
Abstract
Intimate partner violence (IPV) is a challenge in Brazil. The country holds one of the highest rates of femicide in the world, most of which are preceded by IPV. We conducted a cross-sectional study with 34,334 women, aged 18 to 59 years, from the 2019 Brazilian National Health Survey to analyze the prevalence of IPV and its subtypes among the Brazilian adult women in the last 12 months, encompassing their health consequences and the use of health services resulting from IPV. We also used logistic regression models to estimate the association of sociodemographic characteristics and self-perceived health status with IPV. The prevalence of IPV among Brazilian adult women in the last 12 months was 7.6% (95% confidence interval [CI] [7.0, 8.2]). Women aged 18 to 39 years, not married, and with income of up to 1 minimum wage (MW), had higher odds of suffering IPV. Among those who reported health consequences due to IPV, 69% reported psychological consequences, and 13.9% sought health care, mostly in primary or secondary health care services in the Brazilian Unified Health System (41.9%). Regarding the self-perceived health variables, women who reported eating problems (odds ratio [OR] = 1.29; [1.01, 1.65]), lack of interest/absence of pleasure (OR = 1.41; [1.11, 1.79]), depressive feelings (OR = 1.39; [1.03, 1.88]), feeling of failure (OR = 1.75; [1.36, 2.24]), and suicidal thoughts (OR = 1.73; [1.25, 2.41]) had greater odds of reporting IPV compared to those who did not report these same perceptions. The results show that younger, divorced or single, low-income women with eating problems and mental health disorders were more likely to suffer IPV. IPV often led to health problems, and many abused women sought support from public health services. Health professionals must be trained to identify and care for these women, thereby acting as allies in preventing and reducing IPV.
Keywords
Introduction
The physical, sexual, and emotional abuse resulting from intimate partner violence (IPV) against women negatively impacts the health of these women and their children (Black, 2011; Guruge, 2012; World Health Organization [WHO], 2012, 2013a). The consequences of IPV for women include physical injuries, chronic pain, mental health disorders, and sexually transmitted infections (Black, 2011; Campbell, 2002; Dutton et al., 2006). IPV, as well as other forms of violence perpetrated by familiar people, can also have negative consequences on the perception of the health of victimized women (Cruz & Irffi, 2019; De Aquino et al., 2009), including reports of difficulty conducting daily activities, in addition to experiencing pain, memory loss, and dizziness, among other complaints (Ellsberg et al., 2008).
A multicenter study conducted by the WHO in 10 countries estimated that 15% (Japan) to 71% (Ethiopia) of women have suffered physical and/or sexual violence by an intimate partner at some point in their lives; while 4% (Japan) to 54% (Ethiopia) declared to have suffered it in the last 12 months (Garcia-Moreno et al., 2006). IPV against women is more prevalent and challenging in low- and middle-income countries, where there are fewer resources available to cope with the problem (Coll et al., 2020; WHO, 2021). Brazil stands out negatively in this scenario; the country is among those with the highest rates of femicide in the world (Garcia et al., 2015; Waiselfisz, 2015), a crime usually preceded by repeated episodes of IPV (Zara & Gino, 2018).
Brazil is far from reaching the fifth Sustainable Development Goal of the United Nations, which aims at gender equality, empowering women and girls, and eliminating all forms of violence against them (UN, 2015). Recently, the WHO estimated that the prevalence of physical and/or sexual IPV against adult Brazilian women, in the last 12 months, is 6% (WHO, 2021). A preliminary study analyzed data from the 2019 Brazilian National Survey of Health (Pesquisa Nacional de Saúde—PNS 2019), revealing that the prevalence of IPV in adult women was 7.6% (Vasconcelos et al., 2021).
Vasconcelos et al. (2021), however, did not analyze the consequences of IPV in women’s health, the conditions in which health services were sought/used due to IPV, nor the association of IPV with perceived health status. The PNS 2019 is the most recent version of the largest and most comprehensive health survey conducted in Brazil; the survey provides information regarding access to health services, health determinants, and the overall needs of the population, allowing for a robust analysis which helps inform health policies and actions (Malta et al., 2019; Szwarcwald et al., 2014; Vasconcelos et al., 2021). One of the first steps in reducing IPV is knowing how often it occurs, identifying its associated factors, and acknowledging the consequences it has on women’s lives. The WHO has recommended nationwide surveys to measure the impacts of violence on women and on health systems and services (Ellsberg & Heise, 2005; WHO, 2013b).
In this study, we described the prevalence of the types of IPV suffered by adult Brazilian women in the last 12 months, the consequences of IPV on their health, and the condition in which they sought health care. In addition, we investigated the association between self-perception of women’s health status and exposure to IPV to identify predictors of IPV that can help recognize abused women in health services.
Methods
Type of Study, Population, and Sample
This is a cross-sectional study using data from the PNS 2019, the largest and most recent epidemiological survey, including a representative sample of non-institutionalized people aged 15 and over, on health status, lifestyle, and access and use of health services in Brazil (Stopa et al., 2020; Szwarcwald et al., 2014). PNS 2019 used complex cluster sampling, defined from a Master Sample, in three stages of selection: (a) census tracts or aggregate of sectors – Primary Sampling Units (PSU); (b) households, selected in each PSU; and (c) residents aged 15 or over, selected by simple sampling, in each household. A total of 108,525 households were selected, of which 94,114 individuals agreed to participate (response rate of 93.6%). For this study, only women, aged between 18 and 59 years old were included, totaling 34,334 respondents. A previous study by Stopa et al., (2020) describes more information about the PNS 2019 sampling plan and data analysis.
Intimate Partner Violence, Health Consequences, and Access to Health Services
The IPV was defined based on specific questions regarding psychological, verbal, digital/technological, economic, physical, and sexual violence, as well as threat of violence, when committed by an “Intimate Partner” (Spouse/partner, Ex-spouse/ex-partner, boyfriend/girlfriend, and ex-boyfriend/ex-girlfriend). Thus, the occurrence of IPV was informed by answering “Yes” to any questions related to the types of violence practiced and attributed to the intimate partner; answering “No” to all questions informed the absence of IPV.
For analysis of IPV, the following questions were reported: “In the last 12 months, has anyone [. . .]”: “[. . .] offended, humiliated or ridiculed you in front of other people?” (Psychological violence); “[. . .] yelled at you or called you names?” (Verbal Violence); “[. . .] used social media or cell phones to threaten, offend, curse, or expose your image without your consent?” (Digital/Technological Violence); “[. . .] threatened to hurt you or someone important to you?” (Threat); “[. . .] destroyed something of yours on purpose?” (Economic Violence); “[. . .] slapped you?,” “[. . .] pushed you, held you tightly, or threw something at you intending to hurt?,” “[. . .] punched, kicked, or dragged you by the hair?,” “[. . .] tried to or in fact strangled, choked, or burned you on purpose?,” “[. . .] threatened or injured you with a knife, firearm, or any other weapon or object?” (Physical Violence); “[. . .] touched, manipulated, kissed, or exposed parts of your body against your will?”; “[. . .] threatened or forced you to have sex or any other sexual acts against your will?” (Sexual Violence).
Consequences to health as a result of IPV were defined as: consequences in usual activities (“Yes” or “No,” also applied to the following variables); physical consequences (bruises, cuts, fractures, burns, or other physical injuries); psychological consequences (fear, sadness, discouragement, difficulty sleeping, anxiety, depression, or other psychological consequences); sexually transmitted infections or unwanted pregnancy resulting from sexual violence.
The conditions in which women sought health care due to the consequences of IPV were also assessed: did they receive health care assistance (“yes” or “no”); type of health care service (private; primary or secondary public health care; tertiary public health care; other); was hospitalization required for 24 hr or more (“yes” or “no”). The respondent had to answer this block of variables considering the most serious violence suffered.
Sociodemographic Characteristics and Self-Perception of Health
Potential predictors of IPV were selected and organized, according to the contextual dimensions of the analysis:
— Sociodemographic characteristics: age group (18 to 24 years old; 25 to 39 years old; 40 to 59 years old); Race/Color (white; non-white); living with a spouse or partner; Marital status (married; divorced/separated/widow; single); education (no education/incomplete Primary Education (0 to 8 years of study); complete Primary/incomplete Secondary Education (9 to 11 years of study); complete Secondary/incomplete Higher Education (12 to 14 years of study); complete Higher Education/Post-Graduation (>15 years of study)); income (up to 1 Brazilian minimum wage (MW); from 1 to 3 MW; from 3 to 5 MW; above 5 MW). In 2019, 1 MW was R$ 998 (Brazilian Real), which was equivalent to approximately US$ 250.
— Self-perceived health status: self-rated health (Good/Very Good; Fair; Bad/Very Bad); chest pain or discomfort (variable dichotomized into “Yes” or “No,” applied to the other variables of the dimension); sleep problems; eating problems (lack of appetite or eating a lot more than usual); tiredness; disinterest/absence of pleasure; concentration problems; slowness or agitation; depressive feeling; feeling of failure; suicidal thoughts.
Data Analysis
Prevalence of total IPV and IPV types, health status resulting from IPV, and their respective 95% confidence intervals (CIs) were calculated. Logistic regression models were performed to estimate the crude and adjusted odds ratios (ORs) for the association of sociodemographic variables and self-perceived health status with IPV. All statistical analyses were performed using the Stata®16.1 software and, due to complex sampling, the sampling plan design was incorporated to correct point and variance estimates by the survey module. The data set and the questionnaire applied are available on the PNS 2019 website via the Oswaldo Cruz Foundation (FIOCRUZ) (www.pns.fiocruz.br).
Ethical Considerations
This study was approved by the National Research Ethics Commission (CONEP) of the Brazilian Ministry of Health (http://conselho.saude.gov.br/comissoes-cns/conep/). All methods were conducted in accordance with national and international ethical guidelines and regulations. The informed consent was obtained from all participants. The study was approved under number 3,529,376 (August 23, 2019) and complied with Resolution number 196/96 of the Brazilian National Health Council (CNS), guaranteeing voluntariness, anonymity, and the possibility of withdrawing their participation.
Results
Table 1 shows the sociodemographic characteristics and the health status perceived by the 34,334 women interviewed regarding IPV. Women who experienced IPV were more likely to be adults aged 25 to 39 years, living with a partner and reporting being single, having completed Secondary Education or incomplete Higher Education, and earning up to 1 MW than women who did not suffer IPV.
Sociodemographic and Perceived Health Status Characteristics of Women According to Exposure to IPV (n = 34,334).
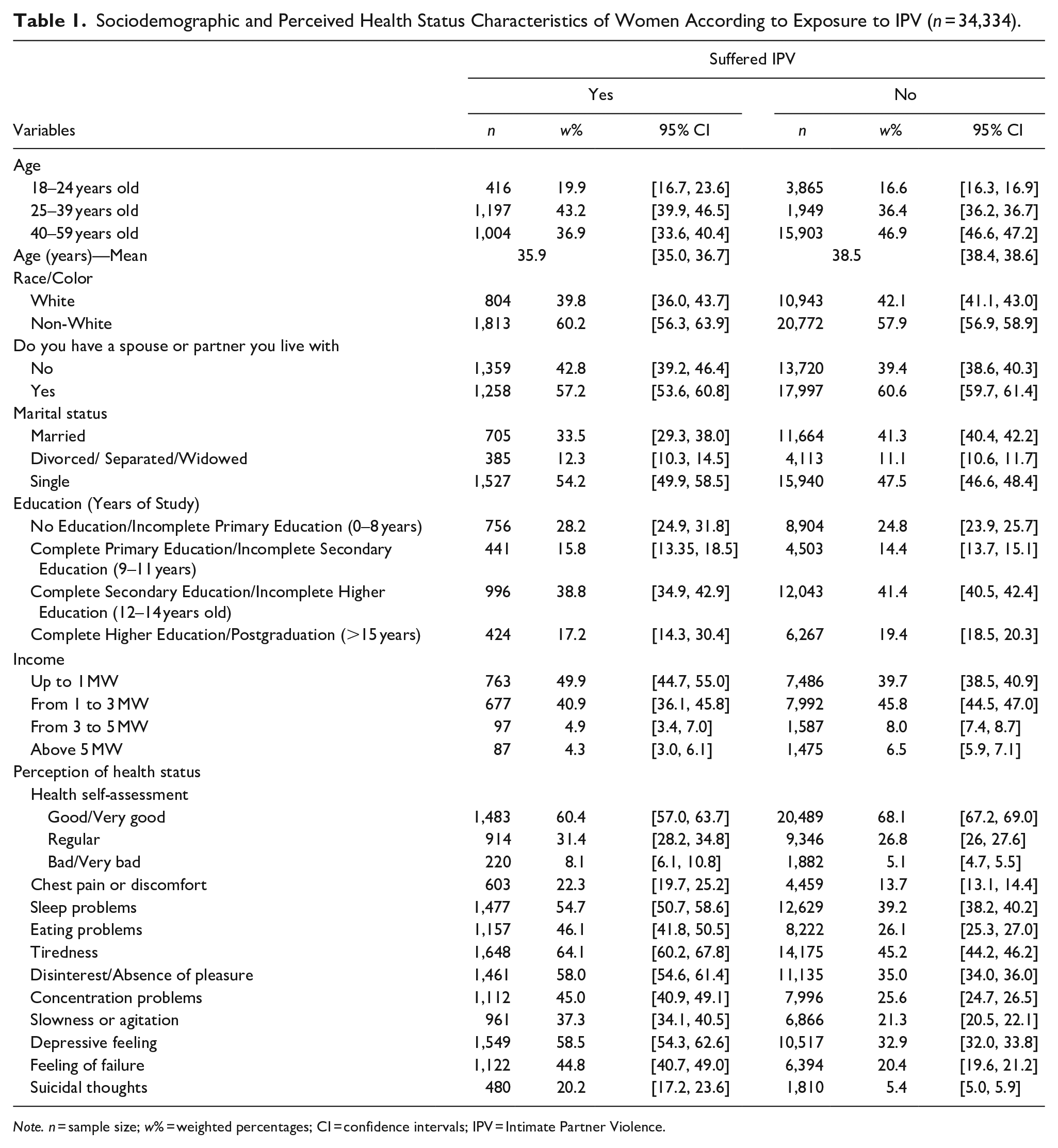
Note. n = sample size; w% = weighted percentages; CI = confidence intervals; IPV = Intimate Partner Violence.
Women who suffered IPV, when compared with those who did not suffer IPV, had a higher prevalence of bad or very bad health status (8.1% vs. 5.1%, respectively), tiredness (64.1% vs. 45.2%), feeling depressed (58.5% vs. 32.9%), disinterest/absence of pleasure (58.0% vs. 35.0%), sleeping problems (54.7% vs. 39.2%), and eating problems (46.1% vs. 26.1%) (Table 1).
The prevalence of IPV in Brazilian women in the last 12 months was 7.6%, (95% CI [7.0, 8.2]) (Table 2). Regarding the types of IPV, the most prevalent were verbal violence (6.2%, [5.7, 6.8]), followed by psychological violence (4.3%, [3.8, 4.8]), threat (2.8%, [2.5, 3.1]), and physical violence (2.7%, [2.4, 3.2]). Although less common, the prevalence of economic violence (1.5%, [1.3, 1.8] and digital violence (1.0%, [0.8, 1.2]) perpetrated by partners were also reported. The least prevalent type was sexual violence (0.7%, [0.5, 0.9]). Table 2 also shows the estimated number of adult Brazilian women who suffered IPV and its subtypes in the last 12 months: a total of 4,949,780 women.
Prevalence of Types of Violence Committed Against Women Aged 18 to 59, Perpetrated by an Intimate Partner in the Last 12 months (n = 34,334).
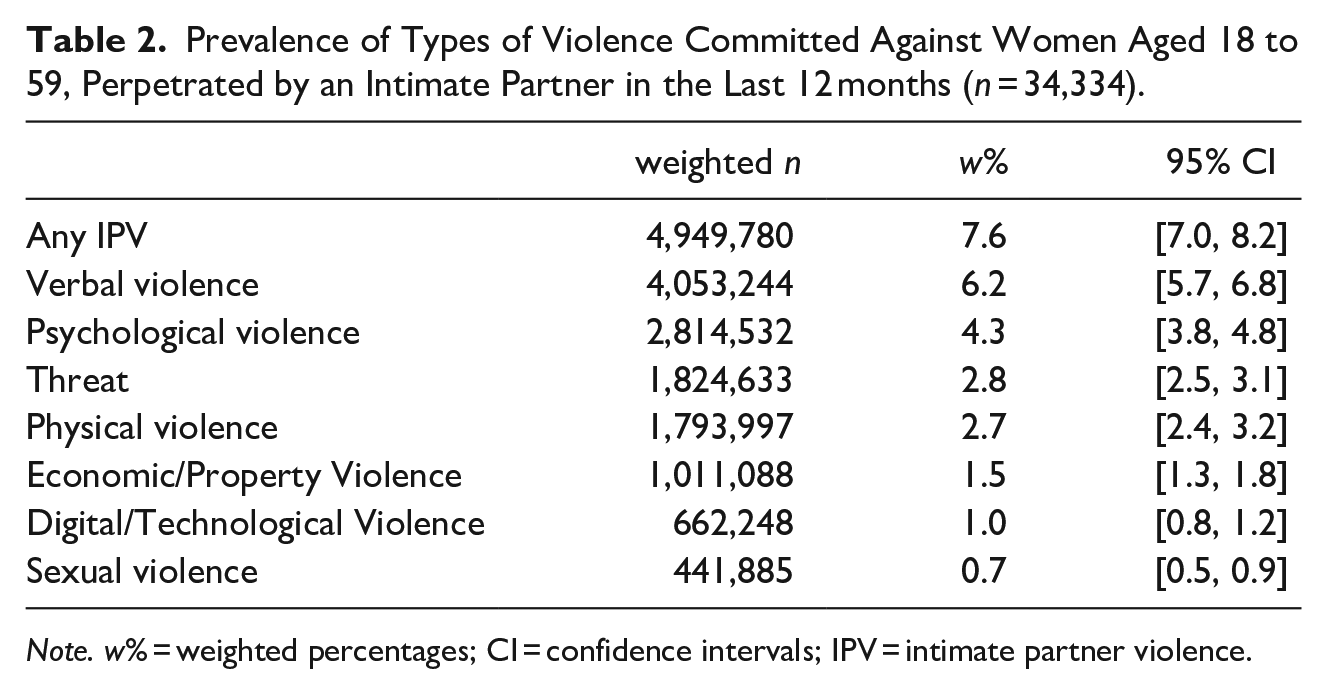
Note. w% = weighted percentages; CI = confidence intervals; IPV = intimate partner violence.
Regarding the health consequences of IPV (Table 3), 69.1% (95% CI [66.1, 72.0]) of women who suffered IPV reported psychological consequences, such as fear, discouragement, difficulty sleeping, anxiety, depression, or other psychological consequences. Among those who suffered sexual violence (8.1%, [6.0, 10.9]), reported having contracted a sexually transmitted infection or unwanted pregnancy due to sexual abuse.
Prevalence of Health Consequences and Aspects of Health Care for Women as Consequence of IPV.
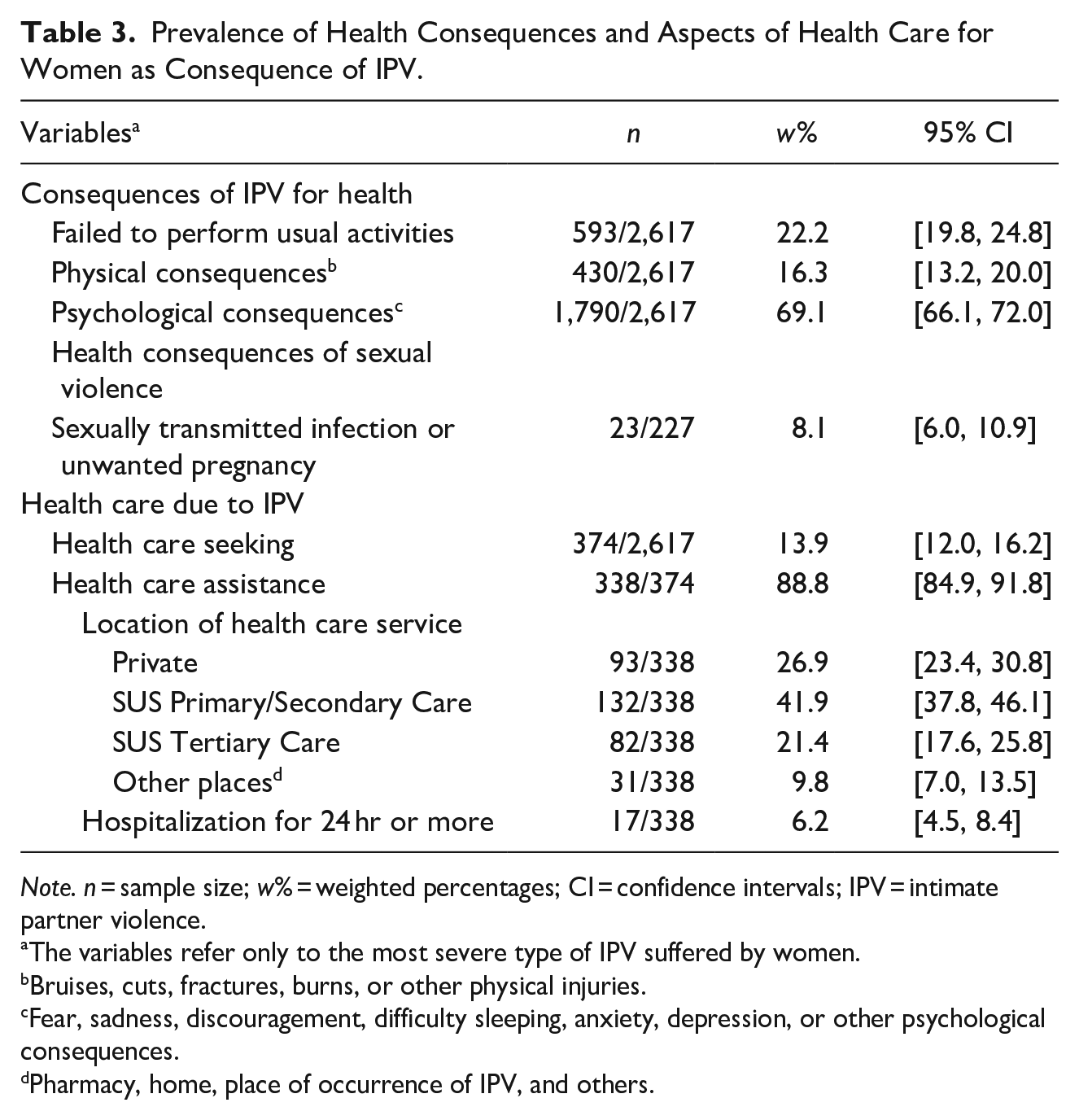
Note. n = sample size; w% = weighted percentages; CI = confidence intervals; IPV = intimate partner violence.
ªThe variables refer only to the most severe type of IPV suffered by women.
Bruises, cuts, fractures, burns, or other physical injuries.
Fear, sadness, discouragement, difficulty sleeping, anxiety, depression, or other psychological consequences.
Pharmacy, home, place of occurrence of IPV, and others.
Among women who suffered health consequences, 13.9% (95% CI [12.0, 16.2]) sought health care, of which 88.8%, [84.9, 91.8] were attended. The most sought-after place was the primary health care (PHC) or secondary care of the Brazilian Public Health System (Sistema Único de Saúde – SUS) (41.9%, [37.8, 46.1]), which along with public hospitals or public emergency units (21.4%, [17.6, 25.8]) accounted for approximately 63% of the assistance provided to victims in public health, in contrast to a minority that received care in private health services (26.9%, [23.4, 30.8]). The sociodemographic characteristics and health status perceived by women who suffered IPV according to whether they sought health care are presented in the Supplemental File. In general, women who sought health care reported a worse perception of their health status compared to women who did not seek health care.
In the multivariable logistic regression model (Table 4), women aged 18 to 24 years (OR = 1.45; 95% CI [1.01, 2.08]) and 25 to 39 years (OR = 1.46; [1.14, 1.87]) had higher odds of IPV compared to women aged over 40 years. Divorced/separated/widowed (OR = 1.64 ( [1.18, 2.27]) and single (OR = 1.38 [1.00, 1.89]) women had higher odds of IPV than married women. Women who earned up to 1 MW had greater odds of IPV (OR = 1.61; [0.99, 2.61]; p = .029) than women with an income above 5 MW. Regarding the health perception variables, women who reported eating problems (OR = 1.29; [1.01, 1.65]), lack of interest/absence of pleasure (OR = 1.41; [1.11, 1.79]), depressive feeling (OR = 1.39; [1.03, 1.88]), feeling of failure (OR = 1.75; [1.36, 2.24]), and suicidal thoughts (OR = 1.73; [1.25, 2.41]) had higher odds of IPV than women who did not report these same perceptions.
Logistic Regression for the Association Between Sociodemographic Characteristics and Perceived Health and IPV (n = 34,334).
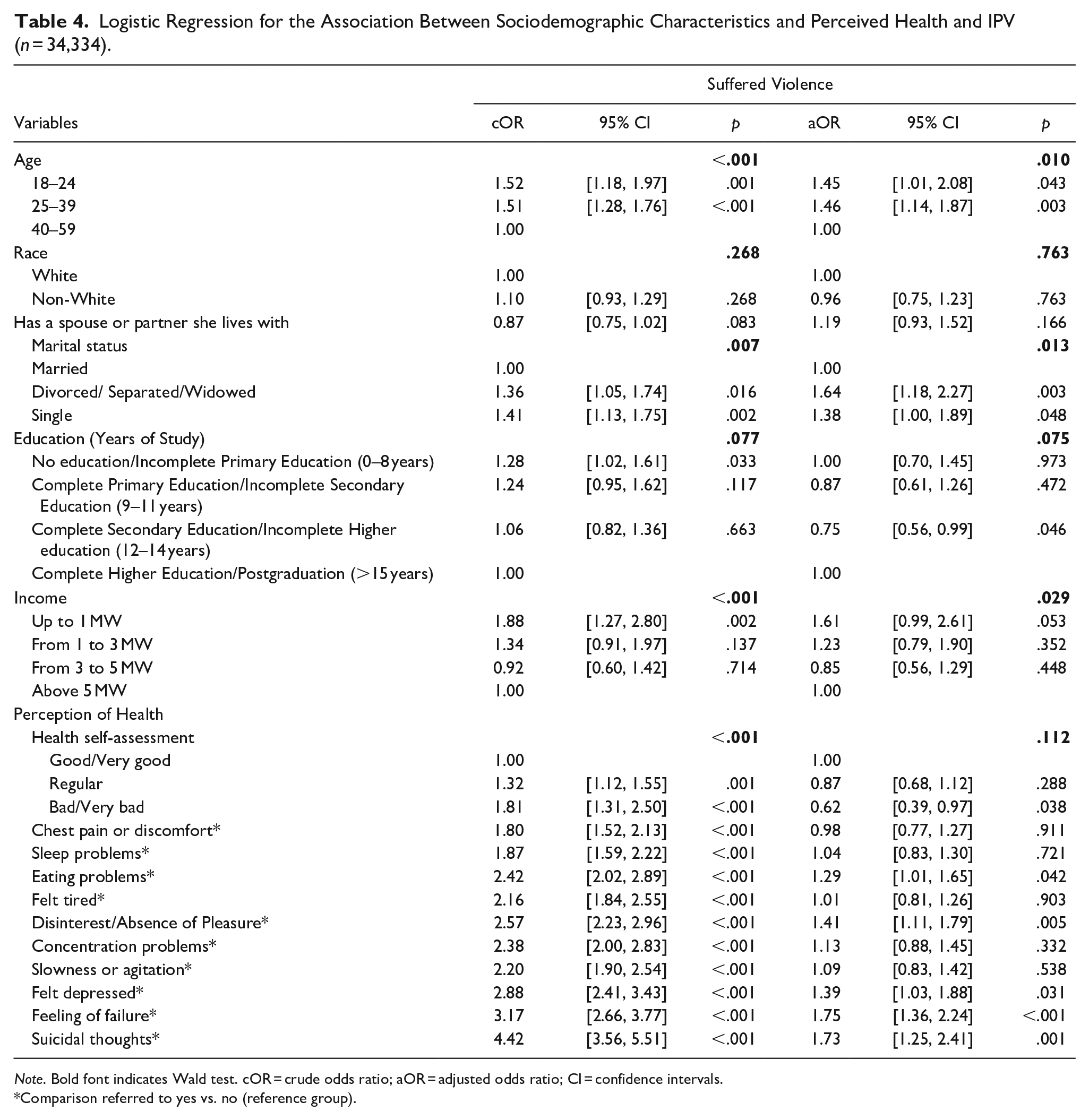
Note. Bold font indicates Wald test. cOR = crude odds ratio; aOR = adjusted odds ratio; CI = confidence intervals.
Comparison referred to yes vs. no (reference group).
Discussion
Our study includes a representative sample of the Brazilian population, and we estimate that 7.6% of adult Brazilian women have suffered IPV in the last 12 months. IPV was more prevalent in younger women (up to 39 years old), divorced or single, of low-income, with eating and mental health problems, such as anhedonia, feeling of disinterest in life, despair, failure, and suicidal ideation. The study also showed that, as a result of IPV, many women reported health consequences and sought care in health services, especially in the context of public health.
The prevalence of IPV found in our study (7.6%) corroborates the most recent estimates by the WHO (World Health Organization, 2021) and preliminary PNS analyses (Vasconcelos et al., 2021). On the other hand, it signals a possible reduction in IPV prevalence when compared with the WHO multicentric study also carried out in Brazil about two decades ago (Garcia-Moreno et al., 2006; Schraiber et al., 2007). In that study, the prevalence of IPV in the previous 12 months for Brazilian women aged 15 to 49 years ranged from 18.7% to 24.2% for psychological violence; 8.3% to 12.9% for physical violence; and 2.8% to 5.6% for sexual violence (Schraiber et al., 2007). Such differences could result from methodological differences between the studies. Another hypothesis is that these differences may be a consequence of specific laws; over the last 17 years Brazil has been making efforts to prevent IPV, with the approval of laws to prevent and restrain violence against women (Brazilian Federal Law Number 13,104, 2015; Brazilian Federal Law Number 14,188, 2021; Brazilian Federal Law Number 11,340, 2006). Brazilian legislation is gradually including other types of violence—beyond physical and sexual violence—such as threats and psychological, economic, verbal, and digital violence (Brazilian Federal Law Number 14,188, 2021; Brazilian Federal Law Number 11,340, 2006; Brazilian National Policy to Combat Violence Against Women, 2011; Brazilian Federal Law Number 13,185, 2015).
The most prevalent types of IPV in our study were verbal and psychological violence. Psychological violence, differently from physical and sexual violence, does not leave visible marks on women’s bodies. Nonetheless, psychological violence is widely recognized as a source of stress, with severe mental health consequences (Dokkedahl et al, 2022). Considering the high prevalence of psychological violence, the Brazilian government recently launched, in 2021, a law targeting this type of abuse (Brazilian Federal Law Number 14,188, 2021). Our results, therefore, support the need for specific legislations for each type of violence.
Our study also reveals unprecedented data on the prevalence of types of IPV that are less described in the literature in population-based studies, such as economic and digital violence, which are also typified in Brazilian legislation (Brazilian Federal Law Number 11,340, 2006; Brazilian Federal Law Number 13,185, 2015). Although physical violence has been less prevalent than other types of violence, perhaps due to being more easily incriminating for the offenders, the negative impacts that non-physical abuse has on women’s health and well-being should be highlighted (Stylianou, 2018; Tiwari et al., 2018). Economic violence is one of the least studied forms of violence and is often included in emotional or psychological abuse since it is a source of stress. This type of violence includes limiting or denying access to financial resources and denying access to basic needs (e.g., food, clothing, medication) (Stylianou, 2018). Digital (or technological) IPV provides a quick and easy method of harassing women via social media, GPS tracking, constant texting, or other forms of intimidation, embarrassment, and control. This type of violence has been described as more frequent due to the COVID-19 pandemic (Maftei & Dănilă, 2021). Digital violence is a type of violence that deserves to be further studied via comparative analyses before and after the pandemic; our study portrays the prevalence in the year just before the pandemic.
Our study also brings unprecedented nationwide findings on the impacts of IPV on the health of Brazilian women. Two out of three women who suffered IPV in the last 12 months reported experiencing psychological consequences from the abuse, while one in six women reported physical consequences, such as bruises, cuts, fractures, burns, or other physical injuries. Sexual violence practiced by intimate partners, including forced sexual intercourse, also had consequences for sexual and reproductive health, such as sexually transmitted infections and unwanted pregnancies for one in every 12 Brazilian women who suffered this type of abuse. These data corroborate the international literature on the impacts of IPV on women’s health (Campbell, 2002; Fanslow, 2017; Loxton et al., 2006; Plichta & Falik, 2001). Consequently, almost one in four women stopped performing their usual activities as a result of IPV. International studies indicate that IPV can increase the odds of women experiencing difficulties with daily activities by up to 60% (Ellsberg et al., 2008). That reinforces the need for public policies and specific interventions aimed at health services, including the training of health professionals to care for these women who seek health services.
Our study also identified predictors of IPV in women. In the adjusted model, younger women were almost 50% more likely to suffer IPV when compared with older ones (over 39 years old), in agreement with the international literature that postulates that the younger ages are strongly associated with increased risk of IPV in the previous year (Abramsky et al., 2011; Yakubovich et al., 2018). Possible justifications for this include that younger women are more likely to live in relationships of greater dependence on their partner (financial and related to childcare); in comparison, older women tend to have greater financial and social autonomy, providing opportunities to leave abusive relationships (Vasconcelos et al., 2021). Odds of IPV are also higher for unmarried women, including single (38% higher odds) and divorced/separated/widowed women (64% higher odds), when compared with married women. These findings are aligned with results from other countries (Yakubovich et al., 2018), in which women who lived with a partner without being formally married had an increased risk of IPV (Abramsky et al., 2011).
Differently from studies conducted in other countries (Abramsky et al., 2011; Edeby & San Sebastián, 2021; Memiah et al., 2021; Yakubovich et al., 2018), the results of our adjusted model did not demonstrate that more educated women are less exposed to IPV. In studies of other low- and middle-income countries, in addition to women with less education, lower partner education was also associated with IPV against women (Koenig et al., 2003; Semahegn & Mengistie, 2015), but the Brazilian PNS did not collect data on the education of partners.
Regarding self-reported health status, women who reported IPV were more likely to report eating problems, lack of interest/lack of pleasure, depressive feelings, feeling of failure, and suicidal thoughts. These findings agree with international studies, showing that women who suffered IPV reported having more health problems, including eating disorders and implications for mental health (Campbell, 2002; Ellsberg et al., 2008; Plichta & Falik, 2001; Wong & Chang, 2016).
As a result of abuse, women suffering IPV used health services more frequently than other women (Black, 2011; Campbell, 2002). Regarding our findings on the use of health services, only one in seven Brazilian women sought health care due to IPV. On the other hand, of those who sought care, the vast majority (9 out of 10) received care, mostly in public health services, with emphasis on primary or secondary health care services. The Brazilian PHC is free and community-based, meaning that every suburb, village, or neighborhood has a PHC Unit, which is the entry point to the Unified Health System (SUS) (Pinto & Giovanella, 2018; Fertonani et al., 2015). These Units are composed by teams of Family Health Doctors, Family Health Nurses, and Community Health Workers, who are co-responsible for their patients. The teams provide periodic consultations and home visits, creating bonds with users in a longitudinal care. Previous studies indicate the key role of these PHC teams in identifying and caring for women in situations of domestic abuse (D’Oliveira et al., 2009; D’Oliveira et al., 2020; Signorelli at al., 2018). The results of this study reinforce the importance of universal, free, and accessible public health services and the important role of PHC for survivors (García-Moreno et al., 2015; Signorelli et al., 2018). Women who have suffered violence can seek health services before seeking police or social services. If violence is identified, survivors can receive care that increases their safety and improves their health (Campbell, 2002; WHO, 2013b). Therefore, health services are privileged spaces to offer care to these women and prevent the escalation of violence (García-Moreno et al., 2015; Signorelli et al., 2018). Health professionals are considered key in supporting women experiencing violence (Ansara & Hindin, 2010), playing a decisive role in identifying IPV and supporting them (Taft et al., 2015). However, such identification is not always easy. Many women are afraid, ashamed, or lack confidence in revealing their IPV situation to professionals, even when questioned (Heron & Eisma, 2021; Shaheen et al., 2020); this causes IPV to be underrecognized by health providers (Fanslow, 2017). Therefore, professionals, especially those working in PHC, need to be aware of the profile of women most exposed to IPV and the signs and symptoms shown by them so that they can provide adequate care. According to our study, these signs and symptoms may include eating problems and mental health issues, such as lack of interest, absence of pleasure, depressive feeling, a sense of failure, and suicidal thoughts.
One of the limitations derived from the study design is that it is not possible to establish whether the exposure to violence occurred before or after the self-perceived health reports. Previous studies and theoretical reasoning suggest that health problems perceived by women are mainly the result of abuse and not its precursors (Campbell, 2002; Ellsberg et al., 2008). It is also possible that the results have a bias in IPV classification since many may not remember or even consider insults, threats, or humiliation suffered as violence. Due to the social stigma associated with disclosing victimization (Fanslow, 2017), feelings such as fear, shame, or repressed memories can decrease the probability of disclosing and discussing violence with a stranger, especially regarding sexual and intimate violence (Plichta & Falik, 2001). Similar to national health surveys from other countries (Atteraya et al., 2015), due to privacy issues and the seriousness of violence in the domestic environment, a possible limitation is that many of the respondents were not willing to report the IPV they suffered. The sample also excluded the homeless, women living in indigenous territories, and women institutionalized in places such as jails or shelters, which may contribute to an underestimation.
Diversity was partially contemplated in this study. Our sample included women from all the 27 Brazilian States, with different backgrounds regarding education, age, marital status, ethnicity, and income. Data were collected in diverse settings, using complex cluster sampling and including 108,525 households from all the 5,570 Brazilian municipalities. However, limitations concerning diversity included the fact that the PNS 2019 did not include gender identity questions and did not release data about sexual orientation, at the moment of elaborating our study. Culturally inclusive methodology was also not reported in the PNS 2019; the interviews were only conducted in Portuguese, reducing diversity by excluding women with limited fluency in this language, such as immigrants and from some Indigenous backgrounds. In contrast, our study contributes to frame diversity from a regional and global perspective. Brazil is the most populous country in Latin America, a region marked by a combination of machismo culture, colonization history, recent dictatorial regimes, and structural racism. This combo tends to naturalize different types of violence, making Latin American women more vulnerable compared to women from high-income countries.
Conclusions
The findings of our study reveal that 7.6% of Brazilian women suffered IPV in the last 12 months, among which health problems were more frequently reported, such as physical and psychological injuries and consequences for sexual and reproductive health. Although not all women who suffer IPV seek help from health services due to the endured violence, most of those who do, seek support from the SUS, especially in primary or secondary health care services. Younger, divorced or single, low-income women with eating and mental health problems were more likely to experience IPV. Training health professionals to identify and care for women who suffered IPV is an important step toward the prevention and reduction of violence against women.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605231155141 – Supplemental material for Panorama of Intimate Partner Violence Against Women in Brazil and its Association With Self-Perception of Health: Findings From a National Representative Survey
Supplemental material, sj-docx-1-jiv-10.1177_08862605231155141 for Panorama of Intimate Partner Violence Against Women in Brazil and its Association With Self-Perception of Health: Findings From a National Representative Survey by Marcos Claudio Signorelli, Felipe Granado de Souza, Raimundo Valdemy Borges Pinheiro Junior, Juliana Valente, Solange Andreoni, Leandro Fórnias Machado de Rezende and Zila Van Der Meer Sanchez in Journal of Interpersonal Violence
Footnotes
Author Contributions
MS conceived the study, collaborated with the analyses, drafted the introduction and discussion, and critically revised the text; FS led the analyses, drafted the results and critically revised the text; RP Jr collaborated in the analyses, drafted the abstract and methods, and critically revised the text; JV collaborated with the analyses, drafted the conclusion and critically revised the text; SA conceived the statistical design, supervised the analyses and critically revised the text; LR supervised the analyses and writing of the article and critically reviewed the text; ZS supervised the analyses and writing of the article, structured the discussion axes and critically revised the text. All authors read and revised the text incorporating significant contributions to the manuscript. The team met weekly for 3 months to discuss the methodological design, conduct the analyses and discuss the results. All approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.