexual aggression (MOAS+). Multilevel random intercept models were used to analyze differences between forensic and civil psychiatric patients in severity of aggressive incidents. In all, 3,603 aggressive incidents were recorded, caused by 344 different patients. Civil psychiatric patients caused more aggressive incidents than forensic patients and female patients caused more inpatient aggression compared with male patients. Female forensic patients were found to cause the most severe incidents, followed by female civil psychiatric patients. Male forensic patients caused the least severe incidents. The findings have important clinical implications, such as corroborating the need for an intensive treatment program for aggressive and disruptive civil psychiatric patients, as well as emphasizing the importance of gender-responsive treatment.
Aggressive incidents occur frequently in psychiatric hospitals, in general psychiatric care as well as in forensic psychiatric hospitals. A review of 424 studies on inpatient aggression found that forensic patients have higher rates of violence than general psychiatric patients, but these differences disappeared when controlling for the longer duration of forensic treatment (Bowers et al., 2011). Taking the occupied bed days into account, the risk of experiencing aggression for staff members was found to be lower in forensic settings than in general psychiatry. However, a meta-analysis on these studies shows a very large variation in study outcomes (Bowers et al., 2011). This heterogeneity is likely due to several factors, such as differences in settings and countries, with different legislations and policies. For example, more aggressive incidents occur on acute wards compared with other types of wards (Bowers et al., 2011). As a result, it is difficult to compare different studies across settings and countries on inpatient aggression.
It is important to compare forensic and civil psychiatric patients regarding their aggressive behavior, as findings of previous research suggest that civil psychiatric patients may resemble or even surpass forensic patients in the risk these patients pose, both during and after their treatment. For example, relatively high rates of inpatient aggression were found in both of these groups, with a higher prevalence rate among the civil psychiatric patients (Verstegen, De Vogel, De Vries Robbé, & Helmerhorst, 2017). A study following male patients with schizophrenic disorders after discharge from a psychiatric hospital found that civil psychiatric patients displayed more aggression toward others in the community than forensic patients (Hodgins et al., 2007). Information on the frequency and severity of aggressive incidents caused by forensic and civil psychiatric patients is important for the implementation of preventive measures and for acknowledgment of the staff members working with these patients, as patient aggression places a considerable burden on the psychiatric staff. The impact of aggression on staff members is dependent on both the frequency and severity of aggression (Nijman, Bowers, Oud, & Jansen, 2005). A systematic review of the impact of patient aggression found that staff members commonly experience posttraumatic stress symptoms, guilt, self-blame, and shame (Needham, Abderhalden, Halfens, Fischer, & Dassen, 2005). Inpatient aggression has a negative impact on an organizational level as well. Absenteeism caused by aggressive incidents results in greater costs for the organization. Furthermore, the risk of experiencing aggression may lead to difficulties in the recruitment of new staff, as well as in retaining current employees (Jackson, Clare, & Mannix, 2002).
Types of Aggression
Research on aggression has been impeded by a myriad of definitions of aggression, which has resulted in considerable differences between studies regarding what types of behavior are considered aggressive. In the past, many studies focused exclusively on physical aggression. Self-harm is often studied separately from aggression directed to others or objects, but there are good reasons to include self-harm in the definition of aggression. It involves the intentional infliction of physical harm toward oneself and can cause psychological harm to others who are confronted with these behaviors. Therefore, following the definition proposed by Rippon (2000), the current study includes verbal aggression, aggression toward objects, self-harm, physical aggression, and sexual aggression, which was carried out with the intent to harm or with indifference regarding whether harm would occur.
Severity
While many researchers have studied factors relating to the occurrence of inpatient aggression, studies focusing on the severity of aggression are rather scarce. The studies that do include severity often lack depth in their operationalization of the construct. For example, some studies consider different types of aggression as a way to distinguish severe and less severe incidents. These studies define severe aggressive incidents as incidents involving physical aggression to others (Daffern, Howells, Ogloff, & Lee, 2005) and/or sexual aggression (Nicholls, Brink, Greaves, Lussier, & Verdun-Jones, 2009) and consider all other forms of aggression to be less severe. However, this approach underestimates the severity of other types of aggression. Verbal aggression can seriously affect the staff member’s psychological well-being and can even lead to the development of posttraumatic stress disorder (Inoue, Tsukano, Muraoka, Kaneko, & Okamura, 2006). Other studies focus on staff injuries to gauge the severity of the incident (Bader, Evans, & Welsh, 2014), even though this limits the severity measure to a small minority of incidents (Nicholls et al., 2009).
There are several instruments available that include a numerical severity measure, such as the Overt Aggression Scale (OAS; Silver & Yudofsky, 1987), the Staff Observation Aggression Scale–Revised (SOAS-R; Nijman et al., 1999), and the Modified Overt Aggression Scale (MOAS; Kay, Wolkenfeld, & Murrill, 1988). All these scales include the same types of aggression, but differ in the way the severity score is calculated. For example, Abderhalden and colleagues (2007) used the SOAS-R to distinguish severe (scores 9-22) and less severe incidents (score ≤8) and included severity in a logistic regression model. Over half of the incidents (52.1%) were coded as severe.
Gender Differences in Aggression
There are several patient characteristics that may influence the relationship between legal status and inpatient aggression (Linhorst & Scott, 2004). Patient sex is one of these characteristics. In the general population, it is a robust finding that men display more aggressive behavior than women (e.g., Bettencourt & Miller, 1996). However, aggressive incidents in psychiatric hospitals often involve female aggressors. In some studies, female and male forensic and civil psychiatric inpatients are found to be equally likely to display physical aggression (Daffern et al., 2005; Nicholls et al., 2009). There is also research suggesting that female inpatients exhibit more aggression compared with their male counterparts (Broderick, Azizian, Kornbluh, & Warburton, 2015; Verstegen et al., 2017). There may be an interaction effect between gender and patient population, as a meta-analysis found that among forensic patients, women are more likely to engage in aggression, whereas in non-forensic wards, male patients are more likely to cause aggressive incidents (Dack, Ross, Papadopoulos, Stewart, & Bowers, 2013).
In addition to differences in the frequency of aggressive behaviors, there may also be gender differences in the severity of the aggression. No gender differences were found in the likelihood of aggressive incidents resulting in injury to others, neither among civil psychiatric inpatients (Lam, McNiel, & Binder, 2000) nor among forensic inpatients (Nicholls et al., 2009). A study among acute civil psychiatric patients found that aggressive incidents caused by female patients had higher SOAS-R severity scores (Grassi, Peron, Marangoni, Zanchi, & Vanni, 2001).
Psychopathology of the Aggressor
Psychopathology may influence the occurrence of aggressive behavior. Psychotic disorders are associated with a higher prevalence of aggression in psychiatric wards than other disorders (Cornaggia, Beghi, Pavone, & Barale, 2011). A higher prevalence of positive symptoms, such as hallucinations and delusions, increases the rate of aggression among psychotic patients (Witt, Van Dorn, & Fazel, 2013). Furthermore, patients with a diagnosis of schizophrenia were found to cause aggressive incidents with higher severity scores on the SOAS-R (Abderhalden et al., 2007; Grassi et al., 2001).
Research Questions
This study compares the aggressive behavior exhibited by forensic and civil psychiatric inpatients who are treated in the same Dutch forensic hospital in a 4-year time period. The main research question on the differences between forensic and civil psychiatric patients is divided into two subquestions.
Frequency
The first subquestion is as follows: Do forensic and civil psychiatric patients differ in the frequency of aggressive incidents in the hospital? Are these differences moderated by the patient’s gender or primary diagnosis of a psychotic disorder? Based on the literature described above, the following hypotheses were formulated:
Severity
The second subquestion is as follows: Do forensic and civil psychiatric patients differ in the severity of the aggressive incidents they cause? Are these differences moderated by the patient’s gender or primary diagnosis of a psychotic disorder?
Method
Setting
The study was conducted in the high-security forensic psychiatric hospital Van der Hoeven Kliniek in Utrecht, The Netherlands. The hospital has a total number of 262 beds. Approximately 183 of these beds are occupied by forensic patients receiving court-mandated treatment following a serious offense (in Dutch: terbeschikkingstelling, TBS). The TBS-order is a judicial measure which can be imposed on offenders suffering from mental illnesses who, as a result of their disorder, are considered to have diminished responsibility for their offense and have a high risk of recidivism. A regular TBS-order does not have a fixed duration, as the offender remains hospitalized as long as the court considers this to be necessary for the protection of others. The hospital provides an evaluation and advice to prolong or end the TBS-order every 1 or 2 years. The average treatment duration for the forensic patients is 8.7 years. The majority of patients serve a prison sentence before the start of the treatment order.
The hospital also includes a 53-bed facility for the treatment of civilly committed psychiatric patients whose treatments in less secured psychiatric settings have failed due to the patient’s severely aggressive or disruptive behavior (Van Rooijen & Neijmeijer, 2014). The average treatment duration is 1 year, after which they are typically transferred to another psychiatric hospital with a lower security status. Finally, a minority of patients are admitted with a forensic judicial status other than TBS. For example, offenders can receive a conditional sentence, under the condition that they are admitted for treatment in a forensic hospital. Treatment under these judicial statuses is less intrusive than treatment under a TBS-order.
Sample
Between January 1, 2014, and December 31, 2017, 542 patients have been admitted to the hospital. This included 302 (55.7%) forensic TBS patients and 212 (39.1%) civil psychiatric patients. Twenty-seven (5.0%) patients had a forensic judicial status other than TBS, and one TBS patient got discharged, but returned a year later as a civil psychiatric patient. These 28 patients were excluded from the analyses including legal status. There were 98 female patients (18.1%) and 444 (81.9%) male patients, with equal proportions of female forensic patients (18.5%) and female civil psychiatric patients (18.4%). Almost half of the patients (47.2%) were diagnosed with any kind of psychotic disorder and 30.8% had a personality disorder as their primary diagnosis, most commonly borderline or antisocial personality disorder. The majority of civil psychiatric patients (63.2%) had a psychotic disorder as their primary diagnosis, versus only 31.8% of forensic patients. Almost half of the forensic patients (49.8%) had a personality disorder as their primary diagnosis, compared with 23.7% of civil psychiatric patients. The average age of patients who displayed aggression was 36.9 years (range = 19-68). Forensic TBS patients who displayed aggressive behavior were on average older (M = 41.4 years, range = 20-68) than civil psychiatric patients displaying aggression (M = 32.8, range = 19-63), t(3275.8) = −25.8, p < .001. Regarding diversity concerns, this study includes all patients who have been admitted to the forensic hospital Van der Hoeven Kliniek during the study period, regardless of their gender, race, age, religion, or any other aspect.
Procedure
This research entails a quantitative study, where data on the aggressive incidents occurring between January 1, 2014, and December 31, 2017 were gathered from daily hospital reports. These reports inform staff members and patients of current events in the hospital, including aggressive incidents. A more comprehensive description of each incident was subsequently retrieved from the daily notes in the patient’s file, which was used to score the severity of the aggressive incident. The hospital does not yet have standard incident registration. Therefore, the information on aggressive incidents was gathered specifically for the purpose of this study. The incidents were scored by the first author. Information regarding the patient’s gender and primary diagnosis was also gathered from the patient’s file. For the two patients with gender dysphoria, each patient’s gender was coded to conform to their gender identity. Ethical approval for this study was obtained from the Ethical Review Committee Psychology and Neuroscience in Maastricht.
Measures
The aggressive incidents were scored on the category and severity of aggression using the MOAS. This is a validated instrument for rating aggressive behavior (e.g., Margari et al., 2005; Oliver, Crawford, Rao, Reece, & Tyrer, 2007). The MOAS consists of four categories of aggression. Within these categories, four different levels of severity are distinguished, ranging from light (1) to extreme (4). Each severity level has a description of what types of behaviors are classified as such. A total severity score is calculated by multiplying the severity level with Factor 1 for verbal aggression, Factor 2 for aggression against objects, Factor 3 for autoaggression, and Factor 4 for physical aggression (Kay et al., 1988). A revised version of this scale called the MOAS+ was developed by Crocker and colleagues (2006). They added a fifth category, sexual aggression, again with four levels of severity ranging from light to extreme. However, the category of sexual aggression was not included in the severity scoring.
A random sample of 10% of incidents was coded independently by the second author to calculate the interrater reliability. This was performed using two-way random-effects consistency intraclass correlation coefficient (ICC), in accordance with the procedure described by Landers (2015). The interrater reliability was excellent, with ICCs ranging from .866 for sexual aggression to .933 for aggression against objects.
Data Analysis
The statistical analyses were carried out using IBM SPSS version 25. For all tests, assumptions were checked as described in Field (2013). First, a general overview of the number of incidents and the number of patients involved in aggressive incidents was provided using descriptive statistics. To test whether forensic and civil psychiatric patients differed in the frequency of aggressive incidents, Mann–Whitney U test was used. The Mann–Whitney U test was chosen due to the positive skew in the distribution (many patients did not display any aggression) and due to a rather large number of outliers. Mann–Whitney U tests were also used to test for gender differences and differences between patients with and without a diagnosis of psychotic disorders in the frequency of aggressive incidents. Hierarchical multiple linear regression analysis with bootstrap resampling of 1,000 samples was used to test for interaction effects.
A multilevel linear regression analysis was carried out to test whether civil and forensic patients differed in the severity of the aggressive incidents they caused. Patient gender and having a primary diagnosis of a psychotic disorder were included in the model as potential moderator variables. A random intercept + scaled identity covariance structure was used for all models involving multilevel analysis.
Results
Frequency
General overview
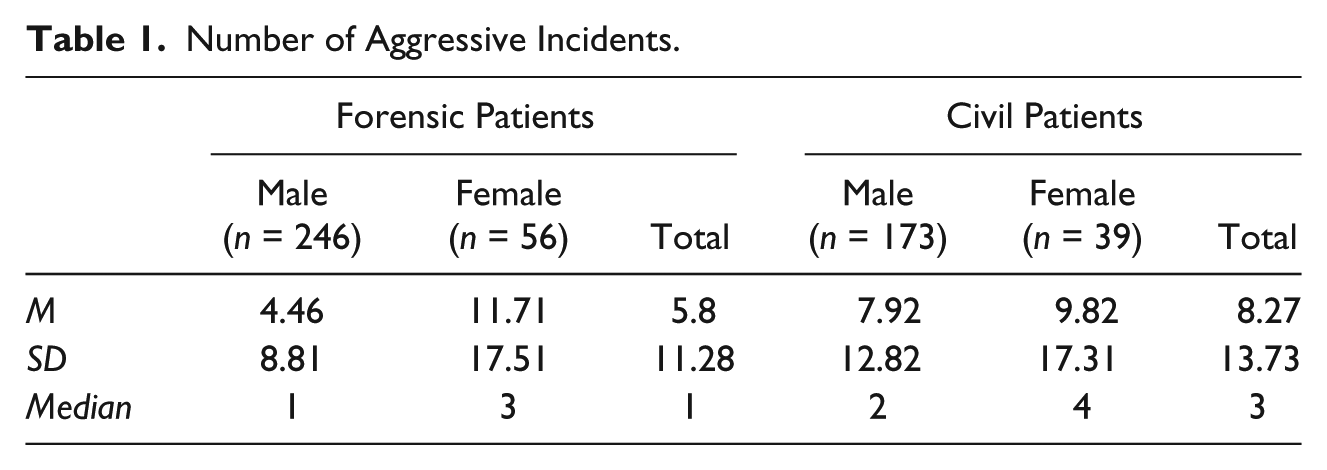
Of the 542 patients admitted to the forensic hospital during the study period, 344 patients (63.5%) caused at least one aggressive incident. Of these 344 patients, 270 (78.5%) caused more than one incident. Thirteen patients caused more than 50 incidents each and one female civil psychiatric patient caused 97 incidents, which included one incident involving aggression toward self and 96 incidents involving aggression toward others and/or objects. Of the 3,603 aggressive incidents recorded, 1,766 (49.0%) were caused by forensic TBS patients, 1,747 (48.5%) were caused by civil psychiatric patients, and 90 incidents (2.5%) were caused by patients with a forensic status other than TBS. Patients differed greatly in the number of incidents they caused, which results in large standard deviations (see Table 1). As a consequence, the median is more appropriate in comparing the frequency of aggressive incidents of forensic and civil psychiatric patients than the mean.
Number of Aggressive Incidents.
Legal status
Patients with a forensic status other than TBS were excluded from the following analysis. The number of aggressive incidents caused by each patient ranged from 0 to 97 among civil psychiatric patients and from 0 to 69 among forensic patients. Civil psychiatric patients caused significantly more incidents than forensic TBS patients, U = 26,901, z = 3.16, p = .002, r = .14.
Patient gender
Female patients were found to cause significantly more aggressive incidents than male patients, U = 17,029.5, z = −3.46, p = .001, r = .15. Almost one third (30.3%) of the aggressive incidents were caused by female patients, even though they only made up 18.1% of the patient population. The median number of incidents was 1 for male patients and 4 for female patients. When incidents involving autoaggression were not included in the analysis, female patients were still found to cause more aggressive incidents than male patients, U = 17,923, z = −2.81, p = .005, r = .12.
Primary diagnosis
No significant differences were found in the number of incidents caused by patients with psychotic disorders or a different primary diagnosis, U = 39,180.5, z = 1.68, p = .093. In addition, having a primary diagnosis of a psychotic disorder did not moderate the relationship between legal status (excluding forensic status other than TBS) and number of incidents, b = −0.58, 95% confidence interval (CI) = [−5.11, 3.94], p = .801.
Interaction between legal status and patient gender
The following analyses exclude patients with a forensic status other than TBS. The main effect of legal status remained significant when controlled for patient gender, b = −2.56, p = .025, 95% bias-corrected and accelerated (BCa) CI = [−4.74, −.039]. The main effect of patient gender also remained significant, b = −5.10, p = .005, 95% BCa CI = [−9.03, −1.89]. Although small differences appeared between men and women in the two patient groups (see Table 1), adding the interaction term between patient gender and legal status did not result in a significant improvement in the model, ΔR2 = .007, p = .057. Thus, patient gender does not moderate the relationship between legal status and number of incidents. Although legal status and gender were significant predictors, the effect size of the total model was small, R2 = .042.
When incidents involving autoaggression were excluded from the analysis, the model did not change. The main effect of legal status remained significant, b = −2.60, p = .015, as well as the main effect of patient gender, b= −4.32, p = .001. Adding the interaction term between patient gender and legal status did not improve the model, ΔR2 = .006, p = .104.
Severity
Verbal aggression was the most frequent type of aggression, with 74% of all incidents including verbal aggression. Sexual aggression was the least prevalent type of aggression, present in only 4.4% of recorded incidents (see Table 2). As sexual aggression is not included in the MOAS severity scoring, the 100 incidents including only sexual aggression were excluded from the following analyses, as were incidents caused by patients with a forensic status other than TBS.
Prevalence of Different Types of Aggression.
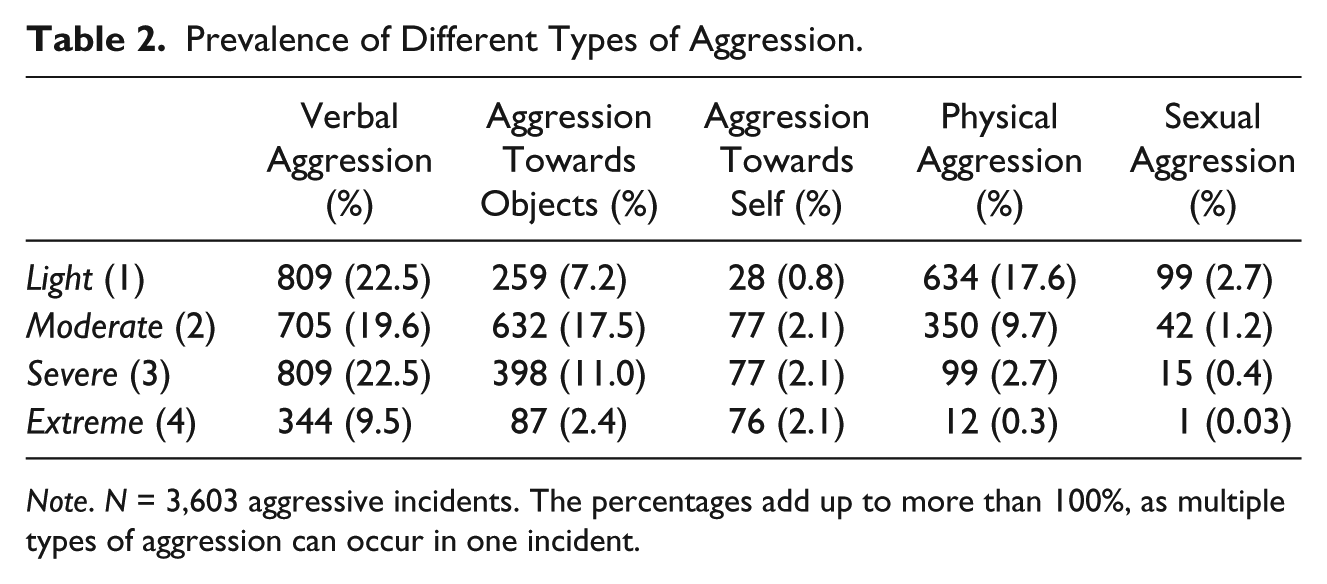
Note. N = 3,603 aggressive incidents. The percentages add up to more than 100%, as multiple types of aggression can occur in one incident.
Legal status and patient gender
The relationship between legal status and incident severity showed significant variance in intercepts across patients, Var(u0j) = 2.41, χ2(1) = 293.12, p < .01. Forensic and civil psychiatric patients did not differ regarding the severity of the incidents they caused, F(1, 292.74) = 0.41, p = .521.
There was significant variance in intercepts across patients regarding the relationship between patient gender and incident severity, Var(u0j) =1.90, χ2(1) = 219.30, p < .01. Female patients caused significantly more severe incidents than male patients, F(1, 230.53) = 39.01, p < .001. The average severity score of incidents caused by female patients was 6.91 (SE = 0.23), compared with an average severity of 5.24 (SE = 0.13) for incidents caused by male patients.
A random intercept model including legal status, gender, and the interaction between legal status and gender as fixed effects was found to be significantly better than the model including only legal status as a fixed effect, χ2(2) = 41.46, p < .01, and significantly better than the model including only patient gender as a fixed effect χ2 (2) = 515.82, p < .01. In this model, patient gender remained a significant predictor, F(1, 228.48) = 30.62, p < .001. However, there was also a significant interaction effect between gender and legal status, F(1, 266.60) = 10.23, p = .002. Female forensic patients were found to cause the most severe incidents, with an estimated marginal mean severity score of 7.23 (SE = 0.29), followed by female civil patients (M = 6.23, SE = 0.36). Male civil patients had a mean severity of 5.58 (SE = 0.19), and the least severe incidents were caused by male forensic patients (M = 4.91, SE = 0.19; see Figure 1).
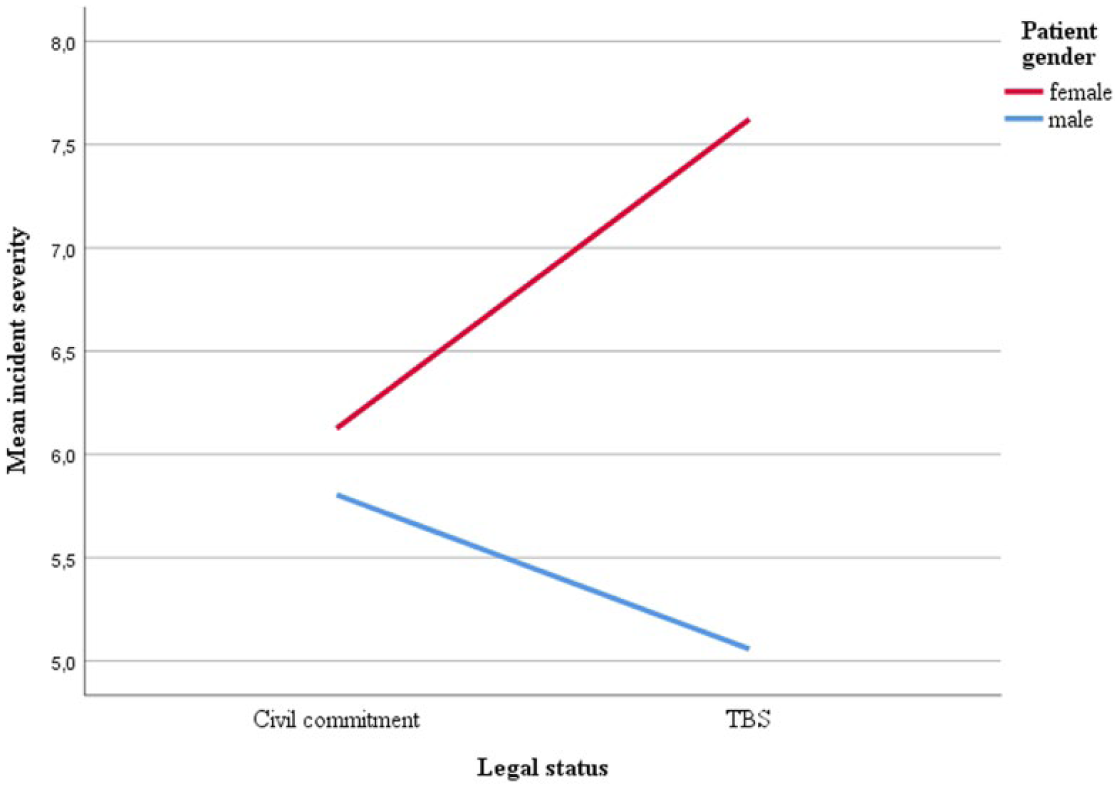
Interaction effect between legal status and patient gender on incident severity.
When the analyses excluded autoaggression, similar results emerged. Patient gender remained a significant predictor, F(1, 219.40) = 4.47, p = .036, as well as the interaction term between patient gender and legal status, F(1, 253.57) = 6.58, p = .011. The interaction effect followed the same pattern as shown in Figure 1, where female forensic patients caused the most severe incidents and male forensic patients the least severe. Adding patient age to the model significantly improved the model fit, χ2(1) = 42.96, p < .01. There was significant variance in intercepts across patients regarding the relationship between age and incident severity, Var(u0j) = 2.31, χ2(1) = 289.27, p < .01. Younger patients caused more severe incidents than older patients, F(1, 314.85) = 15.25, p < .001. Adding patient age did not change the relationship between legal status and incident severity, F(1, 316.73) = 0.43, p = .513.
Primary diagnosis
The relationship between primary diagnosis and incident severity showed significant variance in intercepts across patients, Var(u0j) = 2.37, χ2(1) = 292.01, p < .01. Patients with a primary diagnosis of a psychotic disorder caused less severe incidents than patients with other primary diagnoses, F(1, 228.48) = 6.34, p = .012. Primary diagnosis remained a significant predictor when added to the model, including patient gender, legal status, and the interaction between gender and legal status, F(1, 252.69) = 4.36, p = .038. Adding the patient’s primary diagnosis as a predictor significantly improved this model, χ2(1) = 30.36, p < .01. There was no interaction between the patient’s primary diagnosis and legal status, F(1, 294.86) = 1.08, p = .299.
Discussion
This study compared the frequency and severity of aggressive incidents caused by forensic and civil psychiatric patients in a 4-year time period in a Dutch forensic psychiatric hospital. As expected in Hypothesis 1a, civil psychiatric patients were found to cause more incidents than forensic patients. The civil psychiatric patients admitted to the forensic hospital often have acute psychiatric problems (Van Rooijen & Neijmeijer, 2014). In general psychiatry, inpatient aggression is also found to occur more frequently in acute wards compared with non-acute wards (Bowers et al., 2011). In contrast, forensic patients may have already been stabilized to a certain degree before arriving to the forensic hospital, as most forensic patients serve a prison sentence before the start of their treatment order. Furthermore, the aggressive civil psychiatric patients in the sample were found to be on average younger than the aggressive forensic patients, which might also influence their involvement in aggression. A meta-analysis including 26 studies that compared the age of aggressive and non-aggressive patients found that inpatient aggression is associated with younger age, but also noted that half of the included studies did not find a significant effect of age (Dack et al., 2013).
Female patients were found to cause more incidents than male patients, thus confirming Hypothesis 1b. Previous research has yielded mixed results, with some studies finding no gender differences in inpatient aggression (Daffern et al., 2005; Nicholls et al., 2009) and others finding that female inpatients are more aggressive than their male counterparts (Broderick et al., 2015). Differences between forensic and civil psychiatric patients regarding the severity of incidents were also moderated by patient gender. Female forensic patients caused the most severe incidents, followed by female civil psychiatric patients. Male forensic patients caused the least severe incidents. These findings reject Hypotheses 2a and 2b, which stated the expectation that incident severity would not differ between patients of a different gender or legal status. The differences in both frequency and severity of aggression between male and female patients are not explained by a higher involvement of female patients in autoaggression. One explanation for the finding that female patients caused more incidents and especially female forensic patients caused severe incidents may be that the judicial system tends to be more lenient toward female offenders than to male offenders (Spohn & Beichner, 2000). The female offenders who do get a TBS-order appear to suffer from relatively more complex psychopathology than their male counterparts (De Vogel, Stam, Bouman, Ter Horst, & Lancel, 2016). It may also be that forensic treatment is catered more toward the needs of male patients, which may disadvantage female forensic patients in their treatment (Van Voorhis, Wright, Salisbury, & Bauman, 2010). More research is necessary to understand these differences between male and female patients and between forensic and civil psychiatric patients.
This study found no significant interaction between patient gender and legal status regarding the frequency of inpatient aggression, which rejects Hypothesis 1d, whereas this was found in the meta-analysis by Dack and colleagues (2013). The current data do show a trend similar to the pattern of differences found in severity of incidents, where male forensic patients appear to cause the least number of incidents of all groups of patients. However, the number of incidents varied greatly between individuals and the groups differed in size, with 246 male forensic patients compared with only 39 female civil psychiatric patients.
Finally, patients with a primary diagnosis of a psychotic disorder were not found to cause more aggressive incidents than patients with a different primary diagnosis, which rejects Hypothesis 1c. Hypothesis 2c stated the expectation that patients with a primary diagnosis of a psychotic disorder would cause more severe incidents than patients with a different primary diagnosis. However, patients with a psychotic disorder were found to cause less severe incidents compared with patients with a different primary diagnosis, whereas previous studies found that patients with schizophrenia caused more severe aggressive incidents (Abderhalden et al., 2007; Grassi et al., 2001). More research is needed to find out in what way the incident severity differs between patients with different primary diagnoses.
Limitations
While the current study has some interesting findings, there are also several limitations. All data were retrieved in retrospect from the patient files, which means that the quality of the information is dependent on how well the staff member reported it. Only incidents mentioned in the daily reports were included in this study, which is likely to be an underestimation of the actual aggression rate, as aggression may go unnoticed or unreported. This method of data collection also precluded the possibility of getting each patient’s perspective on the incidents.
Another serious limitation is the severity scoring based on the MOAS. Even though the MOAS is validated in several studies (e.g., Margari et al., 2005), this measure faces a number of shortcomings. Some aggressive behaviors are not mentioned in the instrument and are difficult to weigh according to the current descriptions, such as threatening someone with a weapon. This may result in an underestimation of the severity scores for incidents where weapon use does not result in injuries, as the two most severe categories of physical aggression require the aggressor to cause injuries to the victim. This requirement confounds the severity of the aggression with its outcomes, without taking the intention of the aggressor into account (Bowers, 1999). This means that an incident where a patient throws down an object which accidentally hits and injures someone would be rated as more severe than an incident where a patient intends to kill a ward full of people by shooting a gun at them, but by chance fails to wound anyone. Finally, the comparability of different types of aggression can be called into question. The severity scoring is based on a multiplication of the category of aggression and the level of severity, which means that the same score can be achieved with multiple types of aggression. It is questionable whether repeated and detailed death threats about someone’s children can be considered equally severe as a patient kicking the furniture once, even though both result in a severity score of 4. However, there is no reason to assume the shortcomings of the instrument would affect the scores of aggressive incidents among forensic patients differently compared with civil psychiatric patients, as there appear to be no systematic differences between these groups which would make one of the groups more prone to underestimation of severity.
Finally, it should be noted that this study includes a specific patient population. The civil psychiatric patients in this study have been placed in a forensic hospital because they have already displayed disruptive or aggressive behavior and are therefore considered to be unmanageable in regular psychiatric care. Therefore, these patients cannot be readily compared with civil psychiatric patients in other settings. Similarly, the forensic patients in this study include offenders who are considered to have a high recidivism risk and were deemed to need treatment in a high-security forensic hospital. Thus, both the forensic and civil psychiatric patients in this study have displayed (severe) aggressive or transgressive behavior before their arrival at the hospital, which makes the comparison of their aggression in the forensic hospital interesting, but limits generalization to psychiatric patients in other settings.
Future Research Directions
The current study raises several questions that could be addressed in future research. As the retrospective nature of the present study posed limitations, future research should aim to employ prospective methods of data collection. Future research should expand the topic of severity of inpatient aggression by employing qualitative methods to gain more in-depth insight into the severity of aggression. This would also offer the possibility of including the patient’s perspective. Aggression is likely to have impact on patients too, but this topic has attracted very little research attention.
More research is also needed to improve the available aggression registration instruments. As described above, the MOAS has some serious limitations. However, this is also the case for other instruments such as the OAS and SOAS-R. The severity scoring of the OAS and SOAS-R includes the interventions used to address the aggression, where higher severity scores are given to incidents where restrictive interventions are used. This confounds the incident with its consequences. Furthermore, the SOAS-R gives higher severity ratings to aggression targeted at staff members than to aggression targeted at patients, which seems ethically questionable. New instruments or revisions of the currently used instruments are necessary to address these concerns and to take the intent of the aggressor into account, rather than focusing on outcomes (Bowers, 1999). Bowers, Nijman, Palmstierna, and Crowhurst (2002) developed a new scale for this purpose, called attempted and actual assault scale (attacks), but research on this instrument is very limited.
Clinical Implications
The present study found that female patients and civil psychiatric patients committed more aggression than male and forensic patients, and female forensic patients caused the most severe aggressive incidents. This has important clinical implications. Previous research found that staff members have more positive feelings, such as sympathy and receptiveness, toward the female forensic patients and more negative feelings, such as anxiousness and feeling threatened, toward male forensic patients (De Vogel & Louppen, 2016). It might be helpful for staff members to learn that female patients rather than male patients cause most incidents and female forensic patients cause the most severe aggression. Underestimating the aggression potential of female patients might contribute to higher rates of aggression, for example, when early warning signals are not interpreted correctly. These differences between male and female patients emphasize the need for gender-responsive risk assessment and treatment strategies (De Vogel et al., 2016). Furthermore, the finding that the group of civil psychiatric patients cause more aggressive incidents than forensic patients validates the need for a specialized intensive treatment program in a forensic hospital for a group of civil psychiatric patients with severe aggression problems. This difficult population of civilly committed patients deserves more attention among researchers, health care managers, and policy makers, which is needed to implement successful aggression prevention strategies. Furthermore, staff members deserve acknowledgment of the difficulties of working with these aggressive patients. Health care managers should be cognizant of the impact of aggression on staff members to reduce absenteeism and to retain them as employees.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.