
Abstract
Sexual revictimization is heightened among military service members and veterans and is associated with greater posttraumatic stress symptoms (PTSS) and severity. The heightened distress following revictimization may be due to posttraumatic cognitions (PTC), which include negative beliefs about the self and world, and self-blame. Moreover, it is unclear whether men and women experience different levels of PTC. The current study tested PTC (overall and subdomains) as a possible mediator between sexual revictimization and PTSS severity, and gender as a possible moderator of these associations. Revictimization was defined across time periods (military sexual assault [MSA] only vs. premilitary sexual trauma + MSA) and in military rape frequency (0, 1, 2+). Participants were 400 (n = 200 [50%] male) service members/veterans with a history of MSA and completed online, anonymous, self-report questionnaires. PTC mediated the association between revictimization and PTSS severity. A significant interaction of gender suggested that men reported high overall PTC and PTC about the self regardless of revictimization; by contrast, overall PTC and PTC about the self were lower for women in response to MSA only and increased with revictimization. Results also showed men were more sensitive to PTC about self-blame as it pertains to more severe PTSS compared to women. There were no unique gender interactions when assessing revictimization by rape frequency, although PTC (overall, all subdomains) significantly mediated the association between rape frequency and PTSS severity. PTC may be a beneficial target when treating PTSS in men, and may be especially heightened in women who have experienced revictimization.
Keywords
Posttraumatic stress disorder (PTSD) is one of the most prevalent mental health disorders among Veterans Affairs (VA)-enrolled veterans (Veterans Health Administration, 2013) and active duty service members (Meadows et al., 2018), accounting for over 55% of those with a probable mental health diagnosis (VA, 2017). PTSD and posttraumatic stress symptoms (PTSS) are associated with lower quality of life (Vogt et al., 2017), sexual dysfunction (Blais et al., 2022), poorer interpersonal functioning (Blais, 2020, 2022; Blais & Zalta, 2023), substance misuse (Schumm & Chard, 2012), and suicidal ideation and attempts (Wisco et al., 2014), highlighting the importance of continuing to study risk factors of PTSS to fine-tune assessments and treatments. Traumas that involve sexual violation are associated with the highest risk for PTSS (Blais et al., 2020; Wisco et al., 2014), with repeated exposure conferring even greater risk (see review, Classen et al., 2005; Tirone, Bagley et al., 2020a). Notably, those with a history of military sexual assault (MSA), or sexual assault that occurred during their military service, are 2 to 4.5 times more likely to have experienced previous sexual assault compared to those without a history of MSA (Schry et al., 2015, 2016), and is significantly associated with greater risk for sexual revictimization (see review, Tirone, Bagley et al., 2020a). As such, it is critical to study sexual revictimization within the MSA-exposed population.
One way to measure MSA revictimization is by stage of life in which the sexual assault(s) occurred. Among US military service members, sexual assaults before and during military service demarcate possible critical stages for examination, as those who were revictimized across multiple time periods experienced greater PTSS compared to MSA only (Blais et al., 2022; Creech & Orchowski, 2016). Another way sexual revictimization can be measured is by frequency of sexual assaults. Compared to those who indicated a single exposure of sexual assault, US service members/veterans who indicated a higher sexual assault frequency experienced higher PTSS (Tirone, Smith et al., 2020b).
It is also critical to examine possible mechanisms of this association given that not all who experience MSA develop PTSD (Kimerling et al., 2010). One possible mechanism is posttraumatic cognitions (PTC), or how an individual thinks about their traumatic event and what they believe about themselves and others as a consequence of that event (Tolin & Foa, 2002). PTC are grouped into three domains: negative beliefs about the self (e.g., “I am a weak person”), negative beliefs about the world (e.g., “People can’t be trusted”), and self-blame (e.g., “The event happened because of the way I acted”; Foa et al., 1999). MSA exposure is positively associated with more negative PTC overall (e.g., Carroll et al., 2018; Holliday et al., 2018). It is also theorized that revictimization strengthens one’s negative PTC by confirming their negative beliefs about the world or themselves (Tolin & Foa, 2002). Evidence further shows that greater negative PTC are predictors of worse PTSS severity (e.g., Gómez de La Guesta et al., 2019), suggesting that more severe MSA revictimization history leads to more severe negative PTC, and more severe negative PTC leads to more severe PTSS.
Finally, men and women may have different experiences with negative PTC following MSA, suggesting that gender may act as a moderator of this mechanistic model. Theories suggest women are at greater risk for more severe negative PTC relative to men due to factors such as peri-traumatic fear (e.g., Rattel et al., 2019; Tolin & Foa, 2006) and gender-specific socialization that make women more likely to internalize attributions of blame (Krause et al., 2002), yet evidence is mixed, perhaps in part because not all samples account for trauma type in a uniform manner (e.g., Christ et al., 2022; Sexton et al., 2018). Other studies of gender differences are limited to civilians (e.g., Daie-Gabai et al., 2011), limiting generalizability to military samples. The current study examines gender as a moderator of the association of MSA revictimization history and PTC, and PTC and PTSS severity in a sample of military men and women who all reported exposure to MSA as the index event for PTC and PTSS.
The primary aim of this study was to explore the possible mediation effect of PTC on the association between sexual revictimization and PTSS severity among service members and veterans, and how these associations may differ by gender. A secondary aim of this study was to assess this model with the three subdomains of PTC, including negative cognitions about the self, negative cognitions about the world, and self-blame. It was hypothesized that all forms of PTC would mediate the association between MSA revictimization history and PTSS severity, such that more severe MSA revictimization history would be associated with worse negative PTC, particularly among men. We further hypothesized that worse negative PTC would then be associated with more severe PTSS, with this latter association stronger among men. All models adjusted for the following variables, given their association with PTSS severity in US military samples: military branch (e.g., Xue et al., 2015), combat history (Hoge et al., 2004), junior ranks (Xue et al., 2015), veteran status (Hoge et al., 2004), minority race (e.g., Dursa et al., 2014), minority sexual orientation (Averill et al., 2015), older age (e.g., Armenta et al., 2018), and PTSD treatment history (e.g., Resick et al., 2015).
Method
Participants and Procedure
Participants were 200 female and 200 male service members/veterans who indicated a history of MSA. Participants were recruited via Qualtrics, Inc. and we intentionally sought to recruit an even number of men and women to ensure adequate power to examine gender differences. Qualtrics, Inc maintains survey panels of volunteers who have specific demographic characteristics, such as a history of current or past military experience. Participants opt into panels and can select which surveys they wish to complete. Inclusion criteria included military service in the post-9/11 era, history of MSA, and aged 18+ years. Prospective participants answered military validation questions to limit possible fraudulent responses (e.g., Pedersen et al., 2015, see Supplemental Appendix A). Incorrect responses to any of these validation items resulted in automatic discontinuation. Of the 1,895 respondents who met initial inclusion criteria, 417 (22.01%) passed the validation questions. We are confident that these responses were valid, as the likelihood of answering all four questions accurately by chance, that is without military experience, is only 0.16%. Of the 410 who passed the validation questions and met all study inclusion criteria, 396 (96.59%) completed the survey. Supplemental Appendix B includes a flowchart of participant eligibility and termination. Participants were provided with an electronic Letter of Information and provided informed consent via electronic checkmark. Participants were compensated directly by Qualtrics panels, with recruitment and compensation costs equaling $20/participant. This study was approved by the Institutional Review Board at Utah State University.
Measures
PTSS severity
PTSS was measured by the PTSD Checklist for DSM-5 (PCL-5; Weathers et al., 2013), a 20-item self-report scale with item responses ranging from 0 (not at all) to 4 (extremely) in terms of how much the symptom has been bothering the participant in the past month. Participants were instructed to respond to each item as it related to their MSA. Scores are calculated by adding all item response scores, with a range of 0 to 80. Higher scores indicate more severe symptoms. The PCL-5 shows good validity and internal consistency (Bovin et al., 2015; Wortmann et al., 2016) and good test-retest reliability (Bovin et al., 2015). A measurement model of PTSS severity was used to assess structure and internal consistency using confirmatory factor analysis. Due to the non-normal distribution of the data, the Weighted Least Squares Mean and Variance Adjusted (WLSMV) estimator was utilized in the models to provide more robust estimates (Finney et al., 2016). This approach is shown to work well for sample sizes greater than 200 (e.g., Bandalos, 2014). This confirmatory factor analysis confirmed the presence of a single factor with excellent model fit: χ2(170) = 416.32, p < .001, comparative fit index (CFI) = 0.92, Tucker-Lewis index (TLI) = 0.91, root mean square error of approximation (RMSEA) = 0.06, with factor loadings ranging from 0.72 to 1.02. The internal consistency was also excellent, Cronbach’s α = .96.
Sexual assault history
Sexual assault history was assessed by the Sexual Experiences Survey–Short Form Victimization (SES-SFV; Koss et al., 2006), a 10-item self-report questionnaire assessing one’s history of unwanted sexual experiences. The language was slightly altered to be more inclusive of the possibility of female perpetrators. For instance, instead of, “A man put his penis into my butt, or someone inserted fingers or objects without my consent. . .,” the language was changed to, “Someone inserted a body part (e.g., finger, penis) or object into my butt without my consent” (Item 4). The SES-SFV distinguishes between six severity levels of sexual victimization, ranging from non-victim, sexual contact, attempted coercion, coercion, attempted rape, and rape. Participants were instructed to indicate the number of times (0, 1, 2, 3+) they experienced each level of sexual victimization for each time period (i.e., premilitary, during military service, post-military service). Consultation amongst co-authors determined no adequate justification distinguishing between 2+ and 3+ rape exposures; therefore to ensure adequate cell sizes among those endorsing a higher number of rapes, we decided to collapse these frequencies into 2+. Any missing values on the SES-SFV were coded as zeros to take the most conservative approach so as to not assume victimization when not explicitly reported.
Sexual revictimization by time period
Participants’ sexual victimization severity was coded as no history (code = 0) versus reported history (code = 1) of sexual assault during each time period (i.e., premilitary, military). Sexual assault was defined as endorsement of any level of victimization on the SES-SFV other than “non-victim.” Those in the revictimization group indicated history of sexual victimization both premilitary and during the military, whereas those in the MSA only group indicated history of sexual victimization during their military service. Because the current sample included both service members and veterans, only a portion of the sample (n = 184, 46.00%) could have experienced post-MSA. Therefore, any veteran who was originally coded in the MSA only group, but also indicated experiencing post-MSA, was removed from the analyses (n = 17, 4.25%) due to low cell size precluding powered analyses.
Military rape frequency
Completed rape frequency was examined during one’s military service and defined by the number of times the participant indicated being raped. Responses were coded in the following levels: 0 times, 1 time, or 2+.
Posttraumatic cognitions
PTC were measured by the Posttraumatic Cognitions Inventory (PTCI; Foa et al., 1999). The PTCI is a 36-item self-report Likert scale with item responses ranging from 1 (totally disagree) to 7 (totally agree) in terms of one’s level of agreement to various cognitions. Participants were asked to respond to each item “as it relates to your sexual assault during your military service.” The PTCI has three subscales: Negative Cognitions About the Self (21 items), Negative Cognitions About the World (seven items), and Self-Blame (five items). Three experimental items were not included in the scoring. Total scores were computed by summing all the items within each subscale, with the following possible total score ranges: Self 21 to 147; World 7 to 49; Self-Blame 5 to 35; Overall 33 to 231. Higher scores indicate more severe negative PTC. The PTCI is validated in veteran samples (Sexton et al., 2018) and shows good internal consistency (Foa et al., 1999) and test-retest reliability (Foa et al., 1999). Similar to the PCL-5, a confirmatory factor analysis with the WLSMV estimator confirmed the presence of the three expected subdomains, and showed excellent model fit: χ2 (492) = 943.49, p < .001, CFI = 0.99, TLI = 0.99, RMSEA = 0.05. See Supplemental Appendix C for individual item standardized factor loadings. The PTCI overall scale and subscales of self, world, and self-blame showed excellent internal consistency in the current sample (Cronbach’s α = .96, .96, .89, and .82, respectively).
Other measures
Demographics
A demographic inventory assessed participant gender (cisgender, gender nonconforming, transgender, two-spirit, other), sexual orientation (straight/heterosexual, sexual minority), age, race (Alaska Native/Native American, Black/African American, Latinx/Hispanic, White/Caucasian, other), military branch (Air Force, Army, Coast Guard, Marine Corps, Navy), rank (enlisted, officer), discharge status (veteran, active), and history of PTSD treatment (yes, no).
Combat history
Combat history was assessed with the Combat Exposure Scale (CES; Keane et al., 1989a), a seven-item scale with responses to each exposure ranging from 1 to 5. Total scores were computed by summing the converted item scores, with a possible range of 0 to 41, and higher scores indicative of greater combat exposure. The CES has excellent test-retest reliability (Keane et al., 1989a) and showed good internal consistency in the current sample (Cronbach’s α = .91).
Analytic Plan
Sample characteristics were assessed using descriptive statistics. Bivariate associations between sexual revictimization, PTSS severity, PTC, and gender, as well as covariates were assessed using correlations, analysis of variance (ANOVA), t-tests, and chi-square tests where appropriate. Missing data were rare and ranged from the removal of 5 to 6 (1.25%–1.57%) participants depending on the specification of the model.
Moderated mediation models assessed the mediating role of PTC overall, as well as the three subdomains, in the association between revictimization history and PTSS severity, and the moderating role of gender on the association of revictimization history, PTC, and PTSS severity. As noted above, models were run in two sets to allow us to examine revictimization by time period and revictimization by military rape frequency. Due to the complexity of these moderated mediation models, models were under-identified for structural equation modeling (SEM) analyses. Therefore, observed variables were used in place of latent variables in the moderated mediation models. Multiple linear regression was used to test the moderation of gender for each path (e.g., testing for an interaction between MSA and gender in predicting PTC). When moderated mediation models did not show a significant moderation, gender and its interaction terms were removed to test a more parsimonious mediation model. Such models were appropriately identified so latent variables were used. As with the confirmatory factor models for PTSS severity and PTC, due to the non-normal distribution of the individual items, the WLSMV estimator was utilized in the models to provide more robust estimates (Finney et al., 2016). Due to issues of multicollinearity in the posttraumatic cognition variables, separate models were utilized for PTC overall and its three subdomains. Covariates had direct paths to PTSS in all models. All statistical analyses were conducted in the R environment (R Core Team, 2020).
Results
Descriptive Characteristics
The sample had similar representation of officer ranks (n = 224, 56.0%) versus enlisted ranks (n = 176, 44.0%), as well as actively serving service members (n = 216, 54.0%) versus veterans (n = 184, 46.0%; see Table 1). Most served in the Army (n = 292, 73.0%) versus other branches (n = 108, 27.0%). Further, the majority of the sample identified as White (n = 289, 72.2%) and a minority of the sample indicated a sexual orientation as something other than heterosexual (n = 39, 0.98%; see Table 1).
Study Variable Comparisons, Stratified by Gender (N = 400).
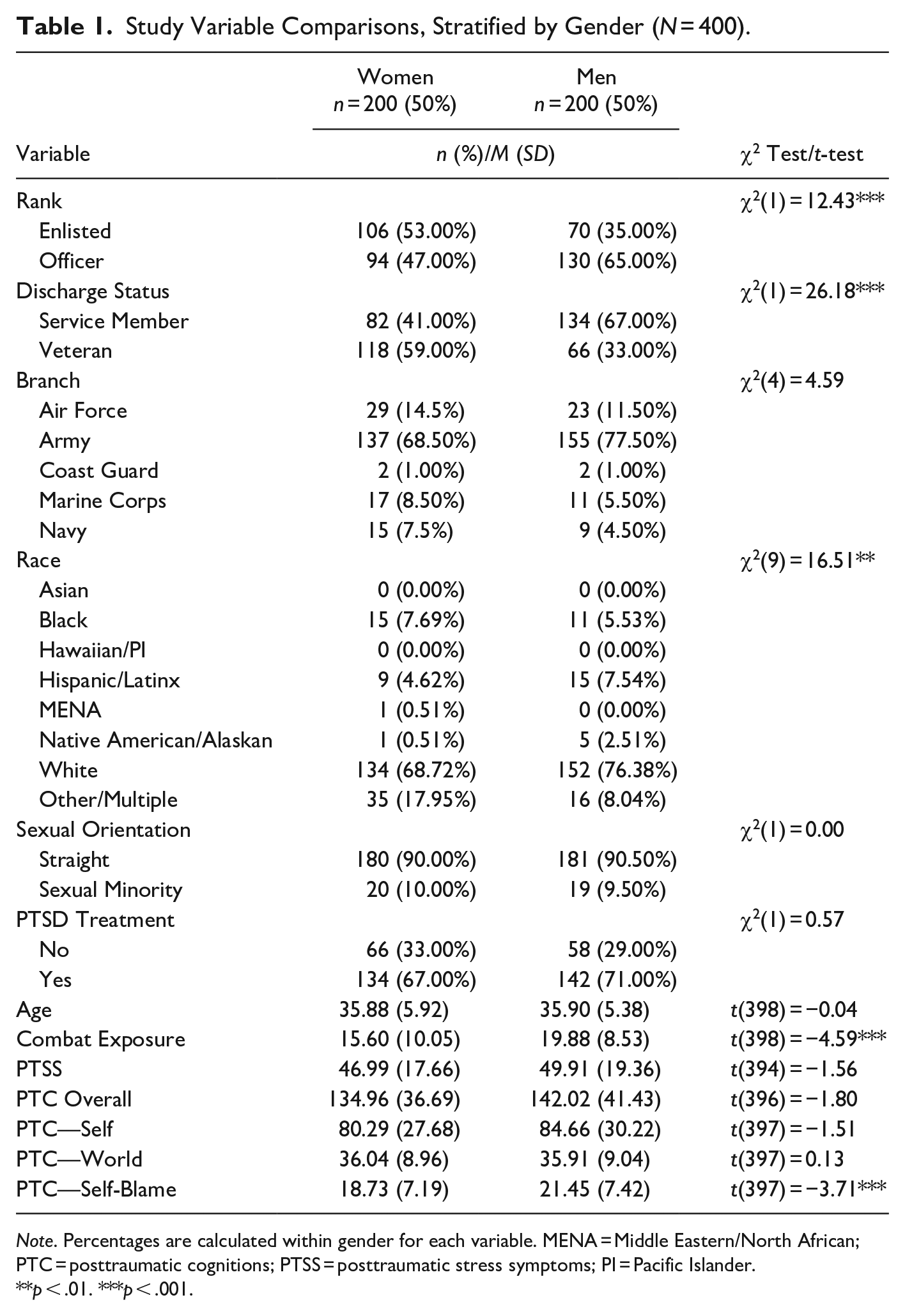
Note. Percentages are calculated within gender for each variable. MENA = Middle Eastern/North African; PTC = posttraumatic cognitions; PTSS = posttraumatic stress symptoms; PI = Pacific Islander.
p < .01. ***p < .001.
MSA exposure and revictimization status of men and women is shown in Table 2. Notably, the majority of men and women reported revictimization across time periods and at least two rapes during military service. The average score on the PCL-5 was 48.46 (SD = 18.57), which is beyond the suggested clinical cut-off score of 31 for probable PTSD (Bovin et al., 2015). The average score on the PTCI was 138.51 (SD = 39.25), which is higher than the median score of 133 in traumatized individuals who meet criteria for PTSD (Foa et al., 1999).
Study Variable Comparisons, Stratified by Revictimization Group (N = 400).
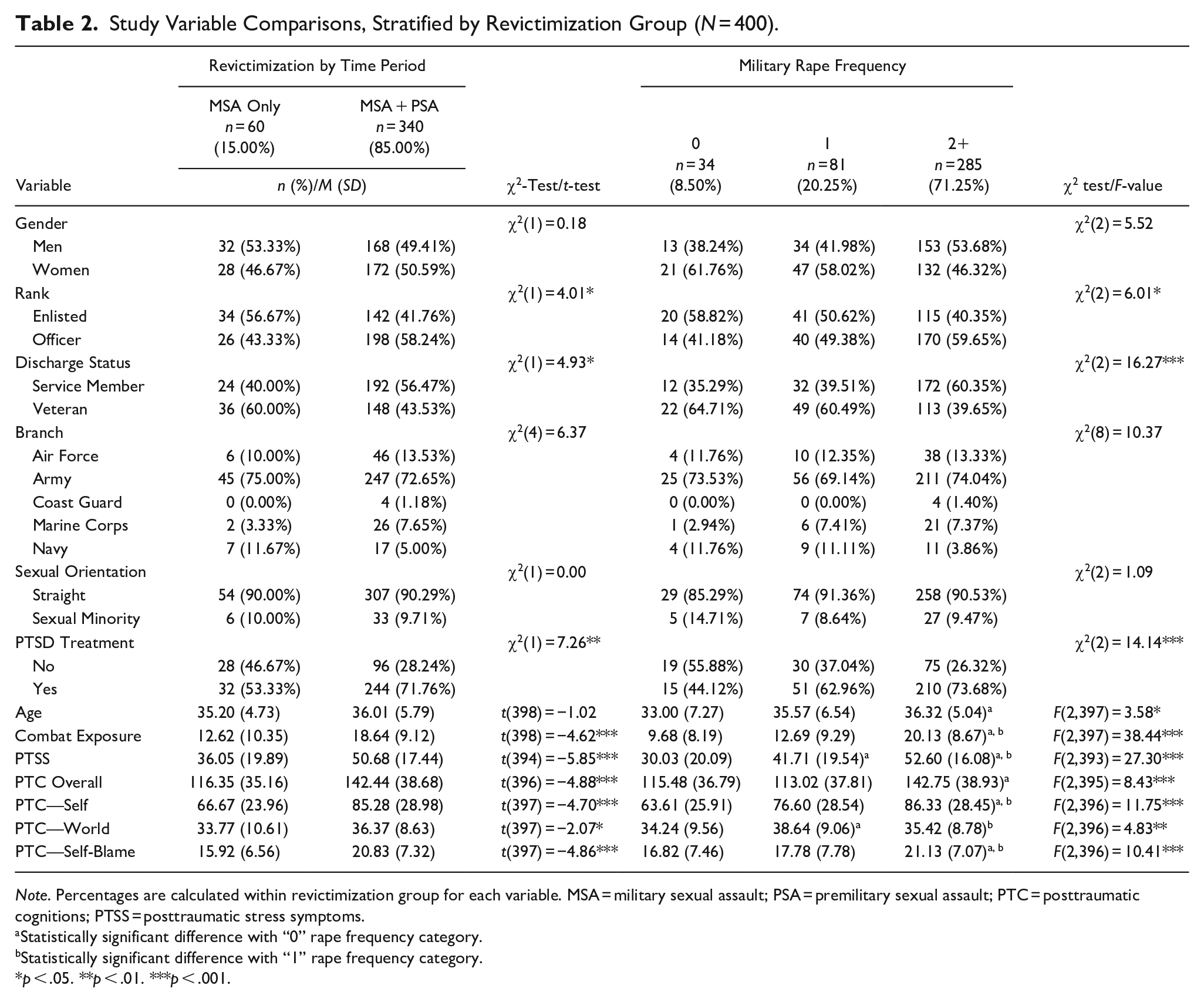
Note. Percentages are calculated within revictimization group for each variable. MSA = military sexual assault; PSA = premilitary sexual assault; PTC = posttraumatic cognitions; PTSS = posttraumatic stress symptoms.
Statistically significant difference with “0” rape frequency category.
Statistically significant difference with “1” rape frequency category.
p < .05. **p < .01. ***p < .001.
Bivariate Associations
There were no differences between men and women with regard to rape by time period or number of rapes. Men had significantly greater PTC about self-blame and greater combat exposure compared to women, but there were no differences in severity of PTSS, PTC about the self, world, and overall cognitions between genders (see Table 1). Those in the revictimization group by time period had significantly higher PTSS, worse PTC overall and about the self, the world, self-blame, and greater combat exposure (p’s < .05; see Table 2) compared to those with MSA only. Compared to those with no military rape history, those with history of one military rape had significantly worse PTSS and worse PTC about the world. Also compared to those with no military rape history, those with 2+ military rapes had significantly worse PTC overall, PTC about the self, PTC about self-blame, greater combat exposure, and older age. Compared to those with history of one military rape, those with 2+ military rapes had significantly worse PTSS, worse PTC about the self and self-blame, less severe PTC about the world, and greater combat exposure. PTSS severity was positively associated with PTC and its subdomains with medium-to-large effect sizes (see Table 3).
Correlations, Means, and Standard Deviations for Continuous Study Variables (N = 400).
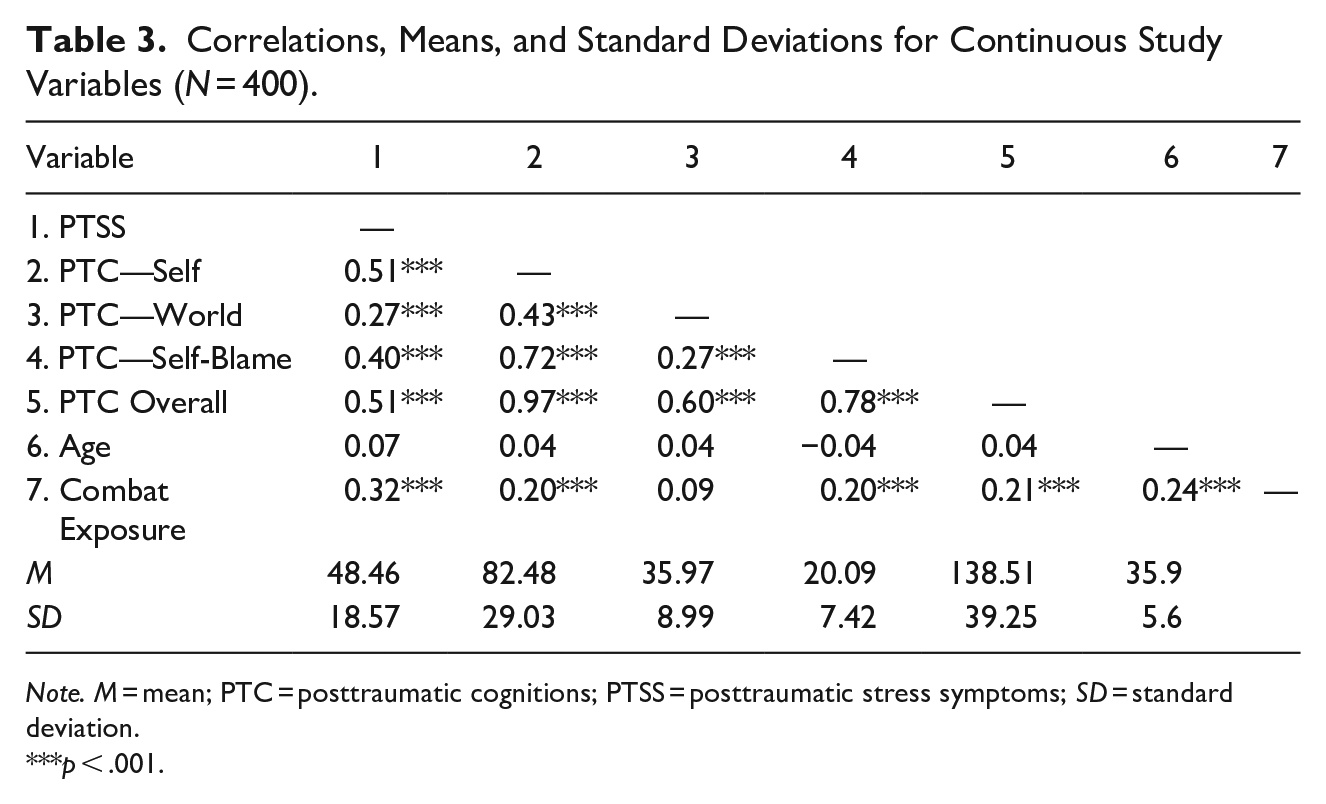
Note. M = mean; PTC = posttraumatic cognitions; PTSS = posttraumatic stress symptoms; SD = standard deviation.
p < .001.
Revictimization by Time Period
Significant moderated mediation models (see Figure 1 for general depiction of models) with PTC overall, PTC about the self, and PTC about self-blame were observed, such that men had relatively high negative PTC overall (β = −.33, p = .043), regardless of revictimization status. By contrast, results for women showed that revictimization (i.e., MSA + PSA), relative to MSA only, was associated with significant increased risk for more severe PTC overall (see Figure 2a). Similar patterns were observed in the model of PTC about the self (β = −.34, p = .039, see Figure 2b). Unlike the previous interactions which were observed on the a-path of the mediation model, we observed a significant interaction on the b-path of the model for the PTC about self-blame model such that men were more sensitive to higher levels of self-blame relative to women (see Figure 2c). In other words, higher levels of self-blame had a stronger relationship with more severe PTSS in men than women. No significant moderated mediation or mediation was observed with PTC about the world.
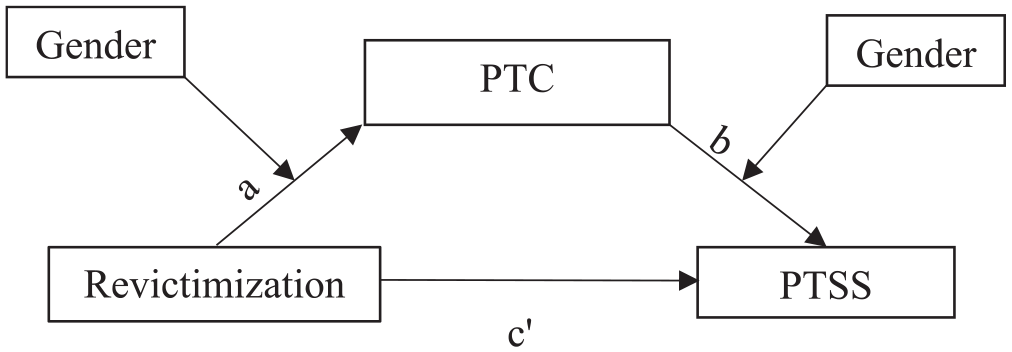
Depiction of moderated mediation model of revictimization by time period, PTC, PTSS, and gender.
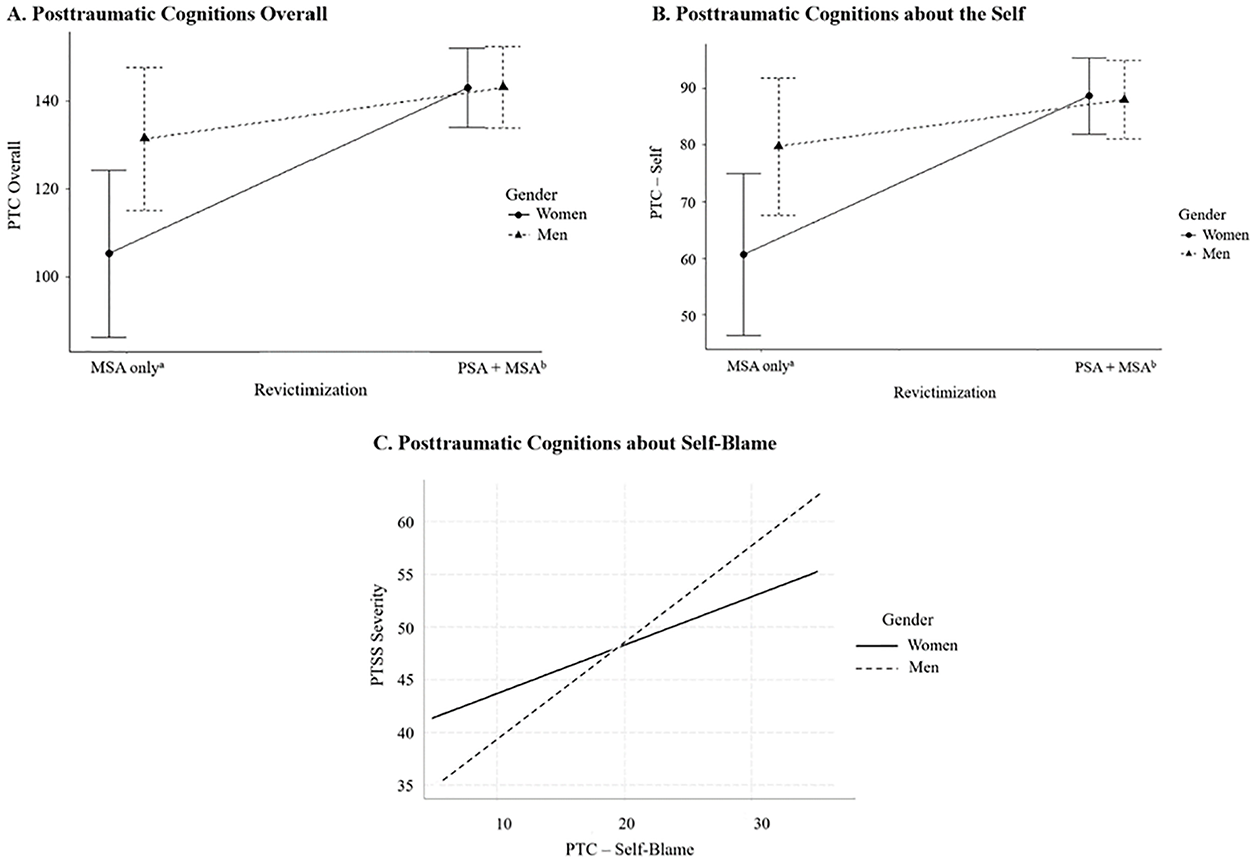
Probe of moderated mediation models of revictimization, PTC, gender, and PTSD symptoms.
Revictimization by Military Rape Frequency
Results showed there were no significant interactions of gender in any of the moderated mediation models of military rape frequency, PTSS severity, and the mediators of PTC overall, PTC about the self, about the world, and self-blame (p’s > .05). Gender was removed from subsequent mediation analyses, resulting in a less complex model that was adequately identified, allowing for the replacement of observed scores with latent variable scores. Significant indirect effects of military rape frequency on PTSS through PTC overall, about the self, the world, and self-blame were observed, such that more severe military rape frequency was associated with worse PTC, and worse PTC was associated with more severe PTSS (see Figure 3a–d). Standard errors vary across paths, resulting in some non-significant results despite the size of the regression coefficient.
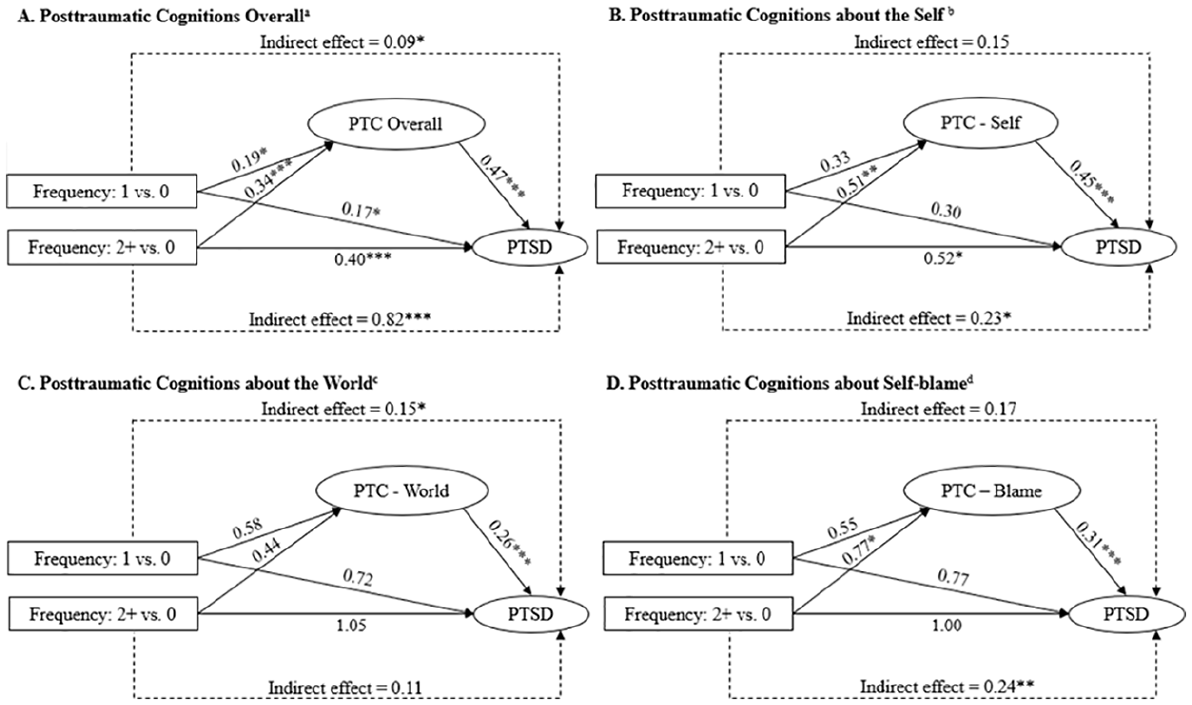
Mediation models of military rape frequency, PTC, and PTSS.
Discussion
The aim of the current study was to determine if PTC were possible mechanisms of the association between sexual revictimization, and PTSS severity among veterans and service members, and if these associations varied by gender. Revictimization history had little effect on men’s level of PTC above the impact of MSA alone. For women however, history of revictimization was associated with increased levels of PTC overall and about the self when compared to MSA alone, such that their severity was similar to that of men. This suggests that while a single occurrence of MSA may result in higher PTC for men, the differences between genders are eliminated if the individuals experienced sexual assault both before and during military service. One possible explanation for this is that MSA is often viewed as an “expected” occurrence amongst women service members (Brownstone et al., 2018), and women may be less likely to internalize an MSA experience that was not preceded by prior exposure to sexual assault. Whereas for men, MSA is not as expected and less common (Wilson, 2018). Therefore, when MSA does occur in men, they may be more likely to question aspects of themselves, such as their masculinity and sexual identity, even without prior sexual trauma (Monteith et al., 2019). By contrast, when an individual is revictimized, it may lead them to make fundamental attributions about themselves (e.g., “I am inadequate”) rather than situational attributions (e.g., “That person took advantage of me”), leading to the similar levels of PTC about the self that were observed in both men and women in the current study.
Results also showed that higher levels of self-blame appear more detrimental to men in terms of PTSS severity. This supports our hypothesis that PTC would be more strongly associated with more severe PTSS in men compared to women. This may be due to possible internalized beliefs about gender roles and rape myth acceptance. For instance, if men hold a prior belief that men cannot be raped (Burt, 1978), they may develop an adapted belief that they are to blame for the assault. The more entrenched their adapted beliefs, the greater the likelihood of more severe PTSS (Resick et al., 2016). While there were significant indirect effects of negative PTC about the self and self-blame on the association between revictimization by time period and PTSS, indirect effects of PTC about the world were non-significant. It is possible that a single exposure to sexual assault impacts one’s view of the world and others to a similar extent as multiple sexual assaults. This warrants further exploration.
There were no significant unique differences between genders on the models operationalizing revictimization by military rape frequency, suggesting that increased frequency of military rape is equally deleterious for both men and women. This was unexpected, given that research shows that men are more likely to have an MSA experience involving multiple offenders and to have been physically injured during the assault compared to women (Morral et al., 2015). That said, severity was assessed by revictimization in the current study and not whether the assault was attempted by multiple offenders or if physical injury was incurred. As such, future studies could build on this literature by determining if measuring MSA in this manner would produce differences in results as a function of gender. Subsequent results showed that PTC overall, as well as PTC about the self, the world, and self-blame, were possible mechanisms of the association between increased frequency of military rape and PTSS severity, similar to the associations found in the revictimization by time period analyses. This again suggests that PTC may become more severe after multiple incidences of sexual victimization (Tolin & Foa, 2002) and are a promising target for treatment.
Results may inform more efficient screening by asking service members/veterans about sexual assault history prior to the military and such results may be used to encourage prevention and early intervention, such as helping the service member improve their threat perception (Messman-Moore & Brown, 2006) and physiological reactivity (Waldron et al., 2015), which are demonstrated as risk factors for revictimization. Furthermore, the majority of the sample reported a history of revictimization across time periods and in military rape frequency, suggesting that sexual assault often does not occur in isolation. It may be helpful for clinicians to take this into consideration when assessing for sexual assault history. Possible interventions for specifically targeting physiological reactivity among survivors of MSA can include mindfulness-based work (e.g., Braun et al., 2021; Gallegos et al., 2015). Additionally, given that PTC were shown to be an important possible mechanism of the link between revictimization history and PTSS severity, it confirms the importance of targeting these thoughts in treatment, such as with Cognitive Processing Therapy (Resick et al., 2016) or Prolonged Exposure Therapy (Foa et al., 2007). Notably, there is evidence to suggest that cognition change is a key mechanism of both of these treatments (Zalta, 2015). There is also evidence suggesting that targeting PTC may even reduce risk for future revictimization (Jaffe et al., 2019), but results are circumscribed to civilians. Further, results suggest that focusing specifically on PTC related to oneself, rather than others, may be most effective, especially when therapy sessions are limited, such as in a deployed environment. Finally, particular attention may be placed on men’s thoughts around self-blame, as these thoughts are especially related to increased PTSS severity and have been shown to be key mechanisms of improvement in PTSS in a military sample with MSA-related PTSD (Holliday et al., 2018).
The field would benefit from studies using longitudinal study designs to better understand the cumulative risk of sexual revictimization over time and changes in cognitions over time. Such studies may also consider the impact of including post-MSA to assess if study trends are replicated with that time period. Indeed, studies show that post-MSA is significantly associated with MSA and pre-MSA (e.g., Creech & Orchowski, 2016), and may have a compounding effect on psychological symptoms. Finally, more research is needed to understand why men are at higher risk for greater PTC following MSA alone than women, and why this difference is attenuated when men and women have had prior military sexual victimization in addition to MSA.
There are limitations to consider. This study utilized anonymous, online self-report data. While the procedures required participants to pass the validation checks, there is no way of ensuring responses are accurate and truthful. Second, analyses were cross-sectional, which precludes causal inference. Although there was some temporality in the model given that past history of sexual victimization was compared to current psychological symptoms, it is possible that the direction of associations may actually be in the reverse direction, such that one’s PTC may influence one’s risk for sexual revictimization. Third, the sample was limited to post-9/11 era service members and veterans and results may not generalize to military populations who served in previous eras. The sample demographics do not necessarily reflect the overall demographics of the US military. The current sample also showed a majority representation of Army service members/veterans, whereas the military shows a more equal distribution across branches (Department of Defense, 2020). The greater representation of Army soldiers may be due to the increased risk for MSA in the Army versus other branches (see meta-analysis, Xue et al., 2015). The sample was also homogenous in terms of gender identity. Research shows that gender identities other than cisgender are at greater risk for sexual victimization and more severe mental health outcomes (e.g., Schuyler et al., 2020). We also were unable to determine if participants’ pre-MSA was during childhood or if it occurred during adulthood but before entering the military. Research shows that trauma exposure earlier in life relative to later in life is more detrimental to one’s mental health (e.g., Dunn et al., 2017). Whereas all participants reported a history of MSA and were asked to respond to questionnaires as it related to their MSA experience, MSA might not have been their index trauma.
Prior studies on MSA have either been restricted to women samples (e.g., Blais, 2020; Blais et al., 2020, 2022; Creech & Orchowski, 2016) or had a small sample of men with MSA (e.g., Tannahill et al., 2021). By having a larger sample of men with a history of MSA, the current study was able to test whether the relationships between revictimization experiences, PTC, and PTSS varied by gender. Moreover, our research highlights the pervasive nature of revictimization and the critical role of PTC as a potential driver of symptoms following revictimization among MSA survivors.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605221127211 – Supplemental material for Posttraumatic Cognitions Differ Between Men and Women after Military Sexual Assault Revictimization in Their Contribution to PTSD Symptoms
Supplemental material, sj-docx-1-jiv-10.1177_08862605221127211 for Posttraumatic Cognitions Differ Between Men and Women after Military Sexual Assault Revictimization in Their Contribution to PTSD Symptoms by Hallie S. Tannahill, Tyson S. Barrett, Alyson K. Zalta, Melissa Tehee and Rebecca K. Blais in Journal of Interpersonal Violence
Footnotes
Disclosure Statement
The authors have no conflicts of interest to disclose. The views expressed herein are those of the authors and do not represent official views of the institution at which the authors are employed. Data available upon request from the authors. The authors do not wish to make any acknowledgements.
Diversity Statement
Prior studies on MSA have either been restricted to women samples or small samples of men. The current study utilized a large sample of men with a history of MSA. A limitation is that the current sample was homogenous in terms of gender identity and sexual orientation. Research shows that gender identities other than cisgender and sexual orientations other than heterosexual are at greater risk for sexual victimization and more severe mental health outcomes. Future research should consider targeted recruitment approaches to better capture the experiences of individuals who identify as part of these groups.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: Funding for this study was provided from the Emma Eccles Jones College of Education and Human Services of Utah State University and the Department of Psychology at Utah State University.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.