
Abstract
The literature has shown a strong correlation between victimization and violence. As the majority of treatment programs for violence and the associated research have been focused on men, it is vital that services are also oriented to the needs of women who perpetrate violence. Beyond Violence (BV) was developed to fill the gap in violence prevention programming for justice-involved women with histories of violence victimization and perpetration. This randomized controlled trial reports the results of a peer-facilitated model of the BV program implemented in a women’s prison. Women volunteered for the intervention and the study. Participants were randomized to either the 20-session BV condition or to a waitlist control (WC) condition. All 145 participants were asked to complete a preintervention (Time 1) and postintervention (Time 2) survey that included validated measures to assess for depression, anxiety, PTSD, anger/aggression, and emotional dysregulation. Preliminary analyses of the background characteristics and preintervention outcome scores showed no significant differences between the groups at Time 1, indicating that randomization was successful. Separate ANCOVAs were run for 13 outcomes measured using the pretest scores from study participants as the covariate and group assignment as the independent variable. Hypotheses were predominantly supported, and findings showed that the BV participants had significant reductions in the majority of the outcome measures at the postintervention assessment when compared to the WC participants. Future research should continue to explore the advantages of peer-facilitated program models and should incorporate postrelease outcomes to assess change over time.
Introduction
I’ve been numb for so long. I felt safe in prison, for the first time. ~Beyond Violence participant, 2016
For over two decades researchers have consistently reported the high prevalence of lifelong trauma and abuse among incarcerated women (Browne et al., 1999; Jones et al., 2020; Kennedy et al., 2016; Messina et al., 2007, 2014). The literature predominantly outlines the negative impact of adverse childhood experiences (ACEs) such as physical and sexual abuse, and household dysfunction (e.g., incarceration of a family member, violence, substance use, and mental illness in the home). ACEs reported among justice-involved women have been retrospectively linked to an increased likelihood of adolescent conduct disorder, adolescent substance use and criminal activity, teen pregnancy, homelessness, prostitution, and interpersonal violence in adolescent and adult relationships (Grella et al., 2005; Messina & Grella, 2006; Reisig et al., 2006; Roos et al., 2016).
These childhood experiences are also significantly associated with the development of adult substance use disorders, mental health problems, and physical health problems (Karlsson & Zielinski, 2020; Kennedy et al., 2020; Messina et al., 2007; Messina & Grella, 2006). Additionally, exposure to ACEs has been associated with female-perpetrated violence against their partners and others (Babcock et al., 2003; Bair-Merritt et al., 2010; Kruttschnitt et al., 2002; Kubiak et al., 2017; Milner et al., 2010; Saxena & Messina, accepted).
The traumas suffered in childhood are often reoccurring and escalating throughout the lives of justice-involved women and can impact their recovery, validating the need for further research on women’s recovery needs and appropriate program development (Messina et al., 2020a). Moreover, victimization and violence often continue for women while in custody, as they may suffer sexual and physical abuse from interpersonal relationships they have formed in prison, from conflict with other residents, and from custody officers (Owen, 1998; Owen et al., 2017). Thus, the violence and trauma experienced in women’s childhood, adolescence, and adult life often continues in their custodial life. The corrections field has recently begun to better understand the relationship of ACEs with adult mental health issues, anger, aggression, and conflict, and that it is imperative to provide trauma-focused programs to address antisocial behaviors while creating a safe environment for both staff and residents.
Understanding Female Perpetrated Violence
The overlapping prevalence of childhood victimization and household dysfunction as potential precursors to violent and aggressive behavior by women has been of recent interest among criminologists and clinicians. Milner et al. (2010) contend there is an intergenerational cycle of abuse and found that women’s victimization in childhood was associated with later perpetration of abuse against their children. Saxena and Messina (accepted) found that when 1,113 incarcerated women self-reported specific types of childhood victimization, they also reported increased percentages of the same types of adult perpetration. For example, prior to the age of 18, 66% of the women reported that they had been victims of minor physical abuse (e.g., hitting, slapping, restraining) and 63% reported severe physical abuse (e.g., choking, burning, punching). Of those, 61% reported perpetrating the same forms of minor physical abuse and 58% reported perpetrating severe physical abuse on another as an adult.
Childhood victimization has also been found to be associated with female perpetrated intimate partner violence (IPV). In a sample of women participating in a pretrial supervision program, child sexual abuse, in particular was found to be associated with general aggression and perpetration of severe IPV (Trabold et al., 2015). A meta-analysis reported that female-perpetrated IPV is common (Archer, 2000), often with the same degree of severity and injury as male-perpetrated abuse (Carney et al., 2007). However, research has shown that women’s IPV is associated with their partners’ perpetration of aggression against them (Allen et al., 2009; Graves, et al., 2005; Magdol et al., 1998). Magdol et al. (1998), who reported findings from a birth cohort study, showed that women who were victimized by their partners were 13 times more likely to be perpetrators of violence in intimate relationships than nonvictimized women. Langhinrichsen-Rohling et al. (2012) conducted a review of 18 studies comparing men and women’s reported motivation for IPV (i.e., power/control, self-defense, anger, jealousy, poor communication, and retaliation) and very few gender-specific motives for perpetration emerged; however, the studies methodologies varied extensively.
There is some evidence among incarcerated women that anger may play a mediating role in the relationship between sexual victimization, interpersonal violence, mental health, substance use disorders, and the perpetration of violence (Kubiak et al., 2017; Maneta et al., 2012). Kubiak et al. (2017) used structural equation modeling (SEM) to assess associations between childhood adversity and perpetration of violence toward partners and others. Victimization, mental illness, substance use, and anger served as mediators in the model. There were no direct effects of mental illness or substance use on perpetration; however, there were significant indirect effects through anger, suggesting that these variables are strongly intertwined. Saxena and Messina (accepted) found that criminal justice involvement before the age of 18 and early experiences with varying forms of abuse also significantly increased women’s perpetration of violence against both intimate partners and others. Regression analyses among 1,118 incarcerated women revealed that multiple types of abuse as a minor, arrest as a minor, and substance use, increased women’s risk of engaging in minor and severe violence as an adult.
Mental health issues (e.g., depression, anxiety, PTSD) have also been found to be strongly correlated with both IPV victimization and perpetration, particularly in criminal justice samples (Goldenson et al., 2007; Leisring et al., 2003; Logan & Blackburn, 2009; Spencer et al., 2019). Kirby et al. (2012) found that women exhibiting PTSD symptoms have higher rates of committing IPV and general violence than women without PTSD. A more recent study suggests that PTSD symptomology may play both a central and mediating role in the pathway from ACE exposure to physical violence perpetration (Jones et al., 2020). Thus, it is not surprising to find literature consistently reporting the high rates of mental illness among incarcerated women. There is also some evidence that poor emotional regulation resulting from childhood victimization is associated with IPV perpetrated by women. Stuart et al. (2006) conducted a pilot study among 87 women in violence intervention programs and assessed the primary reasons for violence perpetration. Self-defense, poor emotional regulation, provocation by the partner, and retaliation for past abuse were the most common reasons for violence perpetration.
Although it is crucial to explore all factors associated with male and female patterns of violence and aggression, it is clear, that ACEs have been shown to increase the risk of women’s trajectories of violence (Olatunji et al., 2010; Orth & Wieland, 2006). Yet, historically services for incarcerated women have been based on the needs of men, despite incarcerated women having very diverse and complex problems in comparison (Bloom et al., 2003; Drapalski et al., 2009; Green et al., 2005; Owen, 1998; Owen et al., 2017; Pelissier et al., 2003; Saxena et al., 2014). IPV prevention often focuses on discontinuing repeat patterns of adult violence for men. However, IPV and victimization during the life course are not isolated incidents in women’s lives. Often victimization becomes a pattern for women, occurring in childhood, repeated from relationship to relationship, and then a contributing factor to the use of aggression toward partners and others (Kubiak et al., 2017; Rivera et al., 2014; Saxena & Messina, accepted).
Rigorous research has shown that when interventions target the unique needs of women (i.e., being gender-responsive, trauma-specific, and relational) behavioral and criminal justice outcomes can be improved at various levels of supervision; including measures beyond abstinence and recidivism; and when compared to gender-neutral or mixed-gender programs (Greenfield et al., 2007a, 2007b; Messina et al., 2016, 2014, 2012, 2010, 2020a; Messina & Zwart, 2021; Prendergast et al., 2011). This growing body of literature outlines the positive impact of theoretically based and trauma-specific programs for incarcerated women with substance use disorders, co-occurring mental health issues, (Messina et al., 2010; Saxena, et al., 2014), and histories of violence (Kubiak et al., 2014; Messina et al., 2014, 2016, 2020b). Thus, gender-responsive and trauma-specific interventions that increase successful relational behaviors while decreasing victimization and perpetration of violence among justice-involved women are needed to enhance success upon release and overall well-being.
Beyond Violence: A Prevention Program for Women (Covington, 2015)
More than 6,500 women currently reside in California’s state prisons, with two-thirds serving lengthy or life sentences for violent crimes (Bureau of Justice Statistics, 2020). There are limited interventions that are responsive to women’s unique pathways to perpetration of violence and aggression. Beyond Violence (BV) was developed to fill this gap in programming for justice-involved women. BV is a 20-session violence prevention program that considers the complex interplay between individual, relationship, community, and societal factors. It addresses the factors that put people at risk for experiencing or perpetrating violence. This is a psychoeducational program that teaches women about the role past trauma has played in their lives including the violence they have experienced, as well as the violence they have perpetrated. This model is used by the Centers for Disease Control and Prevention (CDC) and World Health Organization (WHO) and was used in the Prison Rape Elimination Act (PREA) research on women in prison (Bloom et al., 2004).
BV has been implemented in a variety of criminal justice settings and facilitated by both trained program staff and peer mentors. Multiple studies exploring the efficacy of the program have been conducted. Kubiak et al. (2012) utilized a single group pre- and post-test design to assess whether 35 women participating in the BV program delivered in a Residential Substance Abuse Treatment (RSAT) unit of a women’s prison in a midwestern state experienced improvements in mental health, reductions in anger, aggression, and behavioral conduct problems. Findings from this pilot study showed that the program participants experienced significant declines from the pre- and post-test, with large to moderate effect sizes, in symptoms associated with depression (d = 0.70), anxiety (d = 0.88), and PTSD (d = .50) as well as a measure of serious mental illness (d = 0.67) (Kubiak et al., 2012).
In a randomized controlled trial, Kubiak and colleagues expanded on their pilot study and compared the 20 session BV intervention with a 44 session Assaultive Offender Program (AOP), both delivered by trained clinicians in the general population of a women’s prison in the midwestern region of the United States (Kubiak et al., 2015). The 28 women were convicted of a violent offense and required to participate in a violence prevention program during their incarceration. While both groups experienced improvement in anger and mental health, women randomized to the BV intervention had stronger declines in anxiety (F = 5.32) and state anger (i.e., outward expression or control of others) (F = 8.84) than women in AOP. Furthermore, a longitudinal follow-up study showed that the women who participated in the BV program were significantly less likely to recidivate (i.e., arrest or time in jail) than women who participated in the AOP program during the first 12 months following their release from prison (Kubiak et al., 2016).
In 2015, the BV program was implemented in two women’s prisons in California utilizing peer-facilitators instead of trained staff members. Pre- and post-intervention data was collected from the 29 peer-facilitators initially and subsequently their 62 program participants. The 29 peer-facilitators selected and trained to facilitate the BV program were generally women serving over 20 years to life. The 62 participants had been incarcerated for an average of 14 years. The pilot evaluation of the peer-facilitated BV program used a single-group pre- and post-test design and revealed significantly positive outcomes, with moderate to high effect sizes, on reductions in PTSD, anxiety, anger and aggression, and symptoms of serious mental illness among the facilitators and the participants (Messina et al., 2016). Significant changes were found for 10 of the 13 outcome measures for the facilitators and the majority of the effect sizes were over (Cohen’s d =.70). The peer-facilitators effect sizes ranged from (Cohen’s d =.43) for reductions in anger to (Cohen’s d = 1.04) for reductions in hostility and aggression. Significant changes were found for 12 of the 13 outcome measures for the participants and the majority of the effect sizes were over (Cohen’s d = .40). The participants effect sizes ranged from (Cohen’s d = .26) for reductions in verbal aggression to (Cohen’s d = .57) for instrumental anger (i.e., anger used to manipulate or threaten others).
Current Study
This current study builds upon the prior work of Kubiak et al. (2012, 2015) and Messina et al. (2016) by employing an experimental design to rigorously assess the impact of the peer-facilitated model of the BV program on mental health and anger/aggression. The current study further includes extensive baseline indicators of histories of victimization and perpetration of violence and an additional outcome measure assessing emotional regulation. Specifically, a sample of 145 women incarcerated in California were randomized to the BV program or to a waitlist control group (WC) and given a pre- and post-survey. Based on the pilot study findings and the previous experimental research on BV, it was hypothesized that BV participants, relative to the WC group, would demonstrate the following:
Hypothesis 1. Lower levels of depression, anxiety, and PTSD at the postintervention assessment. Hypothesis 2. Lower levels of anger and aggression at the postintervention assessment. Hypothesis 3. Lower levels of emotional dysregulation at the postintervention assessment.
Methods
Participants
Background Characteristics by Group.
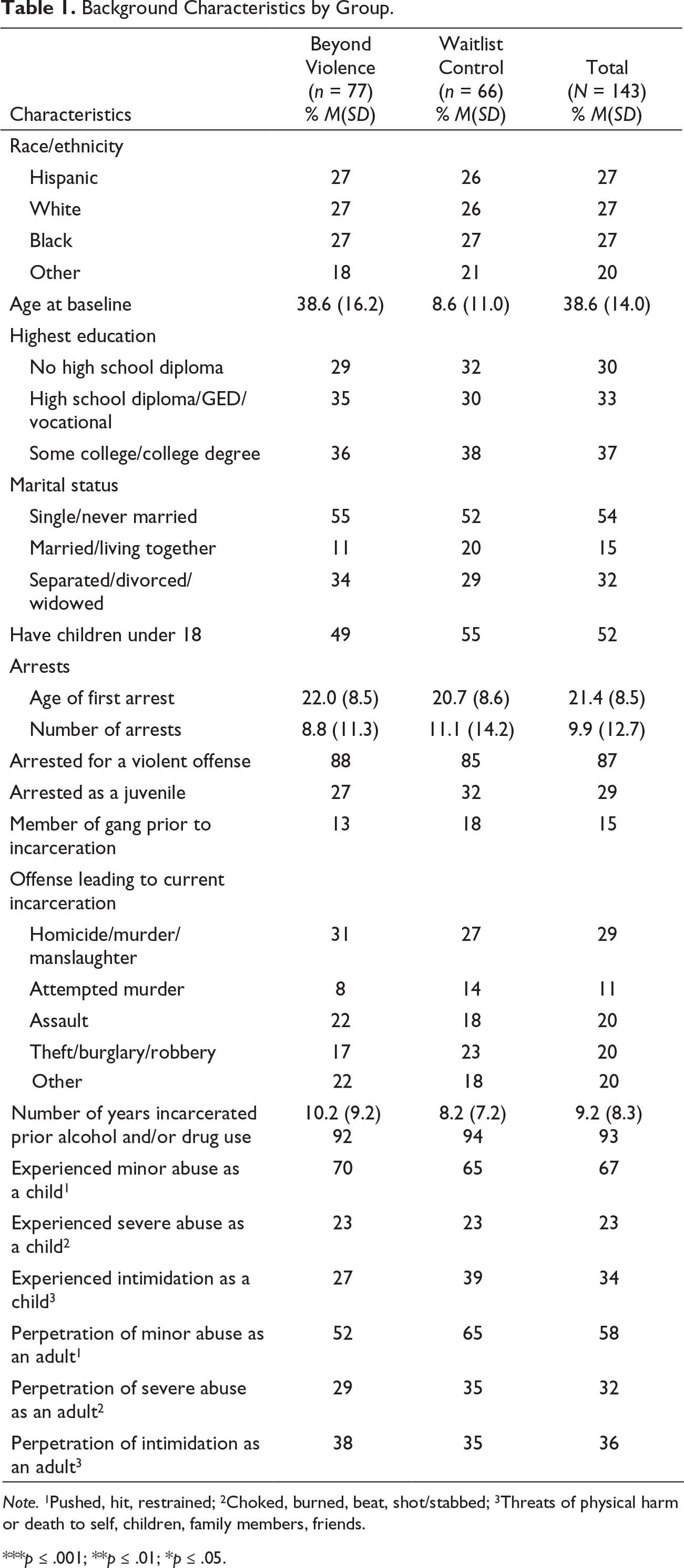
Note. 1Pushed, hit, restrained; 2Choked, burned, beat, shot/stabbed; 3Threats of physical harm or death to self, children, family members, friends.
***p ≤ .001; **p ≤ .01; *p ≤ .05.
Prior to the age of 18, approximately 67% of the study participants reported that they had been victims of minor physical abuse, 23% reported being victims of severe physical abuse, and 34% reported being victims of threats and intimidation. With regard to being the perpetrators of these behaviors as adults, 58% reported perpetrating minor physical abuse as an adult, 32% reported perpetrating severe physical abuse as an adult, and 36% reported being the perpetrator of threats or intimidation as an adult. No significant differences were found between the two groups at baseline.
Procedures
Procedures for this study were reviewed and approved by the University of California, Los Angeles, Institutional Review Board, the U.S. Department of Health and Human Services, Office for Human Research Protections, and the California Department of Corrections and Rehabilitation’s (CDCR) Research Oversite Committee prior to any contact with participants. Enrollment for this study took place from December 2017 through January 2019.
BV program content and delivery. BV is 20-sessions and utilizes a trauma-informed and gender-responsive approach, is based in rational-cultural and trauma theory, and uses a variety of evidence-based techniques (e.g., expressive arts, mindfulness, and guided imagery) to address the interrelationship between trauma, mental health issues, substance use, and anger regulation. BV consists of a facilitator guide and a participant workbook (Covington, 2015). The curriculum content is organized into four modules: Self, Relationships, Community, and Society. Fidelity to the intervention curriculum and feasibility of implementation within a women’s prison setting are discussed extensively in (Kubiak et al., 2014).
A peer-facilitated program model was delivered to 145 women participants and was comprised of six, 2.5-hour group sessions delivered twice weekly (with some interruptions due to prison lock downs or other institutional restrictions). Based on the content focus on past and current trauma and violence, the program was restricted to small, closed groups of 6-10 participants (i.e., participants who began the program together, ended the program together, without the disruption of new participants entering during the program cycle).
Peer facilitators and program coordinators. Typically, 20-25 peers were trained by the BV program author to facilitate multiple simultaneous groups with the goal of graduating 240 women per a year (Covington, 2015). Groups were cofacilitated by the same team of two peers during the 10-week cycle. A Program Coordinator was hired and also trained by the program author and provided oversight and coordinated of all aspects of programming, graduations, documentation of attendance, and access to research staff for data collection. The Program Coordinator was also available to peers and participants who needed any additional support. Peer facilitators were interviewed, chosen, and paired by the BV Program Coordinator. Criteria for the BV peer facilitator position included having the ability to connect with other residents, having social influence, previously holding positions as mentors, and being available during programming hours. Facilitation of the BV program was approved to be a paid position.
All peer facilitators were initially required to participate and graduate from BV, led by the Program Coordinator before facilitating the program to others. It should also be noted that only the peer facilitators and participants were in the group rooms. The Program Coordinator, custody officers, and other prison staff did not interrupt the groups unless of an emergency. Privacy and confidentiality of the groups was fully supported by the institutions. The peer-facilitators were women serving life or long-term offenders serving more than 20 years (the majority were incarcerated for homicide—66%). On average, peer-facilitators were 43.6 years old (SD = 10.59), and had been incarcerated for 16.4 years, (SD = 7.74). Thirty-two percent of facilitators were Black, 27% were White, 19% were Latina, and 22% were multiracial. Over two-thirds completed some college, and a quarter held a college degree obtained during incarceration.
Sample Recruitment and Randomization
Flyers advertising the BV program were posted by the Program Coordinator in the housing units at the prison. All women who signed up to participate in the BV program during the study period were eligible to participate in the study. With the assistance of facility staff, the Program Coordinators arranged access to those who signed up prior to the first session of BV to research staff. The research staff member explained the study, answered questions, and read the IRB-approved consent form to the participants describing the study, the measures used to protect the confidentiality of the responses, and the voluntary nature of the study. Research staff and provided the informed consent form to volunteers in a private room in the prison. There were no ineligibility criteria; however, participants were required by the facility to complete all of the sessions to graduate and receive rehabilitative achievement credits. They could participate in the program and decline to participate in the evaluation with no penalty.
Randomization was based on the last digit of participants’ CDCR identification (ID) number, which is randomly assigned to upon entry into the prison system. Those with IDs that ended in an even number were placed in the BV group (n = 78) and those with IDs that ended in an odd number were placed in the WC group (n = 67). Each of the women approached by the research team went through the informed consent process and consented to participate in the study. Approximately 86% of the participants completed the postintervention assessment (Time 2), which was administered to participants in both conditions after BV ended approximately three months postprogram enrollment. Figure 1 shows a flowchart documenting how participants progressed through the study, by treatment status.
Participant flow and retention at pre- and post-survey assessments.
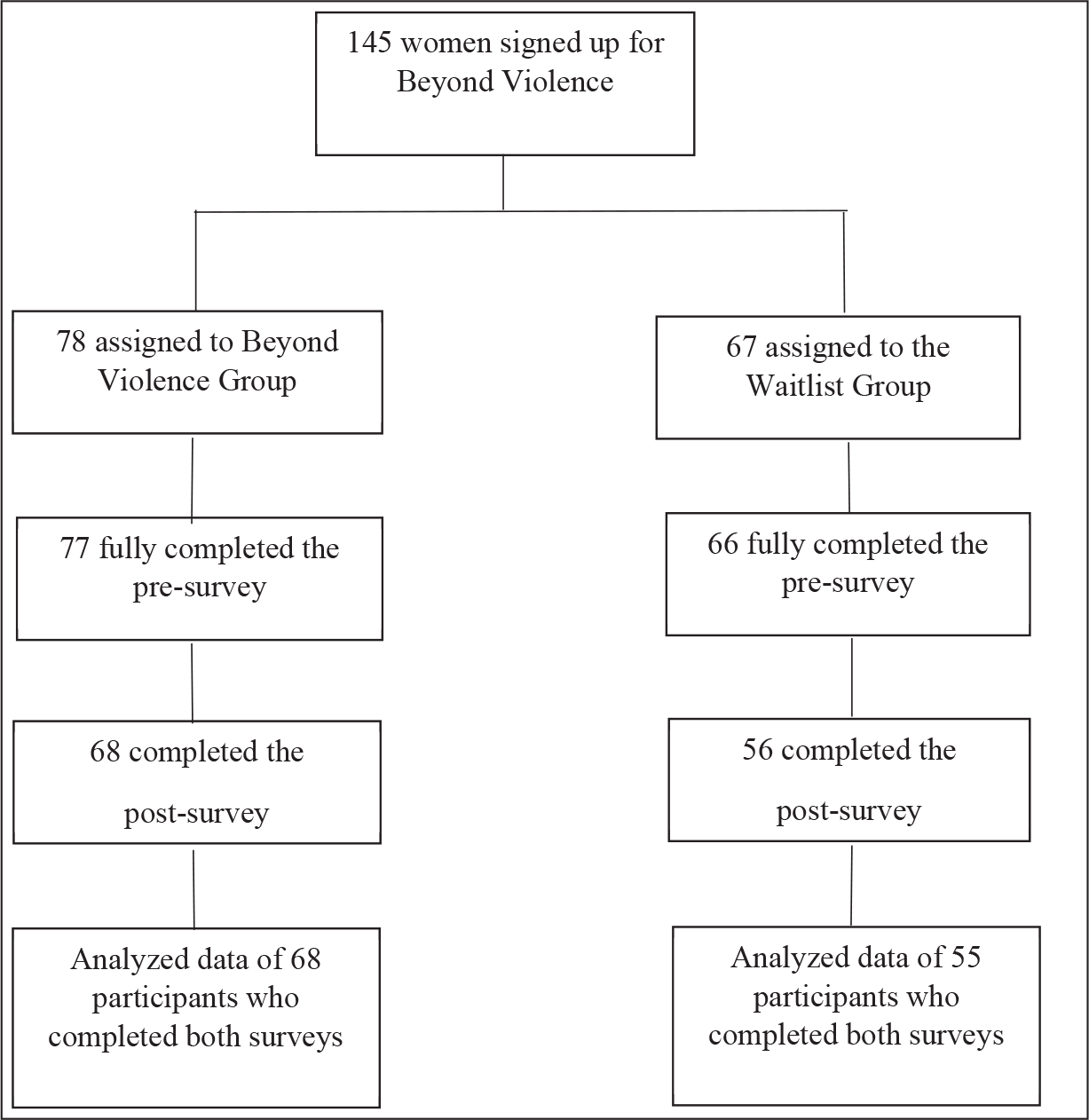
Sixty percent of those assigned to the BV program completed all 20 sessions. On average women completed 16.05 sessions (SD = 6.83). Among those who did not complete the program (n = 31), approximately 42% dropped from the program, 19% were transferred to another facility, 7% were sent to the secure housing unit, 7% were reassigned to another program, 3% had scheduling conflict, and 3% were paroled early. On average, the women who did not graduate completed 2.81 BV sessions (SD = 3.54). Following an “intent to treat” design, all women randomized to the BV group were included in the analysis even if they never attended one group. After the BV intervention group completed the cycle of the 20-session program, the corresponding WC group was then offered the program.
Survey administration. Research staff provided the self-administered surveys prior to the BV program entry (typically after the consent procedures). Groups of 10-20 participants were gathered, surveys were explained, 6th grade reading instructions were provided, and survey administration was proctored by a research staff member who also answered questions as needed. On average, the presurvey was completed within 45 minutes. The postsurvey took place after completion of the intervention or similar time period for the control group (approximately 10-12 weeks). The postsurvey was self-administered using the same procedures, and also took approximately 45 minutes to complete. Participants were paid $15 dollars for completing the preintervention survey and $15 for completing the postintervention survey, with payments placed in the participants’ commissary account. Participants were informed that participation would not impact their eligibility for parole or reduction in security classification.
Measures. Standardized instruments included detailed questions about demographics, childhood and adult trauma, mental health, substance use, and criminal justice involvement. The feasibility of these measures and procedures were previously found to be effective and valid among multiple samples of incarcerated women (Kubiak et al., 2014; Messina et al., 2020b; Messina & Zwart, 2021). The same measures were administered at preintervention and postintervention. In addition, basic demographic information, criminal justice history, substance use history and violence victimization/perpetration history were collected during the preintervention assessment.
Conflict Tactics Scales and Abuse Behavior Inventory. To ascertain the level of victimization and perpetration of violence within the sample, a modified index of perpetration and victimization history was developed based on several of the items from the Conflict Tactics Scales (Straus, 1979; Straus et al., 1996) and the Abuse Behavior Inventory (Shepard & Campbell, 1992). Participants were asked to indicate whether they had ever been the victim or perpetrator of 15 different behaviors which were coded into four major categories: (1) minor physical abuse (three behaviors; pushed, hit, restrained), (2) severe physical abuse (four behaviors; choked, burned, beaten, shot/stabbed), (3) threats and intimidation (seven behaviors; threats of physical harm or death to self, children, family members, or friends), and (4) sexual abuse/assault (one behavior; forced into unwanted sex act). While the Conflict Tactics Scale does not provide a measure of intent (e.g., self-defense or harm) or impact of IPV, this scale does provide a general indicator of the extent to which violence has been a part of the lives of the women in our sample.
For each behavior, participants were asked to indicate whether it had ever happened to them in their lives, or if they had ever engaged in the behavior. If the answer to either was yes, they were then asked to indicate whether (1) it happened to them as a child before the age of 18; (2) they did it as an adult to a romantic partner; or (3) they did it as an adult to someone other than a romantic partner. Data were collapsed into frequencies (Table 1) relating to whether respondents were victims as a child and perpetrators as adults of each major category of behavior. The sum scores of yes and no yielded a Cronbach’s α of 0.67 for severe physical violence victimization, 0.78 for minor physical violence victimization, and 0.79 for intimidation victimization in this sample. The sum scores of yes and no yielded a Cronbach’s α of 0.62 for severe physical violence perpetration, 0.78 for minor physical violence perpetration, and 0.80 for intimidation perpetration in this sample.
Depression (Patient Health Questionnaire—Depression Subscale). The Patient Health Questionnaire Depression Subscale is a 9-item subscale that measures current (past two weeks) depressive symptomology (Kroenke & Spitzer, 2002; Spitzer et al., 1999). Participants report on the symptoms they have experienced in the preceding two-week period. Responses are based on a 4-point Likert-type scale ranging from 0 (not at all) to 3 (nearly every day) and are summed into an overall symptom severity scale score that falls between 0 and 27. In a validation study of over 3,000 participants (with a cut off score of 10 or greater), the sensitivity for major depression was 88%, with a specificity of 88%, and a positive likelihood ratio of 7:1 (Kroenke & Spitzer, 2002). The 7.1 ratio indicated patients with major depression were seven times more likely to have a PHQ depression score of 10 or greater than patients without major depression. The internal consistency for the PHQ depression subscale, estimated by Cronbach’s α, was 0.88 in this sample.
Anxiety (Patient Health Questionnaire—Anxiety Subscale). The Patient Health Questionnaire Anxiety Subscale is a 6-item subscale that measures anxiety symptoms felt over the past 4 weeks (Spitzer et al., 1999). Responses are based on a 4-point Likert-type scale ranging from 0 (Not at all) to 3 (Nearly every day) and are summed into an overall symptom severity scale score that falls between 0 and 18. In a validation study of over 3,000 participants the PHQ anxiety subscale had an overall accuracy of 0.91 (specificity 0.97, sensitivity 0.63) in detecting any anxiety disorder when compared with mental health professionals using the Primary Care Evaluation of Mental Disorders (Prime-MD) (Spitzer et al., 1999). The internal consistency for the PHQ anxiety subscale, estimated by Cronbach’s α, was 0.81 in this sample.
PTSD (Short Screening Scale for DSM-IV PTSD, modified version). The modified version of the Short Screening Scale for DSM-IV Posttraumatic Stress Disorder (Breslau et al., 1999) is used to assess current symptoms of PTSD. Respondents who responded affirmatively to the question “In your life, have you ever had any experience that you considered frightening, horrible, or upsetting?” were then asked to complete a 7-item Short Screening Scale, concerning symptom frequency in the prior four-week period. Item responses were based on a Likert-type scale, ranging from 0 (Not at all) to 3 (Nearly every day), and scale scores ranged from 0 to 21. A validation study of over 2,000 participants found that a score of four or higher defined cases of PTSD with a sensitivity of 80% and a specificity of 97%. The positive predictive value was 71% and the negative predictive value was 98% (Breslau et al., 1999). The internal consistency for the PTSD scale, estimated by Cronbach’s α, was 0.84 in this sample.
Aggression (Buss-Warren Aggression Questionnaire (AQ). Buss-Warren Aggression Questionnaire (AQ), formally the Buss Perry Aggression Questionnaire, is a 34-item instrument used to assess anger and aggression (Buss & Warren, 2000). The respondent rates the description on a Likert-type scale, ranging from 1 (Not at all like me) to 5 (Completely like me). The Buss-Warren includes five subscales: Physical Aggression (eight questions, 8-40 range), Verbal Aggression (five questions, 5-25 range), Anger (seven questions, 7-35 range), Hostility (eight questions, 8-40 range), and Indirect Aggression (six questions, 6-30 range). Buss and Warren ran a standardization sample for the AQ with a sample size of 2,038. The internal consistency estimate total score is 0.94 with the individual subscales internal consistencies ranging from 0.71 for the Indirect Aggression scale to 0.88 for the Physical Aggression scale. In this sample, the internal consistency estimate was 0.90 for physical aggression, 0.74 for verbal aggression, 0.89 for anger, 0.85 for hostility, and 0.78 for indirect aggression.
Revised instrumental and expressive anger. The Revised Instrumental and Expressive Representation Scales includes two subscales with one measuring instrumental anger (i.e., anger used to manipulate or threaten) and the other measuring expressive anger (i.e., anger that erupts from repressed feelings). Responses, based on a Likert-type scale, ranging from 1 (strongly agree) to 5 (strongly disagree). These scales have shown good internal consistency in both community and prison samples (Archer & Haigh, 1997; Campbell et al., 1999). For this sample, the internal consistency for the instrumental anger and expressive anger subscales were high, with alphas of 0.92 and 0.86, respectively.
Emotional regulation (Difficulties in Emotion Regulation Scale). The DERS is a 36-item multidimensional self-report measure assessing individuals’ characteristic patterns of emotion regulation. It contains six subscales that were theoretically formulated and confirmed through factor analysis. Responses made on a Likert scale ranging from 1 (strongly agree) to 6 (strongly disagree). The six subscales are: Nonacceptance of Emotional Responses; Difficulties Engaging in Goal-Directed Behavior; Impulse Control Difficulties; Lack of Emotional Awareness; Limited Access to Emotion Regulation Strategies; Lack of Emotional Clarity. The total score was used in this study. The DERS has been found to have good internal consistency (α = 0.93) and an overall test–retest coefficient of 0.88 with coefficients ranging from 0.57 to 0.89 for the subscales (Gratz & Roemer, 2004; Victor & Kolnsky, 2016). The internal consistency for the total scale, estimated by Cronbach’s α, was 0.86 in this sample.
Analytic plan. Independent-sample t tests for continuous variables and chi-square analyses for categorical variables were used to examine differences between treatment conditions at baseline on background characteristics and outcome variables. Differences between the two study conditions were analyzed using analysis of covariance (ANCOVA) as this method has been shown to be the most powerful and precise approach to analyze pre- and post-data from randomized studies (Van Breukelen, 2006). The post-treatment scores of the mental health, anger/aggression, and emotion dysregulation measures were used as dependent variables, the pretreatment scores of the mental health, anger/aggression, and emotional dysregulation measures were used as the covariates, and the groups (BV and WC) were used as the independent variables.
Results
Mean Outcome Scores at Pre- and Post-survey Assessment by Condition.
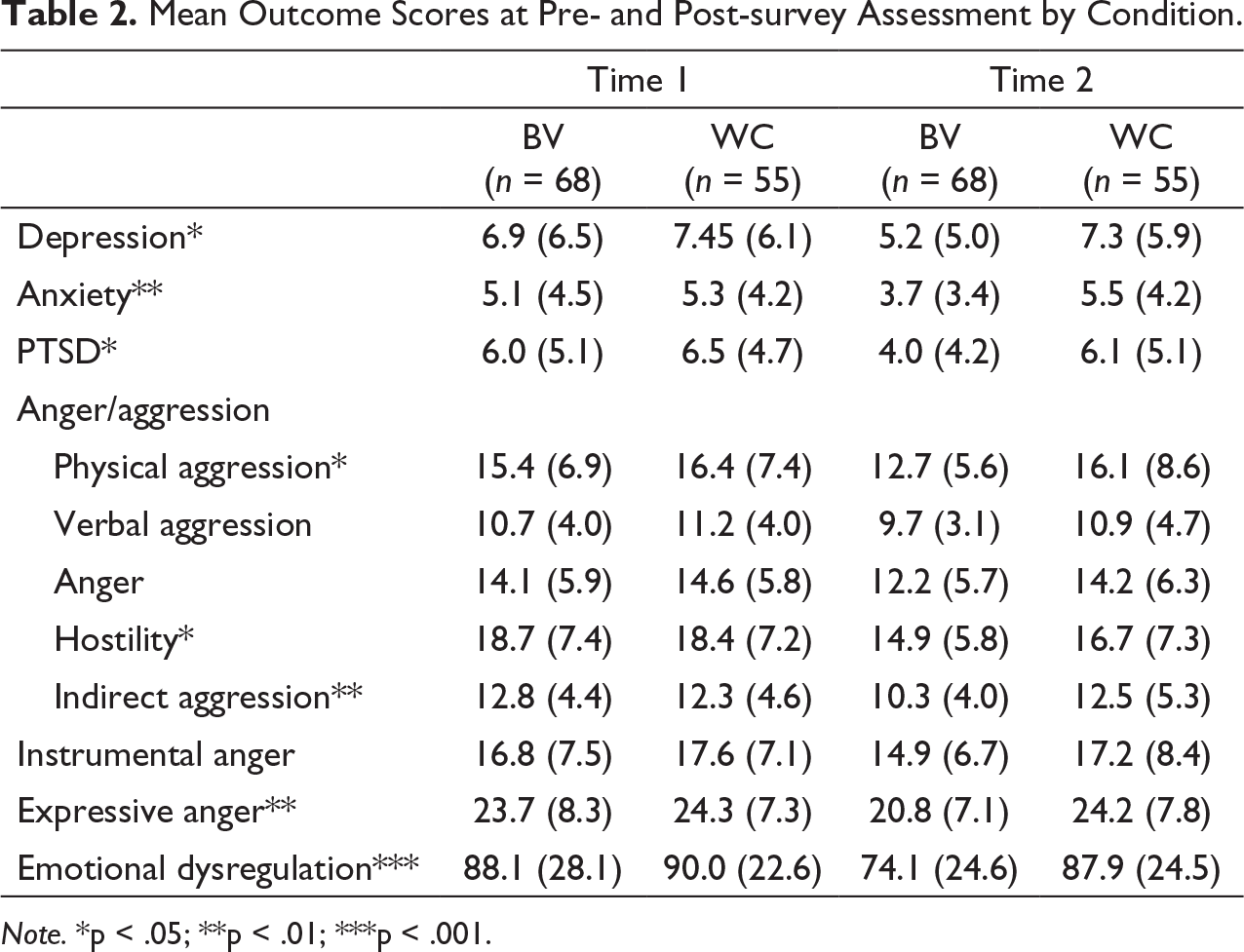
Note. *p < .05; **p < .01; ***p < .001.
Hypothesis 1 regarding mental health was fully supported as the results from the ANCOVA showed that BV participants had significantly lower mean scores than the WC participants on the mental health measures that included validated scales to assess for depression [F(1,120) = 4.973, p = .028], anxiety [F(1,120) = 9.120, p = .003], and PTSD [F(1,93) = 4.681, p = .033].
Hypothesis 2 regarding anger and aggression was partially supported, as findings showed that the BV participants had significantly lower mean scores than the WC participants at the postintervention assessment on the physical aggression [F(1,118) = 6.111, p = .015], hostility [F(1,118) = 4.237, p = .042], indirect aggression [F(1,118) = 9.423, p = .003], and expressive anger (i.e., anger used to manipulate or threaten) [F(1,120) = 7.152, p = .009] scales. There were no significant differences between the two groups with regards to the Buss Warren anger measure, verbal aggression, and instrumental anger (i.e., anger that erupts from repressed feelings).
Hypothesis 3 was fully supported as the BV participants had a lower DERS score than the WC participants at the postintervention assessment [F(1, 120) = 13.043, p = .000], indicating significantly increased emotional regulation (i.e., nonacceptance of emotional responses, difficulties engaging in goal-directed behavior, impulse control difficulties, lack of emotional awareness, limited access to emotion regulation strategies, and lack of emotional clarity).
Discussion
The purpose of this study was to expand and improve on previous research assessing the efficacy of the BV program for violent female offenders and to rigorously assess the effectiveness of the BV program using a peer-facilitated model of delivery. Replicating other studies of BV (Kubiak et al., 2012, 2015; Messina et al., 2016), we assessed the impact of BV on multiple mental health outcomes and anger/aggression among women incarcerated for violent offenses. We further assessed the impact of the BV program on emotional regulation, as there has been some indication that emotional dysregulation may play a role in perpetration of violence among women (Stuart et al., 2006).
The findings are consistent with previous studies and showed that BV participants had lower mean scores on the scales measuring depression, anxiety, PTSD, physical aggression, hostility, indirect aggression, expressive anger, and emotional dysregulation when compared to participants in the WC group. The majority of these findings are also consistent with the earlier pilot evaluation of the peer-facilitated BV program in California. However, the pilot study (Messina et al., 2016) showed significant reductions in levels of anger, verbal aggression, and instrumental anger which were not sustained in the experimental study (although the scores were in the hypothesized direction). It is possible that emotional regulation is highly correlated with instrumental anger, and as emotional regulation improves, additional skills might be developed to deal with anger that erupts from repressed feelings. The finding that verbal aggression did not significantly change is not surprising given the hostile realities of living in prison.
We also gathered extensive data on histories of victimization and perpetration of violence. Although 87% of our sample have a history of violent offenses, the data further substantiated the trajectories of violence within this sample and is consistent with the literature indicating that violence is continued throughout women’s lives (Kubiak et al., 2017; Saxena & Messina, accepted). Experiences of childhood victimization and subsequent acts of perpetration are inextricably linked. Additionally, childhood abuse is an intergenerational behavior suggesting the need for early prevention and intervention to break the cycle of abuse and trauma.
This study further shows the viability of using a peer-facilitated model of program delivery. There is a growing body of literature on the successful implementation of peer-facilitated programs and this study’s findings contribute to the evidence supporting peer-facilitated models of programming (Messina et al., 2020b; Messina & Zwart, 2021). Fiscal barriers requiring contracts with professionally trained program staff can restrict program availability resulting in long wait lists and large group formats. Thus, peer-facilitated programs provide a cost-effective and sustainable addition to program delivery. However, it is highly likely that the program oversight, the manualized Facilitator’s Guides, peer training, and institutional support enhanced the feasibility of the successful peer-facilitated model of the BV program delivery. The BV program has previously been shown produce positive results when facilitated by clinical professionals as well (Kubiak et al., 2012, 2015).
The study findings provide a knowledge base to create larger more rigorous studies, which can ultimately confirm the necessity of trauma-specific programming services for incarcerated women and identify effective program delivery models. The findings may be applicable to corrections services in multiple settings, as they indicate the efficacy of violence prevention interventions as well as peer-facilitated interventions.
Strengths
The study employed a randomized controlled trial to assess the efficacy of the violence prevention program among the largest sample size to date. This is the most rigorous evaluative methodology needed to determine if an intervention is evidence-based. The study proved a successful group randomization procedure without violations and with a high follow-up rate, increasing the reliability and validity of the findings. Additionally, the BV program curricula is a manualized intervention providing both a detailed facilitator guide and a participant workbook. The use of a manualized curricula creates standardization of delivery and the ability to monitor fidelity of peer-facilitation. Peer-facilitators had been trained by the program author and program implementation was provided daily oversight by Program Coordinators also trained by the program author, further enhancing fidelity of facilitation. Moreover, the program facilitators delivered the intervention, and the research staff administered the research survey, reducing the likelihood of social desirability bias. The BV program also uses a variety of therapeutic and evidence-based approaches to address the impact of trauma. It is also gender responsive in that it reflects an understanding of the realities of women’s lives and is theoretically based centered on women’s psychological development.
Finally, we added additional data elements to validate the trajectories of violence in the participant’s lives, both as victims and perpetrators. As the BV program content was created to specifically address violent female offenders’ needs, it was vital to determine beyond commitment offense, that the intervention was efficacious for the target population. The results from the modified perpetration and victimization histories demonstrated the high prevalence of violence throughout the participant’s lives and the high prevalence of perpetration of general violence and IPV.
Limitations
Although this study had several methodological strengths, it also had important limitations. Our sample size was larger than those in previous studies however, it may not have been large enough to detect some effects of BV on some of the outcomes. However, even with only 60% of the sample effectively completing all 20 sessions, the outcome measures were significantly in favor of the treatment group. Next, the study sample may not be representative of female prison populations nationally (or internationally). California’s recent policy changes have enacted lengthy sentences for violent offenders, while lower-level offenders are sentenced to county jails. Yet our findings were replicable of the findings from the randomized controlled trial implemented by Kubiak and colleagues with violent incarcerated women in the Midwest. Additionally, the current study relied on self-report data. We did not have access to objective measures to determine mental health diagnoses, to substantiate self-reported histories of victimization and violence, or to determine in-custody violations. There is also the potential for a biased estimation resulting from sample attrition; however, comparisons between the small percentage lost at follow-up did not show significant differences compared with the 89% who completed the follow up surveys. Finally, we were not able to assess postrelease recidivism due to the lengthy sentences of our participants for serious violent crimes. Thus, it will be important to assess recidivism outcomes in future studies.
Policy Implications
The literature demonstrates the prevalence of violence and aggression perpetrated by women and indicates the need for interventions focusing on the prevention of violence for women, in addition to interventions focused on male aggression. BV has shown indicators of successful models of implementation and effectiveness with a range of women with violent offenses. Responding appropriately to the needs of these women, particularly those with co-occurring disorders, can increase the understanding of female perpetrated violence and potentially prevent continued perpetration. Given the BV intervention is manualized and shown to be feasible to facilitate from a team with a wide range of expertise, it can easily be implemented in multiple corrections settings.
The positive findings also support rethinking rehabilitation and the culture of corrections. Correctional organizations must become both trauma-informed and trauma-responsive to change the culture of the environment and recognize the unmet needs for both residents and staff (Covington & Bloom, 2018; Messina et al., 2020a). Ultimately this requires commitment on the part of leadership to comprehend the process of trauma and to begin to recognize the necessary structure needed for a trauma-informed organization to reduce violence and retraumatization.
Conclusions
Given the aggregate impact of trauma and violence in the lives of women offenders and the potential intergenerational cycle of violence, the field will benefit from research that identifies effective services that moderate the negative impact of such histories. We believe that this experimental study represents a strong contribution to the existing evidence supporting the BV intervention. Future studies need to focus on the sustainability of the benefits of the BV program, incorporate more qualitative measure to unravel the positive dynamics of peer-facilitation, and include post release outcome measures. Additional research should replicate this study with justice-involved women both nationally and internationally. The BV program continues to operate in California women’s facilities using this model of peer-facilitated model of program delivery, and the waitlist of women participants continue to be long.
Anger is the easiest emotion to identify, but when I went back and found the hurt and the pain…and understood how all of it played a part from the very beginning … I didn’t have to struggle anymore because I was able to write it all down, and so in the end, there was no stone left unturned. ~Beyond Violence participant, 2018
Footnotes
Acknowledgments
This pilot project would not have been possible without the strong support and engagement of the California Department of Corrections and Rehabilitation (CDCR) Lead Administrators such as former FOPS Directors, Jay Virbel and Amy Miller, and the institutional staff at the California Institution for Women (CIW) including former Warden Molly Hill, the current Warden Richard Montes, Lieutenant Joseph Spinney, and the former Community Resource Manager, Ronnie Shoupe. We are especially grateful to Dr Stephanie Covington, the author of the trauma-informed violence prevention program for women, Beyond Violence. Dr Covington’s dedication to enhancing the well-being of incarcerated women around the world is demonstrated in her collective publication and gender-responsive curriculum development. We would also like to acknowledge retired Captain Rochelle Leonard for her unwavering dedication and facilitation of the Beyond Violence program inside the facility. We would also like to thank the Supervising Psychiatric Social Worker, Karen Vertti, the Beyond Violence peer facilitators, and the research assistants, Claire Samuelson and Liliana Gregorio. We are also grateful for CDCR’s and CIW’s continued support of the program, graduations, and ongoing navigation of the program in a difficult environment. Finally, we are indebted to the women who so kindly volunteered their time, insights, ideas, and reflections from participating in Beyond Violence to this project.
Declaration of Conflicting Interests
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by Award No. 2016-SI-AX-0008 awarded by the Office on Violence Against Women, U.S. Department of Justice. The opinions, findings, and conclusions or recommendations expressed in this report are those of the authors and do not necessarily reflect those of the Department of Justice.