
Abstract
Law enforcement reporting following sexual assault is lower than for other violent crimes. Sexual assault nurse examiners (SANEs) provide care for patients in the acute period following sexual assault and are well-positioned to identify and address barriers to reporting. We examined data from medical forensic examination records documented by SANEs for a 5-year period (2011–2015). We examined 347 records of women 18 and older to identify factors associated with law enforcement reporting at the time of the exam using binomial logistic regression to construct odds ratios (OR). A total of 56.5% of patients in the sample reported to law enforcement. Patients who did not voluntarily consume alcohol were more likely to report than those who did (OR = 4.45; p = .001). Patients who were not students were more likely to report than students (OR = 3.24; p = .002). Patients who had a medical forensic exam within 32 hr of the assault were more likely to report than those having exams after 32 hr (OR = 2.68; p = .007). Patients who had anogenital and/or bodily injuries were more likely to report than those who had no injuries (OR = 2.50; p = .008). Patients who were penetrated (vaginally, orally, and/or anally) were more likely to report than those who were not penetrated (OR = 2.50; p = .056). Knowing the assailant, having multiple assailants, and patient and assailant race/ethnicity were not associated with different likelihood of reporting to law enforcement. SANEs and others who work with victims of sexual assault can use data to understand and address barriers to reporting.
More than 700,000 sexual assaults occur in the United States each year (Morgan & Oudekerk, 2019). Sexual assault (defined as rape or other unwanted sexual contact) is a crime with potentially severe adverse health consequences (Dworkin et al., 2017; Larsen et al., 2016). Many perpetrators are repeat offenders and at risk of committing other types of crimes (Hanson & Morton-Bourgon, 2005; Lovell et al., 2017; Lussier & Cale, 2013; Zinzow & Thompson, 2015). Therefore, prosecuting perpetrators of sexual assault can protect communities from multiple crimes.
Despite the seriousness of sexual violence, an estimated 60% to 75% of victims do not report the crime to law enforcement (Morgan & Oudekerk, 2019; Rennison, 2002; Sinozich & Langton, 2014). Moreover, the percentage of persons who reported sexual assault declined from 40% to 25% from 2017 to 2018 (Morgan & Oudekerk, 2019). Most published studies examining factors associated with law enforcement reporting of sexual assault relied on retrospective victim interviews. The purpose of the current study was to examine patient, assailant, and assault factors associated with law enforcement reporting at the time of a medical forensic examination (MFE) by a sexual assault nurse examiner (SANE) in the acute period following sexual assault. Examining objective factors rather than self-reported factors obtained retrospectively might yield important additional information regarding why victims do or do not report. Results may improve understanding of how reporting behaviors of victims who have MFEs might differ from victims who do not have MFEs. Results have implications for SANEs and for targeted interventions to reduce barriers to reporting.
SANEs are registered nurses with additional education in providing sexual assault MFEs. SANEs are well positioned to identify and address barriers to reporting because they provide care in the acute aftermath of sexual assault when patients might still be deciding whether to report. Medical forensic exams following sexual assault include treatment of acute injury, prevention of unintended pregnancy and sexually transmitted diseases, referrals to promote optimal health outcomes, and evidence collection for investigation and prosecution (Office on Violence Against Women, 2013). According to the National Protocol for MFE, SANEs “should discuss all reporting options with victims in a language they understand and the pros and cons of each” (Office on Violence Against Women, 2013, pp. 5–6). Reporting options in the United States vary by state law but are required by the federal Violence Against Women Act of 2005 to include non-report evidence collection and anonymous reporting options in addition to regular reporting. Patients have the right to receive MFEs without engaging with law enforcement.
According to the Bureau of Justice, law enforcement reporting of sexual assault is lower than for other types of violent crime; 25% of victims reported to law enforcement in 2018 (Morgan & Oudekerk, 2019). College students may be less likely to report (Sinozich & Langton, 2014). In retrospective self-report studies, victims stated they did not report to law enforcement for the following reasons: did not want others to know; did not acknowledge/felt unclear whether what happened was rape; fear of being treated badly by police; perceived lack of evidence; concern for being blamed; feeling partially responsible; fear of retaliation; use of alcohol or drugs; acceptance of rape myths; and relationship to the perpetrator (Cohn et al., 2013; Heath et al., 2013; Paul et al., 2014; Wilson & Miller, 2016; Wolitzky-Taylor et al., 2011). Also in retrospective self-report studies, victims stated reasons they did report to law enforcement, including: to improve their well-being; sense of social responsibility; to seek information, advocacy, or accommodations; desire for criminal prosecution; encouragement from others; concern about sexually transmitted infections (STIs); fear of injury or death during the assault; and presence of/severity of injuries (Demers et al., 2017; Paul et al., 2014). While these studies relied on retrospective interviews, a single study that queried patients during MFEs regarding their decisions to report found reasons similar to those patients who did not report (Jones et al., 2009).
Most victims of sexual assault do not receive MFEs following sexual assault (Zinzow et al., 2012). Data are limited regarding reasons victims seek medical care but include: to address physical and mental health needs evidence collection and encouragement by law enforcement or health care providers (Du Mont et al., 2009). These findings suggest victims who present for MFEs often intend to report to law enforcement. Having an MFE conducted by a SANE may increase victim participation in the legal process, either due to better documentation and evidence quality, because victims feel supported, or both (Campbell et al., 2009; Crandall & Helitzer, 2003).
While law enforcement reporting generally is low, little is known about reporting by persons presenting for MFEs following sexual assault. Examination of objective factors associated with voluntary law enforcement reporting of sexual assault can reveal additional information about victim motivation for reporting. Objective factors obtainable from MFEs include victim characteristics (e.g., age, race/ethnicity, college student status), assailant characteristics (e.g., race/ethnicity, relationship to victim, multiple assailants), and assault characteristics (e.g., injuries, whether penetration occurred, assault location). The purpose of this study was to examine patient, assailant, and assault factors associated with law enforcement reporting at the time of the MFE. SANEs and others who work with victims of sexual assault can use these data to identify and address barriers to law enforcement reporting.
Method
Sample and Setting
Data for analyses were extracted from deidentified program data forms generated by a hospital-based SANE program at a large academic medical center in the Midwest between 2011–2015 (data are available by contacting the primary author). The program employed approximately 10 SANEs who provided 24-hr coverage at two local hospitals. Each nurse completed, on paper, a data form following exams that included patient demographic data and general information about the assault for program record keeping.
In the state from where data were extracted, SANEs were not required to report sexual assaults of patients 18 years or older to law enforcement, unless they involved serious injury from stabbing or gunshot wounds, or patients were dependent adults. Exams were fully reimbursed directly to the hospital by the state’s Office of the Attorney General and did not require law enforcement requests for exams before reimbursement, nor were patients billed for exams. Patients could receive exams without evidence collection or have anonymous kits collected. Law enforcement collected exam evidence from the SANEs immediately following exams, though patients were not required to interact with law enforcement at that time.
Names, birth dates, and medical record numbers were redacted from 399 program data forms by the program coordinator prior to delivery to the research team. Data from patients under age 18 or dependent adults (n = 35) were excluded due to mandatory reporting laws. Cases involving male victims were excluded due to small number (n = 17) and possible differences in reporting behavior (Sable et al., 2006). This left 347 cases as potential data. The project was reviewed and designated nonhuman subjects research by the institutional review boards at the forensic nursing program site and the lead author’s academic institution.
Data Analysis Strategy
The data analysis strategy was to: (a) examine variables found in patient records (b) identify factors for which there were sufficient and usable data (c) reduce the variable set to conduct reliable and suitably powered statistical analyses, and (d) use binomial logistic regression to identify factors that predicted law enforcement reporting. G*Power 3.1.9.2 (Faul, 2014) was used to determine analytical methods and conduct tests of proportion. Descriptive statistics were used to describe the sample and identify variables with missing data for exclusion from the regression model. Descriptive, predictive binomial logistic regression analyses and post hoc analyses were conducted using Stata 15.2 (StataCorp, 2018).
Binomial logistic regression using dichotomous predictors was selected as the analytic approach for three primary reasons: (a) all variables in the cleaned and final data set were binomial or non-ordinal and categorical, (b) using dichotomous predictors produces odds ratios that are directly comparable without reference to different units of measurement, greatly improving ease of interpretation by multiple disciplines with an interest in factors that predict reporting to law enforcement, and (c) there was substantial variation in the completeness of records. Random variations in record completeness were outside the control of the study design; in which case, “listwise deletion is known to produce unbiased estimates and conservative results” (Kang, 2013, p. 403). Therefore, listwise deletion of cases with missing values was employed, and only complete cases were included in the binomial logistic regression.
The outcome variable of interest was law enforcement reporting. Law enforcement reporting was defined as follows: (a) the patient had an interaction with law enforcement before the MFE voluntarily or because someone else called law enforcement; or (b) patients spoke with law enforcement while at the hospital. Patients who stated they did not want to report, were undecided, or stated intent to report to law enforcement though had not done so before discharge, were coded as not reporting.
Independent variables for predicting law enforcement reporting were based on available data, previously published evidence, and the judgment of SANEs involved in the project. Variables for which there were few incidences (e.g., cognitive disability, incarcerated) or for which there were missing values (e.g., how long an acquaintance was known) were excluded from analyses. Several variables were converted to dichotomous variables. For example, the time between assault and exam was converted to a binomial due to missing continuous data for that variable. Many forensic nurses did not record the exact time of the assault and/or exam on the program data form. Thus, the binomial was created using day of the week and time in 8-hr blocks (0000–0800, 0800–1600, and 1600–2400), which were more faithfully documented. If the exam was within two calendar days and the assault occurred before 1600, it was coded as <32 hr; if the exam was two calendar days apart from the assault and the assault occurred after 1600, or the exam was more than two calendar dates apart from the assault date, it was coded as ≥32 hr.
The original six race and ethnicity categories were converted to a binomial of White non-Hispanic or non-White and/or Hispanic, due to low numbers of assailants in any racial/ethnic grouping except White non-Hispanic. The relationship between the patient and the assailant was originally recorded as one of four categories: related, acquaintance, stranger, or unknown. Assailant relationship was converted to a binomial by coding any assailant known previously by the patient (related and acquaintance) as “not a stranger,” versus “stranger.” (“Unknown” was coded as missing). Penetration was converted to a binomial by coding one or more types of recorded penetration (oral, anal, and/or vaginal) as “penetrated,” versus “not penetrated” if none were recorded. Injuries were converted to a binomial by coding any recorded anogenital and/or bodily injuries as “injuries,” versus “no injuries.”
The following variables were recorded in program data as yes/no binomials: patient was a student; patient voluntarily used alcohol before the assault. Age was removed as a variable because its inclusion in logistic regressions reduced the clarity and explanatory power of the results when confounded with student status. However, mean age for the samples was calculated for descriptive purposes. To assess whether cases with complete data in the logistic regression (n = 202) were comparable with all cases and to cases with incomplete data not included in the regression, two-sample tests of proportions were conducted. Based on prior literature, it was expected patients would be more likely to report the assault to law enforcement if one or more of the following were present: they (a) and/or the assailant were White non-Hispanic, (b) were physically injured, (c) were penetrated, (d) were assaulted by a stranger or multiple assailants, (e) obtained an exam shortly after the assault, (f) were not college students, or (g) had not consumed alcohol prior to the assault.
Results
Table 1 describes patient, exam, and assault characteristics of the sample used in regression analyses (n = 342). Table 1 summarizes the frequency and number of missing values for patient, exam, and assault characteristics in all 347 cases. Table 2 compares complete cases used in the logistic regression model (n = 202) to incomplete cases not used in the logistic regression model (n = 145), and to the combined sample of all cases (n = 347). More than half (56.5%) of all cases in the sample reported the assault to law enforcement. Results of the two-sample tests of proportions indicated cases with no missing values were generally similar to cases with incomplete data. Mean age was similar for all 347 cases (25.27; SD = 10.26), 202 cases with complete data (24.97; SD = 9.48), and 145 cases with incomplete data (25.70; SD = 11.29). However, there were two notable instances in which proportions were higher in the sample with no missing values: (a) penetration (83.6%–44.1%), and (b) law enforcement reporting (60.9%–49.6%). Cases with no missing values used in logistic regression were also mostly representative of all cases in the sample. The sole exception was the proportion that reported penetration was higher in the complete cases than for all cases (83.6%–67.2%).
General Case Characteristics of the Study Sample (n = 347).
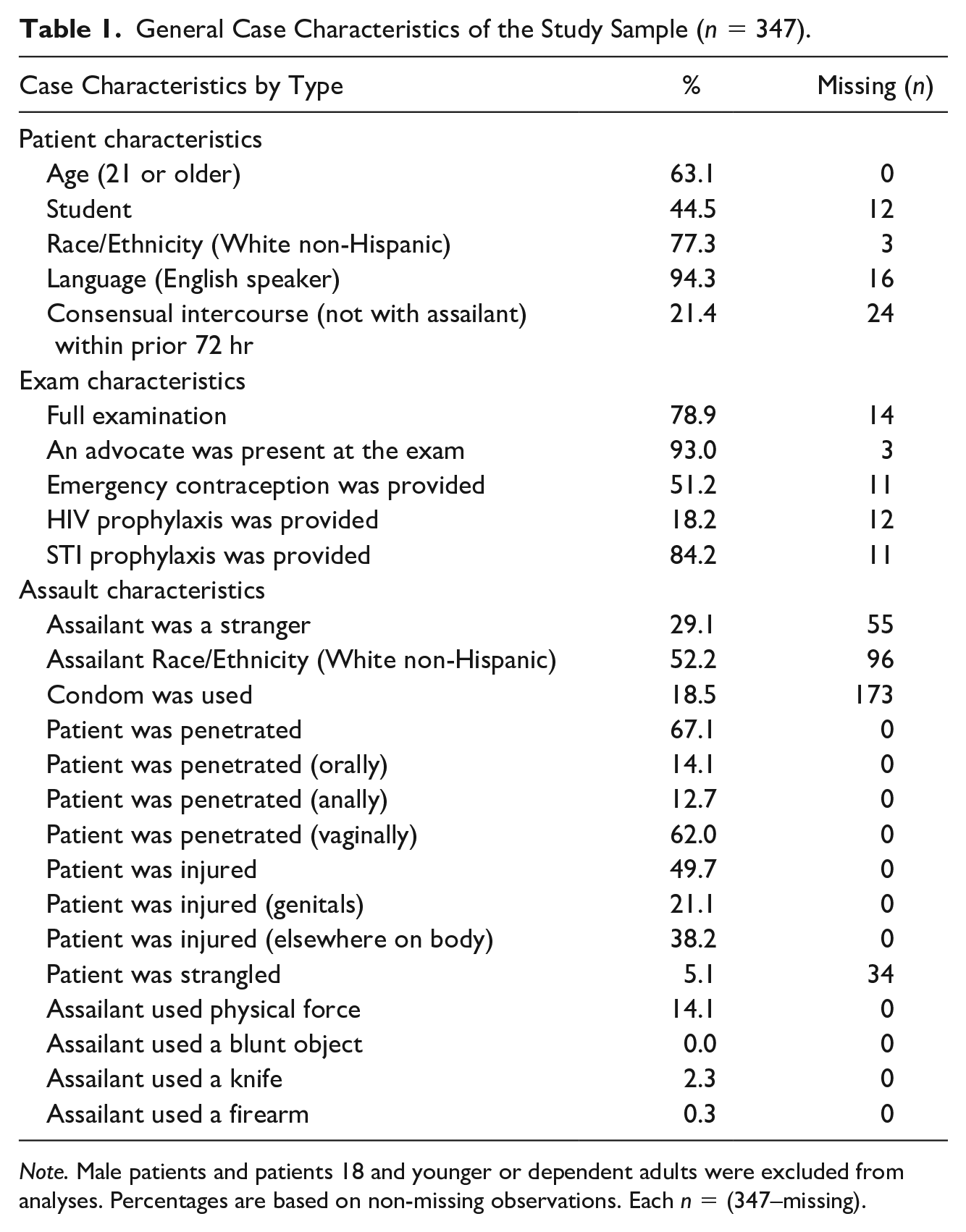
Note. Male patients and patients 18 and younger or dependent adults were excluded from analyses. Percentages are based on non-missing observations. Each n = (347–missing).
Proportions Tests Comparing All Cases and Incomplete Cases to Complete Cases Used in the Final Binomial Logistic Regression.
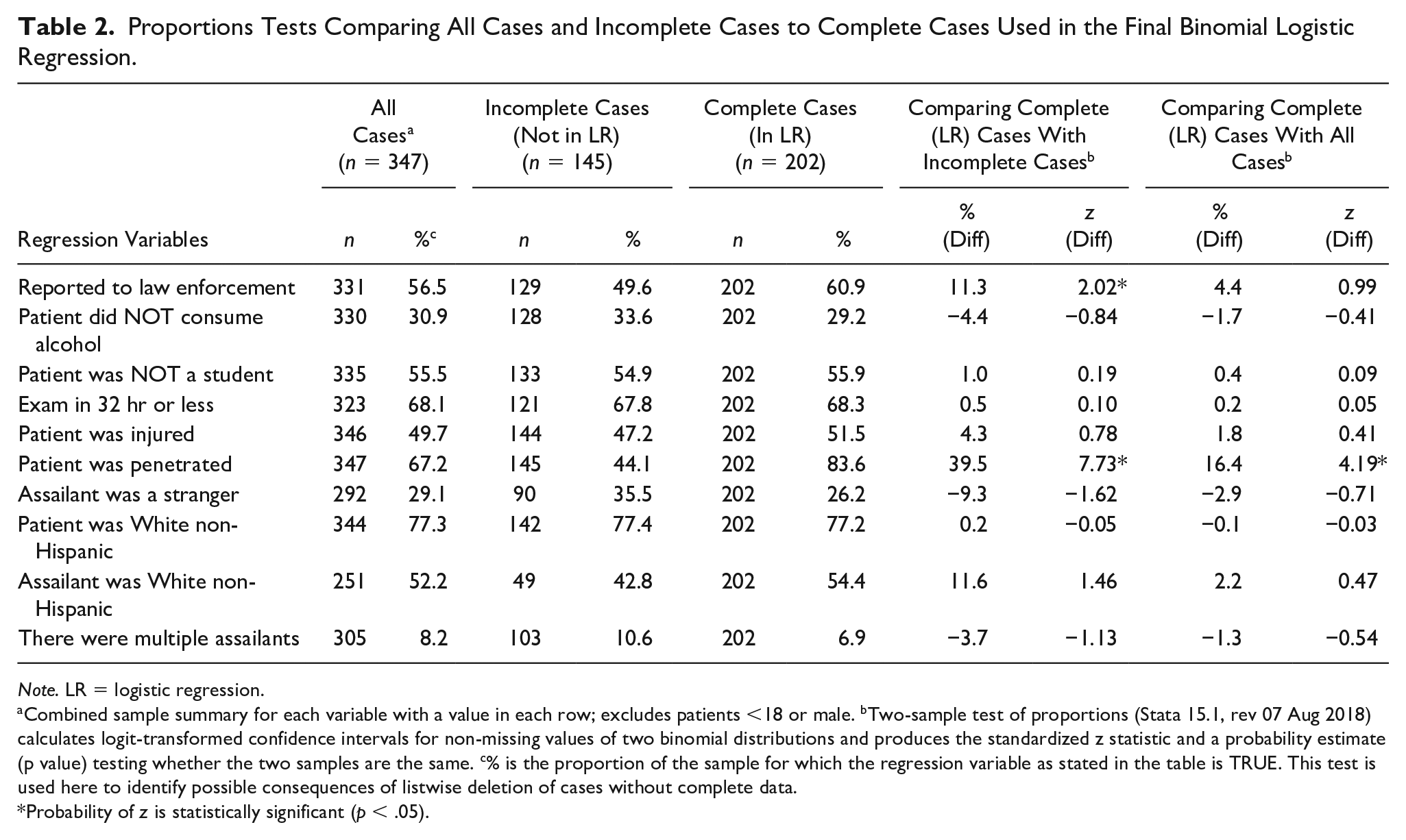
Note. LR = logistic regression.
Combined sample summary for each variable with a value in each row; excludes patients <18 or male. bTwo-sample test of proportions (Stata 15.1, rev 07 Aug 2018) calculates logit-transformed confidence intervals for non-missing values of two binomial distributions and produces the standardized z statistic and a probability estimate (p value) testing whether the two samples are the same. c% is the proportion of the sample for which the regression variable as stated in the table is TRUE. This test is used here to identify possible consequences of listwise deletion of cases without complete data.
Probability of z is statistically significant (p < .05).
Results of the binomial logistic regression are shown in Table 3 (n = 202), with predictors sorted from high to low in terms of their effect on reporting. Variables are presented in terms that reflect greater odds of reporting, for ease of interpretation (e.g., “patient did NOT consume alcohol,” “patient was injured”). The model strongly predicted reporting to law enforcement (χ2 = 46.14 [df = 9], p < .0001), accounting for 17.1% of the variance in reporting. Patients who did not voluntarily consume alcohol prior to the assault were 4.45 times more likely to report (z = 3.38; p < .001). Patients who were not students were 3.24 times more likely to report (z = 3.11; p = .002). Patients who received exams within 32 hr were 2.68 times more likely to report (z = 2.67; p = .007). Patients who were injured were 2.50 times more likely to report (z = 2.65; p = .008). Patients who were penetrated orally, anally and/or vaginally were 2.36 times more likely to report (z = 1.91; p = .056). Patient or assailant race/ethnicity, relationship to the perpetrator, and multiple assailants did not predict law enforcement reporting in this sample.
Factors That Predicted Law Enforcement Reporting, Binomial Logistic Regression (n = 202).
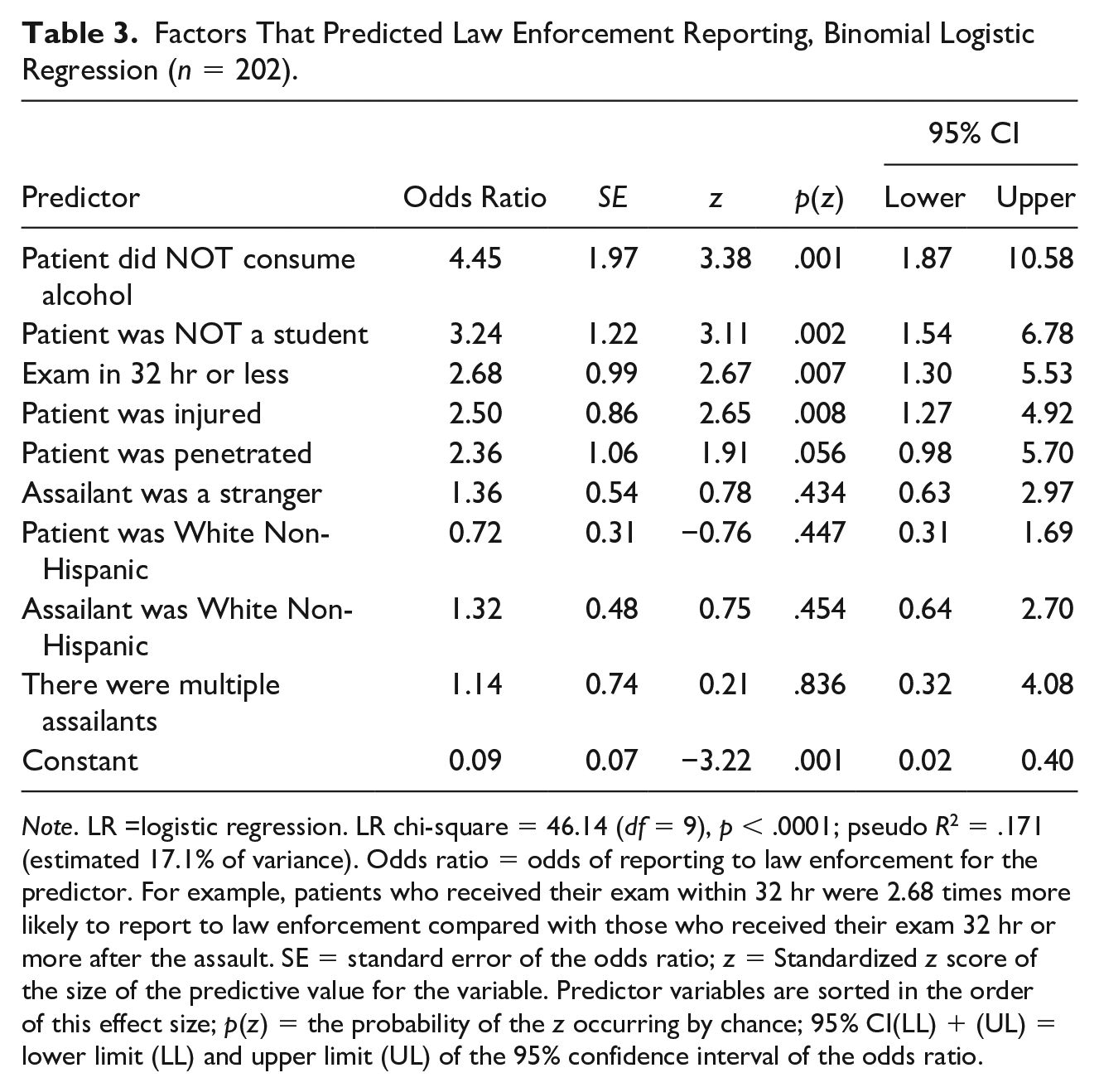
Note. LR =logistic regression. LR chi-square = 46.14 (df = 9), p < .0001; pseudo R2 = .171 (estimated 17.1% of variance). Odds ratio = odds of reporting to law enforcement for the predictor. For example, patients who received their exam within 32 hr were 2.68 times more likely to report to law enforcement compared with those who received their exam 32 hr or more after the assault. SE = standard error of the odds ratio; z = Standardized z score of the size of the predictive value for the variable. Predictor variables are sorted in the order of this effect size; p(z) = the probability of the z occurring by chance; 95% CI(LL) + (UL) = lower limit (LL) and upper limit (UL) of the 95% confidence interval of the odds ratio.
In post hoc bivariate analyses, students were 5.12 times more likely to consume alcohol prior to the assault (p < .001). However, being over 21 (n = 136) and voluntarily consuming alcohol prior to the assault was not associated with greater likelihood of law enforcement reporting than voluntarily consuming alcohol under legal age (n = 96; p = .41).
Discussion
Sexual assault is the least reported violent crime (Morgan & Oudekerk, 2019). To hold perpetrators accountable and prevent them from committing further crimes, it is important to reduce barriers for victims to report to law enforcement. SANEs provide medical care to persons in the acute period following sexual assault and are well positioned to identify and address barriers to reporting. Sexual violence is also a crime with potentially severe adverse health consequences, including STIs (Jauréguy et al., 2016; Jo et al., 2011; Klot et al., 2013), unintended pregnancy (Zinzow et al., 2012), posttraumatic stress disorder (Kilpatrick et al., 2013; Scott et al., 2018), depression, anxiety, and suicidal ideation (O’Neal, 2017), substance use disorder (Ullman et al., 2013), and chronic pain (Ulirsch et al., 2014). Health consequences might be a primary concern for many victims (Du Mont et al., 2009). Most patients in the current study, for example, accepted prophylaxis for STIs and pregnancy, and almost one fifth accepted human immunodeficiency virus (HIV) prophylaxis. At the same time, 56.5% of patients reported to law enforcement either before or at some point during their hospital visit. This percentage is much higher than the estimated 25% in the general population (Morgan & Oudekerk, 2019; Sinozich & Langton, 2014), suggesting many victims may consider the MFE part of the reporting process. A previous study indicated patients who were medically treated were more likely to report (Rennison, 2002). Patients who present for medical treatment might also be made aware of potential health risks they had not considered, such as contracting an STI, which might make them more likely to report (Paul et al., 2014).
The percentage of patients who reported in the current study is also lower than the 75% who reported in a previous study of patients receiving MFEs (Jones et al., 2009). Differences in findings across studies may be due to study settings. Different laws, practices, and policies regarding evidence collection and at what point(s) law enforcement is involved in the process may impact reporting rates. For example, in the prior study examining patient reporting at the time of the MFE, most patients were referred for exams by law enforcement and a crisis hotline (Jones et al., 2009); thus, many patients had prior interactions with law enforcement and/or advocacy who might have informed them of reporting options. Another reason for the high reporting rate may be because that study also included minors, for whom law enforcement reporting is mandatory.
A previous study involving retrospective chart review from a SANE program in Canada (Muldoon et al., 2018) further illustrates how settings and samples may impact law enforcement reporting by patients receiving MFEs. By Canadian law, patients could choose to have a sexual assault evidence kit collected without law enforcement involvement and later decide whether to release the kit to law enforcement. The authors found that 63.9% of patients eligible to have kits collected chose to do so, while only 29.7% chose to release the kits to law enforcement. That number is closer to the 25% who typically report sexual assault in the U.S. general population. In the Canadian study (Muldoon et al., 2018), sexual assault evidence kits were kept at the hospital for 1 year and only released to law enforcement when victims chose that option. In contrast, patients in the current study often presented for medical care without first reporting to law enforcement or advocacy. The law in the state from where data derived required law enforcement to collect kits after the exam was completed. It is unclear from the data what the impact of this process was on law enforcement reporting, but it is possible some patients reported to law enforcement if offered this opportunity by SANEs when law enforcement came to collect the kits. This process provides the opportunity for a “warm hand-off” (Barrett, 2019) to law enforcement. Therefore, while it is possible victims consider MFEs part of the reporting process when they present for an exam, it is also possible patients examined by a SANE, especially with an advocate present, are more comfortable reporting to law enforcement (Campbell, 2006; Fehler-Cabral et al., 2011). Victims who undergo MFEs might also be less conflicted about whether the assault was a crime and might have more ready access to law enforcement at the hospital, reducing two previously identified barriers (Cohn et al., 2013; Wilson & Miller, 2016).
The factor most associated with law enforcement reporting in the current study was patient voluntary use of alcohol; specifically, not consuming alcohol was associated with more than four times greater odds of reporting. In this sample, approximately 70% of patients consumed alcohol prior to the assault, comparable with prior data (Lorenz & Ullman, 2016). Comparison between patients under 21 and patients 21 and over was not significant in a post hoc analysis, suggesting reluctance to report based on underage drinking was not the primary barrier to reporting. In prior data, being impaired by alcohol or drugs during a sexual assault was associated with lower law enforcement reporting (Jones et al., 2009; Wolitzky-Taylor et al., 2011). Victims might be less likely to acknowledge sexual assault if they were drinking (Kahn et al., 2003), and more concerned they will be blamed for the assault (Littleton et al., 2009). Victim alcohol use may decrease the likelihood cases progress in the legal system (Campbell et al., 2009), substantiating victims’ concerns. This barrier appears to persist despite statutes in all states allowing prosecution of sexual assault when the victim was voluntarily intoxicated (Long et al., 2016). SANEs and advocates can educate patients about these laws. Perpetrators purposefully target intoxicated individuals (Lisak, 2011), making it critical to hold them accountable and prevent repeat perpetration.
The next highest factor associated with law enforcement reporting in this study was student status. Patients who were not students were over three times more likely to report, consistent with previous studies (Sinozich & Langton, 2014). Alcohol use is prevalent in sexual assaults involving college students (Kilpatrick et al., 2007), and alcohol use was independently associated with lower reporting in this study and in others (Wolitzky-Taylor et al., 2011). Despite high rates of sexual assault in the student population (Krebs et al., 2016), several studies examined reasons students did not report. The most common reason students stated they did not report in one study was because they did not want assistance or action taken, or they did not think the incident was serious enough to report (Sinozich & Langton, 2014). Unfortunately, not wanting assistance and not wanting action taken are different and neither was well described, making findings difficult to interpret. Other reasons students stated for not reporting in that study, in order of frequency, included: fear of retaliation; concern they might be blamed/get in trouble; concern they would be treated poorly or get an ineffective response; concern about confidentiality; did not know how to report. In another study, students stated they did not want to be defined by their assaults (Khan et al., 2018). College students’ perceptions of law enforcement in general influenced sexual assault reporting, with minority students having more negative views of police and lower likelihood of reporting (James & Lee, 2015). Other data, however, indicated victims had mostly positive experiences reporting sexual assault to law enforcement (Wolitzky-Taylor et al., 2011). SANEs can inform patients of these findings, which can influence a victim’s decision to engage with law enforcement (Patterson & Campbell, 2010).
Students who do not report to law enforcement might also have the option of reporting to campus officials under Title IX protections (Office for Civil Rights, 2020). However, campuses also have low rates of reporting to campus officials (Cantor et al., 2017). Students might be more likely to report to campus officials if they had previously received sexual assault education, were vaginally or annually penetrated, or had a positive perception of their campus climate (Spencer et al., 2017). In a hypothetical sexual assault scenario, students stated they would be more likely to report to law enforcement than campus officials (Moore & Baker, 2018). Some students reported negative experiences reporting to campus officials (Smith & Freyd, 2013), similar to negative experiences of reporting to law enforcement.
Other reasons students are less likely to report to law enforcement than non-students may not be currently captured in the literature. Most students disclosed sexual assaults to peers (Dworkin et al., 2016), suggesting use of informal social support. Persons with higher educational attainment might have greater awareness of negative aspects of reporting, such as not being believed and/or being treated poorly by law enforcement (Patterson, 2011; Shaw et al., 2016; Sinozich & Langton, 2014). Students may also not want to disrupt their academic progress to participate in the legal process, suggested by their declining assistance (Sinozich & Langton, 2014). Thus, students who do not report might believe they are being self-protective. SANEs should have knowledge of and inform patients of all law enforcement and campus reporting options in their communities. They can also work with law enforcement and campus officials to coordinate “warm handoffs” to reduce victims’ concerns regarding how they will be treated.
Having an exam within 32 hr of the assault was associated with more than two and a half times greater likelihood of reporting in this sample. Possible reasons include: (a) victims reported to law enforcement first and were encouraged to receive an MFE as soon as possible; (b) law enforcement were called by a third party and transported victims immediately to the hospital where they were offered an exam; (c) victims who presented for an exam shortly after sexual assault were more likely to acknowledge the assault as a crime; (d) patients seeking care at the hospitals were offered an advocate who discussed legal options with them, and; (e) victims who decided to report more quickly might have considered the MFE an essential part of the reporting process.
In the present study, the 32-hr bifurcation was used to maximize available observations. In general, data are limited on the typical time interval victims accessed medical care following sexual assault. In one study, the median time was 16 hr (McCall-Hosenfeld et al., 2009). Another study (Jones et al., 2009) found a difference between those reporting (11.3 hr) and not reporting (20.2 hr). Time since assault was not significant in another study (Muldoon et al., 2018). The time interval that a person can undergo an MFE after sexual assault is set by state laws, facility policy, and national standards based on how long perpetrator DNA is likely to be obtainable from a patient’s body. Currently the national standard is 120 hr (National Institute of Justice, 2017; Office on Violence Against Women, 2013). Most victims in this study and in others that measured this variable found the vast majority presented much sooner than 120 hr.
Time interval to presentation for an exam might be relevant as previous studies found victims who delayed reporting may be viewed by law enforcement as less credible (O’Neal, 2017). However, there is no agreed-upon definition of what constitutes “delayed” reporting. One study considered reports made more than 1 hr after the incident to be “delayed” (O’Neal, 2017); another considered “prompt” or “timely” reporting to mean within 24 hr (Holleran et al., 2010). Finally, a third study considered “delayed” to mean anything reported beyond the 120-hr MFE time window (Price, 2010). SANEs can inform patients who have not yet reported that if they decide to report, doing so as soon as possible might be helpful. SANEs can also educate law enforcement and prosecutors about reasons victims delay reporting to reduce bias against those who do not immediately report.
Another factor predicting law enforcement reporting in this study was presence of injuries. Patients who had one or more injuries were two and half times more likely to report. Approximately half of patients had anogenital and/or bodily injuries, consistent with prior data (Planty et al., 2013). Anogenital and bodily injuries were combined in the logistic regression to maximize cases for analyses, although each may be associated differently with law enforcement reporting. However, Jones and colleagues (2009) found no difference in penetration type between those reporting and not reporting. Prior studies are inconsistent regarding whether women with anogenital or bodily injuries were more likely to report (Fisher et al., 2013; Jones et al., 2009). In a prior study of patients presenting for MFEs, neither anogenital nor bodily injury were associated with reporting (Jones et al., 2009). Bodily injury might be presumed more indicative of nonconsensual sex, while anogenital injuries can also be associated with consensual penetration (Sommers et al., 2012). Both bodily and anogenital injuries can be considered evidence, and evidence is associated with greater progression through the legal system (Campbell et al., 2009; Holleran et al., 2010). In many sexual assaults, however, there are no documented injuries (Möller et al., 2012). SANEs can educate patients that absence of visible injuries following sexual assault is common and injuries are only one type of evidence, so patients are not discouraged from reporting for this reason. Forensic nurses can also educate law enforcement, prosecutors, and jurors that absence of visible physical injuries is common. They can also emphasize psychological harm, including posttraumatic stress disorder, anxiety, depression, suicidal ideation, and substance use can be more persistent and debilitating than physical injuries (Dworkin et al., 2017; Kilpatrick et al., 2013; Loya, 2015; Scott et al., 2018; Ullman et al., 2013), and are also evidence of trauma.
While there was a tendency toward increased law enforcement reporting when patients were penetrated, it was not statistically significant (odds ratio [OR] = 2.36; p = .056). The proportion of non-penetrative sexual assaults was small in this sample (16.4%) and might have reduced power to detect a significant association. Penetration may be viewed as more traumatic and/or could produce more evidence in the form of DNA or anogenital injuries. However, it is also possible attempted penetration or non-penetration sexual assault are perceived by victims to be equally traumatic and worthy of reporting. Injuries might also be present in non-penetrative sexual assault, which could contribute to greater likelihood of reporting. Persons who were not penetrated might also be less likely to seek MFEs.
Being assaulted by a stranger did not predict law enforcement reporting in this study. Previous findings from retrospective studies found lower reporting rates if the victim knew the perpetrator (Chen & Ullman, 2010; Jones et al., 2009; Paul et al., 2014). Reasons for not reporting known assailants include fear of retaliation (Cohn et al., 2013) or being blamed (Wolitzky-Taylor et al., 2011), or not wanting the perpetrator to go to jail (Jones et al., 2009). Victims assaulted by known perpetrators may experience greater conflict about reporting and may need more time and support before making decisions about law enforcement reporting.
Neither patient nor assailant race/ethnicity were associated with law enforcement reporting in this sample. In the United States, sexual assault rates are similar between White non-Hispanic (2.2 per 1,000) and Black females (2.8 per 1,000), whereas White males commit the majority of sexual assaults (Planty et al., 2013). In general, perpetrators assault persons of their own race (Morgan & Oudekerk, 2019; Stacey et al., 2017). The proportion of non-White/Hispanic patients in this sample was small (22.8%), which could have limited the ability to find differences by race/ethnicity. Persons from minority groups may have negative attitudes toward law enforcement that could impact reporting behavior (Peck, 2015), though this could not be examined with current data. White women were more likely to report in a previous study (Chen & Ullman, 2010), and non-White women were less likely to report non-White assailants due to fear of law enforcement treatment of non-White assailants (Decker et al., 2019). Having multiple assailants was associated with higher law enforcement reporting in a prior study of patients reporting for MFEs (Jones et al., 2009), but not in another (Muldoon et al., 2018). Having multiple assailants has been associated previously with charges being filed (McGregor et al., 2002), making it is reasonable to assume victims might feel more supported by law enforcement when multiple perpetrators were involved. Having multiple assailants was not significant in the current sample, although the proportion of patients who were assaulted by multiple assailants was small (6.9%).
While the current data are mostly consistent with prior studies, nearly all prior studies relied on retrospective self-report. Data presented here provide insight into objective patient, assault, and exam factors associated with law enforcement reporting at the time of the MFE. One other study examined patients’ reporting decisions at the time of MFEs (Jones et al., 2009), though their findings were limited by selection bias: those who agreed to complete questionnaires regarding reporting decisions were three times more likely to have reported to law enforcement. Like the current study, a prior study also relied on retrospective chart review of victim, assailant, and assault characteristics (Muldoon et al., 2018). They found the only significant factors associated with law enforcement reporting were uncertainty regarding assailant identity and the assault location was outdoors. The authors conjectured the high prevalence of drug-facilitated sexual assault (DFSA) in their sample may have accounted for patients being uncertain of assailants’ identities, although DFSA was not associated with higher likelihood of reporting. The data in the current study did not include DFSA. However, the most common substance used to facilitate sexual assault is alcohol (Anderson et al., 2017). Alcohol use was prevalent in this sample and was associated with lower law enforcement reporting. Data about assault location were not collected by the SANE program in this study.
The primary limitation of this study is that data were obtained for programmatic purposes and many data forms were incomplete. Some information on data forms were not routinely obtained during MFEs. If the SANE did not specifically ask, or the patient did not volunteer the information, data were missing. Law enforcement reporting was higher in the sample with no missing values (60.9%–49.6%), indicating SANEs may have been more thorough if they knew patients were reporting. Penetration was also higher in complete cases than in either incomplete cases or all cases together. Patients who reported penetration might have recalled more assault details (i.e., were not highly intoxicated or unconscious) so SANEs were able to complete forms more thoroughly. Thus, there might be overlap between cases with incomplete data and cases involving alcohol, both of which were associated with lower reporting.
Data were also limited by being unable to determine whether patients voluntarily reported to law enforcement before presenting for the exam, or whether a third party contacted law enforcement. However, prior data suggest reporting by third parties is low, at about 7% (Chen & Ullman, 2010). It is also not known whether patients ultimately reported. Prior studies examining factors associated with reporting that relied on retrospective data did not specify whether patients received MFEs. It is possible victims who have MFEs are more comfortable with disclosure, have already decided to report, and/or have fewer concerns about some factors previously identified as barriers to reporting.
These data are not generalizable to every SANE program. SANEs were available at two study hospitals, which were both in a university town with a population that is younger and includes more students than in many other communities with SANE programs. The community had an active sexual assault response team (SART) and residents might have been more aware of sexual assault services. Advocates were almost always present at exams to support patients, which could have impacted patients’ reporting decisions (Campbell, 2006). This sample was also mostly White non-Hispanic, which meant all patients who were non-White and/or Hispanic were combined for analyses, limiting the ability to examine whether race and ethnicity were associated with law enforcement reporting (Shaw & Lee, 2019). Males were also excluded from analyses.
As analyses relied on existing program record data, other variables previously found to be associated with law enforcement reporting were not available. For example, DFSA has been associated with lower reporting (Wolitzky-Taylor et al., 2011), and use of physical force has been associated with higher reporting (Chen & Ullman, 2010). The ways SANEs and law enforcement interact during MFEs varies between states and programs and can also impact reporting. For example, some states (e.g., Texas) require law enforcement to sign requests for MFEs before programs can be reimbursed, making it more likely patients will interact with them at the time of the exam. Some states (e.g., Utah) require health care providers to report all crimes, including sexual assault, although victims are not required to talk to law enforcement.
The primary purpose of MFEs is to provide health care. Medical forensic exams may be harmful if they if they detract from patients’ mental and physical health needs, or if they set unrealistic expectations about their value for successful investigation and/or prosecution (Corrigan, 2013). There is no guarantee having an MFE will lead to investigation or prosecution, or that reporting sexual assault will ensure case progression in the legal system (Campbell et al., 2009, 2014). One analysis showed that of 100 sexual assaults committed, five to 20 were reported to law enforcement, and fewer than 6% were prosecuted (Lonsway & Archambault, 2012). SANEs also cannot guarantee patients’ experiences with law enforcement will be positive (Dworkin & Allen, 2018; Patterson, 2011), and some SANEs may be concerned law enforcement officers will retraumatize victims (Maier, 2012). Sexual assault programs that are more prosecution-focused than health-focused can also result in less comprehensive medical care and lower patient satisfaction (Patterson et al., 2006). At the same time, SANEs are well-positioned to educate patients about reporting options and address barriers to reporting. SANEs provide a safe space for patients to discuss their assaults, which might help patients feel more comfortable participating in the legal process (Campbell et al., 2014), especially when advocates are present (Campbell, 2006).
It is also important for SANEs to respect that victims might have valid reasons for not reporting. SANEs can also educate law enforcement, prosecutors, and the public about misconceptions related to sexual assault that discourage reporting. SANEs can educate law enforcement about how sexual assault impacts victims and encourage them to use trauma-informed interviewing to minimize further trauma (Rich, 2019). Greater public education about the availability and purpose of MFEs might also encourage more victims to seek medical care. It is critical SANEs provide patients with all available options, including non-report and anonymous evidence collection, so they can report later if they do not want to report at the time of the exam (Heffron et al., 2014; Price, 2010). Findings from this study highlight how sexual assault evidence collection processes and reporting laws can impact victim reporting. The impact of laws regarding MFE procedures on law enforcement reporting should be carefully considered when advocating for changes.
Footnotes
Acknowledgements
The authors thank Pamela Terrill, MS, ARNP, SANE-A, for her assistance with providing de-identified SANE program data for this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.