
Abstract
Intimate partner aggression (IPA) victimization and substance use have been well established as risk factors for IPA perpetration (Leonard, 2005; Sprunger et al., 2015). Recent research has identified a negative association between distress tolerance and physical and psychological IPA perpetration, specifically in males in substance use treatment (Shorey et al., 2017). Research examining the interplay of problem substance use, distress tolerance, and other forms of IPA (i.e., sexual coercion, controlling behaviors) in non-clinical samples is limited. The present analysis aimed to examine the potential moderating effect of distress tolerance on problem alcohol use and four types of IPA perpetration (physical assault, psychological aggression, sexual coercion, and controlling behaviors) in a diverse, national sample (N = 323; 44.3% female; 52.9% sexual minority; age M = 33.61 years, SD = 8.71). Results showed that alcohol use and distress tolerance had differing influences on each IPA perpetration type. In line with hypotheses, distress tolerance significantly moderated the relationship between problem alcohol use and two forms of IPA (physical assault and controlling behaviors); this relationship was stronger for individuals with low levels of distress tolerance. Significant interaction effects did not emerge for psychological aggression or sexual coercion. Findings suggest that treatment strategies that focus specifically on increasing distress tolerance may be effective in reducing alcohol-facilitated IPA perpetration involving physical assault and controlling behaviors.
Keywords
Introduction
Intimate partner aggression (IPA) is defined as physical, sexual, or emotional aggression by a current or past partner or spouse (Centers for Disease Control and Prevention [CDC], 2020). IPA is a significant public health concern and accounts for approximately 20% of all homicides in the United States (CDC, 2020). Rates of perpetration are high, with as many as 1 in 4 women and 1 in 5 men reporting IPA perpetration (Desmarais et al., 2012). Moreover, IPA victimization is associated with numerous physical and psychological health consequences (Coker et al., 2002; Dutton et al., 2006; Wu et al., 2010). Researchers have examined various factors that increase risk of victimization (Coker et al., 2002; Gass et al., 2011), however, there has been comparatively less research on risk factors associated with IPA perpetration.
IPA can take different forms, such as physical assault, psychological aggression, controlling behaviors, and sexual coercion. Although physical violence (e.g., grabbing or hitting partner) is the most commonly studied form of IPA, psychological abuse can produce uniquely damaging consequences (Follingstad et al., 1990). Psychological aggression involves both verbal (e.g., shouting at partner) and nonverbal acts (e.g., stomping out of the room) directed toward a partner. Controlling behaviors, which are actions explicitly aimed to establish power and control over one’s partner (e.g., monitoring partner’s time and whereabouts), are distinct from psychological aggression (Hines & Douglas, 2010). Lastly, sexual coercion (e.g., threats to make partner have sex) involves behaviors aimed at making the partner engage in non-consensual sexual activity. Although these distinct forms of IPA may be correlated or co-occur (e.g., Follingstad et al., 1990), they may also have different patterns of risk factors. For example, there are typically higher rates of non-physical aggression (e.g., psychological abuse, controlling behaviors) compared to physical aggression within intimate relationships (Thompson et al., 2006), which may suggest that there are different risk factors or relative strength of risk factors for particular forms of IPA. Furthermore, these differences in rates may or may not be due to the relative weight of disinhibiting influences for each form of aggression.
Alcohol use is one of the most robust predictors of violence perpetration in intimate relationships (Foran & O’Leary, 2008; Leonard, 2005; Leonard & Quigley, 2017; Rothman et al., 2012; Shorey et al., 2011). Research has demonstrated a stronger relationship between alcohol use and IPA perpetration in those who meet criteria for problem drinking (Kessler et al., 2001; O’Leary & Schumacher, 2003; Sugarman et al., 1996). Further, intervention studies reveal that reduction in alcohol consumption is associated with reduction in IPA perpetration (Murphy & Ting, 2010; Stuart et al., 2009). Despite these consistent findings, the linear and causal relationship between alcohol and IPA perpetration seems more complex than previously understood (O’Leary & Schumacher, 2003). Indeed, alcohol consumption alone seems to have only small to moderate effect sizes in predicting IPA perpetration (Cafferky et al., 2018; Foran & O’Leary, 2008; Leonard, 2005). Therefore, more nuanced investigations into moderating factors that have the potential to influence IPA perpetration within the context of problem alcohol use are warranted.
Existing theory describes how alcohol may increase risk for alcohol-related IPA perpetration in relationships. The alcohol myopia theory (AMT; Steele & Josephs, 1990), one of the best-accepted theories detailing the effects of alcohol on behavior, posits that alcohol causes a narrowing effect on attention, which ultimately limits the range and number of both internal and external cues that a person can perceive and process; this results in a person only attending to stimuli and cues in their environment that are the most salient, immediate, and attention-grabbing, which can promote aggressive behavior. Relatedly, the I3 Theory (Finkel, 2007; Finkel & Eckhardt, 2013) suggests that the likelihood of IPA perpetration occurring in a given situation depends on instigation, impellance, and inhibition. Instigating factors refer to factor(s) that produce an urge to behave aggressively. Such factors provide the initial momentum toward an aggressive act and signal that such an aggressive act is available. Feeling provoked (e.g., someone yells at you) would be an instigating factor. Impelling factors refer to situational and/or dispositional factors that prepare or predispose a person to experience a strong urge to respond aggressively when faced with an instigating factor. An impelling factor could be a specific personality trait (e.g., high trait anger) and, when mixed with an instigating factor, results in increased odds that one will feel inclined to aggress. Disinhibiting influences (e.g., alcohol use) further increase the odds that a person will not be able to resist an urge to aggress; disinhibiting factors deplete one’s inhibitory capacity.
Inhibitory factors, in contrast, refer to factors that decrease the likelihood that a person will act on an urge to aggress in response to instigating factors; if a person’s inhibitory surge is equal to or greater than their urge to aggress, they will not behave aggressively (Eckhardt et al., 2015). Recent research has identified a conceptual and neural overlap between inhibitory processes and emotion regulation (Bartholomew et al., 2019). Such top-down control of one’s emotions, whether explicit or implicit, allows one to pursue goal-directed behavior (e.g., not harming one’s partner, engaging in constructive dialog) even in the face of aversive mental or affective states. In fact, research has demonstrated an association between emotion regulation deficits and IPA perpetration (Bliton et al., 2016; Ortiz et al., 2015; Shorey et al., 2011). For example, people are more likely to engage in aggression while intoxicated if they endorse high hostility (Bailey & Taylor, 1991), avoidant coping (Schumacher et al., 2008), high state-trait anger (Eckhardt, 2007), antisocial traits (Jacob et al., 2001), and a verbally aggressive conflict style (Leonard & Quigley, 1999). Furthermore, the “Perfect Storm Theory,” coined by Finkel (2007), posits that individuals are most likely to enact an aggressive behavior in a specific situation when instigating and impellance factors are high and inhibitory factors are low. In the case of alcohol-facilitated IPA, a person is most likely to perpetrate violence when they already have a propensity for violence and anger (high impellance), are provoked (high instigating factor), and are under the influence of alcohol (low inhibition). These three co-occurring factors are considered necessary and sufficient for predicting aggressive behavior, such as IPA (Eckhardt et al., 2015). Thus, individuals with difficulty managing intense emotional states seem more inclined toward alcohol-facilitated aggression.
In a parallel line of work, researchers have found that dysfunction in a specific emotion regulation process, distress tolerance, is predictive of significant alcohol-related consequences. Distress tolerance is the extent to which one can experience and withstand aversive experiential states (Simons & Gaher, 2005). Individuals who engage in problem drinking may have lower levels of distress tolerance (Ali et al., 2013; Bornovalova et al., 2012; Buckner et al., 2007; Daughters et al., 2005) and may drink as a way to cope with negative emotions (Buckner et al., 2007; Howell et al., 2010). Additionally, distress tolerance is associated with several of the aforementioned factors above (i.e., anger reactivity) that increase risk for alcohol-facilitated IPA perpetration (Ellis et al., 2013). Thus, the combination of problem alcohol use and low distress tolerance may significantly increase risk of aggression perpetration. Moreover, research examining the role of inhibitory processes, such as distress tolerance, on different forms of IPA is lacking. Recent investigations point to high distress tolerance as a potential protective factor in certain types of alcohol-facilitated aggression (i.e., psychological IPA), though much of the existing research examines these associations in samples in substance use treatment (e.g., Shorey et al., 2017; Watkins et al., 2016) or those arrested for domestic violence (e.g., Brem et al., 2018), leaving room for greater inquiry into these potentially interacting processes.
The field has well established cognitive theories of alcohol-facilitated IPA, though less is known about the potential inhibitory role of emotion regulation processes, such as distress tolerance, in the relationship between problem alcohol use and different types of IPA perpetration. Importantly, the present study examines the unique and interactive roles of problem alcohol use and distress tolerance in predicting perpetration across four types of IPA (i.e., physical assault, psychological aggression, sexual coercion, and controlling behaviors) in a diverse, national sample. We hypothesize that problem alcohol use will predict IPA perpetration while controlling for the effect of IPA victimization, as research shows that IPA victimization is a strong predictor of perpetration (Sprunger et al., 2015). We also predict that distress tolerance will moderate the relationship between problem alcohol use and IPA perpetration, meaning that at high levels of distress tolerance, the association between problem alcohol use and IPA perpetration will be nonsignificant.
Method
Participants
Participants ages 18–59 years old were recruited using Amazon Mechanical Turk Crowdsourcing Platform (MTurk; Litman et al., 2017). MTurk is a well-validated research platform and allows for recruitment of nationally representative samples (Berinsky et al., 2012). It is an especially useful recruitment methodology for studies concerning clinical phenomena since MTurk participants tend to experience more psychological distress than the general population (Arditte et al., 2016; Shapiro et al., 2013). The 18–59 years age range was chosen to avoid issues related to mandated reporting laws concerning child and elder abuse. Recruitment was stratified to ensure 50% of respondents identified as a sexual minority (SM) as these data are part of a larger study examining IPA in SM and non-SM relationships. In the current analyses, SM status was not related to IPA perpetration on the bivariate level, therefore, we chose to use the full sample and not include SM status as a variable in the model. The mean age was 33.61 years (SD = 8.71). Table 1 includes demographic information for the sample used in analyses, which includes those with and without a history of IPA perpetration (full sample: N = 323). Two-hundred forty-six participants (76.2%) endorsed perpetrating at least one type of IPA in the past year: physical assault (n = 72; 22.3%), psychological aggression (n = 237; 73.4%), sexual coercion (n = 68; 21.1%), controlling behaviors (n = 81; 25.1%).
Demographics.
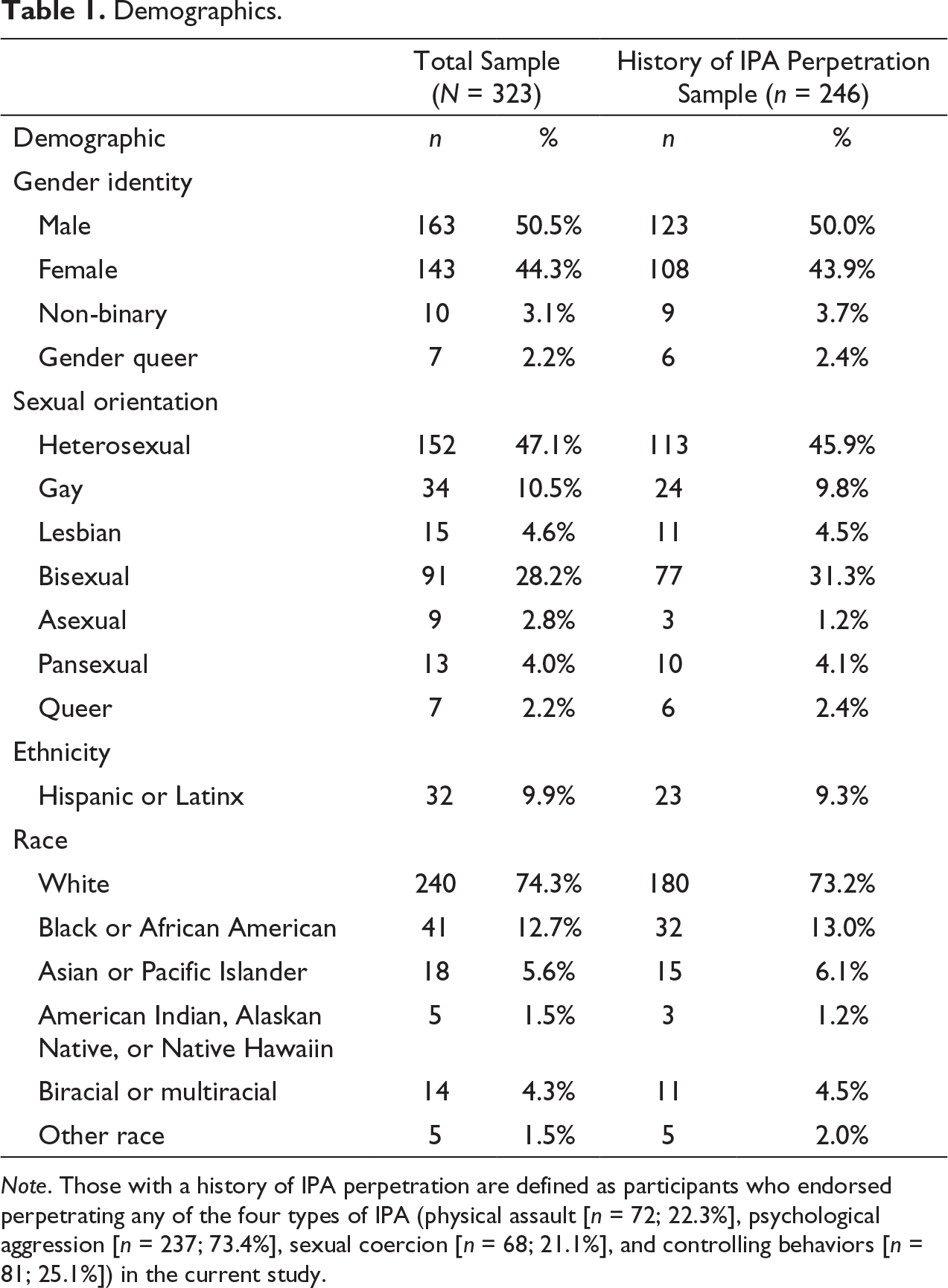
Note. Those with a history of IPA perpetration are defined as participants who endorsed perpetrating any of the four types of IPA (physical assault [n = 72; 22.3%], psychological aggression [n = 237; 73.4%], sexual coercion [n = 68; 21.1%], and controlling behaviors [n = 81; 25.1%]) in the current study.
Procedure
Study methods were approved by the university’s Institutional Review Board. Participants were compensated a minimum wage rate ($11/hour) to complete the online survey using Qualtrics Survey System. The survey took an average of 20 minutes to complete, therefore resulting in payment of about $4 per participant.
Measures
Alcohol Use Disorders Identification Test (Babor et al., 2001).
The Alcohol Use Disorders Identification Test (AUDIT) is a 10-item self-report measure that assesses past-year alcohol use and related consequences. Response options are summed to create a total score, ranging from 0 to 40, with higher scores reflecting greater alcohol use severity. The AUDIT has demonstrated strong reliability and validity in previous studies (Kokotailo et al., 2004; Reinert & Allen, 2007); it showed strong internal consistency in the current sample (α = .89).
Distress Tolerance Scale (Simons & Gaher, 2005).
The Distress Tolerance Scale (DTS) is a 15-item self-report measure of emotional distress tolerance, which consists of four subscales: Regulation, Tolerance, Absorption, and Appraisal. Participants rate items on a 5-point Likert scale ranging from 1 (strongly agree) to 5 (strongly disagree). The present study utilized the average score, with higher scores indicating a greater ability to tolerate distress. This measure has shown good internal consistency and convergent and divergent validity (Simons & Gaher, 2005); it showed excellent internal consistency in the current sample (α = .96).
Revised Conflict Tactics Scale (Straus et al., 1996).
The Conflict Tactics Scale (CTS2) assessed the occurrence of IPA perpetration and victimization in the past year. The present studied utilized the psychological aggression, physical assault, and sexual coercion subscales. In addition, a subscale assessing controlling behaviors (Hines & Douglas, 2010) was also administered. Participants responded to items depicting each of the conflict tactics by indicating the number of times these tactics were used by the participant and/or their partner in the previous year. Participants indicated on a scale from 0 to 6 how many times they experienced each of the acts in the previous year: 0 = 0 times; 1 = 1 time; 2 = 2 times; 3 = 3–5 times; 4 = 6–10 times; 5 = 11–20 times; 6 = more than 20 times. As recommended by Straus et al. (1996), these data were then transformed to create chronicity scores. The transformation results in an approximate count of the number of times each act occurred in the previous year, using the following scale: 0 = 0 acts in previous year (coded 0); 1 = 1 act in the previous year (coded 1); 2 = 2 acts in the previous year (coded 2); 3 = 4 acts in the previous year (coded 4); 4 = 8 acts in the previous year (coded 8); 5 = 15 acts in the previous year (coded 15); 6 = 25 acts in the previous year (coded 25). Missing items were conservatively coded 0. Subscale items were then summed to create past-year perpetration frequency scores for each type of perpetration. A dichotomous score was created for victimization status across the different types of IPA. The CTS2 is a valid and reliable assessment of intimate partner conflict (Straus et al., 1996). The four perpetration subscales had alpha values ranging from .75 (psychological aggression) to .94 (physical assault) in the current sample, which are comparable to the CTS2 reliability statistics reported in Hines & Douglas (2010).
Results
Analytic Strategy
We used R (Version 3.4.2; R Core Team, 2017) and the R-packages haven (Version 1.1.1; Wickham & Miller, 2018), pscl (Version 1.5.5; Zeileis et al., 2008), and interactions (Version 1.1.0; Long, 2019) to run the analyses.
Separate models were conducted for each of the four types of IPA perpetration. As mentioned previously, because SM status was not significantly related to any of the IPA outcomes on the bivariate level, we chose not to include this variable as a predictor in our models. Interaction variables were mean-centered prior to analysis and IPA victimization status was entered as a covariate in each model. As is typical with count data, the perpetration scores were highly skewed and kurtotic; the modal response was 0, indicating that the majority of participants reported no IPA perpetration in the past year, with the exception of psychological aggression. As such, zero-inflated Poisson (ZIP) regression models were used to account for the high frequencies of zero in the scores representing frequency of physical assault perpetration, controlling behaviors, and sexual coercion in the past year. ZIP models can appropriately account for the large number of zeros in count outcomes (Atkins & Gallop, 2007) and have been frequently used with violence perpetration data (e.g., Milletich et al., 2010; Song et al., 2017). Results of ZIP models are divided into two parts: (a) prediction of dichotomous IPA perpetration (i.e., zero-inflation model [binomial with logit link]), and (b) of those who perpetrated IPA, prediction of IPA perpetration frequency (i.e., count model [Poisson with log link]). A traditional Poisson regression model was used to predict psychological aggression because this outcome was not zero-inflated. Significant interactions were visualized using simple-slopes analyses. Table 2 includes correlations, means, and standard deviations for the variables included in each model.
Descriptives and Intercorrelations for Variables in Models (N = 323).
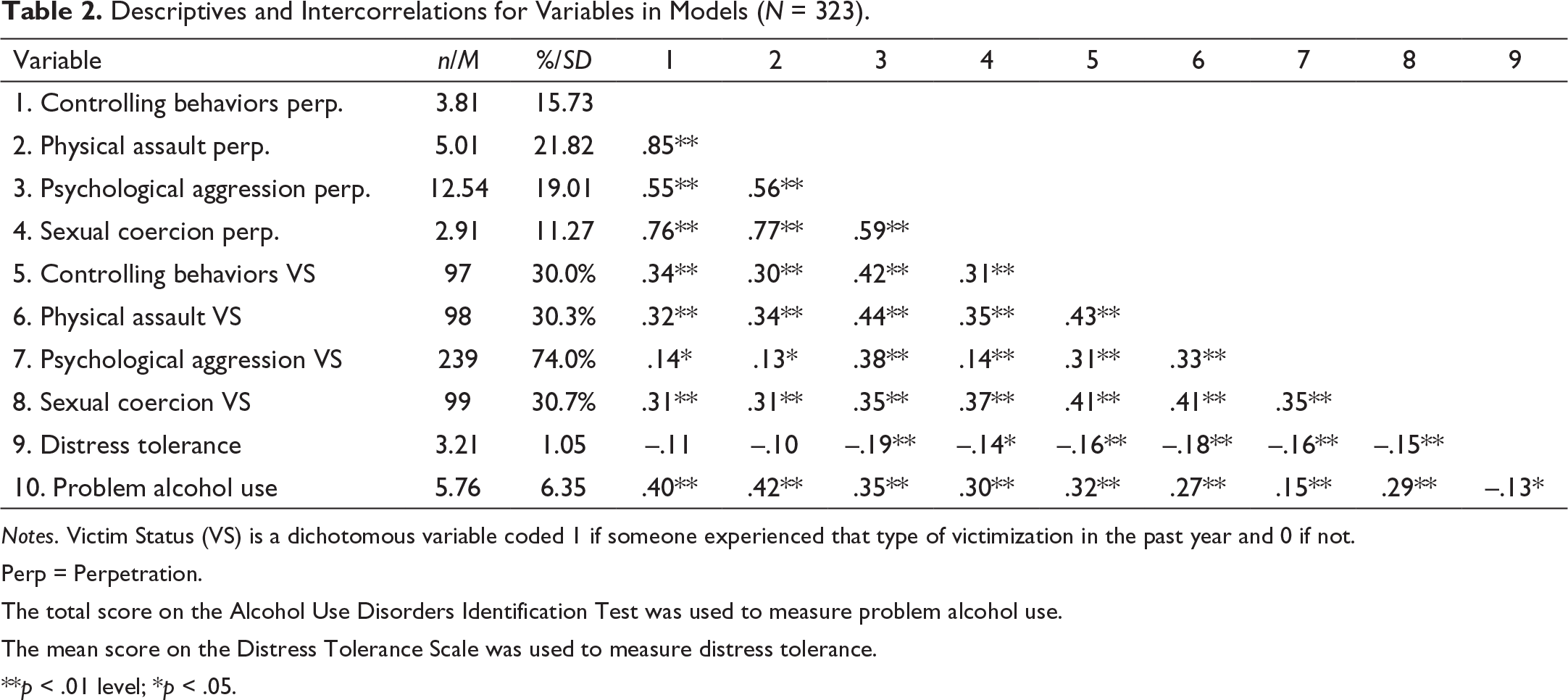
Notes. Victim Status (VS) is a dichotomous variable coded 1 if someone experienced that type of victimization in the past year and 0 if not.
Perp = Perpetration.
The total score on the Alcohol Use Disorders Identification Test was used to measure problem alcohol use.
The mean score on the Distress Tolerance Scale was used to measure distress tolerance.
**p < .01 level; *p < .05.
Poisson Models
Results for the Poisson model predicting psychological aggression perpetration are presented in Table 3. Significant main effects of problem alcohol use, distress tolerance, and victim status emerged. More problem alcohol use and victim status were related to higher rates of psychological aggression perpetration frequency. In contrast, more distress tolerance was related to less psychological aggression frequency.
Poisson Regression Results for Psychological Aggression Perpetration.
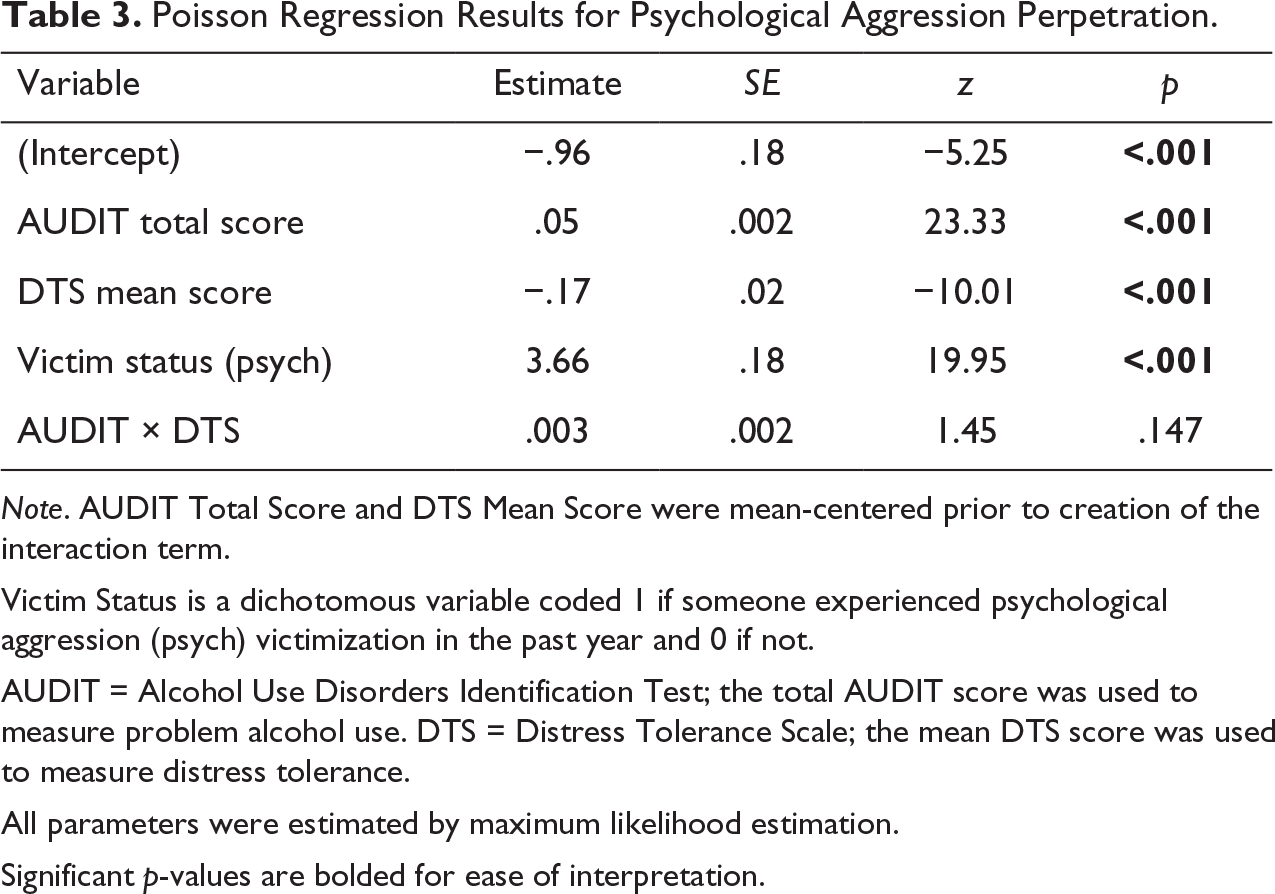
Note. AUDIT Total Score and DTS Mean Score were mean-centered prior to creation of the interaction term.
Victim Status is a dichotomous variable coded 1 if someone experienced psychological aggression (psych) victimization in the past year and 0 if not.
AUDIT = Alcohol Use Disorders Identification Test; the total AUDIT score was used to measure problem alcohol use. DTS = Distress Tolerance Scale; the mean DTS score was used to measure distress tolerance.
All parameters were estimated by maximum likelihood estimation.
Significant p-values are bolded for ease of interpretation.
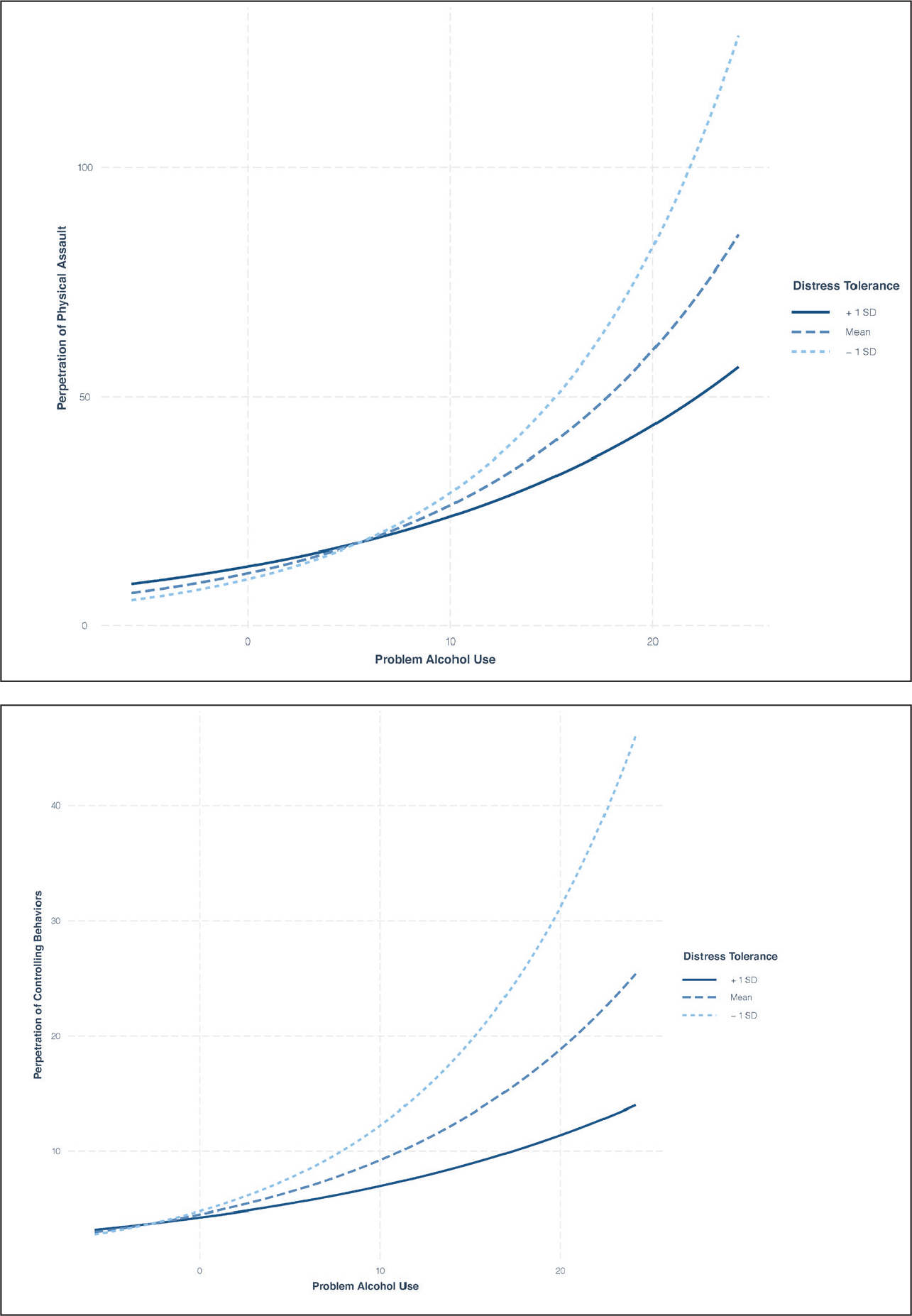
Results for the ZIP model predicting physical assault perpetration are presented in Table 4. For the zero-inflation portion of the model, problem alcohol use and victim status were significantly related to greater odds of perpetration; greater distress tolerance was significantly related to lesser odds of perpetration. For the count portion of the model, of those who perpetrated physical assault, victim status and the interaction between problem alcohol use and distress tolerance emerged as significant predictors. At higher levels of distress tolerance (1 SD above the mean), the relationship between problem alcohol use and physical assault perpetration was weaker than when distress tolerance was average or low. Refer to Figure 1 for a visualization of the simple slopes.
Simple slopes of problem alcohol use predicting perpetration of physical assault frequency (top figure) and controlling behaviors frequency (bottom figure) for 1 SD below the mean of distress tolerance, the mean of distress tolerance, and 1 SD above the mean of distress tolerance.
Zero-inflated Poisson Regression Results.
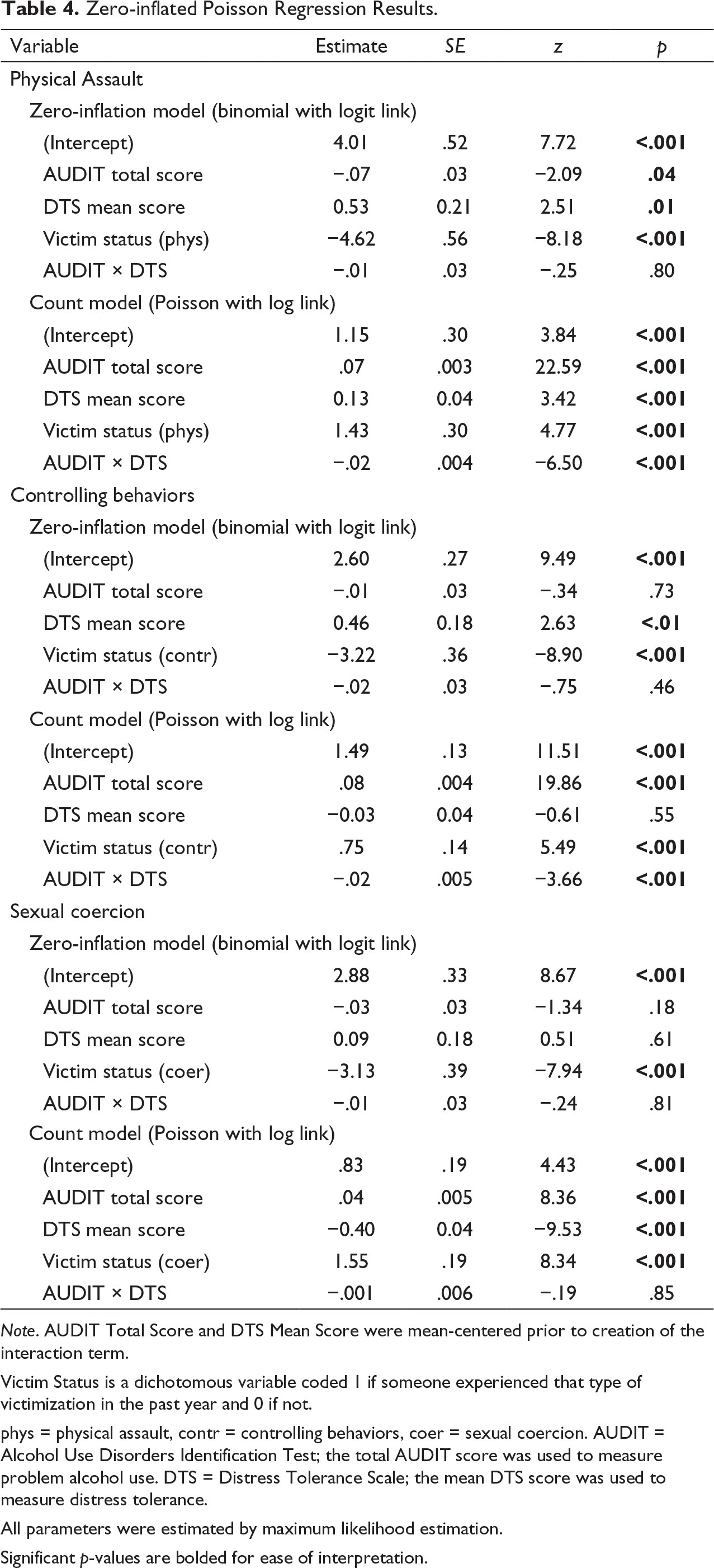
Note. AUDIT Total Score and DTS Mean Score were mean-centered prior to creation of the interaction term.
Victim Status is a dichotomous variable coded 1 if someone experienced that type of victimization in the past year and 0 if not.
phys = physical assault, contr = controlling behaviors, coer = sexual coercion. AUDIT = Alcohol Use Disorders Identification Test; the total AUDIT score was used to measure problem alcohol use. DTS = Distress Tolerance Scale; the mean DTS score was used to measure distress tolerance.
All parameters were estimated by maximum likelihood estimation.
Significant p-values are bolded for ease of interpretation.
Results for the ZIP model predicting controlling behaviors perpetration are presented in Table 4. For the zero-inflation portion of the model, distress tolerance and victim status were significant predictors. Victim status predicted greater odds of controlling behavior perpetration; in contrast, greater distress tolerance was related to lesser odds of perpetration. For the count portion of the model, of those who perpetrated controlling behaviors, victim status and the interaction between problem alcohol use and distress tolerance emerged as significant predictors. At higher levels of distress tolerance (1 SD above the mean), the relationship between problem alcohol use and controlling behaviors perpetration was weaker than when distress tolerance was average or low. Refer to Figure 1 for a visualization of the simple slopes.
Results for the ZIP model predicting sexual coercion IPA perpetration are presented in Table 4. For the zero-inflation portion of the model, only victim status was a significant predictor, such that victim status was related to greater odds of perpetrating sexual coercion. For the count portion of the model, of those who perpetrated sexual coercion, victim status, distress tolerance, and problem alcohol use were significant predictors. Victim status and greater problem alcohol use were related to greater sexual coercion frequency; greater distress tolerance was related to lesser frequency.
Discussion
There is a robust literature documenting the association between problem substance use and IPA perpetration. Distress tolerance has emerged as a significant process related to substance use, and may represent a protective factor in the relationship between problem substance use and IPA. To our knowledge, only one study has investigated the link between distress tolerance and IPA perpetration, namely, physical assault and psychological aggression, within a sample of men in substance use treatment (Shorey et al., 2017). The present study extends the current literature by examining the unique and interactive roles of problem alcohol use and distress tolerance in predicting perpetration across four types of IPA (i.e., physical assault, psychological aggression, sexual coercion, and controlling behaviors) in a diverse, national sample. We found that problem alcohol use was predictive of IPA perpetration occurrence and frequency across multiple types of IPA. Most notably, the relationship between problem alcohol use and two types of IPA frequency (physical assault and controlling behaviors) was stronger for individuals with low levels of distress tolerance.
Results from the current study are consistent with extant theory and research indicating alcohol use as a strong predictor of IPA perpetration. Problem alcohol use significantly predicted odds of perpetrating physical assault while controlling for the effect of IPA victimization. Further, alcohol use was significantly related to the frequency of all four types of IPA, through either a main effect (psychological aggression, sexual coercion) or interaction effect with distress tolerance (physical assault, controlling behaviors). These findings are in line with studies revealing a strong link between perpetration and problem substance use (Foran & O’Leary, 2008; Leonard, 2005; Leonard & Quigley, 2017; Rothman et al., 2012; Shorey et al., 2011), as well as increased risk for violence recidivism among those with a history of violence and problem substance use (Stuart, 2005; Stuart et al., 2007).
Distress tolerance significantly predicted odds of perpetrating physical assault and controlling behaviors. Further, distress tolerance was significantly related to the frequency of all forms of IPA, through either a main effect (psychological aggression, sexual coercion) or interaction effect with problem alcohol use (physical assault, controlling behaviors). Thus, an inability to self-regulate and tolerate aversive emotional states may lead individuals to be more susceptible to perpetrating aggression toward their partners. These findings are in line with previous research highlighting how individuals with a disposition toward distress intolerance may be more prone to act out in violent ways as a way to regulate their internal state or mood (Jakupcak, 2003; Ortiz et al., 2015; Shorey et al., 2011). Moreover, distress tolerance was a significant moderator of the relationship between problem alcohol use and perpetration of physical assault and controlling behaviors, such that for individuals with low distress tolerance, greater problem alcohol use was associated with more severe perpetration, whereas this relationship was significantly weaker for individuals with average or high distress tolerance. This finding suggests that, during drinking episodes, individuals who struggle to withstand negative effects may lack the ability to override violent behavior with adaptive responses. From an I3 Theory perspective, distress tolerance may function as an inhibitory factor that increases the likelihood of resisting an urge to behave aggressively at a specific point in time (Eckhardt et al., 2015). Further, low distress tolerance may exacerbate the disinhibitory effect of alcohol use, leading individuals to become more susceptible to acting on impelling and instigating factors. Moreover, alcohol intoxication’s narrowing effect on attention has the potential to further amplify provocative external and internal cues that can escalate distress in the moment and thus, instigate aggressive behavior (Steele & Josephs, 1990).
Interestingly, although there were significant main effects of distress tolerance and problem alcohol use on psychological aggression and sexual coercion, we did not find a significant interaction between distress tolerance and problem alcohol use for those forms of IPA. These findings suggest distress intolerance may be a risk factor for perpetrating sexual coercion and psychological aggression, but there is no additive effect of distress intolerance and problem substance use that increases risk. Future research should further examine the differences between types of alcohol-facilitated IPA and in the moment affective experiences and distress tolerance processes.
Findings from the current study lend support for distress tolerance as an important treatment target for individuals presenting with problem alcohol use and IPA. Treatment for individuals with a history of IPA perpetration should focus on decreasing alcohol use and developing adaptive strategies for managing distress, specifically by decreasing avoidance and building skills for processing and regulating in the moment. Interventions with a principle focus on distress tolerance (e.g., Dialectical Behavior Therapy, Acceptance and Commitment Therapy) have shown promise in reducing alcohol use and aggression (Bornovalova et al., 2012; Frazier & Vela, 2014; Zarling et al., 2015). Another important implication of this work is to screen for IPA perpetration, victimization, and distress tolerance in substance use treatment settings, as there are high rates of IPA in these settings (Stuart et al., 2009). Finally, future research should investigate how treatment approaches aimed to increase distress tolerance corresponds to reductions in alcohol use and IPA perpetration over time.
This study makes important contributions to the current literature. Our findings are strengthened by the use of a diverse, non-clinical sample of individuals endorsing varying degrees of alcohol use and IPA perpetration. The mean score on the AUDIT fell below the threshold for clinically significant alcohol use (Babor et al., 2001), indicating that alcohol use and distress tolerance were predictive of IPA perpetration among individuals who may not view their use as problematic or consider seeking treatment. Further, much of the current literature focuses on IPA perpetration in heterosexual relationships even though research shows that SMs are at equal, if not greater, risk for IPA perpetration, victimization, and problem substance use (Dermody et al., 2014; Edwards et al., 2015; Shorey et al., 2019). The present study encompassed approximately 50% SMs and found that SM status was not significantly related to any of the IPA outcomes, which may suggest that the relationships among alcohol use, distress tolerance, and IPA perpetration are similar within SM and non-SM relationships. Lastly, the sample was not restricted by gender, which allowed for examination of these relationships across a variety of intimate partner dynamics (e.g., male to female, female to female, female to male, male to male violence).
There are several limitations to the present study that merit consideration. First, this study utilized self-reports of IPA perpetration and may reflect underestimates of actual rates related to a social desirability response bias, especially in terms of sexual and severe IPA items (Dobash et al., 1998; Kimmel, 2002). However, the physical, psychological, and controlling behavior rates are similar to those reported by the community sample in Hines & Douglas (2010); sexual coercion perpetration rates were similar to those reported in Brousseau et al. (2011). Additionally, the data in this study are cross-sectional and the presence of alcohol use and/or negative affect at the time of IPA perpetration could not be determined. Research utilizing longitudinal and event-level designs would elucidate how alcohol use and distress tolerance interact to generate specific instances of IPA. Furthermore, it is important for future research to investigate how specific drinking behaviors, such as binge drinking, and episodes of intoxication confer risk for different types of IPA.
The present study extends the existing literature by clarifying relationships between alcohol use, distress tolerance, and IPA perpetration in a diverse, national sample. Findings show that alcohol is an important risk factor for IPA perpetration. Among those with a history of aggression who engage in problem alcohol use, those with a disposition toward distress intolerance appear to be at greater risk of perpetrating physical assault and controlling behaviors. Thus, results point to distress tolerance as an important protective factor that may reduce the risk of alcohol-facilitated IPA. More broadly, this work encourages further investigation into the inhibitory role of emotion regulation processes, specifically within cognitive theoretical frameworks (e.g., AMT, I3 Theory), in future IPA intervention and prevention research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this work was made possible by the Department of Psychology at Clark University.