
Abstract
This study aimed to clarify the interannual changes in intimate partner violence against pregnant women after the March 11, 2011 Great East Japan Earthquake in target areas of Miyagi Prefecture that were damaged by the earthquake and tsunami. Because of this disaster, in Miyagi Prefecture, approximately 12,000 people died or went missing, and approximately 238,000 buildings were destroyed. According to the U.S. Geological Survey, the Great East Japan Earthquake is the fourth largest earthquake in the world and the largest in Japan since 1900. The present study was part of the Japan Environment and Children’s Study. Data from June 2011 to May 2014 of 79,222 pregnant women were analyzed, calculating the prevalence of physical and mental intimate partner violence in the inland, north coastal, and south coastal areas of Miyagi. These prevalence rates were compared with nationwide rates of intimate partner violence in 2011 using univariate and logistic regression analyses. After the disaster, the incidence of mental intimate partner violence increased in the south coastal area and then improved later (19.4%, 13.1%, and 13.3% for south coastal area, and 13.8%, 13.8%, and 13.1% for nationwide in 2011, 2012, and 2013, respectively). However, in the north coastal area, the incidence of physical intimate partner violence increased after the disaster and then improved later (2.7%, 1.5%, and 1.3% for north coastal area, and 1.4%, 1.3%, and 1.1% for nationwide in 2011, 2012, and 2013, respectively). In the inland area, however, the prevalence of both mental and physical intimate partner violence was consistently higher than nationwide rates after the disaster.
Keywords
On March 11, 2011, a massive earthquake measuring 9.0 on the Richter scale struck northeast Japan and led to severe damage to the East Japan coast (Sakurai et al., 2016). The present authors previously reported that there was an increased incidence of postpartum depression following the Great East Japan Earthquake in areas that were affected by the earthquake and tsunami (Nishigori et al., 2014). Disaster-related mental stress has also been shown to increase the incidence of violence by male partners (Norris, Perilla, Riad, Kaniasty, & Lavizzo, 1999). In particular, intimate partner violence (IPV) has been reported to occur more frequently after disasters (Anastario, Shehab, & Lawry, 2009). IPV against pregnant women is a risk factor associated with perinatal complications and child abuse, and is considered a serious issue in perinatal management.
In Japan, the movement against IPV began in the mid-1970s (Yoshihama, Tsuge, Yunomae, Ikeda, & Masai, 2013). In 2001, a law was enacted on the prevention of IPV and the protection of victims. In 2018, the government allotted a budget of 18.2 billion yen to promote measures to prevent IPV (Ministry of Health, Labour, & Welfare, 2019). Detailed discussions about disaster-related violence against women began only after the 1995 Great Hanshin-Awaji Earthquake. However, only a few studies on the topic have been conducted since then.
Patriarchal traditions and male-centered social systems predominate in Japanese society, wherein discrimination is deeply rooted, though not always obvious. During the Great East Japan Earthquake, social structural issues that were present even in “normal” times (as opposed to during disaster times), such as sexism, became more evident and various contradictions, inequalities, and distortions became more concretely and extremely apparent. Therefore, Domoto, Ohara, Reiko, Hara, and Amano (2013) discussed the importance of gender sensitivity in disaster risk reduction. The Asia-Pacific Input Document for the Post-2015 Framework for Disaster Risk Reduction (Hyogo Framework for Action 2) Final Draft (2015) states that it is important to have a gender perspective and to involve women in decision-making regarding disaster risk reduction policy. Furthermore, Parkinson, Lancaster, and Stewart (2011) reported that the relationship between disaster and violence has not been established because the occurrence of IPV against women during disasters is not known, in addition to stating that the issue of violence against women continues to be ignored in disaster countermeasures. Therefore, it is important to conduct long-term follow-up studies of disaster-affected areas to examine the relationship between disaster and violence against women.
The Ministry of the Environment of Japan launched a large-scale cohort epidemiological research project called the Japan Environment and Children’s Study (JECS) in January 2011. The target cohort included 100,000 children and their parents (Kawamoto et al., 2014). The purpose of the JECS was to investigate the association between environmental factors and children’s health and development (Nishigori et al., 2014). As the JECS has centers nationwide and data can be compared between post-earthquake areas and the whole country, the JECS data were used in this study.
To the best of the authors’ knowledge, there have been no reports on changes over several-year periods in the prevalence of IPV against pregnant women following large-scale disasters. Thus, this study aimed to identify interannual changes in this prevalence in target areas of Miyagi Prefecture (where approximately 12,000 people died or went missing, and approximately 238,000 buildings were destroyed) after the Great East Japan Earthquake, using data obtained from the JECS. This study was part of the JECS, which was initiated by the Japanese Ministry of the Environment as a nationwide, large-scale, prospective birth cohort study. Fifteen regional centers (RCs) in Japan consented to participate in the JECS (Figure 1) (Sakurai et al., 2016). Pregnant women and their partners enrolled more than 3 years in the study between January 2011 and March 2014. Periodic questionnaires and biochemical examinations were conducted both during and after pregnancy; these assessments will be continued until the participating children are 13 years old. Details of the JECS have been described in previous studies (Kawamoto et al., 2014; Michikawa et al., 2018).
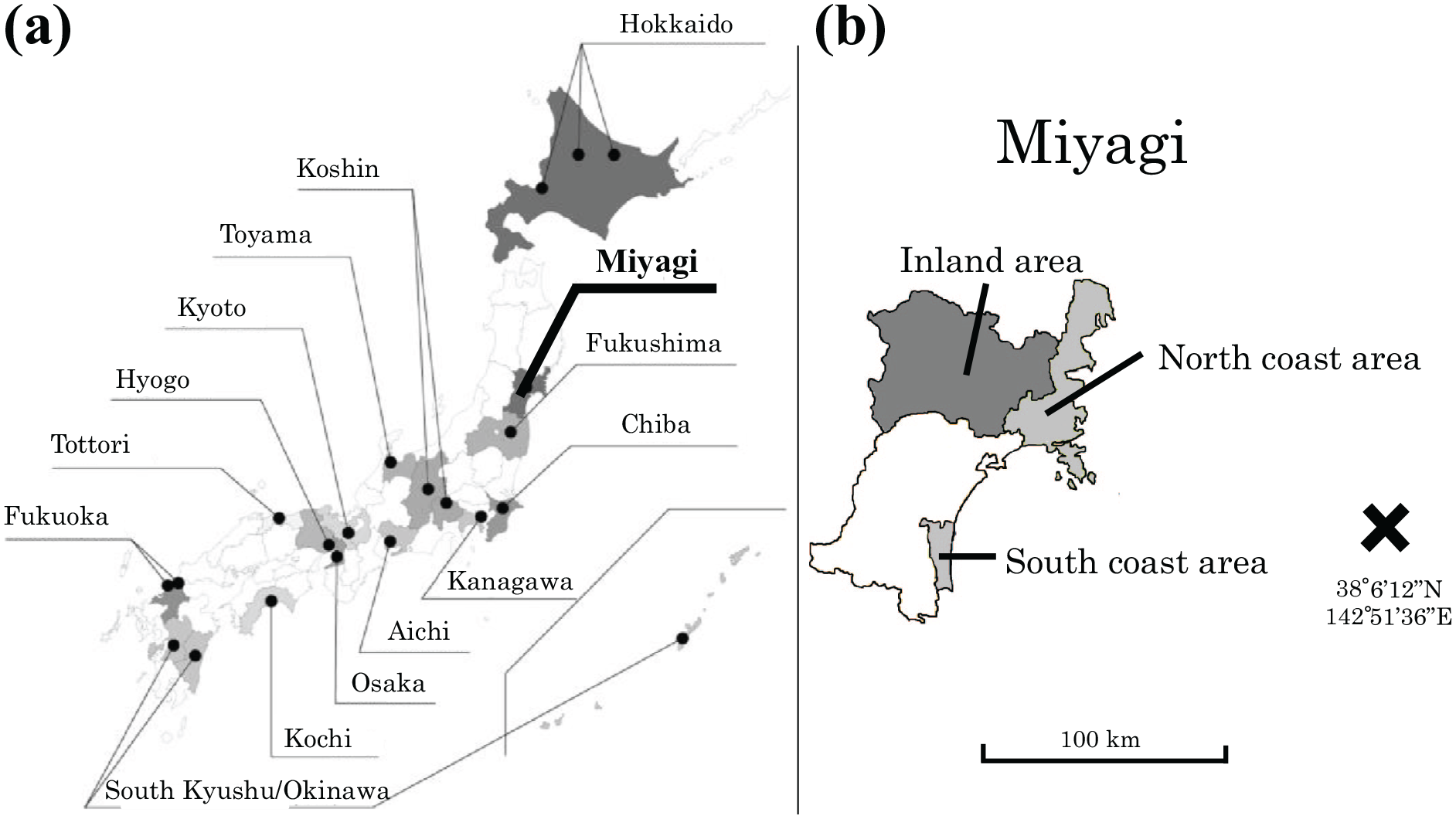
(a) Location of the JECS Regional Centers. (b) Location of the JECS area in Miyagi prefecture.
The current study explored IPV against women in Japan after the Great East Japan Earthquake. However, the type and degree of impact of the disaster differs among victims. Other factors that may cause such differences include (but are not limited to) age, socioeconomic status, race, ethnicity, presence or type of disability or illness, nationality, religion, and native language. It is important to understand the situation of the affected people and provide appropriate support while considering this diversity.
This study examined the actual situation and the subsequent process under the hypothesis that the incidence of IPV to pregnant women increases in the affected area after a large-scale disaster.
Method
Study Design, Data Collection, and Participants
The present analysis is based on the all-birth fixed data sets, “jecs-ag-20160424” and “allbirth_revice001,” which were released in June 2016 and October 2016, respectively. These data sets contain information on 104,102 fetuses and their parents (Michikawa et al., 2018).
The present study included data from 79,222 pregnant women who responded to the JECS questionnaire and were in the second and third trimesters of their pregnancy between June 2011 and May 2014. Participants from the Fukushima unit center were excluded because the nuclear power plant accident at Fukushima was considered to create a huge confounding influence. Participants who had not answered questionnaires on IPV, had given birth to multiples, or had failed to identify their precise residential area in Miyagi were excluded. Participants were divided into three groups based the period in which they were in their second and third trimester: from June 2011 to May 2012, June 2012 to May 2013, and June 2013 to May 2014. The groups were named fiscal year (FY) 2011, FY 2012, and FY 2013 in this analysis, respectively.
Written informed consent was obtained from all participants. Institutional review boards at the Japanese Ministry of the Environment and all participating institutions approved the JECS protocol.
Main Outcome Measurement
All data were obtained from two self-reported questionnaires: the “MT1” questionnaire was administered upon enrollment and during the maternal first trimester (MT1), and the “MT2” questionnaire was administered during the second or third trimester (MT2). The MT2 questionnaire consisted of the following IPV-related questions, which were answered across four response options: “Never,” “Rarely,” “Sometimes,” and “Often.” For the judgment of mental IPV, the women were asked, “Have you ever been insulted or reviled by your partner during the present pregnancy?” (Hereafter, “during pregnancy” refers to the present pregnancy, unless otherwise specified.) For physical IPV, the women were asked, “Have you ever been intentionally hit or beaten by your partner during pregnancy?” To determine the IPV incidence in those recruited at the Miyagi unit center in the study, the answers “Rarely,” “Sometimes,” and “Often” were considered to indicate the presence of mental or physical IPV (Sakurai et al., 2016). The questionnaire on IPV during MT2 is detailed elsewhere (Sakurai et al., 2016). The 14 municipalities of Miyagi Prefecture were classified into three area groups: inland (Tome city, Kurihara city, Osaki city, Shikama-cho, Wakuya-cho, Kami-machi, and Misato-machi), north coastal (Kesennuma city, Ishinomaki city, Minamisanriku-cho, and Onagawa-cho), and south coastal (Iwanuma city, Watari-cho, and Yamamoto-cho; Figure 1) (Sakurai et al., 2016).
Statistical Analysis
The prevalence rates of mental and physical IPV in the north coastal, south coastal, and inland areas of Miyagi, as well as the rates in the remaining 13 RCs other than Miyagi and Fukushima, were calculated for each year. Univariate analysis and logistic regression analysis were used (with 13 RCs in 2011 as the reference group) to compare the prevalence rates for these areas. The risk factors of IPV that were considered were age, marital status, smoking habit, alcohol habit, employment situation, and household income level. SAS version 9.4 (SAS Institute Inc., Cary, North Carolina, USA) was used for the statistical analysis.
Results
Participants’ characteristics are shown in Table 1. Furthermore, the annual changes in mental and physical IPV across the four target areas are presented in Tables 2 and 3, respectively.
Characteristics of Subjects.
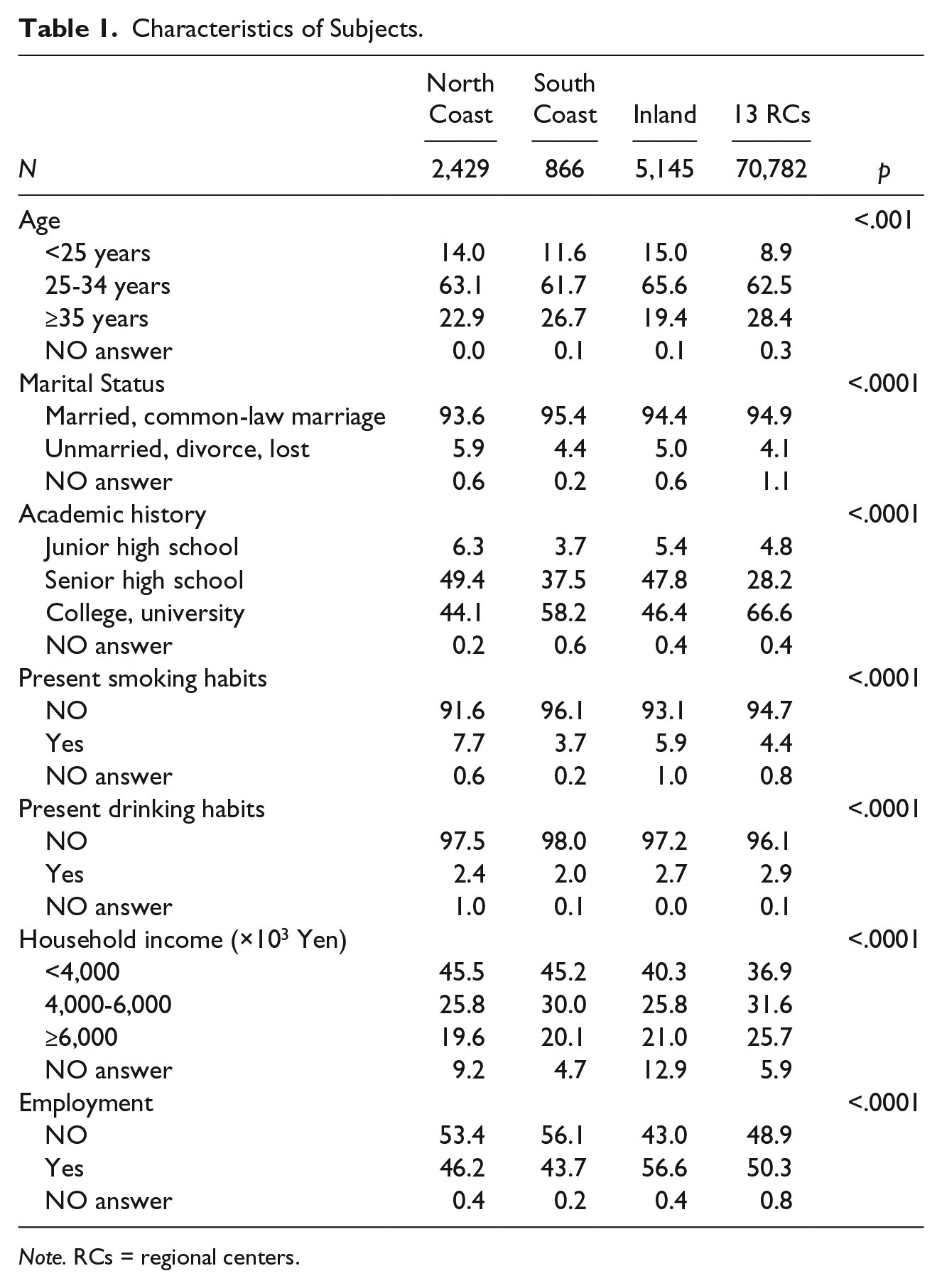
Note. RCs = regional centers.
Interannual Change in Mental Intimate Partner Violence in the North Coast, South Coast, Inland of Miyagi, and 13 RCs.
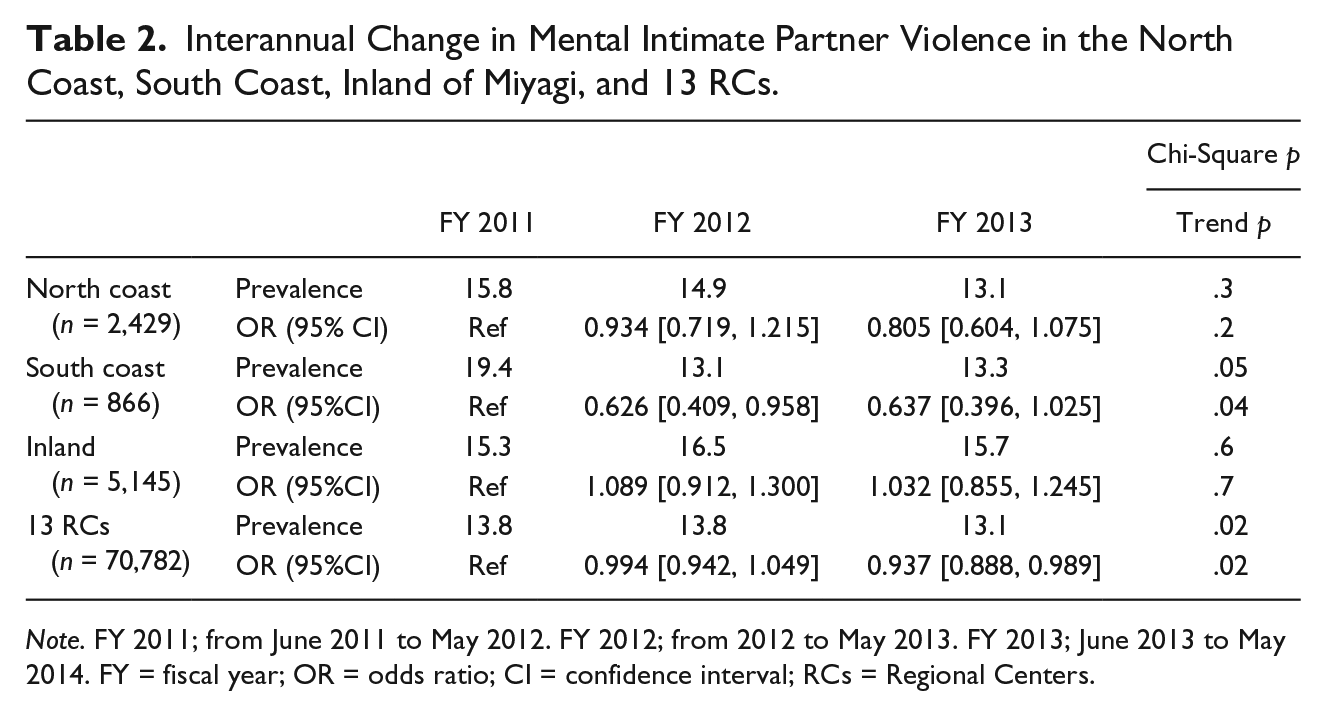
Note. FY 2011; from June 2011 to May 2012. FY 2012; from 2012 to May 2013. FY 2013; June 2013 to May 2014. FY = fiscal year; OR = odds ratio; CI = confidence interval; RCs = Regional Centers.
Interannual Change in Physical Intimate Partner Violence in the North Coast, South Coast, Inland of Miyagi, and 13 RCs.
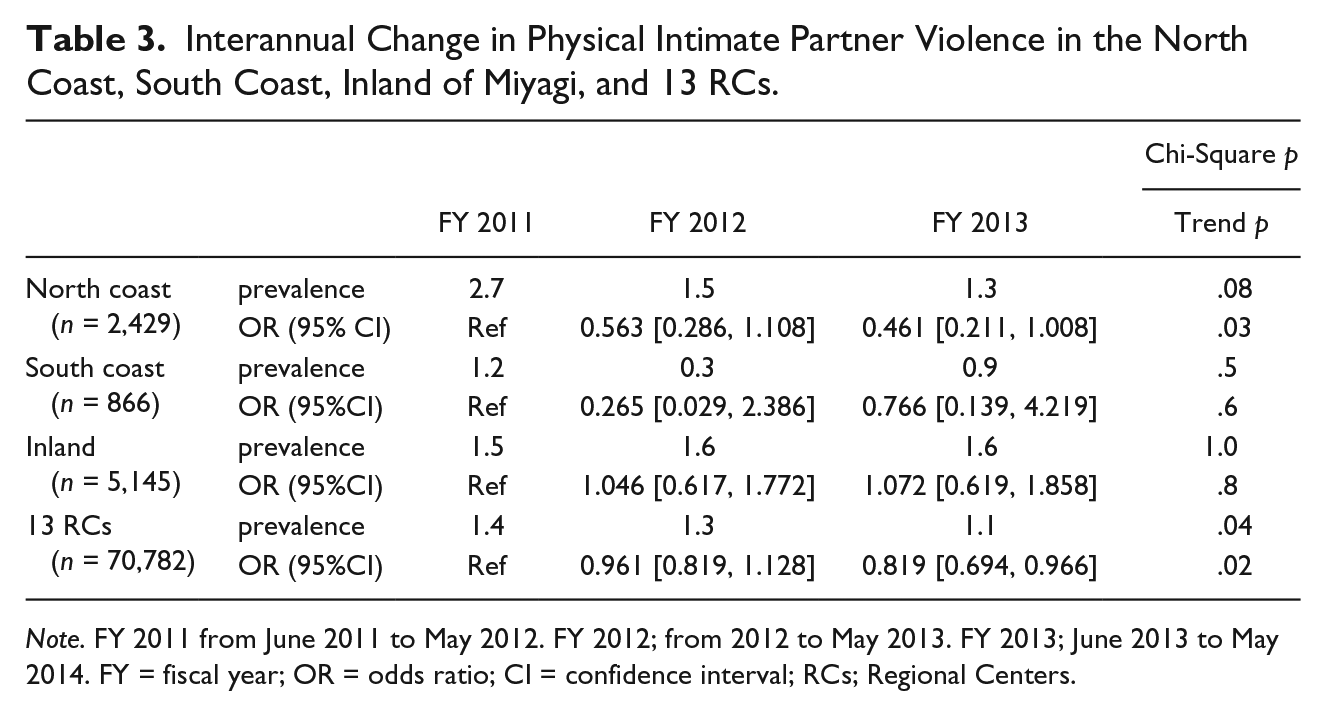
Note. FY 2011 from June 2011 to May 2012. FY 2012; from 2012 to May 2013. FY 2013; June 2013 to May 2014. FY = fiscal year; OR = odds ratio; CI = confidence interval; RCs; Regional Centers.
The proportion of pregnant women who answered that they experienced mental IPV during pregnancy significantly decreased over the years, after reaching a peak following the disaster, in the south coastal area of Miyagi: 19.4%, 13.1%, and 13.3% in FY 2011, FY 2012, and FY 2013, respectively (p = .05, trend p = .04). In contrast, there was no significant difference in the IPV incidence in the north coastal area of Miyagi: 15.8%, 14.9%, and 13.1% in FY 2011, FY 2012, and FY 2013, respectively (p = .3, trend p = .2).
The prevalence of physical IPV improved after reaching a peak level following the disaster in the north coastal area: 2.7%, 1.5%, and 1.3% in FY 2011, FY 2012, and FY 2013, respectively (p = .08, trend p = .03). In contrast, there was no significant difference in the south coastal area of Miyagi: 1.2%, 0.3%, and 0.9% in FY 2011, FY 2012, and FY 2013, respectively (p = .5, trend p = .6).
In the inland area, the prevalence of both physical and mental IPV was consistently higher than that in the 13 RCs after the disaster. Specifically, in the inland area, for mental IPV, the prevalence rates were 15.3%, 16.5%, and 15.7% (p = .6, trend p = .7), whereas for physical IPV, the rates were 1.5%, 1.6%, and 1.6% (p = 1.0, trend p = .8) in FY 2011, FY 2012, and FY 2013, respectively. In the 13 RCs, the prevalence of mental and physical IPV significantly decreased over the years. Specifically, for mental IPV, the prevalence rates were 13.8%, 13.8%, and 13.1% (p = .02, trend p = .02), whereas for physical IPV, the rates were 1.4%, 1.3%, and 1.1% (p = .04, trend p = .02) in FY 2011, FY 2012, and FY 2013, respectively.
The results of logistic regression analyses for pregnant women who experienced mental and physical IPV in the four target areas, with participating women in FY 2011 at the 13 RCs as a reference, are shown in Tables 4 and 5, respectively. In the univariate analysis, compared with participants at the 13 RCs in FY 2011, pregnant women in the south coastal area in FY 2011 had significantly higher odds of experiencing mental IPV (odds ratio [OR]: 1.501; 95% confidence interval [CI] = [1.142, 1.973]). Furthermore, pregnant women in the inland area in FY 2012 and FY 2013 had significantly higher odds of experiencing mental IPV compared with women at the 13 RCs in FY 2011 (OR: 1.227; 95% CI = [1.076, 1.339], and OR: 1.163; 95% CI = [1.006, 1.345]), respectively. However, the odds of experiencing mental IPV for women at the 13 RCs in FY 2013 were significantly lower than those in FY 2011 (OR: 0.937; 95% CI = [0.888, 0.989]).
Logistic Analysis for Pregnant Women With Mental Intimate Partner Violence in the North Coast, South Coast, Inland of Miyagi, and 13 RCs.
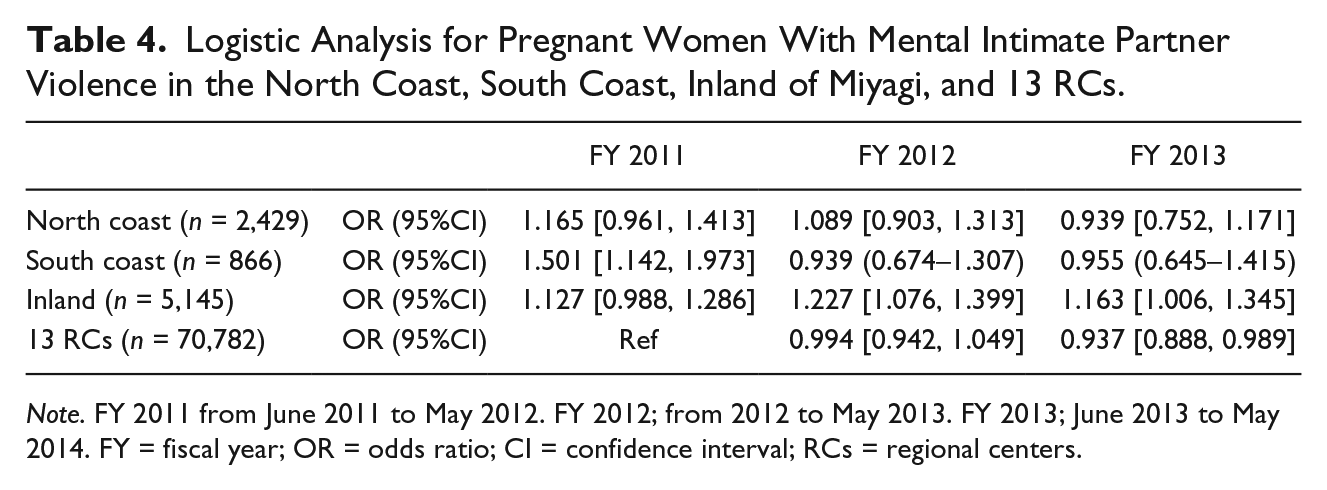
Note. FY 2011 from June 2011 to May 2012. FY 2012; from 2012 to May 2013. FY 2013; June 2013 to May 2014. FY = fiscal year; OR = odds ratio; CI = confidence interval; RCs = regional centers.
Logistic Analysis for Pregnant Women With Physical Intimate Partner Violence in the North Coast, South Coast, Inland of Miyagi, and 13 RCs.
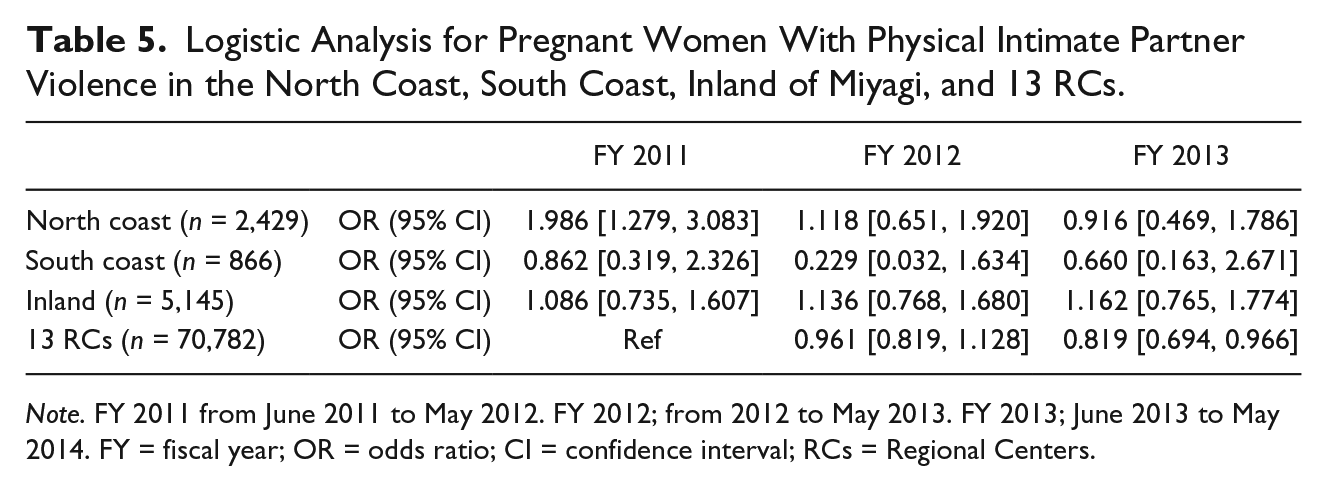
Note. FY 2011 from June 2011 to May 2012. FY 2012; from 2012 to May 2013. FY 2013; June 2013 to May 2014. FY = fiscal year; OR = odds ratio; CI = confidence interval; RCs = Regional Centers.
For physical IPV, pregnant women in the north coastal area in FY 2011 had significantly higher odds than did women at the 13 RCs in FY 2011 (OR: 1.986; 95% CI = [1.279, 3.083]). Meanwhile, the odds of experiencing physical IPV were significantly lower for women at the 13 RCs in FY 2013 than in FY 2011 (OR: 0.819; 95% CI = [0.694, 0.966]). In the present study, the age distribution of pregnant women in the 13 RCs was as follows: <25 years, 8.9%; 25 to 35 years, 62.5%; and ≥35 years, 28.5%. According to previous data from a Japanese nationwide survey in 2013, the age distribution of pregnant women was as follows: <25 years, 10.1%; 25 to 35 years, 62.9%; and ≥35 years, 26.9% (Ministry of Health, Labour and Welfare, 2013). Therefore, the 13 RCs might reflect the pattern of the general Japanese population not affected by disasters.
Discussion
The incidence of IPV against pregnant women worldwide has been reported to be in the range of 0.9% to 20.1% (Campbell, 2002), and this percentage is slightly higher than the rate in the general female population (Gazmararian et al., 1996). Anyone can become a victim of IPV. Previous studies have shown that mental stress after a disaster increases the incidence of violence by male partners (Anastario et al., 2009; Norris et al., 1999). Therefore, attention should be given to pregnant women, who might be especially vulnerable to IPV after major disasters.
In the JECS, it was not possible to compare the incidence of IPV before and after the March 2011 Great East Japan Earthquake due to a lack of pre-disaster data in the affected areas. According to a domestic IPV during pregnancy survey, IPV was experienced by 5% of pregnant women based on the Index of Spousal Abuse (Japanese ver.) and by 24% of women based on the Violence Against Women Screen (Kataoka, 2005). IPV consultations sent to the prefectural police in 2012 was around 30% higher than those in the previous year (Yoshihama et al., 2013). Based on this information, in the present study, it was assumed that the incidence of IPV increased immediately after the earthquake and then improved over the years in Miyagi Prefecture.
In the present survey, the prevalence of mental IPV during pregnancy was found to have significantly improved after reaching a peak level following the disaster over the study period in the south coastal area of Miyagi; the same was true of physical IPV in the north coastal area. However, in the inland area, the prevalence of mental and physical IPV remained consistently higher than that in the 13 RCs. Given that the prevalence of mental and physical IPV significantly decreased over the years in the 13 RCs, the sustained prevalence of IPV in the inland area is concerning.
One may suspect that after the Great East Japan Earthquake, the coastal areas of Miyagi received considerable support from both domestic and overseas sources, particularly in the search for missing people and reconstruction assistance. As a result, the disaster victims of these coastal areas might have received much more physical, environmental, and psychological support, which could have led to a reduction in IPV. By contrast, similar levels of support might not have reached the inland areas of Miyagi.
Anastario et al. (2009) documented increases in the incidence of IPV among people in the U.S. state of Mississippi, who were internally displaced by the 2005 Gulf Coast hurricane season. Based on the interannual changes in the present analysis, it is also possible that many pregnant women were evacuated from the coast to the inland areas, becoming isolated in the process.
Limitations
This study has several limitations. First, comparisons before and after the Great East Japan Earthquake were not possible because pre-disaster data were not available. Furthermore, the study targeted only those who had participated in the JECS, rather than covering all pregnant women living in the target areas. Second, the JECS created an original questionnaire for obtaining data, and standardized IPV screening scales such as the Violence Against Women Screen or Index of Spousal Abuse were not used (Sakurai et al., 2016). The use of an original questionnaire makes it difficult to compare the present findings with previous research. Third, this report merely describes the interannual changes in the prevalence of mental and physical IPV. Although there is a study on the risk and mediating factors of IPV (Schumacher et al., 2010), factors that might have affected IPV prevalence were not included in this study. Fourth, there is a possibility that the circumstances surrounding pregnant women change not only over time but also in different area groups. Despite these limitations, the present study is a unique report showing changes over time in the prevalence of IPV against pregnant women after a large-scale disaster. Disaster-affected areas need long-term support and follow-up to prevent IPV against women. This is also important because IPV is considered a risk factor for child abuse.
Conclusion
This study identified interannual changes in IPV against pregnant women in Miyagi after the Great East Japan Earthquake. The interannual changes in the incidence of mental and physical IPV significantly differed between the coastal and inland areas of Miyagi. The coastal areas of Miyagi showed a downward trend in the prevalence of mental and physical IPV. However, in the inland area, the prevalence of both mental and physical IPV was consistently higher than that in the 13 RCs after the disaster. After a large-scale disaster, IPV for pregnant women may increase in the affected areas. With this in mind, we need appropriate support and long-term follow-up from an early stage.
Footnotes
Acknowledgements
Members of the Japan Environment and Children’s Study (JECS) as of 2017 (principal investigator, Toshihiro Kawamoto): Hirohisa Saito (National Center for Child Health and Development, Tokyo, Japan), Reiko Kishi (Hokkaido University, Sapporo, Japan), Nobuo Yaegashi (Tohoku University, Sendai, Japan), Koichi Hashimoto (Fukushima Medical University, Fukushima, Japan), Chisato Mori (Chiba University, Chiba, Japan), Shuichi Ito (Yokohama City University, Yokohama, Japan), Zentaro Yamagata (University of Yamanashi, Chuo, Japan), Hidekuni Inadera (University of Toyama, Toyama, Japan), Michihiro Kamijima (Nagoya City University, Nagoya, Japan), Takeo Nakayama (Kyoto University, Kyoto, Japan), Hiroyasu Iso (Osaka University, Suita, Japan), Masayuki Shima (Hyogo College of Medicine, Nishinomiya, Japan), Yasuaki Hirooka (Tottori University, Yonago, Japan), Narufumi Suganuma (Kochi University, Nankoku, Japan), Koichi Kusuhara (University of Occupational and Environmental Health, Kitakyushu, Japan), and Takahiko Katoh (Kumamoto University, Kumamoto, Japan).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Japan Environment and Children’s Study was funded by the Ministry of the Environment in the Government of Japan. The conclusions of this article do not reflect the administration’s views.