
Abstract
Keywords
Introduction
Violence against children is a global public health emergency with an annual prevalence of past-year sexual, physical, and/or emotional violence reported to be 54% among children under the age of 18 years (Hillis et al., 2016). Adolescent girls and young women are more vulnerable to childhood violence than young boys and recent studies in sub-Saharan Africa report that 15–25% of adolescent girls and young women experienced sexual violence prior to age 18 while 30–60% experienced physical and/or emotional violence in childhood (Meinck et al., 2016; Sumner et al., 2015; Swedo et al., 2019; Ward et al., 2018). While there is limited data on violence against children in Namibia specifically, some evidence suggest prevalence rates of childhood sexual, physical, and emotional violence are comparable to those reported in other sub-Saharan Africa settings (Andersson et al., 2012; Brown et al., 2009; Devries et al., 2011). Childhood sexual, physical, and emotional violence are associated with a range of adverse physical and mental health outcomes among women including increased risky sexual behavior and HIV acquisition, unplanned pregnancy, suicide, and alcohol and drug abuse (Chen et al., 2010; García-Moreno et al., 2013; Hillberg et al., 2011; Jewkes et al., 2010; Norman et al., 2012; Senn & Carey, 2010). Modeling analyses in sub-Saharan Africa have also found that childhood violence has a significant toll on rates of drug abuse, self-harm and suicide, anxiety, and subsequent experience of intimate partner violence (IPV) at a population level (Hsiao et al., 2018).
Adolescent girls and young women are also more likely to experience IPV than young men, although prevalence estimates of IPV among adolescent girls and young women vary widely (6–59% across several studies in sub-Saharan Africa) and are likely to be frequently underestimated due to difficulties with reporting, social desirability bias, and fears of retribution or punishment from perpetrators, family members or friends, or others in the community (Chiang et al., 2018; Dartnall & Jewkes, 2013; García-Moreno et al., 2013; Kapiga et al., 2017; Shamu et al., 2011, 2016). Several empirical research studies found childhood violence experiences are a significant predictor of subsequently reporting IPV (Chiang et al., 2018; Coid et al., 2001; Shamu et al., 2016), though the majority of these analyses of violence revictimization were conducted in high-income countries and may not be applicable to lower resource contexts with different gender norms, different underlying violence prevalence and levels of community violence, and varying legal definitions and reporting guidelines for IPV (Abramsky et al., 2011; Dartnall & Jewkes, 2013; Fulu et al., 2017; Guedes et al., 2016). In addition, most research in this area has asked about co-occurrence of recent childhood violence experiences and IPV in the same time period rather than asking about childhood violence experiences from a time prior to having an intimate partner to understand cycles of violence or has examined the influence of childhood violence on later violence perpetration rather than revictimization (Abramsky et al., 2011; Fulu et al., 2017; Shamu et al., 2016). Childhood violence may increase the risk for subsequent IPV in early adulthood by causing posttraumatic stress disorder and an impaired ability to respond to dangerous situations or by reducing self-efficacy, empowerment, and feelings of self-worth in relationships (Bensley et al., 2003; Jewkes et al., 2010; Namy et al., 2017; Ullman et al., 2009). Childhood violence and IPV also often co-occur in the same household and share many risk factors that can confound their relationship making it difficult to establish temporality between the two (Carlson et al., 2020; Guedes et al., 2016). Research is needed to understand associations between childhood violence and later IPV among adolescents and young adults in sub-Saharan African settings while better establishing temporality of the relationship and accounting for individual-, interpersonal-, and societal-level confounding factors.
The prevalence of childhood sexual, physical, and emotional violence and later IPV among adolescent girls and young women ages 18–24 was examined using data from the Namibia Violence Against Children and Youth Survey (VACS) (L. F. Chiang et al., 2016). In particular, we sought to understand cycles of violence and revictimization in this setting by examining associations between report of childhood violence prior to age 18 and report of IPV after age 18. We hypothesized that any experience of childhood violence, regardless of type of violence (sexual, physical, and/or emotional), would be associated with subsequent experience of intimate partner violence later in adolescence and early adulthood. However, we also considered the unique influence of childhood sexual, physical, and emotional violence, separately, given that sexual and physical violence can be considered more severe than emotional violence and might have a larger effect on violence revictimization. In addition, we expected to find a dose-response relationship whereby the association between childhood violence and subsequent intimate violence would be stronger for those experiencing more types of violence in childhood. This work has the potential to improve violence prevention and response programs, particularly for youth in Namibia with prior experiences of childhood violence, and may have broader implications for other sub-Saharan African settings.
Methods
Study Design
The 2019 Namibia VACS was a nationally representative, household, cross-sectional survey to assess the prevalence and circumstances of childhood emotional, physical, and sexual violence throughout the country. VACS has been previously conducted throughout Africa and Asia (Centers for Disease Control and Prevention (n.d.); L. F. Chiang et al., 2016; Nguyen et al., 2019).
Study Population and Sampling Procedures
The survey employed a three-stage cluster sampling approach to enroll individuals ages 13–24 from March 2019 to June 2019. In the first stage, a sampling frame was established based on geopolitical subdivisions from the 2010 Census and 2016 Namibia Intercensal Demographic Survey. A total of 274 primary sampling units (PSUs) were randomly selected from 3472 PSUs in the sampling frame. In the second stage, 25 households with at least one eligible 13–24 year old were randomly selected from each PSU using an equal probability systemic sampling method. In the third stage, one eligible individual was randomly selected from each household for an interview. This design assumes that each selected eligible individual can be linked to only one household in Namibia. A split sample approach was used to randomly assign PSUs for either female or male survey administration in order to protect confidentiality of respondents and reduce the chances that a perpetrator of violence and victim of that violence would both be interviewed. The study oversampled girls in three regions where the DREAMS (Determined, Resilient, Empowered, AIDS-free, Mentored, and Safe) program was implemented: Khomas, Oshikoto, and Zambezi. These regions have high HIV prevalence and DREAMS seeks to address this by providing adolescent girls and young women with HIV prevention and empowerment programming (Saul et al., 2018).
Individuals were eligible for survey participation if they were: 1) between 13–24 years old at the time of survey administration; 2) able to understand and speak Afrikaans, English, Damara/Nama, Oshiwambo, Otjiherero, RuKwangali, and/or siLozi; 3) without cognitive or physical disabilities that would prevent the survey administration (e.g., hearing or speech impairment); 4) not living in institutions such as hospitals, prisons, residential child care facilities, and other such establishments; 5) residents of selected households; and 6) not homeless or street youth not living in a household. All individuals provided verbal informed consent for study participation and parent or guardian permission was also sought for those <18 years. Interviewers were fluent in local languages, trained in study procedures, confidential data and health issues, and gender-matched to participants. Close-ended survey questions were interviewer-administered in a private, confidential location at or near home. The survey included a short demographic interview with the head of each selected household and a comprehensive interview with the participant to assess sexual, physical, and/or emotional violence experiences. While both females and males were interviewed, this analysis focuses only on 18–24 year old young women who also provided data on childhood violence experiences prior to age 18 (N = 2434 participants). Additional details on VACS sampling methodology, survey procedures, and ethical conduct of research are reported elsewhere (Centers for Disease Control and Prevention (n.d.); Nguyen et al., 2019).
Exposures
The primary exposure of interest for this analysis is any childhood exposure to violence. Childhood violence experiences were assessed among participants aged 18–24 years by asking about the first instances of violence and their age when the violence occurred. Childhood sexual violence could include any unwanted sexual touching, attempted unwanted sexual intercourse, pressured intercourse, physically forced sex, and/or alcohol-facilitated sex by a parent, caregiver, other adult relative, romantic partner, peer, or other person in the community. Sexual violence was asked about in a series of five questions (one question per type of violence). These questions were followed by items asking about violence perpetrators for each type of sexual violence. Childhood physical violence could include any experiences of being hit with a fist, kicked, beaten with an object, or threatened or attacked with a weapon by a parent, caregiver, other adult relative, romantic partner, peer, or other person in the community. Physical violence was assessed in a series of four questions about each type of violence (e.g., “have you ever been slapped, pushed, shoved”; “have you ever been punched, kicked”; “have you ever been strangled”; “have you ever been threatened with a knife, gun, or other weapon”) per each violence perpetrator. For instance, participants were asked these four questions about physical violence experience by a parent or caregiver, followed by four questions about physical violence experience from a romantic partner, etc. Childhood emotional violence could include any experiences of being told that you were unloved or did not deserve to be loved, being told by someone that they wished you were dead or had never been born, or being ridiculed or put down by a parent, caregiver, other adult relative, romantic partner, peer, or other person in the community. Emotional violence was assessed with three questions (e.g., “have you been made to feel really bad or scared”; “has someone told lies about you”; and “has someone excluded you or ignored you”) and was also separately asked about for each violence perpetrator. For the primary analysis, “any childhood violence” was defined as a binary variable indicating whether any sexual, physical, and/or emotional violence experiences occurred prior to age 18 among 18–24 year old participants. We also considered experiences of any childhood sexual, physical, and emotional violence separately, by creating binary variables for each of these types of violence. In addition, we summed the total number of childhood violence experiences reported and created a four-category categorical variable to indicate whether participants experienced zero, one, two, or three sexual, physical, and/or emotional violence experiences.
Outcomes
The primary outcome of interest for this analysis is any exposure to violence by an intimate partner in adolescence or young adulthood. IPV experiences were assessed among participants aged 18–24 years by asking about the instances of violence and their age when the violence occurred. Sexual and physical violence could include any of the experiences as described in the previous section. Emotional violence by an intimate partner could include being insulted, humiliated, or made fun of in front of others, being kept from having one’s own money, being kept from seeing or talking to family or friends, being kept track of and forced to report whereabouts, and being threatened. Sexual intimate partner violence was assessed with five items, physical intimate partner violence was assessed with four items, and emotional intimate partner violence was assessed with three items. All asked specifically about violence experienced by an intimate or romantic partner. For this analysis, we created a binary “any IPV” variable indicating whether the participant reported any sexual, physical, and/or emotional violence experiences perpetrated by a sexual partner after age 18. This analysis was restricted to 18–24 year old participants who ever reported an intimate partner.
Covariates
Data were collected on demographic and behavioral factors including age, education level, food and material insecurity, orphan status prior to age 18, marital status, sexual behavior (e.g., ever sexually active and age at first sex), and pregnancy history. Family and peer support was assessed with two items asking participants whether they find it easy to talk with their mother or father or friends about things that really bother them (with Likert scale responses ranging from “very difficult” to “very easy”). Responses were coded into binary variables, whereby participants who replied “easy” or “very easy” to these items were considered to have support from parents or friends. Gender attitudes about violence were assessed with five items from the Gender Equitable Men’s Scale (GEMS) (e.g., “Do you believe that only men, not women should decide when to have sex?”) (Gottert et al., 2016). Those who responded “yes” to any of the five items were considered to endorse gender attitudes toward violence. Normative beliefs about domestic violence were assessed with five items from the Demographic and Health Survey (DHS) scale (e.g., “Is a husband justified in hitting or beating his wife if she refuses to have sex with him?”) (Antai, 2011). A response of “yes” to any item was considered endorsement of normative beliefs about domestic violence. Two questions from the Multiple Indicator Cluster Survey (MICS) were used to assess corporal punishment attitudes and each was reported as a single-item indicator (“Do you believe that a parent or caregiver needs to physically punish a child to bring up a child properly?; “Do you believe that a teacher needs to physically punish a child to educate a child properly?”) (Akmatov, 2011). Participants were also asked whether they had ever witnessed violence in their home (“How many times did you see or hear your parent punched, kicked, or get beaten up by your other parent?”) or community (“Outside of your home and family environment, how many times did you see anyone get attacked?”). Those who responded once or more to either item were considered to have ever witnessed violence.
Data Analysis
The data were weighted to be nationally representative by accounting for the probability that each respondent was in our sample (the base weight), the impact of survey nonresponse (nonresponse weight), and potentially imperfect sampling frames (post-stratification weight). Final sample weights were incorporated into all analyses by using SAS 9.4 (Cary, NC) SURVEYFREQ and SURVEYLOGISTIC procedures. Descriptive statistics were used to assess the weighted prevalence of childhood violence, sociodemographic and behavioral characteristics, and experience of IPV as an adolescent or young adult. A weighted logistic regression was used to assess whether childhood violence exposure was associated with experience of IPV after age 18. We explored the potentially confounding influence of age, education level, orphan status, family and peer support, sexual behavior, perpetrators of violence, ever witnessing violence, gender attitudes about violence, normative beliefs about domestic violence, and corporal punishment attitudes on our relationship of interest, given hypothesized associations between these variables, childhood violence experience, and intimate partner violence experience. These covariates were selected for inclusion in our final regression models using a forward stepwise regression procedure whereby we added covariates to our model individually to assess whether any changed our univariable regression coefficient by >10% (an indication of a covariate meaningfully confounding the association between childhood violence exposure and later IPV experiences). Those that resulted in a >10% change from our univariable coefficient were retained in a multivariable model. We modeled the influence of any childhood violence experience on later IPV experiences and also separately considered the influence of sexual, physical, and emotional childhood violence on our outcome. Each of these exposure was included in a different regression model given the collinearity between these childhood violence experiences. We calculated Bonferroni corrected p-values to adjust for multiple comparisons across our models. We also explored a potential dose-response relationship between childhood violence experiences and subsequent intimate partner violence with a regression model examining the association between our four-category childhood violence experience variable and subsequent intimate partner violence experience. We will compare the effect of experiencing violence one, two, or three times on intimate partner violence (with never experiencing childhood violence as the reference group).
Ethical Statement
The survey protocol and informed consent documents were reviewed and approved by the U.S. Centers for Disease Control and Prevention (CDC) and the Namibia Ministry of Health and Social Services ethical review boards.
Results
Participant Characteristics
Demographic Characteristics and Experiences of Violence Among 18–24 Year Old Females, Violence Against Children Survey (N = 2434).
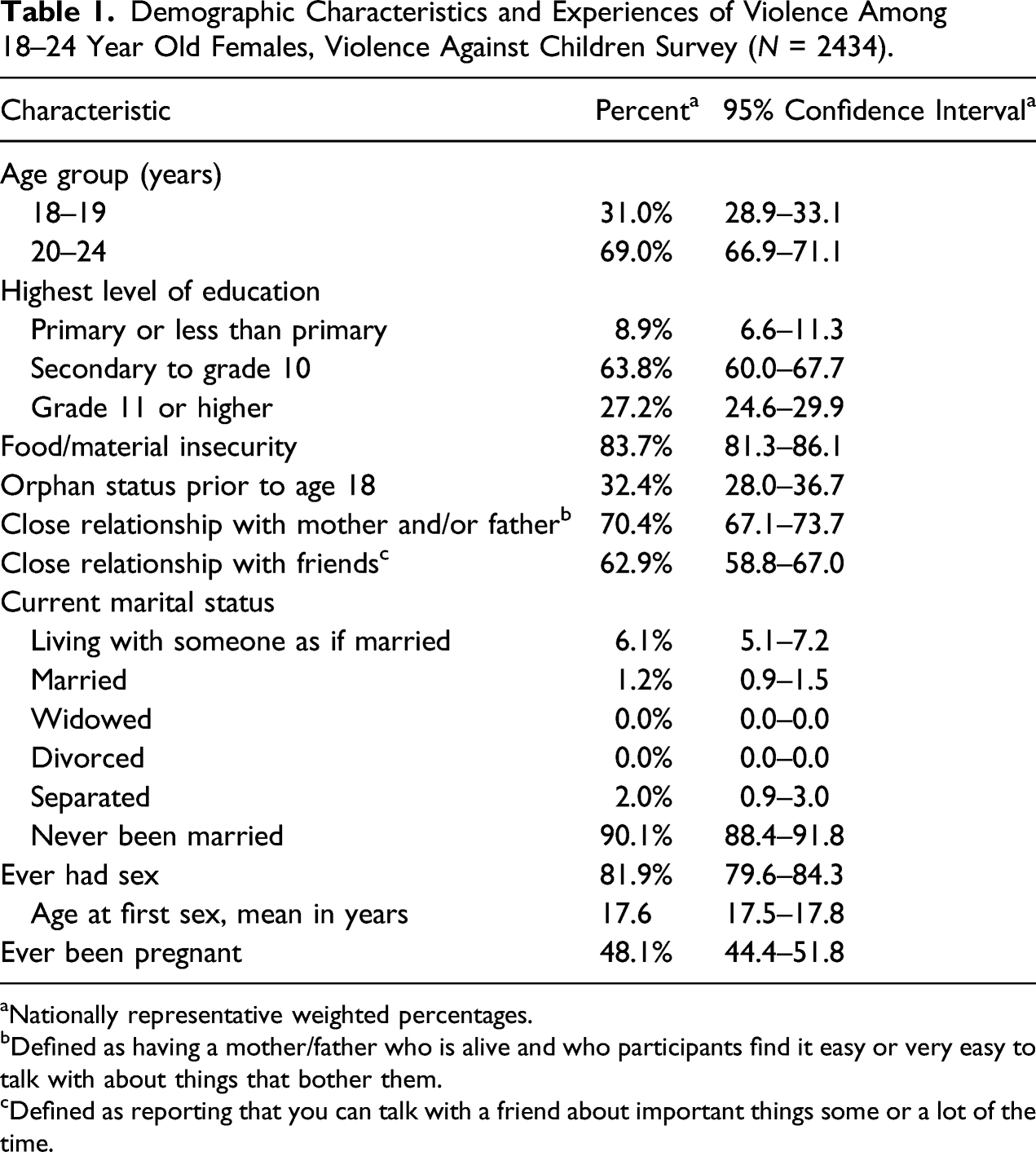
aNationally representative weighted percentages.
bDefined as having a mother/father who is alive and who participants find it easy or very easy to talk with about things that bother them.
cDefined as reporting that you can talk with a friend about important things some or a lot of the time.
Experiences of Childhood and Early Adult Violence
Experiences of Childhood Violence and Later Intimate Partner Violence Among 18–24 Year Old Females, Violence Against Children Survey.
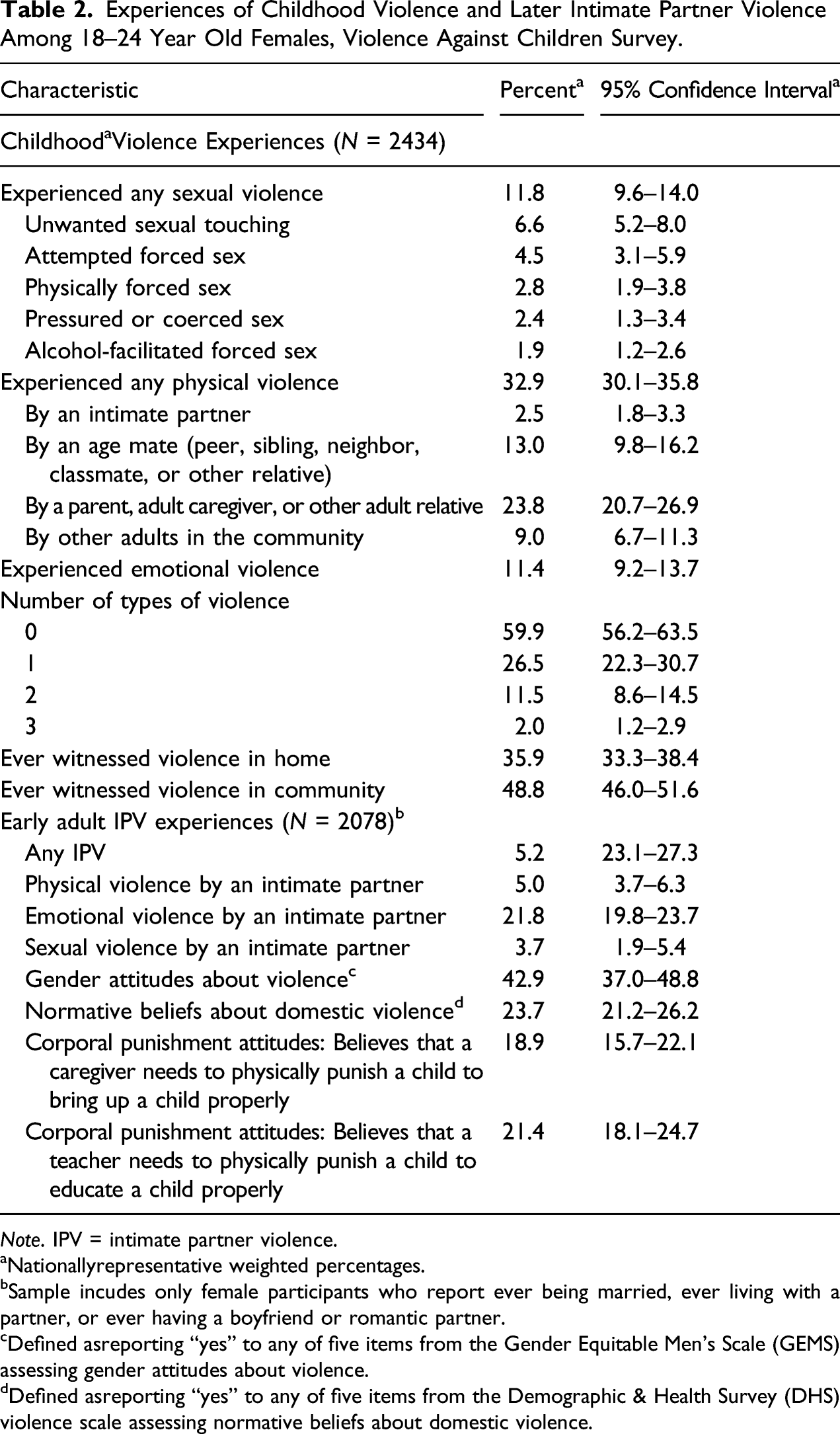
Note. IPV = intimate partner violence.
aNationallyrepresentative weighted percentages.
bSample incudes only female participants who report ever being married, ever living with a partner, or ever having a boyfriend or romantic partner.
cDefined asreporting “yes” to any of five items from the Gender Equitable Men’s Scale (GEMS) assessing gender attitudes about violence.
dDefined asreporting “yes” to any of five items from the Demographic & Health Survey (DHS) violence scale assessing normative beliefs about domestic violence.
The prevalence of experiencing at least one type of IPV after age 18 was 25.2% (95% CI: 23.1–27.3) among Namibian adolescent girls and young women who ever reported an intimate partner (Table 2). The most commonly experienced type of IPV was emotional violence (21.8%; 95% CI: 19.8–23.7), followed by physical violence (5.0%; 95% CI: 3.7–6.3) and sexual violence (3.7%; 95% CI: 1.9–5.4).
Approximately 42.9% (95% CI: 37.0–48.8) of 18–24 year old adolescent girls and young women had attitudes in support of gender-based violence and 23.7% (95% CI: 21.2–26.2) reported normative beliefs about domestic violence (Table 2). In addition, 18.9% (95% CI: 15.7–22.1) believe that corporal punishment from a parent is needed to bring up a child properly and 21.4% (95% CI: 18.1–24.7) believe that corporal punishment from a teacher is needed to educate a child.
Associations Between Childhood Violence and Later Intimate Partner Violence Experiences
Associations Between Types of Childhood Violence and Intimate Partner Violence in Adulthood Among 18–24 Year Old Females in Namibia, Violence Against Children Survey (N = 2078) 1 .
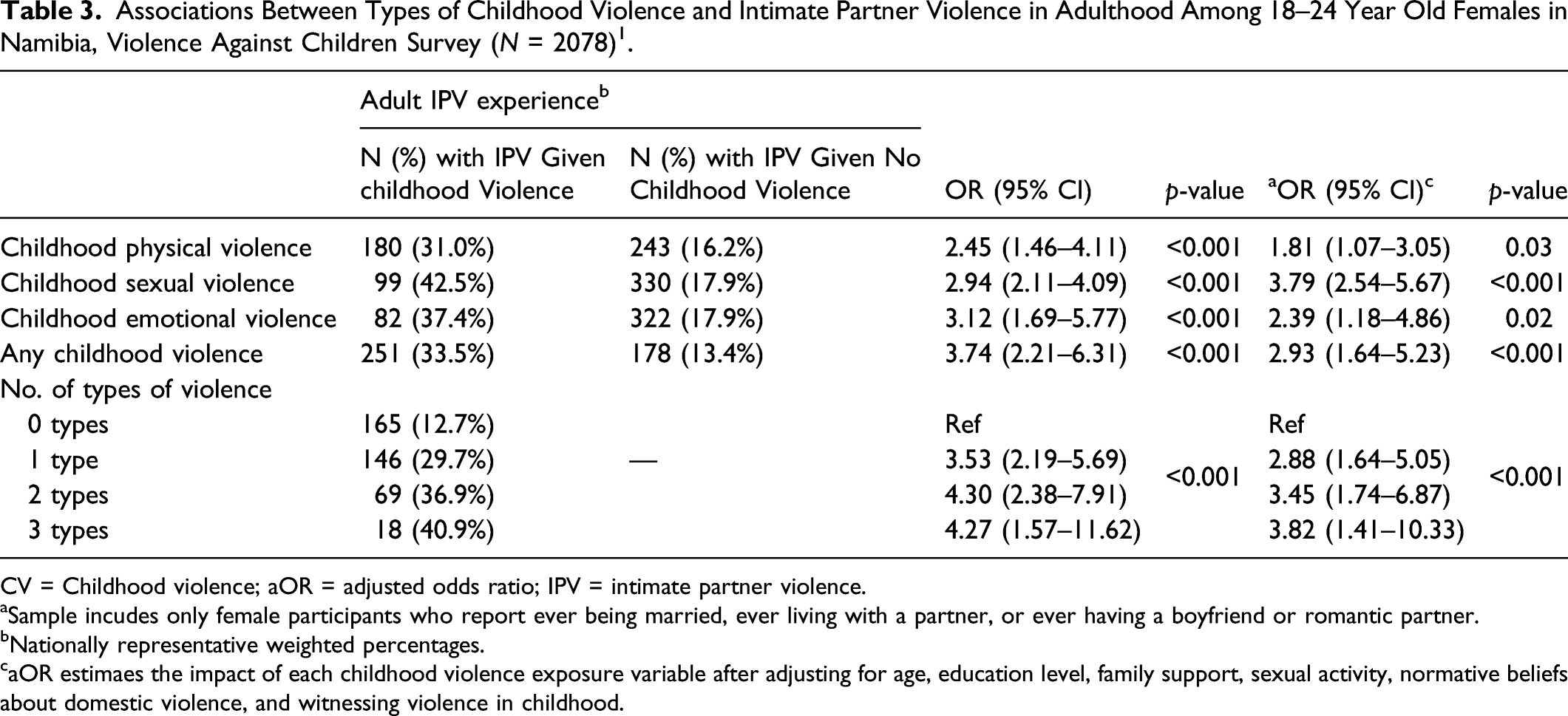
CV = Childhood violence; aOR = adjusted odds ratio; IPV = intimate partner violence.
aSample incudes only female participants who report ever being married, ever living with a partner, or ever having a boyfriend or romantic partner.
bNationally representative weighted percentages.
caOR estimaes the impact of each childhood violence exposure variable after adjusting for age, education level, family support, sexual activity, normative beliefs about domestic violence, and witnessing violence in childhood.
When exploring the impact of each type of childhood physical violence on later IPV, childhood sexual violence (aOR: 3.79; 95% CI: 2.54–5.67; p-value < .001), childhood physical violence (aOR 1.81; 95% CI: 1.07–3.05; p-value: .03), and childhood emotional violence (aOR: 2.39; 95% CI: 1.18–4.86; p-value: .02) were each significantly associated with IPV after controlling for the same set of covariates as in our primary model. There was a dose-response relationship between number of types of childhood violence and IPV. Participants who experienced one type of violence had 2.88 times the odds of subsequent IPV experience (aOR: 2.88; 95% CI: 1.64–5.05), those who experienced two types of violence had 3.45 times the odds of subsequent IPV experience (aOR: 3.45; 95% CI: 1.74–6.87), and those who experienced all three types of childhood physical, sexual, and emotional violence had 3.82 times the odds of subsequent IPV experience (aOR: 3.82; 95% CI: 1.41–10.33; p-value: <.001), compared with those who experienced no childhood violence.
Discussion
Among 18–24 year old adolescent girls and young women in Namibia, we found high rates of childhood violence and IPV in early adulthood and strong associations between childhood violence and subsequent violence experiences. Results show that adolescent girls and young women are significantly more likely to experience IPV if they experienced any violence prior to age 18, particularly if they experienced childhood sexual violence. There was a dose-response relationship between childhood violence and IPV, with young women who experienced more than one type of violence (sexual, physical, and/or emotional) in childhood having a significantly elevated risk of violence revictimization compared with those who reported no childhood violence experiences. This is the first analysis to examine links between childhood violence and IPV in Namibia and provides unique insights on cycles of violence among young women in a sub-Saharan African setting.
The prevalence estimates of childhood violence and IPV from this nationally representative VACS survey were similar to estimates of violence among young women in other sub-Saharan African settings (Breiding et al., 2013; Dartnall & Jewkes, 2013; García-Moreno et al., 2013; Sumner et al., 2015; Vagi et al., 2016). However, there is wide variability in metrics used to measure violence experiences across different studies and surveillance activities (e.g., phrasing of question stem, time period in which violence is assessed, and methods of interviewer- or self-administered data collection) making it difficult to compare widely across cohorts (Ortiz & Mattson, 2018). In addition to our findings on prevalence of violence, 35.9–48.8% of 18–24 year old adolescent girls and young women had witnessed violence at home or in the community, a quarter reported normative beliefs about child violence and IPV, and about half reported gender attitudes about violence. Similar rates of household and community violence and gender norms around acceptability of violence have also been reported in other VACS surveys and longitudinal studies in sub-Saharan African settings (Mulawa et al., 2016; Nguyen et al., 2018; Tsai et al., 2017; VanderEnde et al., 2018).
Our analysis adds to the small but growing body of literature demonstrating a large, statistically significant effect of childhood violence on subsequent IPV victimization among adolescent girls and young women in sub-Saharan Africa (L. Chiang et al., 2018; Shamu et al., 2016). These other recent studies also found two-to-three fold elevated risks of IPV among young women who have experienced childhood physical, sexual, and/or emotional violence and also found a dose-response relationship between number of childhood violence experiences and subsequent IPV demonstrating potential generalizability of these findings (L. Chiang et al., 2018; Shamu et al., 2016).
There are several potential explanations for the mechanism of association observed in our analysis. Individuals who experience childhood violence may also have traumatic stress symptoms, which could result in poor coping behavior and behavioral disinhibition that lead to subsequent revictimization by an abusive partner (Koen et al., 2016; Krause-Utz et al., 2018; Milner et al., 2010). In addition, childhood violence could result in lower self-esteem, lack of empowerment in future intimate relationships, and having a partner who exhibits controlling behaviors (Mwakanyamale & Yizhen, 2019; Shamu et al., 2018). Cultural norms around violence against children and IPV may also place young women at greater risk of violence victimization during their lifecourse, though survey questions were limited in their ability to capture all normative beliefs and community-level factors (Fine et al., 2019; Messersmith et al., 2017; Shamu et al., 2018). Interventions that successfully change gender norms around violence and those that empower adolescent girls and young women through economic and educational means have shown success at reducing IPV, providing some evidence for this mechanism of action and strategies to break cycles of violence (Abramsky et al., 2016; Lundgren & Amin, 2015; Wamoyi et al., 2020). Finally, the same conditions that predispose individuals to violence in childhood could also lead to violence revictimization in adolescence and adulthood (e.g., witnessing violence, low social support, living with the perpetrator, economic, or food insecurity) (Carlson et al., 2020). Specifically, prior analyses have found higher social support to be a buffer against both childhood and intimate partner violence experiences while witnessing violence may be a marker of high rates of community violence and general acceptability of violent behavior (Machisa et al., 2018; Ringwald et al., 2020). We accounted for this by included family support and witnessing childhood violence as potential confounders of the relationship between childhood and IPV as other.
The strengths of this study included the large, nationally representative sample which allowed for an estimated weighted prevalence of childhood violence and IPV among adolescent girls and young women. Overall response rates were high in the survey which minimized bias in our findings. Limitations included the cross-sectional survey retrospectively assessing childhood violence that occurred prior to age 18 among 18–24 year olds which reduces the reliability of estimates and ability to establish temporality with covariates, childhood violence, and subsequent IPV. Responses may have been influenced by recall or social desirability bias and/or stigma. In addition, any recent violence experiences could have resulted in distress that impacted participants’ answers. These issues were mitigated as much as possible by conducting in-depth training with the interviewers on establishing rapport and trust with participants and developing response plans for young women experiencing violence as described elsewhere (Centers for Disease Control and Prevention; Nguyen et al., 2019). Finally, we explored associations between types of childhood violence and any IPV without separately considering the effect of childhood violence on emotional, sexual, and/or physical IPV. However, it is possible that the strength of the relationship between childhood violence and subsequent IPV varies by type of IPV experienced.
These analyses demonstrate a strong link between childhood violence and subsequent violence revictimization by an intimate partner among adolescent girls and young women in Namibia. This study supports the need for interventions to reduce violence against children, and more work, including qualitative research, is needed to explore the psychological and community-level mechanisms for this association to identify early intervention opportunities and to understand the context around childhood violence and IPV experiences. The World Health Organization and U.S. Centers for Disease Control and Prevention package of evidence-based strategies to end violence against children (“INSPIRE”) includes approaches to change norms around childhood violence and improve caregiver support, economic strengthening, and life and social skills (World Health Organization, 2016). Widescale adoption and implementation of these interventions has the potential to address determinants of both childhood and IPV.
Footnotes
Acknowledgments
The implementation of the Namibian VACS survey would not have been possible without the trust and participation of the participants, whose aggregated experiences the authors hope will help inform improved policies going forward. The leadership by the Ministry of Gender Equality and Child Welfare of the multi-sectoral VACS Steering Committee and the Ministry of Health and Social Services of the HIV Testing Technical Working Group, ensured high-quality survey implementation. The Namibia Statistics Agency provided national leadership and survey implementation by a large team of statisticians, enumerators and technical support staff. Lastly, the authors wish to acknowledge the leadership and scientific contributions of Leah Gilbert, Howard Kress, Greta Massetti, and Caroline Stamatakis from the Centers of Disease Control’s (CDC) Division of Violence Prevention; Jennifer Hegle of CDC’s Division of Global HIV & Tuberculosis; and Adam Wolkon from CDC Namibia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project has been supported by the President’s Emergency Plan for AIDS Relief (PEPFAR) through the U.S. Centers for Disease Control (CDC) under the terms of cooperate agreement 5U2GGH001430. Technical expertise for the implementation and evaluation of this project was provided by the CDC Division of Global HIV and TB (CDC/DGHT). The findings in this article are those of the authors and do not necessarily represent the official position of the CDC or PEPFAR. JV was supported by the National Institute of Allergy and Infectious Diseases (grant T32 AI007140) and the National Institute of Mental Health (K99 MH123369).