
Abstract
Colombia endured 70 years of internal conflict, but despite a peace agreement, violence continues to be significant in the post-conflict era. Violence degrades the health and well-being of affected populations and it engenders psychological distress. Little is known about the impact of violence on the mental health of sexual and gender minority populations in Colombia. This study aimed to examine the frequency and sources of violence among cisgender men who have sex with men (MSM) and transgender women and their association with depressive symptoms and substance use. We administered a survey to 942 MSM and 58 transgender women recruited using respondent-driven sampling. We estimated the relationship between mental health indicators and experiences of violence using stepwise logistic and linear regressions, controlling for income, education, age, race, and mistreatment for being effeminate when younger. Respondent-driven sampling adjusted prevalence of any type of violence was 60.9% for the total sample, 59.8% for MSM, and 75.1% for transgender women. Experiences of violence were significantly related to depressive symptoms, binge drinking and drug use for the MSM sample. Violence perpetrated by family members or acquaintances was associated with greater depressive symptoms, and violence perpetrated by partners and strangers was associated with increased binge drinking and drug use. These results provide significant evidence of the negative association of experiences of violence and the mental health of sexual and gender minority people, a vulnerable population in Colombia. This study addresses issues of diversity regarding sexual orientation and gender identity in a Latin American middle-income country.
Colombia experienced the longest internal conflict of any country in the Western hemisphere, roughly 70 years of low-intensity warfare from 1946 through 2016 (Arrubla Yepes, 1985; Bushnell, 1993; The Center for Justice & Accountability, 2016; US Department of State, 2018). Internal conflict of this nature is not limited to Colombia—the civil war in El Salvador lasted 12 years (Americas Watch Committee, 1991; Wood, 2003) and in Guatemala 36 years (Jonas, 2018; Puac-Polanco et al., 2015), and evidence suggests there is often continued violence after cease-fire agreements (Alpers et al., 2019; Escobar, 2012; Puac-Polanco et al., 2015; US Department of State, 2019).
Prolonged conflicts make violence culturally “normal,” which in turn has a downstream effect into civilians’ daily lives (Branas et al., 2013; Flores, 2013; Puac-Polanco et al., 2015). The Colombian conflict originated due to—and has further contributed to—economic inequality, which in turn fuels more violence (Flores, 2013). Despite the 2016 peace agreement between the Revolutionary Armed Forces of Colombia and the government, violence continues. According to recent data, approximately 15% of Colombia’s population is registered as internally displaced persons (United Nations High Commissioner for Refugees, 2018). More than 60,000 people have disappeared between 1970 and 2015 (Ortigosa et al., 2017; United Nations High Commissioner for Refugees, 2018), which surpasses the number of disappeared during the military regimes in Chile and Argentina together. In 2012, around the time we collected data for this paper, there were 15,742 homicides in Colombia, a rate of 34/100,000, whereas in the USA it was 5.3/100,000 (Butchart & Mikton, 2014). In 2018, 145,000 citizens were displaced as a consequence of conflict (Internal Displacement Monitoring Centre, 2019) and in 2019 alone, 250 social leaders were assassinated (El Tiempo, 2019).
Violence degrades the health and well-being of affected populations, not only through direct physical injury, but also by engendering psychological distress manifested in both internalizing (e.g., depression) and externalizing (e.g., substance use) symptoms depending on the domains in which violence occurs (Lo et al., 2017; Roberts & Browne, 2011). A Colombia-based study showed that violence related to armed conflict was associated with depression and anxiety, whereas personal violence from other sources (e.g., child abuse, sexual violence) was linked to aggression and substance use as well as depression (Bell et al., 2012). Two comprehensive reviews of studies in low- and middle-income countries with populations living in areas of conflict found that individuals who had more violent or traumatic experiences presented poorer psychological health outcomes (Roberts & Browne, 2011) and more problematic alcohol use (Lo et al., 2017). Studies in Colombia have also linked exposure to violence, armed conflict, and torture to poorer mental wellbeing among survivors, including increased prevalence of depressive and anxiety symptoms (Harpham et al., 2005; Hessel et al., 2019; Londoño et al., 2012; Santaella-Tenorio et al., 2018). According to findings from the Colombian 2015 nationally representative Mental Health Survey (N = 10,853), socioeconomic inequality, poverty, and exposure to the internal conflict were associated with poorer mental health outcomes (Cuartas Ricaurte et al., 2019). Furthermore, a study in Guatemala found that any exposure to the civil war there was associated with negative mental health outcomes thirteen years later (Puac-Polanco et al., 2015), suggesting that internal conflict can have long-lasting psychological effects on individuals. Notably, these studies did not assess or include in their analyses sexual orientation or gender identities other than male or female, and subsequently potential differences in experiences of violence and mental health outcomes among people with sexual and gender minority (SGM) identities in these samples remains largely overlooked.
Little is known about the impact of violence on the mental health of SGM populations in Colombia (Nieves-Lugo et al., 2019) despite evidence to suggest high levels of victimization among sexual minority populations in Colombia (Alcaldía Mayor de Bogotá et al., 2010; Ritterbusch et al., 2018; Sierra Alarcón et al., 2017; Zea et al., 2013), which they bear in addition to the significant risks to physical safety and life all Colombians face due to the internal conflict and generalized violence in the country (Centro Nacional de Memoria Histórica, 2015; Colombia Diversa, 2020a, 2020b). Many SGM individuals have been targeted for assassination and “social cleansing,” the practice of eliminating people considered undesirable (Schwartz, 1996; Zea et al., 2013). As of May 31, 2020, the official victims’ registry reported 3,974 SGM victims of the armed conflict (Colombia Diversa, 2020a). Armed groups involved in the conflict have used different modalities of violence against SGM people (Colombia Diversa, 2020a). Often, authorities do not investigate or protect SGM victims from sexual abuse, hate crimes, or other human rights violations and sometimes authorities themselves perpetrate human rights violations (Colombia Diversa, 2020b, 2012). Taken together, there is evidence to suggest the violence experienced among people with SGM identities may be compounded in severity and/or frequency. As such, further examination is warranted to understand better the experiences of violence among SGM populations and the relationship between these experiences and mental health outcomes. The current study examines the association between experiences of violence and the mental health of two SGM groups in Bogotá, Colombia: Cisgender men who have sex with men (MSM) and transgender women. Experiences of violence during childhood may also be especially important influences on mental health. A US-based study found that people from sexual minority groups were more likely to report adverse childhood experiences than heterosexual people, and that these experiences predicted negative outcomes such as binge drinking and depression (Austin et al., 2016). It is possible that similar associations may emerge in Colombia.
This study presents descriptive data on the frequency and sources of violence among Colombian MSM and transgender women. We also examined the association between experiences of violence and three indicators related to mental health: depressive symptoms, binge drinking, and drug use. We hypothesized that experiences of violence would be associated to poorer mental health outcomes even after controlling for demographic characteristics and youthful mistreatment for being effeminate. Furthermore, we explored the significance of violence perpetrated by different types of individuals as well as violence experienced by family members.
Methods
This research was part of a cross-sectional, mixed methods study on HIV prevalence, sexual risk, and attitudes toward circumcision among Colombian cisgender gay and bisexual men and transgender women (Zea et al., 2015).
Participants
Participants were recruited via respondent-driven sampling (RDS) (Heckathorn, 1997, 2011) to respond to a computerized survey and receive an HIV test. Inclusion criteria consisted of currently living in Bogotá, having had sex with a man in the previous six months, being assigned male at birth, and being between 18 and 49 years of age. We recruited participants over a period of ten months from 2011 to 2012. The resulting sample consisted of 942 MSM and 58 transgender women.
Demographic questions included age, education, income, and race. Participants’ mean age was 24.6 years (SD = 6.12; range 18–49) for MSM and 30.0 years (SD = 8.64; range 18–47) for transgender women. Level of education ranged from no schooling to having completed graduate school. The educational attainment was as follows: 3% of MSM and 33% of transgender women did not attend high school; 32% of MSM and 47% of transgender women had attended or completed high school or technical/commercial training; 49% of MSM and 17% of transgender women had attended university; and 16% of MSM and 3% of transgender women had completed university education or more. Income was assessed with a question: “Approximately how much money do you earn in a week?” Response options were expressed in Colombian pesos and ranged from 1 = $0–50,000 to 7 = More than 300,000. Median income was between 51,000 to 100,000 Colombian pesos per week (approximately $30–60) for both MSM and transgender women. To examine race, we asked participants “Which do you consider is your race/ethnic group?” There were 7 response options: Mestizo, referring to a biracial identity largely consisting of White and Indigenous ancestry (39.4% MSM and 36.2% transgender women); White (39.2% MSM and 39.7% transgender women); Multiracial/other (18.4% MSM and 15.5% transgender women); Mulatto, typically referring to biracial identity of Black and White (1.7% MSM and 1.7% transgender women); Afro-Colombian/Black (1.1% MSM and 5.2% transgender women); and Indigenous/Native (0.3% MSM and 1.7% transgender women). For the analyses, we collapsed Multiracial/other, Mulatto, Afro-Colombian-Black and Indigenous/Native.
Procedures
Participants completed a quantitative survey using computer assisted self-interview technology with audio enhancement (A-CASI) and touchscreen responding. The survey assessed a variety of topics; for this paper we used data on experiences of violence, psychological or psychosocial characteristics including depression, substance use, mistreatment when younger due to being effeminate, and demographic characteristics.
Measures
Mistreatment due to effeminacy.
A single item asked participants how frequently they had been mistreated for being effeminate when they were younger (Díaz et al., 2001). Response options were never (0), one or two times (1), several times (2), and many times (3). This variable was dichotomized into participants reporting no mistreatment and any mistreatment due to skewness of the distribution.
Experiences of violence.
The measure of experiences of violence consisted of 5 items with follow up questions. Participants were asked to indicate how frequently they had been severely beaten, attacked with a knife, shot, raped, and tortured. Response options included never (0), one or two times (1), several times (2), and many times (3). Participants who endorsed any such experience were also asked who had committed that form of violence. Response options for the follow-up questions were “my intimate partner, a member of my family, an acquaintance, a stranger.” Participants could indicate more than one kind of perpetrator. Participants were also asked if a family member had ever been severely beaten, attacked with a knife, shot, raped, killed, tortured, or kidnapped. This item served as an indicator of vicarious violence in the participant’s family (i.e., witnessing or learning of violence experienced by another).
Recent mental health outcomes.
Depressive symptoms in the previous week were assessed with a seven-item version of the CES-D (Radloff, 1977) (Cronbach’s alpha = 0.83). A sample item was “How often have you felt this way in the past week: I was bothered by things that usually don’t bother me.” Response options ranged from never or rarely (less than one day) (0) to most or all of the time (5–7 days) (3). Because of the extreme skewness of the distribution, we dichotomized this variable to reflect little or no depressive symptoms (i.e., less frequent than one day in the last week; coded as 0) vs. at least moderate frequency of symptoms (one day or more; coded as 1).
Binge drinking was assessed with a question concerning the frequency of having consumed five or more alcoholic drinks on a single occasion during the previous three months, with eight response options ranging from never (0) to at least once a day (7).
Drug use was assessed with a question asking participants how often they had used drugs (e.g., marihuana, cocaine, methamphetamines) in the previous three months. Due to the extreme skewness of the distribution of this variable, responses were dichotomized into participants reporting no such drug use in the previous three months and those reporting any such drug use during this period.
Analytic Plan
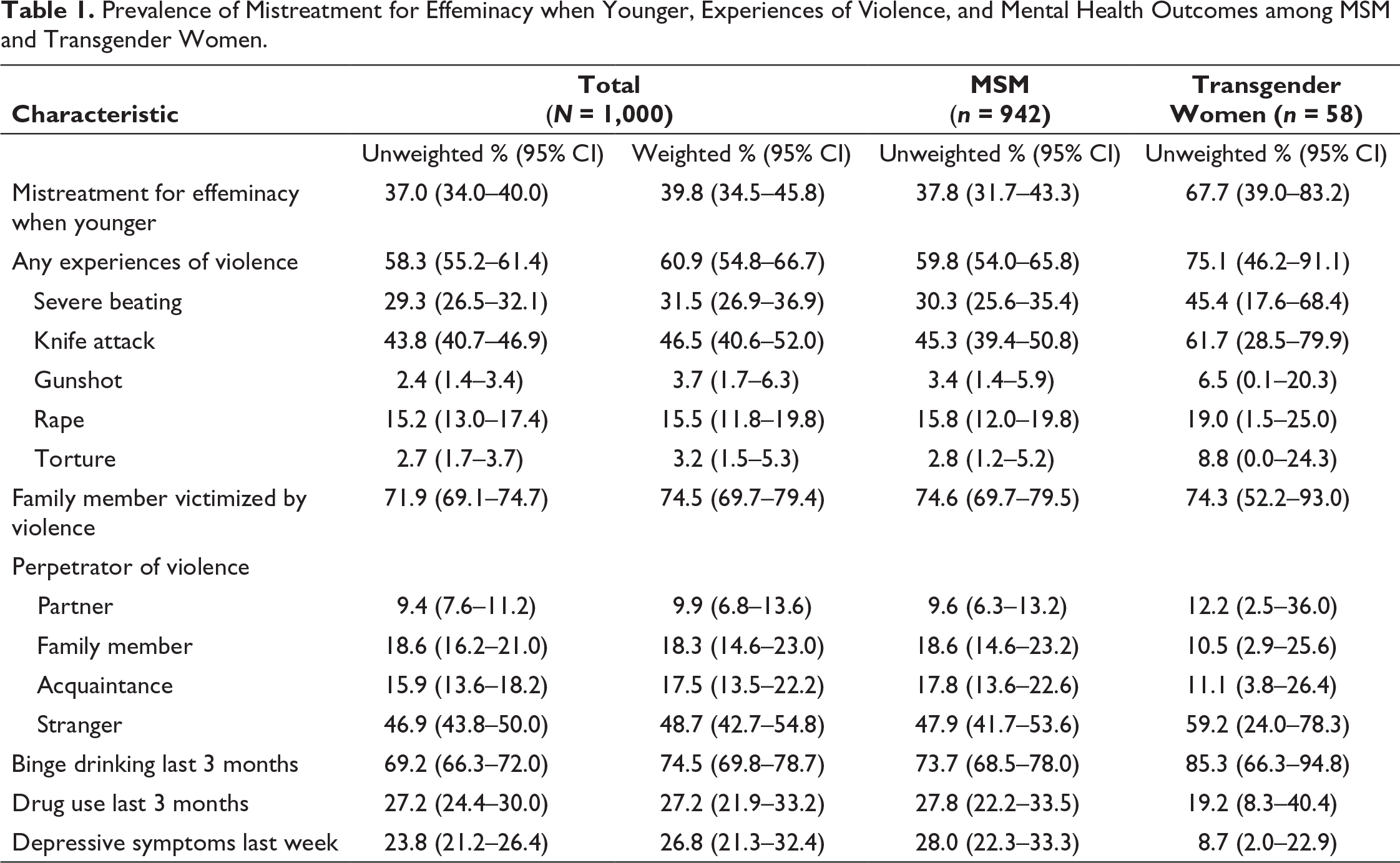
First, we calculated the prevalence of mistreatment for effeminacy when younger, the experiences of violence, and the mental health indicators for the MSM and transgender women samples together. We collapsed types of violence because some were endorsed by relatively few respondents. We used weighting to adjust for the non-random aspects of RDS (Heckathorn, 1997, 2011). To account for differential network size bias, we weighted the cases inversely by group network size. That is, participants who had larger networks were weighted down in the population estimate (Heckathorn, 1997, 2011). We used the Respondent Driven Sampling Analysis Tool (RDSAT) 7.1 to conduct the analyses (Volz et al., 2012). Next, we calculated the prevalence for the same variables of interest for the MSM and transgender women samples separately. The two samples were recruited together, and therefore weights were not available for the separate samples. For this reason, the prevalence estimates for the two samples and all subsequent analyses were unweighted. We investigated whether the prevalence of each of the variables of interest differed between the MSM and transgender women samples using a chi-square test of independence or Fisher’s exact test of independence based on cell size.
We conducted hierarchical set regressions to test our hypotheses. For binge drinking, we used linear regression, and for depressive symptoms and drug use, both of which were dichotomous, we used logistic regressions. The first set of explanatory variables consisted of demographic variables of income, education, and age; the second set consisted of mistreatment for effeminacy when younger; and the third set consisted of the experiences of violence by perpetrator and whether family members had experienced any violence. For each step in the hierarchical linear regression model, we calculated the change in R2 and used an F-test to test if the additional set of variables significantly contributed to the explanation of the outcome variables. For each step in the hierarchical logistic regression models, we calculated the change in the –2 log likelihood between the two models and used a chi-square test to test for significance of each step. This test is comparable to the change-in-R2 approach (Hosmer et al., 2013). We conducted these analyses separately for the MSM and transgender women samples.
Results
Prevalence and Perpetrators of Violence
Prevalence of Mistreatment for Effeminacy when Younger, Experiences of Violence, and Mental Health Outcomes among MSM and Transgender Women.
Frequencies of Type of Violence by Perpetrator among MSM and Transgender Women.
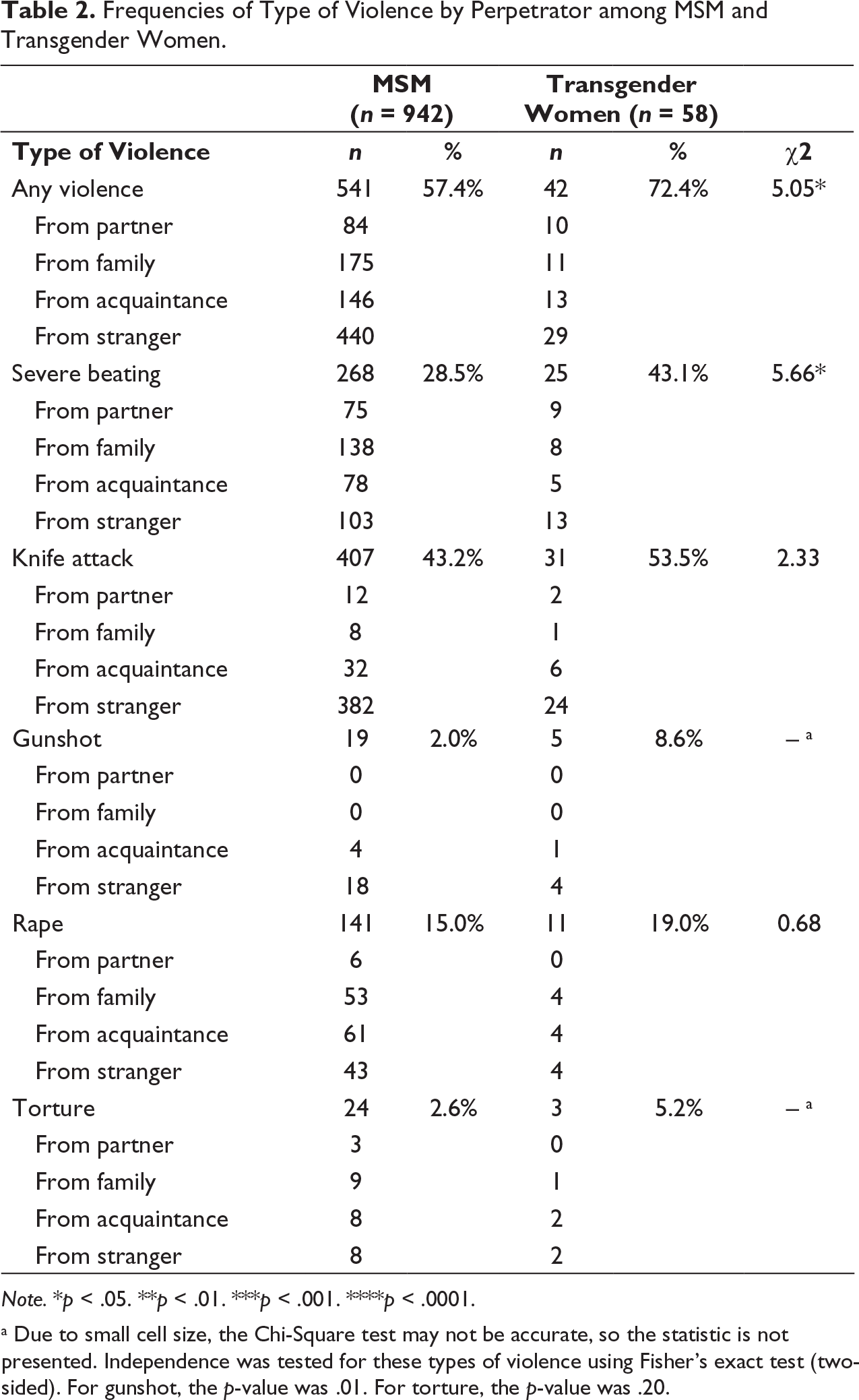
Note. *p < .05. **p < .01. ***p < .001. ****p < .0001.
a Due to small cell size, the Chi-Square test may not be accurate, so the statistic is not presented. Independence was tested for these types of violence using Fisher’s exact test (two-sided). For gunshot, the p-value was .01. For torture, the p-value was .20.
Correlations among Demographic Variables, Perpetrator of Violence, Depressive Symptoms, Binge Drinking, and Drug Use among MSM and Transgender Women.
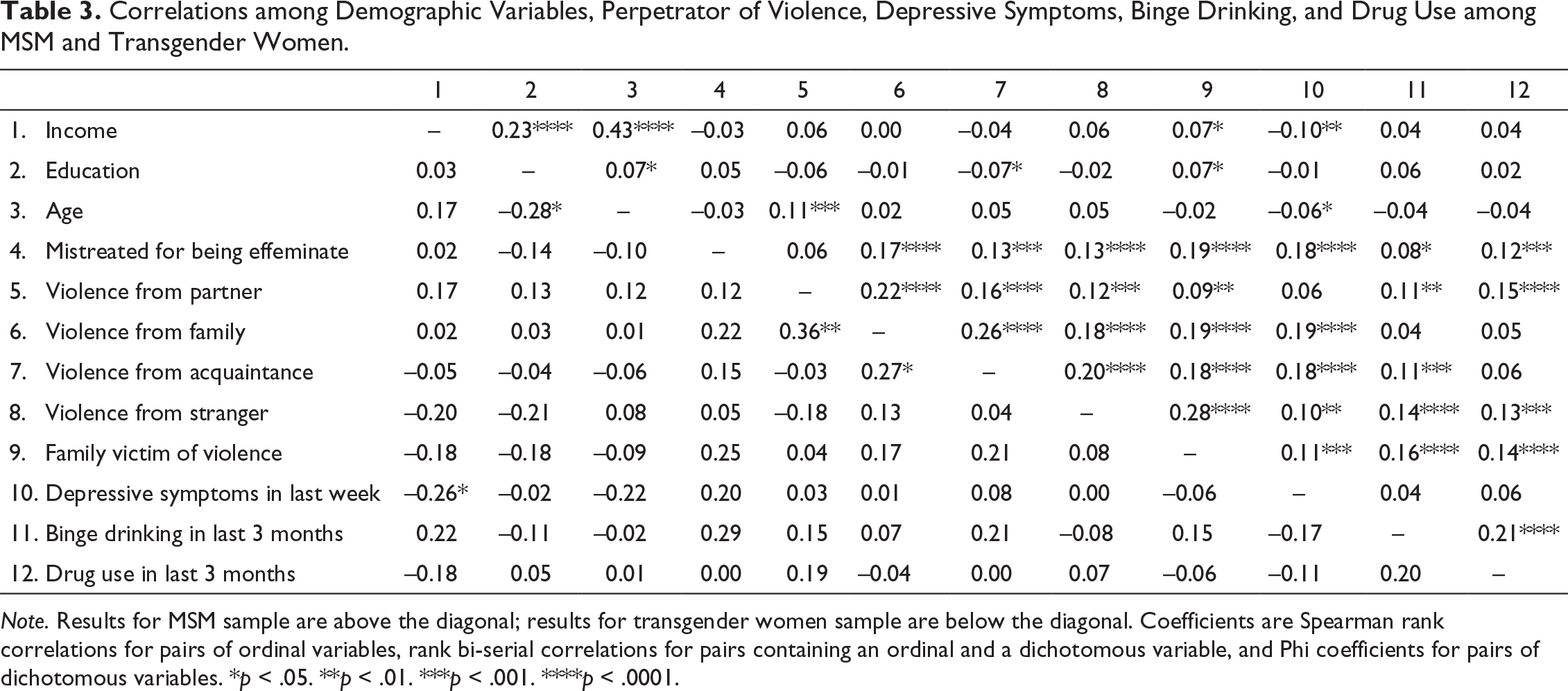
Note. Results for MSM sample are above the diagonal; results for transgender women sample are below the diagonal. Coefficients are Spearman rank correlations for pairs of ordinal variables, rank bi-serial correlations for pairs containing an ordinal and a dichotomous variable, and Phi coefficients for pairs of dichotomous variables. *p < .05. **p < .01. ***p < .001. ****p < .0001.
Associations among Violence and Mental Health Indicators
MSM sample.
Predictions of Depressive Symptoms in the Previous Week, Binge Drinking in the Previous Three Months, and Drug Use in the Previous Three Months among MSM (n = 942).
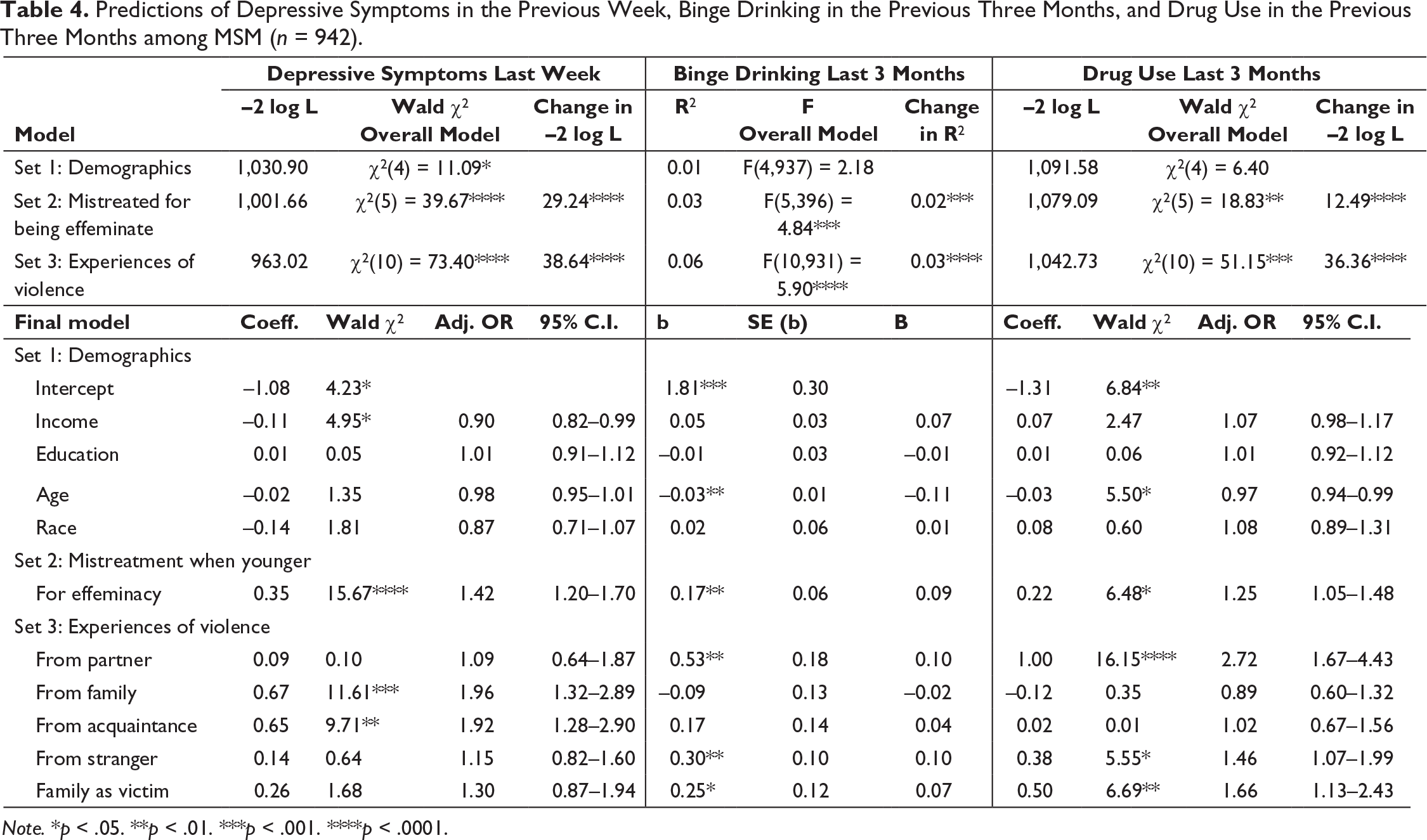
Notes: *p < .05; **p < .01; ***p < .001; ****p < .0001
Transgender women sample.
For the transgender women sample, the Wald chi-square test of the overall model was non-significant for all sets of the model for drug use (results available from author). For depressive symptoms, the Wald chi-square test of the overall model approached significance for set 1 (χ2 = 0.41; df = 4; p = .052) and was significant for set 2 (χ2 = 11.26; df = 5; p = .047); however, none of the individual parameters were significant for either set. For set 3, the test of the overall model was non-significant (χ2 = 16.21; df = 10; p = .094). For binge drinking, the test of the overall model was significant for set 1 (F3,54 = 2.86; p = .045), set 2 (F4,53 = 3.92; p = .01), and the final set (F9,48 = 2.29; p = .03), and the change in R2 was significant from Set 1 to Set 2 only (F1,53 = 6.15; p = .02). In the final model, only income was significantly associated with binge drinking (b = 0.33; SE(b) = 0.13; B = 0.33; p = .01).
Discussion
Violence is a serious public health problem that disproportionately impacts SGM groups throughout the world. The present research was one of the first investigations on the association of experiences of violence and recent mental health outcomes of MSM and transgender women in Bogotá, Colombia. The high prevalence of conflict-related violence in Colombia is well known (Human Rights Watch, 2019; US Department of State, 2018, 2019), and findings in this study demonstrate that MSM and transgender women in particular have been significantly affected. In Colombia, armed groups targeted MSM and transgender women during the internal conflict (El Tiempo, 2019; Zea et al., 2013) and continue to do so in the post-conflict (Colombia Diversa, 2020b; El Tiempo, 2019). Exploring the impact of violence on the mental health of gender and sexual minority populations is of public health significance, and this study contributes to the scant research on this topic (Barnett et al., 2019; Harper et al., 2004). Moreover, this study addresses issues of sexual orientation and gender identity diversity in a Latin American middle-income country.
High Prevalence of Violence among Transgender Women and MSM
There was a very high prevalence of experiences of violence in this sample. Transgender women were significantly more likely to experience any type of violence and severe beatings than MSM, but both groups commonly reported a high prevalence of severe beatings, stabbings, and rapes. Transgender women were significantly more likely than MSM to have experienced mistreatment for being feminine when younger. However, more than a third of the MSM were also mistreated for the same reason, reflecting that cisgender men also endure negative consequences for behavior outside the gender norms in Colombia. Widespread violence is also evident as the vast majority of participants reported that their families had also been victims of violence. The intersection of race, sexual orientation and gender identity was also evident in the prevalence of violence, which was higher for Mestizo and other races than for White participants. This reflects the racial stratification in Colombia. MSM and transgender women of color are more burdened by violence and it is possible that the authorities are less likely to protect them (Colombia Diversa, 2020b).
Findings presented here suggest that transgender women and MSM may be targets of violence from multiple perpetrators. Family members and acquaintances reportedly committed relatively high percentages of the total reported beatings, rapes, and torture. These findings could reflect stigmatization of SGM group members in Colombia, which may lead families and close friends to reject and victimize them because of their sexual orientation or gender identity. Experiencing these types of violence from strangers was also relatively common, but it is unclear whether this is due to heteronormative social norms and/or to the generalized violence that characterizes the country. In contrast, strangers were the overwhelming perpetrators of knife and gun attacks, which could suggest that many of these acts likely arose from the general atmosphere of violence created by internal conflict in the country and its aftermath as well as by the extreme socioeconomic inequality in Colombia (Flores, 2013).
Associations among Violence and Mental Health Indicators for MSM
The results from the present study indicate that the high levels of violence in Colombia are associated with negative mental health indicators for MSM. Experiences of violence among MSM in Bogotá were strongly related to depressive symptoms, binge drinking, and drug use, even after accounting for the impact of demographic factors and gender-based mistreatment when younger. This research extends to sexual minority populations findings from other research and corroborates the link between experiences of violence and negative mental health outcomes among the overall Colombian population (Cuartas Ricaurte et al., 2019; Harpham et al., 2005; Hessel et al., 2019; Londoño et al., 2012; Roberts & Browne, 2011; Santaella-Tenorio et al., 2018). Furthermore, experiences of mistreatment for being effeminate when younger were related to all three negative mental health indicators, suggesting that gender-based discrimination has a harmful impact on Colombian MSM.
The association between experiences of violence and mental health differed based on the perpetrator’s closeness to the participant. Violence enacted by family members and acquaintances was associated with depression, but not binge drinking or drug use. Violence committed by strangers was associated with binge drinking and substance use. The pattern of findings suggests that the degree to which MSM internalize experiences of violence via depression or externalize them through substance use, was related to whether the relationship in which the violence occurred was longstanding versus incidental. Previous studies in Peru and South Africa have found evidence of a stronger relationship between community-based violence and externalizing symptoms (du Plessis et al., 2015; Yearwood et al., 2017), and the results of this study extend these findings beyond US samples (Fowler et al, 2009; Sanchez et al., 2013) by providing support of this association among MSM. We also found that violence from intimate partners was associated with binge drinking and drug use, but not depression. It is possible that increased drug or alcohol use leads to increased risk of violence victimization from intimate partners. This finding did not fit the broader pattern that we observed in the other findings, and therefore, further research is needed to better understand this association.
The relationship between violence experienced by participants’ family and mental health outcomes was weaker than those of direct experiences of violence and was only associated with externalization in the form of binge drinking and substance abuse. This finding is consistent with studies on vicarious violence that report that individuals become desensitized to the emotional effects of the violence that surrounds them and distress related to such vicarious violence is more likely to manifest in externalizing symptoms rather than internalizing (Fowler et al., 2009; Garbarino et al., 1992). Although we measured only one form of vicarious violence—victimization experienced by a family member—our results fit the same pattern.
Limitations
The first limitation to this study is the cross-sectional nature of the data and that we did not assess the exact timeline during which participants experienced the violent acts vis-à-vis the mental health outcomes. Nevertheless, all the outcomes were recent (past three months or previous week); experiences of mistreatment for being effeminate were remote (when younger); and experiences of violence were assessed during the participant’s lifetime, and therefore were potentially more distal than the last week or the last three months. Thus, this study allows some inferences regarding the temporal sequence from experiences of violence to mental health outcomes. Given the overlap in the time periods assessed, it is possible that the causal relationships operate in a direction different than the one hypothesized (i.e., that depressive symptoms, alcohol use, and substance use increase risk for subsequent violence victimization).
Second, we did not assess whether participants attributed the violence they experienced to their sexual orientation or gender identity. For this reason, we cannot disaggregate violence related to the general climate from that related to the participants’ identity. However, victims of violence are not always aware of why they are targeted. A strength of the measure of violence used is that it assessed violence by type and perpetrator, thus providing a detailed picture of participants’ experiences of many different forms of violence.
The small number of transgender women who were available for analysis is a third limitation, but we considered it important to analyze their data despite the relatively small sample. Transgender women are a vulnerable population, yet they are often excluded from studies altogether or subsumed under MSM (Barnett et al., 2019; del Río-González et al., 2018; Harper et al., 2004). We opted to investigate their experiences separately so as not to contribute further to their marginalization and invisibility in the literature.
Fourth, the dataset is not recent, but the findings are relevant given the current context of Colombia in which violence continues to be prevalent and its association with mental health outcomes are likely still similar. Violence usually continues years after conflicts are over because of the breakdown of social norms and practices (Escobar, 2012; Ghobarah, 2003). For this reason, these findings continue to be relevant and fill a gap in the existing literature.
Conclusions
The present study is significant for its use of a sample of Colombian MSM and transgender women, a population at high risk for personal forms of violence due to their sexual orientation and gender identity as well as community violence due to the social disruption caused by the long history of armed conflict in the country. For MSM, we found that violence from strangers was associated with externalizing symptoms such as binge drinking and drug use, whereas violence from family and acquaintances was associated with an internalizing symptom, depression. We shed some light onto the experiences of transgender women as well—particularly the high prevalence of violent victimization among this population—but more robust investigations focused on transgender women and their specific experiences are necessary.
Further research is needed to investigate the associations among violence and mental health indicators for these populations. Specifically, more precise measures of the timing of violent experiences and longitudinal methods could further elucidate the complex relationships between experiences of violence and mental health problems. In addition, future studies should investigate the underlying mechanisms through which widespread violence contributes to internalization and externalization of mental health outcomes.
This study found evidence of a high prevalence of experiences of violence from various sources among MSM and transgender women in Colombia and that these experiences are associated with negative mental health indicators. These findings indicate that reducing the incidence of violent victimization for these populations in Colombia may alleviate some of their burden of psychological distress and that such interventions should target violence at multiple levels, including the community, acquaintances, family members, and partners. Furthermore, results suggest that there is an urgent need for more investigations into violence and its impact among gender and sexual minority groups in low- and middle-income countries.
Footnotes
Acknowledgments
The authors wish to thank the participants in this study, the Executive Director and the project staff at the Liga Colombiana de Lucha contra el SIDA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by Award Number R01HD057785 from the National Institute of Child Health and Human Development (NICHD). The content is solely the responsibility of the authors and does not necessarily represent the official views of NICHD or NIH. During the preparation of this manuscript, the authors also received support from the District of Columbia Developmental Center for AIDS Research (P30AI117970).