
Abstract
Research suggests that Hispanic youth with intimate partner violence (IPV) exposure report fewer trauma symptoms compared with youth from other racial/ethnic groups. However, no study has examined possible explanations for this finding. Our objective was to study the association between acculturation, IPV, and post-traumatic stress (PTS) symptoms among Hispanic youth and to test whether acculturation moderates the relationship between IPV and PTS symptoms. This analysis used data from 271 Hispanic youth aged 8 years or older participating in the second cohort of the National Survey of Child and Adolescent Well-being (NSCAW II). We conducted multiple linear regression analyses to achieve our study aims. We did not find a statistically significant relationship between IPV exposure and PTS symptoms among Hispanic youth (B = 0.21, 95% confidence interval [CI] = [−0.09, 0.52]), or that acculturation moderated this relationship (B = 0.04, 95% CI = [−0.23, 0.32]). However, we found a significant relationship between PTS symptoms and acculturation level. Specifically, higher levels of acculturation were associated with more reports of PTS symptoms (B = 1.03, 95% CI = [0.13, 1.93]). These study results highlight the need to consider the role of acculturation when working with Hispanic youth involved with child welfare.
Keywords
Introduction
Decades of rigorous research has shown deleterious effects of childhood exposure to intimate partner violence (IPV), including a heightened risk of experiencing post-traumatic stress (PTS) and developing post-traumatic stress disorder (PTSD; Chemtob & Carlson, 2004; Graham-Bermann, Castor, Miller-Graff, & Howell, 2012; Kulkarni, Graham-Bermann, Rauch, & Seng, 2011). Children involved with child welfare who have been exposed to IPV may exhibit higher rates of PTSD than children in the general population (Campbell, Thomas, Cook, & Keenan, 2013; Kolko et al., 2010). However, the same may not be true for Hispanic 1 children involved with child welfare who, despite having high rates of poverty and low access to health care, have cultural protective factors that are associated with relatively good child health profiles (Drake et al., 2011). This paradox, termed the “Hispanic Paradox” in the health literature, may be useful in understanding the effects of IPV on Hispanic children’s risk of PTSD; however, few child welfare studies have examined this relationship, and there is no investigation of how this relationship may be influenced by acculturation.
The Hispanic paradox may be used to understand the influence of acculturation on the risk of PTSD among Hispanic children exposed to IPV. Acculturation is defined as a process of social, psychological, and cultural change that results from having contact with a new host culture (Schwartz, Unger, Zamboanga, & Szapocznik, 2010). There is literature that suggests acculturation is significantly associated with various health outcomes in Hispanic children and families and that the process of acculturation may impact both their social and psychological well-being (Altschul & Lee, 2011; Kataoka et al., 2009; Schwartz et al., 2010). Similarly, acculturative stress theory suggests that the process of adapting to a new host culture may cause stress, resulting in negative mental health outcomes (Conway, Swendsen, Dierker, Canino, & Merikangas, 2007).
This study examined the relationship between acculturation and PTS symptoms, and whether acculturation moderates the effects of IPV on PTS symptoms using a framework of acculturative stress theory. The results of this study may aid in the development of interventions aimed at reducing the risk of PTS symptoms among Hispanic youth involved with child welfare and exposed to IPV.
Racial/Ethnic Differences in Trauma Symptoms Among Children Exposed to IPV
Studies examining how race/ethnicity influences the relationship between IPV exposure and PTS symptoms among children have reported mixed findings. For instance, in their study examining the relationship between IPV exposure and PTSD symptoms among a community-based sample of 137 children of four different racial–ethnic groups, Koolick and colleagues (2016) found no ethnoracial group differences in the prevalence of PTSD symptoms. However, other researchers have found that racial/ethnic minority children may adjust better than non-Hispanic White children to IPV exposure (Costello & Klein, 2019; McDonald et al., 2016). For example, Costello and Klein (2019) found that race/ethnicity moderates the relationship between childhood exposure to IPV and trauma symptoms. In their study using a child welfare sample, findings indicated that Hispanic children exhibited fewer trauma symptoms than White children as IPV exposure became more frequent. They also found differential predictors of trauma symptoms in children by race/ethnicity. Specifically, they discovered that caregiver depression predicted trauma symptoms in White and African American children, whereas neighborhood quality predicted Hispanic children’s trauma (Costello & Klein, 2019).
A separate study examining differential effects of childhood exposure to IPV among a nationally representative household sample identified three latent classes of psychopathology: (a) asymptomatic, (b) maladjusted, and (c) highly maladjusted (McDonald et al., 2016). This study found that Latino children were more likely to be in the asymptomatic class compared to White non-Latino, multi-ethnic/racial, and other racial/ethnic minority children. Despite this evidence that suggests Hispanic/Latino children may fare better than White and other racial/ethnic minority children when faced with IPV, there is limited knowledge regarding youth resilience in the context of acculturation and whether acculturation is associated with PTS symptoms in child-welfare-involved Hispanic youth with IPV exposure. Furthermore, considering the inconclusive findings, additional research is needed to further understand the relationship between IPV and PTS symptoms among Hispanic youth.
Acculturation in Hispanic Families
Examining the role of acculturation in how Hispanic youth adjust to their IPV exposure is critical in research examining Hispanic functioning among children with child welfare contact. Aside from the fact that the Hispanic population is the nation’s largest ethnic minority group and is projected to continue growing (Colby & Ortman, 2015), 36% of Hispanics living in the United States are immigrants (Motel & Patten, 2013) and another 39% are first-generation Americans (Second Generation Americans, 2013). Furthermore, there has been a rise in Hispanic immigrant families referred to child welfare services (Dettlaff, Earner, & Phillips, 2009; Dettlaff & Johnson, 2011).
Acculturation is the process of adaptation into a host culture (Mena, Padilla, & Maldonado, 1987) and a salient factor in understanding childhood adjustment to IPV exposure (Costello & Klein, 2019; Dettlaff & Johnson, 2011; Kimber et al., 2015; Millett, Seay, & Kohl, 2015). Although substantial attention has been devoted to the effects of acculturation on health and mental health outcomes, the findings are mixed (DiGangi, Goddard, Miller, Leon, & Jason, 2016). Some research has demonstrated that higher levels of acculturation (i.e., greater adoption of U.S. cultural norms) lead to adverse physical and psychological health outcomes (Acevedo, 2000; Espino & Maldonado, 1990; Ortega, Rosenheck, Alegria, & Desai, 2000; Vega, Scribney, Achara-Abrahams, 2003), whereas other studies have shown that lower levels of acculturation have harmful health effects (Escobar et al., 1986; Miranda, Estrada, Firpo-Jimenez, 2000; Rogler, Cortes, & Malgady, 1991). Regarding the relationship between acculturation and IPV, a recent meta-analysis of 21 studies revealed that studies often found a significant positive correlation between acculturation and reports of IPV (Alvarez, Ramirez, Frietze, Field, & Zarate, 2018).
Two indicators frequently used as proxies of acculturation when an acculturation scale is not available are nativity and language preference (Alvarez et al., 2018). Researchers studying Hispanic samples have found that these measures are associated with adoption of host cultural practices, an index of acculturation (Schwartz, Pantin, Sullivan, Prado, & Szapocznik, 2006). Although not limited to child welfare populations, researchers have examined the association between language and PTSD symptoms among Latino children. Kataoka et al. (2009) surveyed 1,601 Latino children from seven middle schools in Los Angeles and found that children with higher English fluency reported greater exposure to community violence and PTSD symptoms than those with lower English fluency. This finding suggests that acculturation may be a risk factor for PTS symptoms among Latino children and that there are stressful aspects of acculturation. However, whether this may be true for Latino children involved with child welfare is unclear. We are unaware of any child welfare studies that have examined differences in PTS symptoms among Hispanic youth based on nativity and language.
Acculturative Stress Theory
Acculturative stress theory can be used to understand the role of acculturation in Hispanics’ mental health, including PTS symptoms. This theory suggests that the migration process involves cultural, social–economic, and personal challenges and changes that influence mental health outcomes depending on the level of stress experienced (Conway et al., 2007). Moreover, the acculturation process may negatively affect protective factors of traditional Hispanic culture, such as close relationships with extended family members that may buffer the influences of stress and prevent the development of psychopathology (De la Rosa, 2002). Thus, although IPV can have harmful effects on a child’s emotional well-being, how Hispanic youth adjust to their IPV exposure may vary by level of acculturation. However, whether this is true for Hispanic youth involved with child welfare remains uncertain.
Risk and Protective Factors for PTS Symptoms Among Youth Involved With Child Welfare
Researchers have found that additional factors outside of acculturation may impact the mental health effects of IPV exposure in children. A study using a nationally representative sample of children and adolescents referred to child welfare services found that PTS symptoms were higher in children placed in out-of-home care than those maintained in the home (Kolko et al., 2010). This study also found that child age, abuse by a nonbiological parent, violence in the home, and child depression contributed to elevated PTS symptoms in children (Kolko et al., 2010). In addition, Graham-Bermann, DeVoe, Mattis, Lynch, and Thomas (2006) found that family income and the amount of violence witnessed heightened the harmful effects of IPV exposure. Therefore, when possible, we accounted for the potential impact of these variables on youths’ PTS symptoms in the current analyses.
This Study
This study sought to answer the following research questions using a national sample of Hispanic youth with child welfare contact:
This study adds to the nascent literature examining the relationship between IPV and PTS among Hispanic youth involved with child welfare. As indicated in Figure 1 which is based on the prior discussed research and acculturative stress theory, we hypothesized the following:
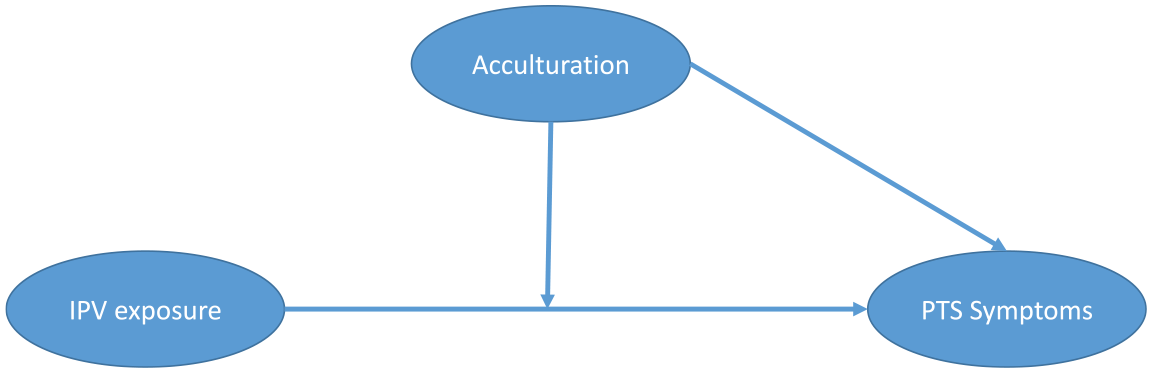
Conceptual model for (a) the moderating effect of acculturation on the relationship between IPV exposure and PTS symptoms and (b) the direct effect of acculturation on PTS symptoms among Hispanic youth aged 8 years or older involved with child welfare.
Method
We used data from the second cohort of the National Survey of Child and Adolescent Well-Being (NSCAW II). The NSCAW II includes a nationally representative sample of children who lived in the United States and were subject of a child abuse or neglect investigation between February 2008 and April 2009. Data were collected during three time points (baseline, 18-month follow-up, and 36-month follow-up) from multiple respondents, including caregivers, teachers, child welfare caseworkers, and children/youth. This study only used data collected from youth, caregivers, and caseworkers at baseline.
NSCAW II used a two-stage stratified sampling design, in which the first stage involved sampling of primary sampling units (PSUs), typically defined as a county. The PSUs included 81 counties in 30 states. Eight states were excluded because of legislation that required child welfare workers to make the first contact with the caregiver of a child, and not an NSCAW II Field Representative. The second stage of sampling entailed randomly selecting children from the PSUs. Excluded from this random sample were children older than 17.5 years, children whose sibling was already involved with the study, children identified as the alleged perpetrator in the child abuse investigation, and children with multiple maltreatment investigations during the study period. Furthermore, the NSCAW II oversampled infants and children placed in out-of-home care to ensure a large enough sample size for sufficient statistical power to understand these vulnerable groups. NSCAW II statisticians created weights to account for the differential selection probabilities and help produce statistics with unbiased and nationally representative estimates. Additional information regarding NSCAW II sampling procedures and methods is available elsewhere (e.g., Dowd et al., 2012).
Analytic Sample
NSCAW II included 5,872 children aged 0 to 17.5 years. The PTS subscale of the Trauma Symptom Checklist for Children (TSCC; Briere, 1996), which measured PTS in the study, was administered to children aged 8 years or older. Therefore, this study was limited to data related to youth aged 8 years or older. Furthermore, given this study’s focus, we only included youth in our sample who were (a) Hispanic and either (b) regularly spoke English, Spanish, or both English and Spanish in the home.
Based on these inclusion criteria, this study was limited to data related to 406 Hispanic youth aged 8 years or older. Of these youth, 135 had missing data on key variables. We defined youth with missing data as a subpopulation and gave them a weight set to zero. We used this subpopulation analytic technique to ensure the NSCAW II sampling weights produced unbiased estimates that we could use to make accurate inferences based on the subpopulation of the 271 youth with complete data included in the final analysis. Furthermore, this estimation technique allowed us to take into account the NSCAW II sampling design (Bell, Kromrey, & Ferron, 2009; West, Berglund, & Heeringa, 2008). We elected to use subpopulation analysis rather than a missing data imputation approach to account for missing data, given that the NSCAW II data are already weighted to account for nonresponse. Findings from a Monte Carlo study conducted by Bell et al. (2009) showed that the subpopulation analysis differs from listwise deletion and performing this analytic technique on complex sample survey data (e.g., NSCAW II data) does not lead to incorrect inferences. Therefore, this approach is suitable for handling missing data.
Measures
Dependent variable: PTS symptoms
The PTS subscale of the TSCC was used to assess how frequently youth experienced PTS symptoms. The TSCC was developed for use with racially and economically diverse groups of children from urban and rural settings (Briere, 1996) and has been proven valid and reliable for children from a variety of cultures (Nilsson, Wadsby, & Svedin, 2008).
The PTS subscale consists of 10 items. Examples of PTS symptoms measured include “bad dreams or nightmares,” “can’t stop thinking about something bad that happened to me,” and “feeling like you were outside of your body.” Response options range from 0 (never) to 3 (almost all of the time). We calculated a total score for each participant by summing responses, with higher scores indicating more frequent PTS symptoms. Raw scores were used in the analytic models; however, we reported age- and gender-standardized T scores for descriptive purposes to indicate clinically significant trauma. T scores of 65 or higher are indicative of clinically significant trauma symptoms (Briere, 1996). The internal consistency reliability of the TSCC in this study was high (α = .99).
Independent variables
Our primary independent variables included measures of acculturation and exposure to IPV.
Acculturation
We included measures of parent nativity and whether Spanish is spoken regularly at home as proxies for measures of acculturation among Hispanic youth. We classified children as living in a household that is more or less acculturated by summing the following two items: parent nativity (0 = foreign-born, 1 = US-born) and language regularly spoken at home (0 = Spanish, 1 = English). We treated these two items like a scale rather than separate variables, given that there are large variations in how people acculturate (Sam & Berry, 2010; Schwartz et al., 2010). Thus, treating these items like a scale allowed us to capture potential variations in levels of acculturation the best way possible using the NSCAW II data. Children with lower scores were considered less acculturated, whereas children with higher scores were considered more acculturated. Internal consistency of the scale in this study was good (α = .70).
Exposure to IPV
We used the 13-item witnessing violence subscale of the Violence Exposure Scale for Children (VEX-R; Fox & Leavitt, 1995) to measure youth’s exposure to IPV events in the home. This subscale includes items that measure both mild and severe forms of violence in the home and are assessed using cards in a cartoon format. Examples of questions in this scale include “How many times have you seen an adult yell at another person in a home you’ve lived in?” and “How many times have you seen a person point a knife or a real gun at another person in a home you’ve lived in?” Response options range from 0 (never) to 3 (lots of times). Frequency scores were heavily skewed. For analysis purposes, we dichotomized each VEX-R item as 0 if youth responded “never” and 1 if youth responded otherwise. We then calculated the score by summing participants’ dichotomized score, with higher scores indicating greater exposure to mild/severe violence in the home. Internal consistency for VEX-R in NSCAW II is high, as indicated by Cronbach’s alpha ranging from .86 to .96 (National Data Archive on Child Abuse and Neglect, 2014). Furthermore, researchers have proven the VEX-R valid showing moderate significant correlations with children’s total reported distress symptoms (Shahinfar, Fox, & Leavitt, 2000).
Control variables
The following variables were included as controls in the study analysis based on empirical evidence that suggests they are important correlates of PTS symptoms among children involved with child welfare (Kolko et al., 2010): youth gender, youth race/ethnicity, basic needs met, youth depressive symptoms, alleged child maltreatment type, placement status, and harm level.
Basic needs met
We measured basic needs using a risk assessment completed by caseworkers. The NSCAW II team developed this risk assessment to understand how safe children were in their current environment. In other words, how likely children were to incur maltreatment in the future. As part of the risk assessment, caseworkers were asked the following yes or no question regarding youths’ basic needs: “At the time of the investigation, did the family have trouble paying for basic necessities such as food, shelter, clothing, electricity, or heat?”
Youth depressive symptoms
The Children’s Depression Inventory (CDI; Kovacs, 1992) was used to measure a range of depressive symptoms as indicated by five factors: Negative Mood, Interpersonal Problems, Ineffectiveness, Anhedonia, and Negative Self-Esteem. Using the 27-item CDI, NSCAW II interviewers asked youth about their engagement in certain activities and their thoughts and feelings (e.g., sad, enjoy being around other people) over the past 2 weeks. Responses were scored using a three-point Likert-type scale (ranging from 0 to 2) and varied depending on the question. The NSCAW II created raw scores by summing each item, with higher scores indicating greater presence of depressive symptoms, and converted raw scores to T scores using the lookup tables in the CDI user manual. For analysis purposes, we used T scores. We analyzed data based on youth’s overall scores rather than scores on each subscale, given research findings that suggest the CDI subscales are not robust (alpha ranged from .59 to .68; Kovacs, 1992). However, in the NSCAW II sample, internal consistency for the overall CDI is good, averaging .81 for 7- to 12-year-olds and .87 for 13- to 15-year-olds (National Data Archive on Child Abuse and Neglect, 2014). In addition, studies (cited in Kovacs, 1992) have established concurrent validity comparing the CDI to other well-known scales such as the Coopersmith Self-Esteem Inventory (α = −.72 for girls and −.67 for boys) and the Center for Epidemiological Studies Depression Scale (α = .44).
Alleged child maltreatment type
The NSCAW II interviewers asked caseworkers to identify the most severe type of child maltreatment they believed led to the child’s involvement with child welfare. Interviews were structured using the Modified Maltreatment Classification System (MMCS; English & The LONGSCAN Investigators, 1997), an instrument that asks specific questions about the nature of alleged abuse and/or neglect. The caseworker reported on all types of child maltreatment in the case report. After recording all child maltreatment types, caseworkers used the MMCS to help determine which maltreatment they perceived as the most serious type.
Placement status
We categorized youth as being in out-of-home care or in-home care. Youth in out-of-home care were youth who resided in kinship care, foster care, group homes/residential programs, or “other” type of out-of-home arrangement. Conversely, youth living in home care resided either in-home with their biological parent(s) or in-home with their adoptive parent(s).
Harm level
NSCAW II collected information regarding caseworkers’ perceptions of the level of harm the alleged child maltreatment caused the child, regardless of whether or not the report was substantiated. Caseworkers rated their perceived severity of harm to the child as either none, mild, moderate, or severe.
Statistical Approach
We conducted analyses using Stata 13.1 statistical software program. The first analysis step involved conducting descriptive statistics to summarize sample characteristics. Second, we conducted linear regression analyses to examine whether IPV and acculturation were associated with PTS symptoms, adjusting for control variables. Last, to understand whether acculturation moderates the relationship between IPV and PTS symptoms, we added an interaction term exploring the synergistic effect of combined IPV and acculturation to our linear regression model.
We conducted all analyses using the “svyset” command. This command was used to set up the survey data in a manner that provided Stata with information regarding the sampling design, including the stratum, sampling weight, and PSU variables. Then we used the svy: prefix before each analysis command so that Stata remembers the survey setup of the dataset and applies it during the analysis. By default, the svy command in Stata uses the Taylor series linearization method for estimating standard errors (StataCorp, 2013). Using this variance estimation technique produced statistics that allowed for unbiased estimates.
Results
Sample Description
Table 1 presents the sample characteristics of the 271 Hispanic youth included in the analytic sample. On average, youth were 11.85 (SE = 0.26) years old, and slightly more than half (55.86%) were female. Regarding primary child maltreatment report, the majority reported was neglect related to lack of supervision (28.53%) and physical abuse (20.75%). Furthermore, approximately half the sample had a caseworker who determined the risk of harm as either mild (33.43%) or moderate/severe (16.71%); the majority of the sample were resided in in-home care (86.95%). Caseworkers identified 22.44% of the youth as being in a family that had difficulty paying for basic needs. The mean depressive symptom score was 51.58 (SE = 1.28, range = 34-96), and the average PTS symptom score was 50.73 (SE = 1.43, range = 33-89). On average, youth witnessed or were direct victims of 5.10 (SE = 0.37, range = 0-18) instances of mild or severe IPV in the home. Acculturation scores ranged from 0 to 2, with the average being 0.92 (SE = 0.09).
Weighted Sample Characteristics of Hispanic Youth (n = 271).
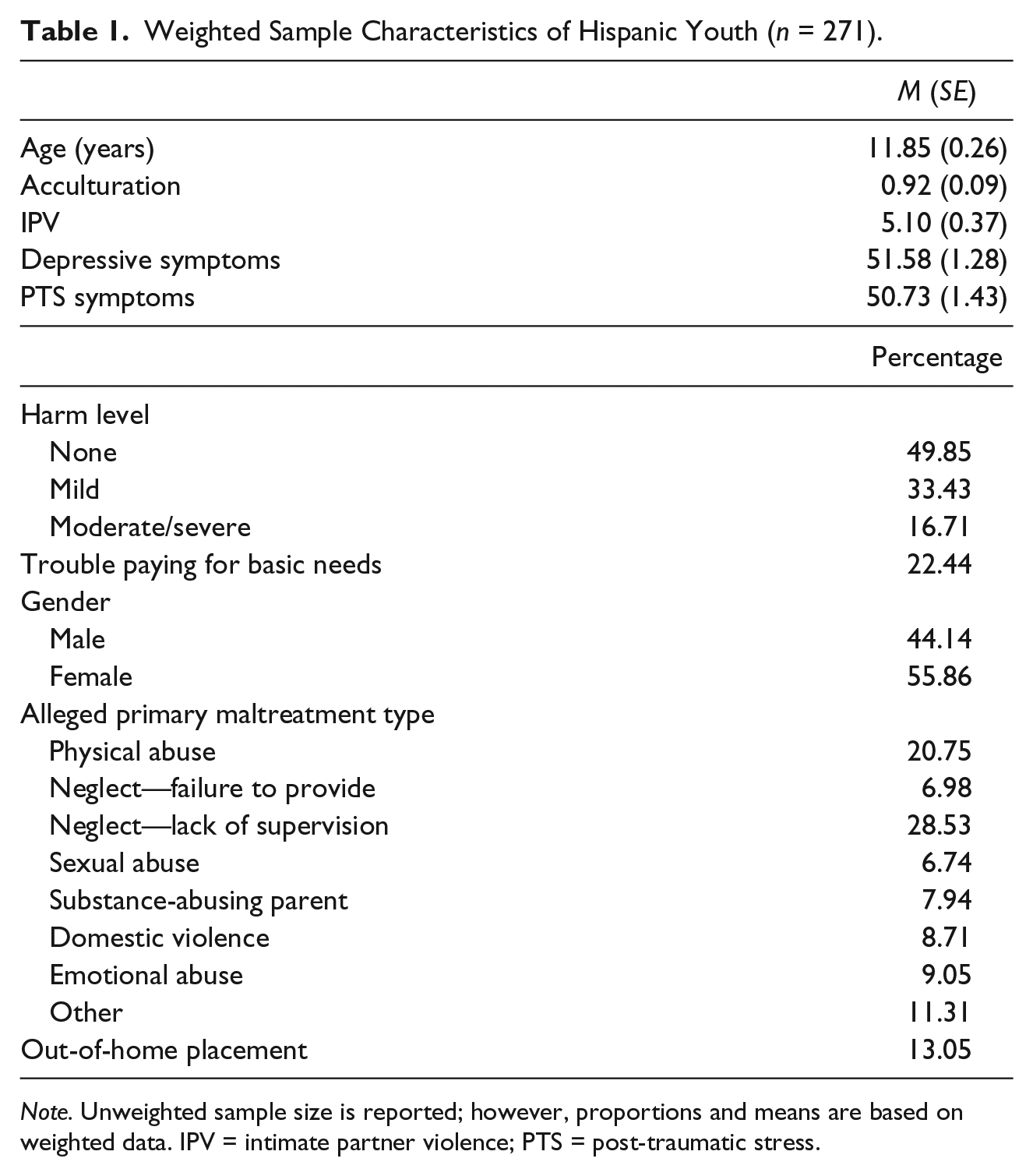
Note. Unweighted sample size is reported; however, proportions and means are based on weighted data. IPV = intimate partner violence; PTS = post-traumatic stress.
Multivariate Analyses Predicting Increased Risk of PTS Symptoms
Table 2 presents the results of the regression model showing the relationship between IPV and acculturation and PTS symptoms. Estimates are adjusted for all variables in the model. Findings showed that acculturation level was significantly associated with PTS symptoms. Explicitly, youth with higher levels of acculturation reported higher levels of PTS symptoms (B = 1.03, 95% confidence interval [CI] = [0.13, 1.93]). We also found that youth with reports of mild harm reported lower levels of PTS symptoms than youth with no harm (B = −2.23, 95% CI = [−4.25, −0.21]). Similarly, youth with reports of neglect/lack of supervision (B = −3.72, 95% CI = [−5.64, −1.79]), substance-abusing parent (B = −3.94, 95% CI = [−6.16, −1.71]), and emotional abuse (B = −369, 95% CI = [−7.26, −0.11]) as alleged primary maltreatment types had lower levels of PTS symptoms than youth with physical abuse reported as the primary maltreatment type.
Multiple Linear Regression Predicting PTS Symptoms Among Hispanic Youth (n = 271).
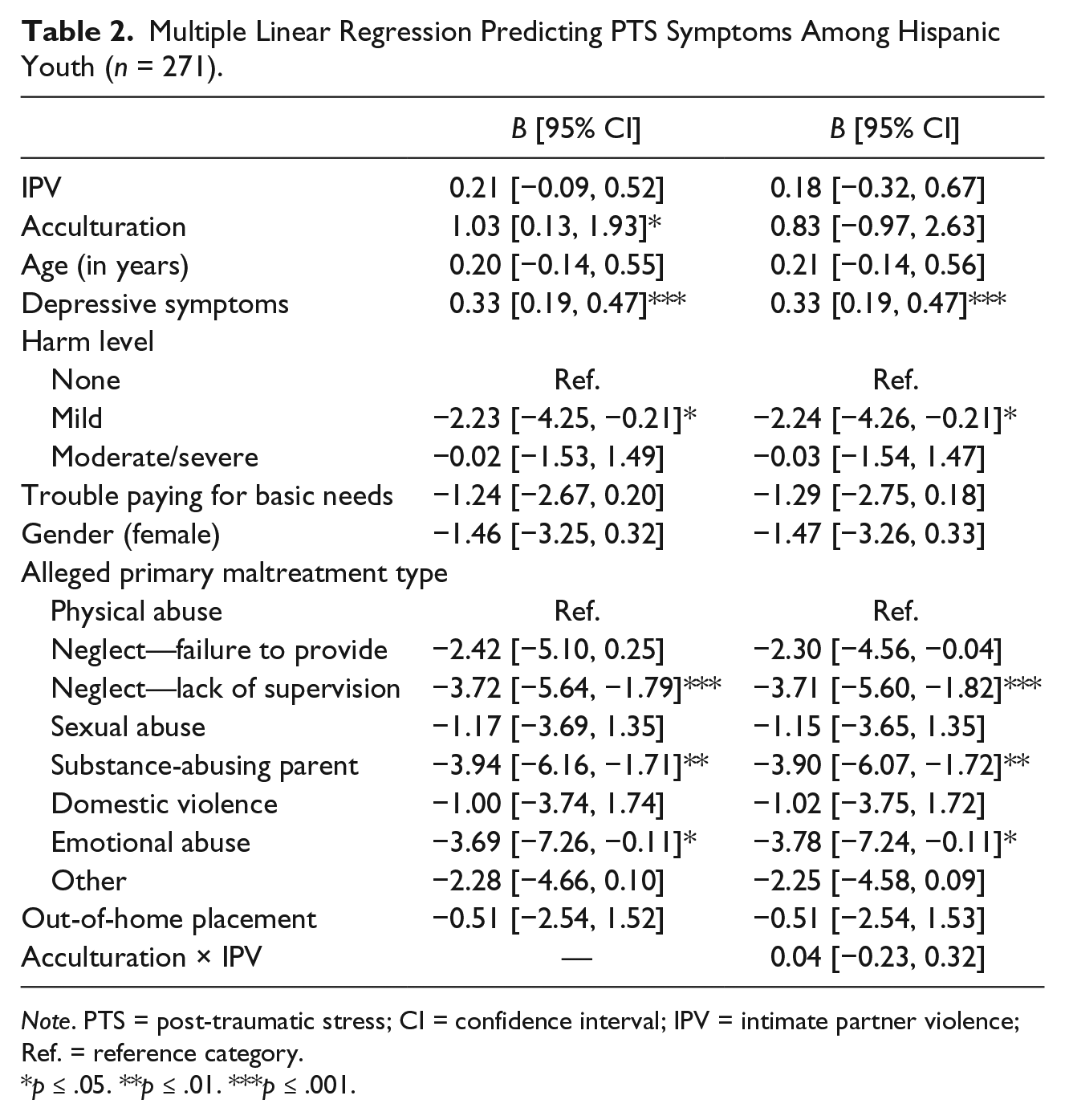
Note. PTS = post-traumatic stress; CI = confidence interval; IPV = intimate partner violence; Ref. = reference category.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
We did not find a significant association between IPV exposure and PTS symptoms (B = 0.21, 95% CI = [−0.09, 0.52]). In addition, the relationship between IPV exposure and PTS symptoms did not vary by acculturation level (B = 0.04, 95% CI = [−0.23, 0.34]).
Discussion
This study examined how IPV and acculturation are associated with PTS symptoms in Hispanic youth with child welfare contact. Findings from this study extend prior child welfare studies of PTS symptoms; however, this novel study is the first to document differences in PTS symptoms among Hispanic youth involved with child welfare by acculturation level. Different from prior child welfare research (Fusco & Cahalane, 2013; Lieberman, Chu, Van Horn, & Harris, 2011) and negating our first hypothesis, we did not find a significant association between IPV exposure and PTS symptoms among Hispanic youth. The lack of support for our first hypothesis is likely due to our sample being entirely Hispanic. Prior research studying the impact of IPV on PTS symptoms among Hispanic/Latino children compared to White children indicates that Hispanic children exhibit lower levels of PTS symptoms (Costello & Klein, 2019; McDonald et al., 2016). Therefore, factors other than IPV may be stronger predictors of PTS among Hispanic youth involved with child welfare. For example, our study findings suggest that depressive symptoms, abuse type, harm level, and acculturation may be more significant indicators of PTS symptoms than IPV among Hispanic youth involved with child welfare.
Similar to existing research (e.g., Castro et al., 2017), we found that youth with reports of physical abuse as the primary form of child maltreatment had higher rates of PTS symptoms compared to youth with other types of child maltreatment. However, contrary to prior research (e.g., Kataoka et al., 2009), we found that youth with child welfare reports of mild levels of threatened harm reported lower levels of PTS than youth with reports of no harm. This finding may have been a result of perception bias, as harm level was determined by the caseworkers’ perception of whether or not a report of child maltreatment was substantiated. We recommend that future research use a more objective measure of harm level.
We also found a significant association between acculturation and PTS symptoms, supporting our second study hypothesis that Hispanic youth with higher levels of acculturation will report higher PTS symptoms than Hispanic youth with lower levels of acculturation. However, contrary to our third hypothesis, acculturation level did not moderate the relationship between IPV and PTS symptoms among Hispanic youth. This result may be related to us finding no statistically significant direct effect between IPV and PTS symptoms. Despite this insignificant finding, our finding indicating that acculturation was significantly associated with PTS symptoms may be reflective of the Hispanic paradox that proposes immigrant families may hold on to protective cultural factors, like their native language and native identity that are associated with good child health outcomes (Gonzalez-Burchard, 2005). Thus, highlighting the need to design interventions that incorporate language spoken at home and native origin in a way that is attuned with the culture of Hispanic immigrant families.
It is also important for child welfare providers to consider the potential effects of acculturation on family functioning and PTS symptoms in Hispanic children. The stress of acculturation may be an added burden on children and families. Although this study did not measure for acculturative stress or biculturalism, we suspect that these concepts may also be essential aspects of Hispanic culture in the United States within the context of acculturation. We recommend that future studies with child welfare populations include measures of acculturative stress and biculturalism to further understand their role in family functioning and PTS symptoms in children. Furthermore, as we start to see an increment of children remaining in the home following child maltreatment investigations as a result of the Family First Prevention Services Act (FFPSA; Brown, 2018), service providers may also consider the role of specific cultural constructs like familismo (family attachments) and confianza (trusting relationships and reciprocity) when engaging Hispanic families in services (Ayón & Aisenberg, 2010).
Limitations
Although this study highlights some of the cultural implications to consider when working with Hispanic families referred to child welfare, there are a couple of limitations to this study that should be noted. First, we relied on self-reported data. Therefore, although researchers have deemed the PTS subscale of the TSCC a valid and reliable measure with children from a variety of cultures, reports of PTS are subjective to interpretation. Furthermore, there could be response bias producing potential underreporting of IPV and PTS symptoms due to fear of consequences linked to child welfare involvement (e.g., being removed and placed into foster care).
Relatedly, we may have excluded children with the most severe IPV exposure or PTS symptoms from our sample due to missing data. Thus, study results may not generalize to some of the most marginalized families involved with child welfare. However, given the complex sampling design, our use of subpopulation analysis to handle missing data offers the best estimates available for this highly vulnerable population. Using another method to impute missing data based on estimates that are already weighted may have produced inaccurate and nonreplicable parameter estimates. We encourage future research using a larger sample. In addition, doing so may increase statistical power for detecting the hypotheses proposed in this study.
Second, we recommend replication of this study using a standardized acculturation measure, such as the Bicultural Involvement Questionnaire (BIQ; Szapocznik, Kurtines, & Fernandez, 1980) to provide a more valid and comprehensive measure of acculturation. However, given the mixed findings around the effects of acculturation on physical and mental health outcomes, and the lack of consensus on the most effective standardized measure of acculturation, we used the two most widely used proxy measures of acculturation. In addition, this is the first study that we are aware of to assess the relationship between acculturation and PTS symptoms using a child welfare sample. Thus, our study findings add to a knowledge base that is sorely lacking.
Finally, because the data used in this study were collected between 2008 and 2009, caution should be taken when interpreting the results. There may have been changes in child welfare policy and practice that have led to improved outcomes for more acculturated Hispanic youth. Nevertheless, children and families with child welfare contact face similar risks today than they did 10 years ago. Therefore, the findings of this study are still relevant.
Conclusion
In spite of the study limitations, our results may have important implications for child welfare policy, practice, and further research. Our results highlight the need for services that are more attuned to the culture of Hispanic immigrant families and elucidate some of the potential factors that may mitigate the risk of poor mental health outcomes in Hispanic youth exposed to IPV. Furthermore, our results bring to light the role of acculturation in understanding the risk of PTS symptoms among Hispanic youth referred to child welfare services. It appears that acculturation may be associated with adverse mental health outcomes in Hispanic youth with child welfare contact, including PTS symptoms. We recommend additional research to examine different aspects of acculturation, including the role of acculturative stress and biculturalism, to better understand its impact on mental health outcomes in Hispanic families referred to child welfare services.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.