
Abstract
Intimate partner violence (IPV) is common in men who have sex with men (MSM). MSM also face increased risk of human immunodeficiency virus infection. However, it is not known whether IPV experience of MSM in China would affect their attitudes toward pre-exposure prophylaxis (PrEP) use. A cross-sectional study was conducted to explore the associations between different types of IPV and willingness to use PrEP in a sample of 608 MSM from November 2018 to May 2019 in Chengdu, China. Univariate and multivariate logistic regression analyses were used to explore the associations between different types of IPV and willingness to use PrEP. The average age of the participants was 31.8 ± 12.3 years, 48.9% of them were aware of PrEP before this study, and only 7.2% were aware of long-acting injectable PrEP (LAI-PrEP). The overall willingness to use any type of PrEP in the next 6 months was 82.2%. Approximately one third of the participants (n = 198) had experienced at least one type of IPV. We found that experience of sexual perpetration was negatively associated with the willingness to use on-demand PrEP (adjusted odds ratio [ORa] = 0.33, 95% CI = 0.16–0.67) and the overall willingness to use any type of PrEP (ORa = 0.31, 95% CI = 0.15–0.64). The willingness to use LAI-PrEP also had negative associations with any type of monitoring IPV (ORa = 0.58, 95% CI = 0.38–0.91), controlling victimization (ORa = 0.41, 95% CI = 0.21–0.82), and emotional victimization (ORa = 0.58, 95% CI = 0.35–0.97). The findings of this study demonstrate that IPV experiences are negatively associated with willingness to use PrEP among MSM, suggesting that PrEP promotion programs should consider IPV screening and develop explicit intervention strategies for both perpetrators and victims.
Keywords
Introduction
Intimate partner violence (IPV) includes physical violence, sexual violence, stalking, and psychological aggression by a current or former intimate partner (CDC, 2020). Globally, among men who have sex with men (MSM), the lifetime prevalence of victimization ranges from 32 to 82% (with a pooled prevalence of 48%) (Buller et al., 2014) and the lifetime prevalence of perpetration ranges from 16.3 to 35.9%, respectively, which were about 2 times higher than among heterosexual couples (Bacchus et al., 2017; Blosnich et al., 2009; Messinger, 2011; Tjaden et al., 1999; Welles et al., 2011). In China, the reported prevalence of IPV is also higher among MSM than the general population. In Shenyang, in the northeast of China, the prevalence of any type of IPV victimization in the past 3 months among MSM is 18.7% (Wang et al., 2018a). In Shanghai, in the east of China, the lifetime prevalence of any type of IPV victimization is 24.3% (Liu et al., 2018), and in Chengdu, in the southwest of China, the lifetime prevalence of any type of IPV victimization and perpetration is 32.7 and 32.5%, respectively (Wei et al., 2020b). IPV victimization is associated with substance use, depressive symptoms, unprotected anal sex, and human immunodeficiency virus (HIV) positivity, and IPV perpetration is associated with substance abuse (Buller et al., 2014).
Pre-exposure prophylaxis (PrEP) is a medicine taken to reduce the risk of HIV infection (Grant et al., 2010; Thigpen et al., 2012). In this approach, HIV-negative individuals take antiretroviral drugs (tenofovir disoproxil fumarate with emtricitabine [TDF/FTC]) before HIV exposure. PrEP, with a high level of adherence, is recommended for persons at high risk of HIV infection, such as the MSM population (Günthard et al., 2016). There are three types of PrEP: daily oral PrEP, on-demand PrEP, and long-acting injectable PrEP (LAI-PrEP). On-demand PrEP, or sexual activity-dependent PrEP with TDF/FTC, refers to taking two pills of TDF/FTC 2–24 h before risky sexual behavior and then taking a third and fourth pill every 24 h after taking the first pill. Studies have reported that on-demand PrEP reduces the risk of a new HIV infection by 86% (Molina et al., 2015). However, the effectiveness of daily oral and on-demand PrEP is highly dependent on medication compliance, which may be reduced due to low levels of adherence (Marrazzo et al., 2015; Van Damme et al., 2012). LAI-PrEP refers to the injection of a PrEP with a longer half-life (injection every 4–8 weeks), which reduces the medication frequency (Landovitz et al., 2021). A noninferiority trial (HPTN 083, NCT02720094) demonstrated that long-acting injectable cabotegravir, an LAI-PrEP given every 8 weeks, is superior to daily oral PrEP in MSM (Landovitz et al., 2021). The International Antiviral Society-USA Panel first recommended LAI-PrEP in 2020, indicating the great potential to increase the range of HIV prevention options (Saag et al., 2020).
The promotion of PrEP use among MSM with IPV experience is necessary to reduce their risk of HIV infection because MSM with IPV victimization experience is more likely to have unprotected anal sex and higher risk of HIV infection than those without any IPV experience. The willingness to use PrEP may affect the promotion of PrEP use and HIV prevention. However, whether IPV experience would affect attitudes toward PrEP has not been well explored. Previous studies, which examined the relationship between IPV experience and PrEP, mainly focused on heterosexual women in resource-poor areas/regions and reported that IPV may have negative effects on PrEP acceptability, adherence, and usage (Cabral et al., 2018; O'Malley et al., 2021; Roberts et al., 2016). Few studies investigated the effect of IPV experience on PrEP use among MSM, reporting inconsistent results. A cross-sectional study of 863 MSM in the United States found that 31.9% of participants reported current use of PrEP, forced sex and emotional IPV were negatively associated with PrEP use, and the experience of partners’ controlling behaviors was positively associated with PrEP use (Braksmajer et al., 2020). Another study found that MSM victims were more likely to believe their partner would not support their PrEP use; however, the prevalence of IPV was not reported in the study (Kahle et al., 2020).
Very few studies have investigated both various types of IPV and various types of PrEP. To our knowledge, there is no published study examining the relationship between IPV and PrEP use in China. Therefore, using cross-sectional data in Chengdu, China, this study aimed to investigate the prevalence of the intention to use different types of PrEP among MSM in Chengdu, China, and to explore the associations between IPV experience and willingness to use PrEP. We hypothesize that the intention to use different types of PrEP would be high, and IPV experience would hinder the willingness to use PrEP in MSM.
Methods
Study Setting, Sample, and Procedure
This cross-sectional study was conducted at a local gay-friendly health consulting service center operated by a non-governmental organization (NGO), in Chengdu, China, from November 2018 to May 2019. Chengdu is the capital city of Sichuan Province in southwest China. The prevalence of HIV infections among MSM was reported to be 10.21% (95% CI = 7.67–13.13) in southwest China in 2010, which was higher than the prevalence in other regions of China (Zhang et al., 2013). There was no PrEP promotion policy or program in Chengdu during the study period.
The study included participants who (1) were male, (2) were at least 18 years old, (3) were living in Chengdu, (4) had had anal sex with at least one man in the last 6 months, (5) were HIV-negative, and (6) had had at least one regular intimate partner in their lifetime. Two experienced full-time staff from a local NGO facilitated recruitment and data collection. The NGO has a contact list that includes clients that have agreed to be contacted for a research purpose and only the staff have access to it. The staff made phone calls through this contact list to approach potential participants, briefly introduced them to the aim and the procedure of the study, and invited them to participate. Most of the surveys were done during their visits to the NGO for general services such as HIV testing. Free HIV testing and ¥50 (approximately $7) were offered to the participants as compensation for their time. After providing written informed consent, the participants completed an online survey on the questionnaire platform Wenjuanxing (wjx.cn) (Li et al., 2020; Tian et al., 2021). Logical errors and completeness were automatically checked by the Wenjuanxing platform. After the survey, participants were provided a brief introduction to the three types of PrEP, including basic information, the benefits and methods of use, the frequency of use (daily, on-demand, or every 8 weeks), and the potential risks. The details of the study procedure are described elsewhere (Wei et al., 2019).
One thousand and twenty-four potential participants were successfully approached, and 800 (response rate: 78.1%) completed the survey. Of these 800 respondents, 192 were excluded (24.0%) based on the inclusion and exclusion criteria, resulting in 608 participants. The Human Studies Committee of Sun Yat-Sen University approved this study (ID: [2018] 049).
Measurements
Background information
Sociodemographic information, including age, ethnicity (Han or other), educational level (below university, university, or above), personal monthly income (≤¥1,000, ¥1,001–3,000, ¥3,001–6,000, ¥6,001–8,000, ¥8,001–10,000, ¥10,001–20,000, ¥20,001–50,000, or ≥¥50,000), sexual orientation (homosexual, heterosexual, bisexual, others), history of sexually transmitted diseases (STDs; “yes” or “no”), age at first homosexual intercourse (<18 years, ≥18 years), the total number of sexual partners, and alcohol consumption (“yes” or “no”; “no”: ≤1 time per month, or “yes”: >1 time per month), were collected. Marital status was also requested, with the following four available responses: currently single (having neither a boyfriend nor a girlfriend), currently in a male–female marriage, currently having a boyfriend, and other. The perceived risk of HIV infection during the next 6 months was determined based on a self-constructed 5-point Likert-type scale ranging from 1 (very high) to 5 (very low). Choices 1 and 2 on this scale were regarded as indicating a high risk while choices 3, 4, and 5 were regarded as indicating a low risk.
HIV literacy
A 12-item self-constructed scale was used to evaluate the participants’ knowledge of HIV, including HIV prevention, diagnosis, and treatment (Cao et al., 2020). Each item was phrased as a statement, and the participants were required to make a true or false judgment based on their knowledge. One point was awarded if the answer was correct, and no points were added or deducted if the answer was incorrect. The level of HIV literacy was calculated based on the total score, which ranged from 0 to 12, with a lower score indicating a lower level of HIV literacy. The Cronbach’s α coefficient for this scale was 0.647.
Awareness of, willingness to use, and intention to adhere to PrEP
PrEP awareness
The participants were initially asked whether they had heard of PrEP before this study. For those who had heard of PrEP, the following four dichotomous (“yes” or “no”) statements were used to explore the participants’ level of PrEP awareness: (1) “Have you ever heard of PrEP?,” (2) “Have you ever heard of daily oral PrEP?,” (3) “Have you ever heard of on-demand PrEP?,” and (4) “Have you ever heard of LAI-PrEP?” The Cronbach’s α coefficient for this measure was 0.721.
Willingness to use PrEP
A 5-point Likert-type scale with the following 3 items was designed to explore participants’ willingness to use PrEP: (1) “Given that PrEP is free and decreases the risk of HIV infection by up to 90%, would you use daily oral PrEP in the next 6 months?”; (2) “Given that PrEP is free and decreases the risk of HIV infection by up to 90%, would you use on-demand PrEP in the next 6 months?”; and (3) “Given that PrEP is free and decreases the risk of HIV infection by up to 90%, would you use LAI-PrEP in the next 6 months?” The responses were scored from 1 (definitely would not) to 5 (definitely would). For each type of PrEP, those who gave responses from 1 to 3 were classified as having a low level of intention, and those who chose 4 or 5 were classified as having a high level of intention. The overall willingness to use PrEP was defined as having a high level of intention in one or more of the 3 items. The Cronbach’s α coefficient for this measure was 0.854.
Perceived PrEP adherence intention
A self-constructed 3-item scale was used to measure the perceived PrEP adherence intention based on the response to the following question: “If you were taking PrEP, would you take it strictly as prescribed?” The response was entirely hypothetical because none of the participants were taking PrEP during the study, nor had they previously taken PrEP. The response was a 5-point Likert-type scale ranging from 1 (definitely would not) to 5 (definitely would). Choices 1, 2, or 3 were designated as a low level of intention and choices 4 and 5 were designated as a high level of intention. The self-reported hypothetical adherence to PrEP was determined for each of the three types of PrEP use. The Cronbach’s α coefficient for this measure was 0.791.
Perceived benefit of PrEP at reducing condom use
The participants were asked, “Are you likely to reduce condom use during anal sex after taking PrEP?” The responses were on a 5-point Likert-type scale (1 = definitely not, 2 = probably not, 3 = uncertain, 4 = probably will, 5 = definitely will). Choices 3, 4, and 5 were designated “yes” and choices 1 and 2 were designated “no.”
IPV
We used 5 items from the Intimate Partner Violence Among Gay and Bisexual Men (IPV-GBM) Scale to explore the participants’ IPV experience. The IPV-GBM was developed for MSM (Stephenson & Finneran, 2013), and it has been widely validated and used worldwide and in China (Kahle et al., 2020; Wei et al., 2019). We used the following questions to assess dimensions of physical violence, sexual violence, monitoring behaviors, controlling behaviors, and emotional violence: (1) “Have any of the following happened in your relationship with your intimate partner: destruction of property, grabbing, restraining, pushing, kicking, slapping, punching, threats of violence or other acts of physical intimidation?” (2) “Have you ever had compulsive sex with an intimate partner? Examples may include any of the following: oral or anal sex, having sex with others, having sexual partners outside the relationship, or any other sexual activity that made you feel uncomfortable.” (3) “Have any of the following happened in your relationship with your intimate partner: demanding access to cell phone and email, reading email or text messages without partner knowledge and repeatedly posting on a partner’s social network pages?” (4) “Have any of the following happened in your relationship with your intimate partner: preventing a partner from seeing his family/friends/ colleagues or communicating with them?” (5) “Have any of the following happened in your relationship with your intimate partner: insulting a partner (by making insulting comments about him), criticizing him (by criticizing him for being fat, for dressing up, for sexual behaviors, their appearance, etc.), threatening him (by threatening to break off the relationship), yelling at him or demanding that he be more manly?” The responses to each statement were as follows: (A) “I have done the above to my partner,” (B) “My partner has done the above to me,” (C) “Both A and B,” or (D) “Neither A nor B.” The participants who chose A or C were defined as IPV perpetrators and those who chose B or C were defined as IPV victims. Thus, we identified IPV experience categorized as specific types of IPV perpetration (participants who chose A or C), specific types of IPV victimization (participants who chose option B or C), and specific types of IPV violence (participants who chose A or B or C). Moreover, the following three additional variables were defined: (1) any type of IPV perpetration (participants who chose either A or C in any of the five types of IPV), (2) any type of IPV victimization (participants who chose either B or C in any of the five types of IPV), and (3) any type of IPV (participants who chose either A or B or C in any of the five types of IPV). The Cronbach’s α coefficient for this measure was 0.574.
Statistical Analysis
Continuous variables are expressed as the mean ± standard deviation and categorical variables as relative frequency percentages. Four dependent variables, including the willingness to use daily oral PrEP, the willingness to use on-demand PrEP, the willingness to use LAI-PrEP, and the overall willingness to use PrEP, were analyzed in this study. In the first step, univariate logistic regression analyses were performed, and the odds ratio (ORs) of background variables (such as educational level, history of STDs, and HIV literacy) and different types of IPV (five types of victimization, perpetration, and any IPV) were calculated (un-adjusted OR [ORu]). In the second step, multivariate logistic regression analyses were performed to explore the associations between different types of IPV and four dependent variables, after adjustment for the statistically significant background variables identified in the first step (p < 0.05). The adjusted OR (ORa) and 95% CI were calculated in this step. All analyses were performed using SAS software (Version 9.4; SAS Institute Inc., Cary, NC, USA). The level of statistical significance was set as p < 0.05 (two-sided).
Results
Overall
The average age of the 608 participants was 31.8 ± 12.3 years, and 47.9% of them had a university-level education or above. The marital status was reported to be single for 43.8% of the participants, whereas 29.9% currently had boyfriends and 17.1% were in a male–female marriage. Most of the participants were of Han nationality (97.9%) and self-reported as homosexual (74.5%). A history of STDs was reported by 7.2% of the participants, and 15.0% reported having their first homosexual intercourse before 18 years old. Twelve percent of the participants were perceived to have a high or very high risk of HIV infection and 22.0% reported alcohol consumption. The mean score for the HIV literacy scale was 9.1 ± 2.1, ranging from 0 to 12. These details are shown in Table 1.
Demographic Characteristics of the Participants (N = 608).
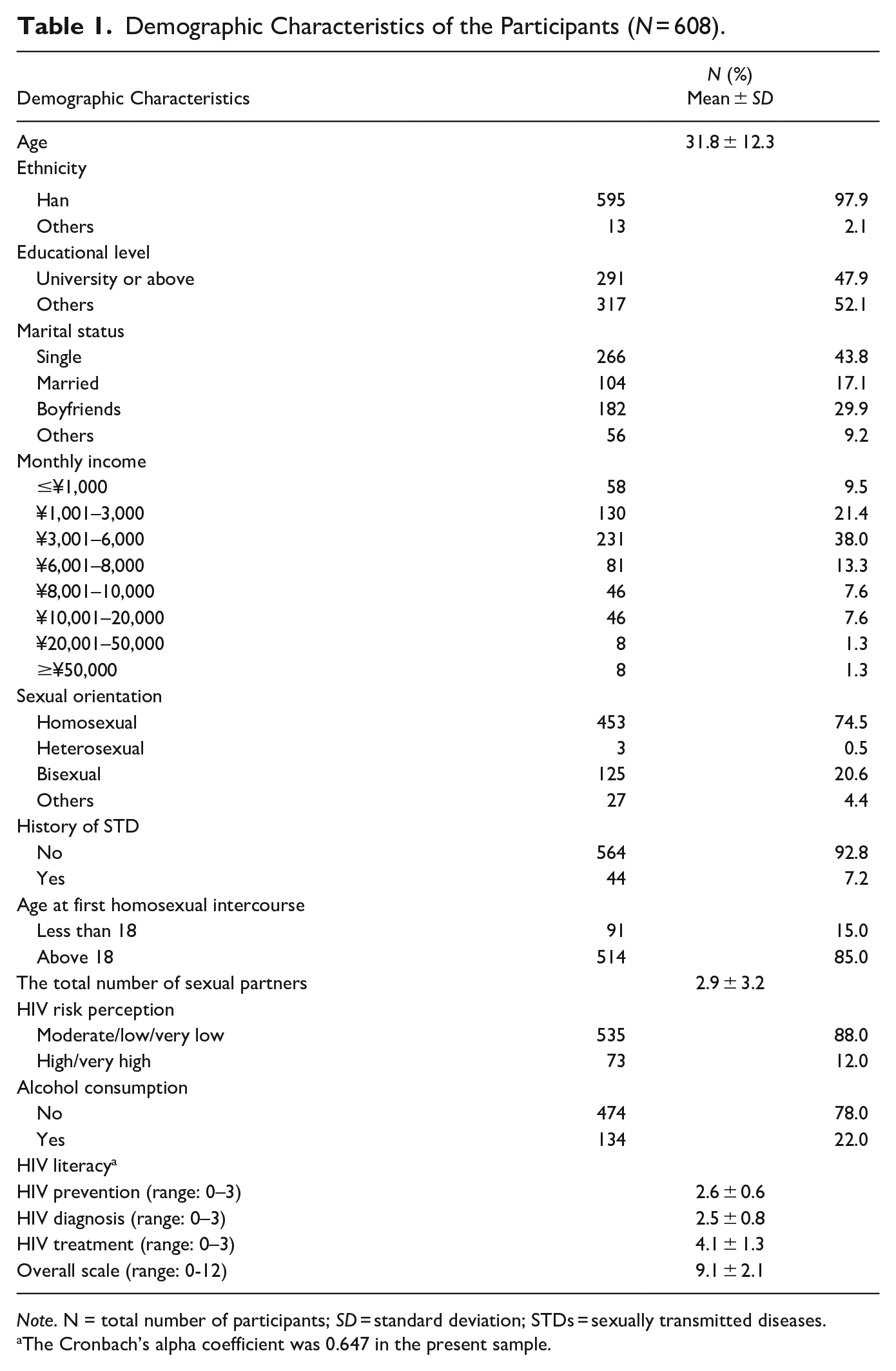
Note. N = total number of participants; SD = standard deviation; STDs = sexually transmitted diseases.
The Cronbach’s alpha coefficient was 0.647 in the present sample.
Approximately half of the participants (48.9%) were aware of PrEP before this study, and only 7.2% of participants were aware of LAI-PrEP. Most (82.2%) of the participants were willing to use any type of PrEP, and the willingness rate for daily oral PrEP, on-demand PrEP, and LAI-PrEP was 60.5, 77.0, and 61.2%, respectively. The adherence intention rate was 70.2, 83.2, and 69.7% for daily oral PrEP, on-demand PrEP, and LAI-PrEP, respectively. Approximately one third (33.7%) of the participants reported that they may reduce condom use if they began to take PrEP. These details are shown in Table 2.
PrEP-Related Cognitions in the Study Participants (N = 608).
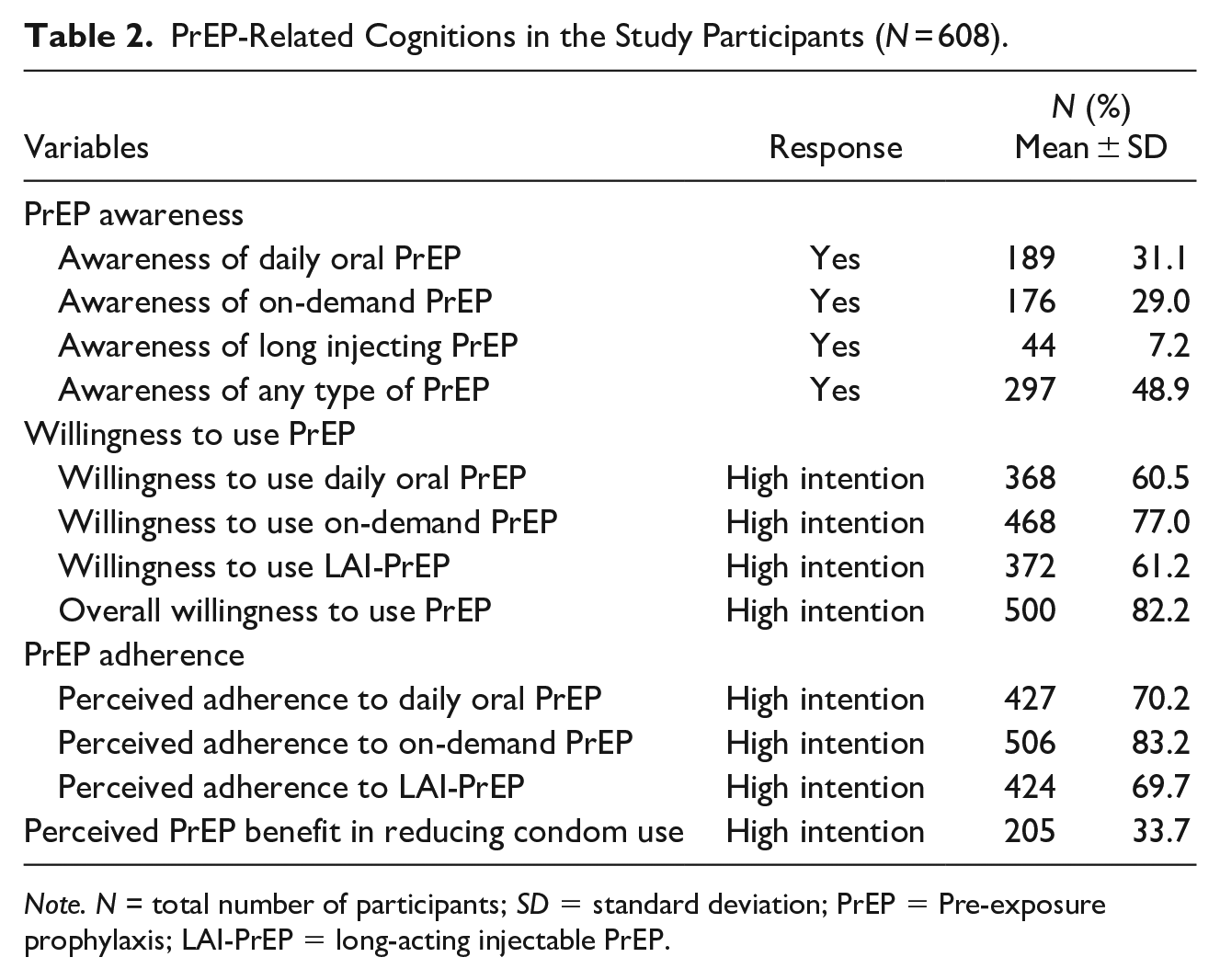
Note. N = total number of participants; SD = standard deviation; PrEP = Pre-exposure prophylaxis; LAI-PrEP = long-acting injectable PrEP.
The prevalence of any IPV victimization and perpetration was 25.3 and 26.0%, respectively. Specifically, 32.6% of the participants (198/608) had experienced at least one type of IPV. Monitoring was the most common type of IPV (16.1%), followed by emotional violence (14.8%), physical violence (10.2%), sexual violence (9.5%), and controlling (7.4%). These details are shown in Table 3.
The Prevalence of Different Types of IPV in MSM in Chengdu (N = 608).
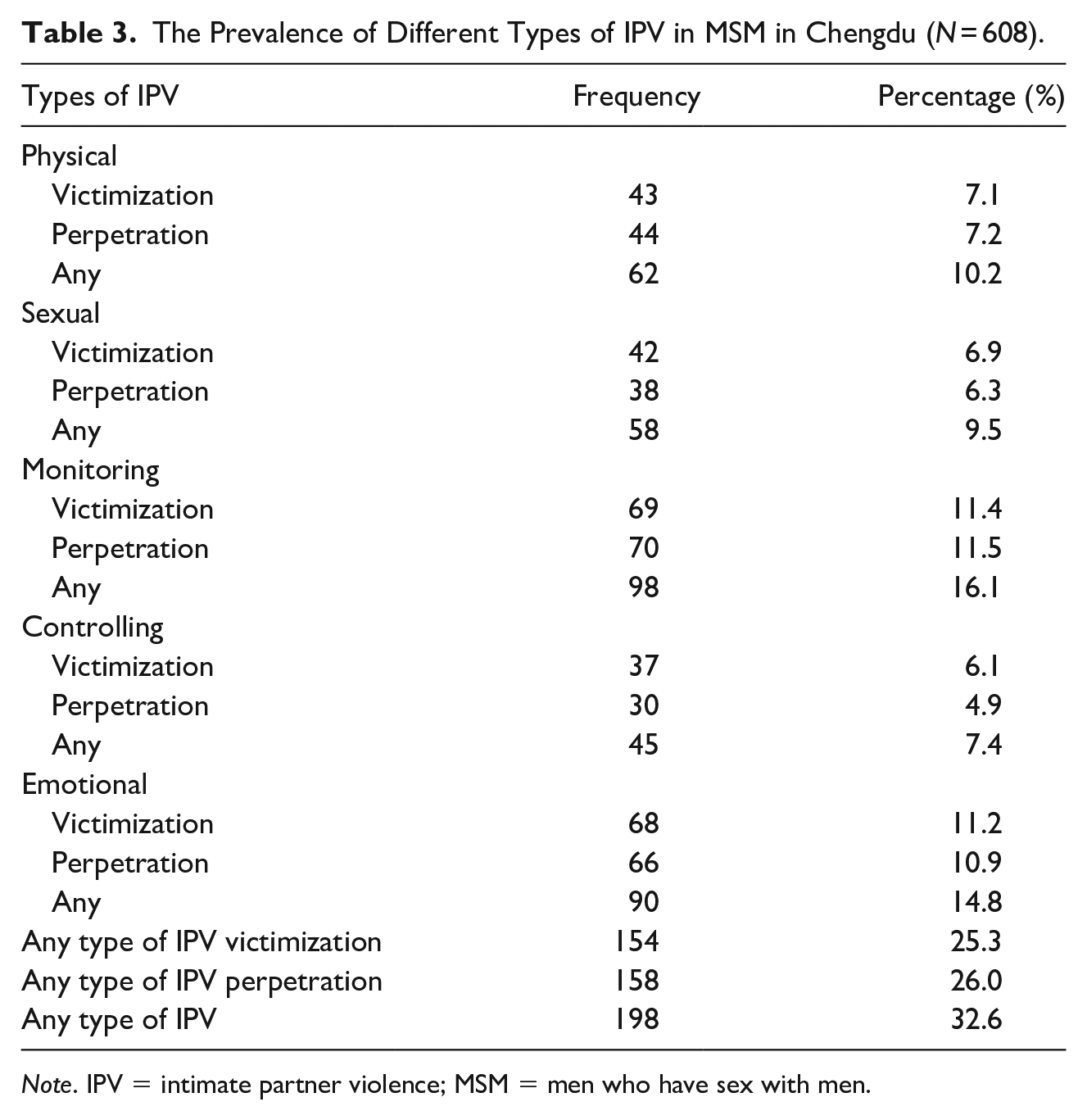
Note. IPV = intimate partner violence; MSM = men who have sex with men.
IPV and Willingness to Use PrEP
IPV and willingness to use daily oral PrEP
In a univariate analysis, four background variables (i.e., education, marital status, age of first homosexual intercourse, and HIV perception), the perpetration of emotional IPV, and perpetration of any type of IPV, were significantly associated with a willingness to use daily oral PrEP and were included in the multivariate logistic analysis. The results of these analyses are shown in Tables 4 and 5. The results of the multivariate logistic regression analysis showed that after adjusting for significant background variables, the perpetration of any type of IPV was negatively associated with the willingness to use daily oral PrEP (ORa = 0.64, 95% CI = 0.43–0.94).
Univariate Analysis on Different Types of IPV and Background Variables Associated With Willingness to Use PrEP.
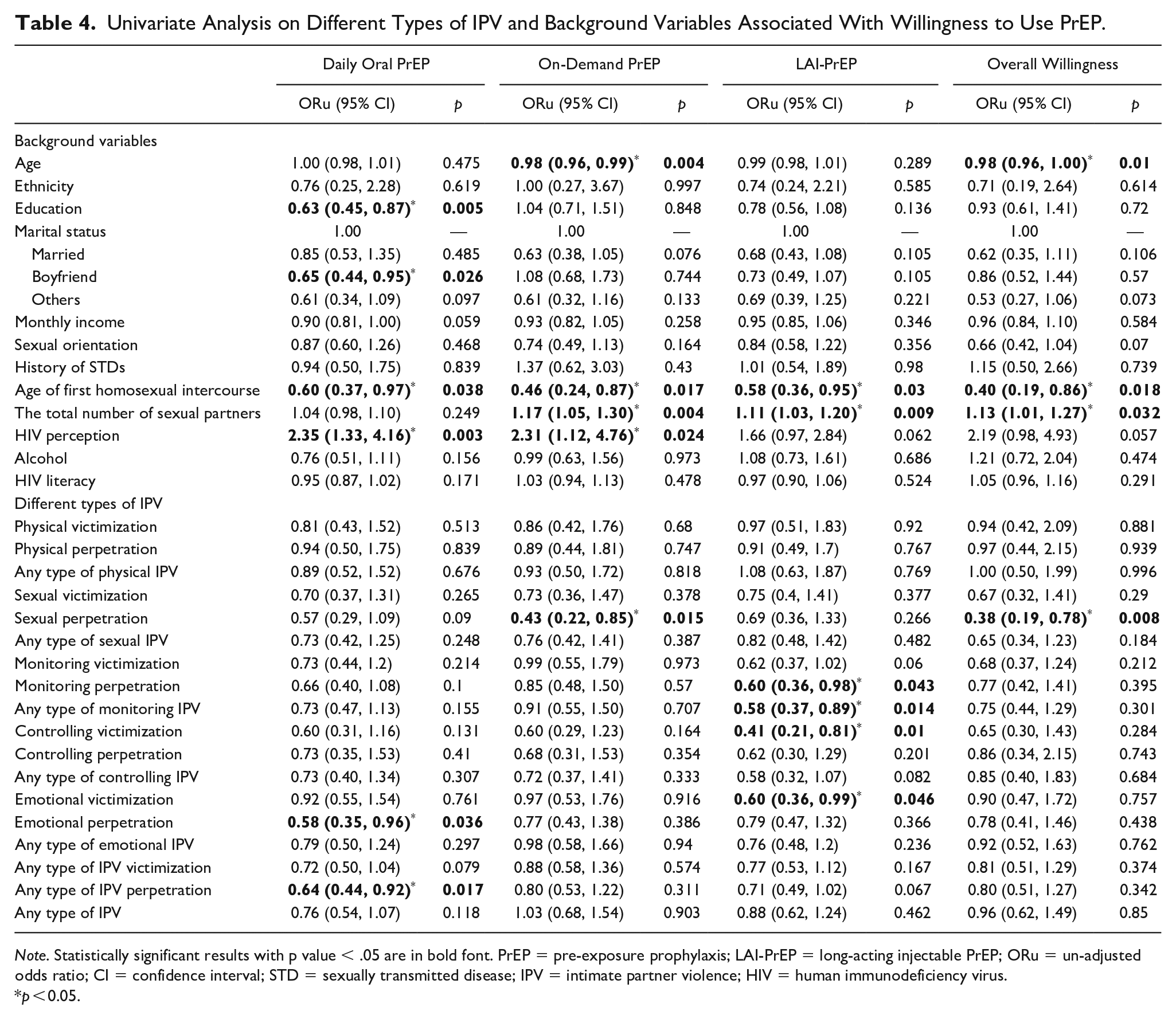
Note. Statistically significant results with p value < .05 are in bold font. PrEP = pre-exposure prophylaxis; LAI-PrEP = long-acting injectable PrEP; ORu = un-adjusted odds ratio; CI = confidence interval; STD = sexually transmitted disease; IPV = intimate partner violence; HIV = human immunodeficiency virus.
p < 0.05.
Multivariate Analysis on Different Types of IPV Associated With Willingness to Use PrEP.
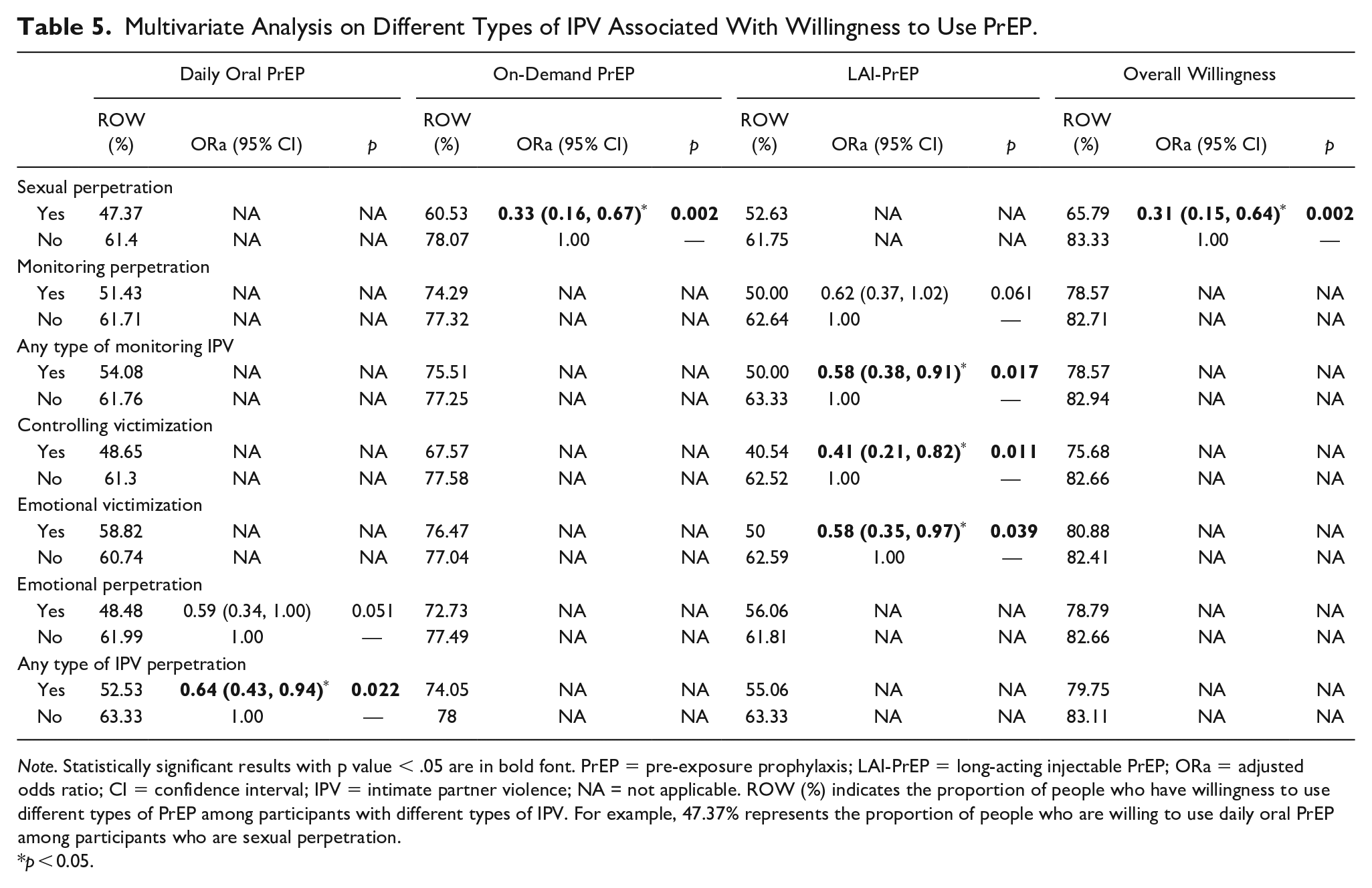
Note. Statistically significant results with p value < .05 are in bold font. PrEP = pre-exposure prophylaxis; LAI-PrEP = long-acting injectable PrEP; ORa = adjusted odds ratio; CI = confidence interval; IPV = intimate partner violence; NA = not applicable. ROW (%) indicates the proportion of people who have willingness to use different types of PrEP among participants with different types of IPV. For example, 47.37% represents the proportion of people who are willing to use daily oral PrEP among participants who are sexual perpetration.
p < 0.05.
IPV and willingness to use on-demand PrEP
In a univariate analysis, four background variables (i.e., age, age of first homosexual intercourse, total number of sexual partners, and HIV perception) and sexual perpetration of IPV were associated with a willingness to use on-demand PrEP and were included in the multivariate logistic regression analysis (Table 4). In the multivariate logistic analysis, sexual perpetration of IPV was negatively associated with a willingness to use on-demand PrEP after adjusting for significant background variables (ORa = 0.33, 95% CI = 0.16–0.67, Table 5).
IPV and willingness to use LAI-PrEP
Two background variables (age of first homosexual intercourse and total number of sexual partners), monitoring perpetration, any type of monitoring IPV, controlling victimization, and emotional victimization were associated with a willingness to use LAI-PrEP in a univariate analysis (Table 4). In the adjusted analysis, a willingness to use LAI-PrEP was negatively associated with any type of monitoring IPV (ORa = 0.58, 95% CI = 0.38–0.91), controlling victimization (ORa = 0.41, 95% CI = 0.21–0.82), and emotional victimization (ORa = 0.58, 95% CI = 0.35–0.97, Table 5).
IPV and overall willingness to use PrEP
Sexual perpetration of IPV (ORu = 0.38, 95% CI = 0.19–0.78) was negatively associated with an overall willingness to use PrEP in a univariate analysis (Table 4). This association remained significant after adjusting for significant background variables (ORa = 0.31, 95% CI = 0.15–0.64, Table 5).
Discussion
Summary
This is the very first study to investigate the association between IPV and willingness to use three different types of PrEP (daily oral PrEP, on-demand PrEP, and LAI-PrEP) among MSM in China. We found that MSM with IPV experiences had lower levels of willingness to use PrEP, especially LAI-PrEP, and participants had a lower awareness of LAI-PrEP than of daily oral and on-demand PrEP.
The Prevalence of Different Types of IPV in MSM
In this study, the prevalence of any type of IPV victimization and perpetration was 25.3 and 26.0%, respectively. Monitoring was the most common type of IPV (16.1%), followed by emotional violence (14.8%). These results were consistent with those of previous studies showing that Chinese MSM have a high prevalence of IPV (18.7–35.5%) (Davis et al., 2015; Liu et al., 2018; Wang et al., 2018a; Wei et al., 2019). The most recent meta-analysis, including 52 studies with 32,048 participants, reported that the pooled prevalence of IPV victimization was 33% and the pooled prevalence of IPV perpetration was 29% across all recall periods in the MSM population, and these values were similar to or even higher than the prevalence of IPV in heterosexual couples (Liu et al., 2021). It is worth mentioning that previous studies have usually categorized monitoring, emotional, and controlling behaviors as psychological violence (in contrast to physical or sexual violence) and have reported that psychological violence is the most common type of IPV (Dokkedahl et al., 2019; Liu et al., 2021; Wei et al., 2020a). We determined the prevalence of different types of IPV and found that monitoring was the most common type, followed by emotional violence, both of which may be labelled as psychological violence. Similarly, in a study in the United States, Braksmajer et al. reported that monitoring and emotional violence were the most common types of IPV in MSM in the past 6 months (45.1 and 36.3%, respectively) (Braksmajer et al., 2020). Other studies reported that emotional violence is the most common type of IPV, with a pooled prevalence of 33% for emotional victimization and 41% for emotional perpetration (Davis et al., 2016; Liu et al., 2021; Stephenson & Finneran, 2017). Psychological violence could result in post-traumatic stress disorder, depression, and anxiety (Lagdon et al., 2014); and it is less visible, less frequently investigated, and more difficult to distinguish than physical and sexual violence, and therefore, it requires more attention (Wei et al., 2020a).
Associations Between IPV Experience and Willingness to Use PrEP
We found that perpetration of sexual IPV was negatively associated with the willingness to use on-demand PrEP and the overall willingness to use PrEP, and IPV perpetration was associated with a low level of willingness to use daily oral PrEP. Consistent with our findings, Braksmajer et al. found that forced sex resulted in decreased PrEP use among MSM in the United States (Braksmajer et al., 2020), and Stephenson and Finneran reported that partnered MSM in South Africa and Namibia, who had experienced IPV, showed lower willingness to use PrEP (Stephenson et al., 2021). However, these studies did not address IPV perpetration. We found that experience of IPV perpetration was negatively associated with the willingness to use PrEP. MSM who experience sexual IPV are more likely to experience risky sexual behaviors (Davis et al., 2018; Zhu et al., 2021), including inconsistent or no condom use during sex, forcing sexual intercourse without a condom, and substance use (Duncan et al., 2018; Raj et al., 2006; Stephenson & Finneran, 2017; Stults et al., 2015; Tran et al., 2014). We hypothesize that perpetrators of sexual IPV usually take an insertive role versus receptive during intercourse and have low awareness of HIV risk, leading to negative attitudes toward and low willingness of PrEP use. We also found negative associations between monitoring, controlling victimization, and emotional victimization and the willingness to use LAI-PrEP. To our best knowledge, there are no studies exploring the association between the willingness to use LAI-PrEP and IPV experience among MSM. Despite the underlying causal relationship between IPV and the willingness to use PrEP cannot be explored in detail in this cross-sectional study, our findings benefit the promotion of PrEP and address particular attention to IPV experience in Chinese MSM. Previous modeling studies (Li et al., 2018, 2022; Wang et al., 2018b) have suggested that scaling up PrEP is the key to achieving HIV elimination in a near future among Chinese MSM who are facing an increasing risk of HIV infection. MSM with IPV experience is the target population for PrEP because IPV experience was associated with increased risky sexual behaviors including multiple casual partners and inconsistent condom use (Zhu et al., 2021). In this study, we report IPV experience was an obstacle to PrEP use, which is important in implementing evidence-based PrEP uptake strategies. Thus, we recommend future studies consider the impact of IPV in implementation. However, the results of this study should be interpreted cautiously. Methodological approaches including the measurement of IPV experience, PrEP-related measurements, and the sampling process may be biased. Further studies are needed to clarify the association between IPV and PrEP acceptability and PrEP-related factors.
Low Awareness of and Willingness to Use LAI-PrEP
In this study, only 7.2% of the participants were aware of LAI-PrEP, and the rate of willingness to use LAI-PrEP was 61.2%. Although LAI-PrEP was still in clinical trials and was not available for the public at the time of this study, the results were inspiring and showed great potential for expanding the range of HIV infection prevention options (Landovitz et al., 2021; Saag et al., 2020). The willingness to use LAI-PrEP among MSM in studies was not consistent. Some studies reported that LAI-PrEP was less preferred than daily oral PrEP and other modalities including condoms, non-visible implants, and rectal microbicides, while others reported the opposite (Greene et al., 2017; Meyers et al., 2014, 2018a, 2018b; Oldenburg et al., 2016; Parsons et al., 2016; Wheelock et al., 2013). For example, Meyers et al. studied gay and bisexual men with at least 12 months of oral PrEP experience in New York City and found that two thirds (66.7%) of current oral PrEP users would switch to LAI-PrEP (Meyers et al., 2018a). A Chinese cohort study of MSM reported that more than three quarters (76.0%, 152/200) of the participants said that they would be willing or very willing to use LAI-PrEP rather than daily oral PrEP (Meyers et al., 2018b). These diverse findings suggest that different modalities are preferred by different people depending on their priorities, preferences, and personal situations (Meyers et al., 2018b).
Currently, only daily oral PrEP and on-demand PrEP are promoted for mainstream use in China, and most of the participants of this study had not previously heard of LAI-PrEP. Moreover, people who are experiencing IPV may be concerned about surveillance, financial monitoring, or threats from their partners if they went to clinics or made appointments for PrEP injections. Further, before LAI-PrEP being publicly available, how users may react to the invasive injection procedure is unknown, which we believe could explain the low awareness of and low willingness to use LAI-PrEP in this study.
Limitations
Our study had limitations that should be noted. First, with a cross-sectional design, we could not explore the causal relationship between IPV and willingness to use PrEP. Second, the prevalence of IPV may be underreported and social desirability bias may exist, because IPV is a sensitive topic and self-reporting measurements were used. Third, we explored lifetime IPV experience and consequently, recall and misclassification bias may have occurred. Fourth, our results for MSM in Chengdu may not be generalizable to MSM living in other parts of China or in other countries. However, our results may provide a valuable reference for the link between IPV and willingness to use PrEP. Fifth, we used a questionnaire to assess the willingness of the participants to use PrEP instead of the actual use of PrEP, and the differences between the intention to use and actual use may exist. Finally, information about some key confounders, such as drug usage and the HIV infection status of the participants’ partners, was not collected.
Conclusions
We investigated the association between IPV and the willingness to use PrEP in Chinese MSM. We found that MSM in Chengdu had a much lower awareness of LAI-PrEP than of daily oral or on-demand PrEP. Moreover, we found that IPV experience had a negative association with the willingness to use PrEP, especially LAI-PrEP. These results remind us that, compared with simply focusing on sexual risk reduction, interventions addressing IPV in addition to PrEP may be more effective at reducing HIV infection risk in MSM. Based on the findings of this study, we recommend that PrEP promotion programs should consider IPV screening, establish social support for MSM, and develop specific intervention strategies for both perpetrators and victims.
Footnotes
Acknowledgements
We thank all the field staff and participants for their cooperation and their support in the data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This research was supported by the Shenzhen Science and Technology Innovation Commission (JCYJ20190809162411393) and the National Natural Science Foundation of China (grant numbers 81803334).