
Abstract
Few bystander intervention trainings programs have evaluated behavioral outcomes in previously trained upper-level undergraduate students. Rigorous study designs are necessary to understand how multi-topic programs influence student outcomes to intervene against sexual violence, racism, and high-risk alcohol situations. A single-session bystander training for emphasizing communication strategies was developed for juniors and seniors on a private, Midwestern college campus. The training addressed sexual violence, racism, and high-risk alcohol situations and was evaluated using a randomized waitlist-control design in student-housing units. Online Qualtrics surveys were completed by 101 student participants (57 in the intervention group and 44 in the control group). Students responded to nine harm scenarios involving sexual violence, racism, and high-risk alcohol situations at baseline and 7 weeks follow-up. Between-group changes in scores were compared to determine the effect of the program on students’ (a) readiness to intervene; (b) confidence to intervene; (c) bystander behaviors among students who witnessed actual or potentially harmful events; and (d) bystander reports of their experiences. Qualitative analysis assessed how the program influenced the use of positive verbal communication strategies. Program effects increased positive bystander experiences when helping someone who had too much to drink and needed assistance. Over time both groups reported increased confidence levels to intervene when someone intoxicated was being isolated with sexual intent. There were no further significant findings in readiness, confidence, behaviors, or other experiences, though some positive nonsignificant trends emerged. The program demonstrated little efficacy. Results suggest opportunities to improve bystander outcomes in low-risk primary prevention situations and racist scenarios, suggesting that targeted intervention of these outcomes may be useful when developing programming with previously-trained students. As universities expand prevention work beyond the first year, lessons learned may help inform multi-year programming across health topics to prevent harm and create healthier college campuses.
Racism, sexual violence, and high-risk alcohol use are common harmful behaviors on university campuses (Ash et al., 2020; Cantor et al., 2020; Carey et al., 2016; Daigle et al., 2008; Karjane, 2005; Lopez, 2005; Rankin & Reason, 2005). Systematic reviews indicate that experiencing sexual and racial violence and engaging in excessive alcohol use yield multiple negative costs to the health and well-being of students, including academic failure, mental health disorders, physical injuries, mental trauma, reproductive health concerns, increased suicidality, and mortality (Basile et al., 2011; Carter et al., 2017; Hanson et al., 2020; Iconis, 2014; Parrish & Ryan, 1996; Turchik & Hassija, 2014;). 1
Bystander intervention is one approach college professional staff use to address these health outcomes. The term bystander refers to an individual who is present or witnesses a situation, but who is not the one directly involved as a target or perpetrator and chooses to step in and help others (Banyard, 2008; Banyard et al., 2007). Training in bystander intervention aims to increase behaviors that interrupt undesired outcomes such as sexual violence, racism, and alcohol-related harm. Many training programs are based on the landmark five-step model to explain the bystander process by Latané and Darley (1970): (a) notice an event; (b) interpret that intervention is appropriate; (c) take responsibility for action; (d) decide how to help; and (e) take action and intervene (Burn, 2009; Nelson et al., 2011).
The literature on bystander intervention has focused primarily on intervening against sexual violence. Four systematic reviews have found positive outcomes of bystander training against sexual violence in college populations, with meta-analyses demonstrating positive small to moderate effects of training on bystander attitudes or behaviors (Jouriles et al., 2018; Katz & Moore, 2013; Kettrey & Marx, 2019; Mujal et al., 2021). Literature on bystander anti-racism is emerging. It is defined by Nelson and Dunn (2011) as “action taken by a person or persons (not directly involved as a target or perpetrator) to speak out about or to seek to engage others in responding (either directly or indirectly, immediately, or at a later time) against interpersonal or systemic racism” (p. 265). Two trainings that directly confront racial prejudice found that participants of various racial backgrounds increased bystander behaviors after training, suggesting this approach may help college campuses address interpersonal forms of racism (Bozeman, 2015; Lawson et al., 2010). Lastly, literature on alcohol-related bystander intervention is rare, as trainings primarily address individual drinking behaviors; however, some programs incorporate a component on helping friends with alcohol poisoning or those at risk of other adverse consequences (Boekeloo et al., 2009; Fasone, 2016). Few studies have evaluated whether these trainings increase bystander behaviors. However, data suggest that students actively engage in helping behaviors around alcohol; Oesterle et al. (2018) found that only 14% of college students reported they had never helped someone with alcohol poisoning, primarily because they hadn’t been in a situation to assist.
While bystander training programs are frequently focused on one topic, some programs aim to build bystander skills and confidence simultaneously across various topics, such as the STEP UP! Program from the University of Arizona/National Collegiate Athletic Association (NCAA) (University of Arizona, 2008). However, no studies known to the authors have used an experimental design to assess differences in bystander training outcomes after multi-topic programs with students who have already received training in earlier college years. Subsequently, it is unknown whether multi-topic bystander programs effectively build skills across topic areas.
The pilot study described in this paper assesses a multi-topic bystander intervention training using a randomized control trial among college juniors and seniors. This training was provided to upper-level students who had been previously trained in bystander intervention, with the rationale that it could be overwhelming to tackle multiple topic areas in one session without any previous training. While most single-session programs are considered insufficient dosage for behavior change (Nation et al., 2003), this program was configured as a session situated in a multi-year effort. It is unclear how the accumulation of numerous one-time sessions offered over multiple years may impact college students. Since single-session programming is more feasible for universities, determining the multiplicative effect of cumulative one-session programs can evaluate prevention work as it commonly happens in practice. With few interventions developed specifically for previously trained students, this research may inform recommendations for upper-level undergraduates.
Bystander Program Description
The TAKES ACTION program operates with the belief that “the entire campus community has a vital and valuable role to play in preventing acts that violate the basic dignity of an individual,” and that this can be accomplished by training potential bystanders to prevent or intervene in violent and unhealthy situations (Staff, personal communication, 2018). The name is an acronym, found in Table 1. TAKES ACTION was first developed and implemented at a private Midwestern university by student services staff and campus police. It was implemented with first- and second-year students from 2011 to 2016 and received positive process evaluation results in a post-test only one-group design (Staff, personal communication, 2018). After this time, changes were made to the prevention programming on campus, so that students received other evidence-based bystander training in their first and second years. TAKES ACTION was updated with more current content, video clips, scenarios related to racism, and additional time to address more advanced bystander scenarios in an upper-level undergraduate audience. Without existing multi-topic evidence-based programs available for juniors and seniors, it was deemed most appropriate by staff to adapt TAKES ACTION, since it was already a multi-topic training and had been well received on campus over multiple years of implementation.
The Theoretical Orientation of the TAKES ACTION Program.
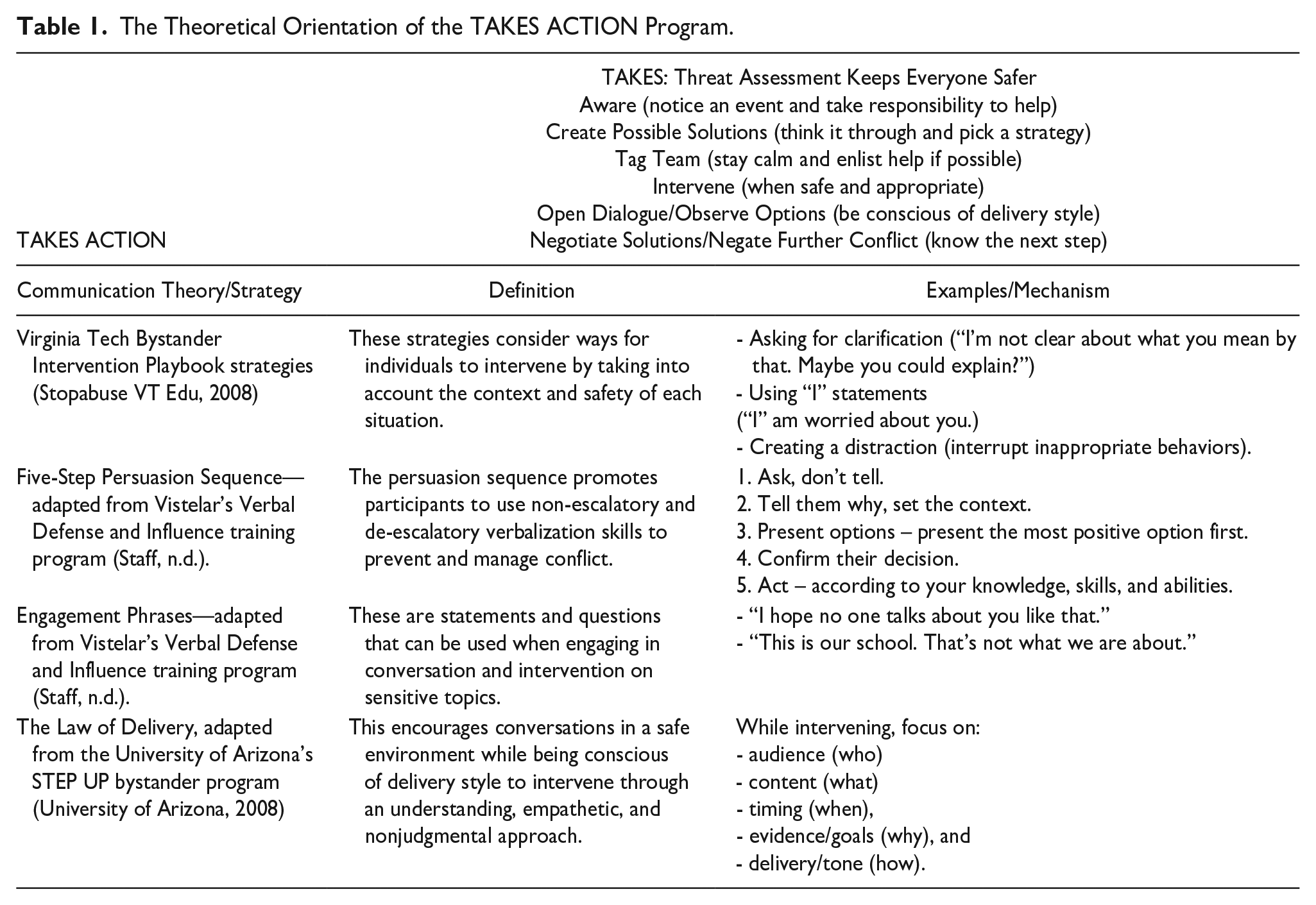
TAKES ACTION is a 90-min one-session program implemented by trained peer facilitators that aims to increase bystander behavior against sexual violence, racism, and high-risk alcohol outcomes among juniors and seniors (who have already received prevention programming in bystander education, sexual violence, and alcohol awareness). Peer facilitators were part of a paid and trained cohort who were selected through an application process and received continuous training to implement numerous wellness programs on campus. The three topic areas of sexual violence, racism, and alcohol were selected by staff as priority areas for intervention on their campus. The program is based on Latané and Darley’s (1970) five-step bystander model and multiple communication strategies described in Table 1. The Integrated Model of Behavioral Prediction was further used to understand underlying mechanisms leading to bystander intervention behavior against harm scenarios in this population and is described and evaluated elsewhere (Hennessy, 2020). General fidelity checklists suggested that the program was implemented overall as intended, with all four main components of the program covered in each session: theory, model, strategies, and scenarios.
The Research Aims
The goal of this pilot study was to assess the outcomes of a single-dose multi-topic bystander intervention training in upper-level undergraduate students who had received previous training. Four research questions comprised this aim: Does the TAKES ACTION program (a) increase student readiness to intervene in bystander situations; (b) increase bystander behaviors and improve experiences intervening; (c): increase participant confidence to intervene; and (d) influence the use of positive verbal communication strategies? The goal of the program was to increase positive bystander outcomes in each of nine scenarios that assess these four questions, further described in the methods below.
Methods
Setting and Participants
Junior and senior college students at a private, Midwestern university were recruited from three student-housing buildings consisting of 520 student residents. All were recruited to participate in the study, and 209 baseline surveys were started. Surveys were excluded for having a completion rate of 45% or less (n = 14), not providing identification as a junior or senior (n = 10), living outside of the building (n = 2), having a duplicate response at baseline based on anonymous code/demographics (n = 6), completing only a baseline measure during a follow-up period as part of the waitlist-control group (n = 13), or missing a matching follow-up survey to a baseline survey using anonymous participant-created ID codes (n = 63; 62% of the 164 students included at baseline were retained to follow-up). All remaining 101 participants had surveys with response rates of 99% or higher; this final sample represented 19% of eligible students of the population in the three buildings.
Procedures
From the sample of juniors and seniors residing in the three housing buildings, participants were randomly assigned to receive the program TAKES ACTION at the beginning of the 2019 Spring semester (the intervention group) or at the end of the semester (the waitlist-control group). For the assignment, participants were first stratified by building and then clustered into floors or combinations of floors with low sample sizes. Study recruitment included flyers hung in housing buildings and delivered to student mailboxes, personalized emails to students by campus prevention staff, and in-person recruitment by the researcher. In-person recruitment occurred in residence hall lobbies in the hour before each session; students who were entering or exiting the building were reminded of the study and invited to attend the upcoming session or the next session available based on the study assignment of their housing floor. Students were required to attend the program to register for future classes but were given the option to participate in the study. Participants completed an online consent and survey at baseline and 7 week follow-up in Qualtrics. Surveys were anonymous and were matched using personal identification codes. Separate tracking was used to provide students with incentives. Participants received a $10 gift card to complete a pre-survey and a $10 gift card to complete a follow-up survey. Referrals for sexual assault and campus services were provided. All study procedures were approved by the Institutional Review Board of the university where the study took place.
Measures
Demographics and training
Demographic data were collected on class standing/grade, gender, Hispanic ethnicity, race, U.S. citizenship status, religious affiliation, sexual orientation, year of enrollment at the university, and race-related training (having taken a class or in-depth training on race or racism). Questions mirrored those collected at the university.
Experiences relevant to sexual violence
Sexual violence was assessed with an adaptation of the sexual abuse subscale of the Conflict in Dating Relationships Inventory (CADRI), which includes mirrored questions about victimization and perpetration and is supported as a research-based measure of abusive behavior (Wolfe et al., 2001). The four items (forced sex; threatened sex; forced kissing; and forced sexual touching) were combined to create binary scores to indicate any victimization and any perpetration. Students were also asked about knowing a victim or perpetrator of sexual violence (Hoxmeier, 2015).
Alcohol use
Students were asked about alcohol use and binge drinking with questions from the Youth Risk Behavior Surveillance System using the following variations (Youth Risk Behavior Surveillance System, 2018): “During the past 30 days, (a) on how many days did you have at least one drink of alcohol?” And a follow-up for women “(b) on how many days did you have 4 or more drinks of alcohol in a row, that is, within a couple of hours?” For men this was changed to 5 or more drinks. Responses included “0 days,” “1 or 2 days,” “3 to 5 days,” “6 to 9 days,” “10 to 19 days,” “20 to 29 days,” or “All 30 days.”
Bystander intentions and behaviors
Nine brief harm scenarios related to sexual violence (n = 3), racism (n = 3), and unhealthy alcohol outcomes (n = 3) were presented in short statements to students (see Supplemental Appendix Table 2). These harm scenarios were adapted from the literature and portrayed low-risk, medium-risk, and high-risk statements corresponding to McMahon and Banyard’s (2012) nomological model of low-risk primary prevention (addressing violent and coercive language), high-risk primary prevention (addressing potential harm to an individual), and secondary prevention scenarios (interrupting harm as it is happening) (Hoxmeier et al., 2018; Krieger et al., 2005; Mäkelä & Maunu, 2016; McMahon et al., 2011, 2017). This measurement strategy allowed for the assessment of changes in each scenario. As part of a participatory design, program implementers assisted in selecting the specific scenarios used for evaluation.
To assess bystander intentions, students were asked “If you were to encounter this situation, what would you be most likely to do?” and presented with eight categorical options including (a) “go along with it (agree, laugh, etc.)”; (b) “nothing”; (c) “say something”; (d) “actively intervene (i.e., protect the person that could be harmed, stop the aggressor)”; (e) “use body language (i.e., silent stare of disapproval)”; (f) “create a distraction”; (g) “go and get assistance from someone else”; or (h) “other.” Bystander response options were adapted and informed from Hoxmeier et al. (2020) and Moisuc et al. (2018). For each harm scenario, “nothing” and “go along” were merged to represent no intention to intervene (0) and all other strategies were combined to represent a positive intention to intervene (1).
To assess bystander behaviors, students were asked if they had witnessed each of the nine harm scenarios since starting at the university. If witnessed, they were asked the number of times they witnessed the harm scenario in the past 6 weeks and the number of times they intervened as a bystander. For those who reported witnessing a harm scenario at least once since starting at the university, the following question was provided: “During a time when you were in this situation, what did you do?” Participants received the past tense version of the same items (a) through (g) provided for intentions. For each harm scenario, “nothing” and “went along” were merged (0 = no intervention) and all other strategies were combined (1 = intervention).
Low readiness to intervene
Two variables were created to assess readiness to intervene. (a) A binary intentional low readiness-to-intervene variable was created for any respondent who selected “I’m not sure what I would do” in at least one of the nine intention scenarios (hypothetical scenarios) at baseline and follow-up (“low intentional readiness” or “high intentional readiness”). (b) A binary behavioral low readiness-to-intervene variable was created for any respondent who selected “I wasn’t sure what to do” in at least one of the nine behavior scenarios (actual scenarios) witnessed at baseline and follow-up (“low behavioral readiness” or “high behavioral readiness”).
Bystander helpfulness and personal experience
Across the nine items, using the same singular scenario that students selected to report past bystander behavior, participants answered questions using a 7-point Likert scale: (a) “How helpful do you believe your response was in addressing the comment or action?” From “1” (harmful) to “7” (helpful); and (b) “How would you describe your personal experience as a bystander in this situation?” From “1” (negative) to “7” (positive). Questions were adapted from the Sexual Assault Bystander Behavior Questionnaire (Hoxmeier, 2015).
Bystander confidence
After selecting the intended strategy to intervene in each of the nine bystander intention questions, participants answered the following question adapted from Hoxmeier (2015), “How confident are you that you could take the action you selected/described?” From “1” (not very confident) to “7” (very confident).
Qualitative measure: Verbal communication strategies
After students selected the multiple-choice option for what they would do for intentions, and what they actually did for behaviors, they were asked to write a short statement indicating what they would say or actually said, respectively. A team of four graduate and undergraduate students used a combination of deductive and inductive coding to code data for the communication strategies taught in the program. Deductive coding was initiated with a codebook that corresponded to the communication strategies taught in the program. Inductive coding was necessary to modify codes and to add new codes to accurately describe the responses of students that were not captured from the deductive codebook (see Qualitative analysis for more details).
Analysis
Quantitative analysis
Quantitative data were analyzed in STATA 15.1 and checked for missingness and outliers. Fewer than 5% of data were missing and further imputation methods were not pursued (Jakobsen et al., 2017). Linear and logistic mixed-effects models tested for significant differences in outcome variables between the intervention and the control groups at baseline and follow-up. Linear models were fit using restricted maximum likelihood estimation to produce less biased estimates of covariance parameters (West et al., 2007).
Fixed effects in the model included the group (intervention or control), the time of assessment (baseline or follow-up), and an interaction term of the two to test the intervention effects. Covariates were included as fixed effects and included time (duration between assessments), gender, class standing/grade, and cohort status. 2 Models were estimated with respondents as the only random effect. The building of residence was excluded as a random effect since key variables of interest were not significantly related to building and random assignment distributed students between buildings within groups without significant differences.
Mixed-effect model fit statistics were assessed with the Wald chi-square statistic, and when significant, coefficients were interpreted using z-scores. Residuals were plotted and inspected to review the assumption of linear additivity. Multicollinearity was assessed in each model using the variance inflation factor to ensure that values were less than 10 for each predictor in each model (Errickson, 2019). The literature suggests a sample size of 10 to 20 observations per predictor (Errickson, 2019). Overfitting could potentially impact the results of mixed-effects models, but the model selection was based in theoretical reasoning, with predictors justified under this rationale.
Qualitative analysis
Qualitative analysis by four coders sorted open-ended comments of verbal communication strategies into predetermined categories that matched positive verbal communication strategies taught in the TAKES ACTION program. These included statements that (a) gather clarification, (b) “bring it home” by humanizing a person being demeaned or objectified, (c) use “I” statements that center personal experiences of the bystander, (d) use humor, (e) appeal to friendship to have a discussion, (f) exhibit other non-escalatory and de-escalatory verbalization skills, or conversely (g) did not use any verbal communication strategies taught in trainings (no verbal communication strategy used). 3 Coders reviewed 650 shared coding lines together, and interrater reliability was calculated on these lines using intraclass correlation coefficients (ICC). ICC estimates and their 95% confidence intervals were calculated based on a single-rater, absolute agreement, two-way random effects model (Koo & Li, 2016).
Unfortunately, the seven communication strategies sought out in responses were rare, and the original coding strategy was deemed infeasible. As a result, all positive verbal communication strategies were collapsed into one category, called “verbal engagement strategies” to assess any use of positive communication. Two additional categories were created to capture other verbal responses: “verbal disagreement” (any statement that indicated direct disagreement from the bystander, e.g., “That’s not okay” or “You shouldn’t do that.”) and “verbal other” (any other verbal statement, e.g., “Look over there.”). Even with this designation and numerous discussions among coders, interrater reliability for “verbal engagement strategies” was calculated below 0.5 and considered too poor to use via recommendations by Koo and Li (2016). Due to low reliability and few overall responses for “verbal engagement strategy” to indicate positive communication strategies, no further analysis was pursued. It was concluded that positive communication strategies were rarely used among participants.
Participation
There were 101 participants who completed follow-up surveys at approximately 7 weeks follow-up. The mean follow-up was 49.6 days with a standard deviation of 19.5 days. The sample was predominately U.S. citizens (96.04%), heterosexual students (96.04%), Christians/Catholics (72.28%), women (70.30%), and senior undergraduates (52.48%). All remaining students were junior undergraduates. The majority of students were non-Hispanic (90.10%). Students were White (69.31%), Asian (21.78%), and other races (4.95%) (comprising American Indian or Alaska Native and Black or African American), in addition to those who preferred not to respond to the question on race (2.97%) or were missing (0.99%).
Over half of participants were friends with someone who had been a victim of sexual assault (61.39%), but few identified having a friend who perpetrated sexual assault (3.96%). Over one-third of participants had a history of sexual violence victimization (35.64%), and 3.96% of participants experienced victimization in the 6 weeks prior to the baseline survey. Only one student identified as having perpetrated sexual violence (0.99%), with none having perpetrated it in the past 6 weeks. The majority of participants consumed alcohol at least once in the past 30 days (78.22%) and almost half the sample engaged in binge drinking on at least one day in the past 30 days (48.52%). While previous trainings in sexual violence and alcohol use were mandated, less than half the students had ever taken a class or in-depth training on race or racism (42.57%).
Students were randomized by housing floor before participating, resulting in 57 participants in the intervention group and 44 in the control group. Differences between demographic variables were tested between the groups using Pearson’s Chi-square test. Fisher’s Exact Test was used in cases with cells containing less than five observations. Statistical differences were found between class standing/grade (p < .001) and cohort status (p < .001). There were significantly more juniors in the intervention group than in the control group. The control group had significantly more students that started before or after their traditional 4-year cohort. No additional differences were found between groups (see Supplemental Appendix Table 3).
Results
Question 1
Does the TAKES ACTION program increase student readiness to intervene in bystander situations? A binary variable was created for any respondent that selected “I’m not sure what I would do” in at least one hypothetical scenario at baseline and follow-up (low intentional readiness to intervene). A second binary variable was created for any respondent that selected “I wasn’t sure what to do” in at least one actual scenario that they witnessed at baseline and follow-up (low behavioral readiness to intervene). The percentage of respondents who indicated being unsure was reviewed descriptively by the group over time and is visualized in Figure 1.
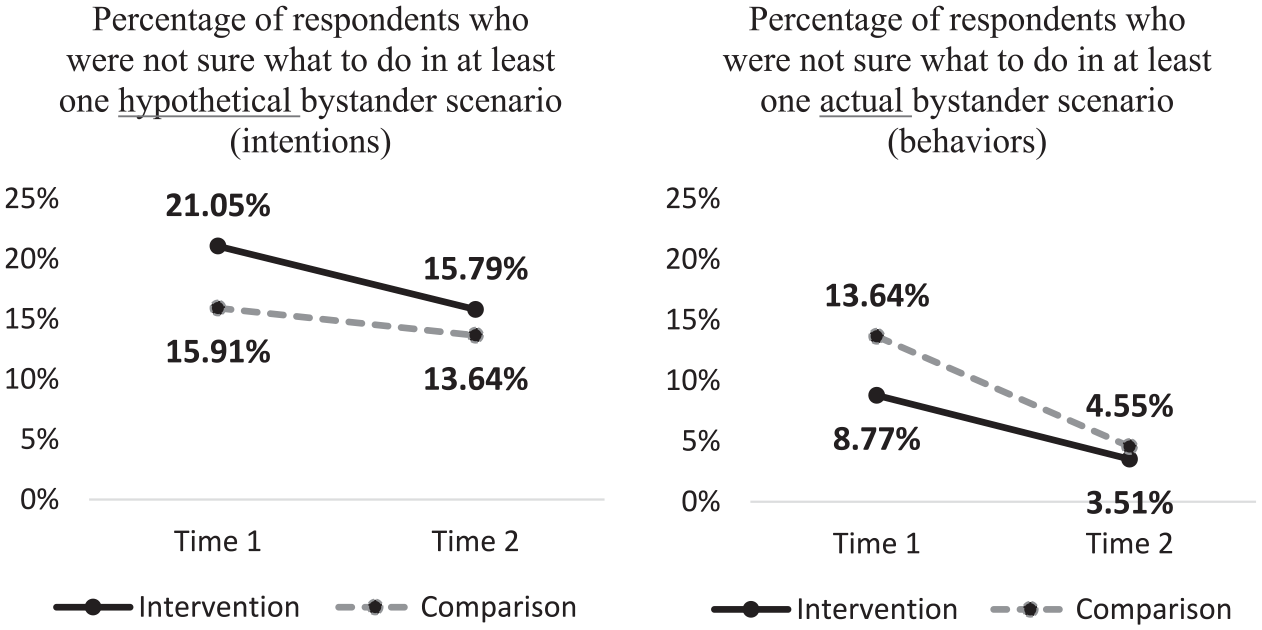
Intention and behavior readiness by group over time.
Multilevel mixed-effects logistic regression was used to test for intervention effects with covariates of time (between surveys), group, time, gender, class standing/grade, cohort status, and the interaction of time and group. Cohort status was dropped in the behavioral model as it was a perfect predictor of the outcome: 100% of students who were “not sure” what to do were in the traditional cohort group.
The overall model to test for changes in low readiness to intervene between the intervention and the control groups from baseline to follow-up was not significant for intentions (group n = 101; n = 202; X2(7) = 5.56, p = .59) or behaviors (group n = 101; n = 202; X2(6) = 4.94, p = .55). 4 The results of the models suggest no significant changes in the number of students who were unsure of what to do in at least one scenario in the intervention and control groups from baseline to follow-up after controlling for covariates, although data trended in the hypothesized direction.
Question 2
Does TAKES ACTION increase bystander behaviors and improve experiences intervening? Mixed-effects linear models were used to test differences in the bystander behavior likelihood scores, helpfulness of intervening, and bystander experiences in actual bystander scenarios with responses from at least 15 participants at follow-up. 5 Three scenarios met the sample size criteria and are analyzed below: degrading comments about women, racist comments or jokes, and someone drinking who needs assistance. The time period between the baseline and follow-up surveys was included (duration) as a covariate, along with group, time, gender, grade, cohort status, and the interaction of time and group. The marginal effects of all nine models were graphed at baseline and follow-up from the intervention and control groups in Figure 2. Model statistics can be found in Supplemental Appendix Table 4.
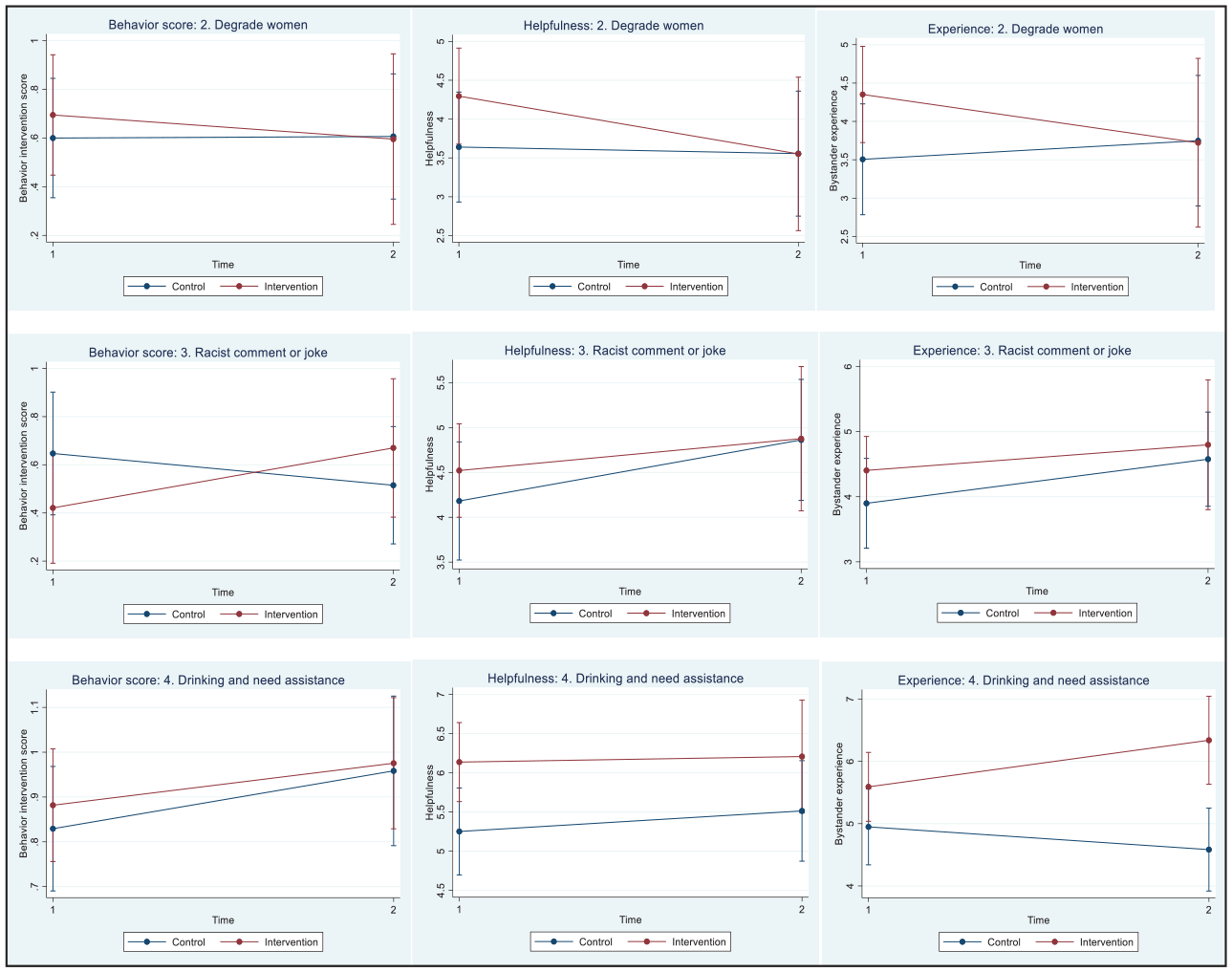
Graphs of the marginal effects of behavior likelihood scores, helpfulness, and experiences between the intervention and control groups at baseline and follow-up.
Accounting for covariates, there were no program effects on participants’ actual responses to degrading comments toward women as measured by their behavior likelihood score (group n = 36; n = 45; X2(7) = 3.30, p = .86), helpfulness of intervening (group n = 56; n = 75; X2(7) = 4.76, p = .69), or bystander experience (group n = 56; n = 75; X2(7) = 5.01, p = .66) between the intervention and control groups from baseline to follow-up.
Accounting for covariates, there were no program effects on participants’ actual responses to racist comments or jokes as measured by their behavior likelihood score (group n = 40; n = 50; X2(7) = 4.63, p = .71) or the helpfulness of intervening (group n = 64; n = 82; X2(7) = 13.03, p = .07). The model for the bystander experience was significant for racist comments or jokes (group n = 64; n = 82; X2(7) = 14.42, p = .04). The only statistically significant variable in the model was duration, which indicates that for every 0.02 decrease in the number of days between baseline and the follow-up completion of the survey, there is a one-unit increase toward a positive bystander experience, after accounting for all confounders (p = .004). This suggests that taking the follow-up survey sooner was associated with a more positive experience.
There were no program effects on participants’ responses to someone who was drinking and needed assistance as measured by their behavior likelihood scores (group n = 44; n = 54; X2(7) = 5.23, p = .63) or the helpfulness of intervening (group n = 73; n = 98; X2(7) = 5.93, p = .55). The model for the bystander experience was significant for the scenario where someone was drinking and needed assistance (group n = 73; n = 98; X2(7) = 15.16, p = .03). The one statistically significant variable in the model was the group-by-time interaction (p = .004). Since the intervention group increased from a baseline value of 5.59 to 6.34 and the control group decreased from a baseline value of 4.95 to 4.58 (on a scale of 1 to 7 where “1” = negative experience and “7” = positive experience), this suggests that the intervention had a statistically significant effect on increasing the bystander experience to be more positive when helping someone who was drunk and needed assistance, after accounting for covariates.
Question 3
Does TAKES ACTION increase participant confidence levels to intervene? Confidence levels were assessed on bystander intentions using a 7-point Likert scale, with higher values indicating higher confidence. Mixed-effects linear models were used to test differences in the levels of confidence to intervene for all nine hypothetical scenarios (intentions) using the same covariates as previous models. The marginal effects of all nine models are graphed at baseline and follow-up in Figure 3.
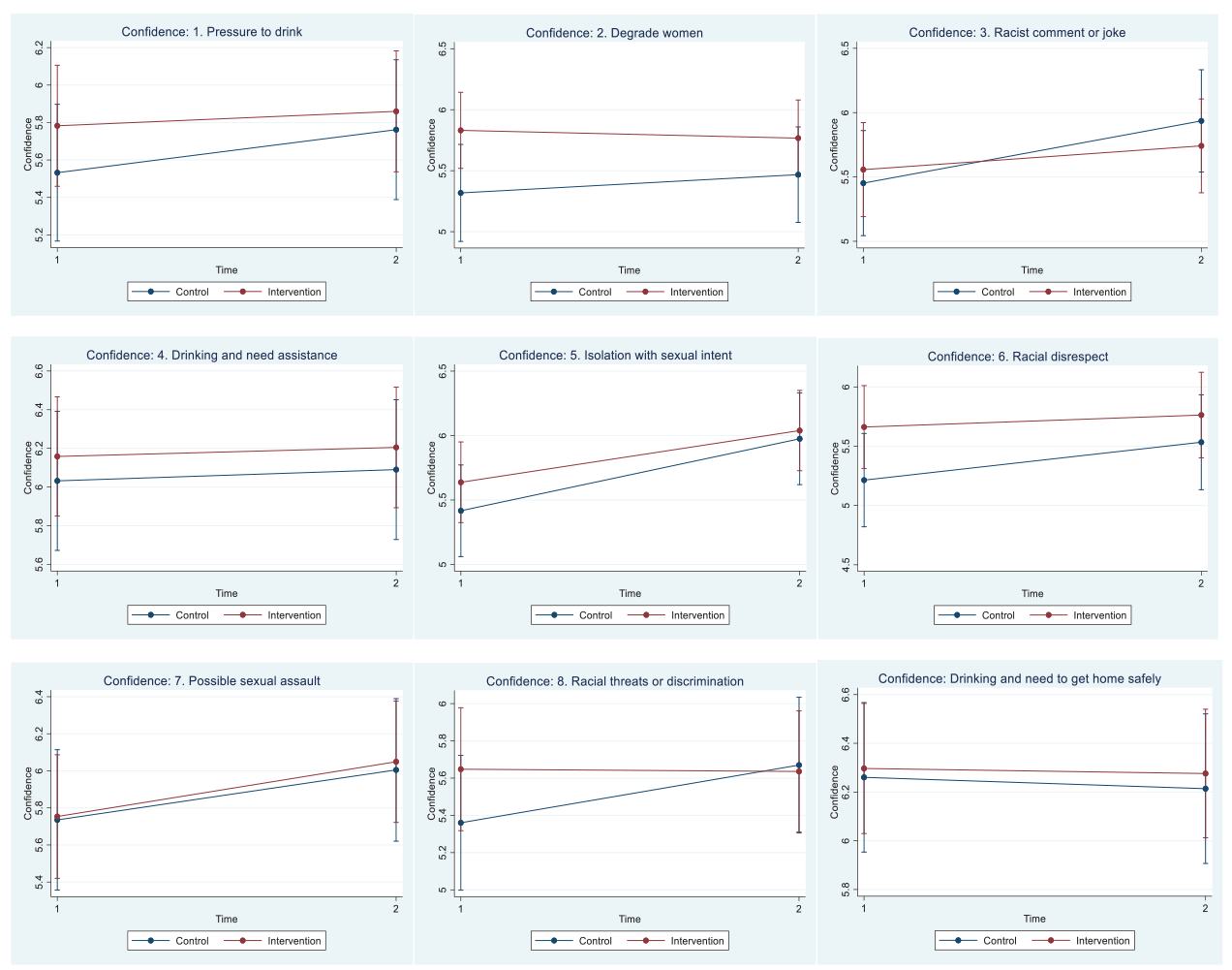
Graphs of the marginal effects of confidence levels to intervene between the intervention and control groups at baseline and follow-up.
Accounting for covariates, there were no program effects on participants’ confidence levels to intervene between the intervention and control groups from baseline to follow-up for the following scenarios: someone being pressured to drink (group n = 98; n = 188; X2(7) = 4.12, p = .77); degrading comments about women (group n = 95; n = 175; X2(7) = 9.88, p = .20); racist comments or jokes (group n = 92; n = 167; X2(7) = 9.21, p = .21); someone drinking who needs assistance (group n = 100; n = 195; X2(7) = 3.34, p = .85); racial disrespect (group n = 98; n = 187; X2(7) = 5.45, p = .61); possible sexual assault (group n = 100; n = 193; X2(7) = 8.28, p = .31); racial threats or harassment (group n = 96; n = 182; X2(7) = 7.22, p = .41); and someone who had too much to drink and needed help to get home safely (group n = 100; n = 198; X2(7) = 3.00, p = .89).
The overall model for confidence levels to intervene in a situation of isolation with sexual intent was significant (group n = 98; n = 195; X2(7) = 18.75, p = .009); the one statistically significant variable in the model was time (coefficient = 0.56, SE = 0.19, p = .004), which suggests that confidence to intervene when witnessing isolation with sexual intent increases from baseline to follow-up in the intervention and control groups together, accounting for covariates. The intervention group increased from 5.64 to 6.04, and the control group increased from 5.42 to 5.98 (1 = not very confident; 7 = very confident). See Supplemental Appendix Table 5 for model statistics.
Discussion
This pilot study of the TAKES ACTION program used a mixed-methods design to assess bystander intervention training outcomes related to sexual violence, racism, and alcohol. We employed a waitlist-control randomized trial to test the effects of a bystander program on upper-level undergraduate students with previous years of training in sexual violence, alcohol awareness, and bystander intervention. The results of this study expand our understanding of how students intervene in high-risk situations and provide evidence of how a single-session program, after previous trainings in earlier years, impacts bystander outcomes.
The TAKES ACTION bystander program significantly improved bystander experiences when helping someone who had too much to drink and needed assistance. Across both the intervention and control groups, it significantly increased confidence levels to intervene when someone was being isolated with sexual intent. The later finding may have resulted from a testing effect where taking the pretest increased confidence in this situation (Fink, 2005). A few positive but nonsignificant patterns emerged and are worth examining in a larger study sample. Fewer students reported they “did nothing because I wasn’t sure what to do” from baseline to follow-up, with more pronounced changes in the intervention group than in the control group. Positive trends also suggested that confidence levels increased in the intervention group in some scenarios. The intervention group was more likely to intervene against racist comments and jokes than the control group at follow-up. While not statistically significant, this finding suggests an emerging positive effect on willingness to intervene that is especially important given that at baseline, students intervened in less than half of situations involving racist comments or jokes.
The program improved participants’ experiences intervening in an alcohol-related scenario. On the other hand, no significant findings were found in any racist or sexually violent scenarios. Drawing upon the guiding model by Latané and Darley (1970), it is possible that it is easier to apply the communication strategies and other intervention methods from the TAKES ACTION program to high-risk alcohol situations when deciding how to help (step 4) and when actually taking action to intervene (step 5). These situations do not require a bystander to also confront oppression when helping someone who has had too much to drink, which may lead to a more positive overall experience.
The remaining findings of the study suggest that the intervention did not significantly improve confidence to intervene, experiences intervening, helpfulness of intervening, and that behaviors either did not increase or the sample sizes were too small to test differences that may have occurred. This is in contrast to previous reviews of bystander intervention with college students, which have demonstrated small to medium effects on bystander efficacy, intentions, and behaviors (Jouriles et al., 2018; Katz & Moore, 2013; Kettrey & Marx, 2019). Duration of programming and student characteristics may explain the null findings in this study compared to previous studies. Other programs have included longer sessions to previously untrained students. For example, Katz and Moore (2013) studied college students who went through an average of 140 min of bystander training while the TAKES ACTION program averaged 60 min, based on fidelity checklists. Katz and Moore (2013) also found larger effect sizes for younger and likely untrained students, in contrast with our study of later-year students with previous training. Thus, the TAKES ACTION curriculum may see greater program benefits by concentrating on advanced communication strategies and practice time, especially with students who have already received previous trainings.
While TAKE ACTIONS is based on research to promote communication strategies and the five-step model (Latané & Darley, 1970), it is also possible that the program lacked a theoretical or evidence-based background to successfully train students and modify behavior. The lack of a behavioral theory of change is common across bystander programs; a previous review found that only four of 10 bystander programs were based in theory beyond Latané and Darley’s (1970) five-step bystander model; theories that were included focused more on the dissemination of content (i.e., Theatre of the Oppressed and Diffusion of Innovation), instead of internal psychological constructs (such as attitudes) used to elicit individual changes in bystander behavior or behavioral intentions (Hennessy, 2018). Continued theoretical development and the adaptation of existing evidence-based programs are likely to improve sexual violence prevention through bystander intervention. For example, researchers have found that gender-equity and pro-feminist anti-violence approaches are essential for effective culture change, particularly efforts to address empathy, rape myths, social constructed notions of masculinity, and heteronormativity (Casey et al., 2013; Lonsway, 1996). Similarly, public education campaigns to foster a culture of racial and ethnic inclusion could exist alongside group-norming efforts to cultivate empathy and intolerance of sexism and racism within particular social contexts (e.g., schools, work, recreation) (Aboud & Joong, 2008; Nesdale & Lawson, 2011).
Furthermore, although meta-analyses of bystander intervention trainings demonstrate positive outcomes, not every program achieves significant changes in bystander behaviors (Hennessy, 2018). Previous research with youth has demonstrated that one-time, brief, interventions are not commonly effective for behavior change (Nation et al., 2003). This may be the case for TAKES ACTION, despite the desire to situate the program as a booster session within a multi-year strategy to increase bystander behaviors across health topics. More research to study this multi-year approach to violence prevention is necessary to determine the definitive impact of single sessions across collegiate years.
Results also made it difficult to assess how the program separately influenced the health topics of sexual violence, racism, and high-risk alcohol outcomes. Research from this study’s baseline data demonstrated that upper-level students were less likely to intervene against sexual violence and racism compared to high-risk alcohol situations, and they were less likely to intervene in low-risk scenarios compared to higher-risk ones (Hennessy Garza et al., 2021). These findings coincide with research showing the decision to intervene is also based on perceived level of seriousness of the offense; or, whether a racist comment or joke is deemed acceptable or normalized within peer groups (Mulvey et al., 2016). Thus, bystander intervention models would benefit from the situational skill-building and theoretical application of the interactions between group functioning, social setting, and perceived seriousness of the risky behavior or “acceptability” of microaggressions (Abbott & Cameron, 2014; Aboud & Joong, 2008; Mulvey et al., 2016).
As less than half the sample had received any formal anti-racism training through either an in-depth training or class previous to receiving TAKES ACTION, few baseline behaviors to intervene against racism suggest that earlier anti-racism bystander intervention training may be necessary to prepare students to intervene. Interpersonal racism does not occur in isolation and is embedded into a society based in systemic racism. Similar to deconstructing sexism in order to prevent sexual violence, additional programming on the effect of discriminatory behaviors, microaggressions, and the interplay between peer-level norms and societal or institutional norms is necessary to promote anti-racist bystander behaviors (Nesdale & Lawson, 2011). It is critical to improve outcomes in anti-racism bystander intervention to increase intervention not only in racist situations, but also when victims of sexual violence are students of color (where research demonstrates White students may have lower intentions to intervene (Katz et al., 2017)), and in interactions that combine sexist and racist acts of violence. Centering intersectional pedagogy in future prevention programs, especially multi-topic programs, moves us toward more inclusive bystander intervention that can more concretely address participants’ perceived obstacles to intervention across boundaries of race, ethnicity, gender, sexuality, and class. Such identities can often coalesce around peer culture and group identification (Aboud & Joong, 2008; Mulvey et al., 2016). Anti-racist education depends upon the interplay and prioritization of peer/group norms and “generic norms” (those held by a society or institution such as a school or university) (Nesdale & Lawson, 2011). Despite individual moral judgments or generic norms, prioritizing in-group identification and peer-level norms can create obstacles to bystander actions against racist talk (Abbott & Cameron, 2014; Abrams et al., 2014; Nelson et al., 2011).
Finally, qualitative analyses revealed participants rarely used positive verbal communication strategies, despite receiving two bystander intervention trainings focused on such tactics. Rather, our coding was frequently and reliably able to detect both direct and aggressive verbal responses to racist comments (i.e., “You shouldn’t talk like that” or “Shut up”). While more analysis is needed, preliminary findings suggest that students commonly use or plan to use direct verbal communication strategies. This raises interesting questions for bystander programs in general: Should programs continue to promote positive verbal strategies that students don’t naturally use? Or should they instead promote more direct responses that students use in real life, even if they may be more confrontational? This is a critical point for future research given that many bystander intervention programs, including TAKES ACTION, promote strategies for using nonaggressive verbal communication strategies such as “I” statements, asking for clarification, or humanizing victims.
Limitations
The sample size in the pilot test may not have been large enough to detect statistically significant outcomes with adequate power and was further limited by additional attrition from the inability to match a subset of anonymous IDs. A 7 week follow-up time may have been too short to detect differences between groups and further limited witnessing less common bystander situations. However, this duration was necessary to reach many graduating seniors before they left the university. Not implementing an immediate post-test may have masked outcomes that attenuated over time, but was avoided to minimize testing fatigue. There may have been spillover effects, as it is likely that students assigned to different groups by housing floor may have interacted with each other in their university housing or elsewhere on campus.
Measurement challenges may also limit the results of the study. The measurement strategy in this study was novel, as each scenario was assessed separately for each outcome of interest. However, rigorous psychometric analyses were not conducted to assess the validity and reliability of this strategy, which may influence the findings. Assessment reactivity from taking the pretest may have raised awareness of bystander situations/responses. Social desirability bias could have led to more desirable responses overall, as there are societal expectations about intervening, especially among friends and acquaintances. When asking students to share their experiences and responses to intervening, they were asked to select “a time” they witnessed a scenario, which may not represent all witnessed scenarios. While all study participants identified as women and men, our questionnaire assessed for “other” gender and provided a write-in option. To avoid the harmful practice of “othering” in our future research, we recommend the two-step question method to obtain sex assigned at birth and gender identity, which includes the prompt “I use a different term: [free text]” (National Academies of Sciences, Engineering, and Medicine, 2022, p. 117).
Finally, characteristics of the study sample due to selection bias may limit the external generalizability of the results. Results from this private university may not translate to all institutions of higher learning. Students of color and men were underrepresented in the sample and recent victims of sexual violence were likely overrepresented. A lack of racial/ethnic diversity and an underrepresentation of men are problematic in sexual violence bystander intervention research, despite the diversity found in most college campuses, and requires proactive recruitment and investment to obtain more representative samples (Hennessy, 2018; Labhardt et al., 2017).
Conclusions
This study contributes to our understanding of how cumulative single-dose bystander sessions impact student bystander outcomes across a variety of harmful situations in sexual violence, racism, and high-risk alcohol situations. Our findings suggest that a one-time session with upper-level students may influence some bystander outcomes, but further and improved programming may be warranted in upper-level college students to increase bystander behaviors and experiences. In particular, it may be helpful to expand skill-building to practice communication strategies, utilize a theory of change to guide program content, and provide more foundational training in anti-racism bystander intervention that focuses on the delicate interplay between communicative intervention strategies and maintaining interpersonal relations. In fact, a review of anti-racism programming demonstrates that there is untapped potential of bystander anti-racism to unsettle or disrupt normalized, everyday acts of racism (Nelson et al., 2011). A more holistic bystander anti-racism program might focus more on context, social norms, and interpersonal relations to help shift burdens away from the targets of racism toward bystanders who feel safe and confident intervening (Hyers, 2007).
Supplemental Material
sj-docx-1-jiv-10.1177_08862605231165778 – Supplemental material for A Multi-Topic Bystander Intervention Program for Upper-Level Undergraduate Students: Outcomes in Sexual Violence, Racism, and High-Risk Alcohol Situations
Supplemental material, sj-docx-1-jiv-10.1177_08862605231165778 for A Multi-Topic Bystander Intervention Program for Upper-Level Undergraduate Students: Outcomes in Sexual Violence, Racism, and High-Risk Alcohol Situations by Rose Hennessy Garza, Young Cho, Heather Hlavka, Lance Weinhardt, Tajammal Yasin, Sara Smith, Katharine Adler, Kacie Otto and Paul Florsheim in Journal of Interpersonal Violence
Footnotes
Acknowledgments and Credits
The lead author thanks all members of her dissertation committee for providing feedback on this study, in particular, her academic advisor and the senior author Dr. Paul Florsheim. She further extends gratitude to the three students who coded the qualitative data, the violence prevention staff, and peer educators who implemented the program, the university that hosted the study, and all the students who participated in this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was generously funded by the anonymous donors of the Joseph J Zilber Dissertation Award from the University of Wisconsin, Milwaukee.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.