
Abstract
While primary care physicians (PCPs) have opportunities to recognize patients who encounter domestic violence (DV) by intimate partners, warning symptoms such as unexplained physical injury, bruising, anxiety, and depression are often missed during clinic visits. This study investigated the barriers of Hong Kong PCPs toward managing DV, including recognition, management, and referrals of these patients. Four focus group interviews were conducted to explore the in-depth opinions of PCPs on managing DV in Hong Kong. The themes identified were investigated in a questionnaire survey with data from 504 PCPs working in public and private sectors. Factor analysis of the survey data suggested four major barrier factors: (a) worries about the potential harms of intervening in patients’ domestic affairs and DV issues, (b) lack of guidelines and support services, (c) limited skills and time in managing DV, and (d) patients’ reluctance in disclosing DV issues. PCPs with more years of practice had more worries about intervening in domestic issues (Factor 1), while the younger PCPs tended to perceive limited skills and time in managing DV cases as barriers (Factor 3). PCPs working in the public setting were more likely to ask patients about DV (M = 5.4 vs. 2.9), suspected DV (M = 3.8 vs. 2.3), and managed DV (M = 1.7 vs. 1.0) in the past 5 years compared with the private PCPs. Some PCPs in the focus groups expressed the view that DV cases should be handled by social workers instead of doctors. Survey respondents who held such views about doctors’ limited role in DV management also scored higher in all of the barrier factors. The findings suggest that there are boundaries between domestic and medical realms, especially in a Chinese context. Resolving PCPs’ worries by training, provision of DV management guidelines, and referral pathway to social workers may be good starting points to bridge the gaps.
Introduction
Domestic violence (DV), understood here as intimate partner violence, includes any behavior within an intimate relationship that causes physical, emotional, and sexual harm to the adult partner (Ramsay et al., 2012; The Royal Australian College of General Practitioners, 2014). While the phenomenon of DV is common worldwide, the vast majority of victims are women (Lee, 2002; Piterman, Komesaroff, Piterman, & Jones, 2015; Tiwari et al., 2014). Studies in Hong Kong showed that the prevalence of DV against women ranged from 10.4% to 15.7% (Leung, Leung, Lam, & Ho, 1999; Ma & Pun, 2016). Apart from physical injuries, international studies revealed that there was also a high prevalence of mental health problems experienced by women victims of DV, including posttraumatic stress disorder (63.8%), depression (47.6%), suicidal behavior (17.9%), alcohol abuse (18.5%), and drug abuse (8.9%) (Lee, 2002).
As most women are reluctant to actively disclose experiences of being abused due to fears and concerns about the consequences of disclosure (Ma & Pun, 2016), universal or targeted screening for DV among female patients has been promoted in some countries such as the United States and Israel (Daoud et al., 2019). Patients might be screened (with the use of a questionnaire) or asked by doctors and/or nurses for DV issues (O’Doherty et al., 2015). Nonetheless, the conventional approach of case-finding is common in many other countries where patients are asked only if they present with symptoms or signs suggestive of DV (Daoud et al., 2019). Theoretically, primary care physicians (PCPs) have opportunities to recognize patients who encounter DV (Miller & Jaye, 2007), because patients may present with unexplained physical injury, bruising, chronic fatigue, anxiety, depression, insomnia, or undifferentiated somatic symptoms that are associated with DV (Hegarty, Gunn, Chondros, & Small, 2004; Piterman et al., 2015). However, these warning signs and symptoms are often missed during clinic visits. Even if doctors suspect and recognize them, they may not initiate follow-up actions. As reported by a qualitative study in New Zealand, the barriers included complexity and stress for doctors to deal with DV, lack of time, confidence, or experience, as well as lack of information and access to referral agencies (Miller & Jaye, 2007). Some also worried that raising the possibility of DV might cause offense, pain, or shame to the patient. Similar findings were reported by a U.K. study, wherein many PCPs felt poorly prepared to ask questions about DV or to make appropriate referrals (Ramsay et al., 2012).
In Hong Kong, there has been limited research on PCPs’ management of DV. A recent survey, however, investigated PCPs’ attitudes toward child abuse (Leung, Wong, Tang, & Lee, 2011). Although child abuse is commonly classified into a separate category, the findings may still be of some relevance to DV. The study found that only 35.8% of its respondents reported every suspected child abuse case they encountered to governmental authorities, while 40.0% had never reported. The most common barriers to reporting were lack of sufficient evidence of abuse (65.5%), reluctance to get involved with the court or legal systems (42.9%), and thinking that the reporting process would be too time consuming (42.1%). Besides, one third (33.3%) felt that reporting might do more harm than good for the child (Leung et al., 2011). The attitudes of PCPs toward DV with specific focus on spouse battering and sexual aggression in a Chinese context need further research. Many women in Asian countries believe that family matters, including DV, are private and to some extent shameful, and should be kept confidential. The patriarchal nature of family relationships favors male dominance, and accepting the husbands’ behavior may be viewed as loyalty to marriage and preserving family unity (Othman, Goddard, & Piterman, 2014). It is uncertain how these values may have affected the professional judgments of doctors trained in a mixed Chinese-Western cultural environment such as Hong Kong. Moreover, practice settings may also affect the type and amount of support, such as protocols and referral mechanism, for the PCPs in terms of DV management. Those working in the private sector who provide 75% of Hong Kong’s primary care services, often in solo practices, may receive less support from the health care system (Sun, Lam, Lam, & Lo, 2015).
This study aims to investigate the barriers of Hong Kong PCPs toward managing DV, including barriers of recognition, management, and referrals of these patients. The findings will be instrumental for medical educators and policy makers to design interventions and education programs for PCPs, other health service providers, and patients.
Method
A combined qualitative and quantitative approach was adopted for this study. Ethics approval was obtained from the local Institutional Review Board of The University of Hong Kong/Hospital Authority Hong Kong West Cluster (UW 16-2077).
Qualitative Approach
We started with focus group interviews to explore the opinions of the PCPs on the study topic. We purposively recruited participants from both public and private settings with a wide range of characteristics and experience. Honorary teachers of the Department of Family Medicine and Primary Care of the University of Hong Kong were contacted to recommend participants for the interviews based on their professional network. Invitation letters were sent to them and followed by telephone contact. We conducted four focus group interviews of 7 to 10 participants each between September and November 2017. There were two focus groups for PCPs working in the public sector and another two groups for those working in private settings, with a total of 26 participants. Among them, 57.7% were male and 42.3% were female. The mean years after graduation from medical school were 18.8. Questions on participants’ views toward the barriers to managing DV were raised and discussed in the interviews. We aimed to avoid presumption of attitudes of the participants who were encouraged to share their opinions freely. An interview schedule was used to ensure relevant questions were covered.
Two experienced facilitators led the 90-min interviews, which were audiotaped and then transcribed verbatim. Using the content analysis approach described by Hsieh and Shannon (2005), coding categories were inductively derived from the text data. The data were coded independently by two investigators of the research team who are experienced in qualitative research. The coding consistency between the two sets was checked, and the majority of the codes were consistent. Inconsistencies were resolved by discussion between the two investigators to reach an agreement for a common theme. The key themes of barriers and attitudes on DV management identified from the focus group findings were incorporated into the questionnaire for the quantitative survey.
Quantitative Approach
Sample
We invited all members of the Hong Kong College of Family Physicians (HKCFP) to complete a structured questionnaire. Similar to the U.S. practice, a PCP in Hong Kong can be a family physician or general practitioner, as well as general pediatrician, internal medicine physician, or a physician of some other fields practiced as PCP. The total number is around 6,000 but there is no government published list to classify them as PCPs. To set a clear sampling frame for the survey, we selected all 1,515 members from the HKCFP as they provided the most readily available list of PCPs. The college members were reached with the help of the HKCFP, and a total of three rounds of invitations were sent between January and August 2018. A total of 504 questionnaires were returned with an overall response rate of 33.3% (504/1,515).
Questionnaire
The questionnaire itself was anonymous but coded with a unique reference number to identify the respondent for subsequent rounds of reminders. The code was known to one research assistant only and not available to members of the research team. The questionnaire was sent with an invitation letter that asked for consent of the subject to fill in the questionnaire. A completed and returned questionnaire indicated that the respondent agreed to participate in the study. The questionnaire was designed based on findings from the qualitative interviews with PCPs, a review of relevant literature, and comments from research team members. The questionnaire, which mainly asked for descriptive facts, attitudes, and experience, was pilot-tested for its face- and content-validity, and minor modifications were made. The questionnaire contained sections on barriers to DV management, characteristics of clinical practice relating to DV (e.g., number of DV cases suspected and managed), attitudes on DV management, and respondents’ background information. A 4-point Likert-type scale (1 = strongly disagree, 2 = disagree, 3 = agree, 4 = strongly agree) was adopted as the options for the questions about experiences, while answers for personal and demographic information and clinical practice characteristics were mainly of yes/no responses and numbers.
Statistical analysis
The quantitative data were analyzed using JMP—Statistical Discovery from SAS (Release 10.0.0). We used frequencies and percentages to summarize the responses to the barrier items. Factor analysis on the barrier items was carried out to determine whether there were underlying dimensions among the responses to these items. Principal components analysis with a varimax rotation was adopted on the correlation matrix. New barrier scores based on the factors identified were derived for further analysis. One-way ANOVA was carried out to determine the effect of the PCPs’ attitudes, personal, training, and practice characteristics on the barrier scores and number of DV cases handled. A p value <.05 was considered statistically significant.
Results
Focus Group Participants’ Views on the Barriers to DV Management
Participants discussed their views on different kinds of barriers to managing patients encountering DV. The themes of barriers and relevant quotes are summarized in Table 1.
Qualitative Results of the Themes for Barriers to Management of DV.
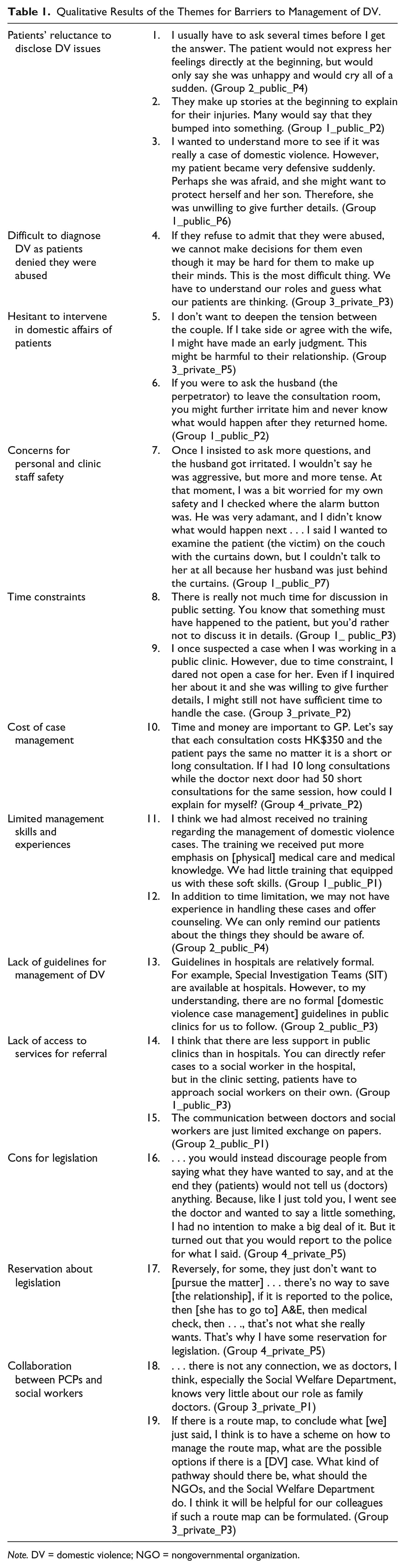
Note. DV = domestic violence; NGO = nongovernmental organization.
Patients’ reluctance to disclose DV issues and difficulty in diagnosis
A major barrier faced by PCPs in managing DV was patients’ reluctance to disclose their DV issues. When doctors suspected a possible case of DV and attempted to collect further information from the patient, many patients were reluctant to reveal details (Quote 1). They even made up stories to explain their injuries (Quote 2). Some patients were unwilling to disclose information, as they wanted to protect their family members despite the abusive behaviors (Quote 3). Apart from being reluctant in disclosing information, some patients denied that they had been abused. This made it difficult for the PCPs to diagnose DV. Moreover, some victims were indecisive and were unsure about whether they wanted to seek help. The PCPs often had to guess what these patients were thinking of (Quote 4).
Hesitant to intervene in domestic affairs of patients
Some PCPs were also hesitant about interfering in the domestic affairs of their patients. They were worried that taking sides with the patient would imply involving themselves in the couple’s conflict, which might worsen patients’ relationship with their spouse/families (Quote 5), or feared that their interference would trigger more severe abuses (Quote 6).
Concerns for personal and clinic staff safety
Some also expressed concerns over personal and clinic staff safety, as some had witnessed the abuser who accompanied the patient (victim) to see the doctor getting irritated and becoming aggressive when the doctor attempted to obtain further information from the victim (Quote 7).
Time constraints and cost
Longer consultation time was required when doctors looked into a case of DV. Although suspecting a case, doctors in public settings tended not to dig into the details, as they doubted they had sufficient time to handle it (Quotes 8 and 9). The doctors in private settings were also concerned about the financial cost of managing DV cases as their income would drop with longer consultations (Quote 10).
Limited management skills and experiences
Participants also doubted that they had sufficient skills and experience to manage cases of DV. They believed they lacked counseling skills (Quote 11) as the training they received mainly focused on medical knowledge (Quote 12).
Lack of management guidelines and access to services for referral
Moreover, no formal management guidelines for DV were available (Quote 13) and access to referral services was lacking in both public and private primary care settings. Only doctors in public hospitals could directly refer DV cases to medical-social workers (MSW) for follow-up, while there is no similar formal mechanism for PCPs working in public or private primary care clinics to gain access to MSWs. They often had to request victims to approach social workers on their own (Quote 14). Communication between doctors and social workers was also limited (Quote 15).
Participants’ Views on the Role of PCPs in DV Management
Legislation for reporting of DV
A few doctors expressed their reservation about whether the government should legislate for the mandatory reporting of DV cases by medical professionals. Some doctors believed there was not much a third party could do to help, and preferred to downplay any suspected encounter due to oversensitivity of their own. Besides, they pointed out that patients might be concerned about being reported by the PCPs and were no longer willing to disclose anything about the abuse (Quotes 16 and 17). A doctor emphasized that it was always uncertain whether a doctor should intervene in the relationship between couples, as patients might simply seek someone to talk to but are not asking for intervention. Instead, they suggested a nonjudgmental platform where patients could seek professional help with minimal labeling effect and judicial concern. More training in family medicine to enhance family perspective would be required to make this happen.
Collaboration between PCPs and social workers
Recognizing the social aspects of DV, the doctors complained about too little communication between PCPs and social workers. They wished to have a knowledge exchange on handling DV encounters and a referral map for better management (Quotes 18 and 19). Due to the absence of a clear protocol and referral system, they felt that “actions should be taken” more on a moral than a professional ground. Furthermore, a doctor argued that an abuser would not remain an abuser forever due to societal changes.
Results of the Questionnaire Survey
Of the 504 respondents, 59.4% were male and 40.6% were female; 49.3% were from the public and 50.7% from the private service sector. The mean (SD) years after graduation from medical school were 22.0 (SD = 12.42). Details of their personal, training, and practice background are shown in Table 2.
Personal, Training, and Practice Characteristics of Survey Respondents.
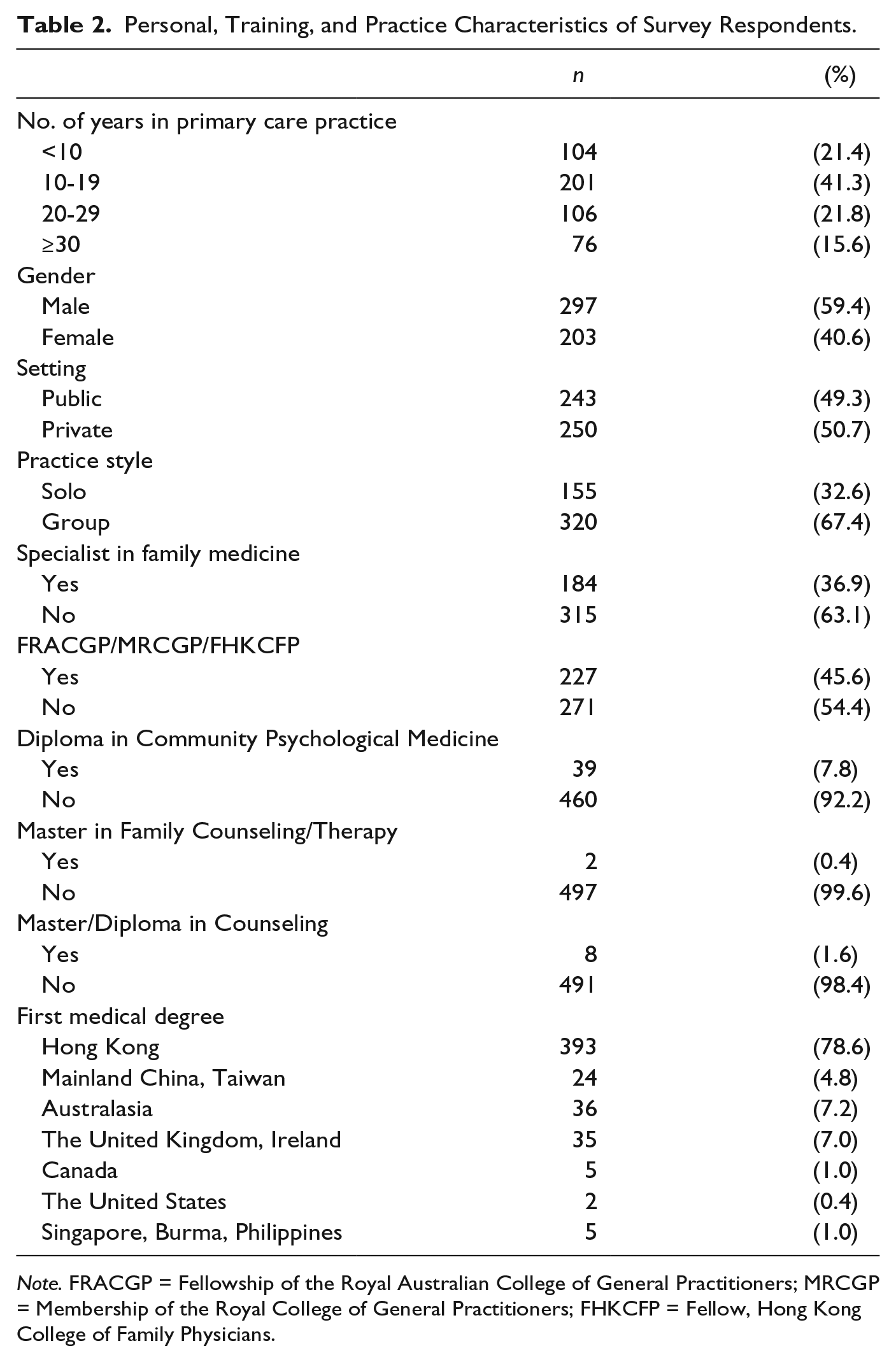
Note. FRACGP = Fellowship of the Royal Australian College of General Practitioners; MRCGP = Membership of the Royal College of General Practitioners; FHKCFP = Fellow, Hong Kong College of Family Physicians.
Our survey results revealed that about one third of the PCP respondents had never asked (38.1%) their patients about nor suspected (32.1%) them of DV issues, while more than half (56.5%) had never managed such cases in the past 5 years (Table 3). For those who did ask, suspect, and manage their patients’ DV issues, most of them (40%-60%) had handled one to five cases. Overall, the mean numbers for the survey respondents’ dealing with DV cases over the past 5 years were small: 4.06 for asking about DV issues, 3.00 for suspecting, and 1.32 for managing DV cases, respectively.
Number of Patients Being Asked About DV, Suspected, and Managed for DV in the Past 5 Years.
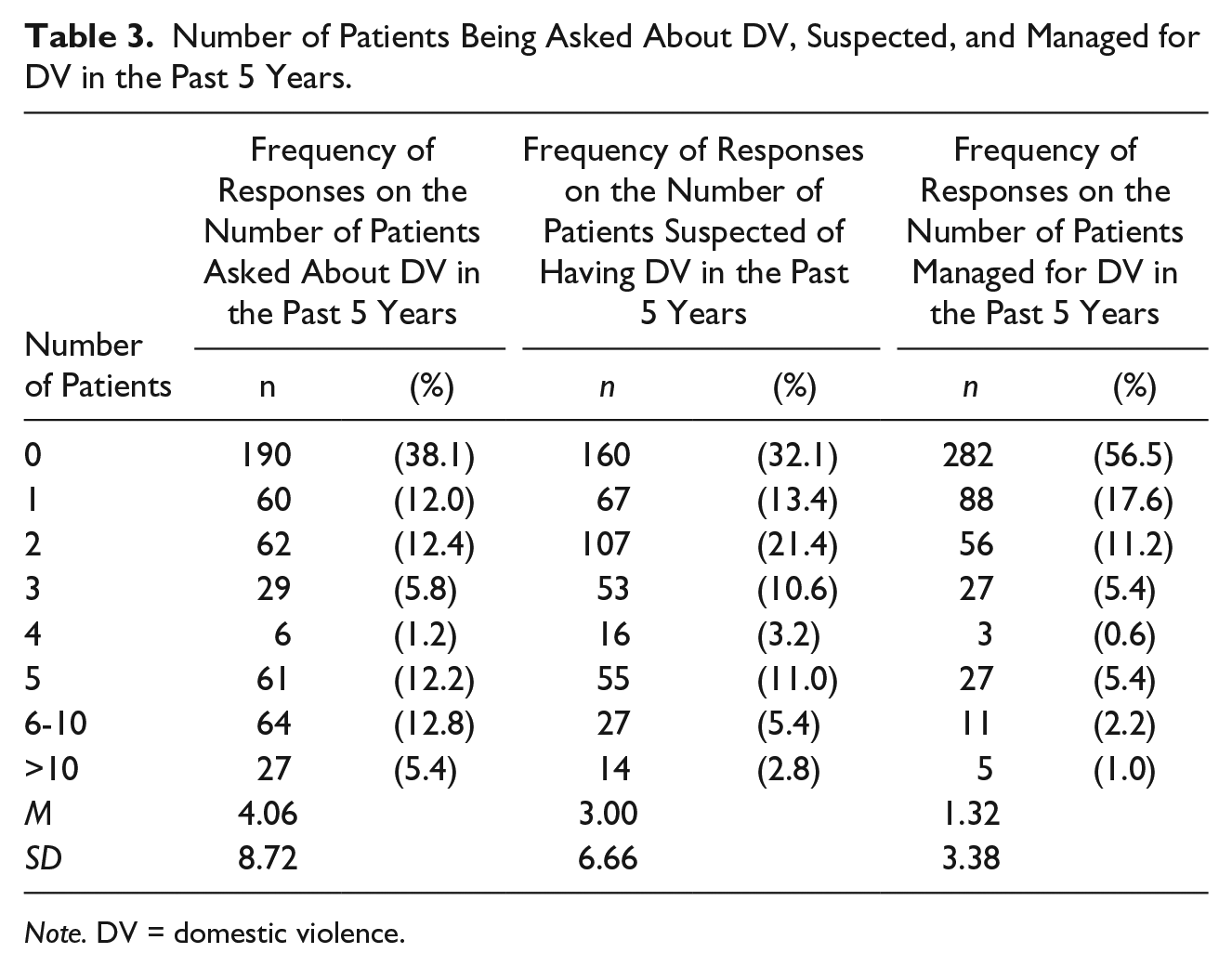
Note. DV = domestic violence.
The respondents were asked about their attitudes to the barriers based on the themes identified from the qualitative interviews. The perceived barriers were ranked by their combined percentages of agree and strongly agree responses (Table 4). Among the 14 items, the top five barriers included patients’ denial of being abused (91.9%), followed by time constraints (90.1%), patients’ reluctance to disclose DV issues (90.0%), limited experience (89.9%), and lack of guidelines for managing DV issues (88.7%). More than 70% of the respondents agreed that limited skills (84.6%), lack of access to services for referral (76.1%), and lack of support from social workers (72.2%) were barriers to the management of DV. Less than one third of respondents were worried that managing DV cases would do more harm to patients and their families (23.4%) or would threaten the safety of the clinic staff (28.8%).
Survey Results on the Barriers to Management of DV.
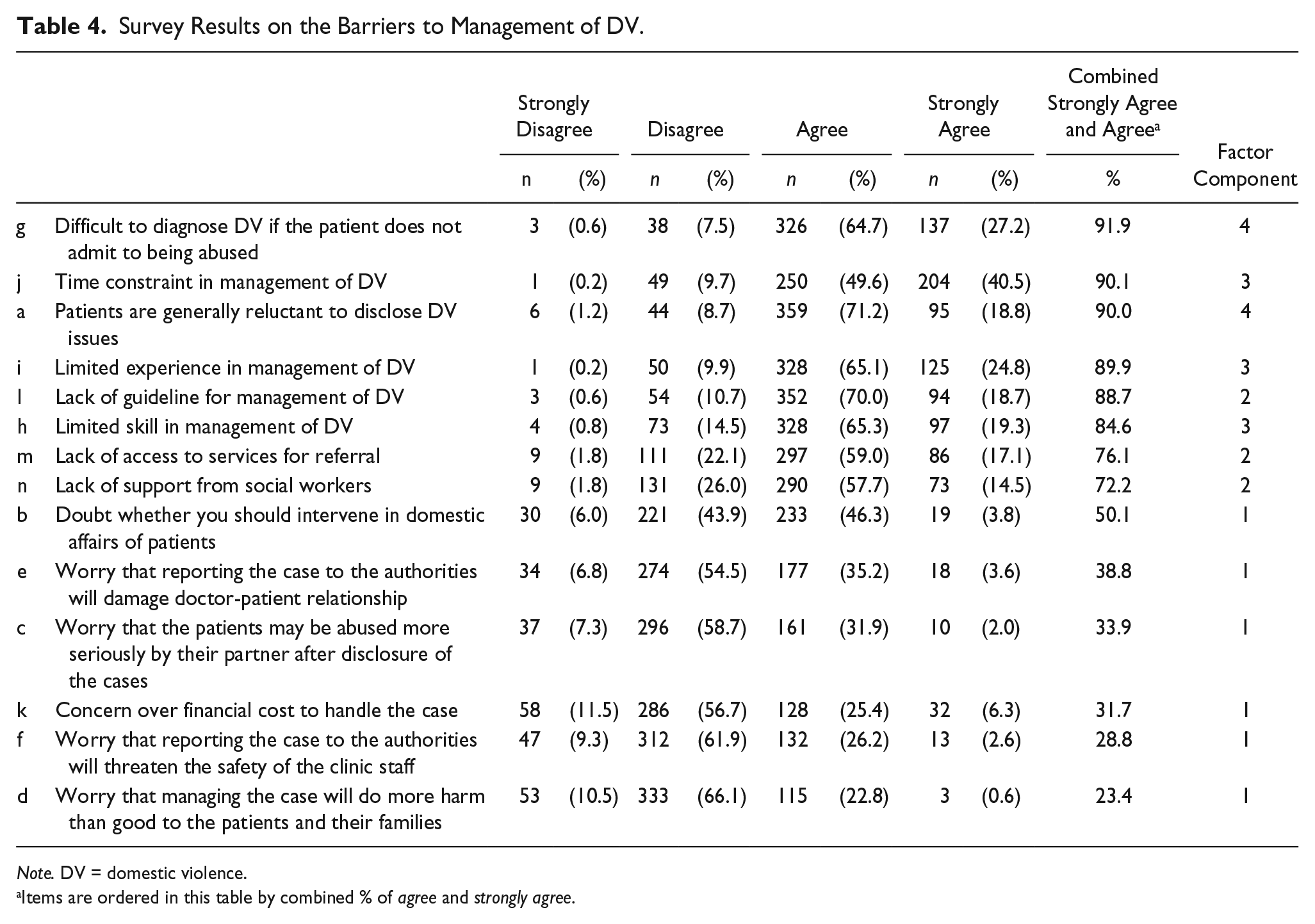
Note. DV = domestic violence.
Items are ordered in this table by combined % of agree and strongly agree.
Factor Analysis of the Barrier Items
A factor analysis was conducted for all the barrier items. The result suggested four factors, which explained 60% of the total variation. The four factors could be closely approximated by the average of the survey responses to specific items according to their factor loadings (shown in the Supplemental Material). The four barrier scores are based on the following four factors:
Factor 1—mean score of the six responses to Items b-f, k, which are barriers relating to the worries about intervening domestic issues.
Factor 2—mean score of the three responses to Items l, m, n, which are barriers relating to lack of guideline and referral services.
Factor 3—mean score of the three responses to Items h, i, j, which are barriers relating to the PCPs’ limited skills and time in managing DV.
Factor 4—mean score of the two responses to Items a, g, which are barriers relating to patients’ reluctance in disclosure.
A higher score means greater perceived barriers related to the corresponding variables. The four factors comprised all 14 items, and the corresponding factor for each item is shown in Table 4.
Association of PCPs’ Background Characteristics With Barriers and Number of Cases Handled
Table 5 compares the mean barrier scores of different factors and the mean number of DV cases handled among PCPs with different groupings of characteristics. A higher mean score implied a stronger perceived barrier. Significant differences (p < .05) were indicated by the results of ANOVA. We found that PCPs with more years of practice perceived greater barriers under Factor 1 (worries about intervening in domestic issues). In contrast, those with shorter years of practice, as well as being female, perceived greater barriers under Factor 3 (limited skills and time in managing DV cases). PCPs in the private sector perceived greater barriers under Factor 1 (worries about intervening in domestic issues), Factor 2 (lack of guideline and referral services), and Factor 4 (patients’ reluctance in disclosure), but perceived fewer barriers under Factor 3 (limited skills and time in managing DV cases). PCPs having a specialist qualification in family medicine perceived fewer barriers under Factor 1 and Factor 2, while those graduated from medical schools in Western countries perceived fewer barriers under Factor 3.
Association of PCPs’ Background Characteristics With Barriers and Number of Cases Handled.
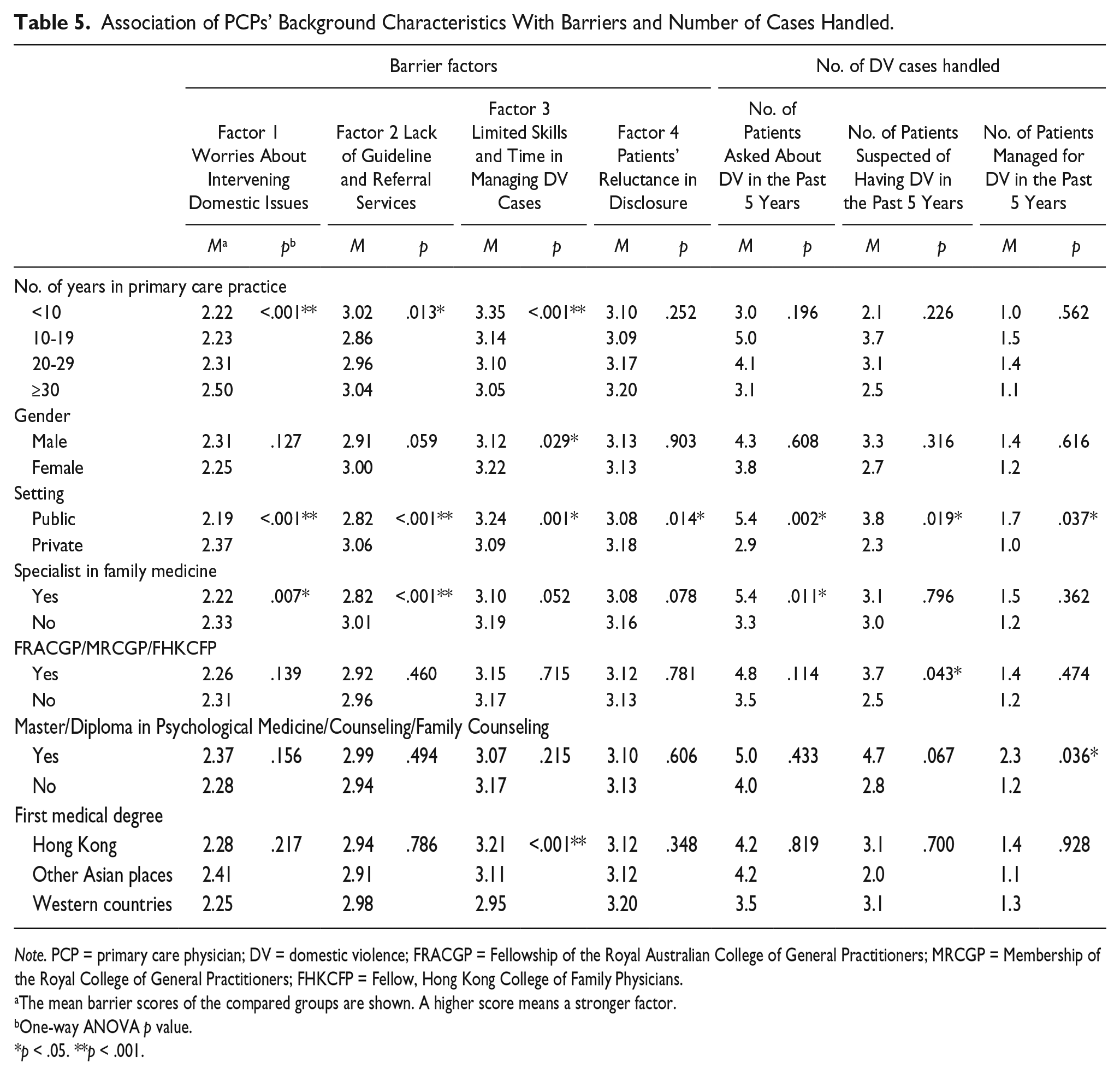
Note. PCP = primary care physician; DV = domestic violence; FRACGP = Fellowship of the Royal Australian College of General Practitioners; MRCGP = Membership of the Royal College of General Practitioners; FHKCFP = Fellow, Hong Kong College of Family Physicians.
The mean barrier scores of the compared groups are shown. A higher score means a stronger factor.
One-way ANOVA p value.
p < .05. **p < .001.
PCPs working in the public setting had significantly higher mean numbers of patients being asked about DV (M = 5.4 vs. 2.9), suspected DV (M = 3.8 vs. 2.3), and managed DV (M = 1.7 vs. 1.0) in the past 5 years compared with the private PCPs. PCPs being specialist in family medicine asked more patients about DV (M = 5.4 vs. 3.3). PCPs with a fellowship of HKCFP reported more suspected DV cases (M = 3.7 vs. 2.5), while PCPs with master/diploma in psychological medicine, counseling, or family counseling had more patients managed for DV (2.3 vs. 1.2) on the average.
PCPs’ Attitudes to DV Management and Association With Barriers and Number of Cases Handled
Only 37.8% of the respondents agreed with legislation for mandatory reporting of DV cases. Instead, 65.9% thought that reporting or not reporting DV cases to the police should be decided by the patients. Almost all (97.8%) agreed that they needed to have stronger collaboration with social workers. Besides, 87.4% agreed that training in family medicine would be helpful for management of DV, and 95.0% agreed that specific DV training programs should be provided to PCPs. Regarding their role in DV management, 77.2% thought that social workers have a stronger role than doctors, and 59.0% agreed that they had a limited role to help if the DV case did not involve medical issues. In addition, 83.9% thought that DV behaviors of the abusive partner might reduce when his or her psychosocial state got better.
We further analyzed the association of PCPs’ attitudes to DV management with the mean barrier scores and mean number of cases handled (Table 6). PCPs who agreed that social workers had a stronger role than doctors in DV management also showed greater concurrence with barriers under Factor 1, Factor 2, and Factor 3. Furthermore, for PCPs who agreed that doctors had a limited role to play in DV cases that did not involve medical issues, their scores of barriers in all aspects were also higher, and they also had a smaller mean number of patients suspected of having DV (M = 2.5 vs. 3.8). PCPs who agreed that specific training programs on DV management should be provided perceived fewer barriers under Factor 1, but had a smaller mean number of patients managed for DV (M = 1.2 vs. 2.9).
Association of PCPs’ Attitudes on DV Management With Barriers and Number of Cases Handled.
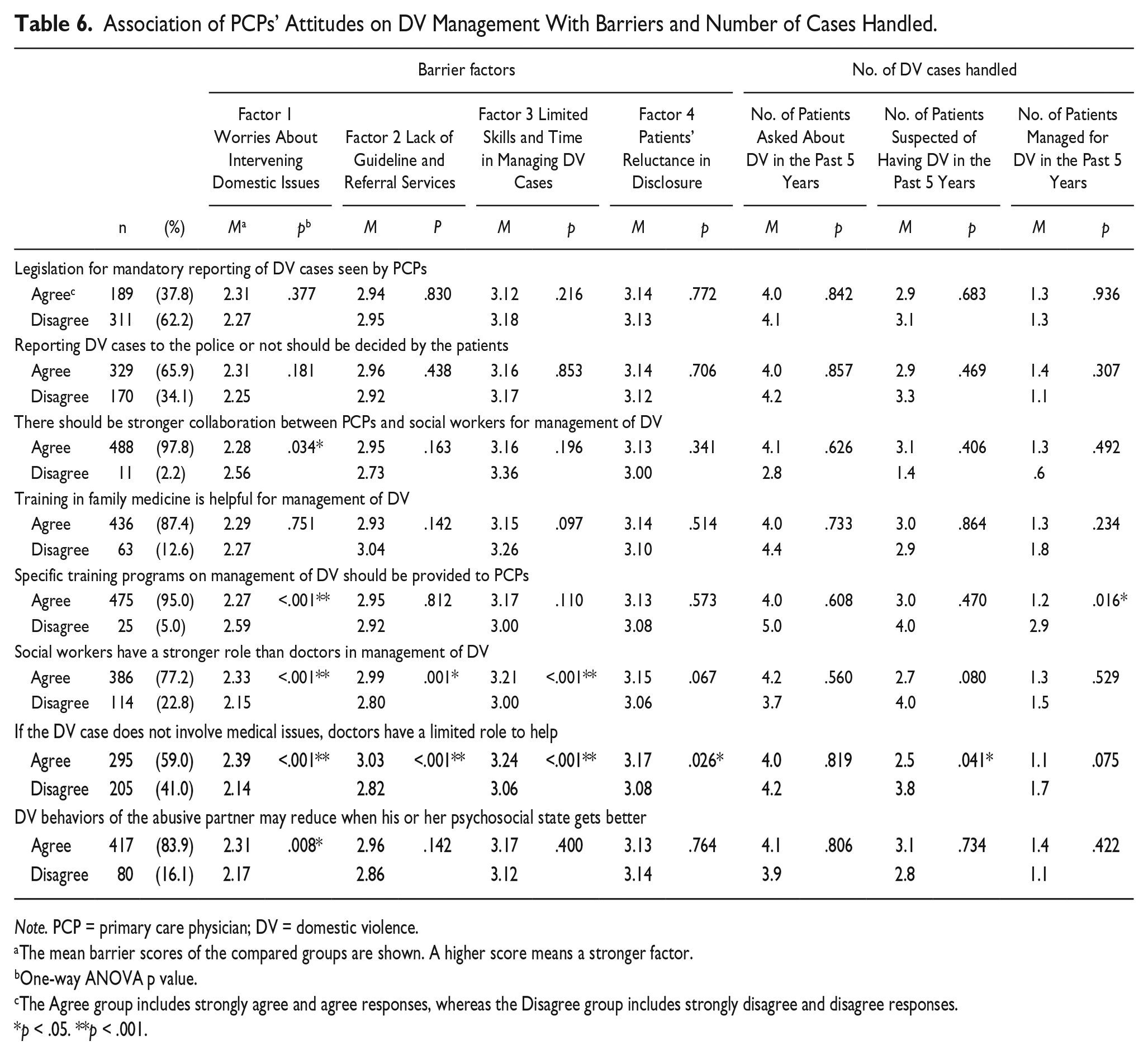
Note. PCP = primary care physician; DV = domestic violence.
The mean barrier scores of the compared groups are shown. A higher score means a stronger factor.
One-way ANOVA p value.
The Agree group includes strongly agree and agree responses, whereas the Disagree group includes strongly disagree and disagree responses.
p < .05. **p < .001.
Discussion
This study aims to investigate the barriers of Hong Kong PCPs toward managing DV. Our findings showed that DV issues were not frequently taken up by PCP respondents, the mean numbers for their management of DV cases, including 4.06 for asking, 3.00 for suspecting, and 1.32 for managing DV cases, respectively, in the past 5 years, were small. Considering a total population of nearly 6,000 PCPs in Hong Kong, the estimated number of DV cases managed per year was about 1,500. This number was low when compared with a total of 3,321 newly reported spouse/cohabitant battering cases in 2016 (Social Welfare Department, n.d.), not to mention cases unrecognized and unknown to the authorities. As reports on the number of DV cases handled by PCPs were limited, except for a study in Iran that reported 10% of its PCP respondents would always screen patients for DV, and 30% to 40% would follow up or make referrals for DV during the past 3 months (Rasoulian, Shirazi, & Nojomi, 2014), it is difficult to compare the figures with other areas and regions.
The four barrier factors identified in our study, including worries about potential harm to patients if intervened, lack of guidelines and support, limited skills and time, and patients’ reluctance to disclose, concur mostly with findings from other Western countries (Miller & Jaye, 2007; Ramsay et al., 2012), and they also bear cultural-specific implications to the Hong Kong context. Factor 1 reflected PCPs’ concern toward the desirability and outcomes of DV management. Half (50.2%) of our respondents had doubts about intervening in patients’ domestic affairs, and about one third or less worried about the adverse effects of DV management on the patients, doctor–patient relationship, or clinic staff safety. While Western experiences suggested positive instead of negative outcomes from DV management were often the case (Glowa, Frazier, Wang, Eaker, & Osterling, 2003), there was also evidence that indicated that abuse would get worse if victims notify health practitioners or authorities. The important point is PCPs need to provide patients with a “safe sanctuary” for help-seeking (McCall-Hosenfeld, Weisman, Perry, Hillemeier, & Chuang, 2014), such that the fear of adverse effect caused by disclosure and management of DV can be overcome. That would require adequate skills from the PCPs and good support from the health authorities. Our study also confirmed that PCP respondents who possessed more training in family medicine, psychological medicine, counseling or family therapy, had more patients being asked, suspected, and managed for DV. Relevant and higher training in those areas enabled PCPs to have greater confidence to engage themselves in DV screening and management.
Moreover, uncertainty about intervention in the domestic realm may also reflect a cultural alertness to the rigid boundary of “family,” especially among the older generation doctors, that they did not want to involve themselves in the conflicts between the couple or to take sides with either the wife or husband, while the younger doctors were concerned more about practical constraints such as time and limited experience in DV management. It is noteworthy that PCPs’ attitudes toward the role of doctors and other professionals in DV management had also influenced their perception and practice considerably. Doctors in the focus group discussions had expressed their beliefs that DV cases should be handled by social workers instead of doctors who were specialized in taking care of patients’ physical and mental health but not their family conflicts. In the survey, 59.0% of the respondents agreed that they had a limited role to help if the DV case did not involve medical issues. Respondents who held such views also scored higher in all of the four barrier factors. While there are boundaries between domestic and medical realms, doctors’ prime concern is how domestic conflicts and violence would have led to health problems caused by physical harm and psychological distress. The harm and distress that resulted from DV cannot be adequately treated if PCPs omit or neglect the underlying causes. Doctors’ “limited” role may not be so limited if patients’ mental well-being is seen as the focus of attention in DV management at the primary-care level.
Another problem the PCPs faced, especially those working in the private sector, was their limited access to referral services and the absence of a mechanism to facilitate medical-social collaboration in DV management. Collaboration with social service agencies, such as referring DV patients to social workers for follow-up was carried out on the PCPs’ initiative depending on how enthusiastic and ready she or he was to be involved in DV management. While universal or targeted screening of female patients about DV is considered a useful approach to identify DV (Daoud et al., 2019; Ma & Pun, 2016; McCall-Hosenfeld et al., 2014), it would not be a viable option for PCPs if related management guidelines and training, referral systems, and support were not provided.
Presently, doctors working in local public hospitals are formally linked to MSWs where referrals are more accessible, and that partly accounts for the greater number of patients being asked, suspected, and managed for DV among the PCPs in the public sector, especially those working in hospital settings. However, medical–social collaboration is much weaker or lacking in public outpatient clinics and private clinics, which a large proportion of patients attend for care. There are no established referral systems and access to social workers for PCPs. To overcome the barriers, several areas need to be emphasized and enhanced. It is hoped that public health education can reduce patients’ resistance to seeking help for DV, while more training and institutional support including time allowance, management guidelines, referral sources, and formal mechanisms help improve the skills and confidence of PCPs to manage DV patients.
Strengths and Limitations
This study addressed a knowledge gap of DV management by PCPs in a Chinese context. The findings will also be useful for health care professionals who look after Chinese patients. However, this study had some limitations. First, there might be potential recall bias for self-reported data but it should be minimal as the questions were mainly about their usual practice characteristics and experiences. Second, the response rate of this study was 33.3%. It is not great for this kind of study, but is higher than most other surveys among doctors in Hong Kong (The Harvard Team, 1999; Leung, Ho, Chan, & Wong, 2002). Third, the proportion of survey respondents from the public sector (49.3%) was higher than the corresponding proportion (about 25%) in the local system. This might reflect that the public PCPs had higher interest in the study topic. We analyzed the effect of PCPs’ work sector (public vs. private) on the barrier scores and number of cases handled in Table 4.
Conclusion
The frequency of Hong Kong PCPs’ recognizing and managing DV issues of their patients was not high, owing to a variety of barriers and the perception of the PCPs about the role of doctors and the nature of DV issues. The barriers comprised PCPs’ worries about intervention, the lack of management protocols and referral support, time constraints, limited skills and experience, and patients’ reluctance to disclose and seek help. The barriers are interrelated and resolving one may help reduce the obstacles of the other barriers. Resolving PCPs’ worries through training in how to ask explicit questions about abuse, enhancing clinical skills in DV diagnosis and management, provision of DV management guidelines, and referral pathways may be good starting points to bridge the gaps. Moreover, cooperation and mutual support between PCPs and social workers are also important, with the building of a medical-social platform being beneficial for DV management in the long run.
Supplemental Material
Appendix – Supplemental material for Management of Domestic Violence by Primary Care Physicians in Hong Kong: Association With Barriers, Attitudes, Training, and Practice Background
Supplemental material, Appendix for Management of Domestic Violence by Primary Care Physicians in Hong Kong: Association With Barriers, Attitudes, Training, and Practice Background by Kai Sing Sun, Tai Pong Lam, Leon Piterman, Kwok Fai Lam, Wai Sin Tang, Kit Wing Kwok, Hoi Yan Chan, Dan Wu and Agnes Tiwari in Journal of Interpersonal Violence
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work described in this article was fully supported by Seed Fund for Basic Research, University Research Committee, The University of Hong Kong.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.