
Abstract
Sexual trauma (ST), which includes both sexual harassment and sexual assault, is associated with a variety of adverse mental and physical health outcomes in military and civilian populations. However, little is known about whether certain individual or military attributes or prior experiences may modify the relationship between recent ST and mental or physical health outcomes. Data from a longitudinal cohort study of current and former military members were used to examine whether individual and military factors modify the association between recent ST and health outcomes (posttraumatic stress disorder, depression, multiple somatic symptoms, and insomnia). Results indicated that demographic (sex, sexual orientation, race/ethnicity) and military factors (service branch, service component, military separation) generally did not modify the main effect of ST on the outcomes examined. On the other hand, factors known to be protective (spirituality, social support) and risk factors (childhood trauma, combat deployment, and mental health status) did modify the effect of ST on multiple outcomes examined; notably, protective effects were diminished among those who experienced recent ST. Protective factors were associated with the lowest risk of adverse outcomes among those with no ST, while risk reduction was less among survivors of ST. Diminished impacts also were found for cumulative risk factors, with the influence of multiple individual risk factors associated with increased risk but in a subadditive manner. We conclude that the effect of recent ST on the outcomes examined was persistent in the presence of potential protective factors, but that it may be impacted by ceiling effects in combination with other risk factors.
Introduction
Sexual trauma (ST), defined as sexual harassment (SH) and/or sexual assault (SA), presents a persistent threat to the health and well-being of military members. According to the most recent Department of Defense (DoD) survey results, an estimated 28.6% of women and 6.3% of men experienced SH, while 8.4% of women and 1.5% of men experienced SA in the past year in the active component (Breslin et al., 2022). The same survey estimated 16.4% of women and 3.5% of men experienced SH, while 4.6% of women and 0.7% of men experienced SA in the past year in the Reserve component. Given the prevalence of ST, extant literature has explored the impacts of these experiences on the health and well-being of survivors. While researchers have found that ST experiences are associated with a variety of negative mental health and physical health outcomes, including posttraumatic stress disorder (PTSD; Millegan et al., 2016), depression (Millegan et al., 2016), multiple somatic symptoms (MSS; Millegan et al., 2016; Stein et al., 2004; Ulirsch et al., 2014), and insomnia (Gibson et al., 2020; Hall Brown et al., 2015), limited research exists to evaluate differences among specific subgroups that may elucidate important considerations for treatment and response.
With so many military members impacted by ST, it is imperative that health professionals treating current and former service members not only know the potential adverse health outcomes associated with ST, but also understand if certain associations are different among specific subgroups. Stress process theory (Pearlin et al., 1990) suggests multiple contextual and pre-existing factors may lead to subgroup differences in response to trauma exposure, such as SA. These include prior trauma history and access to resources, as well as individual factors. Compared to civilians, service members may experience a more homogenous context and consistent access to support resources; however, inequalities, as well as differences in access to support and coping strategies likely still exist in the military that may create subgroup differences that are important to explore to develop and refine policy and treatment recommendations for at-risk populations.
Factors That Impact Response to ST
A limited number of previous studies have examined how individual and military service characteristics may modify the relationship between ST and health outcomes in military or veteran populations. For example, Shipherd et al. (2009) reported that higher levels of ST were associated with worse perceived physical health among male Marines, while lower levels of ST were associated with worse perceived physical health among female Marines. Ziobrowski et al. (2017) reported that male veterans were more likely than female veterans to experience depression following ST. Another study of veterans demonstrated that SA during military service was significantly associated with depression among lesbian and bisexual women, but not among heterosexual women (Lehavot & Simpson, 2014).
Previous research among a general, nonmilitary population, also provides insight into which demographics may modify the relationship between ST and health outcomes. Differences by race or ethnic group are plausible given reports that women of color are less likely to seek care following ST, likely due to fear of stigma and racism (Roberts et al., 2011). While ST is more prevalent among lesbian and bisexual women than heterosexual women (Canan et al., 2019), researchers have only begun to examine whether sexual orientation modifies the relationship between ST and outcomes among currently serving military members (Trump-Steele et al., 2021).
In addition to demographic characteristics, it is plausible that other individual factors, such as spirituality, social support, mental health status (depression and/or PTSD), and childhood trauma, may modify the associations between ST and health outcomes. Ahrens et al. (2010) reported that positive religious coping was associated with higher levels of psychological well-being and lower levels of depression in a community sample of SA survivors, while negative religious coping (i.e., negative or angry feelings about God) had the opposite effect. It is unknown, however, whether this pattern holds true for military members with varying experiences of ST. Monteith et al. (2018) found that post-deployment social support moderated the relationship between deployment ST and suicidal ideation for male veterans, but not female veterans. Specifically, only male survivors of ST with low post-deployment social support had a significant risk for suicidal ideation, indicating that social support may buffer the negative effects of ST for men more than women. Moreover, evidence indicates that childhood trauma is associated with a variety of negative outcomes in adulthood (Mercado et al., 2015), though we are not aware of any research that has examined the moderating effect of childhood trauma on the association between adult ST and health outcomes among current and former military members.
Characteristics of one’s military career may modify the effect of ST on health outcomes as well. Risk of ST varies by service branch and component (Breslin et al., 2022), though, to our knowledge, no research has tested whether these differences modify the relationship between ST and health outcomes. LeardMann et al. (2013) found that combat experience during deployment is associated with ST among women. Cobb Scott et al. (2014) found that ST interacted with combat exposure to increase the odds of PTSD in female veterans, and a meta-analysis found that type of trauma (i.e., combat vs. SA) modified the association between trauma and somatic symptoms (Afari et al., 2014). However, to our knowledge, no research has extended these findings to examine if these military factors modify the associations between ST and health outcomes in service members or veterans.
The Present Study
Given the deleterious effects of ST on survivors, it is important to better understand how certain factors influence the relationships between ST and associated health outcomes. To address these knowledge gaps, we undertook an exploratory investigation of the largest ongoing military cohort study to date, the Millennium Cohort Study (Ryan et al., 2007; T. C. Smith, 2009). Specifically, we examined whether certain individual and military factors modify the longitudinal associations between ST and several health outcomes among current and former military members. Findings from this study may help to inform and advance clinical research and treatment strategies for current military members and veterans who are survivors of ST as well as inform DoD and Department of Veterans Affairs (VA) policies related to prevention and response to ST (Stander & Thomsen, 2016).
Methods
Participants
The Millennium Cohort Study was designed to investigate the short- and long-term health effects of military service. Four groups (enrollment panels) of participants were enrolled approximately every 3 to 5 years, beginning with the 2001 to 2003 enrollment cycle (n = 77,019), and followed by 2004 to 2006 (n = 31,110), 2007 to 2008 (n = 43,438), and 2011 to 2013 (n = 50,052). A fifth panel was enrolled after these analyses were completed and were not included in this study. Military participants were randomly selected from personnel files and invited to enroll in this confidential study, with oversampling of several underrepresented subgroups, such as servicewomen. Previous studies have determined the Millennium Cohort to be representative of service members and veterans (Littman, 2010; B. Smith, 2007; Wells, 2008). These four panels include 201,619 participants from all service branches and components (active duty, Reserve, and National Guard). Participants completed a confidential, self-administered survey at enrollment and were requested to complete follow-up surveys, even if they had left the military, periodically every 3 to 5 years. Surveys covered a broad scope of topics, including military and nonmilitary life experiences, and assessments of physical and mental health and behavioral characteristics. Written, informed consent was obtained from all participants at enrollment (Ryan et al., 2007).
Eligible study participants for the current study included those who completed surveys from the 2011 to 2013 and 2014 to 2016 survey cycles (n = 92,614); for the purpose of this study referred to as “baseline” and “follow-up,” respectively. All analyses excluded those who were missing recent ST status (n = 367) and covariate (n = 4) data. Further, analyses excluded participants missing the individual and military factors of interest (n = 9,518 for the PTSD and depression outcomes, and n = 9,861 for the MSS and insomnia outcomes), resulting in a study population of 82,725 for the PTSD and depression outcomes and 82,382 for the MSS and insomnia outcomes. The three factors accounting for most of the missing data were sexual orientation (n = 2,599), childhood trauma (n = 2,505), and history of combat experience (n = 2,019). The final sample size for each outcome differed after those missing a particular outcome and/or its prior history were excluded, but final sample sizes were very similar across all outcomes tested (Table 1; n = 81,675–82,340).
FDR p-Values of Interaction Terms Between Recent ST and Individual and Military Factors for Each Outcome.
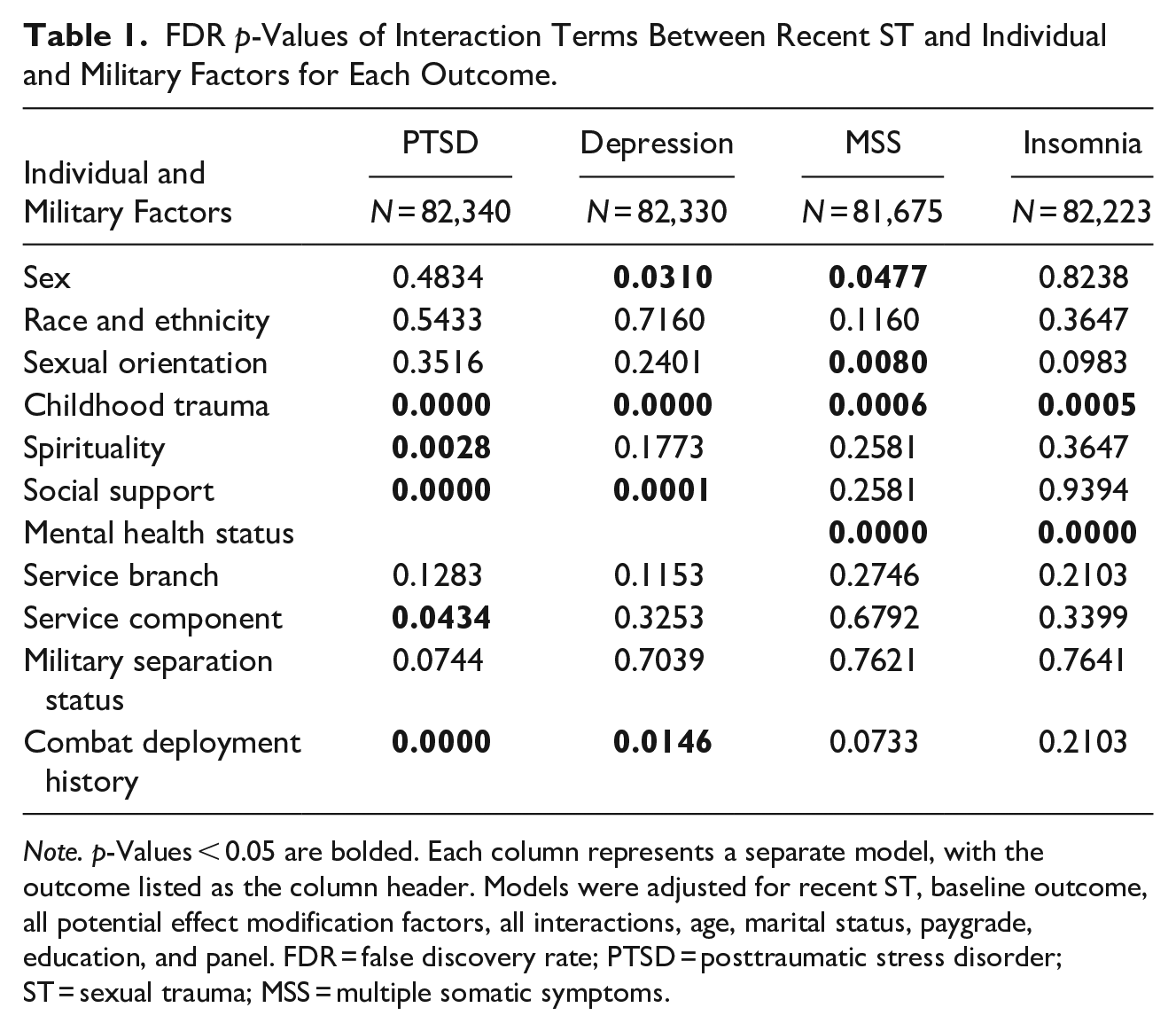
Note. p-Values < 0.05 are bolded. Each column represents a separate model, with the outcome listed as the column header. Models were adjusted for recent ST, baseline outcome, all potential effect modification factors, all interactions, age, marital status, paygrade, education, and panel. FDR = false discovery rate; PTSD = posttraumatic stress disorder; ST = sexual trauma; MSS = multiple somatic symptoms.
Measures
We evaluated four health outcomes: PTSD, depression, MSS, and insomnia in this study. Outcomes were assessed at follow-up with baseline values included for adjustment purposes. Outcome measures are briefly summarized below, with more detail in Table A1.
Posttraumatic stress disorder
PTSD was assessed using the 17-item PTSD Checklist–Civilian Version (PCL-C) based on the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV; Weathers et al., 1993). Symptoms in the last month were rated using five options, ranging from “not at all” to “extremely.” Those who endorsed “moderately,” “quite a bit,” or “extremely” on one or more intrusion items, two or more hyperarousal items, and three or more avoidance items met criteria for PTSD.
Depression
Depression was assessed using 8 items from the Patient Health Questionnaire (PHQ), to which a standardized scoring algorithm was applied (Kroenke et al., 2009; Wells et al., 2013). Those who met the DSM-IV criteria for major depressive disorder endorsed 5 or more of the 8 items as “more than half the days” or “nearly every day,” including the endorsement of anhedonia or depressed mood in the last 2 weeks.
Multiple somatic symptoms
MSS was assessed using the 15-item physical symptoms scale on the PHQ. The first 13 items (e.g., back pain, chest pain, shortness of breath) were assessed in the last 4 weeks using a 3-point Likert-type scale ranging from 0 “not bothered“ to 2 “bothered a lot” and the last 2 items were assessed in the last 2 weeks using a 4-point Likert-type scale ranging from 0 “Not at all” to 3 “Nearly every day” (Kroenke et al., 2002). Using the validated approach of Kroenke et al. (2002), a score ranging from 0 to 32 was calculated by summing the responses. For this study, MSS was dichotomized as none/low (0–9) and moderate/high (10 or higher).
Insomnia
Insomnia was assessed using the Insomnia Severity Index (Bastien et al., 2001), which evaluates the nature, severity, and impact of insomnia using 7 items (e.g., difficulty staying asleep, satisfaction with current sleep patterns). Each item was rated on a 4- or 5-item Likert-type scale and then the total score (range = 0–28) was used to classify insomnia as nonsignificant (0–7), subclinical (8–14), clinically important/moderately severe (15–22), and severe insomnia (23–28). For this study, insomnia was dichotomized as none/subthreshold insomnia (0–14) and moderate/severe insomnia (15–28) (Markwald et al., 2021).
Recent ST
Recent ST, the main exposure of interest, was categorized as “neither,” “SH only,” or “SA,” to align with previous research studies (Millegan et al., 2015; Seelig et al., 2017). Specifically, recent ST was assessed using two “no/yes” items that asked whether participants had (a) “experienced sexual harassment” or (b) “suffered forced sexual relations or sexual assault” in the past 3 years, with the exception of Panel 4 participants, enrolled in 2011 to 2013, whose baseline survey assessed “ever” ST instead of during the last 3 years. Because most participants responded to the question within the past 3-year time frame, we described ST as “recent” throughout this paper. Participants who answered “yes” to forced sexual relations or SA (with or without harassment) on either baseline or follow-up survey comprise the “sexual assault” (recent SA) category. Those who endorsed SH and did not report SA on either survey comprised the “SH only” (recent SH) category. Participants who answered “no” to both items at baseline and follow-up comprised the “neither” category.
Individual and military factors
Eleven individual (sex, race/ethnicity, sexual orientation, childhood trauma, spirituality, social support, and mental health status) and military (service branch, service component, military separation status, and combat deployment history) factors were investigated for effect modification (see Table A1 for more details on each measure). Factors were assessed on the baseline survey, except for combat deployment history (all available surveys up through the follow-up survey), sexual orientation and childhood trauma (new items on follow-up survey). Sex (male, female) and race/ethnicity (Asian or Pacific Islander, Hispanic, non-Hispanic Black, non-Hispanic White, Multiracial) were defined using administrative records from the Defense Manpower Data Center (DMDC). Sexual orientation (heterosexual/straight, homosexual/gay, bisexual, prefer not to answer) was self-reported on the survey. Childhood trauma (none, 1, 2, or 3 or 4 types of traumas experienced) was assessed by self-report using 4 items from the Juvenile Victim Questionnaire on traumatic experiences that occurred prior to age 18 (Finkelhor et al., 2005). Spirituality (low, moderate, high) was assessed using two survey items which assessed religious faith and understanding of spiritual matters from the Current Standing Posttraumatic Growth Inventory–Short Form (Kaur et al., 2017; Tedeschi et al., 2017). Social support (high, low) was assessed using 1 item from the PHQ (Spitzer et al., 1999). Mental health status (PTSD only, depression only, both PTSD and depression, neither) was measured using the self-reported responses to the PCL-C and PHQ-8 described previously (Blanchard et al., 1996; Kroenke et al., 2009). Mental health status was only assessed as a modifying factor for the MSS and insomnia outcomes because we adjusted for baseline measures of each outcome in their respective models (e.g., we adjusted for baseline PTSD in the PTSD outcome model).
Military factors included service branch, service component, military separation status, and combat deployment history. Service branch (Army, Navy/Coast Guard, Marine Corps, Air Force), service component (active duty, Reserve, National Guard), and military separation at baseline (yes, no) were determined using DMDC records. Deployment in support of the operations in Iraq and Afghanistan was assessed using deployment records obtained from DMDC. Combat experience was assessed at all available surveys up through the follow-up and determined from endorsement of at least 1 of 18 items (e.g., witnessing death, being attacked or ambushed, being wounded or injured). Self-reported combat experiences were linked to deployment dates to determine if the reporting period overlapped with deployment (Porter et al., 2018); combat deployment history was then categorized into three groups (never deployed, deployed without combat, and deployed at least once with combat experience). Covariates included in the final models for adjustment purposes included baseline age and pay grade obtained from DMDC, baseline marital status and education by self-report, and enrollment panel.
Statistical Analyses
Panels 1 to 4 were pooled for this study. Descriptive analyses compared recent ST, baseline outcomes, individual and military factors to be tested for effect modification, and covariates by health outcomes. Additionally, we confirmed the unadjusted association between recent ST and the four health outcomes examined. The following three steps were repeated for each of the four health outcomes to assess the main effect of recent ST and then determine if effect modification was present. Using logistic regression models, (a) the adjusted association between recent ST and the outcome was modeled, adjusting for the baseline measurement of the outcome, each potential effect modifier (e.g., sex, childhood trauma, component), and covariates. Covariates (i.e., age, pay grade, marital status, education, and enrollment panel) were selected a priori and remained in all multivariable models, regardless of statistical significance. Next, (b) to assess for presence of effect modification, step (a) was repeated with the addition of all first-order interaction terms between recent ST by each potential effect modifier in one model. For each significant interaction term, that factor was considered an effect modifier. Lastly (c) odds ratios (ORs) were estimated for recent ST and each effect modifier in one adjusted model, where nonsignificant interactions were excluded. The final multivariable models did not indicate multicollinearity (defined as a variance inflation factor ≥4).
When examining which factors were effect modifiers, a false discovery rate (FDR) adjustment was applied to account for multiple comparisons (Benjamini & Hochberg, 1995). When conducting multiple comparisons, FDR adjustment procedures control the expected proportions of type I errors in null hypothesis testing, which is slightly less stringent than Bonferroni corrections but has greater power. Effect modification was determined to be present if the post-FDR adjustment interaction term was significant (p < .05). Analyses were conducted using SAS statistical software, version 9.4 (SAS Institute, Cary, NC, USA).
Results
Participant Characteristics
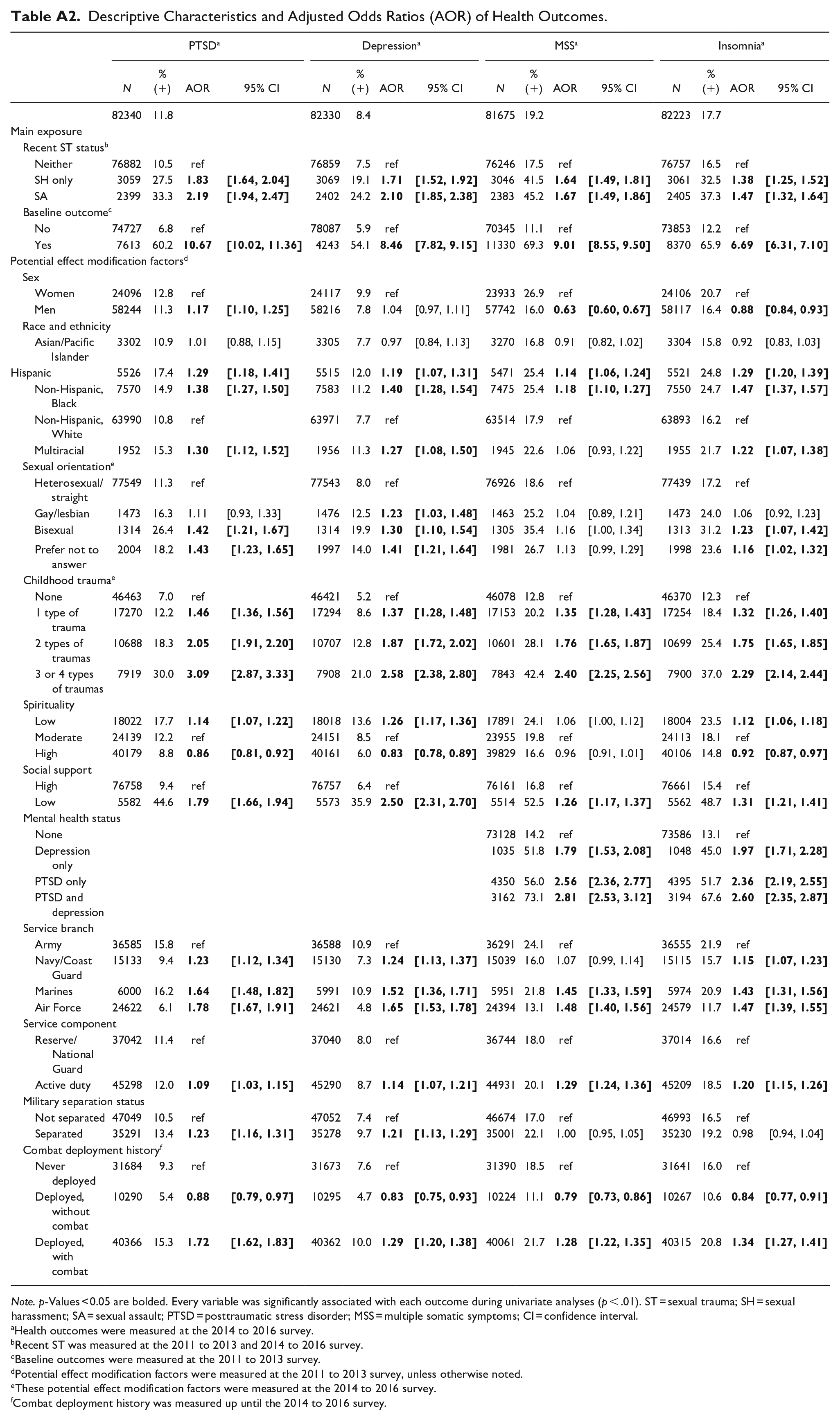
At baseline, the average age of participants was 37 years, though mean age differed by panel (Panel 1 = 46 years, Panels 2–4 = 29 years). Most of the participants in these analyses were non-Hispanic White men (78%), heterosexual (94%), married (67%), obtained a Bachelor’s degree or higher (46%), active duty (55%), in the Army (44%), enlisted (71%), and still serving in the military at the time of the baseline survey (57%; see Table A2 for descriptive characteristics across each sample, results for covariates not shown). Approximately 4% (n = 3,059) reported experiencing recent SH only and 3% (n = 2,399) recent SA with or without recent SH. Nearly half the sample had deployed and experienced combat (49%), endorsed high spirituality (49%), and reported one or more types of childhood trauma (44%), while most reported high social support (93%; Table A2).
Adjusted Associations Between Recent ST and Health Outcomes
Results of the adjusted logistic regression modeling confirmed that those who reported recent SH or SA had higher odds of PTSD, depression, MSS, and insomnia compared with those with no recent ST (p < .05; Table A2).
Testing for Effect Modification
Several factors were determined to be effect modifiers. Sex, sexual orientation, childhood trauma, spirituality, social support, mental health status, service component, and combat deployment history modified the effect of recent ST on at least one outcome (Table 1). Race/ethnicity, service branch, and military separation did not significantly modify the effect of recent ST on any of the outcomes examined (Table 1).
Effect Modification Models
The adjusted odds for each outcome by recent ST and stratified by effect modifiers are shown in Figures 1 to 4 and detailed below.
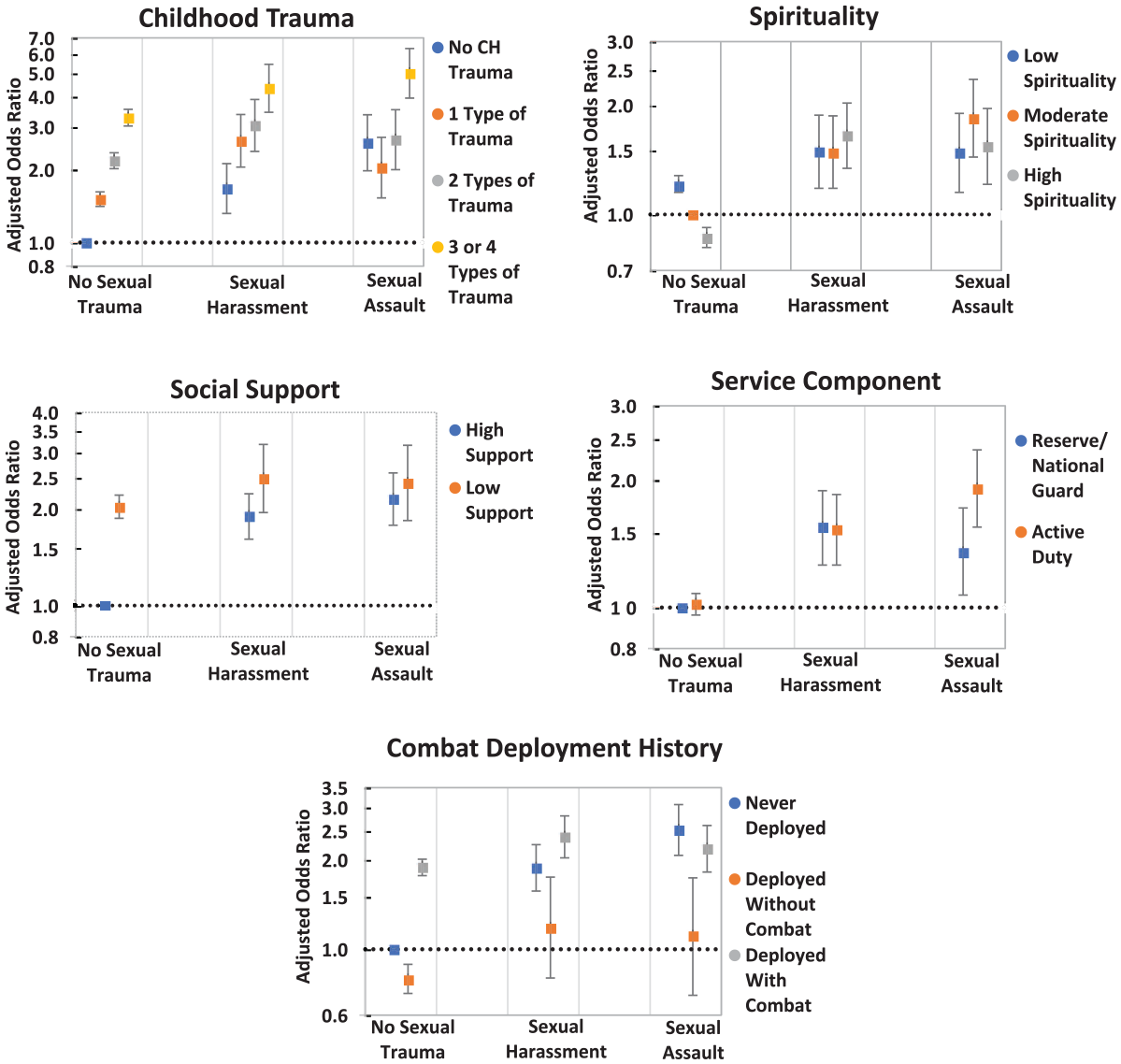
Adjusted odds of PTSD in relation to recent ST, by key effect modifiers.
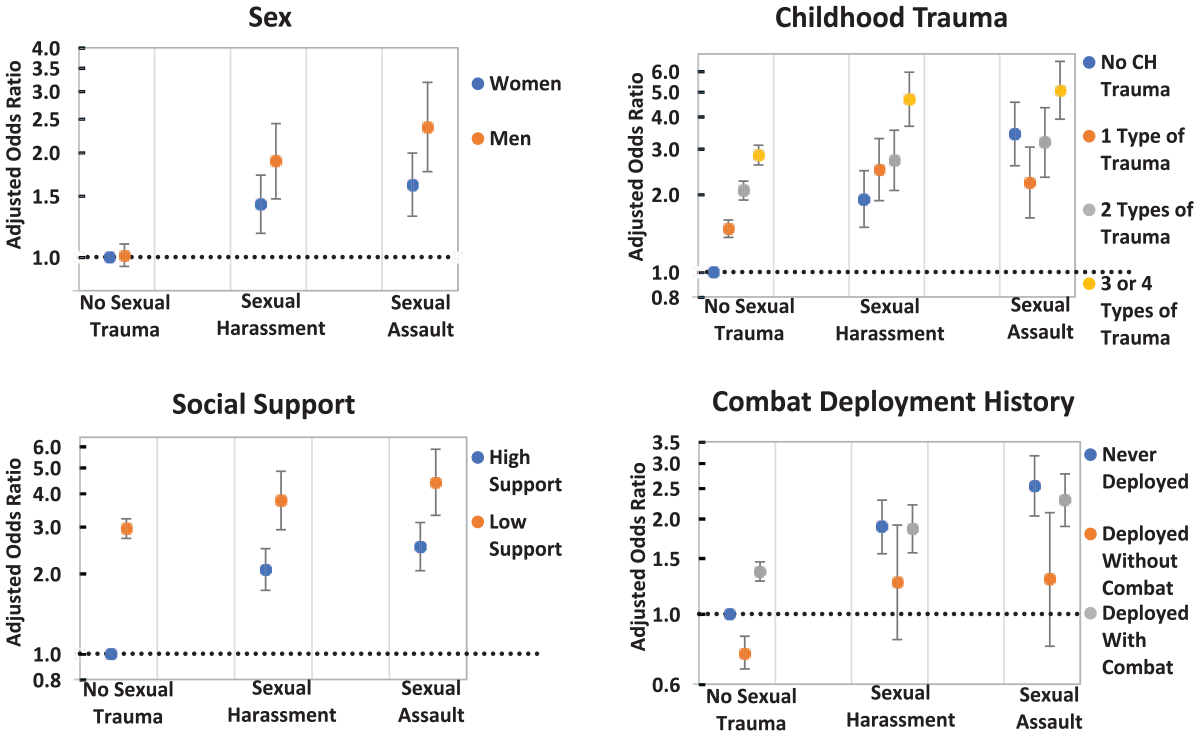
Adjusted odds of depression in relation to recent ST, by key effect modifiers.
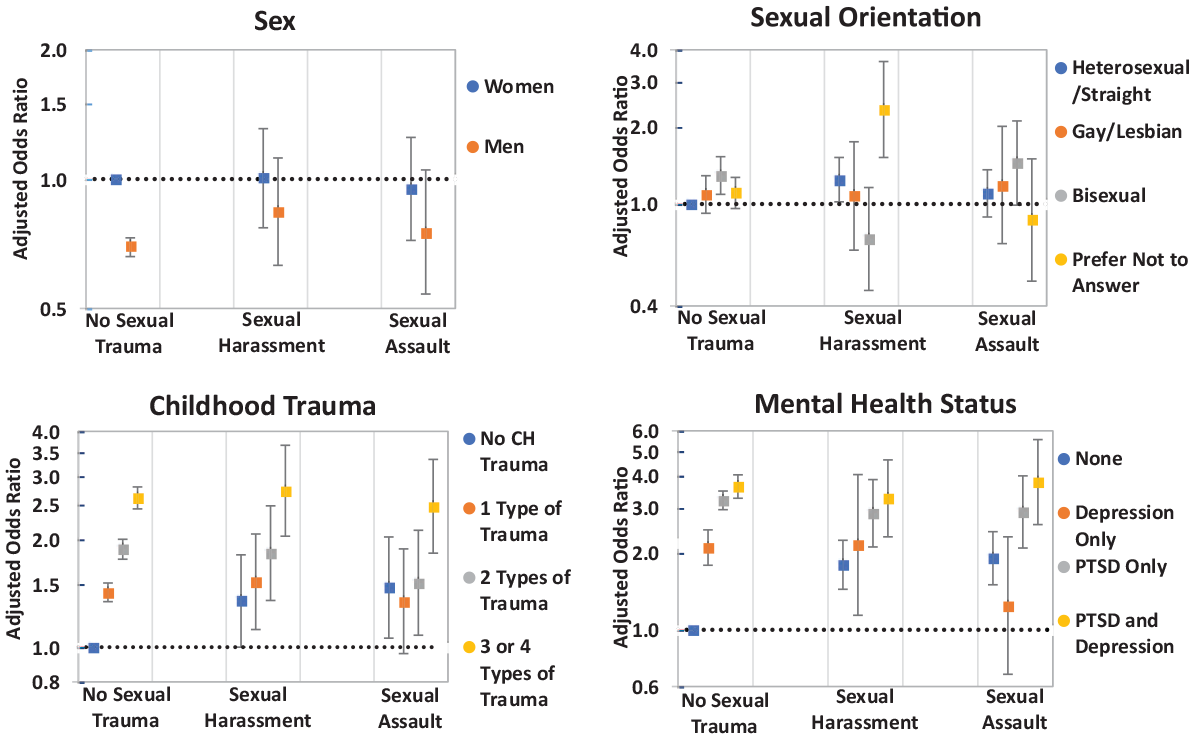
Adjusted odds of MSS in relation to recent ST, by key effect modifiers.
Adjusted odds of insomnia in relation to recent ST, by key effect modifiers.
Posttraumatic stress disorder
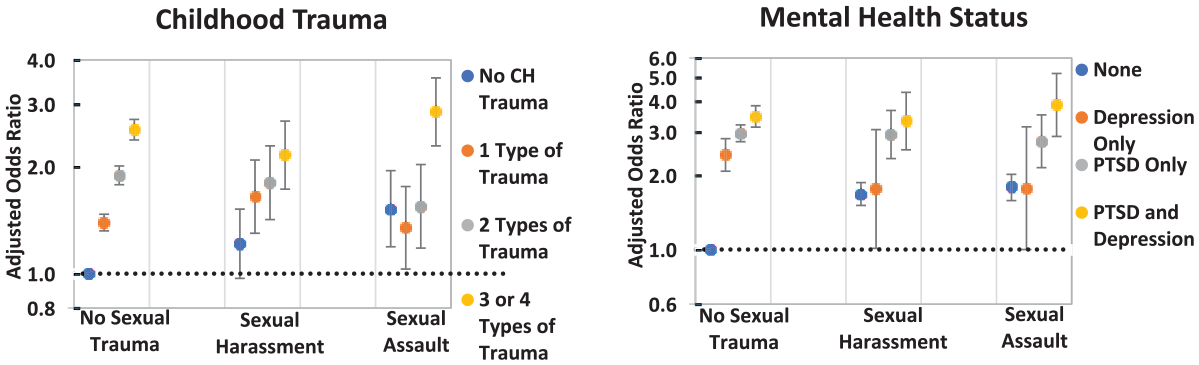
Childhood trauma, spirituality, social support, service component, and combat deployment history modified the association between recent ST and PTSD (Figure 1). The odds for PTSD generally increased as the number of reported types of childhood trauma increased. Among those reporting the same level of childhood trauma, such as three to four different types of childhood trauma, the odds of PTSD were fairly consistent across all levels of recent ST (e.g., 3.28–5.00). There was one exception to this overall pattern: those who experienced recent SA and reported 0, 1, or 2 types of childhood trauma had similar odds of PTSD (OR = 2.01-2.66). Among those without a history of recent ST, reporting high spirituality was associated with lower odds of PTSD than reporting low or moderate spirituality (OR = 0.86, 95% confidence interval [CI] [0.81, 0.92]), while this protective effect of spirituality did not appear to reduce the odds of PTSD in the presence of recent SH or SA (OR range 1.48–1.84) (Figure 1). Similarly, among those with no recent ST history, low social support was significantly associated with higher odds of PTSD compared with high social support (OR = 2.03, 95% CI [1.87, 2.21]). However, this protective effect of high social support was not observed among those who experienced recent ST; the odds of PTSD were approximately doubled, regardless of the level of social support reported among those with recent SH or SA (OR range 1.90–2.49). Among those with no recent ST, active-duty members had the same odds of screening positive for PTSD compared with Reserve/Guard members. Elevated odds of PTSD among those with a history of recent ST were found, regardless of service component. The association between recent SH and PTSD appeared similar in magnitude by service component, whereas the odds of PTSD were slightly higher for active-duty personnel compared with Reserve/Guard members among those with recent SA (OR = 1.91 vs. 1.35). Combat deployment history showed distinct patterns with respect to the association of recent ST and PTSD. Among those who never deployed, odds of PTSD increased with recent ST severity in a dose–response pattern (OR = 1.00, 1.88, 2.52). In comparison, among those who deployed without combat, there was no significant impact of recent ST exposure on PTSD risk. The effect of recent ST on PTSD risk was also diminished for those who deployed with combat exposure; however, odds of PTSD were consistently elevated for this group overall (Figure 1).
Depression
The association between recent ST and depression was modified by sex, childhood trauma, social support, and combat deployment history (Figure 2). With respect to sex, among those with no recent ST, men and women did not differ in the odds of depression. However, the odds of depression among those with recent ST were elevated among both men and women, and men had slightly higher odds than women. The trends in the effects of childhood trauma, social support, and combat deployment history on the association between recent ST and depression were similar to the results observed with the PTSD outcome (Figure 2).
Multiple somatic symptoms
The association between recent ST and MSS was modified by sex, sexual orientation, childhood trauma, and mental health status (Figure 3). Among those with no recent ST, men had lower odds of MSS (OR = 0.70, 95% CI [0.66, 0.73]) compared with women, while the odds for MSS were similar for men and women reporting either type of recent ST (Figure 3). Across subgroups based on sexual orientation, odds of MSS were generally similar, regardless of recent ST. However, those reporting recent SH alone presented the greatest odds for MSS among the group that preferred not to answer the sexual orientation question (OR = 2.34, 95% CI [1.52, 3.60]). Higher odds of MSS were also found among the heterosexual/straight group with recent SH (OR = 1.24, 95% CI [1.02, 1.52]) and the bisexual group with no history of recent ST (OR = 1.29, 95% CI [1.09, 1.53]). The modifying influence of childhood trauma on risk for MSS related to recent ST followed a similar pattern as described earlier in this paper with respect to the PTSD and depression outcomes (Figure 3). Lastly, among those without mental disorders, odds of MSS were significantly elevated among those who reported recent SH or SA. By comparison, among those with a mental disorder, odds of MSS were consistently elevated across all levels of recent ST (Figure 3).
Insomnia
The association between recent ST and insomnia was modified by childhood trauma and mental health status (Figure 4). The effects of childhood trauma on the association between recent ST and insomnia were consistent with the trend reported for PTSD, depression, and MSS outcomes. The modifying influence of mental health status also followed a similar pattern as with the MSS outcome (Figure 4).
Discussion
In this large prospective study of current and former service members, we explored the impact of ST on research participants volunteering from all branches and components of the U.S. military. Using data from the Millennium Cohort Study (Ryan et al., 2007; T. C. Smith, 2009), we specifically tested individual and military factors that might heighten the vulnerability of specific subgroups of personnel in the aftermath of ST exposure. Recent ST was associated with higher odds for all outcomes examined (PTSD, depression, MSS, and insomnia) compared with individuals who did not report any recent ST experiences. Several individual and military factors were identified as effect modifiers as well; however, the associations tended to differ more by factors related to social support, traumatic life events, and mental health than demographic or military characteristics.
With few exceptions, we found that the health impact of recent ST did not differ by the demographic (sex, sexual orientation, race and ethnicity) or military (service branch, service component, and military separation) characteristics of our participants. For instance, race/ethnicity did not significantly modify the effect of recent ST on any outcome examined. However, we observed that those who preferred not to give information about their sexual orientation and had experienced recent SH had elevated risk for MSS. It is difficult to interpret this finding but fearing consequences of outing oneself has been noted as a reason for sexual orientation nonresponse in clinical settings (Brooks et al., 2018). Further study is needed to confirm and explain this finding.
Results suggest that men were more negatively impacted from recent ST compared with women in terms of MSS and depression, indicating that male ST survivors may need additional resources and support. Ziobrowski et al. (2017) reported similar sex differences for depression, and previous examinations of recent ST in this cohort have noted differing coping behaviors by sex that may impact the development or severity of depression symptoms (Seelig et al., 2017). Additional research is needed to better understand the factors influencing health outcomes following ST among men. Stigma and lack of resources for men who have experienced ST may be barriers to reporting ST and care seeking, resulting in worse outcomes over time. Policy aimed at supporting and providing targeted resources for male ST survivors may help lessen the health burden following ST.
While there were few differential effects by recent ST in terms of demographic and military characteristics, some sub-groups were still more likely to experience negative health outcomes regardless of recent ST status. We found that people of color, and lesbian, gay, and bisexual individuals had higher risk for adverse health outcomes, underscoring the need for improved equity initiatives that foster cultural acceptance. In general, we also found higher odds of adverse health outcomes among Marines, Army, and Navy/Coast Guard personnel (vs. Air Force), active duty (vs. Reserve/Guard), and veterans (vs. currently serving). Differences in adverse health outcomes among these groups have been noted previously (Carey et al., 2022; Markwald et al., 2021; Riddle et al., 2007) and may be associated with minority stress experiences not measured in this study; additional research is needed.
Combat deployment history and childhood trauma, typically considered risk factors for poorer health, had the most consistent influence across the outcomes examined. While the odds for PTSD, depression, MSS, and insomnia were generally elevated for those who experienced recent SH or SA compared with those who had no recent ST history, the effect of combined traumas was lower than expected. Those who experienced combat deployment and recent ST had similar risk for PTSD as those experiencing combat deployment without recent ST. This may indicate a potential ceiling effect for the negative impact of combined traumas or that the experience of childhood trauma or combat outweigh that of recent ST exposure for the participants in this study. Cabrera et al. (2007) reported a similar finding where the odds for PTSD and depression were similar but lower among the post-deployment group than the pre-deployment group for service members who had experienced four or more childhood traumas. In addition, an interesting pattern was revealed among those experiencing recent SA and childhood trauma. This pattern showed that the odds of a given outcome (e.g., depression) among those reporting recent SA was smallest in magnitude for participants experiencing one type of trauma, even lower than those who reported no childhood trauma. It is possible that surviving one or even two childhood traumas built resilience to trauma over time. Service members and veterans are more likely to have experienced childhood trauma than civilians (Laird & Alexander, 2019), meaning multiple traumas are common in this population who also experience combat deployment and providers should consider those factors in their treatment, despite the noted risk ceiling.
Mental health status (depression and/or PTSD) was a consistently significant effect modifier for MSS and insomnia. The OR estimates were similar across recent ST groups among those with the same mental health condition. These findings expand on previous research indicating that PTSD and depression have a negative impact on physical health (Nichter et al., 2019) by suggesting that experiences of recent ST do not further exacerbate the risk of adverse physical conditions above and beyond the experience of mental disorders, again identifying a potential risk ceiling. Integrated care, such as VA’s Whole Health model of care, may help reduce the health burden associated with multiple traumas. An initial evaluation showed improvements in perceived stress, engagement in health care, pain, life meaning, and self-care among those who participated in the whole health system, compared to those who received standard care (Bokhour et al., 2022).
A similar diminishing impact was observed among effect modifiers often considered to be protective, such as spirituality and social support, in the presence of recent ST. The risk of PTSD differed by social support and spirituality among those who did not experience recent ST; however there was little or no difference in PTSD risk by those same factors among those with recent ST. Similar social support results were noted for the depression outcome. While social support and spirituality typically confer a level of protection from PTSD and depression, that protection may not be enough to counteract the effects of ST among service members. Social support may be particularly impacted in a military sample due to the close live-work environment. ST perpetrators are often known to the survivor and may even be a part of the same military unit, making it difficult to maintain strong social support following ST. Additional coping and support resources may be needed to bolster the mental well-being for those service members who have experienced recent ST.
The main strengths of this study included the large sample size and longitudinal design of the Millennium Cohort Study (Crum-Cianflone, 2013) and the ability to adjust for several individual and military factors and confounders that could potentially bias findings. Notable limitations of this study include that the time frame used to measure recent ST experiences differed for Panel 4 participants (“ever” experienced) compared with the other three panels (experienced in the “last three years”) and limitations of data collected in the surveys. For example, recent ST may have been underreported because some participants may not use the terms “sexual assault” and “sexual harassment” to describe their experiences (Cook et al., 2011). Similarly, sexual orientation did not collect all possible responses (Suen et al., 2020). Several measures used in this study (i.e., recent ST and social support) were also not based on standardized scales or instruments and were assessed using only one or two survey items. Thus, these measures may not fully capture the desired construct; however, the methods used are consistent with previously published studies (Millegan et al., 2016; Pflieger et al., 2018; Seelig et al., 2017). Finally, collected survey data are confidential and self-reported, which may be susceptible to reporting and recall bias and limit generalizability. However, previous investigations of the Millennium Cohort Study have not demonstrated systematic sampling bias to date (Horton et al., 2013; Littman et al., 2010; T. C. Smith, 2009).
To our knowledge, this is the first study to examine whether certain individual and military factors modified the effect of recent ST on health outcomes in a large cohort of current and former service members. Our findings confirm that exposure to recent ST increased the odds of PTSD, depression, MSS, and insomnia, and the effects of recent ST on these outcomes were generally stable across demographic and military factors, with limited exceptions. However, we identified several potential effect modifiers. Social support and spirituality, factors that might be expected to ameliorate the effects of ST, were only protective for mental health among those who had not experienced recent ST. We also identified a pattern in which potential risk factors, such as combat experience and childhood trauma, had an attenuated impact on those with a history of recent ST. Many other factors not investigated as part of this study, such as specifics of the incident or perpetrator, may impact the effect of ST on health outcomes. A previous study of college students found that socioenvironmental factors such as assault setting and relationship with the perpetrator had significant associations with distress (Blayney & Read, 2018). Future research should examine these factors in a military sample given the close live-work environment in the military.
Conclusion
This study suggests that the main effect of recent ST on the outcomes examined was mostly unchanged in the presence of potential protective factors and worsened in the presence of other factors. Therefore, while focused efforts to eradicate these behaviors within DoD are ongoing (Stander & Thomsen, 2016), efforts to improve prevention and mitigation measures for SH and SA in the military should continue. Findings from this study can help guide and inform these policy discussions to reduce the health burden on survivors of ST. Findings can also be utilized by healthcare providers in the military, VA, and civilian sectors to ensure that additional information is collected from their patients regarding other potentially traumatic events such as childhood traumatic experiences or combat, since these combined experiences may exacerbate certain mental health outcomes and point toward whole health patient-centered treatment approaches.
Footnotes
Appendix
Descriptive Characteristics and Adjusted Odds Ratios (AOR) of Health Outcomes.
| PTSD
a
|
Depression
a
|
MSS
a
|
Insomnia
a
|
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % (+) | AOR | 95% CI | N | % (+) | AOR | 95% CI | N | % (+) | AOR | 95% CI | N | % (+) | AOR | 95% CI | |
| 82340 | 11.8 | 82330 | 8.4 | 81675 | 19.2 | 82223 | 17.7 | |||||||||
| Main exposure | ||||||||||||||||
| Recent ST status b | ||||||||||||||||
| Neither | 76882 | 10.5 | ref | 76859 | 7.5 | ref | 76246 | 17.5 | ref | 76757 | 16.5 | ref | ||||
| SH only | 3059 | 27.5 |
|
|
3069 | 19.1 |
|
|
3046 | 41.5 |
|
|
3061 | 32.5 |
|
|
| SA | 2399 | 33.3 |
|
|
2402 | 24.2 |
|
|
2383 | 45.2 |
|
|
2405 | 37.3 |
|
|
| Baseline outcome c | ||||||||||||||||
| No | 74727 | 6.8 | ref | 78087 | 5.9 | ref | 70345 | 11.1 | ref | 73853 | 12.2 | ref | ||||
| Yes | 7613 | 60.2 |
|
|
4243 | 54.1 |
|
|
11330 | 69.3 |
|
|
8370 | 65.9 |
|
|
| Potential effect modification factors d | ||||||||||||||||
| Sex | ||||||||||||||||
| Women | 24096 | 12.8 | ref | 24117 | 9.9 | ref | 23933 | 26.9 | ref | 24106 | 20.7 | ref | ||||
| Men | 58244 | 11.3 |
|
|
58216 | 7.8 | 1.04 | [0.97, 1.11] | 57742 | 16.0 |
|
|
58117 | 16.4 |
|
|
| Race and ethnicity | ||||||||||||||||
| Asian/Pacific Islander | 3302 | 10.9 | 1.01 | [0.88, 1.15] | 3305 | 7.7 | 0.97 | [0.84, 1.13] | 3270 | 16.8 | 0.91 | [0.82, 1.02] | 3304 | 15.8 | 0.92 | [0.83, 1.03] |
| Hispanic | 5526 | 17.4 |
|
|
5515 | 12.0 |
|
|
5471 | 25.4 |
|
|
5521 | 24.8 |
|
|
| Non-Hispanic, Black | 7570 | 14.9 |
|
|
7583 | 11.2 |
|
|
7475 | 25.4 |
|
|
7550 | 24.7 |
|
|
| Non-Hispanic, White | 63990 | 10.8 | ref | 63971 | 7.7 | ref | 63514 | 17.9 | ref | 63893 | 16.2 | ref | ||||
| Multiracial | 1952 | 15.3 |
|
|
1956 | 11.3 |
|
|
1945 | 22.6 | 1.06 | [0.93, 1.22] | 1955 | 21.7 |
|
|
| Sexual orientation e | ||||||||||||||||
| Heterosexual/straight | 77549 | 11.3 | ref | 77543 | 8.0 | ref | 76926 | 18.6 | ref | 77439 | 17.2 | ref | ||||
| Gay/lesbian | 1473 | 16.3 | 1.11 | [0.93, 1.33] | 1476 | 12.5 |
|
|
1463 | 25.2 | 1.04 | [0.89, 1.21] | 1473 | 24.0 | 1.06 | [0.92, 1.23] |
| Bisexual | 1314 | 26.4 |
|
|
1314 | 19.9 |
|
|
1305 | 35.4 | 1.16 | [1.00, 1.34] | 1313 | 31.2 |
|
|
| Prefer not to answer | 2004 | 18.2 |
|
|
1997 | 14.0 |
|
|
1981 | 26.7 | 1.13 | [0.99, 1.29] | 1998 | 23.6 |
|
|
| Childhood trauma e | ||||||||||||||||
| None | 46463 | 7.0 | ref | 46421 | 5.2 | ref | 46078 | 12.8 | ref | 46370 | 12.3 | ref | ||||
| 1 type of trauma | 17270 | 12.2 |
|
|
17294 | 8.6 |
|
|
17153 | 20.2 |
|
|
17254 | 18.4 |
|
|
| 2 types of traumas | 10688 | 18.3 |
|
|
10707 | 12.8 |
|
|
10601 | 28.1 |
|
|
10699 | 25.4 |
|
|
| 3 or 4 types of traumas | 7919 | 30.0 |
|
|
7908 | 21.0 |
|
|
7843 | 42.4 |
|
|
7900 | 37.0 |
|
|
| Spirituality | ||||||||||||||||
| Low | 18022 | 17.7 |
|
|
18018 | 13.6 |
|
|
17891 | 24.1 | 1.06 | [1.00, 1.12] | 18004 | 23.5 |
|
|
| Moderate | 24139 | 12.2 | ref | 24151 | 8.5 | ref | 23955 | 19.8 | ref | 24113 | 18.1 | ref | ||||
| High | 40179 | 8.8 |
|
|
40161 | 6.0 |
|
|
39829 | 16.6 | 0.96 | [0.91, 1.01] | 40106 | 14.8 |
|
|
| Social support | ||||||||||||||||
| High | 76758 | 9.4 | ref | 76757 | 6.4 | ref | 76161 | 16.8 | ref | 76661 | 15.4 | ref | ||||
| Low | 5582 | 44.6 |
|
|
5573 | 35.9 |
|
|
5514 | 52.5 |
|
|
5562 | 48.7 |
|
|
| Mental health status | ||||||||||||||||
| None | 73128 | 14.2 | ref | 73586 | 13.1 | ref | ||||||||||
| Depression only | 1035 | 51.8 |
|
|
1048 | 45.0 |
|
|
||||||||
| PTSD only | 4350 | 56.0 |
|
|
4395 | 51.7 |
|
|
||||||||
| PTSD and depression | 3162 | 73.1 |
|
|
3194 | 67.6 |
|
|
||||||||
| Service branch | ||||||||||||||||
| Army | 36585 | 15.8 | ref | 36588 | 10.9 | ref | 36291 | 24.1 | ref | 36555 | 21.9 | ref | ||||
| Navy/Coast Guard | 15133 | 9.4 |
|
|
15130 | 7.3 |
|
|
15039 | 16.0 | 1.07 | [0.99, 1.14] | 15115 | 15.7 |
|
|
| Marines | 6000 | 16.2 |
|
|
5991 | 10.9 |
|
|
5951 | 21.8 |
|
|
5974 | 20.9 |
|
|
| Air Force | 24622 | 6.1 |
|
|
24621 | 4.8 |
|
|
24394 | 13.1 |
|
|
24579 | 11.7 |
|
|
| Service component | ||||||||||||||||
| Reserve/National Guard | 37042 | 11.4 | ref | 37040 | 8.0 | ref | 36744 | 18.0 | ref | 37014 | 16.6 | ref | ||||
| Active duty | 45298 | 12.0 |
|
|
45290 | 8.7 |
|
|
44931 | 20.1 |
|
|
45209 | 18.5 |
|
|
| Military separation status | ||||||||||||||||
| Not separated | 47049 | 10.5 | ref | 47052 | 7.4 | ref | 46674 | 17.0 | ref | 46993 | 16.5 | ref | ||||
| Separated | 35291 | 13.4 |
|
|
35278 | 9.7 |
|
|
35001 | 22.1 | 1.00 | [0.95, 1.05] | 35230 | 19.2 | 0.98 | [0.94, 1.04] |
| Combat deployment history f | ||||||||||||||||
| Never deployed | 31684 | 9.3 | ref | 31673 | 7.6 | ref | 31390 | 18.5 | ref | 31641 | 16.0 | ref | ||||
| Deployed, without combat | 10290 | 5.4 |
|
|
10295 | 4.7 |
|
|
10224 | 11.1 |
|
|
10267 | 10.6 |
|
|
| Deployed, with combat | 40366 | 15.3 |
|
|
40362 | 10.0 |
|
|
40061 | 21.7 |
|
|
40315 | 20.8 |
|
|
Note. p-Values < 0.05 are bolded. Every variable was significantly associated with each outcome during univariate analyses (p < .01). ST = sexual trauma; SH = sexual harassment; SA = sexual assault; PTSD = posttraumatic stress disorder; MSS = multiple somatic symptoms; CI = confidence interval.
Health outcomes were measured at the 2014 to 2016 survey.
Recent ST was measured at the 2011 to 2013 and 2014 to 2016 survey.
Baseline outcomes were measured at the 2011 to 2013 survey.
Potential effect modification factors were measured at the 2011 to 2013 survey, unless otherwise noted.
These potential effect modification factors were measured at the 2014 to 2016 survey.
Combat deployment history was measured up until the 2014 to 2016 survey.
Disclaimer
Amber D. Seelig, Samantha M. Daniels, Valerie A. Stander, and Edward J. Boyko are employees of the U.S. Government. This work was prepared as part of their official duties. Title 17, U.S.C. §105 provides that copyright protection under this title is not available for any work of the U.S. Government. Title 17, U.S.C. §101 defines a U.S. Government work as work prepared by a military service member or employee of the U.S. Government as part of that person’s official duties. Report No. 21-68 was supported by the Military Operational Medicine Research Program, Defense Health Program, and Department of Veterans Affairs under work unit no. 60002. The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, Department of Veterans Affairs, nor the U.S. Government. The study protocol was approved by the Naval Health Research Center Institutional Review Board in compliance with all applicable Federal regulations governing the protection of human subjects. Research data were derived from an approved Naval Health Research Center Institutional Review Board protocol, number NHRC.2000.0007.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The Millennium Cohort Study is funded through the Military Operational Medicine Research Program, Defense Health Program, and Department of Veterans Affairs. The Department of Veterans Affairs Puget Sound Health Care System supported Dr. Boyko’s involvement in this research. The Department of Veterans Affairs Cooperative Studies Program supported Ms. Seelig’s involvement in this research.