
Abstract
Domestic violence has severe consequences for women, both psychologically and physiologically. Violence during pregnancy is even riskier, endangering women’s lives and the lives of their fetuses. A nationwide survey in Turkey in 2014 revealed that 7% of women who have experienced a pregnancy were exposed to physical violence perpetrated by an intimate partner during pregnancy. In this study, the risk and protective factors for this particular type of violence and how it can be addressed in Turkey are discussed using nationally representative data for the first time. Data are obtained from surveys conducted in 2008 and 2014 on domestic violence against women. The analysis is based on multinomial regression models in which the dependent variable consists of three groups of women: those who have not been exposed to intimate partner violence (IPV), those whose have been exposed to physical IPV but not during pregnancy, and those who have been exposed to physical IPV during pregnancy. In this way, the factors that have a significant effect on this severe form of violence can be identified. Our findings show that earlier age of first intercourse; the nature of first intercourse; men’s affairs; men’s controlling behaviors over women; men’s use of alcohol, drugs, or gambling; and experience with violence in the family are all significant factors for IPV during pregnancy. Women’s empowerment and the restructuring of the unequal power relations between women and men should be targeted to eradicate the problem in the long run. It is concluded that, for the time being, it is crucial to ensure that legal procedures for domestic violence function well and that health institutions are key components in identifying pregnant women exposed to violence and in guiding them toward institutional and social support mechanisms.
Keywords
Introduction
Violence against women (VAW) is a violation of human rights, an act of gender discrimination, and an important public health problem (García-Moreno & Stöckl, 2009; Stöckl, Watts, & Mbwambo, 2010). VAW studies indicate that most of the perpetrators are intimate partners (IP), and intimate partner violence (IPV) during pregnancy is one of the common types of IPV. International surveys 1 such as the Multi-country Study on Women’s Health Survey (World Health Organization [WHO] study), Demographic Health Surveys (DHS), the International Violence against Women Surveys (IVAWS) and Violence Against Women: An EU-wide Survey (known as the FRA survey) have produced comparable estimates on IPV during pregnancy. The estimates of IPV during pregnancy ranged from 1% to 28% according to the WHO study, from 2% to 14% in the DHS, and from 2% to 7% in the IVAWS (Devries et al., 2010; García-Moreno, Heise, Jansen, Ellsberg, & Watts, 2005).
The literature on IPV during pregnancy and its health consequences underlines that the negative consequences of IPV are not limited to women but also extend to fetuses and newborns. IPV may increase the risk of fetal death from trauma, elective pregnancy termination, preterm delivery, fetal distress, low birth weight (Mohammad-Alizadeh-Charandabi, Bahrami-Vazir, Kamalifard, & Mirghafourvand, 2016), miscarriages, placental abruption leading to birth asphyxia and death, insufficient weight gain during pregnancy, premature labor or delivery (Mohammad-Alizadeh-Charandabi et al., 2016), or stillbirths or fatal fractures (Arslantaş et al., 2012; Campbell, 2002; Devries et al., 2010; Mohammad-Alizadeh et al., 2016; Moraes, Amorim, & Reichenheim, 2006; Murphy, Schei, Myhr, & Du Mont, 2001; Rodrigues, Rocha, & Barros, 2008; Taft & Watson, 2007; Valladares, Ellsberg, Peña, Högberg, & Persson, 2002). Women’s physical and psychological health (García-Moreno et al., 2005) in the short- and long-terms is affected by IPV in various ways. Women can delay seeking antenatal care (Curry, 1998; Mohammad-Alizadeh-Charandabi et al., 2016), can be subjected to injuries (Devries et al., 2010; El Kady, Gilbert, Xing, & Smith, 2005), may develop substance abuse (Curry, 1998; Mohammad-Alizadeh-Charandabi et al., 2016), and may suffer from vaginal bleeding and anemia Mohammad-Alizadeh-Charandabi et al., 2016). They may experience higher levels of depression during and after pregnancy (Martin et al., 2006; Mohammad-Alizadeh et al., 2016), reduced levels of breastfeeding (Devries et al., 2010; Lau & Chan, 2007), and increased suicide attempts (Campbell, 2002), even after the end of abuse.
The introduction of the ecological framework for IPV studies by Heise (1998) paved the way for frequent use of the framework with the risk and protective factors of IPV. The ecological framework helps to understand interpersonal violence by considering personal, situational, and sociocultural factors and is used in studies of child abuse, youth violence, IPV, and elder abuse. For example, four levels were defined in the WHO multi-country study: individual-, relationship-, community-, and society-level factors (García-Moreno et al., 2005). Similarly, Stöckl and others (2010), in their study of IPV during pregnancy in Tanzania, defined individual factors, relationship factors, and sexual and reproductive health factors in their framework.
Many studies in the literature explore the determinants of IPV during pregnancy using various data sources. These studies have identified exposure to violence in childhood and to witnessing violence at home during childhood (Arslantaş et al., 2012; Clark, Hill, Jabbar, & Silverman, 2009; Devries et al., 2010; Stöckl et al., 2010); some spousal habits, such as alcohol use, drug use, and smoking (Clark et al., 2009; Idoko, Ogbe, Jallow, & Ocheke, 2015; Moraes et al., 2011; Shamu, Abrahams, Zarowsky, Shefer, & Temmerman, 2013); and extramarital affairs (Shamu et al., 2013) to be significant risk factors for IPV during pregnancy. Age, educational level, and working conditions of women and men as well as socioeconomic conditions were also significant individual factors reflecting the characteristics of women and their partners (Ansari et al., 2017; Arslantaş et al., 2012; Idoko et al., 2015; Şahin & Şahin, 2003; Stöckl et al., 2010; Taşpınar, Bolsoy, & Şirin, 2005). The following factors representing the relationship between couples were significant: man forcing the woman for the first sexual intercourse (Shamu et al., 2013; Stöckl et al., 2010), marriage-related variables such as age at first marriage (Bolu, Mayda, & Yılmaz, 2015; Yanikkerem, Karadaş, Adıgüzel, & Sevil, 2006), marriage decision (Arslantaş et al., 2012; Bolu et al., 2015), and bride price (Shamu et al., 2013; Stöckl et al., 2010).
In Turkey, most studies on IPV during pregnancy have been based on the clinical or hospital/local health centers’ data, providing a variety of related indicators of IPV. Karaoglu and others (2006) interviewed 824 pregnant women and estimated the prevalence of physical violence as 8.1%, emotional violence as 26.7%, and sexual violence as 9.7% in Malatya province. The results of their study showed that the husband’s smoking behavior, low level of education, low family income, and being in the second trimester of pregnancy led to an increased risk of exposure to violence during pregnancy (Karaoglu et al., 2006). Deveci, Acik, Gulbayrak, Tokdemir, and Ayar (2007) estimated the prevalence of physical violence as 28.9% for their sample of 249 pregnant women in Elazig province. This study identified the husband’s alcohol consumption, number of children, and socioeconomic status as factors significantly associated with physical IPV during pregnancy. The study by Ergönen et al. (2009) in Izmir province showed that 4.7% of pregnant women were subjected to violence during pregnancy by partners and other close family members. Yilmazel, Baykan, and Cetinkaya (2016) conducted another hospital-based study in Corum province with 109 pregnant women who had applied to a government hospital. They estimated that 62.4% of the women were exposed to at least one form of violence (verbal, economic, physical, or sexual), while 29.4% of them experienced physical violence during pregnancy. They highlighted the number of children, husband’s low education level, presence of violence before pregnancy, and the spouse having a history of violence among the risk factors of violence during pregnancy. Topbaş, Ünsal, Çan, Bacak, and Özgün (2008) estimated the prevalence of physical or sexual violence during pregnancy as 1.6% on a survey of women who gave birth at a public hospital in Trabzon province in 2004. Age, education of either partner, employment, income, or parity were not found to be significantly associated with physical or sexual IPV in this study. Similarly, some studies, particularly local studies, have not found a significant association between age and physical IPV during pregnancy (Giray et al., 2005), age and physical/sexual/economic/psychological IPV during pregnancy (Yanikkerem et al., 2006) or educational level and physical IPV during pregnancy (Giray et al., 2005).
Health center–based studies provide valuable data on VAW during pregnancy and provide insight on its determinants; however, Gelles (as cited in Bergen & Logue, 2009) mentions certain limitations that may apply to the measurement of violence based on how questions are asked and small sample sizes. Thus, nationally representative studies with standardized tools are needed for both international and national comparisons of VAW during pregnancy. This need is also highlighted in studies from Turkey (Karaoglu et al., 2006; Yilmazel et al., 2016). Another benefit of using national-level household survey data obtained through face-to-face interviews is the ability to include women of different socioeconomic statuses and ethnicities. Participants are not limited to a certain locality, to women who can access health centers, to women who are literate, or to women who can speak Turkish.
The nationally representative domestic VAW surveys in Turkey indicated that the levels of IPV during pregnancy were 10% and 8%, and levels of physical IPV were 39% and 36%, respectively, for 2008 and 2014. In one quarter of the cases in 2008 and one third of the cases in 2014 in which violence took place during pregnancy, the violent acts targeted pregnancy directly, and women were punched or kicked in the abdomen by a partner (Directorate General of Women’s Status [DGSW] & Hacettepe University Institute of Population Studies [HUIPS], 2009, 2015).
The intent of this study is to contribute to the literature through assessing IPV during pregnancy using these aforementioned nationally representative domestic violence surveys in Turkey. More specifically, the aim is to assess the risk and protective factors of IPV during pregnancy by comparing these incidents with situations where IPV was present at other times but not during pregnancy. Two surveys are used to determine whether both scenarios would suggest similar risk and protective factors. The risk and protective factors of IPV in Turkey are determined according to the ecological framework, where IPV was assumed to be affected at three different levels: individual factors for women and their husbands, relationship factors including sexual and reproductive relations between the couples, and societal factors, as shown in Figure 1. The abbreviation “IPV” refers to physical intimate partner violence in the rest of the article whenever the word “physical” is omitted.
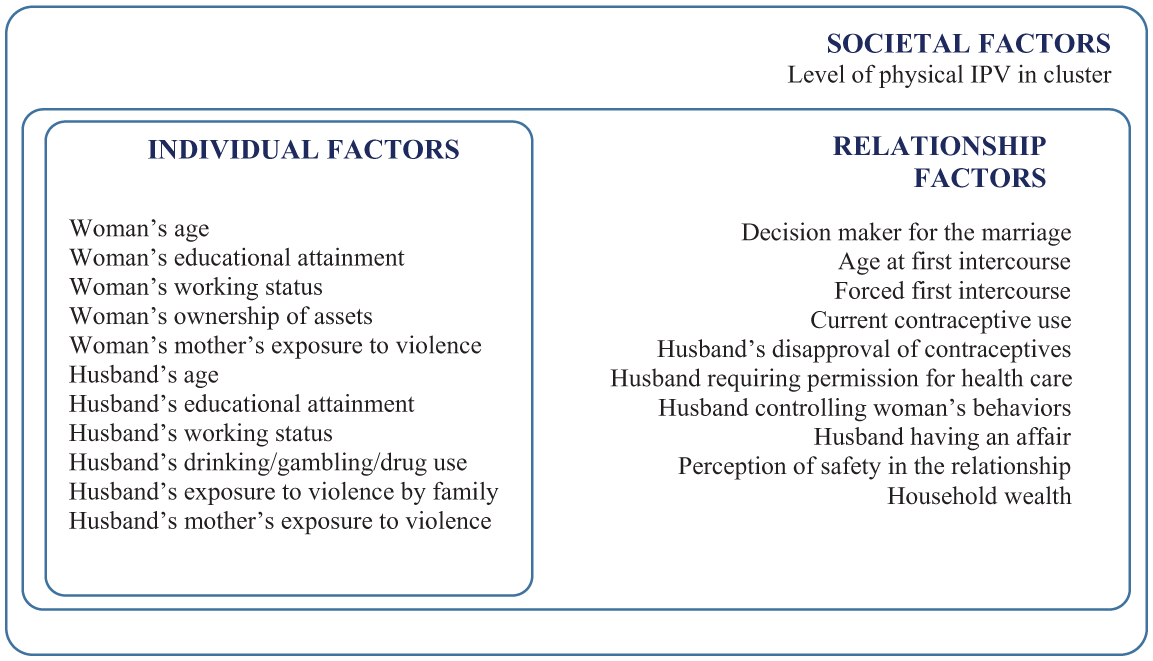
Framework for physical intimate partner violence during pregnancy.
Data and Method
Survey Design and Fieldwork
This study is based on the aforementioned nationally representative population-based surveys. 2 The first survey, titled “National Research on Domestic Violence Against Women in Turkey,” was conducted in 2008, and the second was implemented in 2014 as another independent cross-sectional survey. As is the case with most large-scale household surveys, the sample designs deviated from a simple random sample approach, thus leading to complex sample designs with multistage selection, stratification, and clustering. Clusters were composed of household addresses that were almost always within the same small administrative unit, often indicating the same neighborhood. Sample weights based on selection probabilities and nonresponses were calculated at the data-processing stage. In 2008 and 2014, 12,795 and 7,462 women aged 15 to 59 were interviewed, respectively, with response rates above 80% in each group.
The questionnaires used in the surveys were based on the WHO’s “Multi-country Study on Women’s Health and Domestic Violence Against Women.” These questionnaires were developed after “a long process of discussion and consultation” by international experts and pretested in numerous countries, and they allow for international comparisons of different types of VAW (García-Moreno et al., 2005). A household and a woman’s questionnaire were used. In the former, eligible women were enlisted, and one was randomly selected.
The Ethical and Safety Guidelines (WHO, 2001) prepared and suggested by the WHO were followed, and only one respondent was selected per household through the Kish table in the household questionnaire (DGSW & HUIPS, 2009, 2015). Further measures were taken in line with the WHO Guidelines, such as the use of a safe name for the survey. Both surveys were conducted under the safe name of “Turkish Women and Family Survey” in the field. Interviewers signed a consent form for each interview stating that they had informed the respondent about the nature of the study and had received their approval for the interview. Privacy was emphasized during training, and interviewers ensured that they were alone with the respondents during the interviews. Contact information of public and private institutions that provide services in cases of domestic violence was provided to the interviewers to hand out to respondents if required. The fieldwork was carried out by teams of interviewers with field editors and supervisors who received theoretical and practical training for 2 weeks that covered topics on gender and VAW and communication skills in addition to the questionnaire training.
Data and Unit of Analysis
The analysis in this study is restricted to women aged 15 to 49, as is often employed in the literature, who have had at least one pregnancy (Figure 2). The sample was also restricted to women who had been married only once because the questionnaires do not include information to determine which partner has been the perpetuator of IPV during pregnancy in the case of multiple marriages, and use of partner-level variables would not be possible if women with more than one marriage were included. In total, 8,311 women in 2008 and 4,619 women in 2014 were eligible for the study. Data sets for both studies are available via request from the Turkish Statistical Institute.
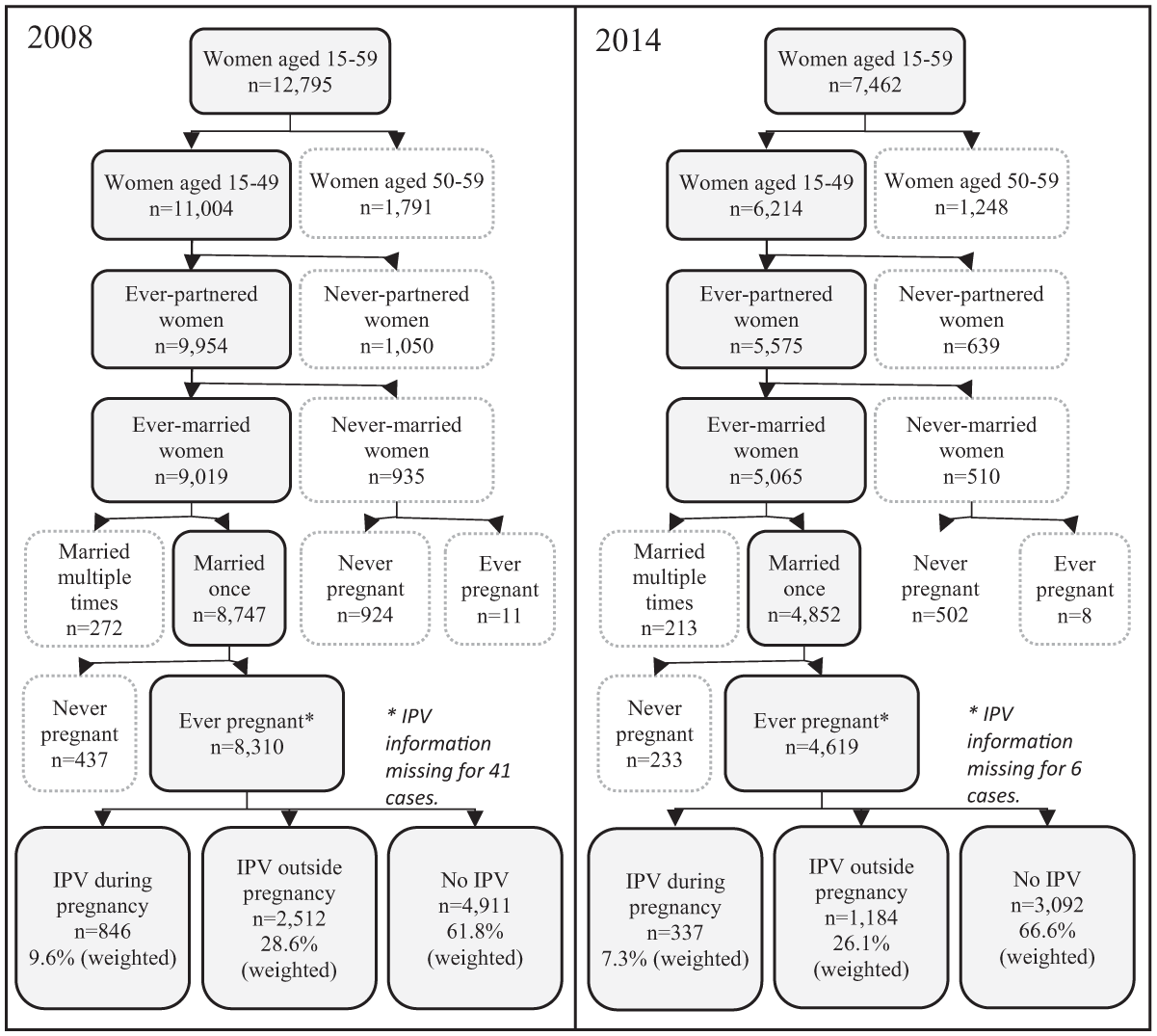
Number of cases associated with the outcome variable (2008, 2014 Turkey).
Outcome Variable
The definitions used in the outcome variable are based on the standard WHO measures. Physical violence was measured through a set of questions asked to women who have reported having at least one partner/husband in their lifetime. These questions were about ever having experienced the following acts: being (a) slapped or the target of something thrown that could hurt; (b) shoved or assaulted or having hair pulled; (c) hit with a fist or with something else that could hurt; (d) kicked, dragged, or beaten; (e) choked or having a part of the body burned; and (f) threatened with a weapon such as a knife or a gun. Women who answered “yes” to any of the above items were defined as having experienced lifetime physical violence. Moreover, women who had experienced at least one pregnancy were asked the following question: Did (any of) your husband(s)/partner(s) slap, hit, or beat you or cause you any physical damage while you were pregnant?
Accordingly, women who experienced IPV and women who experienced IPV during pregnancy are not mutually exclusive groups, because some women may experience both types of IPV. The outcome variable was based on three mutually exclusive categories, all of which were lifetime measures: (a) exposure to IPV during pregnancy (regardless of answers to the physical violence question), (b) exposure to IPV outside pregnancy (excluding women who experienced IPV during pregnancy), and (c) no exposure to IPV at all.
Exposure Variables
The independent variables used in this study are listed in the framework shown in Figure 1 and were selected according to the literature, data availability, and presence in both surveys used for analysis. 3 Since only women were interviewed in both surveys, information about their husbands was also collected through the women’s questionnaire. Characteristics of women and their husbands were included in the individual-level factors based on the ecological framework. Women’s individual factors include age, educational level, working status, ownership of assets (defined by ownership of land, house, business, money in bank account or other) as well as witnessing mother’s exposure to violence during childhood. Similarly, the variables for husbands are age, educational level, working status, childhood experience of physical violence, witnessing mothers’ exposure to violence, as well as current use of alcohol, drug, and gambling. Husband’s mother’s exposure to violence as given in women’s reports was used as an independent variable by Shamu et al. (2013) and was significant despite a high proportion of the unknown category. Thus the variable was added to the model despite the limitations of proxy reporting.
Relationship-level factors were defined as variables concerning both partners. These included decision maker for marriage, current contraceptive use, whether the husband disapproves of contraceptive use, whether the husband requires the woman to get his permission to go to a health facility, and some other controlling behaviors 4 by the husband. In Turkey, premarital sex is socially unacceptable and is assumed to be uncommon. Therefore, this study assumed that the variables in the data set of woman’s age at first intercourse and whether she was forced into her first intercourse 5 were experiences with the husband. Women were also asked whether they were afraid of their husbands, and this answer was taken as an indicator of perception of safety in the relationship. The husband having an extramarital affair was based on the respondent’s evaluation and included a “not sure” category. As a proxy of socioeconomic status, the household wealth index was used, which was calculated according to ownership of selected household goods based on which quintiles were formed and then regrouped into three levels for simplicity. The level of physical violence in the cluster was employed as the community variable, as previously used by Ansari et al. (2017), denoting whether the level was higher or lower than the national average. Other residential variables were omitted to avoid multicollinearity with the cluster-level variable.
Statistical Analysis
Multinomial logistic regression was used to explain the relationship between the physical violence variable at three levels and the factors specified in the theoretical framework. The factors were entered as blocks in accordance with the framework. The complex sample designs of the samples were considered using the svy (survey) commands of Stata 12 and the Complex Samples Module of SPSS 18, where stratum, cluster, and sample weight variables were specified. A descriptive analysis of the outcome variable (exposure to IPV during pregnancy, IPV outside pregnancy, and no exposure to IPV) was conducted with major types of violence to ensure that the three-level outcome variable for IPV during pregnancy represents different experiences of violence for women. Bivariate analysis of all variables used for regression models was carried out using SPSS Complex Samples Crosstabs, where cases selected for regression were specified as a subpopulation for correct statistical inference. Stata neither produces R2 values nor performs block regression for the svy: mlogit command; thus, all pseudo R2 values were obtained through the regular mlogit command, whereas final regression parameters and their significance were obtained through the svy: mlogit command. Multicollinearity was assessed through variance inflation factors prior to producing final models, using the reg procedure in Stata. Women’s personal income was omitted in the final models due to multicollinearity with household wealth and women’s working status.
Results
Characteristics of Respondents
The characteristics of women who were interviewed in the two surveys are presented in Table 1. The respondents had a mean age of 34 in 2008 and of 35 in 2014. Most of them were married at the time of the survey (96% in 2008 and 86% in 2014), with the proportion of divorced women increasing from one survey to the next (2% and 6%, respectively). Most women were primary school graduates (62% and 60%, respectively), and the proportion of women with more education increased over time (20% and 25%, respectively). The majority of women were not enrolled in the labor force (73% and 69%) in either survey; however, findings from 2014 showed slightly higher employment in the formal sector (Table 1).
Basic Characteristics of Respondents (2008, 2014, Turkey).
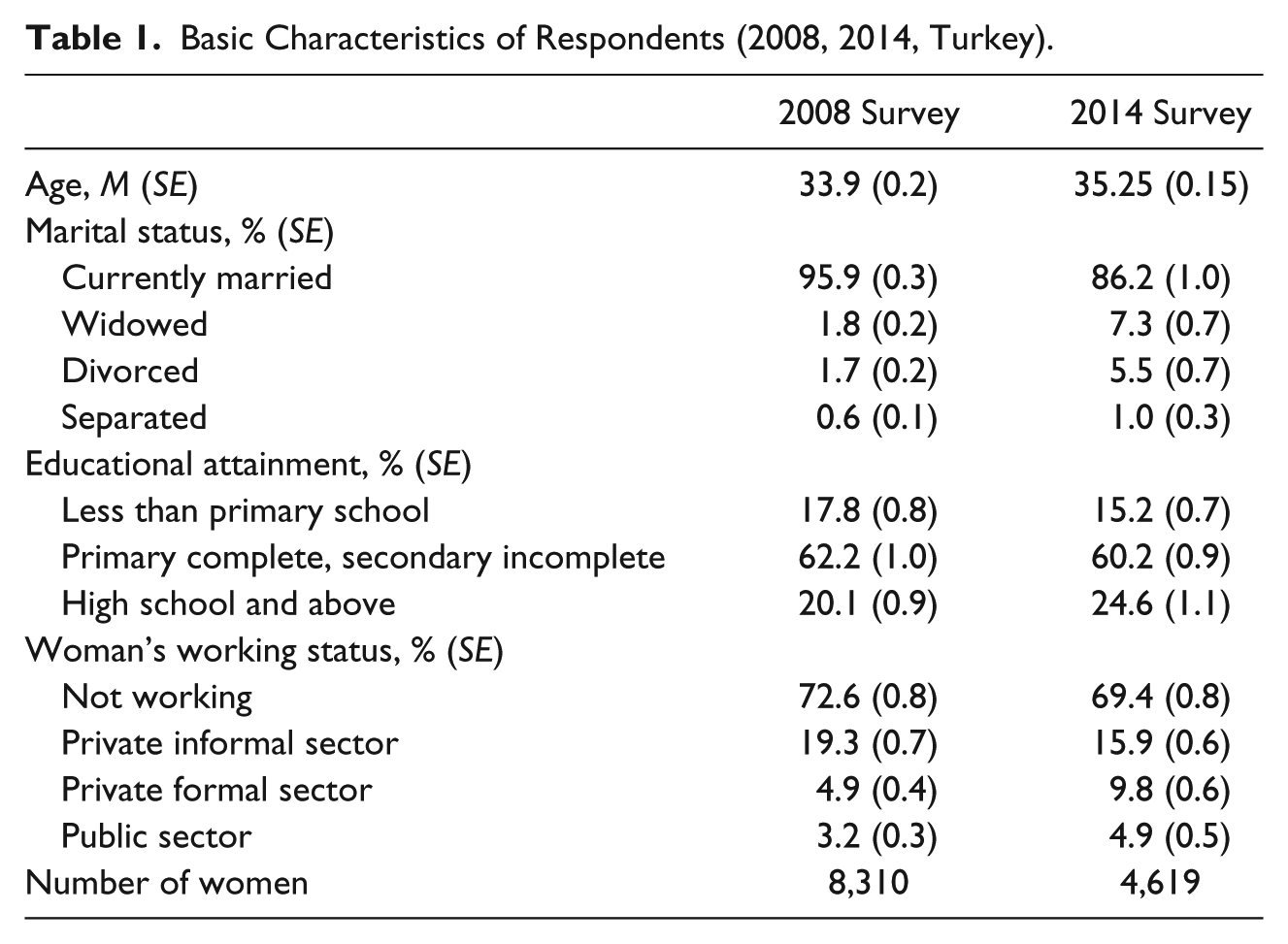
Figure 3 shows the levels of types of violence and suicide-related attitudes and behavior based on the outcome variable at three levels: for women who experienced IPV during pregnancy, women who experienced IPV but not during pregnancy, and women who did not experience IPV at all. The figure shows that IPV during pregnancy is a more intense form of physical violence and more often coexists with other types of violence compared with IPV outside pregnancy. The proportion of women exposed to sexual violence or emotional violence was highest for women who experienced IPV during pregnancy, lower for women who experienced IPV outside pregnancy, and lowest for those who did not experience IPV at all. The outcome variable did not show striking differences for controlling behaviors. This result could be because these behaviors are very common in general or because they may not serve as direct indicators of IPV such as emotional violence or sexual violence.
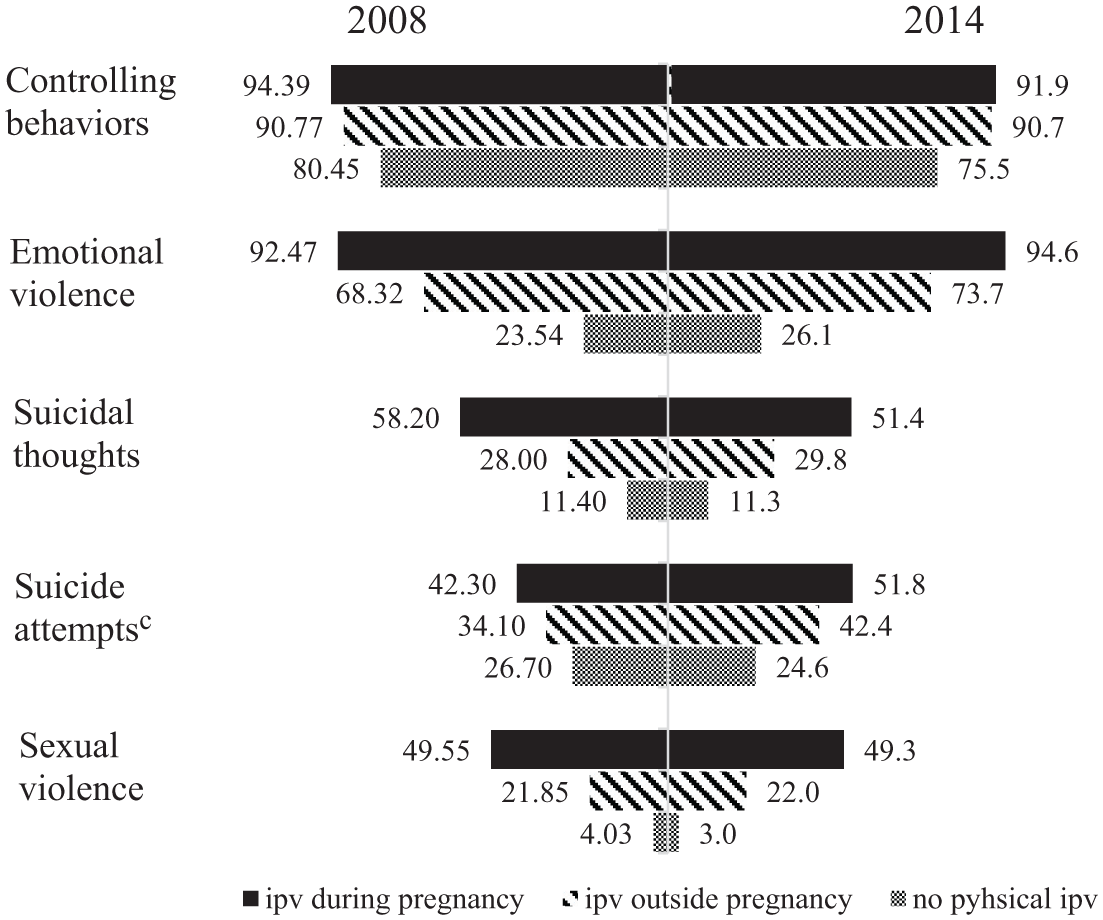
Levels of different types of violencea and adverse mental effectsb among ever-pregnant women, by their lifetime experience physical IPV during or outside pregnancy (2008, 2014 Turkey).
There is also evidence to suggest that different levels of the outcome variable—IPV during pregnancy, IPV outside pregnancy and no IPV—are associated with women’s emotional distress (Figure 3). Thoughts of suicide and suicide attempts are more prevalent among women who experienced IPV during pregnancy, less prevalent for those who experienced IPV but outside pregnancy, and even less prevalent for women who did not experience IPV at all.
Descriptive Findings
Table 2 shows the bivariate analysis of variables selected as potential risk and protective factors. Although IPV during pregnancy was taken as a lifetime measure, it did not change substantially due to women’s age. However, it was higher when the husband’s age at marriage was higher, often indicating a high age gap between spouses. Higher education for either the women or their husbands was associated with a lower prevalence of IPV during pregnancy. For either partner, IPV during pregnancy was observed most frequently in unemployment and employment in the informal sector. Women’s ownership of economic assets, such as a house or a car, seemed to be protective against IPV during pregnancy; however, this association was not significant in 2014. The husband’s use of alcohol or drugs or frequent gambling and his childhood exposure to physical violence were risk factors in each survey. Witnessing one’s mother’s exposure to physical violence by either partner was also a risk factor for IPV. Among relationship factors, IPV during pregnancy was higher in cases when the marriage decision was made by those other than the couple and when the woman had her first sexual intercourse before the age of 18 or against her will. Current contraceptive use was not significantly associated with the outcome variable in either survey. However, the husband interfering with woman’s control over her body, measured by requiring permission for health facility visits or preventing contraceptive use, was associated with the IPV status outcome variable. Moreover, when husbands displayed controlling behaviors or women stated they were afraid of their husbands, IPV during pregnancy was more prevalent. Cross tabulation by household wealth suggested IPV during pregnancy was more common in less wealthy households. The community-level variable showed that in neighborhoods where IPV was higher than average, so was IPV during pregnancy.
Bivariate Comparison of IPV During Pregnancy, Outside Pregnancy, and No IPV by Selected Risk and Protective Factors (2008, 2014 Turkey).
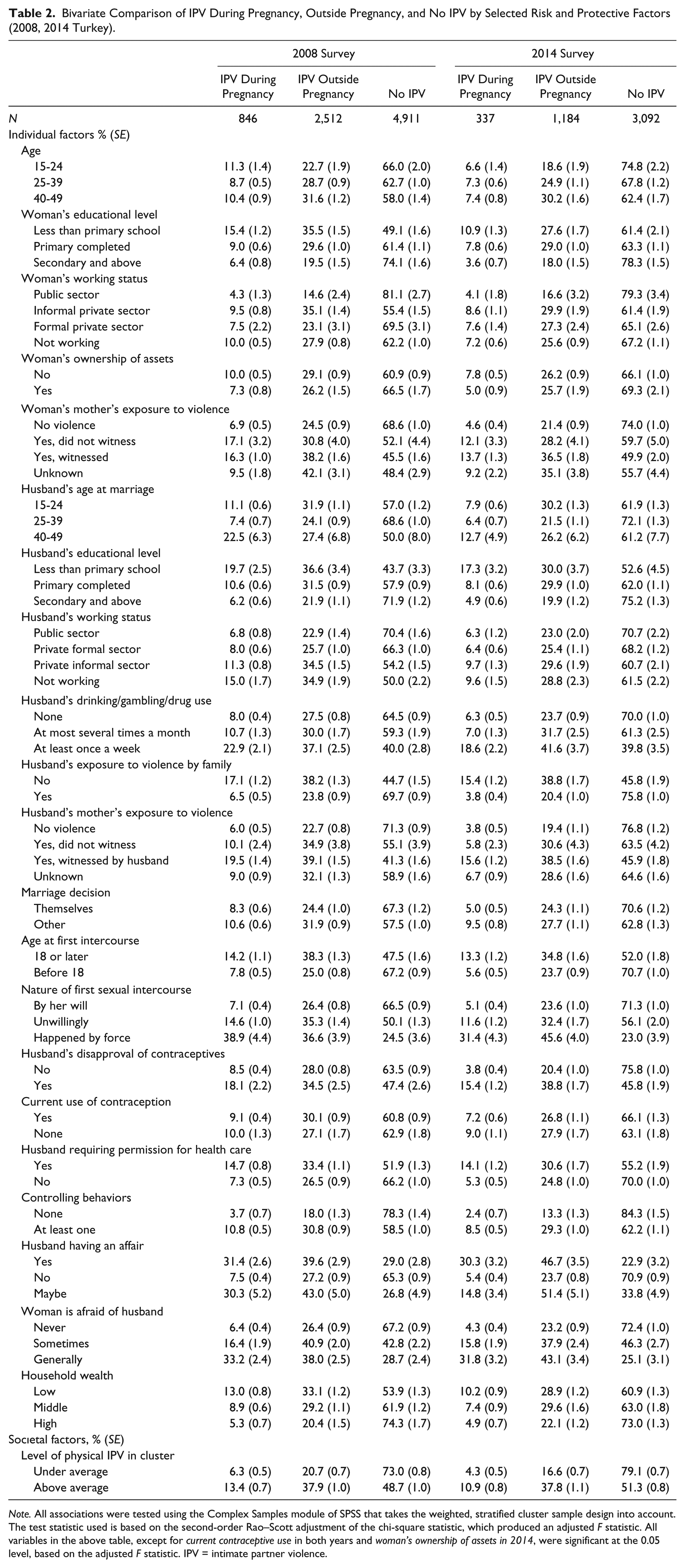
Note. All associations were tested using the Complex Samples module of SPSS that takes the weighted, stratified cluster sample design into account. The test statistic used is based on the second-order Rao–Scott adjustment of the chi-square statistic, which produced an adjusted F statistic. All variables in the above table, except for current contraceptive use in both years and woman’s ownership of assets in 2014, were significant at the 0.05 level, based on the adjusted F statistic. IPV = intimate partner violence.
Findings From the Multivariable Models
The outputs for the models are presented in Table 3 (variables that were not significant in either survey were omitted from the table). For each survey, the relative risk ratios (RRR) of IPV during pregnancy and IPV outside pregnancy are calculated against the reference group of no IPV. Model Pseudo R2 values were 0.11 and 0.12 for the 2008 and 2014 surveys, respectively; once individual-level variables were entered into the models as Block 1, these figures increased to 0.16 and 0.20 with the addition of relationship-level variables, and finally reached 0.18 and 0.23 after the inclusion of the societal-level variable. More than half the total variations explained by the models are due to individual-level variables. Among individual-level variables, sociodemographic variables were generally not significant in the models (woman’s age, husband’s age, woman’s education, husband’s education, woman’s working status) for IPV during pregnancy. However, some of these were significant for IPV outside pregnancy (woman’s age and woman’s working status). Women who were in the 45 to 49 age group had a greater RRR of reporting IPV outside pregnancy. Being employed in the informal private sector as opposed to the public sector also had a significantly higher RRR of IPV outside pregnancy in the 2008 survey.
Results of Multinomial Logistic Regression Models: Risk and Protective Factors of Physical IPV During and Outside Pregnancy With No Physical IPV as Reference Category (2008, 2014 Turkey).

Note. For the 2008 model, pseudo R2 value was .1102 for Step 1 after individual-level variables were added, .1599 at Step 2 after relationship-level variables were added, and .1771 after the societal-level variable was added. The corresponding Pseudo R2 values were .1245, .1984, and .2320 for the 2014 model. All mentioned models were significant at p < .001. All pseudo R2 values were produced using mlogit in Stata without the svy prefix. IPV = intimate partner violence; RRR = relative risk ratios; CI = confidence interval.
p < .05. **p < .01.
Witnessing one’s mother being exposed to violence was significant for both types of IPV and for both women and husbands, whereas mother’s exposure to violence was not significant if not witnessed. According to the 2014 model, the risk of IPV during pregnancy for women witnessing their mother’s exposure to violence was 1.63 times higher than the corresponding risk for women who reported that their mothers were not subjected to violence. This RRR was 2.56 for husband’s mother’s exposure to violence. Husbands’ own exposure to violence in their own families was significant in both models. In 2014, the risk of IPV during pregnancy was 2.77 times higher when the husband was exposed to violence in his childhood family, and the risk of IPV outside pregnancy was 1.90 times higher under this condition.
Men’s alcohol, gambling, or drug habits were also significant risk factors in both surveys. In the 2008 models, the risk of IPV during pregnancy was 2.66 times higher in the presence of one of these behaviors at least once a week, and the risk of IPV outside pregnancy was 1.93 times higher. The corresponding RRR values were 2.18 and 1.83, respectively, in the 2014 models.
Most relationship factors were significant in the multinomial models. Age at first intercourse for women and whether this first sexual intercourse happened by force or by will was significant in both years. If women were below 18 at the time, the risk of IPV was 1.63 times higher in the 2014 model. Women being forced for first sexual intercourse increased the risk of IPV during pregnancy by approximately 5 times in both surveys (5.16 in 2008 and 4.83 in 2014). Risks of IPV both during and outside pregnancy were significantly higher in each survey year when women reported that their husbands had had or were suspected to have had affairs. When women said their husbands had had affairs, the risk of IPV during pregnancy was 10.54 times higher in 2014.
Women who stated that they were afraid of their husbands showed a risk of IPV during pregnancy that was 6.05 times higher in 2008 and 4.60 times higher in 2014. Husbands’ controlling behaviors were significantly associated with risk of IPV in both surveys. The community-level variable comparing the cluster-level IPV with the national level was significant in both surveys.
A few findings differed slightly for the two data sets. Husbands requiring women to get their permission to seek health care showed higher RRRs of IPV during pregnancy in both survey years, but this variable was not statistically significant in 2008. Similarly, RRRs were above 1 when husbands prevented contraception, but this variable was only significant for IPV during pregnancy in 2008 and for IPV outside pregnancy in 2014. Higher risks of IPV were observed when household wealth was low, but this variable was significant in 2014 only.
Discussion
This work presented here is the first to study the risk factors of IPV during pregnancy in Turkey using nationally representative data. It is also the first study in Turkey attempting to compare how risk factors differ for women who experienced IPV during pregnancy against women who experienced it at other times. Sociodemographic factors significant in descriptive analysis, such as age and education for any partner and working status for women, were no longer significant once other variables were controlled for. Variables showing intergenerational transfer of violence, as denoted by mother’s exposure to violence for any partner and the husband himself being exposed to violence by his family as a child, were significant in a multivariable setting.
Multivariable analysis showed that the risk of IPV during pregnancy was significantly higher if husbands exhibited certain behaviors. These included alcohol/drug use or gambling, behaviors directed at controlling women, and certain behaviors that could be related to sexual and reproductive health: husbands having affairs outside marriage or behaviors disrupting women’s control over their own bodies (women having to get permission from husbands to go to health facilities and husbands being opposed to contraception). Furthermore, under the assumption that most women in Turkey have their first sexual intercourse within marriage, another husband behavior significantly associated with the risk of IPV during pregnancy was forcing women for this first experience.
Models showed that families avoiding their daughters’ early marriage could potentially be a protective factor against IPV for women. Women who had their first sexual intercourse at the age of 18 or above (as a proxy of marital age) were at lower risk of IPV during pregnancy. The societal-level variable being significant suggested that in neighborhoods where above-average physical IPV was observed, this phenomenon perhaps had higher social acceptance, putting women at greater risk for further IPV.
The two survey years did not show major differences in terms of findings, suggesting that no substantial changes have occurred from 2008 to 2014 and providing better confidence in pointing out risk and protective factors of IPV during pregnancy in Turkey. The use of multinomial models helped identify factors that differentiated the experience of IPV during pregnancy as a unique type of physical IPV. All risk factors of IPV during pregnancy were also significant for IPV outside pregnancy, but the opposite did not hold. Although the number of risk factors was higher for IPV outside pregnancy, the magnitude of the risk factors as determined by the RRRs was higher for IPV during pregnancy compared with IPV outside pregnancy (Table 3). This elevated risk phenomenon applied for all variables related to the husband’s behaviors.
The findings of this study showed that many risk factors were, in fact, related to husbands’ behaviors, and therefore, the elimination of the problem involves changing men’s attitudes. There are examples of interventions targeting men in the literature with various degrees of success (Flood, 2015). In the case of Turkey, it could be suggested that gender equality training be given to teenagers at school, and men’s compulsory military service in Turkey could include workshops on the issue. From a wider perspective, there is a need for collaboration among (Non-governmental organizations) NGOs, local administrations, and government agencies as well as individuals to achieve social change. Since VAW is rooted in gender inequality, it cannot be addressed without changing the norms and attitudes that legitimatize such violence.
Despite this necessity, obtaining change through change of the perpetrators, who already rank highest in the power hierarchy within the household, is very challenging and could take generations to achieve. For the time being, ensuring that legal regulations regarding domestic violence function well is crucial. Turkey was the first country to sign the Council of Europe Convention on Preventing and Combating Violence against Women and Domestic Violence (Istanbul Convention) and the first country to put it into action in 2011. In 2012, Law Number 6,284 on Protection of the Family and Prevention of Violence against Women was issued. Unfortunately, there are practical problems related to the implementation of the law and provision of services to women (DGSW & HUIPS, 2015), and thus, legislation to combat IPV did not significantly improve women’s lives.
Descriptive analysis revealed that women with higher education and participation in formal labor were exposed to lower levels of IPV. In a setting where controlling women’s sexuality, preventing women’s participation in the labor force and decision making at all levels, and violence are labeled as acceptable and normal, combating IPV is a challenge for women. The findings of the multinomial models confirm the importance of these social norms, showing that women’s characteristics are insignificant once relationship and society variables are controlled for. The 2014 survey showed that the higher the educational level of women was, the higher the help-seeking behavior for IPV (Ergöçmen, Türkyılmaz, & Özgören, 2015).
Women’s high education does not guarantee the absence of IPV, but it does improve their resistance strategies toward violence. In contrast, the lack of financial autonomy forces women to stay in abusive relationships. Empowerment of women could allow them to escape a relationship that signals physical violence through other forms of abuse, that is, in the presence of controlling behaviors, emotional, or sexual violence.
Reliable data are crucial for developing strategies to effectively combat IPV against women; however, surveys are still the main source of data. Improvement of registration systems, as suggested in the Istanbul Convention, hands responsibility for data collection to different ministries, including the Ministry of Health. This responsibility is important not only for providing statistics that show how many women were subjected to IPV during pregnancy but also for understanding the source of women’s problems and providing higher quality health services. It is important to identify women who are subjected to violence, both during pregnancy and other medical treatments. Health professionals are naturally among the first points of contact for women who have experienced violence. Defining VAW as a health problem, in addition to defining it as a human rights violation and a form of discrimination, gives health care personnel the responsibility for protecting women who are exposed to violence and better ensures the prosecution of perpetrators (United Nations Population Fund & WAVE Network and European Info Center Against Violence, 2014).
This study also had some limitations. One was the cross-sectional nature of the data; questions on IPV during pregnancy were lifetime measures that could not be attributed to a specific pregnancy/pregnancies. This characteristic left the timing of exposure unknown, and whether the exposure to IPV during pregnancy was the first-ever exposure to physical violence by partner could not be determined from the data. Furthermore, there were no questions on sexual violence during pregnancy, and therefore, another major type of IPV during pregnancy was omitted. Finally, as is the case in all surveys studying sensitive issues through face-to-face surveys, there may have been respondents who chose not to report their experiences of IPV to interviewers. For further studies, a qualitative approach is needed to understand women’s experiences during this period, as well as qualitative research on men to shed light on their perceptions and opinions as the primary perpetrators.
Conclusion
All previous studies on IPV during pregnancy in Turkey were based on local data. Therefore, this study made an important contribution to the literature providing information about IPV during pregnancy with the use of nationally representative data, which allows for generalization of the results. The results of this study highlight the importance of husbands’ behaviors, especially those related to sexual and reproductive health, as important risk factors for IPV during pregnancy. Thus, these findings highlight the role of health professionals in the detection of IPV during pregnancy and show that IPV can be combated through raising awareness of sexual and reproductive rights within health care services. Programs that aim to eliminate all forms of VAW should consider these findings for empowering women and include gender equality training not only for perpetrators but also for all men.
Footnotes
Acknowledgements
We thank the anonymous reviewers for their thorough reviews and Meltem Duran for proofreading the earlier version of our manuscript.
Authors’ Note
Research and field work were conducted by the Hacettepe University Institute of Population Studies. This study is dedicated to the memory of Hande Fulya Tunçkanat who had special interest in studying this topic.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study used the data from two nationally representative surveys: the first survey was financially supported by the European Commission, and the second was supported by the Turkish Republic Ministry of Family and Social Affairs.