
Abstract
Patients with substance use disorder (SUD) who undergo treatment present a high prevalence of lifetime physical and/or sexual abuse. Studies about this phenomenon and the specific needs of patients with a history of abuse must be carried out to tailor treatment programs. The first goal of this article was to determine the prevalence of physical and/or sexual abuse among patients with SUD, and the second goal was to analyze the specific characteristics of these patients. A sample of 418 subjects was assessed to achieve the first goal and 104 subjects (52 with and 52 without a history of physical and/or sexual abuse) were examined to reach the second goal. All patients sought treatment for SUD in two Spanish clinical centers. The results showed that 15.5% of the sample had a history of physical and/or sexual abuse (42.3% of women and 9.9% of men). Patients with a history of abuse presented a higher need for SUD treatment in family and psychiatric areas and more psychopathological symptoms than patients without a history of abuse. According to this more serious profile, a patient-centered intervention considering the history of abuse is recommended. This will allow the specific needs of these patients to be met, thus improving SUD treatment success.
Introduction
A history of physical and/or sexual abuse is common in patients who undergo substance use disorder (SUD) treatment (Daigre et al., 2015; Fernández-Montalvo et al., 2015; Schneider et al., 2008). These patients present with worrisome rates of abuse comparing with the general population (Jakubczyk et al., 2014). This is mainly relevant in patients with SUD and comorbid disorders or dual diagnosis (De Waal et al., 2017). Rates of physical and sexual abuse in these patients range from 22.3% to 53.7% and from 9.7% to 22.7%, respectively (Daigre et al., 2015; Grundmann et al., 2018; Potthast et al., 2014). In a recent study carried out in Spain, 18% of patients with SUD in outpatient treatment had a history of physical abuse and 9.2% had experienced some type of sexual abuse (Fernández-Montalvo et al., 2015). These rates could be related to the use of substances as a coping strategy by people who have suffered a traumatic event, specifically interpersonal trauma to regulate negative emotions and consequences derived from that experience (Farley et al., 2004; Hawn et al., 2020; Khantzian, 1997; Ullman et al., 2013).
Patients with SUD who have suffered lifetime physical and/or sexual abuse present worse characteristics than those who have not experienced these traumatic events. Specifically, they show higher levels of alcohol and other substance consumption (Brems, et al., 2004; Clark et al., 2001; Danielson et al., 2009; Fernández-Montalvo et al., 2015; Schneider et al., 2008; Zaorska & Jakubczyk, 2019) and greater treatment needs in family, social and psychiatric areas of daily life (Daigre et al., 2015; Fernández-Montalvo et al., 2015; Lotzin et al., 2016). They also present a higher severity of psychopathological symptoms (Brems et al., 2004; Zaorska & Jakubczyk, 2019). In addition, patients with lifetime abuse and addiction problems have a greater risk of suicidal ideation and attempts (Darke & Torok, 2013; Fernández-Montalvo et al., 2019; Yuodelis-Flores & Ries, 2015). In summary, these studies show a higher severity associated with specific treatment needs.
On the other hand, some studies have found gender-based differences. In fact, Fernández-Montalvo et al. (2017) found that women who had suffered lifetime physical and/or sexual abuse were more likely to drop out of SUD treatment. This gender-related aspect is another gap for the treatment of SUD in women. Women present specific treatment barriers that difficult their access to an adequate intervention. Consequently, they seek treatment for SUD in minor proportion than men (Agterberg et al., 2020). Bailey et al. (2020) found that this is mainly relevant in women who have suffered histories of abuse.
In a recent meta-analysis, Parisi et al. (2021) found considerable gaps in the literature about effective treatments for individuals with lifetime abuse and SUD. Specifically, these authors highlighted the scarce number of studies that evaluate sexual abuse in SUD patients with standardized measures. In fact, in Spain there is only one study with these characteristics (Fernández-Montalvo et al., 2017). Thus, to fill this gap, more studies that evaluate the specific needs of SUD patients with a history of abuse should be carried out.
Therefore, the aims of this study were: (a) to explore the prevalence of physical and/or sexual abuse in patients undergoing treatment for substance addiction and (b) to analyze the specific and differential characteristics of patients with and without lifetime physical and/or sexual abuse in SUD treatment in Spain. According to the abovementioned literature, it is hypothesized that patients with SUD will present with a higher prevalence of lifetime physical and/or sexual abuse than the general Spanish population. Moreover, SUD patients with a history of physical and/or sexual abuse will show a greater severity of addiction and more associated problems than those without a history of abuse. Specifically, they will present more psychopathological symptoms, a higher prevalence of suicidal behaviors, and higher levels of maladjustment to everyday life.
Methods
Participants
The sample consisted of patients at the beginning of their treatment for SUD in the Proyecto Hombre Navarra (inpatient and outpatient) and ANTOX (inpatient) addiction programs in Navarra (Spain) between February 2017 and June 2019. These are cognitive behavioral-based programs that are geared towards abstinence.
This study took place in two different phases. For phase 1, related to the prevalence goal, the initial sample consisted of 418 consecutive patients. Every single patient who consecutively attended the clinical center during the selected period was considered for the study. The inclusion criteria were as follows: (a) meeting the diagnostic criteria for SUD according to the DSM−5 (American Psychiatric Association, 2013), (b) being older than 18 years, and (c) signing the informed consent to participate in the study. No patient was excluded, and, therefore, 418 subjects were included in the study. Of these, 82.8% were men (n = 346), and 17.2% were women (n = 72). The average age of the subjects in phase 1 was 39.5 years.
For phase 2, related to the comparison goal, one admission criterion was added to the previously mentioned criteria: presenting a history of physical or sexual abuse. Moreover, two exclusion criteria were included: (a) the existence of serious mental illness advising against participation in the study (e.g., psychotic disorders) and (b) a lack of knowledge of the Spanish language. According to these criteria, 52 patients (38 inpatients and 14 outpatients) were selected. To achieve a well-balanced sample size, an ad hoc comparison group of 52 patients without histories of physical and/or sexual abuse was formed (38 inpatients, 14 outpatients) using a table of random numbers. Thus, 104 subjects were included in phase 2. Of these, 70.2% were men (n = 73) and 29.8% women (n = 31). The average age of the sample in phase 2 was 40.1 years (SD = 12.2).
Instruments
The EuropASI (Kokkevi & Hartgers, 1995; Spanish version by Bobes et al., 1996) is the European version of the Addiction Severity Index (ASI; McLellan et al., 1980). It is a semi structured interview that assesses the need for treatment in addicted patients in seven different areas: (a) general medical condition, (b) employment and financial situation, (c) alcohol consumption, (d) use of other drugs, (e) legal problems, (f) family and social relationships, and (g) psychological state. Interviewer Severity Rates, which are directly related to the severity of consumption (López-Goñi et al., 2012; López-Goñi et al., 2010), have been used. The scores range from 0 (there is no problem and no need for treatment) to 9 (there is an extreme problem and the treatment is absolutely necessary). Moreover, some items of the EuropASI were used to obtain specific information about the presence of lifetime psychopathological problems in the sample (psychiatric scale: Items 3, 4, 6, 7, 8, 9, 10, and 10 A). For the assessment of lifetime abuse, two specific items of the family/social area of the EuropASI were used: 18B (“Has anyone ever physically abused you?”) and 18C (“Has anyone ever sexually abused you?”). The short-term test-retest reliabilities of the ASI severity ratings have been reported to be greater than or equal to .92 for all domains (McLellan et al., 1985).
The Symptom Checklist (SCL−90-R; Derogatis, 1992) is a self-report that assesses psychopathological symptoms. It is composed of 90 items, which are answered on a five-point Likert scale, from 0 (nothing) to 4 (extremely). This tool aims to reflect the symptoms of psychological distress over the last two weeks. It consists of nine primary symptom dimensions: somatization, obsession-compulsion, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. In addition, it has three global indices of severity: the Global Severity Index (GSI), which reflects overall symptom severity, the Positive Symptom Distress Index (PSDI), which indicates symptom intensity, and the Positive Symptom Total (PST), which includes the number of items answered with a score different from 0. The internal consistency ranges from .70 to .90. Cronbach’s alpha for the current sample ranges from .64 to .95.
The Maladjustment Scale (Echeburúa et al., 2000) reveals how each patient is affected in six different areas of everyday life: labor, social, leisure, partner, family and general. Scores for each area range from 0 (nothing) to 5 (extremely) on a six-point Likert scale. The total scale range is 0–30. Higher scores indicate higher levels of maladjustment. The internal consistency of the instrument is .94. Cronbach’s alpha for the current sample is .81.
Procedure
The ethics committees of the Universidad Pública de Navarra (PI−006/16), Proyecto Hombre Navarra (PHN2016-01) and ANTOX approved the protocol for this study. All participants signed informed consent forms.
For all patients, the assessment of addiction and psychopathological variables was carried out in two sessions at the beginning of the addiction treatment by psychologists specialized in addictions from each treatment setting. During the first session, sociodemographic data, history of physical and/or sexual abuse and EuropASI variables were evaluated. In the second session, the remaining instruments were completed. The interviewers supervised the administration of self-report measures and offered support if there was some doubt. In the cases in which patients reported histories of physical and/or sexual abuse, a more in-depth interview related to history of abuse was carried out in a third session. This interview was carried out by an additional psychologist who was specialized in the evaluation of trauma. This professional was specifically dedicated to the study data collection.
Data Analysis
Descriptive analyses were conducted for all variables. The distribution of missing data was studied and no significant differences were found between subjects with and without available data in each of the variables studied. Therefore, when some data were missing, the pairwise deletion method was selected; this method involves analyzing the available cases in each variable. In the bivariate analyses, comparisons between the groups with and without physical or sexual lifetime abuse were performed using χ2 or Student’s t-test for independent samples, depending on the nature of the variables analyzed. Effect sizes (Cohen’s d or Phi coefficient) were provided for all of the analyses. Regarding multivariate analysis, a logistic regression analysis (forward stepwise entry method) was conducted to determine which specific factors were the most important to differentiate between the two groups studied. In this analysis, the variables with statistically significant differences in the bivariate analysis were included. The variable entry criterion was set to 0.05, and the variable retention criterion was set to 0.10. Moreover, the Hosmer-Lemeshow test was used to assess the goodness of fit of this model. A difference of p < .05 was considered significant. All statistical analyses were performed using SPSS (vs. 25.0) software.
Results
Prevalence of Physical and/or Sexual Abuse (Phase 1)
The results showed that the prevalence of lifetime abuse was 15.5% (n = 63). Regarding the type of abuse, 12.8% (n = 52) of patients had experienced physical abuse and 6.7% (n = 27) of patients had suffered sexual abuse. Significant gender differences were observed (χ2 = 46.5; p < .001), with a moderate effect size (Phi = .339): the prevalence of lifetime abuse among women was 42.3% (n = 30), whereas the prevalence among men was 9.9% (n = 33). Regarding physical abuse, 9.0% (n = 31) of men and 29.2% (n = 21) of women had experienced it, with significant differences (χ2 = 22.3; p < .001) and a low effect size (Phi = .231). Related to sexual abuse, 1.5% (n = 5) of men and 30.6% (n = 22) of women had suffered it, with significant differences (χ2 = 85.5; p < .001) and a moderate effect size (Phi = .447).
Comparison Between Groups With and Without a History of Abuse (Phase 2)
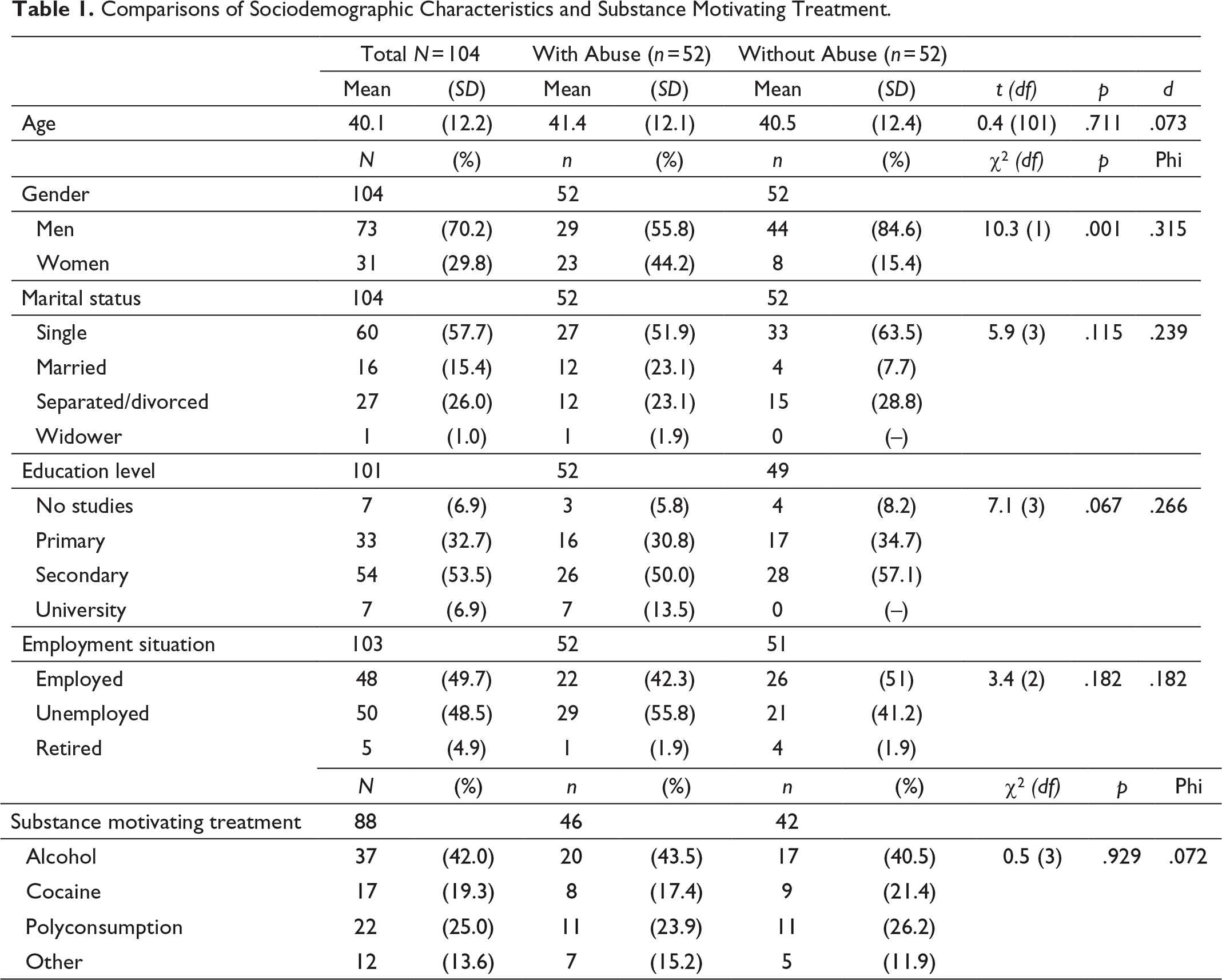
The results showed a differential profile between patients with and without a history of abuse. Regarding sociodemographic variables, only gender was significantly different between groups (Table 1). There was a higher rate of women in the group with a history of abuse than in the group without a history of abuse (χ2 = 10.3, p = .001).
Comparisons of Sociodemographic Characteristics and Substance Motivating Treatment.
Related to the severity of addiction, assessed by the EuropASI, the group with a history of abuse obtained significantly higher scores in the family (t = 3.8; p < .001) and psychiatric (t = 3.1; p = .002) categories than the group without a history of abuse (Table 2). Moreover, the group with a history of abuse presented a higher prevalence of lifetime anxiety (χ2 = 4.0; p = .045) and lifetime suicide attempts (χ2 = 4.71; p = .030), as well as a higher number of suicide attempts (t = 2.3; p = .026), than the group without a history of abuse.
Comparisons of the Severity of Consumption and Psychiatric Characteristics.
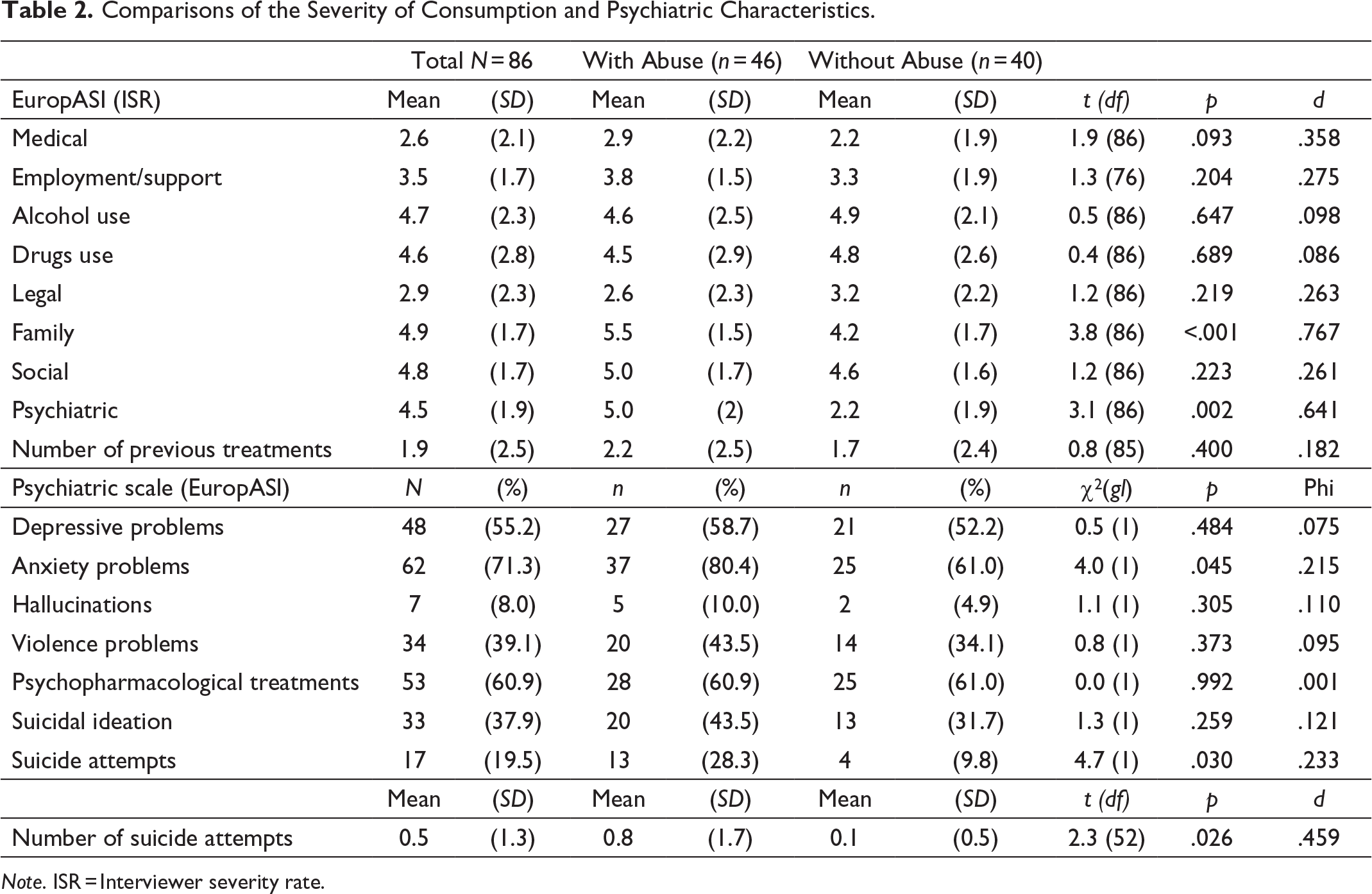
Note. ISR = Interviewer severity rate.
Patients with a history of abuse obtained significantly higher scores on the somatization (t = 2.6; p = .010), obsession-compulsion (t = 2.4; p = .016), depression (t = 2.7; p = .008), anxiety (t = 2.2; p = .008), GSI (t = 2.4; p = .018) and PSDI dimensions (t = 3.1; p = .003; Table 3), assessed by the SCL− 90-R. Finally, patients with a history of abuse obtained higher scores on social maladjustment than patients without a history of abuse (t = 2.3; p = .024).
Comparisons of Personality, Psychopathological Symptoms, Impulsiveness, and Maladjustment Characteristics.
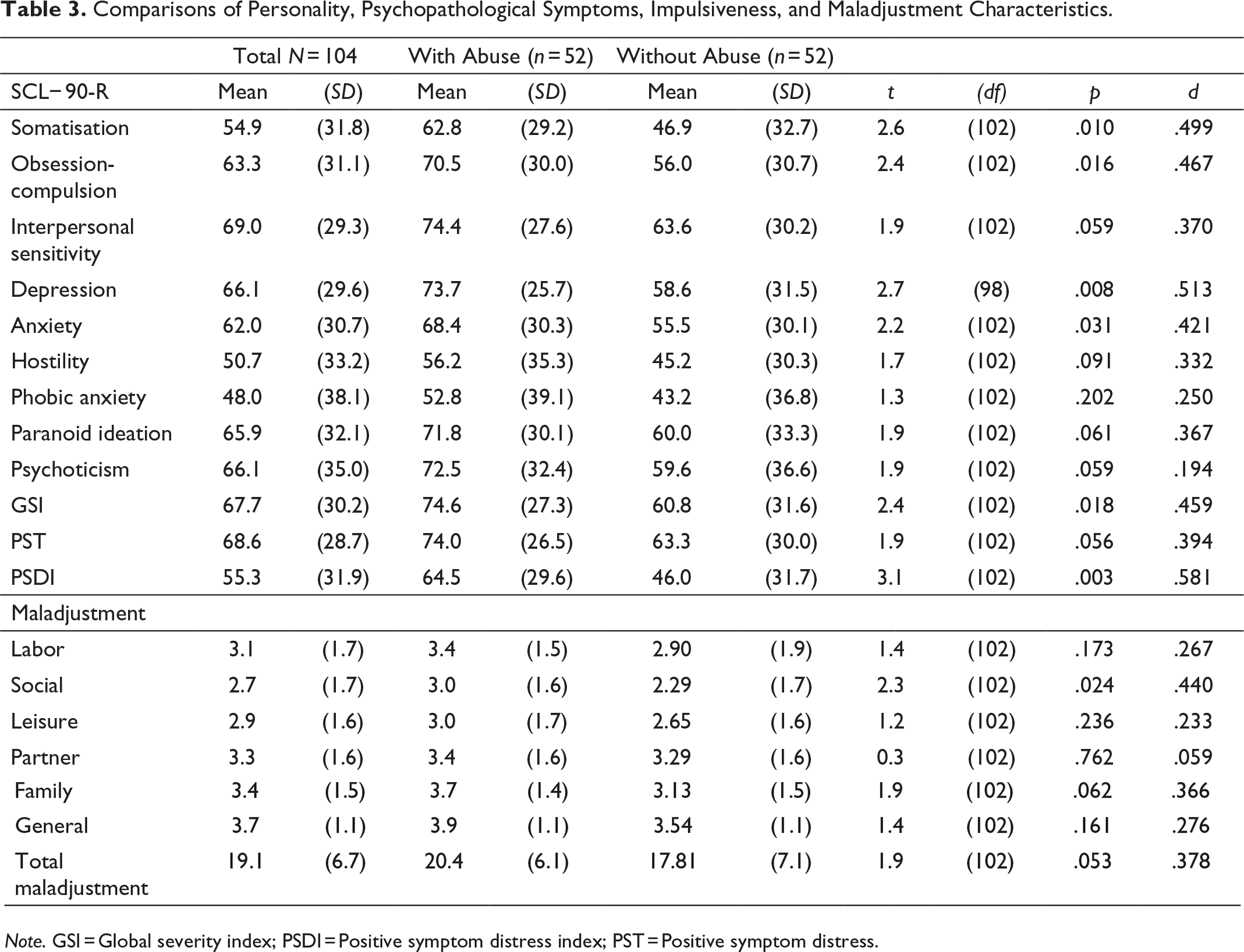
Note. GSI = Global severity index; PSDI = Positive symptom distress index; PST = Positive symptom distress.
Multivariate Analysis (Phase 2)
The logistic regression analysis showed that the three variables that best differentiated individuals with and those without a history of physical and/or sexual abuse were gender (female), the family scale of the EuropASI (higher score), and the social scale of the Maladjustment Scale (higher score). These variables explained 37.4% of the variance and correctly classified the patient’s history of physical or sexual abuse in 72.9% of cases (Table 4).
Multivariate Analysis (Logistic Regression).
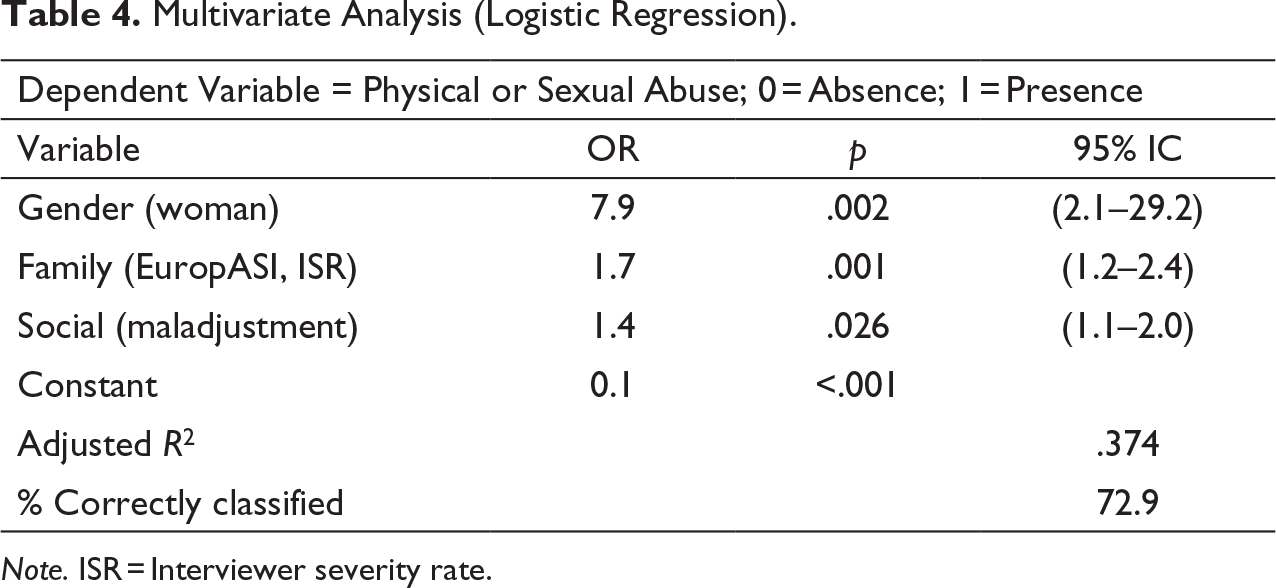
Note. ISR = Interviewer severity rate.
Discussion
This study was specifically aimed at assessing physical and/or sexual abuse in SUD patients and its correlates (severity of consumption, psychopathological symptoms, and maladjustment). A total of 15% of SUD patients had a history of physical and/or sexual abuse: almost half of women (42.3%) and only 1 out of 10 men (9.9%). Moreover, patients who had a history of abuse presented a more severe profile in some studied variables. These results confirm data from previous studies that have found a close relationship between a history of physical and/or sexual abuse and the severity of SUD, specifically in women (Brems et al., 2004; Daigre et al., 2015; Fernández-Montalvo et al., 2015, 2017; Pereira-Morales et al., 2017).
The prevalence of histories of abuse among patients in SUD treatment is high. In Spain, there is scarce information to compare this prevalence with the global rate of physical and/or sexual abuse in the general population. In an exploratory study of traumatic events, Olaya et al. (2015) estimated that 16.4% of the Spanish population had suffered various types of physical maltreatment and 2.6% of different diverse events of sexual abuse. According to these results, only the sexual abuse rate is higher in SUD patients than in general population. From a gender perspective, there is a greater prevalence of histories of abuse among women with SUD compared to men, which is consistent with previous research (Brems et al., 2004; Daigre et al., 2015; Fernández-Montalvo et al., 2015; Pereira-Morales et al., 2017), even though women continue to be vastly underrepresented in SUD services (Langeland et al., 2001). In this sense, women are particularly vulnerable to treatment barriers (Chen et al., 2020; Taylor, 2010), mainly those related to family responsibilities, relational factors, mental health, and stigma (Agterberg et al., 2020; Poole & Isaac, 2001). Moreover, women with addiction problems experience greater levels of perceived stigmatization compared to men (Agterberg et al., 2020; Brown, 2011).
On the other hand, in this study, patients with a history of physical and/or sexual abuse presented a higher need for treatment in family and psychiatric areas. These results have also been found in previous studies in Spain (Fernández-Montalvo et al., 2015) and worldwide (Daigre et al., 2015; Lotzin et al., 2016). These patients presented a greater maladjustment in the social area, which could indicate that social skills are underdeveloped and that it would be necessary to reinforce them. Most likely, due to their history of abuse, these patients have not based their coping skills in social relationships (Sullivan et al., 2017). In addition, patients with a history of physical and/or sexual abuse presented a greater proportion of lifetime anxiety problems and suicidal behaviors. Moreover, they showed greater psychopathological symptomatology. All these data are involved in a worse psychiatric status (Darke & Torok, 2013; Fernández-Montalvo et al., 2019; Yuodelis-Flores & Ries, 2015; Zaorska & Jakubczyk, 2019). These results are worrisome because the family and psychiatric areas are crucial for the progression of patients in SUD treatment and could jeopardize treatment completion. Therefore, persons without family support and with psychiatric problems need more intensive and accurate treatment in these areas in the context of patient-centered interventions (López-Goñi et al., 2012).
From a different perspective, being a woman and having greater family and social problems were the main variables related to the presence of a history of physical and/or sexual abuse among patients in these Spanish SUD treatment settings. This result also highlights the more severe profile in SUD patients who have suffered lifetime abuse (specifically in women), who present a greater deterioration in the family and social areas probably related to trauma consequences. In this sense, Bailey et al. (2020) have emphasized the need of addressing a trauma-informed practice in SUD treatment due to the high prevalence of women experiencing co-occurring substance use, histories of abuse, and symptoms of post-traumatic stress disorder. SUD treatments should be adapted to generate a patient-centered intervention that considers consequences of trauma that could deteriorate psychiatric, family, and social areas in these patients. In summary, it is necessary to evaluate lifetime physical and/or sexual abuse and to provide specific trauma interventions among SUD patients who undergo treatment.
This study presents some limitations. First, due to its exploratory and descriptive nature, neither the specific causal role of abuse in the development of SUD nor the relationship between physical/sexual abuse and treatment completion can be established. Future research should study how the differences between patients with and without physical and/or sexual abuse may influence the treatment completion rate. Second, this study included patients who sought treatment in two specific centers. This bias prevents generalizing the results obtained to all individuals with substance use problems. Future studies should include larger samples in other settings and countries. Third, the results of this study must be considered cautiously due to the limited sample size. Although they are promising, this is a preliminary study that sets the guidelines for further investigation. Finally, due to the high rate of histories of physical and/or sexual abuse found in women, a larger sample of women would be necessary to compare the results according to gender. These limitations might influence the findings and future research should consider them.
In conclusion, the specific assessment of physical and/or sexual abuse carried out in this study confirms the high relevance of these traumatic events and the greater severity in patients in SUD treatment who have suffered them. This serious profile supports the need to develop a patient-centered intervention that attends to the specific needs of these patients to improve SUD treatment success.
Footnotes
Acknowledgments
The authors thank the “Proyecto Hombre Navarra” and “ANTOX” programs’ staff for their help with assessing the clinical sample.
Declaration of Conflicting Interests
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant (code PSI2016-76511-R) from the Agencia Estatal de Investigación (AEI) of the Spanish Government and Fondo Europeo de Desarrollo Regional of the European Union (FEDER, EU).