
Abstract
Studies on adverse childhood experiences (ACEs), which have been conducted predominantly with samples from Western cultures have found ACEs to be associated with poor health outcomes and relational impairments in adulthood. This study sought to contribute to the ACEs literature by investigating the long-term consequences of ACEs on the interpersonal functioning of adult survivors in Ghana, a non-Western culture. In the current study, the associations of five ACEs (high parental conflict, physical abuse, sexual abuse, emotional abuse, and neglect) with four types of relational impairments (alienation, insecure attachment, egocentricity, and social incompetence) were examined using a community sample of 403 adults who retrospectively provided self-reports of ACEs. The most frequently reported ACE in this sample was high parental conflict, while sexual abuse was the least frequently reported ACE. Participants with ACE histories had significantly more relational impairments than those with no ACE histories, however multiple regression analyses revealed no significant relational impairments in adulthood following any ACE experience, whether alone or in any combination, suggesting that cultural values such as collectivism and religiosity may play a protective role against ACEs negative effects in the interpersonal domain. The study’s limitations, and the implications of these findings for the Ghanaian and other similar contexts are discussed.
Introduction
Childhood adversity has been linked to a number of long-term harmful outcomes including cognitive deficits in performance, memory, and executive functioning; morbidity; low quality of life; and mortality (Briere & Runtz, 1988; Brodsky & Stanley, 2008; Cicchetti, 2004; Edwards et al., 2003; Egeland et al., 1983; Felitti et al., 1998; Gilbert et al., 2010; Mansueto et al., 2021; Metzler et al., 2017; Opaas & Varvin, 2015; Pechtel & Pizzagalli, 2011; Spilsbury et al., 2007; Tolin & Foa, 2008; Wamser-Nanney & Cherry, 2018). In addition, childhood adversity which takes place in an interpersonal context (i.e., relational trauma) from a person with whom a child has a close relationship negatively affects right brain development and hinders children’s abilities to regulate their emotions. This inability to regulate emotions is a risk factor which has been implicated in all personality disorders and in the development of most psychological disorders (Aldea & Rice, 2006; Beauchaine & Cicchetti, 2019; Cloitre et al., 2019; Cole & Hall, 2008; Gross & Levenson, 1997; Marganska et al., 2013; Milojevich et al., 2019; Mullen et al., 1996; Schore, 2001; Weissman et al., 2019).
Relational trauma in childhood has also been associated with long-term impairments in survivors’ social and relational functioning (e.g., Elliott, 1994; Reyome, 2010; Tardif-Williams et al., 2017), as these early experiences build a foundational expectation of abuse in subsequent relationships. Bowlby (1982) postulated that infants internalize early experiences of the physical environment, attachment figures, and self into working models for subsequent interpersonal relationships, which result in secure or insecure attachment formations. According to Bowlby, secure attachments develop in the absence of environmental deprivation, unavailable caregivers, and other relational traumas such as physical or sexual abuse, while insecure attachments develop when children are exposed to traumatic events which “wound” (from the Greek root of trauma) their psyches, and cause them to have poor object relations. Object relations as defined by Greenberg and Mitchell (1983) is “an individual’s interactions with external and internal (real and imagined) other people, and to the relationship between their internal and external object worlds” (pp. 13–14). Given that past interpersonal experiences prime individuals to expect pleasurable or threatening encounters when relating to others, object relations therefore mediate affective expectations in interpersonal relationships (Westen, 1990) and can cause significant emotional distress for individuals when impaired.
The literature shows that the negative associations of childhood relational trauma extend past survivors to their children. Studies have found that children of parent(s) with relational trauma histories often have behavioral and emotional problems since parent(s) with histories of adversity in childhood both fail to present themselves as reliable objects whom their children can securely attach to, and unconsciously communicate and transfer their traumatic symptoms to their children (e.g., Fenerci & DePrince, 2018; Fitzgerald et al., 2020; Fraiberg et al., 1975; Lev-Wiesel, 2007).
The seminal adverse childhood experience (ACE) study’s (Anda et al., 2006; Felitti et al., 1998; Hughes et al., 2017) findings that the greater the number of ACEs in the form of childhood abuse or household dysfunction that an individual was exposed to, the more at risk that individual would be to several of the leading causes of death in adulthood provided a new approach to understanding the long-term health implications of different ACEs.
While a number of studies have explored the long-term associations of specific childhood relational trauma, such as sexual or physical abuse, on adult relational capacities (e.g., Brenner et al., 2021; Elliott, 1994; Fuchshuber et al., 2019) using Western samples, few studies have explored the long-term associations of ACEs with physical, psychological, or social well-being outcomes in non-Western samples
This study seeks to contribute to the literature on the associations of ACEs with adult interpersonal functioning in non-Western cultures and to the knowledge of trauma’s sequalae in the Ghanaian context. As noted by Badoe (2017) for example, studies on child abuse in Africa are in a fledging state, and there is a gap in knowledge of the prevalence and long lasting consequences of child abuse in the region.
The Ghanaian Context
Ghana is a lower middle income country in West Africa which is categorized as a collectivist culture (Affum-Osei et al, 2019; Hofstede Insights, 2023). Hofstede (1998) defines collectivism as “the extent to which people in a society from birth onwards are integrated into strong, cohesive ingroups, which throughout people’s lifetime continue to protect them in exchange for unquestioning loyalty” p. 26. Individuals in collectivist cultures tend to avoid conflict, value high power distances (i.e., accept that power is distributed unequally), favor emotional responses in decision-making, and define self in terms of collective identity (e.g., Günsoy et al., 2015; Hofstede, 1998; LeFebvre & Franke, 2013; Ma & Schoeneman, 1997; Triandis et al, 1988). These cultural variables may therefore mitigate the effects of ACEs for individuals in such cultures. In addition, Ghanaian culture is highly religious (Asante, 2020, Kyei, 2022) and Christian values of forgiveness and beliefs in God as the righter of wrongs may result in individuals with traumatic experiences in Ghana having different outcomes than their counterparts in Western countries.
In investigating this hypothesis, the study explored the associations of the following five relational ACEs: physical abuse, sexual abuse, emotional abuse, neglect, and high parental conflict with relational impairments in adult survivors. The study also explored the contributions of each ACE to specific adult relational impairments.
Method
Participants and Procedures
A cross-sectional survey was conducted with 420 participants randomly selected from institutions of higher learning and workplaces in the capital, Accra. With the consent of the educational institutions and workplaces conveniently targeted for the study, participants were individually approached and asked to consent to taking part in the survey. Participants then sealed and returned their completed questionnaires in provided envelopes. To be included in the study, participants had to be literate adults between the ages of 21 and 65 years. Seventeen participants returned their questionnaires unfilled, and the analyzed data were from the 403(response rate, 96%) completed questionnaires.
Measures
Relational ACEs Checklist
This checklist required participants to respond “yes” or “no” retrospectively to experiencing four relational traumatic experiences that directly involved them: emotional abuse, physical abuse, sexual abuse, and neglect in childhood; and one relational trauma that did not directly involve them: growing up in a dysfunctional household with high parental conflict.
The Bell Object Relations Inventory (BORI)
The BORI is a self-report object relations inventory which assesses the way an individual conducts relationships and experiences himself or herself in relation to others (Bell, 1995, p. 48). The BORI comprises 45-item true/false statements, and assesses four domains of object relations: alienation (ALN), insecure attachment (IA), egocentricity (EGC), and social incompetence (SI). The ALN scale score describes an individual’s characteristic ability to experience trust in the context of intimate relationships; the IA score indicates a person’s sensitivity to rejection and their likelihood of being easily hurt by others; the EGC scale focuses on the tendency to perceive others only in relationship to oneself; and the SI scale describes a person’s perception of their own ability to successfully engage in social activity. The object relations scale report Cronbach alphas ranging from .78 to .90. The BORI has been used in a Ghanaian sample (Kyei, 2015) with reported Cronbach alphas ranging from .65 to .76, which demonstrates its validity for use with this population. In the present sample, Cronbach alphas for the ALN, IA, EGC, and SI scales were .76, .78, .71, and .66, respectively.
Ethical Considerations
Ethical clearance for this study was obtained from the Noguchi Memorial Institute for Medical Research’s institutional review board and all participants of the study consented to taking part in the study voluntarily.
Statistical Analyses
The study’s data were analyzed using IBM SPSS Statistics (Version 23). Frequencies for participants’ demographic characteristics, individual ACEs, and the number(s) of ACEs reported by participants were obtained. Bivariate correlations were used to explore the relationship between individual ACEs and specific kinds of adult relational impairment. Hierarchical regressions were used to examine the contribution of ACEs to relational impairments in adulthood after controlling for demographic variables. Missing data were excluded from the analyses.
Results
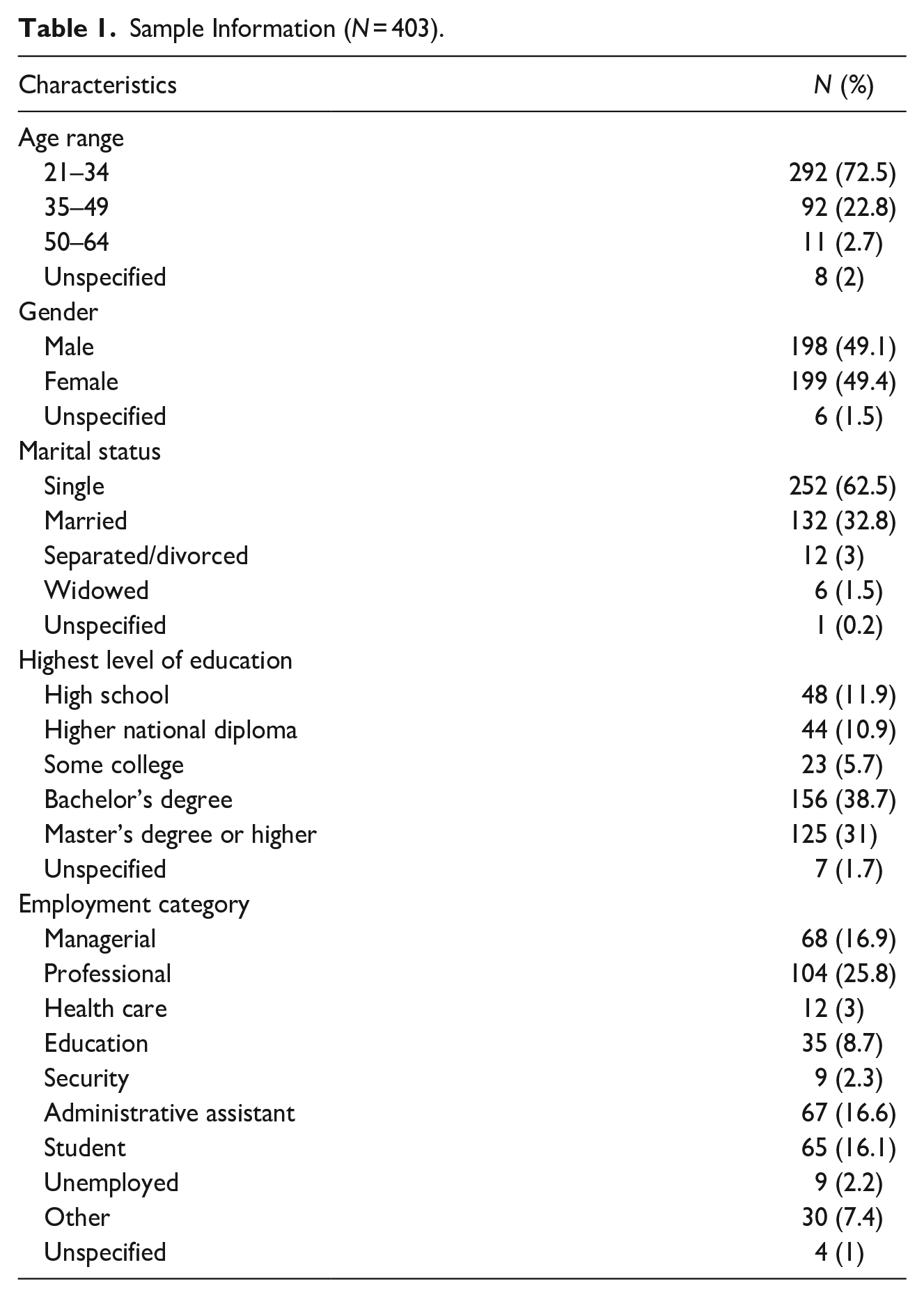
The demographic characteristics of participants are shown in Table 1. 49.4% of the sample were female, 62.5% of the sample was single, 38.7% had a bachelor’s degree, 25% identified as professional workers, and 72.5% of participants were in the age range of 21 to 34 years.
Sample Information (N = 403).
Frequencies of ACEs
42% (n = 165) of the total sample reported experiencing an ACE. The most frequently experienced ACE in the sample was growing up in dysfunctional households with high parental conflict (26.4%), followed by emotional abuse (18.7%), neglect (14.8%), physical abuse (10.1%), and then sexual abuse (6%). Among participants who reported experiencing any ACE, almost 50% (n = 82) reported experiencing more than one ACE. Table 2 presents frequencies of ACEs in the sample, and Table 3 presents the total number of ACEs experienced by participants. The mean number of ACEs reported by participants was 1.79 ± 0.97.
Frequencies of Individual ACEs.
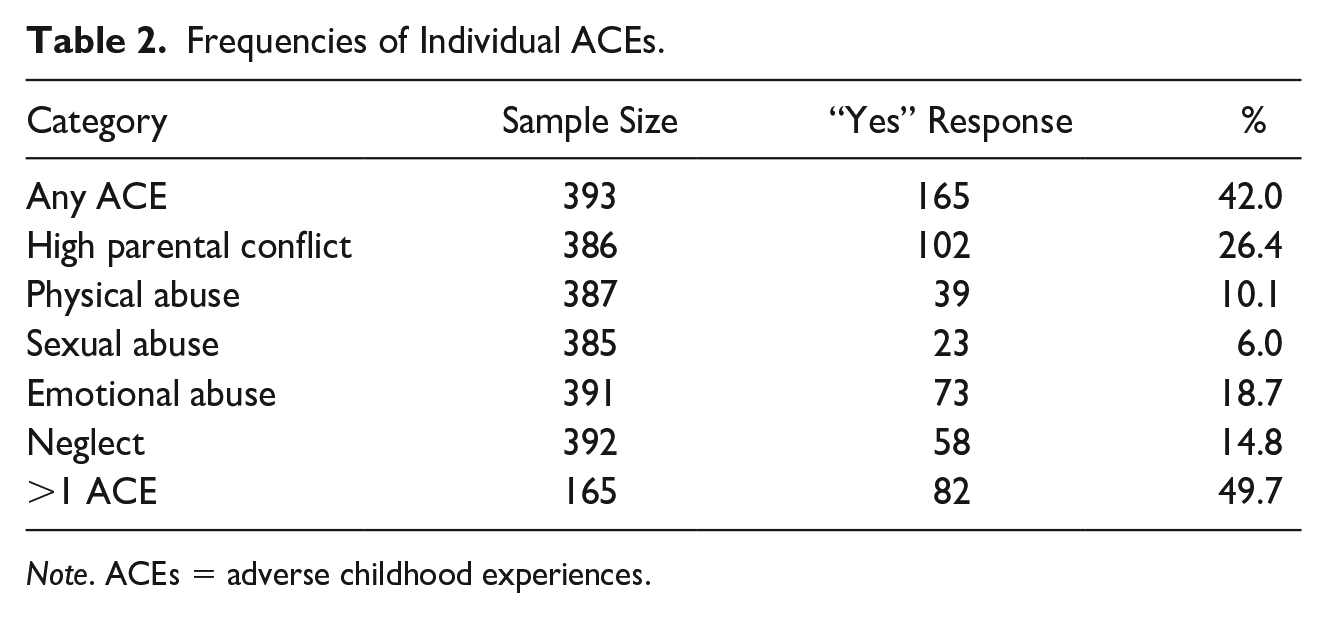
Note. ACEs = adverse childhood experiences.
Frequencies and Percentages Among Participants With ACEs (N = 165).
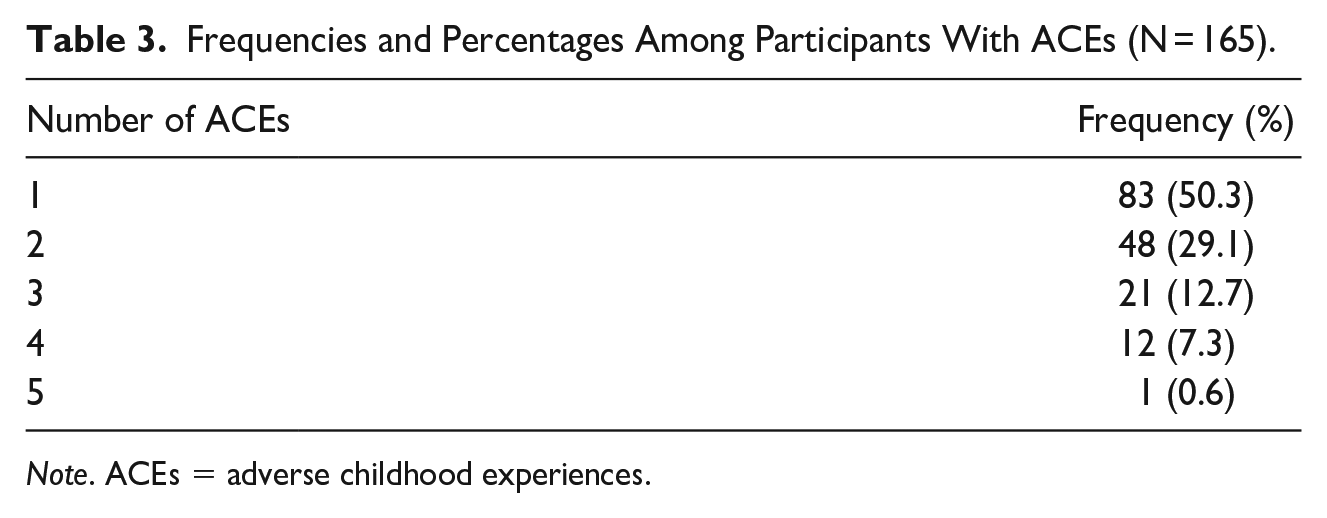
Note. ACEs = adverse childhood experiences.
Mean Group Differences of Participants With and Without ACEs
Participants who reported having an ACE had significantly more relational impairments than those who reported no ACEs. Experiences of adversity in childhood were found to significantly result in three types of relational impairments: ALN; F (1,381) = 5.50, p = .004; IA; F (1, 381) = 4.30, p = .014; and EGC; F (1,381) = 5.03, p = .007. Participants with self-reports of ACEs scored significantly higher in ALN, IA, and EGC scores compared to participants with no ACEs. As indexed by omega squared, 1.50%, 1.58%, and 1.95% of the variances in ALN, IA, and EGC scores were accounted for by ACEs. No significant difference on the SI object relations domain was found between the two groups. The current study had 44% to detect a small effect, 95% power to detect a medium effect, and 99% power to detect large effect if there was one in the population (J. Cohen, 1977). Therefore, there are probably no medium and large effects on the SI type of relational impairment following relational adversity in childhood in this population. The findings are however inconclusive for small effects (Table 4).
ANOVA Results: Mean Differences in Object Relations Impairment by Participants’ With and Without ACEs.
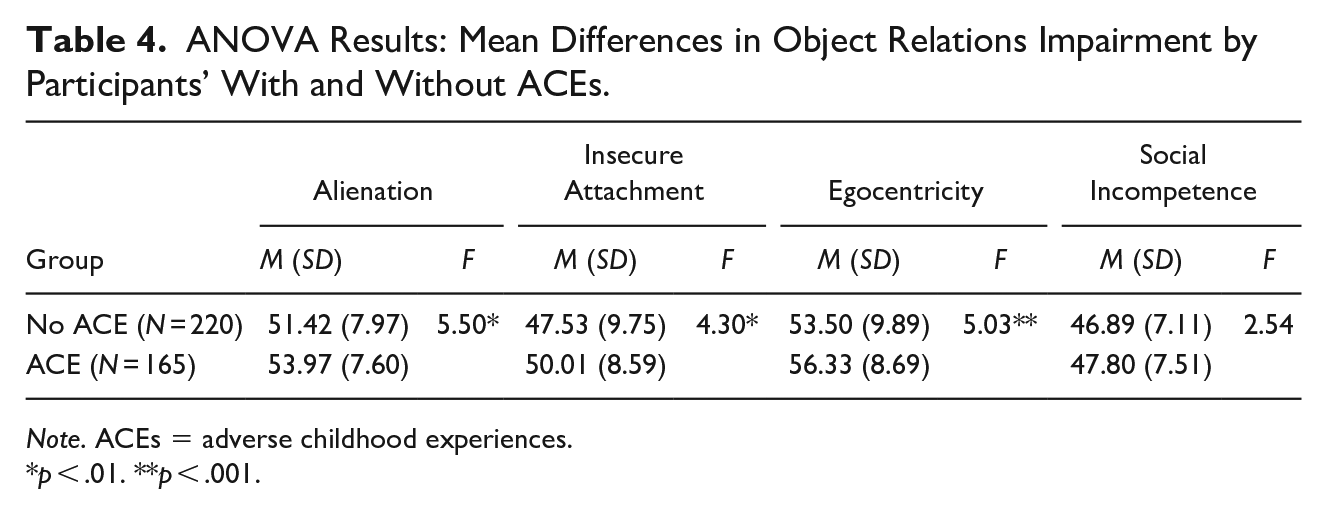
Note. ACEs = adverse childhood experiences.
p < .01. **p < .001.
Associations of ACEs With Adult Relational Impairments
The associations of individual and multiple ACEs with relational impairments are shown in Table 5. For each individual ACE, the associations with relational impairment in the sample were small (J. Cohen, 1988). Sexual abuse was associated with impairments in all four relational capabilities: an inability to experience trust in intimate relationships (ALN; r = .15, p < .001), a sensitivity to rejection and a likelihood of being easily hurt by others (IA; r = .12, p < .05), a tendency to perceive others only in relationship to the self (EGC; r = .13, p < .05), and a self-perception of an inability to successfully engage in social activity (SI; r = .19, p < .001). Growing up in a dysfunctional household with high parental conflict was found to be associated with three types of relational impairments: ALN; r = .17, p < .001, IA; r = .17, p < .001, and EGC; r = .16, p < .001. Physical abuse was found to be associated with one type of relational impairment: ALN; r = .12, p < .05, while emotional abuse was associated with three types of relational impairments: ALN; r = .11, p < .05, IA; r = .14, p < .001, and EGC; r = .10, p < .05. Finally, neglect was associated with all four types of relational impairment: ALN; r = .15, p < .001; IA; r = .11, p < .05; EGC; r = .18, p < .001; and SI; r = .15, p < .001.
Correlation Results: Associations of Object Relations Impairments by ACE Category.
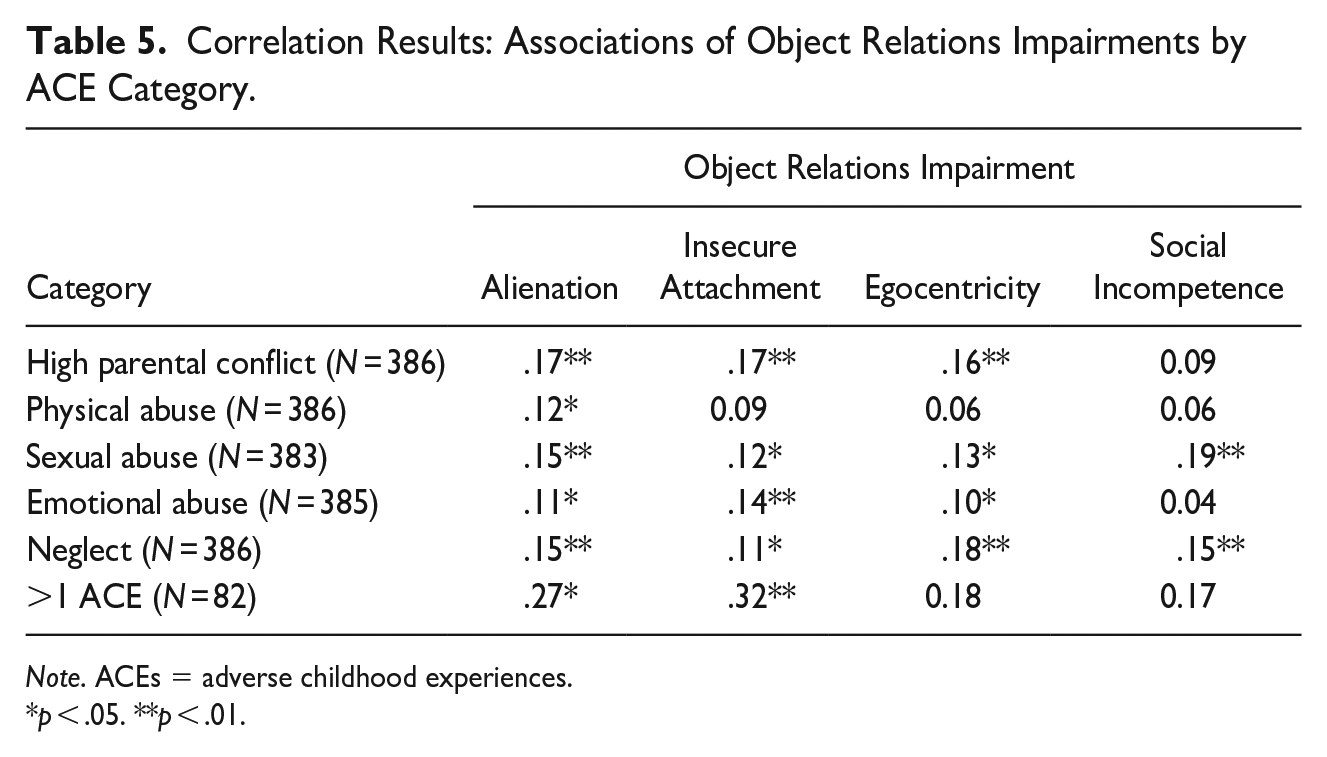
Note. ACEs = adverse childhood experiences.
p < .05. **p < .01.
Relational capability following experiences of more than one ACE was significant for impairments in ALN; r = .27, p < .05, and IA; r = .32, p < .001. The effect sizes of these associations were moderate (Cohen, 1988).
Predicting the Type of Adult Relational Impairment Outcome From Specific ACEs
Hierarchical regressions were used to examine the ability of ACEs to predict each type of relational impairment in adulthood. For all four predictive models, the demographic variables of the three age groups, gender, marital status, and level of education were entered in the first step. In the second step, the five independent ACEs were entered, and in the final step, any two ACEs, and any greater than 2 ACEs were entered.
The regression models were significant for all four types of relational impairments, with 2.3% of the variance in ALN scores accounted for in the final model (F(16,341) = 3.84, p < .001); 2.7% of the variance in EGC scores accounted for by the predictors in the final model (F(16, 341) = 4.18, p < .001); 1.4% of the variance accounted for in the final model for predicting IA impairments (F(16, 341) = 2.88, p < .001); and 0.6% of the variance in SI accounted for by the predictors in the SI final model (F(16, 340) = 1.82, p < .05). While neither of the individual ACE categories nor in combination with another ACE had a significant relationship with relational impairments in adulthood, the demographic variables of marital status and level of education were significant predictors of adult relational impairments following ACEs. It is therefore likely that other variables not included in the current study account for a greater portion of the variances in adult relational impairment in this population. The final models for each type of relational impairment are presented in Tables 6–9.
Final Regression Model for Predicting Alienation Impairments.
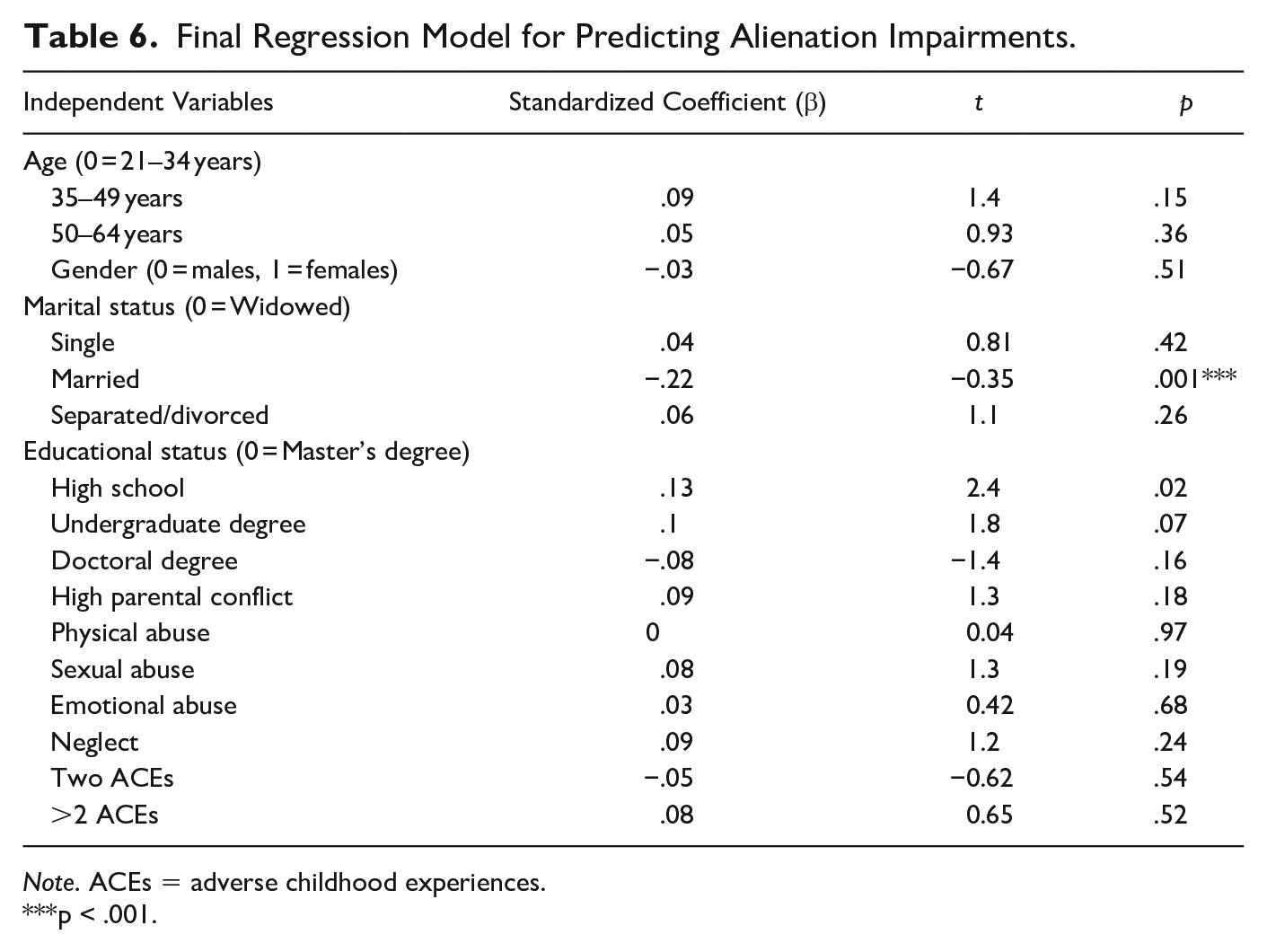
Note. ACEs = adverse childhood experiences.
p < .001.
Final Regression Model for Predicting Egocentricity Impairments.
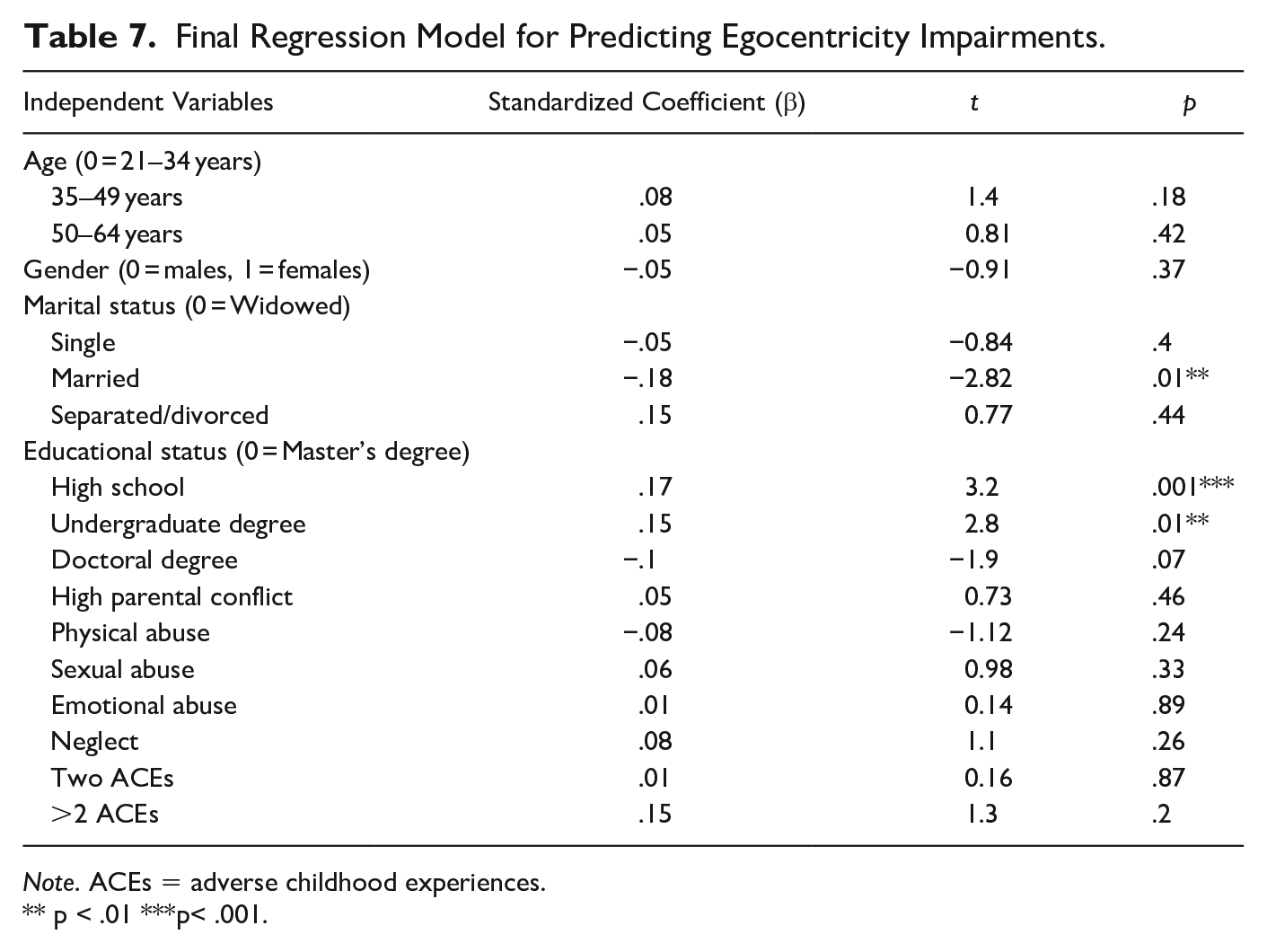
Note. ACEs = adverse childhood experiences.
p < .01 *** p< .001.
Final Regression Model for Predicting Insecure Attachment Impairments.
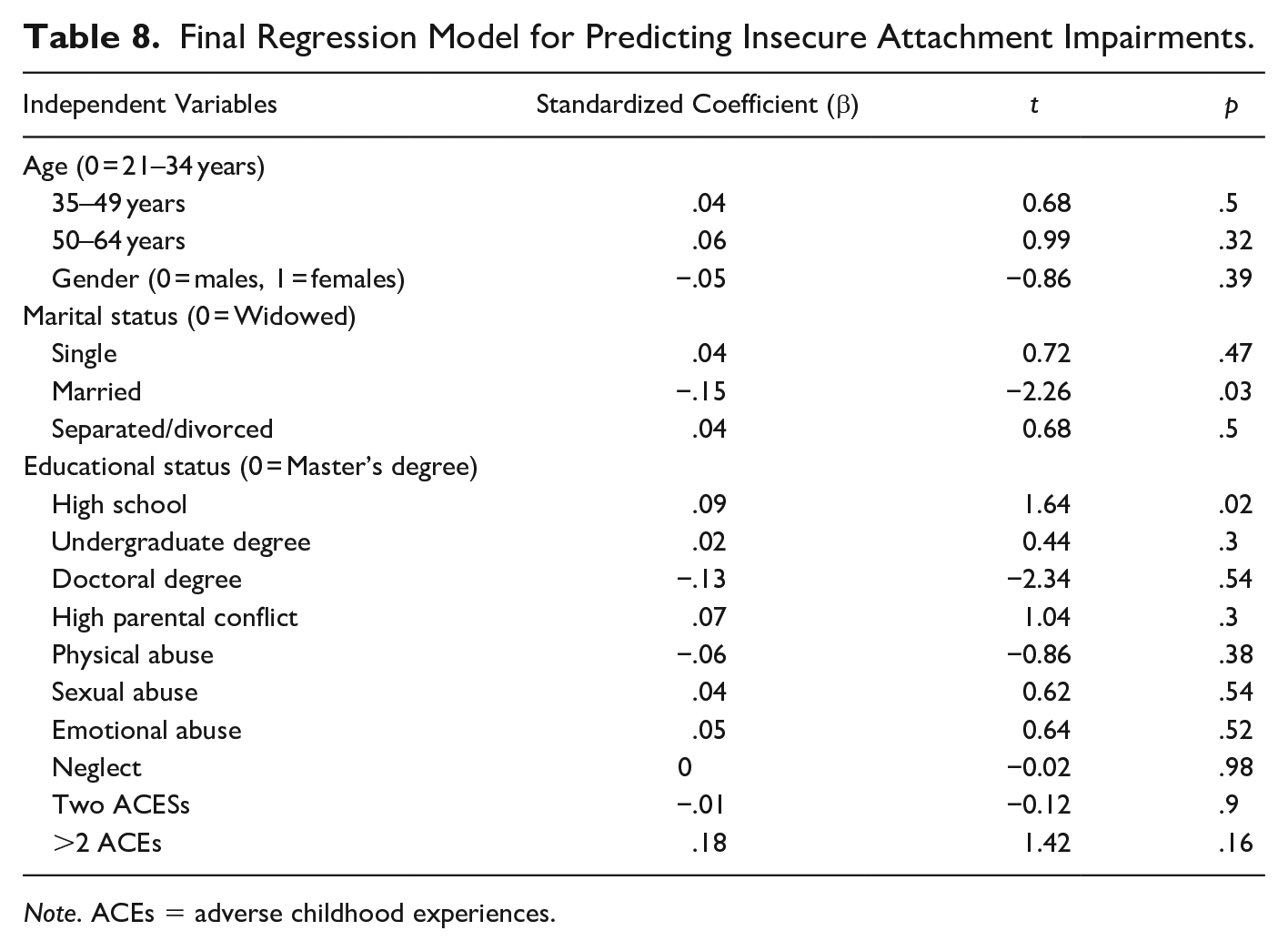
Note. ACEs = adverse childhood experiences.
Final Regression Model for Predicting Social Incompetence Impairments.
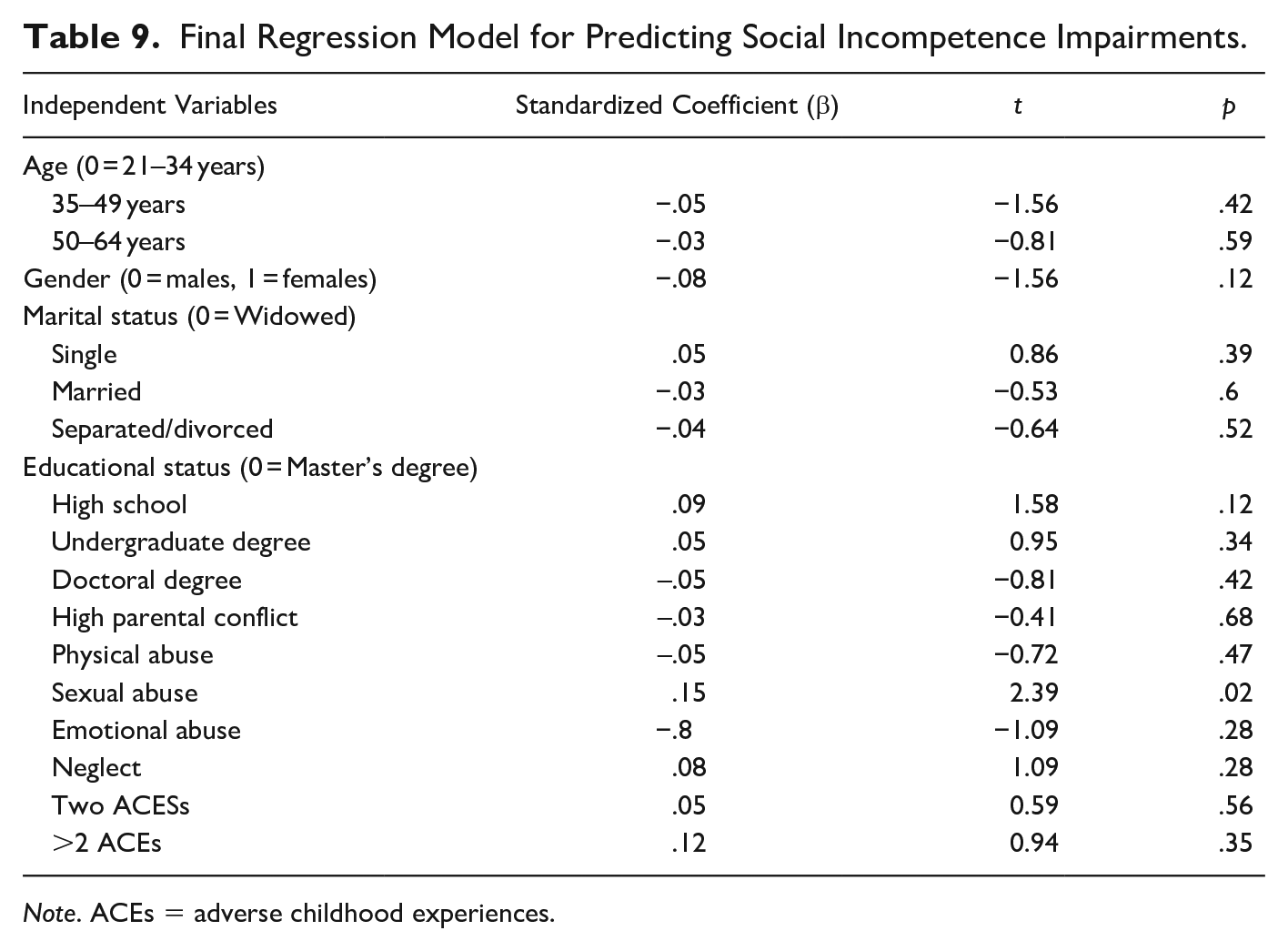
Note. ACEs = adverse childhood experiences.
Discussion
The current study sought to explore the associations of specific relational traumas in childhood with specific types of relational impairments in adulthood using a Ghanaian sample. The study found that while participants who experienced adversity in childhood had more relational impairments compared to participants with no experience of childhood adversity, the effect sizes of these differences were small. Thus, no observable differences in relational impairments exist between participants with ACEs versus those without ACEs in this population.
At the bivariate level, each individual ACE was associated with at least one type of relational impairment. While the strength of correlation was weak for all ACEs investigated in this sample, the cultural variables hypothesized to mitigate ACEs effects may explain these findings. Physical abuse in childhood’s low association with relational impairment in adulthood for example, is likely due to culturally accepted corporal punishment practices (e.g., Alhassan, 2013; Lokot et al., 2020) that take literally the biblical admonition to not spoil the child by sparing the rod.
In addition, although the global literature shows that the more ACEs a person experiences, the more at risk that person would be for social and emotional impairments (e.g., R. A. Cohen et al., 2006; Nurius, 2015) in adulthood, the study found that demographic variables such as marital status and education were better predictors of relational impairments in the sample than either a single or multiple ACEs. In addition, the present study’s finding that over half of the sample endorsed no ACE is dissimilar to findings from studies conducted in Western countries in which over half of participants report experiencing at least one ACE. In seeking to understand this finding of low ACEs in this sample, it may be possible that some participants in this study underreported their ACEs in line with cultural dictates of “not washing one’s dirty linen in public” (e.g., Amoakohene, 2004), while other participants were in denial of, or had repressed ACEs in order not to burden their loved ones (e.g., Dressler, 1985, Engelbrecht & Papaikonomou, 2018) in line with collectivist values. This hypothesis will need to be tested in further studies with different community samples in Ghana.
Another understanding of the study’s findings can be related to other cultural variables such as the culture’s high religiosity (c.f. Kyei et al., 2014), which has been found to be a protective factor for resilience in the global literature (e.g., Pokimica, et al., 2012; Powell et al., 2003; Rosmarin et al., 2009). In addition, communal mastery, that is, “a sense that individuals can overcome life challenges and obstacles through and because of their being interwoven in a close, social network” (Hobfoll et al., 2002, p. 856), with one’s extended family, neighbors who play surrogate familial roles, or belongingness in a religious community, may be a protective factor against severe impairments in relational capabilities following ACEs in this setting.
Implications for Research and Practice
The study’s findings suggests that cultural norms can mitigate against ACEs, although further studies are needed to understand how these norms can be employed to mitigate the effects of relational trauma in both child and adult survivors in the Ghanaian context.
In addition, while the study did not find relational impairments to be significantly different between participants with ACEs and those without ACEs, different findings may exist within different populations in the country, such as those from lower socioeconomic status (SES) households. Studies with a qualitative focus could therefore uncover specific resilience capacities in individuals with ACE histories that could aid in the tailoring of effective interventions for individuals with past and/or current trauma histories.
Limitations of the Study
This study has a number of limitations, such as the retrospective and self-reported nature of the obtained data which could not be verified. In addition, the childhood socioeconomic backgrounds of participants were not investigated, and this could have possibly provided a better understanding of children at risk of ACEs in this setting. Chronicity of abuse was also not assessed and thus it is unknown whether chronicity of abuse would result in more relational impairments compared to acute experiences of ACEs.
Furthermore, the high functioning and highly educated characteristics of this sample limits the generalizability of the study’s findings to lower functioning and less educated individuals in the country who may be less resilient. Future studies will therefore need to investigate the outcomes of ACEs on relational impairments from different socioeconomic classes in the country for a more accurate understanding of ACEs impact on relational capabilities. The associations of ACEs on physical health outcomes were also not assessed, which if similar to findings from studies using Western samples, can better inform public health policy in the country. Finally, neither factors which could have moderated participants’ experiences, such as the relationship of perpetrators to survivors, nor unobserved factors (e.g., social support, parental education) which can impact relational capabilities were investigated in the study.
This study however provides a starting point for examining the prevalence and negative associations of ACEs on adult interpersonal functioning as well as adult physical and mental health outcomes in cultures like Ghana.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.