
Abstract
Childhood sexual abuse (CSA) is a pervasive problem impacting a broad range of mental health outcomes. Previous research has shown that spiritual and religious (S/R) factors both positively and negatively relate to mental health issues among survivors of CSA, but mediating mechanisms of effect are unclear. The present study examined CSA, anxiety, depression, and positive/negative religious coping among 372 Jewish community members with and without CSA histories. Individuals who experienced CSA endorsed significantly higher anxiety and depression as well as negative religious coping than those without CSA. Negative religious coping mediated the relationship between CSA and anxiety and depression. We discuss clinical and social implications of these findings, including the need to address S/R factors in treatment of CSA, especially within religious communities. Further research examining abuser identity, survivors’ disclosure experience, and other S/R mediators of effect is warranted.
Prevalence of CSA
Childhood sexual abuse (CSA) is a pervasive problem affecting between 1% and 17% of men and 10% and 30% of women in the United States, and 3% and 29% of men and 7% and 36% of women worldwide (Finkelhor et al., 2014; Pereda et al., 2009; Stoltenborgh et al., 2011). Race and ethnicity do not appear to moderate risk for CSA, and prevalence rates for CSA are comparable among religious groups with strict rules regarding sexuality as well (Putnam, 2003; Spröber et al., 2014). At the same time, there is a paucity of research exploring the impact of sexual abuse in specific religious and ethnic minority populations, making it difficult to understand the effects of this kind of trauma on individuals from particular communities and backgrounds. It is therefore of utmost importance to study CSA within a cultural framework in order to understand factors that may underlie prevalence, disclosure, and effects on physical health and psychological well-being for survivors of abuse.
Regarding prevalence differences among various racial and ethnic groups, Putnam’s 2003 review of CSA research found that race and ethnicity did not appear to affect risk for CSA, though age, disability, socioeconomic status, and coming from a single-parent family did increase risk for CSA. Disability may render a child more vulnerable to several types of abuse because of lack of autonomy or power, while lower socioeconomic status and family structure may place children at a disadvantage because of a lack of resources or support (Putnam, 2003). Other studies, such as by Perez-Fuentes et al. (2013), found that individuals who endorsed CSA were more likely to be Native American or black than white and less likely to be Asian. Stoltenborgh et al. (2011) found that while the highest prevalence of CSA was reported for girls in Australia and for boys in Africa, ethnicity did not significantly affect prevalence rates except that African American boys reported more CSA than Caucasian boys in the United States and Canada. In another study of college-age women self-identifying as Latter-Day Saints, Mormon, Catholic, Protestant, or Other, which included Jewish, Muslim, and other religious affiliations, lifetime prevalence rates of CSA were comparable across participants regardless of denomination, with a total of about 13% of all participants reporting CSA history (Doxey et al., 1997). In a study of 1,005 Israeli adults, 25% (31% of females and 16% of males) endorsed a history of CSA (Schein et al., 2000). Most recently, a longitudinal study of 372 Jewish men and women in the United States and Canada found that 18% of men and 27% of women endorsed a history of any child sexual abuse (Rosmarin et al., 2018).
Though cultures with strict rules regarding sexuality and sexual restraint might exhibit more or less deviant sexual behavior; theoretically speaking, there may be an increase in abuse because of sexual repression, or lower rates of abuse because sexual acts are strongly forbidden. Kenny and McEachern (2000) cite the taboos in Hispanic cultures against girls losing their virginity before marriage and against boys’ homosexual experiences as factors that may contribute to lower rates of abuse, or reported abuse. Such taboos are not unique to Hispanic cultures, however; the widespread report of CSA within the Catholic church is likely one of the most well-known examples of how laws limiting sexuality do not necessarily prevent CSA (McLaughlin, 1994). This underscores what Sprober et al. (2014) note, namely that despite strong rules about sexual behavior, prevalence rates of CSA remain comparable across secular and religious groups. Overall, these studies indicate that CSA is a national and international problem that has affected anywhere between 4% and 36% of adults worldwide.
Cultural Context
In addition to prevalence rates, it is also important to understand the impact of CSA within a cultural context. For example, Latino girls who were sexually abused exhibit more emotional and behavioral problems than sexually abused girls who identify as African American or White (Putnam, 2003). Other studies demonstrate that the impact of CSA may be more universal. Overall, CSA survivors tend to endorse a higher prevalence of posttraumatic symptomatology than nonabused peers at baseline (Briere & Elliott, 1994; Deblinger et al., 1996; Steine et al., 2017). Furthermore, CSA is associated with many long-term problems and adverse mental and physical health outcomes, including anxiety, depression, substance use, sexual problems, self-injury, eating disorders, increased risk for revictimization or perpetration of abuse, and other interpersonal problems (Briere & Elliott, 1994; Finkelhor, 1990; Garnefski & Diekstra, 1996; Hornor, 2010; Maniglio, 2009; Polusny & Follette, 1995).
While many studies have compared the effects of CSA depending on gender, few studies examine the role of culture, race, or religion on the manifestation or occurrence of these problems. In addition to impacting a CSA survivor’s willingness to and/or likelihood of seeking treatment, cultural differences can influence the long-term impact of abuse on mental and physical health (Kenny & McEachern, 2000). While there are few significant differences across cultures, races, religions, or ethnicities, CSA must still be understood within a cultural context in order to understand the impact of culture on outcomes for survivors of CSA.
CSA in the Jewish Community
The present study sought to bridge this research gap specifically within the Jewish community. While there is a paucity of research on CSA within specific religious groups in general and the Jewish community in particular, existing research suggests that CSA occurs at similar rates among Jewish individuals as in the rest of society in both Orthodox and non-Orthodox sects (Blau, 2017; Mansbach-Kleinfeld et al., 2015; Rosmarin et al., 2018; Schein et al., 2000; Yehuda et al., 2007). And in the Orthodox Jewish community as well as among other religious minority populations with strict laws governing sexual behavior, prevalence rates are still high and comparable to secular groups (Resnicoff, 2012; Rosmarin et al., 2018; Spröber et al., 2014; Yehuda et al., 2007). Given the nearly universal prevalence rates cited previously, cultural factors likely contribute to lower rates of disclosure in certain groups, but do not necessarily influence whether or not CSA will occur. In fact, CSA is largely underreported in the Orthodox Jewish community because of stigma related to sexual behavior, and because of Jewish laws about reporting misdeeds within the community (Brofsky, 2017; Katzenstein & Fontes, 2017; Resnicoff, 2012). Due to the sensitive nature of the topic and impact of stigma on its exploration, research examining the impact of CSA in religious minority populations, such as the Jewish community, is therefore particularly important. Such research is also fundamental to understanding CSA in a cultural and religious context.
Effects of CSA
Impact of CSA on Mental Health
The World Health Organization defines mental health as “a state of wellbeing in which an individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and is able to make a contribution to his or her community” (WHO, 2018). As mentioned previously, CSA is associated with many short- and long-term mental health consequences, or effects on individuals’ psychological well-being, including symptoms of posttraumatic stress, depression, anxiety, substance use, and suicidality. In particular, children and adolescents who have experienced CSA are more likely than their peers to receive diagnoses of anxiety and depressive disorders, and commonly exhibit behavior problems in school and at home (Briere & Elliott, 1994; ; Devries et al., 2014; Garnefski & Diekstra, 1996; Hornor, 2010; Lindert et al., 2014; Maniglio, 2009; Neumann et al., 1996; Paolucci et al., 2001; Steine et al., 2017). In the Jewish community, CSA survivors have higher rates of treatment seeking for depression, anxiety, and other emotional and behavioral concerns (Yehuda et al., 2007). Furthermore in the Jewish community, CSA is linearly correlated with mental health concerns such that higher levels of CSA predict increased likelihood and severity of psychiatric diagnosis (Feinson & Meir, 2015; Rosmarin et al., 2018).
CSA, Spirituality, and Religion
Spirituality and religion (S/R) can affect outcomes for victims of CSA in both positive and negative ways (Bryant-Davis et al., 2012; Ganje-Fling & McCarthy, 1996; Jenkins & Pargament, 1995; Pargament et al., 1990; Smith, 2004). On the one hand, research demonstrates that S/R can provide positive coping mechanisms to help survivors overcome the adverse effects of trauma, and survivors who use S/R to grow and gain support are more likely to experience posttraumatic growth in the aftermath of CSA (Bryant-Davis et al., 2012; Gall, 2006). Along these lines, women with CSA histories who report higher levels of spiritual well-being experience lower rates of anxiety and mood disorders (Walker et al., 2009). At the same time, many CSA survivors report struggles in the domain of S/R including difficulty connecting to a faith community, difficulty trusting in God, and viewing God as more punitive or unfair (Ganje-Fling & McCarthy, 1996; Walker et al., 2009). All of these are collectively referred to in the literature as spiritual struggles, part of an effort to rescue one’s S/R from a place of conflict (Pargament et al., 2000). Religious coping is one way of grappling with difficult S/R questions and experiences. Generally speaking, positive forms of religious coping are associated with better psychological outcomes, whereas negative religious coping predicts greater distress, both in the general population (Ellison & Lee, 2010) as well as the Jewish community (Rosmarin et al., 2009b).
Clinical wisdom and some empirical studies suggest that religious coping can be utilized in the aftermath of CSA to help survivors make meaning of their experience and/or gain support from their religious community (Ahrens et al., 2010; Leitenberg et al., 1992), but little else is known about the role of religious coping in CSA. Importantly, the extant literature on S/R and mental health among CSA survivors has been correlational and failed to model mechanisms of why and how these variables may be connected. The present study therefore sought to explore these factors using a mediational model.
The Present Study
The authors’ decision to examine spiritual struggles, measured specifically by negative religious coping, as a mediator of the relationship between CSA and anxiety and depression was based on a theoretical model derived from the existing literature on these topics. Previous research has demonstrated that negative core beliefs about God, or higher levels of mistrust in God, can predict greater overall distress in both Jewish and Christian individuals (Rosmarin et al., 2009a). Additionally, in a study of 200 college students, difficulty forgiving God or maintained anger toward God predicted greater depression, anxiety, and anger, increased difficulty forgiving oneself and others, and negative impacts on religious beliefs and spirituality (Exline et al., 1999). Furthermore, Ellison and Lee (2010) found that in a community sample of 1,445 American men and women, divine struggles were the strongest predictor of overall psychological distress (Ellison & Lee, 2010). Additionally, with regard to our specific measure of spiritual struggles, positive religious coping tends to be generally related to lower levels of anxiety/depression whereas the reverse is true for negative religious coping (Krumrei et al., 2013; Pirutinsky et al., 2011). As such, we sought to identify these patterns specifically among individuals with and without CSA, and hypothesized that there would be significant differences in religious coping, anxiety, and depression among CSA survivors versus those without CSA, and that religious coping would mediate correlations between CSA and anxiety/depression.
Methods
Participants and Procedures
The present study examined data from a community sample of 372 Jewish men and women who participated in the Harvard Medical School Study on Judaism and Mental Health (Rosmarin et al., 2018). The parent study utilized anonymous, self-report survey instruments and assessments administered to adult participants in six waves over a three-year period. Participants were recruited via advertisements sent by a broad array of Jewish organizations and through snowball sampling. All materials asked for participation in a study on Judaism and mental health but did not discuss or describe anything related to sexual abuse, thereby decreasing the possibility of sampling bias (e.g., selective recruitment by participants with CSA histories). Participants were able to participate in the study if they self-identified as Jewish, were at least 18 years old, lived in the United States or Canada, were fluent in English, and had access to the internet (Rosmarin et al., 2018). Participants were allowed to skip waves and were not required to complete every measure, and they were eligible to receive up to $45 in Visa gift cards for participating. Additionally, each participant was assigned a random ID used to link responses throughout the study. This random ID was paired with an email held in a separate database. We asked that participants to create a new anonymous email for the purposes of the study such that anonymity could be maintained while keeping track of data across the waves of the study over three years.
As mentioned earlier, the larger Harvard Medical School study contained six waves, and participants received a prompt to complete study surveys twice a year or every six months over a three-year period. During the first wave, conducted between January 2013 and February 2014, participants completed an anonymous, over-the-phone, semi-structured interview regarding DSM-IV disorders. Participants then completed different self-report surveys about mental health, religion and spirituality, and religious practice. Data regarding CSA history was collected during Wave 5 of the study, conducted between January 2015 and June 2016, from 372 study participants. Sexual abuse history was not asked about until Wave 5 of the study because as a global study on Judaism and mental health, CSA was just one of many variables examined throughout the study. In order to reduce sampling bias and increase participants’ trust toward the researchers and comfort level with the study to increase response rates, the investigators chose to wait until two full years into the study to address this more sensitive topic with participants (Rosmarin et al., 2018). Depression, anxiety, and religious coping data were also measured during this wave. As such, the data for the present study was derived from the same time point, and all analyses were cross-sectional. Table 1 summarizes the demographic and religious affiliation characteristics for the entire sample (n = 372). Study participants were 69.9% female (n = 260), and ranged in age from 18 to 83 years (mean = 37.5, SD = 15.3). Participants were mostly White (n = 349) and living in the United States (n =350). Pair-wise deletion, in which cases with missing data were excluded from specific analyses, was used in the present study.
Sample Demographics.
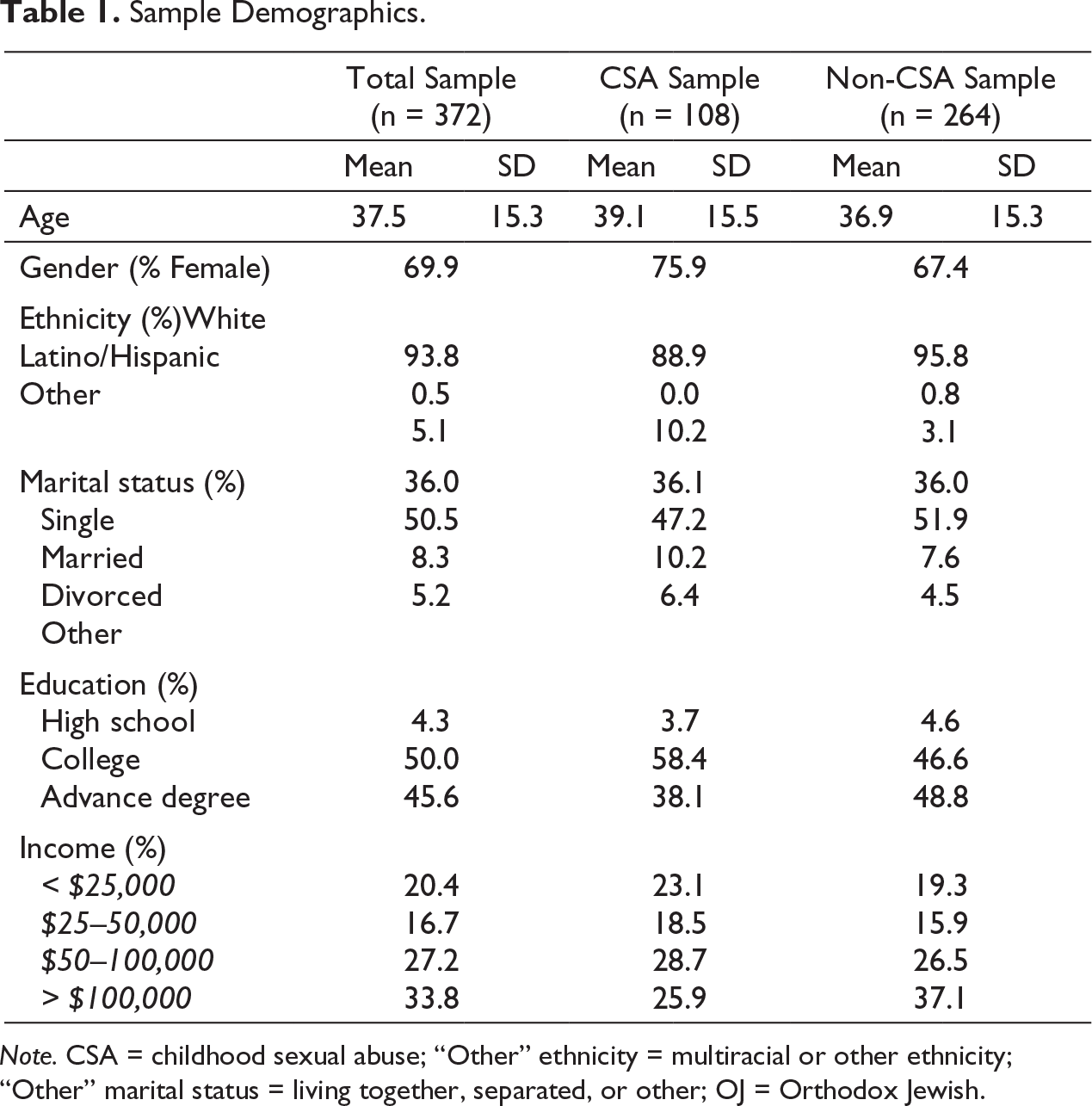
Note. CSA = childhood sexual abuse; “Other” ethnicity = multiracial or other ethnicity; “Other” marital status = living together, separated, or other; OJ = Orthodox Jewish.
Measures
Sexual abuse history. To assess participants’ sexual abuse history, a series of four questions adapted from Finkelhor et al. (2014) were used, asking whether the following kinds of unwanted experiences had occurred to the participant before the age of 18: (a) Being touched in an uncomfortable way, (b) being made to touch another person’s private parts involuntarily, (c) having one’s private parts (breasts or genitals) touched involuntarily, and (d) being subjected to involuntary vaginal, oral or anal sex. Participants were given the option of describing the CSA event(s) in more detail if they wanted to, however this data was not coded due to nonresponse by a significant minority of CSA victims and heterogeneity in responses. A prompt was provided at the start of the survey to remind participants that their responses were entirely anonymous.
Anxiety and depression. Anxiety and depression were assessed using the Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983). The HADS contains 14 questions regarding participants’ feelings and experiences in the last two weeks. Participants chose one of four responses to rate the degree to which each statement applies to them. This scale was originally developed for use in hospital outpatient mental health clinics and shows strong reliability and validity for measuring anxiety and depression for community samples (Crawford et al., 2001), including the present sample.
Religious coping and spiritual struggles. Religious coping was measured by the JCOPE, an adaptation of Pargament et al. (2000) RCOPE scale for the Jewish community (Rosmarin et al., 2009c). The JCOPE assesses the ways that Jewish individuals use religion to cope with stressful life events across positive and negative strategies. The scale contains 16 items (12 positive and 4 negative) on which participants rate how often they utilize various religious coping strategies to deal with stress on a 5-point Likert type scale (1: never; 2: hardly ever; 3: sometimes; 4: most of the time; 5: always). For example, items 2 “I get mad at God,” and 10, “I question whether God can really do anything” factor into the negative coping subscale, while item 4, “I try to see how God may be trying to teach me something,” and item 9 “I look for a stronger connection with God,” are part of the positive coping subscale. Reliability and validity of the measure are high within previous Jewish community samples, and the present sample as well. Given that multiple studies on religious and spiritual struggles have shown that doubt, anger toward God, and questioning God are all fundamental elements of what researchers collectively refer to as spiritual struggles (e.g. Exline et al., 2014; Stauner et al., 2016), the authors will hereon use the term “spiritual struggles” to refer to negative religious coping in this study.
Results
Consistent with previous research within the Jewish community, about a third of females and one quarter of males reported any form of CSA (n = 108; 33% female, 23% male). As illustrated in Table 2, correlations between variables suggested that CSA was significantly correlated with both anxiety (r = .12, p = .02) and depression (r = .12, p = .02). As expected, negative religious coping was significantly positively correlated with both CSA (.12, p < .05) and anxiety (r = .39, p < .001) and depression (r = .32, p < .001). However, positive Jewish religious coping was only significantly negatively correlated with anxiety (r = –.12, p = .007) and depression (r = –.19, p < .001), and not CSA. To further explore the relationships among CSA, anxiety and depression, and religious coping, four independent sample t-tests were conducted to compare differences in mean scores of depression, anxiety, and positive/negative religious coping between the CSA and non-CSA groups. As expected, participants who experienced CSA reported significantly more anxiety t(370) = 2.345, p = .020 and depression t(370) = 2.398, p = .017 than participants who did not endorse any abuse, with small but meaningful effect sizes (Cohen’s d = .27). Also as expected, CSA participants reported greater negative religious coping (t(343)= 2.061, p = .040, Cohen’s d = .24), but not positive religious coping. Results of these t-tests are depicted in Table 3.
Study Variable Correlations.
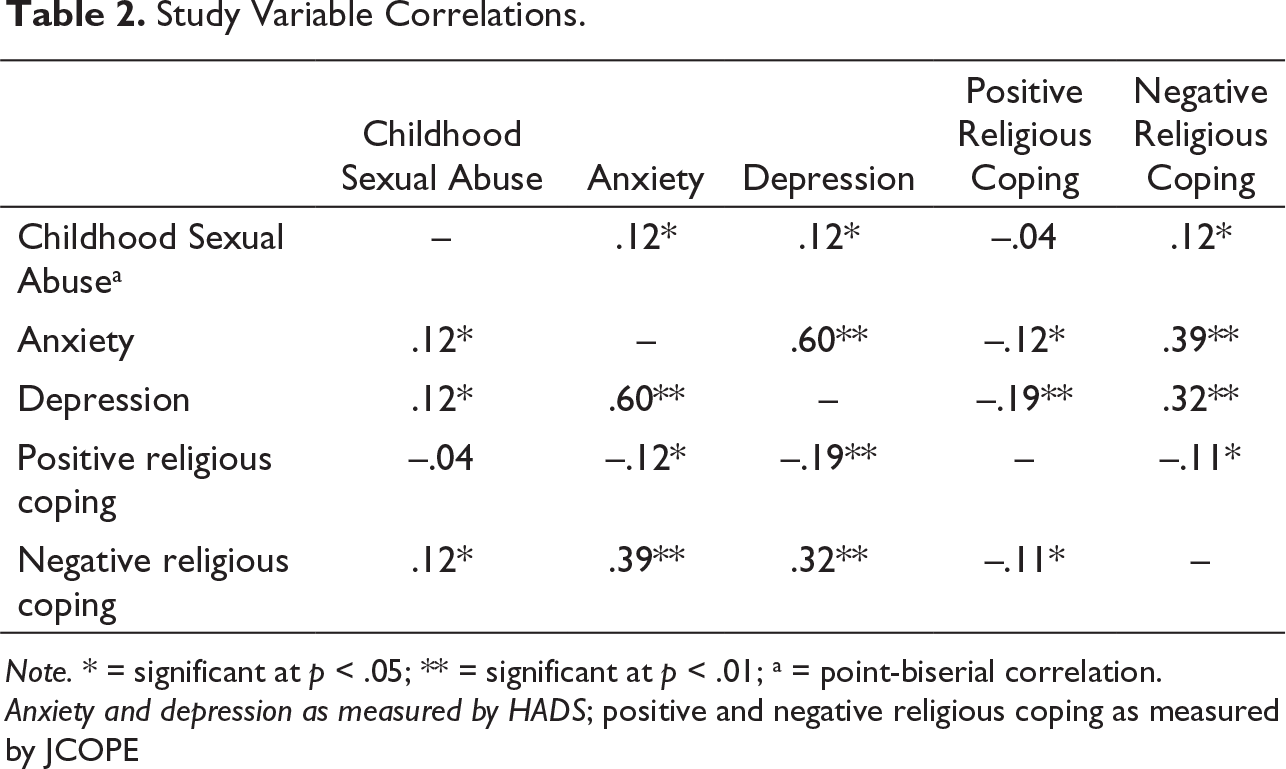
Note. * = significant at p < .05; ** = significant at p < .01; a = point-biserial correlation.
Anxiety and depression as measured by HADS; positive and negative religious coping as measured by JCOPE
Differences in Scores for Participants in the Abused and Nonabused Groups.
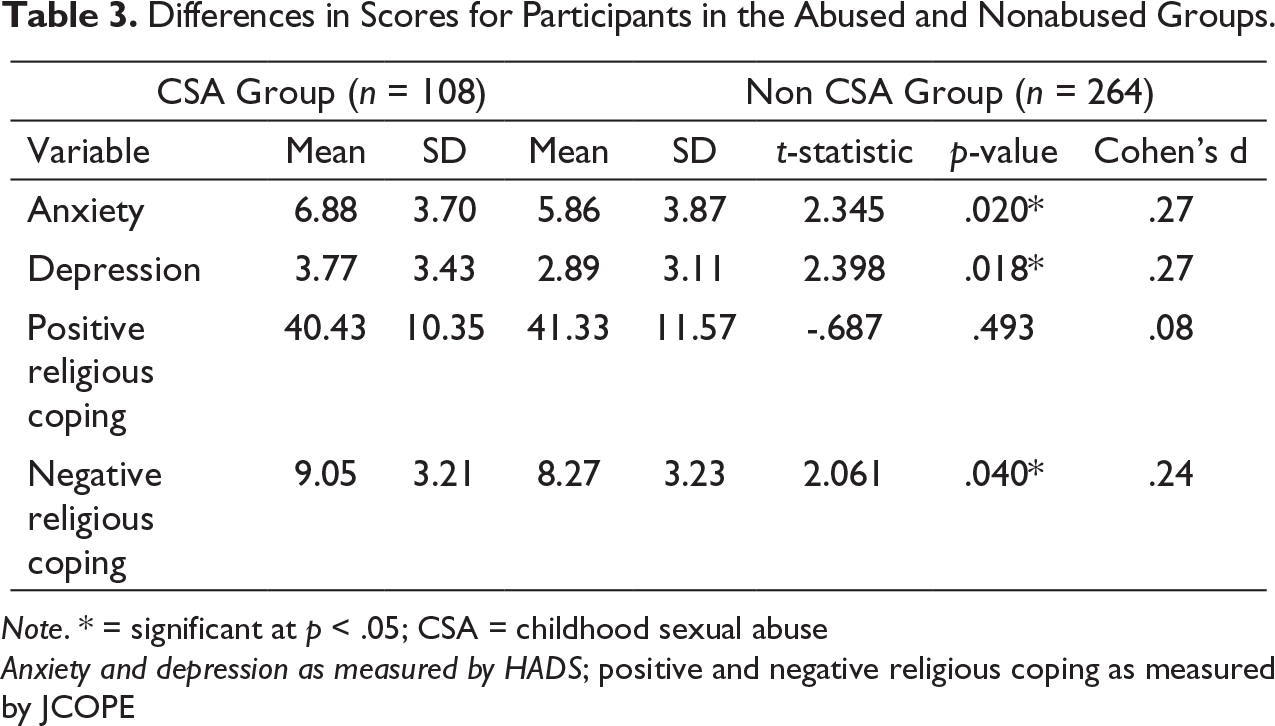
Note. * = significant at p < .05; CSA = childhood sexual abuse
Anxiety and depression as measured by HADS; positive and negative religious coping as measured by JCOPE
Given that only negative and not positive religious coping was significantly associated with depression, anxiety, and CSA, our mediation analyses focused exclusively on negative religious coping, or spiritual struggles. A linear regression was then conducted to test whether spiritual struggles mediated the relationship between CSA and anxiety/depression. Mediation analyses were conducted first for anxiety and then again for depression scores using the Process macro for SPSS (Hayes, 2017). As depicted in Figure 1, spiritual struggles as measured by the NCJOPE predicted anxiety when controlling for CSA (b = .449, t(358) = 7.72, p = .000) and accounted for 16% of the variance in anxiety scores with a small but meaningful effect size (R2 = .16, Cohen’s f2 = 0.183). Results based on 1,000 bootstrapped samples indicated that while the total effect of CSA on anxiety was significant (TE = 1.02, SE = .441, p= .02), the direct effect was not (DE = .629, SE = .413, p = .13). The indirect effect of negative religious coping on anxiety was significantly different from zero at p < .05 (two tailed).
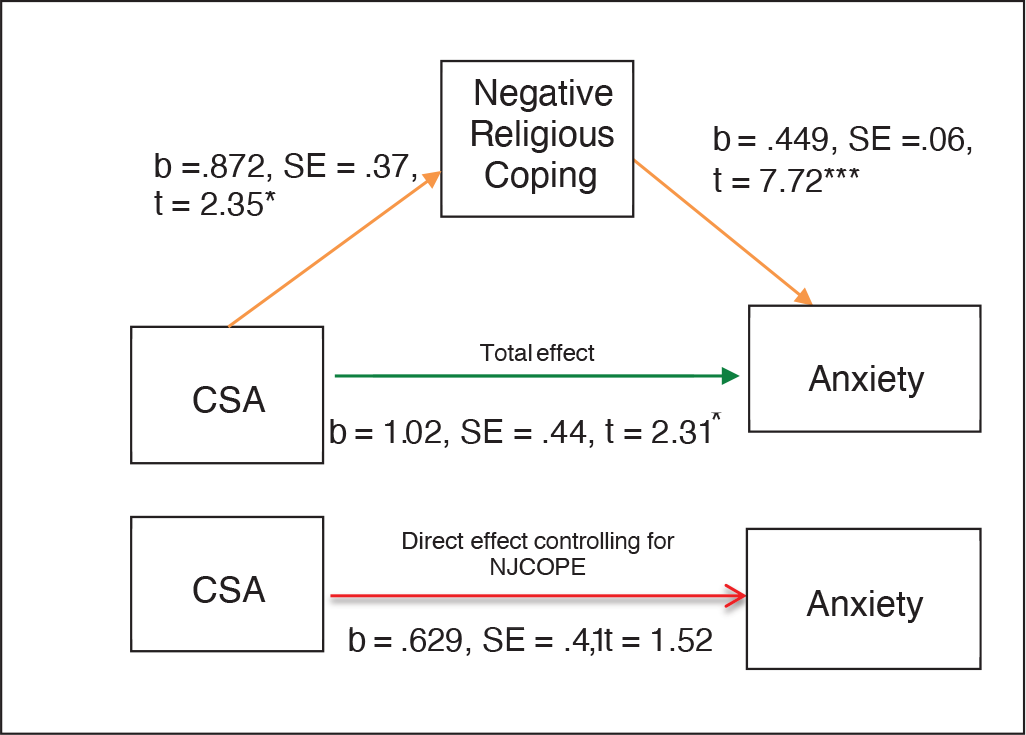
Note. *p < .05. **p < .01. ***p < .001.
With regards to depression, as depicted in Figure 2, spiritual struggles as measured by the NJCOPE also predicted depression scores (b = .312, t(358) = 6.20, p = .000) and accounted for 11% of the variance in HADS depression scores with a meaningful effect size (R2 = .11, Cohen’s f2 = 0.122). Results based on 1,000 bootstrapped samples indicated that while the total effect of CSA on depression scores was significant (TE = .825, SE = .372, p= .03), the direct effect of CSA on depression scores was no longer significant after controlling for negative religious coping (DE = .553, SE = .357, p = .12). The indirect effect of religious coping on depression was significantly different from zero p < .05 (two tailed).
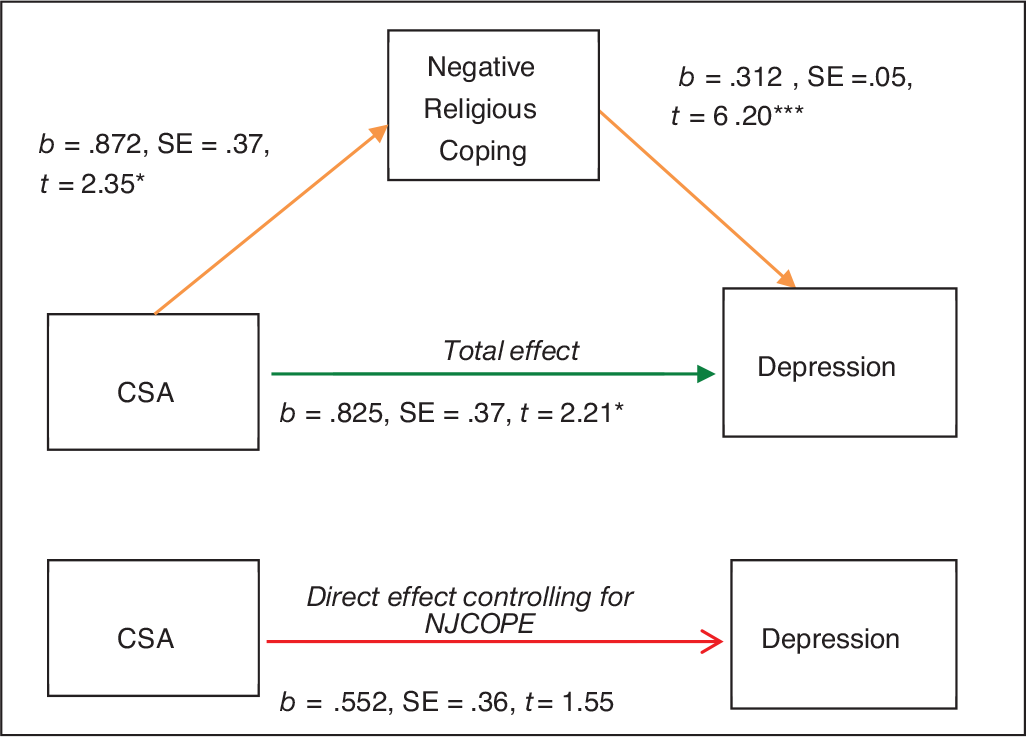
Note. *p < .05. **p < .01. ***p < .001.
Discussion
The present study examined relationships among CSA, anxiety, depression, and positive/negative religious coping within a Jewish community sample. As expected, CSA victims reported higher levels of anxiety, depression, and negative religious coping than those without a history of CSA. As well, spiritual struggles, as measured by negative religious coping, were significantly positively associated with CSA, anxiety, and depression, and mediated relationships among CSA and these aspects of mental health. As a whole, these results underscore the importance of spiritual struggles as a potential mechanism by which individuals with CSA develop anxiety and depression, at least in as much as can be demonstrated by cross-sectional research. It could be that CSA is a risk factor for the development of spiritual struggles, given that traumatic events could engender religious questioning along the lines of “Why did God allow this to happen to me?” Such normative religious questioning, if not addressed, could lead to lasting engagement with negative religious coping, which in turn could negatively impact mental health. In addition, spiritual struggles may engender culturally dissonant behavior, which may in turn create social risk factors for anxiety and depression. All of these possibilities warrant further research and evaluation, and longitudinal research is most necessary to examine these ideas further to understand the precise direction of these relationships.
Positive religious coping was associated with less anxiety and depression, but not CSA, and mediating effects were thus not present. Furthermore, individuals with and without CSA histories reported equivalent levels of positive religious coping. These results seem to suggest that individuals who have experienced CSA are equally likely to engage in positive religious coping behaviors as their peers without CSA histories, and furthermore that such engagement is equally relevant vis a vis mental health. With that said, it is notable that items on the positive subscale of the JCOPE primarily include behavioral aspects of religious involvement, such as praying, talking to one’s Rabbi, looking forward to Shabbat, and observing “Mitzvot” (Jewish religious commandments). Such aspects of faith, as well as the social connectivity that is intrinsically tied to these observances within Jewish religious culture (Cohen et al., 2005), may be particularly likely to persist among CSA survivors. On the other hand, internal aspects of religion such as faith, trust, religious values, and a sense of connection to God, may be more tenuous among those with CSA. Notably, the negative subscale of the JCOPE assesses for more internal aspects of religious life, such as getting mad at God, questioning whether God can help, and wondering whether God cares. Future research should seek to evaluate whether other aspects of (positive) religious involvement are predicted by CSA.
Clinically speaking, our results suggest that S/R should be assessed for and addressed in the treatment of anxiety, depression, and other mental health concerns among individuals with CSA particularly those from religious communities. The aspects of negative religious coping described earlier map onto general themes that are commonly discussed in Cognitive Processing Therapy for Trauma, which posits that trauma disrupts a person’s schemas about the world, himself, and others (Resick et al., 2016; Williams et al., 2011). Changes in religious schemas related to power, control, safety, trust, esteem, and intimacy, are entirely possible—if not likely—in the aftermath of trauma, and such themes are reflected in the JCOPE negative subscale. Put differently, it makes sense that those who experience CSA may question their religion more than those who did not, given that trauma impacts existing belief systems about oneself and the world. Our results suggest that this is not simply a spiritual or religious developmental process, as such struggles predict anxiety and depression, and mediate ties between CSA and these variables. In a similar vein, feelings of anger toward God may simultaneously result from CSA and serve as a cognitive risk factor for anxiety and depression. In their important study on anger and hostility in depressed individuals, Riley et al. (1989) found that individuals with depression endorsed significantly higher levels of anger, and tended to repress such feelings more than controls. Exline et al. similarly demonstrated that difficulty forgiving God predicts depressed mood (Exline et al., 1999). All of these findings underscore the potential clinical relevance of spiritual struggles among religious individuals with CSA, and the importance of addressing S/R factors in treatment.
The present study was limited by several factors. First, while the parent study included data collected over three years, the sexual abuse questionnaire was only administered at Wave 5 of the study. As such, all the data in the present study was culled from that wave, and as a result our analyses were cross-sectional rather than longitudinal. This may limit the reliability of replicating the meditational model in future longitudinal research given that there is some concern that cross-sectional examination of supposedly longitudinal processes can be problematic (e.g. O’Laughlin et al., 2018). Additionally, while the parent study can be viewed as longitudinal research, this study’s results do not provide an understanding of anxiety, depression, or spiritual struggles in survivors of CSA over time. At the same time, however, Koenig et al. (2019) and others have pointed out that S/R and mental health factors such as religious coping and anxiety/depression are dynamic constructs that can change over time, and as such their relationship to one another may be similarly dynamic (Koenig et al., 2019; Koenig et al., 2020). Therefore, while cross-sectional analyses are somewhat limited, we are confident that our results are still quite meaningful in capturing the relationship between these variables at a given time point.
A further limitation of our study was the exclusive use of self-report measures, though this was seen as necessary to preserve anonymity of participants, which was in turn viewed as integral to the study design given the sensitive nature of the topic area. As well, use of pair-wise deletion to address problems with missing data is a shortcoming of online research, but still a limitation of the study. Additionally, the S/R measures used presupposed belief in God as an entity, though participants were able to self-identify as Atheistic and/or refuse to complete any individual items or groups of items. As noted earlier, we also assessed for a limited range of S/R items and focused exclusively on anxiety and depression. Future studies should explore effects of CSA on other aspects of S/R and potential mediating effects on other facets of mental health and distress. Finally, we did not assess for many aspects of CSA including identity of the perpetrator, duration of abuse, and whether/how CSA was identified and handled by primary caregivers, all of which can potentially affect (both spiritual and emotional) outcomes for survivors of CSA. Lastly, though our study was exclusive to the Jewish community, this was also a strength given the paucity of previous research on CSA among Jews. As the stigma against both CSA and spiritual struggles in the Jewish community is quite strong, this research is especially important in exploring a phenomenon that is highly prevalent and yet not spoken about often enough. As there is little published research on CSA and S/R, especially among Jews, the present study stands as an important contribution. Future research should expand upon our findings and examine broader issues with special attention to these and other missing factors.
Examining the effects of CSA from both a spiritual/religious and psychological/emotional vantage point is a key component to clinically and culturally sensitive trauma research. The present study sought to contribute to an important gap in the literature on interpersonal violence within understudied populations such as the Jewish community, where stigma against both mental health and sexual abuse is highly prevalent. By exploring the mediating role of spiritual struggles in the impact of CSA on anxiety and depression on Jewish individuals, the authors hope to shed light on a global phenomenon affecting diverse populations in both universal and unique ways. It is our fervent wish that this and other studies enables researchers and clinicians alike to gain a better understanding of the impact of childhood trauma within a culturally competent context.
Footnotes
Declaration of Conflicting Interests
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Financial support was received from McLean Hospital development fund (#041537).