
Abstract
This study aimed to gain insight into factors that have an impact on Syrian abused refugee women’s decision for seeking professional help regarding intimate partner violence (IPV) against them. This study attempted to answer the following question; what are the reasons for not seeking professional help by victims of IPV among refugee women? The qualitative method was used with semi-structured interviews in an accessible sample of 30 abused refugee women, who were identified by cooperated local community organizations working with the refugee. Five reasons emerged from the interviews affecting seeking help behaviors for refugee women: misconceptions about IPV problem; difficulties to access and approach different care centers; lack of awareness about the negative consequences of IPV; unaware, negative expectations, negative experiences, and incorrect thoughts about IPV’s services; and psychological and physical health difficulties. The authors suggested some recommendations in light of this study results. Raising awareness activities toward the negative impact of violence on women’s and children well-being, improving service availability, building professional capacities to work with abused women, and providing professional services for depressed and amputee’s refugee women.
Intimate partner violence (IPV) occurs when a person who is currently or previously in an intimate relationship uses violent behavior, abusive actions, threatening or harassing acts as a means to physically, psychologically, sexually or financially coerce, dominate and control the other member of the personal intimate relationship (Holtmann & Rickards, 2018). The prevention and management of IPV are highly relevant and critical for all governmental and nongovernmental institutions. It involves ethical, social, economic, humanitarian, legal, and medical aspects.
In 2013, violence occurring within families accounted for 11% of all reported and unreported crimes. For example, the U.S. Department of Justice (2005) reported that 3.5 million crimes were committed by one family member against other, where 49% being against spouses, and 38% of all murders of women are committed by intimate partners (WHO, 2013).
Women with difficult living situations (e.g., local culture that supports women’s discipline, lack of protection legislation, living in exile, refugee) are more vulnerable to be victims of violence by husbands or other family members than other women (Menjivar & Salcido, 2002). The prevalence of violence against refugee women (VARW) or immigrant women in the host countries is exceeding its rates in women’s original countries (Kulwicki et al., 2010). Women might suffer more from violence in the host countries as a result of losing their supportive resources, such as their own families and supportive systems (Menjivar & Salcido, 2002).
VARW appears to be an especially complicated problem among immigrant families and it was known to claim more lives among minorities than the modern communities (Abu-Ras, 2007; Hammoury et al., 2009; Khawaja & Barazi, 2005). VARW has not been sufficiently explored in previous studies (Al-Shdayfat, 2017; Menjivar & Salcido, 2002). Nonetheless, various selected small-sampled studies had revealed that women who are from Asian and African backgrounds and living in exile were frequently experiencing IPV (Thapa-Oli et al., 2009). A remarkable prevalence of physical and psychological VARW has been reported by some studies in the Middle East and North Africa region, the United States, and Europe (Al-Shdayfat, 2017; Zakar et al., 2012). For example, Raj and Silverman (2002) demonstrated that 30% to 50% of immigrant women have been sexually or physically abused by a male intimate partner.
Violence against women is a complicated issue not only because it disrupts every aspect of the victim’s mental health and well-being but also because of the many limitations and obstacles that woman has to overcome to ask help to eliminate violence (Kulwicki et al., 2010). These obstacles include lack of access to psychological and social support, lack of awareness; and interaction with women’s decision to stay within the abusive relationships (Kulwicki et al., 2010).
Some researchers attributed refugee women’s avoidance of asking help to cope with their violence to the possibility of inequalities in social services, the lack of capacity to respond to immigrant’s needs in a culturally appropriate way and victims’ suffer from other psychological difficulties. These circumstances might put the refugee women at a higher risk for more problems in addition to their unique previous stressful life experiences (cultural and political conditions) (Liao, 2006).
Due to the limited number of research about reasons for not seeking professional help by refugee women to cope with violence, this study attempted to clarify the actual reasons and possible difficulties that might limit refugee women’s decisions to ask help and support to deal with their IPV problem. Furthermore, this study attempted to answer the following question; what are the reasons for not seeking professional help by victims of IPV among refugee women?
Knowing the reasons for not seeking professional help and the factors that affect women’s decisions for seeking help and the difficulties that victims are facing would influence the policymakers to organize a training program for the care providers. Such programs would provide the care providers with the needed knowledge and skills to help victims to seek professional help. Also, findings might help care providers and mental health professionals in planning tailored support programs for women to educate them about their rights to ease such vulnerable women’s decisions in seeking help behaviors.
Method
Study Design
This study used a descriptive qualitative design with semi-structured interviews to address major data from a sample of abused refugee women (ARWs). These data were concerned with factors that affect women’s decisions in asking professional help to deal with their IPV problem. We used a qualitative method to understand the emotional, social, and interpersonal contexts, as well as the personal experiences and perspectives of these hard-to-access cases.
Study Participants
Thirty Syrian refugee women participated in this study. The women were within the reproductive age (15–45 years), who were in marriage relationships with Syrian husbands and fled from south Syria with their families. For the recruitment of study participants, nine local community organizations (LCOs) working with the refugee in north of Jordan were contacted, where three of them confirmed their cooperation. The researchers explained the study objectives and procedures for LCOs’ administrators. The social workers who were working in LCOs reviewed all saved referred women’s files and documents related to their work with the refugees. Sixty-eight women were identified as abused women who were suffering from IPV at their homes and registered as IPV cases in LCOs’ documents. Social workers contacted them either by telephone or sent a message (SMS) and introduced the study objectives and procedures. Initially, the study sample was enrolled out of this group of women who consented to participate in the interviews (34 women), where just 30 of them approached and attended at their addressed appointments, four women canceled the appointments (due to vocational, psychological, and marital [parental] reasons) and did not show up and could not be reached to reschedule.
Measures
The study was based on 30 in-depth semi-structured interviews (30 Syrian ARWs) conducted in three small villages where usually Syrian refugees living in Jordan (Al-Saadia, Al-Zaitarri camp, and Al-Khalidia in the north of Jordan). The semi-structured interview was developed based on Damra and his colleagues’ previous study in Jordan (Damra et al., 2015). An expert panel group who has experience in research designing, and assessment, evaluation, and psychological counseling reviewed the semi-structured interview and validated it.
Study Procedures
The researchers implemented the 30 structured interviews at a convenient time and place (i.e., social workers’ offices) for ensuring confidentiality and privacy. Researchers ensured that data saturation was achieved and no new information was obtained. Each interview required 60 to 75 min to be completed and was being conducted between March 16, 2018 and September 23, 2018. Participants received a US$10 gift voucher in recognition of their assistance, transportation, time, and efforts. For the study purposes, IPV was defined for ARWs as any experience of physical, emotional, or sexual abuse committed by a current partner. The semi-structured interviews started with welcoming, greeting, questions regarding the demographic characteristics of the women, ensuring that all women have a full understanding to study objectives, gradually moved from broad questions on IPV, and seeking help styles. The social workers defined the seeking help behaviors for women “as any behaviors, reactions in purpose to ask help by refugee women to cope with IPV problem (i.e., whether an individual prefers to seek help at an established specialized center, refugees protection agencies, a hospital, counseling clinic, visit traditional healers, or to seek assistance from family or friends or relatives or via self-treatment)" (Umubyeyi, 2015).
Women’s rights were protected throughout the study conduction. The institutional review board was obtained from Hashemite University and permission to access was obtained from the LCOs’ administrators. Women were informed that they could withdraw from the study at any time without explanation and can refuse to answer any question without affecting their care. To protect their confidentiality, their names were kept in a secured computer and replaced with numbers for the following credibility. Women were informed that they would be contacted later for the credibility of the result and they signed for that. Women gave their written consent after verbal full disclosure by the researchers and after reading thoroughly the information sheet. All interviews were audio-recorded and transcribed by the research assistants. Collected data include demographic characteristics, past or current with substance abuse; IPV; asking help to deal with IPV problem, psychiatric history, personal history of witnessing and/or experiencing violence at original family, stressful life events, and economic\educational status.
Data Analysis
Descriptive statistics were used to describe the characteristics of the study participants by SPSS version 20. The recordings of the interviews were verbatim transcribed and processed manually. Two involved experts independently analyzed all interviews after reviewing and reading them at least 3 times to familiarize themselves with the written data. Thematic content analysis (TCA) approach (Berg, 2004) was used to analyze the data. They coded the raised themes in the interviews and discussed with each other to reach agreements. Raised codes in each interview were compared between the experts. If there were additional codes that emerged from the mutual discussions, they also were applied to the transcripts. This was done to dissect and label the data into meaningful parts. The results of the TCA were discussed between the two experts and researchers. The found quotes and illustrations that underline the results were translated from Arabic into English.
Results
Descriptive and Demographic Results
Participants’ age ranged between 15 and 45 years (M = 29 years). Most of the women have low educational level (n = 23 women, 76.7%). Most of the family household monthly income in U.S. dollars was less than US$100 (n = 19, 63.3%), and the family income resources were from United Nations Higher Commission of Refugee (UNHCR) financial support (n = 24, 80%) and personal salary (n = 6, 20%). All women were unemployed and Muslims. Only two women (7.6%) were without children where the rest have. Women’s husbands were the perpetrators (n = 30, 100%). Regarding violence exposure, most of the women (n = 19, 63.3%) had experienced IPV in the past 6 months and 27 women (90%) did not report the IPV directly and voluntarily. Almost all of them (n = 29, 96.6%) did not ask any protection services (except one woman), and 15 women (50%) tried to ask informal and unprofessional help from their friends. For more information, see Table 1.
Characteristics of the Study Participants.
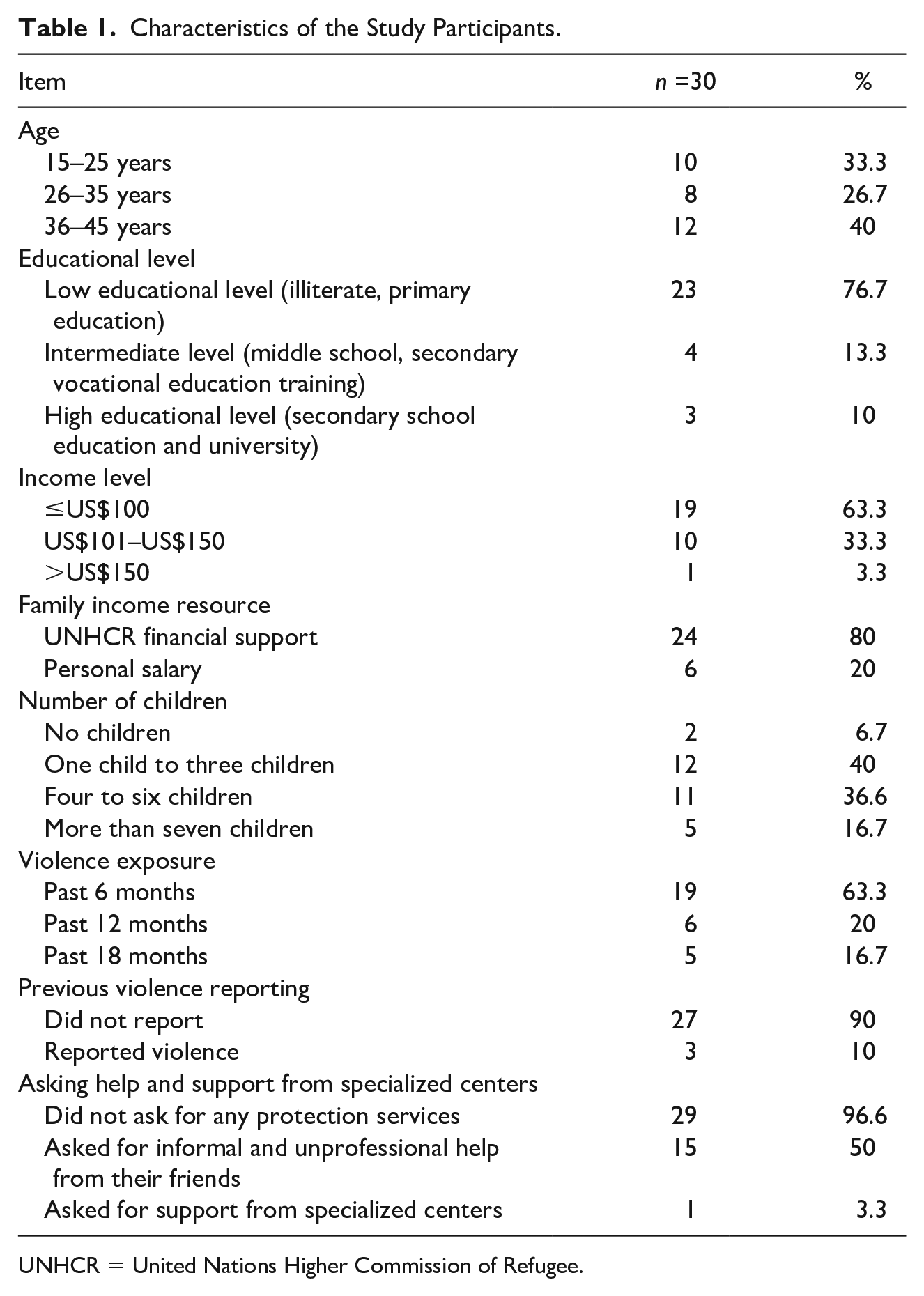
UNHCR = United Nations Higher Commission of Refugee.
Factors affecting help-seeking behaviors for IPV refugee women
Five factors were found to affect women’s help-seeking behaviors, they included misconceptions about IPV problem; difficulties to access and approach different care centers; lack of awareness of the negative consequences of IPV; unaware, negative expectations, negative experiences and incorrect thoughts about IPVs’ services; and psychological and physical health difficulties.
Theme 1: Misconception about IPV problem
Although all interviewed women felt uncomfortable in their current marital relationship due to IPV, 23 women (76.6%) did not feel that they need help because of this problem, even if we considered it a problem, it will disappear soon. Twenty-five women (83.3%) did not consider their IPV problem serious enough to seek professional help. One interesting finding was two thirds of the interviewed women (n = 20) did not recognize the partner’s aggressive behaviors as a human right violation, but they considered it a normal reaction. Furthermore, several women (86.6%) stated that they did not consider solving IPV problems as their highest priority in the meantime as basic needs were more important. The following quotation clarifies this: I am a refugee woman, raised 5 children without any income resources [just UNHCR support], every morning I have opened my eyes to different needs, pains, and suffering. IPV is not my priority now.
Twenty-two women (73.3%) think violence is limited to physical type while emotional, sexual, or psychological types were not recognized as violence or a personal violation.
Theme 2: Difficulties to access and approach different care centers
Twenty-nine women (96.6%) were earning less than US$150 monthly. All of the interviewed women were living in the north of Jordan, where 20 women (66.6%) lived in a refugee camp and the rest of them live in poor scattered villages. All participants indicated that they faced difficulties to access and approach different care centers as a result of high transportation costs, lack of accessibility, low transportation quality, and long-distance between their homes and located caring centers.
All interviewed women faced legal problems due to illegal residence in Jordan. Twenty-seven women (90%) thought that they could not move freely because of their illegal residence. Fifteen women (50%) believed that the police would arrest if they left the camp without prior approval of the camp administration. The following illustration clarifies this: I have lived in the Zaatari refugee camp since the crisis began in Syria. It was not allowed for us to move out of the camp freely, and some of the needed services were offered out of it. Therefore, facing violence was better than facing police and detention.
One of the women mentioned the following statement about security problems that prevented her from receiving help outside the camp: If you wanted to get out of the camp, you were under the risk of facing outside community hostility; I have been subjected to a lot of sexual harassment because I was a refugee woman, it was better to seek help from a friend or a family member.
Theme 3: Lack of awareness of the negative consequences of IPV
This theme has three components: (a) lack of awareness of the relationship between IPV and marriage dysfunction, (b) lack of awareness of the negative impact of observing violence on children, and (c) lack of awareness of the relationship between IPV and different physical complaints. The researchers asked all women if they suffered from unknown physical complaints. Twenty-three women (76.6%) answered positively, but at the same time, none of them justified their complaints to IPV exposure. Consequently, they did not disclose the IPV to their doctors. The following illustration clarifies this: For a long time, I was beaten, kicked, and insulted by my husband. At the same time, I used to visit health centers’ doctors to deal with unexplained physical complaints in my head, back and abdomen. I have not thought before that these complaints might be associated with IPV.
All ARWs expressed having negative feelings such as guilt, sleep problems, loss of appetite, unsecured, and lack of interest with any activity combined with poor concentration. Twenty-three women (76.6%) indicated that they did not link their psychological complaints to IPV. One woman illustrated the following: I have suffered from a low mood in the morning, no interest, long periods of crying, and isolation. I have repeatedly had different suicidal thoughts, but my children’s responsibility stopped me. You know this was the first time that I talked about my suffering; I needed to rethink all these feelings concerning my experience of violence.
Witnessing IPV by children was affecting their mental, social, and emotional health. Fifteen women (50%, most of them had sufficient educational level) stated that, if children witnessed violence, their mental, social, and emotional development would be hampered negatively. These women indicated that they tried to hide the abuse from their children (verbal, physical, and sexual ones). As a result of this, these 15 women had participated in some LCOs’ activities about IPV. The following quotation clarifies this: I knew that violence could hurt my children’s mental health and hampers their development at different levels, I used to behave as nothing had happened in front of them.
On the other side, 15 women (50%) did not believe that witnessing IPV could hurt their children. These women were deprived of any local activities regarding women’s empowerment and violence programs. The following quotation clarifies this: When I was a child, I had witnessed many different violent events in my original family, nothing happened to me. The same for my children, they did not suffer from any problems.
Theme 4: Unaware, negative expectations, negative experiences, and incorrect thought about IPVs’ services
Twenty-nine (96.6%) women tried to solve their marital problems by themselves. They have never asked for any formal help from LOCs (e.g., police, protection shelters, mental health professional\family physician). Just one woman asked help from the police department and reported severe physical violence. Most of them (23 women, 76.6%) did not believe that the police’s help would solve their problem. A woman illustrated: Oh my God . . . this was the first time to know that such service was available for refugee women in Jordan. I thought that the protection services and interventions against violence were exclusive for Jordanian women.
All ARWs have never sought professional help for their marital difficulties. Twenty women (66.6%) thought that seeking help could cause a personal scandal and would be interpreted as a personal weakness. Furthermore, asking for outside help was considered a taboo. Half of them were sure that no one will understand them if they decided to report their suffering to the police or LOCs. One woman illustrated: This was my first time to talk about my IPV experience, speaking to outsiders was not recommended and considered odd. No one could understand you well. It was better to keep your problems inside your home.
Most of them (21 women, 70%) thought that their counselor, mental health professional, or physician were not capable of handling their problems. Twenty-five (83.3%) women thought that they would not benefit from the services. Women did not believe in the services’ providers and their abilities in providing any kind of help. This hampered them from asking professional support. One woman said, One day I decided to speak about IPV with the counselor during my visit to LOCs. She hardly listened, so I did not think that any good change would happen.
Fear from negative expected outcomes was influencing women’s behaviors to seek help and professional support. Twenty-five women (83.3%) believed that asking help would eventually lead to divorce and separation from their children and families. Furthermore, it could hurt their families because of the possibility of expelling the perpetrator (husband) and returning him to his country of origin (deportation), which might increase their family suffering.
Some women (21, 70%) were refraining from seeking professional help due to the expected low privacy procedures from professional staff. The following quotation clarifies this: I did not trust to discuss my issues with strangers, I was a refugee and afraid that they would send my husband away. You should, therefore, be so careful when you decide to share any personal information with these professionals.
Another remarkable issue was related to the possible women’s misunderstanding of the interaction between IPV exposure and the resettlement process in the UNHCR. Nine women (30%) thought that if they reported any IPV incidents to UNHCR or other organizations their resettlement process would be hampered. The following quotation by woman clarifies this: I have heard from my neighbor who was abused by her husband, if any abused woman has reported her IPV, the UNHCR would help her immediately, but her resettlement file would face difficulties.
Theme 5: Psychological and physical health difficulties
Half of the abused women (50%) reported depressive symptoms (sadness, loss of interest in activities, loss of pleasure, fatigue, excessive crying, feeling of guilt, sleep difficulties, worthlessness, and helplessness). Seven women (23.3%) were referred before to mental health clinics for their depressive symptoms.
One woman indicated the following depressive symptoms: Depression for me came out of nowhere and hit me like a ton of bricks. I could not eat, sleep or connecting with pleasure and enjoyment. I was an IPV victim with a traumatic history, I could not stand up again.
Five women (16.6%) suffered from physical limitations resulted from exposure to torture. Three women (10%) suffered from leg amputation resulting from different war accidents. One amputee woman mentioned: As you see I had a physical disability, I could not work or go out of my home.… I hoped that IPV’s services could be modified to be mobile and provided their services at home.
Discussion
Although our participants were having common reasons for not seeking professional help, each woman has her unique story to tell. We understood each woman’s personal experience and kept conscious about our position to not to generalize women based on race, class, nationality, or status. We recognized that our nationality as Jordanians informs our research. We kept our personal position in mind all the time, so we could present out findings with integrity and contemplation (Berrien, 2018). Refugee women have experienced many serious stressful events because of oppression, war, migration, and resettlement (Refugee Health Technical Assistance Center, 2011). For the Syrian refugee women, political oppression intersects with other forms of oppression, such as racism, classism, religious, and sexism oppression (Berrien, 2018) that powerfully affected women’s experiences, specifically being a refugee who has experienced IPV.
We found some factors affecting ARWs’ decision for seeking professional help. These factors included: misconceptions about IPV problems; difficulties to access and approach different care centers; lack of awareness of the negative consequences of IPV; unaware, negative expectations, negative experiences, and incorrect thoughts about IPVs’ services; and psychological and physical health difficulties.
Our participants had misconceptions about IPV. The main important result of this study was, although participated ARWs were dissatisfied with their marriage relationship, they did not consider themselves as IPV victims and this could be their husbands’ view of point, but we did not ask about the husband in our study. This might affect women’s seeking help behaviors and resulting in a lack of motivation for seeking professional help. This result went with other studies line (Alotaby et al., 2012; Damra et al., 2015; Qasem et al., 2013) which reported that women tended not to disclose or ask for help for IPV as they considered it as usual family interaction.
The results revealed that dealing with violence was not a priority for ARWs, because of their suffering from difficult living situations inside and outside refugee camps. All interviewed women faced various problems such as low income (less than US$100 monthly), living in rented homes, living in refugee camps, facing persecution and; difficulties in traveling due to illegal residency in Jordan with significant fears and distrust. This result was congruent with McColl and Johnson’s (2006) findings, which indicated that the majority of psychiatric suffering of refugee individuals were not only related to violence experience but also associated with persecution, social isolation, and separation from families.
Women did not consider the aggressive behavior of their partners as dangerous and violent. This could be understood in light of abused woman’s changing stages theory by Burke and her colleagues (2004). Burke et al. (2004) described the change in abused women as a gradual process with several stages. The first stage: precontemplation, which could be defined as: A woman does not recognize the partner aggressive behaviors like violence and is not motivated for action. The second stage: The contemplation can be described as the abused woman identifies the problem as a kind of abuse; this stage is followed by increasing awareness and weighs the benefits and disadvantages of enrolling in the changing process. Burke et al. (2004) described additional two processes, which help IPV victims to move from the precontemplation to the contemplation stage, which are consciousness-raising and therapeutic alliance (helping relationships). Unfortunately, most of our participated ARWs were still in the precontemplation stage and they had a low level of awareness toward the violence’s negative consequences and did not ask for any professional help. So, they were not ready to move into the contemplation stage.
Another finding was women’s difficult living conditions (camps and illegal residency) resulted in difficulties to access and approach different care centers. Our finding is supported by Prosman et al. (2014) study, who found that IPV refugee victims have materialistic problems to access professional help. Women’s limited resources and their illegal residence made it difficult to access care. Furthermore, women thought that they might lose their freedom if they were arrested by police or they might face community hostility and sexual harassment. All these factors were preventing women from approaching health centers. Abused women’s conservative behaviors toward approaching health centers could be understood through the perspective of conservation of resources theory (COR), which is among the most popular attempts to describe interpersonal regulation and coping processes with stress (Hobfoll, 2012). Based on COR, people are consciously aware that their resources are under the risk of loss or are unstable, they are more likely to move toward decreases possible stressors rather than increases personal resources within contingent domains (Hobfoll, 2011). This process can interfere with ARWs behaviors toward experienced violence. All interviewed women were living in difficult situations and limited personal resources, they tended to save and keep their present or current resources (e.g., living with family, freedom, being close to her children) rather than fighting violence and abuse and adapting self-empowerment behaviors.
Not seeking professional help might be related to women’s lack of awareness of violence’s negative consequences on themselves and their children. For that reason, some of them tried to neglect their problems, sufferings, and not asking for help. A woman in an early stage of change like our sample lacks the awareness of what exposure to violence does to her children (Lemmey et al., 2001). According to Burke et al. (2004), a woman who is in a late or advanced stage of change can recognize the violence impact on her children and herself. Such a woman is ready to be in a change process and she will take action to eliminate violence, which was not the case with our study participants.
Our findings are similar to Randell et al. (2012) work, who have divided all factors, which can affect an abused woman for seeking help, into two broad categories, internal and external motivators. The importance of labeling the husband’s behaviors as abusive by the IPV victim and woman’s awareness of the abuse consequences are examples of internal motivators. While negative experience with provided services and health staff is an example of external motivators. Furthermore, our findings are congruent with Zink et al. (2003), who found that lack of awareness among women of the impact of violence on the physical and mental health of their children could lead them to lose their motivation for asking professional help which is highly recommended.
Our findings showed that all women reported that they were having negative somatic feelings, where most of them indicated that they did not link their complaints to IPV. This could be explained that these women might relate their physical complaints to their suffering from displacement and limited financial resources rather than from violence.
Our study also revealed that ARWs had a lack of awareness, negative expectations, negative experiences, and incorrect thoughts about IPVs’ services, which led them not to ask professional help. The incorrect thoughts about IPVs’ services could be explained by the gap between the offered health services and the needs of ARWs. This gap ended up in making women not motivated to accept the services and seek professional help. Our findings are similar to Jordan Population and Family Health Survey results (Department of Statistics & ICF International, 2013), which showed that victims of IPV did not consider the available services (LOCs or other health centers) as helpful resources for dealing with their family and marital problems or distress. Moreover, our findings are supported by Morrison et al. (2017) study, as they reported that abused women’s mistrusts with health care providers and counselors’ capacities are considered as the main problem that faces providing services to IPV victims (Morrison et al., 2017).
The results revealed that some interviewed women have faced physical and mental health problems (e.g., depression, amputation, and movement limitations), that prevented them from asking help. The result is consistent with Raj and Silverman’s (2002) study, who reported that ARWs might experience high levels of depression, mainly because of asylum, trauma, torture, rape, and witnessing acts of war and destructions, in addition to their daily suffering from IPV. The depressive symptoms could prevent women from asking help, because of the lack of hope for changing to a better life. Furthermore, these results are consistent with Guruge et al. (2012) findings, who found that a substantial proportion of the refugee women had experienced physical and mental health impairments as a result of various types of violence inside and outside their families. Another study finding which supported ours was done by Javanbakht and her colleagues (2019), who have revealed that depression and anxiety rates were the highest among newly resettled in the U.S. Syrian refugee women. Also, they found that a high prevalence of possible psychiatric disorders was related to trauma exposure (e.g., violence, torture) and stress.
Most of the participated ARWs tried to solve their marital problems with their husbands by themselves. They preferred asking for help from their relatives or friends rather than receiving professional help. This could be discussed in light of the emerged wrong expectations and thoughts toward professional help (e.g., incorrect relationship between their resettlement process and IPV exposure). This result highlights the importance of working to change these incorrect thoughts and cognitive contents by LOCs, UNHCR staff, and other care providers.
As researchers, we need to understand the extent of the IPV problem by getting into women’s stories to understand the pressure of their displacement, culture, and norms, as well as the gender-based violence that they were facing. We, as researchers, are trying to contact policymakers to get them involved in understanding the actual reasons for seeking help for the IPV that the women faced and the changing pattern of IPV since displacement from Syria. Such an understanding could help in preparing programs to prevent violence among refugees.
Limitations
Our study results have some limitations. Results cannot be generalized to other communities of women or refugees as a qualitative design was used. Our findings could not be applicable for all ARWs in different nationalities or women who were living in Jordan at the same time of the study, as we gathered a small group of participants who accepted to be involved.
Only women visiting cooperative three LOCs (accessible sample) have been enrolled in the study. The procedures excluded a group (of unknown extent) of women who are currently in an abusive relationship but not visiting the LOCs.
Moreover, many LOCs refused to be involved in the study because of ethical considerations. For that, the sample might not reflect the real IPV problem among the Syrian refugee community in Jordan, even though we were able to interview 30 Syrian ARWs with different characteristics. This means that ARWs (as other abused women) are very difficult to be studied or reached, and hence limit our understanding of their psychological, social, and medical needs.
Implications for Practice
There are administrative, clinical, and community implications for this study. Professionals who are working in national and international refugee centers and other LOCs need to be appropriately trained to screen and recognize abuse. International refugee centers should facilitate and offer adequate resources for refugee women (e.g., a variety of services, facilitating ARWs mobility in and outside the refugee camp, outreach activities, financial support). Furthermore, LOCs should raise women’s awareness about the importance of professional help and reality of IPV consequences to modify women’s incorrect cognition toward them (e.g., violence has no negative impact, reporting violence might complicate your resettlement file in UNHCR, available services are exclusively limited for Jordanian IPV women, reporting IPV to police can lead to arrest or deport my partner to our original country). Moreover, professionals need to adopt structured working procedures, start from IPV’s screening, and end with effective interventions. For clinical implications, the care provider and mental health specialist (e.g., social worker or counselor) must consider IPV as one of the main problems for refugee women and developing his\her capacities to screen and intervene to solve it, in the light of changing cycle for IPV victims. Victims need empathetic, supportive, and nonjudgmental counseling from their care providers to change their daily suffering, and this might ease their mental health status.
The results of this study revealed that most of the participants did not consider violence as a human right violation. The suitable implication in this situation is adapting a comprehensive community prevention and treatment program against violence not only for refugee women but also for all women in the community. This comprehensive and recommended program should involve all IPV parts; women, men, and children. This could raise their awareness about the negative consequences of violence and could prevent men from engaging in violent behavior and could enhance community efforts in preventing men from abusive behavior. Furthermore, such programs could support women and rebuild their self-confidence and offering them additional resources.
Conclusion
Most of the ARWs of our study group is depending on receiving informal support but not professional help. Most of the interviewed women were unaware of the possible negative consequences of abuse, faced different difficulties for approaching services (logistics or personal), had incorrect thought and negative perceptions toward receiving professional help; suffered from psychological and physical difficulties which, resulted from long exposure to war. All of these barriers can hinder women from asking for professional help. Family counselors with other professionals (e.g., physicians, social workers, and refugee workers) can play an important role in recognizing ARWs and facilitate their access for help.
Footnotes
Acknowledgements
The authors thank the local community organizations working with the refugee in north Jordan and to the women who participated in the study for their friendly cooperation with the data collectors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was self-funded.