
Abstract
Some individuals show abnormal reactions to extreme fear and life-threatening situations, including tonic immobility (TI) and peri-traumatic dissociation (PTD). We aimed to investigate the association of TI and PTD with posttraumatic stress disorder (PTSD) in women who experienced sexual violence and the risk factors for PTD occurrence. We compared PTSD severity in 86 young adult women with PTSD after a sexual violence exposure grouped according to the presence of PTD and TI. In addition, we investigated whether PTD is associated with depression and anxiety symptoms and assessed potential risk factors for PTD reaction. We found a significant positive correlation between PTSD severity and PTD occurrence (R2 = .132; p = .001). PTD was also positively correlated with all clusters of PTSD symptoms except the Clinician-Administered PTSD Scale avoidance cluster (p = .058). PTD was strongly correlated with anxiety (R2 = .619; p < .001) and depressive symptoms (R2 = .547; p < .001). Multiple logistic regression showed that history of physical abuse (odds ratio [OR]: 1.386; p = .011) and sexual abuse (OR: 1.947; p = .004) during childhood were associated with PTD occurrence. Other risk factors for PTD were having less years of study (OR: 0.216; p = .016) and lower income (OR: 7.403; p = .028). TI measures were available for a subsample of 29 women. We found no association between TI and PTSD severity. PTD, but not TI, is significantly associated with more severe PTSD, depressive, and anxiety symptoms. Less-educated women with a history of childhood abuse and a lower income are at risk of PTD occurrence during a sexual violence episode.
Introduction
Extreme fear and life-threatening situations trigger flight or fight responses, which are mediated by the autonomic, sympathetic, and parasympathetic nervous systems. However, some individuals present maladaptive fear responses during or shortly after violent events. Tonic immobility (TI) and peri-traumatic dissociation (PTD) are two frequent phenomena that characterize individuals’ peri-traumatic responses (Bovin, Ratchford, et al., 2014).
TI is caused by extreme fear and perceived inescapability, and it is characterized by a state of involuntary motor inhibition, muscular rigidity, and analgesia (Marx et al., 2008; Volchan et al., 2017). TI is thought to occur when a life-threatening situation is extremely imminent, for example, physical contact with the aggressor, and fight or flight is not possible to avoid danger (de Kleine et al., 2018). Both TI and PTD developed through evolution as coping reactions to extreme conditions. TI is observed in a wide range of species and requires not only intense fear, but also physical restraint/entrapment by a predator (Abrams et al., 2009). It is an unlearned, involuntary behavioral response occurring when all volitional attempts to escape danger have failed. Unlike PTD, when recollection of events is mostly fragmented, studies suggest that there is no disruption in memory and consciousness in individuals experiencing TI and, although unresponsive to stimuli, the organism is in fact highly alert (Marx et al., 2008).
PTD involves a complex reaction to trauma, including depersonalization, derealization, and emotional blunting (Thompson-Hollands et al., 2017). Trauma survivors who experience PTD may show reduced awareness of the situation and may not be able to remember some aspects of the traumatic event (van der Velden & Wittmann, 2008). PTD is a cognitive response that has been studied only in humans. Its onset is understood as a detachment from reality to avoid overwhelming emotional and physical pain during the traumatic event (Bovin, Ratchford, et al., 2014).
PTD and TI are two different peri-traumatic experiences that may co-occur during the same traumatic event. However, as both involve different mechanisms regarding memory and alertness, it has been proposed that the two responses may differ in their underlying physiology and occur in different stages of the human defense cascade (Bovin, Ratchford, et al., 2014; Schauer & Elbert, 2010). Both TI and PTD have been identified as risk factors for the development of depression and anxiety symptoms (Bronner et al., 2009; Heidt et al., 2005; Möller et al., 2017; Rizvi et al., 2008), as well as significant predictors of the development and severity of posttraumatic stress disorder (PTSD) (Aho et al., 2017; Bovin, Ratchford, et al., 2014; De Soir et al., 2015; Gandubert et al., 2016; Peltonen et al., 2017; Werner & Griffin, 2012).
PTSD is a psychiatric disorder triggered by a traumatic event and is characterized by intrusive memories and thoughts about the event, avoidance of trauma-related reminders, alterations in mood and cognitions, and hyperarousal (Friedman et al., 2011). Lifetime prevalence of PTSD is estimated to affect 4% to 12% of individuals (Kessler et al., 1995; Ribeiro et al., 2013) and clinical studies suggest that nearly 40% of patients develop a chronic course of the disorder (Santiago et al., 2013). Chronic PTSD is associated with early onset of age-related diseases (Miller et al., 2017) and comorbidity with other psychiatric disorders (Walter et al., 2018).
Women develop PTSD at higher rates compared to men in a female-to-male ratio of approximately 2:1 (Olff et al., 2007). Women also exhibit higher rates of persistent PTSD symptoms (Breslau, 2001) and comorbid depression and anxiety compared to men (Olff, 2017). One possible explanation for these observed differences in the development and course of PTSD is that women are exposed to more high-impact trauma than men, and at a younger age (e.g., sexual trauma; Olff, 2017). Previous research estimated that approximately 45% to 75% of women develop PTSD following sexual assault, which suggests that this particular traumatic event is a significant predictor of PTSD (Dworkin et al., 2021; Luz et al., 2016).
Research findings suggest that women experience higher levels of TI and PTD during sexual assault compared to other traumatic events (Christiansen & Hansen, 2015; Gbahabo & Duma, 2021; Kalaf et al., 2015). PTD is thought to influence the development and persistence of PTSD by preventing the initial processing of the traumatic event and disrupting elaboration during memory encoding (Bedard-Gilligan & Zoellner, 2012). Thus, the fragmented memories implicated in PTD may result in poor recovery from the high peritraumatic emotions (van der Kolk & Fisler, 1995). However, the evidence for the strength of PTD as a predictor of development and severity of PTSD is mixed. One meta-analysis found PTD to be the most significant peri-traumatic risk factor for PTSD status and symptoms compared to six other predictors (Ozer et al., 2003). This is supported by another meta-analysis, particularly among survivors of childhood abuse compared to other types of traumatic events (Lensvelt-Mulders et al., 2008). Another meta-analysis found that PTD is a moderate risk factor for PTSD independent of sex or type of trauma (Breh & Seidler, 2007) and one critical literature review concluded that PTD is a modest predictor for PTSD (Bryant, 2007). Moreover, a meta-analysis of prospective studies, including survivors of accidents, natural disasters, and life-threatening illnesses, found a weak association (van der Velden & Wittmann, 2008). Taken together, these studies suggest that PTD is a significant predictor of PTSD, though with some variation in the strength.
Given the variability in findings related to PTD and PTSD, presuming a linear relationship between the traumatic event, PTD, and PTSD may be overly simplistic, and it may be the case that PTD is often associated with PTSD due to its association with other risk factors for PTSD, such as childhood trauma (Bryant, 2007). For example, research has connected childhood trauma to experiences of dissociation (Banyard et al., 2001), underscoring the importance of assessing early trauma to understand PTD and subsequent PTSD. However, the mechanisms through which childhood trauma, PTD, and PTSD are connected are unclear. One literature review suggested that childhood trauma impairs the ability to understand and regulate emotions in adulthood (Dvir et al., 2014). Emotional dysregulations (e.g., ineffective strategies to deal with emotions in the context of distress, nonacceptance of negative emotional responses), in turn, may influence PTSD through PTD due to the individual’s emotional inability to access adaptive strategies (Jones et al., 2018).
Further risk factors implicated in PTSD are socioeconomic status (SES), increased alcohol use, and younger age at the time of the traumatic event (Olff et al., 2007; Tang et al., 2017). However, there is very little evidence on how they may influence PTSD through PTD. Stressful situations related to SES may play a role in eliciting dissociation (Gušić et al., 2016), although studies that specifically investigated its association with PTD found no association (Briere et al., 2005; Lewis et al., 2014). Increased alcohol use and younger age have been reported among individuals who have experienced PTD, suggesting that these factors may be associated with how individuals process information related to the traumatic event (Grieger et al., 2003; Marmar et al., 1996). The lack of consensus as to how certain risk factors for PTSD may also be risk factors for PTD may indicate that other relevant factors may exist to help clarify the relationship between PTD and PTSD.
As for TI, studies tend to report a significant impact on PTSD symptom severity (Abrams et al., 2009; de Kleine et al., 2018; Magalhaes et al., 2021; Maia et al., 2015; Portugal et al., 2012) and a poorer recovery from PTSD symptoms (Fiszman et al., 2005; Hagenaars & Hagenaars, 2020; Lima et al., 2010). TI is more prevalent in women (Kalaf et al., 2017) and may exacerbate PTSD symptoms due to the preserved awareness during the trauma and subsequent guilt for not reacting (Bovin, Dodson, et al., 2014). Although PTD has been extensively researched, TI remains largely understudied in psychopathology literature and only recently has become a more prominent topic of study (Bovin, Ratchford, et al., 2014; Kozlowska et al., 2015). The mixed literature on PTD and PTSD and the lack of evidence to support TI as a predictor for PTSD severity highlight the need for more studies to investigate how these peri-traumatic experiences affect PTSD.
The present study aimed to help clarify this relationship by evaluating the association of TI and PTD with PTSD severity in women who experienced a recent sexual assault within the previous 6 months. Furthermore, we aimed to evaluate the association between PTD and depressive and anxiety symptoms, as a secondary objective. Studies to date focus mainly on PTD as a risk factor for PTSD, but limited research investigates whether risk factors for PTSD are also risk factors for PTD. Thus, we also aimed to identify the potential risk factors (e.g., childhood trauma and low SES) for more severe PTD reactions in our sample.
We made the following hypotheses: (1) women with higher PTD scores on the Peritraumatic Dissociative Experiences Questionnaire, Self-Report Version (PDEQ-SRV) develop more severe PTSD, and have more severe symptoms of depression and anxiety; (2) women who present TI during the sexual assault, as measured using the Tonic Immobility Scale (TIS), develop more severe PTSD; and (3) risk factors that often mediate poorer mental health outcomes such as childhood abuse/negligence, younger age, lower SES, and substance/alcohol use are associated with more severe PTD reactions.
Methods
Study Design and Setting
This study recruited participants between 2016 and 2019 as part of a larger study on PTSD and neuroprogression following sexual assault. The study took place at the Federal University of São Paulo (UNIFESP). The main project on PTSD and neuroprogression included the following procedures: (a) screening interview, (b) laboratory analyses to assess neuroprogression, followed by (c) a clinical trial for PTSD treatment. The protocol article for this research was published elsewhere (Coimbra et al., 2020). For the present cross-sectional study, we used data provided by the patients in the screening interview.
All women were referred from Hospital Pérola Byington (HPB), which is a women’s health care center in São Paulo (Brazil) that provides specialized gynecological care following sexual assault. HPB staff initially screened patients for sexual assault within the previous 6 months and PTSD symptom development using the National Stressful Events Survey PTSD Short Scale. HPB informed our team of potential participants.
Participants
We contacted patients by telephone to invite them to participate in the study and, if so, schedule an appointment for detailed screening at UNIFESP. All patients were evaluated by a psychiatrist and clinical psychologist who administered the informed consent form approved by the UNIFESP Committee Board and explained all procedures of the study on PTSD and neuroprogression. We included individuals who provided informed consent and were considered eligible according to the inclusion and exclusion criteria. Patients showing severe suicidal risk were excluded and referred to immediate standard psychiatric treatment. Patients’ transportation expenses were covered, but no other financial compensation was offered.
The inclusion criteria were as follows: (1) aged 18 to 45 years; (2) having experienced sexual assault within the previous 6 months regardless of the history of childhood sexual abuse; (3) current PTSD diagnosis based on the Mini-International Neuropsychiatric Interview (MINI); (4) a Clinician-Administered PTSD Scale for the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (CAPS-5) score >26; and (5) having signed an informed consent form approved by the Ethics Review Board.
The exclusion criteria were as follows: (1) ongoing psychiatric or psychotherapeutic treatment; (2) being at severe suicidal risk as determined through a clinical interview with a trained researcher; (3) pregnancy; (4) chronic corticosteroid use; (5) having an unstable medical condition or neurologic disease; (6) the researcher considering the participant as unable to understand the informed consent form or research objectives; (7) having substance dependence in remission for <6 months; and (8) having bipolar disorder or schizophrenia.
Procedures and Assessments
All patients were evaluated by a psychiatrist and clinical psychologist who administered the informed consent form approved by the UNIFESP Committee Board and explained all procedures of the study on PTSD and neuroprogression. We included individuals who provided informed consent and were considered eligible according to the inclusion and exclusion criteria. Patients showing severe suicidal risk were excluded and referred to immediate standard psychiatric treatment. Patients’ transportation expenses were covered, but no other financial compensation was offered.
During the screening interview, patients were assessed using the MINI to determine a diagnosis of PTSD, and the CAPS-5 to confirm the diagnosis of PTSD and determine PTSD symptom severity. Patients also completed the Beck Depression Inventory (BDI); Beck Anxiety Inventory (BAI); Childhood Trauma Questionnaire (CTQ); TIS; and PDEQ-SRV. Of note, the MINI was also used to screen out patients with comorbidities that were exclusion criteria for this study. All instruments used to assess patients have been translated and validated to Brazilian Portuguese. As the TIS was included in the screening interview after the study had begun, only a subsample of patients (n = 29) was evaluated for TI. All data were stored in RedCap, which is a secure web-based application that is widely used in research for building and managing online surveys and databases.
Measures
Full sociodemographic inventory and history of the sexual assault episode: We developed a detailed sociodemographic inventory to collect participants’ relevant sociodemographic characteristics, such as age, race, civil status, education, and income. Specifically, we collected the following data regarding the sexual violence episode: (a) assault type (rape, attempted rape, or drug-facilitated rape); (b) whether the perpetrator(s) was (were) a known person (family member, friend, or acquaintance) or a stranger; (c) location (home, public place, working place, etc.), date, and time of the assault; (d) whether the victim had notified the police authorities, and if so, whether there was an ongoing investigation; and (e) details regarding the assault. Additionally, we monitored whether the participants adhered to the gynecological treatment offered at the HPB.
CAPS for DSM-5: This scale is the gold standard for assessing the PTSD diagnostic status and symptom severity. It is a 30-item questionnaire administered by a clinician through a structured interview to evaluate the PTSD symptom frequency and intensity, as well as trauma-related variables, using a frequency/severity scale ranging from 0 (never/not severe at all) to 4 (most of the time/severe). The symptom-related questions are divided into four clusters: re-experiencing (cluster B); avoidance (cluster C); negative alterations in cognition and mood (cluster D); hyperarousal (cluster E). Each cluster is presented with a score, and the sum of all cluster scores gives the CAPS-5 total score. A large-scale psychometric study confirmed the validity and reliability of the CAPS-5 as a measure of PTSD symptoms (Oliveira-Watanabe et al., 2021; Weathers et al., 2018).
MINI: MINI is a short standardized diagnostic interview (15–30 minutes), compatible with the DSM-III-R/IV and ICD-10 criteria, intended for the use in clinical practice and research in primary care and psychiatry settings. MINI presents psychometric qualities similar to those of other more complex standardized diagnostic interviews, allowing a reduction of 50% or more in the time of evaluation (Amorim, 2000).
BDI: The BDI has been extensively applied as a self-report measure of depression. It consists of 21 items containing four statements that reflect the increasing severity of a given symptom of depression. It is used to assess depressive symptoms in clinical settings (Gomes-Oliveira et al., 2012). The sum of all individual item scores corresponds to the total score. A total score of 10 to 18 is interpreted as mild depressive symptoms, 19 to 29 as moderate, and 30 to 63 as severe (Beck & Steer, 1984).
BAI: The BAI a self-administered 21-item questionnaire assessing the intensity of anxiety symptoms. Items consist of a brief statement describing the symptoms of anxiety rated on a 4-point scale (Cunha, 2001). The values for each item are summed, yielding an overall or total score for all 21 symptoms that can range between 0 and 63 points. A total score of 0 to 7 is interpreted as a minimal level of anxiety, 8 to 15 as mild, 16 to 25 as moderate, and 26 to 63 as severe (Beck et al., 1988).
CTQ: The CTQ is internationally accepted as a key tool for the assessment of childhood abuse and neglect experiences. It assesses physical, emotional, and sexual abuses, as well as physical and emotional neglect during childhood across 28 items using a 5-point Likert scale (Grassi-Oliveira et al., 2006, 2014).
PDEQ: This is a self-reported 10-item measure of dissociative symptoms experienced during or immediately after a traumatic event using a 5-point Likert scale ranging from 1 (not at all true) to 5 (extremely true) (Fiszman et al., 2005). The total PDEQ score ranges from 10 to 50 points, with a score >15 being the cutoff point. This questionnaire is comprised of questions regarding the loss of awareness of events or “blank mind”; feeling of acting on automatic pilot; altered time perception; sensation of unreality; feeling of being in a dream or movie; feeling of floating above the scene; feeling detached from the body or a distorted body perception; inability to distinguish events that occurred to the individual from those that occurred to others; inability to notice facts that happened during the event, which would usually be noticed; difficulties in understanding the current situation; and disorientation. Four studies have confirmed that the PDEQ has high reliability and validity (convergent, discriminant, and predictive) (Marmar et al., 1994, 1996; Tichenor et al., 1996; Weiss et al., 1995). The PDEQ scores can correctly predict PTSD symptoms independent of the severity of trauma exposure and dissociation (Marmar et al., 2004).
TIS: This is a self-report instrument designed for evaluating TI presence and severity in sexually assaulted women (Heidt et al., 2005). We used four items extracted from the Tonic Immobility Scale Child Abuse Form to avoid overlapping with the PDEQ scale (Lima et al., 2010). Rocha-Rego et al. (2009) conducted an exploratory factorial analysis using 506 victims of violence and extracted a solution with three factors from the aforementioned four factors, which were responsible for 48% of the variance. Moreover, this scale was found to have satisfactory internal consistency (Cronbach’s α = .83; Rocha-Rego et al., 2009). The adapted four “motor” items were as follows: (i) question: rate the degree to which you froze or felt paralyzed during the event, answer: 0 = not at all frozen or paralyzed/6 = completely frozen or paralyzed; (ii) question: rate the degree to which you were unable to move even though not restrained during the event, answer: 0 = could move freely/6 = could not move at all; (iii) question: rate the degree to which you were unable to call out or scream during the event even though you were willing to, answer: 0 = felt able to scream/6 = wanted to scream but felt unable to; and (iv) question: rate the extent to which you felt unable to escape during the event even though you were willing to, answer: 0 = felt able to escape/6 = wanted to escape but remain fixed. Immobility report scores were calculated by adding the answer ratings for the four questions (minimum = 0; maximum = 24). The minimum cutoff score of 9 criteria proposed by Heidt et al. (2005) is 9 for inclusion, based on a TI criterion.
Alcohol Smoking and Substance Involvement Screening Test: This structured questionnaire contains eight questions about using nine psychoactive substances (tobacco, alcohol, marijuana, cocaine, stimulants, sedatives, inhalants, hallucinogens, and opiates). The questions address the frequency of use, in life and the last 3 months, problems related to use, concern about the use by people close to the user, impairment in the execution of routine tasks, unsuccessful attempts to cease or reduce use, feeling of compulsion, and use by the injectable route. Each answer corresponds to a score ranging from 0 to 4, and the total sum can range from 0 to 20. The score ranges from 0 to 3 indicates occasional use, from 4 to 15 as abuse, and ≥16 as suggestive of dependence (Henrique et al., 2004).
Statistical Analysis
Statistical analyses were performed using SPSS software (IBM Corp. Released 2020. IBM SPSS Statistics for Macintosh, version 27.0. Armonk, NY, USA) and the R software. For sample description using the relative and absolute frequencies, we assumed a 5% level of significance. Continuous variables were presented as the average and standard while categorical variables were presented as percentages. Between-group comparisons were performed using Pearson’s t-test; moreover, the correlation between the scale scores was examined using Spearman’s test. Simple logistic regression was used to measure the association of interest, which was reported as the odds ratio (OR) with a 95% confidence interval (CI). Linear and multiple regression analyses were used to evaluate the CAPS-5, BAI, BDI, and PDEQ scores.
Results
A total of 149 women were contacted and invited to participate in this study, of which 34 refused. In all, 100 patients came for the screening interview, of which 86 were eligible for the present study. Table 1 presents the sociodemographic characteristics of participants with and without reported PTD (defined as a PDEQ score of 15 or higher). Table 2 presents clinical scale scores and CTQ scores, among those with and without reported TI. Across the entire sample, participants’ scores indicated severe PTSD (37.8 ± 3.7) with comorbid severe depressive (28.7 ± 1.3) and anxious symptoms (24.5 ± 1.5). Moreover, the average PDEQ score (20.3 ± 1.5) of all the included patients was indicative of severe PTD. As the TIS was added partway through data collection, a subsample of 29 patients from the patient group was evaluated. Using the TIS cutoff score to assess the presence of TI, 21 patients (72.4%) had TI during the traumatic event.
Sociodemographic Characteristics.
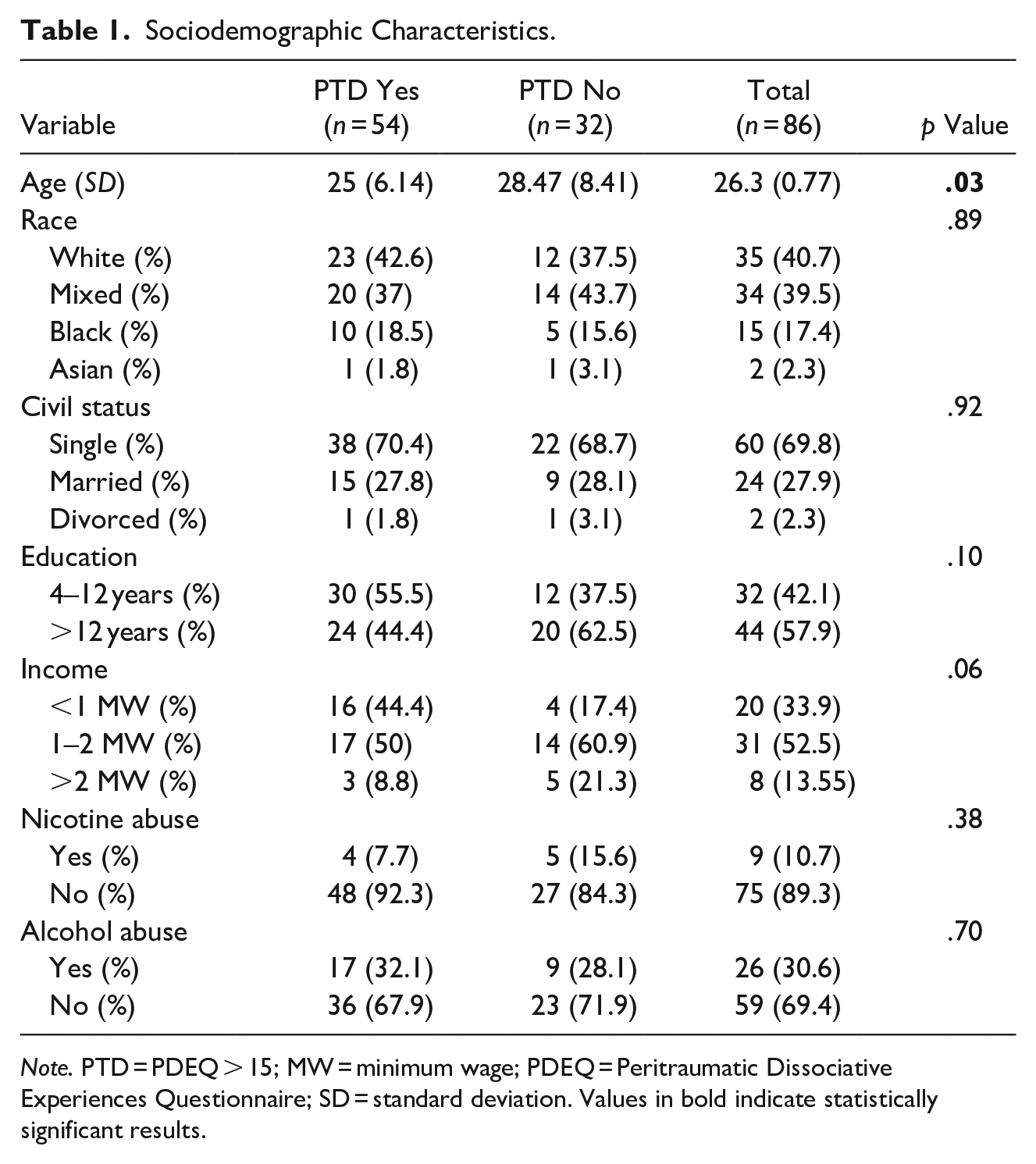
Note. PTD = PDEQ > 15; MW = minimum wage; PDEQ = Peritraumatic Dissociative Experiences Questionnaire; SD = standard deviation. Values in bold indicate statistically significant results.
Average Scores of Clinical Severity Scales.
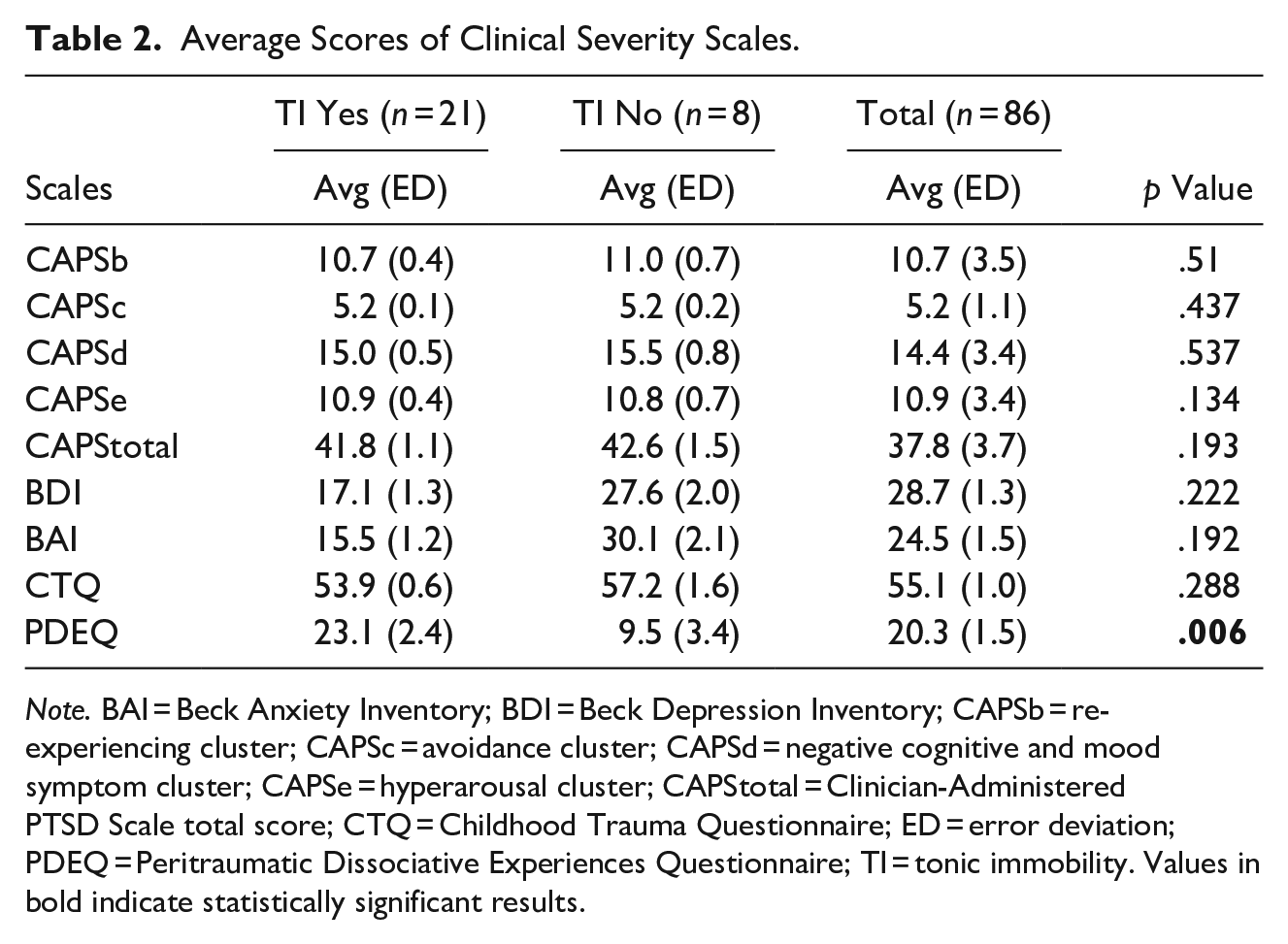
Note. BAI = Beck Anxiety Inventory; BDI = Beck Depression Inventory; CAPSb = re-experiencing cluster; CAPSc = avoidance cluster; CAPSd = negative cognitive and mood symptom cluster; CAPSe = hyperarousal cluster; CAPStotal = Clinician-Administered PTSD Scale total score; CTQ = Childhood Trauma Questionnaire; ED = error deviation; PDEQ = Peritraumatic Dissociative Experiences Questionnaire; TI = tonic immobility. Values in bold indicate statistically significant results.
Regarding our hypothesis that PTD reaction predicts severe symptoms in women, we found a significant but weak correlation between the PDEQ and the CAPS-5 scores, using a regression analysis model with coefficient of determination (R2 = .132; p = .001), and a strong correlation with depressive and anxiety symptoms (R2 = .547; p < .001; R2 = .619; p < .001), respectively. Secondary analysis with specific symptom clusters revealed a significant correlation of PDEQ scores with re-experiencing symptoms (cluster B; R2 = .268; p = .018), negative cognitive and mood symptom (cluster D; R2 = .301; p = .008), and hyperarousal (cluster E; R2 = .306; p = .006), but not with avoidance (cluster C; R2 = .215; p = .058). These results support our hypothesis that women who experienced PTD present more severe PTSD, depression, and anxiety symptoms.
Our hypothesis that occurrence of TI leads to more severe PTSD symptom was not confirmed, as there was no correlation between the TIS and total CAPS-5 scores, either when considered continuous (total TIS score), or categorical (TI presence during the rape event) variables. Our findings indicated no correlation between TI and PTSD severity.
Table 3 presents risk factors for PTD during the traumatic event. In the simple logistic regression, all CTQ domains (except physical negligence) had a significant positive correlation with total PDEQ score. Also, being younger, having less years of study, and lower income increased PDEQ scores. In multiple logistic regression model, CTQ domains of physical abuse (OR: 1.386, p = .011) and sexual abuse (OR: 1.947, p = .004) remained significant with PDEQ scores, meaning that patients with a history of childhood abuse showed higher PDEQ scores and more severe PTSD symptoms. Being younger was no longer significant with PDEQ scores in the multiple regression model, but having less years of study (OR: 0.216, p = .016) and lower income (OR: 7.403, p = .028) remained associated with higher PDEQ scores. There was no correlation of PDEQ with declared race, nicotine abuse, or alcohol abuse.
Risk Factors Involved in the Occurrence of PTD Reaction During Sexual Assault.
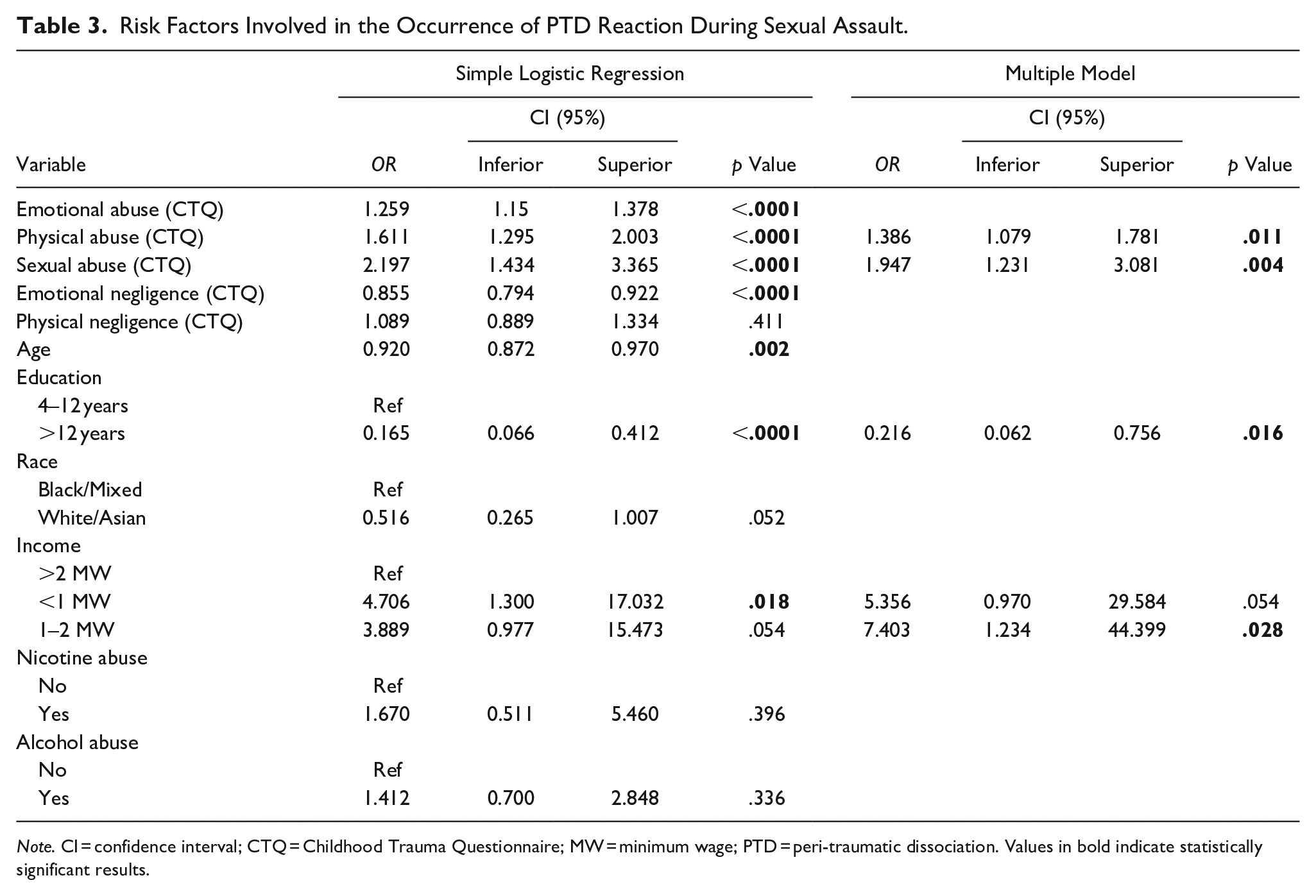
Note. CI = confidence interval; CTQ = Childhood Trauma Questionnaire; MW = minimum wage; PTD = peri-traumatic dissociation. Values in bold indicate statistically significant results.
Discussion
In the present study, we aimed to evaluate PTD and TI reactions in association with PTSD severity in a sample of women who had experienced a recent sexual assault. Results show that women showing PTD symptoms, as evaluated by the PDEQ, presented with more severe PTSD symptoms as indicated by the CAPS-5. This is consistent with previous research reporting the effects of PTD on PTSD severity (Duagani Masika et al., 2019; Lensvelt-Mulders et al., 2008). PTD was correlated with the severity of symptoms in the re-experience (CAPSb), negative mood and cognition (CAPSd), and hyperarousal cluster (CAPSe); however, it was not associated with the avoidance symptom cluster (CAPSc). Although research exists on the associations between PTD and PTSD in general, there is a lack of research investigating how peri-traumatic experiences predict specific PTSD symptom clusters (Dewey et al., 2014). Our findings indicate that PTD is potentially a clinically feasible outcome predictor and a possible indicator of the mechanism underlying specific PTSD symptom clusters, which supports previous findings that PTD may contribute to the formation of intrusive memories, higher dysphoria, and hyperarousal symptoms (Danböck et al., 2021; Daniels et al., 2012; Kumpula et al., 2011; Massazza et al., 2021). This demonstrates the importance of evaluating PTD in victims of sexual abuse given their high risk of PTSD development.
Although PTD disconnects the individual from reality, reducing consciousness and awareness, and acts initially as a protective mechanism to cope with extreme fear during the traumatic event, the mechanism through which PTD impacts PTSD could be related to the interference in decoding, processing, and integrating the traumatic memories. The inability to access the entirety of the fragmented memories may impair psychological functioning and impede opportunities to successfully process the traumatic event, increasing the subsequent risk of PTSD development and severity (Bovin, Ratchford, et al., 2014; Brooks et al., 2009; Koopman et al., 1995; Van der Kolk & Van der Hart, 2006). Additionally, as PTD has been suggested to be a maladaptive behavior used to disrupt overwhelming emotional experiences during trauma (Fikretoglu et al., 2006), it may signal specific emotion regulation deficits to deal with enduring trauma-related emotions, with detrimental effects on mental health (Jones et al., 2018).
Furthermore, we found an association between PTD and childhood trauma. This is consistent with previous studies suggesting that childhood trauma may increase dissociation when re-experiencing traumatic situations in adulthood (Banyard et al., 2001; Thomas et al., 2018). A history of prior trauma may elevate the appraisal of threat and loss of control, and exacerbate symptoms of arousal in response to new trauma, all of which have been linked to dissociative tendencies (Cardeña et al., 2021; McDonald et al., 2013). Thus, it is plausible that revictimization may lead to a stronger propensity to distance oneself from the negative emotions and cognitions elicited when re-experiencing trauma, resulting in the higher observed scores on the PDEQ and the CTQ in our sample.
Our findings on SES (less years of study and lower income) and PTD are inconsistent with reports from previous studies (Briere et al., 2005; Lewis et al., 2014). The observed positive correlation may relate to the higher exposure that low SES groups have to traumatic events in Brazil. Low SES and exposure to urban violence have been linked to psychopathology in Brazil (Fidalgo et al., 2018; Ribeiro et al., 2013). It may be the case that low SES and prior trauma are two interrelated factors that influence peritraumatic responses, which may, in part, account for the mixed findings in the literature regarding PTD and PTSD. Unfortunately, we did not assess a complete history of traumatic events other than childhood trauma, which limits our interpretations. However, our findings suggest that PTD may be one pathway throughout which low SES and previous trauma could impact PTSD severity and outcome.
In our study, we found that PTD was positively correlated with the severity of depressive and anxious symptoms, as measured by the BDI and BAI, respectively, which is consistent with previous findings (Azoulay et al., 2020; McCanlies et al., 2017). Comorbidity of PTSD with other psychiatric disorders such as major depression and anxiety disorder is the norm rather than the exception (Frewen et al., 2013; O’Donnell et al., 2004), varying from 79% to 85% of individuals (Geng et al., 2019; Kessler et al., 1995). In the case of PTSD following sexual assault in women, co-occurrence of PTSD and depression can be over 90% (D’Elia et al., 2021). The symptom overlap between PTSD, depression, and anxiety may underlie shared vulnerabilities to the development of mental disorders in the aftermath of trauma (Flory & Yehuda, 2015) and increase the psychological burden for patients (McMillan et al., 2017; Nichter et al., 2019; Panagioti et al., 2012). Our findings that PTD leads to more severe PTSD, depression, and anxiety symptoms may be an indication for clinicians to assess for and attend to experiences of PTD among patients.
Our initial hypotheses were partially refuted since there was no association between TI occurrence and more severe PTSD. This contrasts with the current body of evidence implicating TI in the severity of PTSD (de Kleine et al., 2018; Hagenaars, 2006; Hagenaars & Hagenaars, 2020; Lima et al., 2010; Möller et al., 2017), though it is consistent with two previous studies (Abrams et al., 2012; Van Buren & Weierich, 2015). It is necessary to highlight that our study has a small sample of participants who completed the TIS, which likely impacted our findings. Only recently has TI emerged in research as an important peri-traumatic response in the progression of PTSD, warranting further studies to continue to investigate its mechanisms (Bovin, Ratchford, et al., 2014). However, despite the lack of association between TI and PTSD severity, TI was highly prevalent in our sample, as 72.4% of participants reported a significant TI reaction, according to the TIS cutoff score. This corroborates the evidence that TI is a common reaction among sexual assault survivors (Kalaf et al., 2017; Marx et al., 2008; TeBockhorst et al., 2015). Sexual assault often involves high levels of fear and physical restraint, similar to the circumstances that induce TI in animals when confronted with the inescapabilty threat of an imminent attack (Fusé et al., 2007; Suarez & Gallup, 1979). Although maladaptive, as TI may be a frightening response itself, the involuntary paralysis observed in TI may protect women from additional violence (Marx et al., 2008).
There is a need for further research on PTD and TI; moreover, professionals dealing with victims of sexual abuse should perform a systematic clinical evaluation of PTD and TI presence as a pathological reaction to extreme violence. PTD and TI are often erroneously interpreted as the victim giving consent since they do not offer a fight. These misinterpretations could have an intense negative impact on the victims, which increases their helplessness, distrust, and guilt (Bovin, Dodson, et al., 2014; Dorahy et al., 2017; Schiewe, 2019).
Our study has limitations that must be addressed. First, we assessed PTD in a sample of 86 women and TI in a reduced subsample of 29 women. The small sample size may have affected our findings. Second, we based our analysis on a cross-sectional design, having assessed PTD and TI between 1 and 6 months of the exposure to the sexual assault. Previous evidence highlights that assessing PTD and TI retrospectively may be biased, as it is difficult for patients with PTSD to provide an accurate recount of past emotional states, and that peri-traumatic experiences should be investigated in the immediate aftermath of trauma (Candel & Merckelbach, 2004; van der Hart et al., 2008).
This study has clinical implications for female victims of sexual abuse. Specifically, it suggests that the initial evaluation should involve active assessment for PTD symptoms and that PTD is possibly influenced by childhood trauma and SES. Also, we found that PTD relates differently to PTSD symptom clusters, suggesting the value of PTD assessment as a predictor and indicator of specific PTSD symptom clusters. Moreover, given that PTD symptoms may be indicators of severe PTSD development, our findings highlight the importance for more research on early risk detection of PTSD severity among women survivors of recent interpersonal violence. Identifying such vulnerabilities may contribute to earlier and more specific interventions to decrease the psychological and physical burden of sexual trauma.
Footnotes
Acknowledgements
The authors thank the social workers, psychologists, and gynecologists of Hospital Pérola Byington for their enormous contribution to the development of this research. We gratefully acknowledge UNIFESP team members Cecilia Proença, Cecilia Zylberstajn, Bruna Nicoletta, Thauana Oliveira-Watanabe, Ana Teresa D’Elia, Nina Valente, Luciana Porto, Thays Mello, Euthymia Prado, Rosaly Braga, Samara Hipolito Nitzsche, Flavia Strumpf, Roberta Constantino, Camila Matsuzaka, Nathalia Balloni, Fernanda Gomes, Tania Camargo, Adriana Mozzambani, Paula Maria Serafim, Magda Bignotto, Mary Yeh, Ana Carolina Milani, Vinicius Calsavara, and Fernando Rodrigues Grecco. We also thank Dr. Rachel E. Williamson of the University of Montana, Missoula, U.S., for revising the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was sponsored by the FAPESP grant number 2014/12559-5. Additional grant support was provided by CNPq 303389/2016-8. This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001. The funders had no role in the study design or the decision to publish this article.