
Abstract
In the United States alone, 10 million people are affected by family and domestic violence (DV). DV survivors experience many forms of victimization, including physical, psychological, and sexual abuse resulting in trauma. The DV workforce, including healthcare providers, social workers, advocates, and other providers, utilize trauma-informed care in a variety of settings to help DV survivors heal and recover from their traumatic experiences. Given the intensity of DV work and occupational stressors associated with navigating complex survivor cases and systems of care, health and mental health professionals can experience burnout, compassion fatigue, and secondary traumatic stress. The purpose of this qualitative study was to explore how professionals in the DV workforce, including healthcare and mental health professionals, experience and mitigate occupational stress. Twenty in-depth interviews were conducted with DV professionals, who worked in medical settings like urban hospitals as well as DV shelters and rape crisis centers in Boston, MA. A semistructured interview guide was developed, and pilot tested and addressed the following topics including experiences of occupational stress, and mitigators of occupational stress. The interviews were audio recorded, transcribed, and analyzed using a thematic analysis approach. Codes were organized into themes and subthemes, which were reviewed and refined during research team discussions. Risk factors of occupational stress included caseload quantity and intensity, workplace isolation, and length of time in the field. Protective factors spanned individual, interpersonal, and organizational level factors. Participants described various strategies for mitigating occupational stress, including training, supervision, and self-care. Findings from this study have the potential to inform policies and practices among healthcare organizations that support professionals in the DV workforce who work with DV survivors.
Keywords
Background
Healthcare and mental health professionals in the domestic violence (DV) workforce who work with DV survivors have demanding roles and can experience stress resulting from their roles (Bemiller & Williams, 2011). There is a need for more research on the manifestations, individual and organizational drivers, and mitigators of occupational stress among these professionals to better support professionals who work with DV survivors.
Effects of DV
In the United States alone, 10 million people are affected by family and DV (Huecker & Smock, 2020). Survivors of DV are subjected to many forms of victimization, including physical, psychological, and sexual abuse (Huecker & Smock, 2020). The effect of the violence can result in a myriad of physical and emotional health outcomes, including, in more severe cases of trauma, depression and anxiety (Sullivan et al., 2018), and other physical and mental health outcomes (SAMHSA’s, 2014).
In one study of DV survivors, mental health outcomes included anxiety and depression, while physical health outcomes include injuries and chronic diseases including osteoarthritis (Coker et al., 2002). In addition to the physical and emotional repercussions of experiencing DV, survivors can also feel like they lack autonomy, power, and a sense of self-worth (Lagdon et al., 2014). A study analyzing the National Violence Against Women Survey, which surveyed women and men 18 years or older, showed that feelings of fear and low-self-esteem can hinder a survivor’s ability to seek care, and drug abuse, sleep disturbance, and suicidal ideation can become coping mechanisms (Carbone-López et al., 2006). For survivors to overcome these feeling and recover, it is critical to provide them with opportunities to regain a sense of control over their lives, make healthy connections, and recognize and recover from their trauma (Sullivan et al., 2018).
Providers in the DV workforce typically work with these survivors using a trauma-informed approach, which is strengths-based, recognizes the cultural context of clients, and supports survivors in gaining a sense of control (Goodman et al., 2016). However, the impact of a survivor’s trauma and addressing it can also take a mental and emotional toll on providers (Yang & Hayes, 2020). Professionals in the DV workforce who work with DV survivors, such as social workers, therapists, and shelter workers, can themselves experience stress resulting from the demands of their roles and professional environments that can be traumatic. Thus, there is a need to better understand how providers who provide care to DV clients experience stressors related to their occupational demands, how this stress manifests, and how it is connected to multilevel factors that contribute to and mitigate this stress.
The Demands of DV Work for Health and Mental Health Professionals in the DV Workforce
Professionals in the DV workforce who work with DV survivors can themselves experience stress resulting from the demands of their roles and professional environments. Rising rates of DV, the high-demand, crisis nature of the work, feelings of helplessness when providers perceive themselves unable to keep clients, coupled with the fact that some DV providers carry their own personal experiences with violence or trauma (Wood, 2017), merits exploring the impact of DV providers caring for DV survivors. DV work is especially demanding given that professionals are in the position of helping survivors, navigate the intricacies of their victimization, interact with complex systems of care, provide ongoing emotional support, and teach survivors to cope with their difficult situations (Macy & Ermentrout, 2008). Furthermore, many DV professionals working with survivors are also exposed to traumatic stories of violence and may find themselves experiencing anger toward their client’s perpetrators (Brown & O’Brien, 1998). In addition to prioritizing client safety, providers can also worry about their own safety and experience adverse reactions to DV caseloads (Baird & Jenkins, 2003). In a questionnaire given to staff of U.S.-based shelters for battered women, most respondents had received threats from a resident’s partner (Stout & Thomas, 1991). In an Australian study of counselors with high DV caseloads, counselors expressed a reduction in confidence and security in their cognitive schema and taking too much responsibility for the clients’ safety when assessing the initial impact of their own DV counseling (Iliffe & Steed, 2000).
Additionally, challenges associated with the organizational environments navigated by DV professionals, which can include limited resources, high caseloads, and poor compensation, can also contribute to provider stress (Maier, 2011; Ullman & Townsend, 2007; Wachter et al., 2020).
Manifestations of Occupational Stress Among Health and Mental Health Professionals in the DV Workforce
Given the demands, complexities, and stressors associated with their occupations, it is not surprising that professionals in the DV workforce who work with DV survivors can experience burnout, compassion fatigue, and secondary stress traumatization (Baird & Jenkins, 2003).
Burnout is defined in the literature as having three key components: exhaustion, cynicism, and inefficacy (Wood et al., 2022). One meta-analysis of 62 studies of mental health providers across 33 countries found that 40% of respondents suffered from “professional burnout” (O’Connor et al., 2018). Though not specific to mental health professionals, a systematic review of 36 prospective studies found burnout to be a significant predictor of numerous health outcomes, including coronary heart disease, type 2 diabetes, as well as mental health outcomes including depressive symptoms and insomnia (Salvagioni et al., 2017). For those involved in DV casework, burnout can more specifically be related to hearing and responding to intense situations, concern for client safety, and watching the client go back to the abuser, limited resources, and work overload (Bemiller & Williams, 2011). For batterer intervention program workers, burnout when working with perpetrators can be caused by stress on the job, depersonalization from a decreased level of agreeableness, and increased feelings of anger (Bahner & Berkel, 2007).
Studies also show that DV professionals who are exposed specifically to traumatic narratives through their professional roles can also experience compassion fatigue resulting from emotional exhaustion. Figley (2002) noted that “The very act of being compassionate and empathic extracts a cost under most circumstances. In our effort to view the world from the perspective of the suffering we suffer.” Among a sample of intimate partner violence and sexual assault providers, compassion fatigue was associated with an organizational environment of chronic stress and traumatic material in addition to factors such as age, years of experience, and workload (Voth Schrag et al., 2021). Previous research has also shown the connection of higher levels of compassion fatigue predicting higher levels of burnout in victim advocates due to similar factors of heightened emotional involvement in clients’ lives and its accompanying stress symptoms (Singer et al., 2020).
Finally, with prolonged exposure to the trauma of others, secondary traumatic stress (STS) can also occur, described by Figley (1995) as “the natural and consequent behaviors and emotions resulting from knowing about a traumatizing event experienced by a significant other—the stress resulting from helping or wanting to help a traumatized or suffering person” (p. 7). Studies show that the symptoms of STS are similar to post-traumatic stress disorder, including nightmares, difficulty sleeping, and other psychological responses (Bride, 2007). An extensive literature documents the pervasiveness of STS, mainly among social workers (Benuto et al., 2019). Studies show that other types of providers, for example victims’ advocates (Slattery & Goodman, 2009) and rape crisis center staff, also experience STS (Dworkin et al., 2016). From a systematic review of adult protective social work in gerontology, re-experiencing of a survivor’s traumatic event can lead to avoidance toward the client, isolation from colleagues, and ignoring problems that arise personally as well as detachment from work, emotional exhaustion, cynicism, job inefficacy, and a lack of sense of purpose (Bourassa, 2009). Cognitive shifts through vicarious trauma, including guilt, fear, and powerlessness, can be initiated by intrusive imagery in flashbacks, thoughts, and emotions specifically in situations of safety and trust, and intimacy and control (Baird & Jenkins, 2003). In a study of family violence and sexual assault social workers, the likelihood of experiencing STS varied based on a worker’s ability to separate their own emotions from their clients’ traumatic experiences especially if the social worker has had personal traumatic events in their life (Choi, 2011).
Factors Associated with Manifestations of Occupational Stress Among Health and Mental Health Professionals in the DV Workforce Who Work with DV Survivors
A variety of patient, provider, and organizational level factors are associated with manifestations of occupational stress among professionals in the DV workforce who work with DV survivors. Yang and Hayes (2020) systematically reviewed 44 studies focused on psychotherapists’ burnout and identified predictors of burnout ranging from organizational factors such as job control, workload, and caseload to factors specific to the psychotherapist, including history of mental health, psychological distress, self-efficacy, and coping strategies. In a meta-analysis of 38 studies of 17 risk factors for STS among professionals (including DV workers) working with trauma, significant risk factors included caseload frequency, volume, and ratio and having a personal trauma history (Hensel et al., 2015). Other studies have examined organizational characteristics such as sociopolitical support, organizational strategic information, performance feedback, and supervision quality (Choi, 2011).
However, there are also inconsistencies regarding risk factors that lead to occupational stress in the literature. For example, Voth Schrag et al. (2021) found a significant relationship between perception of one’s organizational climate and burnout in a study of intimate partner violence and sexual assault providers while Kim et al. (2018) found no relationship between organizational climate perceptions and emotional exhaustion among community mental health therapists. Other studies have shown that a sexual assault trauma provider’s own personal history of trauma can also impact their level of occupational stress (Ghahramanlou & Brodbeck, 2000). Some studies have demonstrated increased emotional exhaustion and greater emotional involvement with trauma victims among younger DV providers with less experience and heavy caseloads (Baird & Jenkins, 2003). DV providers may experience stress from watching their clients returning to unsafe situations, listening to difficult stories (Kulkarni et al., 2013), managing clients’ transition to shelter life, and letting go of “being the hero” (Merchant & Whiting, 2015). In a study of DV and sexual assault shelter workers, these advocates reflected on their beliefs of meaningful sacrifice as a component of their work and noted that their heightened sensitivity to the well-being of others made them more susceptible to sacrificing their own well-being (Bemiller & Williams, 2011). Beyond further understanding the risk factors for occupational stress associated with providing this type of intensive, therapeutic care, it is critical to understand mitigators of occupational stress.
Mitigators of Occupational Stress Among Health and Mental Health Professionals in the DV Workforce Who Work with DV Survivors
Studies have found that a variety of factors at the individual, interpersonal, and organizational levels help DV professionals mitigate and manage experiences of occupational stress (Dworkin et al., 2016). For instance, individual-level restorative activities can help DV providers create a balance between their work and their personal lives, which allows them to better avoid compassion fatigue and STS (Kulkarni et al., 2013). In a systematic review of burnout among mental health professionals, adaptive coping strategies, including leisure activities, mindfulness practices, and utilizing social support networks, with work-related self-care activities such as avoiding overtime work, receiving psychotherapy, and setting client boundaries were especially important for therapists with difficult work demands (Yang & Hayes, 2020).
Interpersonal-level factors including peer support and cohesive communication within a team have also been shown to reduce occupational stress. In a study of shelter workers who had DV caseloads, the feeling of personal accomplishment and self-efficacy, especially if facilitated by workplace support, aided shelter workers in reducing burnout when they had high work demands (Baker et al., 2007). In a study of DV advocates, coworker support protected against adverse provider effects such as STS (Slattery & Goodman, 2009). Finally, at the organizational level, the literature shows that strategies including training, supervision, and organizational resources are most relevant to the health and well-being of TIC DV providers (Babin et al., 2012). In a study of victim advocates, increased autonomy at work and improved supervision decreased secondary traumatization and burnout (Benuto et al., 2019). Studies have also shown that training programs focused on trauma allow for DV providers in training to learn to separate between their professional and personal selves, which, in turn, improves their perception of their role competence and self-care practices (Ben-Porat & Itzhaky, 2011).
While there is some evidence of the manifestations, risk factors, and mitigators of occupational stress among DV professionals, there are gaps in this evidence that merit further investigation. First, there is a critical need to continue to better understand the impact of providing DV care on providers themselves (Britt et al., 2021), particularly given the growing concern about increasing rates of DV punctuated by the COVID pandemic and the increasing need for these professionals (Wood et al., 2022). While much of the existing research is based in nonclinical settings and with specific DV provider groups such as social workers or therapists, this study includes clinical DV providers spanning various departments. Second, there is a need to better understand protective factors that mitigate occupational stress at multiple levels as posited by the socioecological model (Bronfenbrenner, 1989) including at the at the organizational level so that organizations can ultimately support the emotional and physical well-being of many different types of DV professionals and promote workforce stability (Molnar et al., 2017). To address these gaps in the scientific literature, we conducted a qualitative research study to identify and understand the (a) manifestations of occupational stress, (b) risk factors of occupational stress, and (c) protective factors of occupational stress among DV health and mental health professionals. The results of this research uniquely contribute to greater DV literature by offering insight into how factors at multiple levels, that is, individual, interpersonal, and organizational levels, interconnect as they impact DV providers practicing trauma-informed care (TIC) in various clinical settings.
Methods
Study Sample
Healthcare and mental health professionals in the DV workforce who work with DV survivors in the Boston area were selected into the study via purposive sampling (Naderifar et al., 2017). The first author attended a conference organized by The Domestic Violence Program Evaluation and Research Collaborative and was introduced to DV professional networks at this event. Through the initial introduction of a clinical social work director of violence and recovery, the researcher enrolled her first participant and continued recruitment with the director’s colleagues. After each addition of a participant for an interview, the participant shared contact information for additional study candidates. Snowball sampling (Naderifar et al., 2017), in which professionals were asked to spread the word about the study to peers in their networks, was also used to sample participants. Participants consisted of 20 health and mental health professionals, including doctors, nurses, clinical social workers, and medical advocates who all work with survivors of DV at various institutions, including hospitals, medical advocacy organizations, DV shelters, and mental health clinics and practices, in Boston, MA. Forty-five percent of participants were clinical social workers in emergency, trauma, general medicine, a center for violence and recovery, and primary care units in medical settings. Fifteen percent of participants were therapists, and the other 15% were medical advocates at a rape crisis center. Ten percent were sexual assault examiners, and the remaining 5% had the roles of nurse, doctor, and shelter worker.
Data Collection
A semistructured interview guide using the existing literature was created to explore the views, perceptions, and experiences of health and mental health professionals who work with DV clients. The socioecological model in public health (Bronfenbrenner, 1989) also guided the development of this guide to ascertain how societal factors at multiple levels of influence, including the individual, interpersonal, and institutional/organizational level, impact these professionals (Kilanowski, 2017). The interview guide was reviewed by the second and third authors and additionally modified based on an interview review test with 30 members of the first author’s Applied Qualitative Research Methods course at her university. The guide consisted of open-ended questions and probes pertaining to the participant’s role and experiences providing care to DV clients, manifestations of occupational stress, perceptions of supervision, training, and self-care practices. Once participants were identified, the first author scheduled a time via email to meet at a location chosen by the participant. Written consent was obtained prior to the interview, and ongoing consent was secured periodically throughout the interview. Interviews were conducted in English and audio recorded. Interviews lasted between 15 and 45 min (average: 35 min), and an Amazon gift card of $10 was given at the end.
Human Subjects Statement
The first author obtained human subject research approval from the Social, Behavioral, and Education Research Institutional Review Board from the authors’ university on 10/18/19 (IRB number #1910006). Confidentiality was maintained in all procedures in accordance with the research protocol approved by the Institutional Review Board (IRB).
Data Preparation and Analysis
Template thematic analysis was identified as a concrete method for data analysis that enables identification of themes across data to develop hierarchical coding (Brooks et al., 2015). This included familiarization with the data, preliminary coding, generating initial themes, modifying the initial coding template to then apply the final template to the full data set, and defining and naming themes. Audio recordings were listened to and transcribed by the first author, and the transcriptions were uploaded onto a secure platform for analysis. The quality of the data collection was also noted in terms of level of detail in responses and the qualities of the interviewing, recording, and note-taking processes (Braun & Clarke, 2006). Prolonged engagement with the data allowed for a better development of codes and themes in Lumivero’s NVIVO (Version 12.5.0; 2019). Credibility was maximized through prolonged engagement with the data and collaborative coding (Cope, 2014).
A hybrid, deductive, and inductive approach to coding was undertaken, and all coding occurred in NVIVO (Version 12.5.0; 2019). A hybrid approach was undertaken because of the interest in commencing the analysis with a short list of codes central to the research question, such as occupational stress. There were seven a priori codes developed based on a review of the literature and the research question; however, the vast majority of codes were developed inductively. There were 31 inductive codes, consisting of 13 codes and 18 subcodes.
Collaborative coding between the first and third authors of the thickest (richest in content) interview at the time of early codebook development (MacQueen et al., 1998) produced a robust codebook, which enhanced transferability. Through this process, labels and short-hand designations were used to assign meanings to the transcript. Open coding, or initial coding, allowed every transcript to be labeled with codes and the large quantity of 28 initial codes allowed for a refinement in a more focused, second round of coding (Braun & Clarke, 2019). Codes were reflected on individually to then identify patterns throughout the data in order to draw shared meanings that were underpinned by central concepts or ideas. Themes were given working titles, and, at this stage, there were 4 overarching themes and 19 subthemes. Prevalent themes were broken down into subthemes to make the data more digestible for analysis. The structure of themes and subthemes were also refined through consensus between the first and last author and codebook modifications were made. Networks between themes and subthemes were described and explored to reveal more global, overarching ideas. Through triangulation, peer examination, and an audit trail of the codebook, dependability was also maximized (Guest et al., 2020).
Participants were recruited until it was deemed that sufficient information power (Malterud et al., 2016) was achieved, meaning that the data collected were discussed and examined by the authors alongside the descriptive aims of the study and the quality and the duration of the interviews. The first author, who collected all the interview data, was extensively trained over 4 months on qualitative data collection and analysis, and thus, the quality of the interview data collection was strong. Ultimately, data were collected from 20 participants.
NVIVO was used to organize the coding process and visualize the number of codes and emerging themes in the transcripts.
Results
This qualitative study of health and mental health professionals in the DV workforce identified three overarching themes consisting of risk factors of occupational stress, key manifestations of occupational stress, and protective factors of occupational stress among these providers (See Figure 1). Risk factors included high caseloads, case complexity, length of time in the field, workplace isolation, and a challenging work environment. Manifestations of occupational stress were physical and emotional burnout, STS, and changes in self-view. Finally, protective factors were identified at the individual- (e.g., individual self-reflection), interpersonal- (giving and getting support), and organizational-level protective factors (e.g., institutional culture of self-care). These findings are described in greater detail with illustrative quotes below.
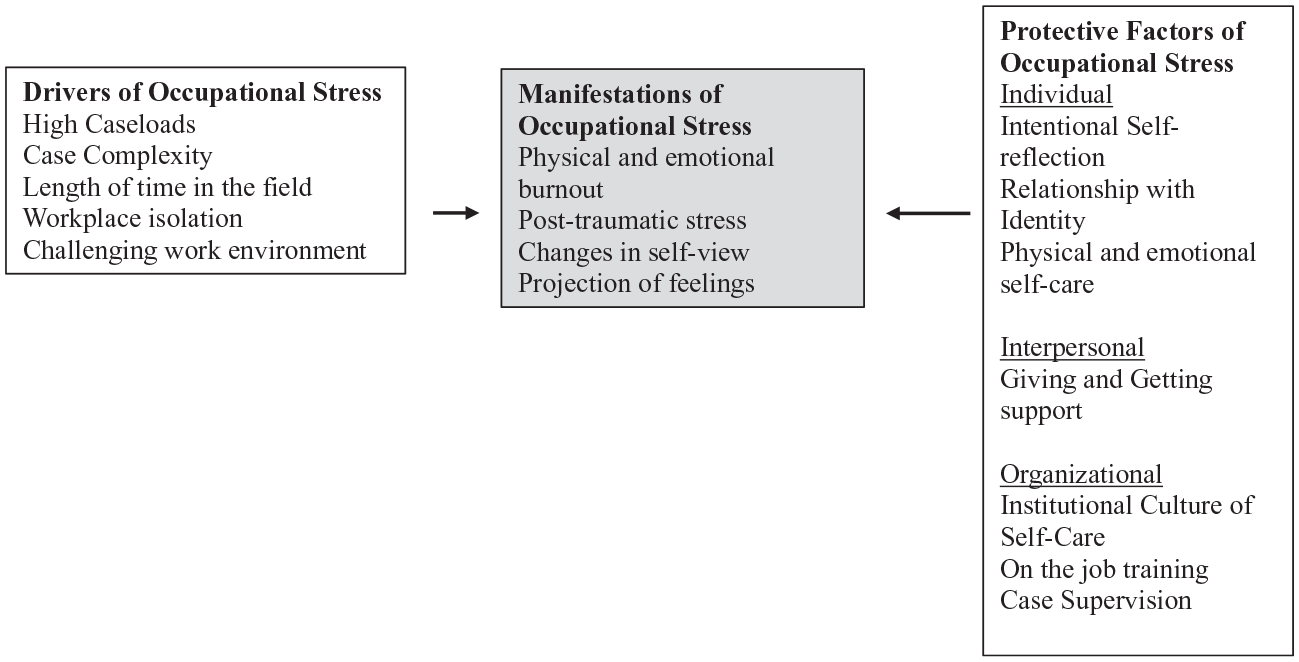
Manifestations, drivers, and protective factors of occupational stress.
Theme 1: Risk Factors of Occupational Stress Among DV Workers
Providers discussed many risk factors contributing to manifestations of occupational stress. The five factors most mentioned were high caseloads, case complexity, length of time in the field, and workplace environment. These factors were described as resulting from inadequate staffing resources to match the needs of cases that can span specialties. As shared by participants, care of DV patients requires specific considerations that may come up against obstacles such as loud and bright medical settings that are not conducive to strategies and techniques implemented in TIC. Furthermore, providers noted facing unique challenges when operating in high-intensity environments of compounding stressors and responded differently based on their prior professional experience. When provider teams including social workers, doctors, and psychiatrists must collaborate for an individual patient’s care, a supportive peer environment was shared by participants to be important especially within challenging physical environments.
“Being Pulled in Ten Different Directions”
Several participants noted that heavy caseloads resulting from having limited staff contributed to occupational stress. With each case requiring adequate attention and resources, the heightened demand for each individual provider due to staff limitations increased the stress and busyness of an already fast-paced medical environment. This was especially true for providers working in emergency departments and cases that required coordination across different provider types and departments. A clinical social worker shared that as a hospital, they had “been struggling with acuity, which means a higher demand and not enough of you to meet the demands—the time, the energy, the resources” (Participant 2). With larger caseloads, a different participant noted feeling that I’m being pulled in ten different directions because there may be ten different cases that are really tough when all of it is happening at once that’s when I notice the negative talk I hear from others pick up too (Participant 7).
Being pulled in different directions was especially true for an emergency department manager, who is “called in a million different directions, I don’t get to spend more than 5 or 10 minutes at most with a patient, and during that time I might be interrupted 5 times” (Participant 6).
“Cases That Really Stick With You”
Case complexity, in the form of high-risk or resistant patients, also impacted provider occupational stress. Providers are aware that DV patients often times come in with multilayered experiences and comorbidities, which require a high quality of care and sensitivity. By taking into consideration each patient’s identities, many providers shared that this leads to frequently responding to cases that hold a particular weight that can be long-lasting. Cases that involved children or multiple negative experiences with the medical system were described as some of the hardest cases providers looked back on.
A general medicine clinical social worker reflected on this noting, When someone is resistant to receiving care, especially if they’re homeless, struggling with addiction, have an extensive trauma past, they haven’t necessarily always received trauma-informed care. . .they can come in very guarded, very distrustful, and it’s hard to build rapport with someone in a short-term environment (Participant 11).
One psychologist described a previous work experience where she “saw a lot of really sick people, chronically traumatized, a lot of homeless, substance-abusing people, had a lot going on for them and it was a high burnout experience” (Participant 15). A clinical social worker predominantly working with children discussed challenging cases involving DV and child protection issues, noting that there are “certain cases that really stick with you where there’s a lot of levels of complexity and maybe risk, it can be DV or risk to the child, where you go to bed at night and you think about it” (Participant 20). A clinical social worker within a medical surgical department shared that she finds it helpful setting those boundaries with difficult patients, going in at the offset and saying “I have 10 minutes I wanted to check in” so you don’t get stuck in there for an hour and barraged by all the things they’re putting out. . .I kind of start to know I’m feeling fatigued or burnt out. . . switching from a “what happened to them” perspective to a “what’s wrong with them.” When at that point I realize I need to take a step back and reevaluate what I’m doing and how I’m thinking and maybe take a pause form that [patient] (Participant 4).
One medical advocate described struggling when observing complex patients being treated by providers who lacked TIC training, acknowledging that as providers, “. . .seeing survivors who may have multiple forms of marginalized identities, or historically marginalized identities by society, not getting the same level of care can be really hard” (Participant 19).
Professional Confidence and Length of Time in the Field
Several providers connected the length of treating DV clients to their feelings of professional confidence. Those who were well-seasoned in their field perceived the benefit of having many years to learn how to navigate workplace stressors, caseload management, operating with interdisciplinary clinical teams, and finding solutions to feelings of burnout. Pressure from peer perceptions or personal criticisms were shared more commonly from providers who had been in the field for a shorter period of time. These newer providers also expressed a focus on learning and improving their growing skillset.
A clinical social worker on the acute surgical trauma floor had been professionally working for 3 to 5 years and noted feeling a little bit of imposter syndrome. . . I’m in the process of getting my independent licensure now so that will make me feel a little more established even though it doesn’t necessarily mean very much in terms of the actual day to day (Participant 7).
An emergency trauma surgical ICU social worker at the beginning of her career questioned how could I be a person to fix this or help this person, or what if they’re not safe. But as I had more experience, I became more comfortable with that and learning the resources in the community and getting more information about the services that they can provide (Participant 8).
A manager for therapeutic mentorship for children who had been in the field for 20 years commented that “the longer that you work in the field you get more jaded and tired so you have to find your inspiration and your passion throughout and you can’t get overwhelmed by all of the need that’s out there” (Participant 16). A primary care physician who had been in the field for 24 years expressed that “with greater experience at this point nothing would surprise me anymore. . . so I have a greater sense of calm with whatever people disclose to me and that is useful because it helps people relax a little bit more” (Participant 12). Participants did not explicitly connect length of time and professional confidence with occupational stress.
“Feeling Like I’m Doing It On My Own”
Many participants talked about different characteristics of their workplace environments contributing to manifestations of occupational stress including feeling isolated or disempowered in their workplace environments. Other participants mentioned challenges associated with working in fast-paced and triggering medical environments.
A clinical social worker “found one of the biggest things that’s led to compassion fatigue and burnout for me is feeling like I’m doing it in isolation, feeling like I’m doing it on my own which over time feels pretty ineffective” (Participant 5). Similarly, a primary care provider felt as though she’s “not in a safe environment, there’s no transparency, there’s no peer support, no collaboration, no empowerment” which she found the symptoms of that are that people pick up coping mechanisms that are not so great to be able to survive, so just like a trauma survivor, maybe they become avoidant, they come they get their work done, they get out of there to another job which is what I do (Participant 12).
In addition to feeling isolated in workplace environments, many of the participants who worked in medical environments described the unique challenges associated with these types of fast paced and triggering workplace environments. One medical advocate noted that “the actual [emergency] room is not that trauma informed” with harsh lighting and uncomfortable beds (Participant 10). A clinical social worker for violence and recovery described the intense hospital environment of a hospital where providers deal not only with mental trauma but medical trauma as well, noting “I don’t think people realize how triggering hospitals are. We’re loud, we’re noisy, it’s fast-paced. People often have not only sometimes trauma in the community but also medical trauma, so a lot can get triggered” (Participant 2). An emergency department clinical social worker noted that “the emergency department is so fast paced it’s hard to breathe and it’s hard to take time and pause. I think the fast-paced nature of it has really burnt me out a bit” (Participant 8). The same participant described the difficulty for patients in performing breathing and mindfulness exercises in a loud and stimulating environment such as the emergency room and “the feeling of not knowing what happens to a patient when they leave the emergency room becomes really challenging, you’re going through a whole process of grief” (Participant 8).
Theme 2: Manifestations of Occupational Stress Among DV Workers
Manifestations of occupational stress described by providers included physical and emotional burnout and STS, mirroring feelings, and changes in self-view. The specific experience of interacting with DV survivors and stories on a regular basis was seen to impact providers significantly at work and even in their personal lives. Some reported a heightened sense of hypervigilance and disturbance listening to stories involving violence.
“I Wasn’t Being My Full Self”
Most providers spoke about manifestations of physical and emotional burnout and corresponding impacts resulting from the nature of their occupation. The physical aspect of burnout included irritability, exhaustion, and a lack of sleep, while the emotional aspect included difficulty connecting with others and feelings of frustration both at home and at work. Being aware of this burnout can lead providers to reflect on the sustainability of continuing this work in the long term. One clinical social worker for violence prevention and recovery shared, “I’m tired, I feel irritable, I don’t want to listen; I’m exhausted. I’m sleep-deprived” which led to her feeling “kind of in this rut, feeling stuck sometimes within the work. . .I was going back-to-back from person to person and I wasn’t being my full self” (Participant 2). A therapist commented that “my clients have indicated before that they think I’m some sort of perfect human being that doesn’t experience any distress or burnout or anything, but we’re human beings as well. Therapists can carry a lot with you” (Participant 15).
Many providers discussed different consequences of burnout including compassion fatigue and negative talk. A former shelter worker noted that “sometimes in other people who have done this work much longer than I have is that they lose their sense of compassion for survivors, and not on purpose” (Participant 14). A clinical social worker discussed the manifestation of burnout in negative talk noted in colleagues, it kind of comes out in ways that I try to be mindful of and I can help to modulate more but I think when other folks are really taxed I notice the negative talk and I see that as a sign of burnout (Participant 7).
The impact of burnout was also noted to affect provider job satisfaction. A participant mentioned “every other week I want a new job” (Participant 16). Similarly, a therapist understood her job’s stresses to be unsustainable, realizing that I really love the work but I definitely don’t want to keep doing it. That’s how I’m seeing compassion fatigue and burnout manifesting. . .even though I’m passionate about the work and the families I work with, I know it’s not sustainable (Participant 17).
One medical advocacy coordinator noted I get really frustrated or angry easily about things that have no reason to be angry or frustrated about, so I need to take a step back or ask for help. It’s cyclical. If you’re doing well, you burn out, and you forget you burn out again, you continue and it’s like a spiral and you’re going to have periods of burnout (Participant 19).
Secondary Traumatic Stress
Participants also described symptoms aligned with STS directly attributable to hearing client stories, experiences, and interactions. A participant talked about the stress of “awful things that people have endured, have lived through. . .it is hard at times to sort of not take that on, to take that home with me” (Participant 5).
Another participant also mentioned her sleep being affected by listening to client stories that were “hard to sit with, you notice maybe sleeplessness or, hypervigilance” (Participant 1). One provider described challenging interactions with patients and the avoidant feelings this raised, describing patients “screaming in your face and swearing at you. . .that can certainly be hard and I start to notice it myself when a consult comes up and I don’t want to see that person, I start to feel myself dreading it” (Participant 4). A therapist acknowledged that “you definitely get kind of numb. I’ll hear stories and think, ‘Oh, but he didn’t throw anything at you, you had a really easy day’” (Participant 17). Similarly, another participant discussed that I think you don’t realize you have [stress] until something bad really happens. Maybe you’re crying and you’re like why am I crying. . .or when you go home and your partner says “I sat in traffic and it was horrible” and you want to say “you want to know what’s actually horrible?”. . .when your partner’s allowed to have a bad day (Participant 10).
A clinical director at a shelter described experiencing nightmares and avoiding violent movies, noting “. . .I avoided movies with overt violence, specifically things related to DV. I just wanted to see light-hearted things” (Participant 9). Notably, another participant articulated that exposure to difficult stories helped her become “immune to seeing bad stuff, like I can watch bad movies, I can respond to something awful happening in front of me and sort of jumping in and that crisis mode of helping in the immediate moment” (Participant 8).
Mirroring Feelings
Listening to client stories and experiences also resulted in several providers experiencing feelings similar to their clients. One clinical social worker shared that while listening to the difficult experiences of her clients, she would “. . .[mirror] what my client’s experiencing. I’m feeling something and maybe because your story represents my history or you look like me, or there’s something unconscious that’s triggering some of my stuff” (Participant 2). A violence and recovery clinical social worker reflected that she has had many “clients that have felt close to home, like they’ve experienced something that someone I know has experienced and that’s felt particularly triggering, or something about that patient that reminds me of myself” (Participant 5). Several providers talked about the important of distancing oneself from their patient’s traumatic experiences as noted by a primary care social who remarked “It’s seeing everyone’s trauma and not reacting with your own stuff, it’s holding your own stuff” (Participant 18). A medical advocacy discussed the complexity associated with emotionally detaching from clients stating You need to distance yourself emotionally from this work in order to sustain it. At the same time, it can get to a point in which you’re not able to be empathetic because you’re feeling that too much or you’re distancing yourself too much (Participant 19).
Changes in Self-view
Several participants described experiencing changes in their own perspective and beliefs related to themselves and others in response to caring for DV clients. These providers were able to reflect on how their work changed their greater outlook over time. A clinical social worker specializing in violence and recovery noted that each story alone has an acute and cumulative impact “just sitting with these really tough stories, day in and day out, that shifts your worldview” (Participant 1). The manifestation of this worldview was particularly jarring when the participant had a nightmare that she would “be assaulted at some point while running in the woods by myself. And it wasn't a completely distressing thought, but that was what was more notable for me is that it didn't distress me” (Participant 1). A manager and sexual assault examiner for an emergency department who has been doing this work for 25 years felt a shift in her professional mindset over time, that “I had to make a difference, I had to be the savior, and if I didn’t do that I was a failure. I took everything really personally. . .” (Participant 6). Another participant, a manager for medical advocates described a shift through loss of creativity “like you don’t want to do anything creative you just want to do things as they are, as well as your work life, you’re not allowing yourself to have new ideas or to accept new ideas from other people” (Participant 10). One participant felt more distrustful due to the nature of her work at a DV shelter, giving the example that when she hears of “new relationships in my clients’ lives, I don’t trust the other person or I don’t trust their judgement and that’s not helpful to be honest” (Participant 9).
Theme 3: Multilevel Mitigators of Occupational Stress Among DV Workers
Finally, providers reflected on factors that mitigate experiences of occupational stress noting factors at the individual, interpersonal, and organizational levels. Most commonly identified factors included self-reflection and physical and emotional self-care, social and structural support on the job training, and case supervision from senior professionals. Providers closely examined their own degree of self-knowledge toward their experiences with occupational stress and how this understanding may influence their professional outlook and self-care strategies. Some took into consideration in their self-reflections how their personal identities may assist in their ability to connect with patients from various backgrounds. Throughout the theme of mitigating occupational stress, the methods of receiving support, whether through technical training or empowerment from colleagues across levels of seniority, were highly beneficial to all participants. Feeling connected to a caring team gave many providers an outlet for brainstorming patient obstacles and a sense of fulfillment toward the important work of TIC.
Individual Factors
“It’s Important to Listen to Yourself”
Multiple providers discussed integrating the practice of self-reflection. As providers encountered contributing factors to occupational stress, an awareness of the presence of this stress helped some to take a step back and better understand their workplace experiences. Some providers that were able to identify this individual awareness were also able to validate the challenging nature of their work. Those that shared their reflections with others shared that it can cause conversations to spark, leading to a space for knowledge-sharing and professional support that not only positively impacts peer relationships but patient interactions as well. One therapist noted that self-reflection was critical for mitigating the stress associated with treating DV clients because “it’s important to listen to yourself when you’re starting to feel numb to how bad things are and to be able to adjust your work accordingly” (Participant 17). A clinical social worker noticed “a lot of behind closed doors venting. . .for myself, when I have the space to really process [the stress] in a mindful way and have someone more senior than me make suggestions. . .” (Participant 7). A clinical social worker who had been in the field for 14 years and managed sexual violence cases noted that having more years of experience enabled her to reflect more effectively: The work is hard and I still get impacted by it. It’s just a matter of recognizing that and mitigating it better than I used to. I think experience helps, knowledge helps, so all of that has made me more confident at the work I do over time (Participant 1).
A clinical social worker shared that “always being aware of your own past mistakes makes you a good practitioner, so having some awareness of your own biases before approaching people and your own lived experience” (Participant 11). Finally, one participant encouraged her coworkers to also engage in the same self-reflection therapeutic strategy as her patients through a peer mentoring model, using “the power of understanding your story, how it brought you here, and being able to share it, and at capacity that is healing for the staff but it’s also really helpful for the clients” (Participant 16).
“If We’re Not Taking Care of Ourselves. . .”
Many providers also discussed various self-care practices including exercising, making healthy food choices, and seeking emotional support from others as mitigators of occupational stress. A mental health psychologist noted the importance of self-care as instrumental in her ability to support herself and her patients by using the analogy of the oxygen mask exercise in the plane when you’re traveling, they tell you to secure your mask before you secure someone else’s and I think that’s so true like if we’re not taking care of ourselves we can’t be fully there for our clients (Participant 15).
Notably, almost all of the twenty providers mentioned exercise as a method to practice self-care. One clinical social worker on a general medicine inpatient unit noted that a big part of self-care is recognizing what your body needs to be healthy, so in my case it’s regular exercise, healthy food that I’m cooking that’s not high in sodium, sleeping enough which for my body is a lot of hours (Participant 11).
A former shelter worker related her healthy habits to her effectiveness as a provider, describing that if I feel like I can’t sleep or don’t have any time with people that I love or things like that, would negatively impact how I’m feeling and make me less efficient and effective provider in a lot of ways (Participant 14).
Numerous participants mentioned connecting with others to mitigate occupational stress. A participant expressed that “my own social outlets like seeing friends and family, having healthy personal relationships” (Participant 11) were essential for her. Of those providers, many characterized these social relationships as including both colleagues who do this work and then folks who don’t do this work. . .it helps to have a community who really understands what you do and it helps to have a community that really doesn’t understand and you can step outside this piece of work (Participant 1).
A few providers also mentioned struggling with self-care. When reflecting on her self-care practices a Sexual Assault Nurse Examiner acknowledged “honestly I should do more of that, I watch TV to relax or go to the gym, I probably should do more” (Participant 13).
Relationship with Identity
Many participants discussed aspects of their own identity, including race/ethnicity, sexuality, and gender and how these enabled them to build connections with others and be motivated to care for others. Understanding how personal identities come into play professionally was shared by certain providers as an additional element in their self-reflection practices. By taking account of the interplay of identities between themselves and their patients, these providers felt prepared to detect and address the nuances with biases in the medical field.
A clinical social worker shared that everything about you personally impacts the way you give care, how you’ve lived, what disadvantages you’ve had, the more in tune you are with that the better you are with connecting with people or even acknowledging the difference in the room (Participant 11).
A mental health psychologist acknowledged her own history with mental health, I’m also an immigrant and experienced some traumatic experiences relative to moving to this country, so part of my work is to really be a model that it’s possible to work through some challenging stuff (Participant 15).
A primary care doctor working with a diverse patient population attested to the power of her own personal experiences as a queer woman, as someone who lived on a couple of different continents as a young person, those things really colored my interest in being able to take care of a large diversity of people and do it in a fairly broad way (Participant 12).
Several participants acknowledged that their own racial and ethnic identity influenced their ability to be attuned to the needs of diverse clients. An Asian clinical social worker admitted that as a clinician of color I’ve noticed how challenging it can be. . . it’s hard to hear certain folks talk about patients and families in ways that may be very assuming, I think there’s a lot of lack of understanding for the traumas that folks go through, for example community violence, so that has been challenging to work with over time (Participant 7).
In other instances, providers talked about the distance a lack of shared identity created in provider–client relationships. A white clinical social worker was explicitly conscious of navigating a racial power dynamic while providing care to women of color, saying that my difference of that identity, the white privilege of that work, inquires then in this space to make sure that even as clients are securing safety, that there’s an intersectionality of systems of structural violence and oppression, and making sure that that’s named and there’s space for that (Participant 2).
Interpersonal-Level Factors
“Never Worry Alone”
Many participants discussed the benefit of being supported by others, including peers and supervisors within their professional organizations and also the value of offering support to others. Mitigating burnout and stress through evaluating shift hours and caseload quantity was incorporated as a component of supervision for participants. The opportunity for collaboration and guidance in structured supervision or informal peer support was shared by providers to be a positive contributor in professional success and development, especially when faced with new and complicated cases. In addition, multiple providers noted that a sense of unity and appreciation among coworkers made their work feel more valuable, which improved their own sense of workplace satisfaction.
In some cases, the support came in the form of training or supervision sessions with supervisors and was particularly useful in managing burnout and dealing with complex cases. Several participants described supervision sessions with senior professionals as an important mitigator of burnout. Supervision included discussions of specific cases and caseloads, as well as the impact of the cases on providers. A medical advocacy coordinator found it to be helpful to have a supervisor who can recognize when you take on too many volunteer shifts, or work too many hours, a sign of emotional burnout, and so being able to recognize that in an employee, as well as giving people permission to take a break (Participant 19).
An inpatient clinical social worker for the medical surgical department also felt that talking [complicated patients and their care] over with our supervisors is helpful just to get someone’s separate insight, helping us to have the different perspective and learning from their experience as well, because often times supervisors have been here longer and they probably have seen some of these cases (Participant 4).
For a clinical social worker of violence prevention and recovery, supervision was named “the number one mitigator” to emotional burnout and compassion fatigue (Participant 1). A clinical social worker on a trauma surgical floor reflected on two different supervisors she has had: It’s helped to be able to process those really difficult cases, but personally, emotionally, while also helping with knowing what to do from a more senior person and steps to consider taking and having another point of reference to bounce ideas off of and to simply feel heard in the discomfort and the sadness (Participant 8).
Finally, one participant shared that case supervision was not just available to early career providers but all providers. A clinical social worker of violence prevention and recovery explained that “even our most senior people get it. So, if you’ve been here for 20 years you still get supervision, they just hire outside consultants to have more advanced.” (Participant 2).
Notably, not all participants felt that supervision was equally available to all DV providers. A primary care physician commented on not receiving any supervision, “you’re on your own when you’re a physician except for the institutions that are telling you to jump faster, work harder, see more patients” (Participant 12).
Other participants described mutually beneficial offerings of support and the camaraderie it built among colleagues. A Sexual Assault Nurse Examiner nurse noted feeling especially close to her colleagues which helps to decrease the chance of getting compassion fatigue because I feel like my coworkers and I we’re all there for each other and when there’s a difficult situation or case I can easily text my supervisor or one of my colleagues (Participant 13).
One provider found that being on a supportive team makes you recognize the value of what you do more and it’s helpful when people see it as valuable as well. . . and knowing that I’m not as a social worker in a case alone but that there’s other providers as a team helps me in some way (Participant 20).
A former shelter worker highlighted the importance of giving peer providers the same support that they are giving to survivors, saying that “anyone who feels like they’re in a safe space and inherently having support whatever that means for them, helps them to do their job” (Participant 14). As the only social worker on her floor, a participant emphasized “building up other providers so that the burden is not only on the mental health provider. . .to do the best that they can do so that they reserve you for the hardest things and not every little thing” (Participant 11). Social work departments were especially structurally supportive spaces for providers, with one clinical social worker of the acute surgical trauma floor discussing that I don’t think I’m going to necessarily go to my doctor or nursing colleagues for necessarily sympathy in some of the difficulties that we struggle with on the job day to day I think I would talk with other folks who I know to be likeminded or have similar training so that we cannot dissociate from it (Participant 7).
Three clinical social workers mentioned the motto “never worry alone,” with one noting so when something feels heavy or burdensome and you’re feeling stuck clinically on how to approach something, don’t worry about it alone, talk to someone about it, doesn’t need to be the context of clinical supervision, it can be with a more senior peer, in my case it’s many of my senior nursing colleagues on the floor, or attending physicians that are on the floor, that’s really important (Participant 11).
An inpatient clinical social worker also commented on the importance of consultation with more specialized clinical social workers finding it “really nice to learn from them. . .it’s helpful to get their perspective on ambivalences that people might be feeling about their attackers” (Participant 4). Working in a social work department with varying levels of experience was beneficial for a clinical social worker and program advocate, since some people have been here for longer they’re able to model what’s helpful in preventing burnout. So things like being able to have places to talk about how everything is impacting you has been really helpful, sort of having a team mentality or normalization or validation that self-care is important (Participant 5).
Organizational-Level Factors
On-the-job Training
Many participants noted a myriad of personal and professional benefits related to on-the-job training. They commented on this type of support enabling them to be current in their field, promoting professional effectiveness and how participation in training created a venue to access support.
A primary care physician expressed training to be “valuable because it keeps you up in the field in how to take better care of the patients so everyone chooses the things that they feel that they most need training in” (Participant 12). A clinical social worker noted the training enabled her to not just build her professional skills but reinvigorated her, noting that by “continuing to educate [herself] in ways and topics and resources and different ways to approach folks therapeutically, it continues to revive [her]” (Participant 7). One participant working in the ICU felt more confident as a result of her training, being “used to dealing with very difficult situations so professionally I feel through my training and my experience very well equipped to care for these patients” (Participant 13). Another participant who had gone through a sexual assault examiner program that offered “education on different topics, people often bringing up difficult cases, we’ll talk about it and get support from each other, but also a chance to get support and talk about things that nobody else would begin to understand” (Participant 6). Finally, one participant, a mental health psychologist reflected back on the importance of early career training in teaching her how to recognize and manage manifestations of occupational stress. She noted that her graduate training helped us to parse out okay when do we need to take breaks, when is it too much, when do we need to say okay I need to step away from what is going on. I was fortunate that I had training experiences in a graduate program that really understood that and encouraged us to take those breaks when we needed them (Participant 15).
“We Want You to Go Home After 8 hours”
While many participants talked about support from individuals, many participants also noted an organizational culture of support and self-care, supported by institutional practices. One clinical social worker shared that her team meetings included “self-care at the end of our meetings for 10 minutes whether that’s coloring or listening to music, just making sure there’s some sort of moment to pause because our days can be pretty busy” (Participant 5). A manager for medical advocates felt as though her organization had “good time off, good sick time, we have self-care days built into our package so you can just take a quick day off” (Participant 10). Additionally, another participant noted that a culture of competition and stress was avoided when the organization communicated the message that “we want you to go home after 8 hours, we want you to have a work-life balance, the culture of where you work has a huge influence on your ability to take care of yourself” (Participant 19). One clinical social worker on the trauma and surgical floor was encouraged to seek out her own mental health treatment knowing that there’s an emphasis on practicing what I preach of taking care of your mental health, knowing that that is normal for providers to do even if you’re one of them yourself, like seeing a social worker while you are also a social worker (Participant 8).
Another participant felt that encouraging self-care within organizations showed that “our culture is changing, it feels more okay in the right space to ask for what you need and I think that’s huge because that wasn’t there until very recently in my experience” (Participant 14). A participant commented on working in an environment where self-care was encouraged by supervisors. especially when dealing with difficult cases: so it wasn’t just my responsibility for self-care but also my director immediately thought organizationally, do you need a day off so that you could do self-care versus having to come in and have all the responsibility. . . that’s an organizational structural thing that’s going to promote wellness (Participant 2).
Discussion
The themes identified in this study using a thematic analysis approach consisted of (a) manifestations of occupational stress, (b) drivers of occupational stress, and (c) protective factors that mitigate experiences of occupational stress among health and mental healthcare providers who provide care to DV survivors. Notably, over half of our sample consisted of DV providers working in medical settings, which is unique in the literature.
Despite the differences in organizational settings among participants, our study found that all these providers reported manifestations of occupational stress associated with the demands of their jobs. Some providers who worked specifically in medical settings talked about the added challenges of working with DV survivors in environments where they had to deal both with mental and physical trauma. This merits further exploration in future research. In general, our findings related to manifestation of occupational stress are consistent with other studies of occupational stress among DV providers. For example, in a qualitative study of trauma therapists, providers expressed feelings of countertransference influenced by the therapists’ own personal history of trauma and the duration of time in the field (Cavanagh et al., 2015). In another study, Adult Protective Services social workers acknowledged that they no longer believed that they could change the world, or even the lives of their patients (Bourassa, 2009). This shift in worldview, a sign of vicarious traumatization, was also noted in a study of DV shelter workers (Merchant & Whiting, 2015). Additionally, in a study of DV advocates, providers described manifestations of STS in the form of flashbacks or nightmares, and rumination over disturbing patient stories (Bemiller & Williams, 2011). They described working through this stress, a concept named “good soldiering,” to highlight providers prioritizing client care despite stressors they were personally facing. In another study of masters-level social workers, occupational stress manifested in the form of hypervigilance and fatigue (Bride, 2007).
Providers in this study also described several drivers of occupational stress ranging from quantity and intensity of caseload to challenges in the physical workplace environment. Other studies have identified similar risk factors. For example, in a school of social work’s field instructors, a larger and more complex caseload was also associated with occupational stress ranging from STS to burnout (Wagaman et al., 2015). Dworkin et al. (2016) found that rape crisis staff members with large client loads and less supervision had high levels of STS, as did staff with a personal history of sexual assault in another study of both individual and setting-level STS risk factors. Experiencing anxiety and stressful emotional involvement with clients while engaging in therapeutic work resulted in emotional exhaustion in a study of therapists (Steel et al., 2015). Another study demonstrated that psychotherapists at fast-paced agencies experienced organizational inefficiency or a lack of support which contributed to burnout among the providers (Yang & Hayes, 2020). Lazarus and Folkman’s (1984) theory of stress and coping helps to contextualize these findings through the component of appraisal, which involves evaluating stressful encounters such as those experienced by DV providers. Lazarus and Folkman (1984) identified that cognitive appraisal consists of assessing the challenge and the resources needed in a situation before moving on to coping. Among DV providers, application of this theory requires recognition of the challenging nature of responding to large and complex caseloads. Finally, providers in this study talked about a range of factors that mitigate occupational stress at the individual and interpersonal level. Other studies have similarly noted that reflecting on personal identity, including a provider self-awareness that improves the patient-provider relationship (Reeves, 2015) and that emotional intelligence (defined as the ability to manage and understand emotions) has the potential to act as a buffer for occupational stress for providers (Newton et al., 2016). In Wagaman et al.’s study (2015), it was also observed that the capacity to maintain boundaries was also a protective factor against STS along with self-reflection and self-care practices. In the present study, self-care was viewed as a protective factor against compassion fatigue and emotional burnout both at an individual level and within an organizational context. In a recent study, while leisure time including passive strategies (i.e., watching TV) did not reduce emotional burnout, more active self-care strategies such as making a time commitment for stress management were shown to be more likely to reduce emotional burnout among DV service providers (Kulkarni et al., 2013). In the present study, common individual self-care activities were eating, exercising, and sleeping well, and connecting with those in the provider’s support networks. These practices have been listed as biobehavioral strategies, as well as opportunities to maintain creative outlets and spiritual connections (Newell & MacNeil, 2010). At the interpersonal level, support from colleagues decreased a provider’s individual sense of burden from occupational stress in a review of symptoms, risk factors, and theoretical terms regarding occupational stress (Newell & MacNeil, 2010).
Lastly, at the organizational level, our study identified factors that mitigate experiences of stress, namely an institutional culture of self-care, on the job training and case supervision.
A culture of balance and creating opportunities to practice self-care have been shown to mitigate vicarious traumatization, burnout, STS, and countertransference in a study of staff from Southwestern intimate partner violence and sexual assault coalitions (Wachter et al., 2020). Studies also show that training and supervision, also noted in our study, can be an important protective factor against emotional burnout and compassion fatigue (Kim et al., 2018). Fifteen quantitative studies of work-related factors and compassion fatigue were analyzed and found that job demands of social workers, therapists, and nurses associated with occupational stress were mitigated by job resources through supervision, coworker support, and organizational support (Singh et al., 2020). Similarly, in an Israeli study (2011) of social workers at DV centers, providers had more compassion satisfaction and feelings of competence when they had a weekly time and place to discuss caseload management and difficulties regardless of their level of experience (Ben-Porat & Itzhaky, 2011). In Slattery and Goodman’s study (2009), engaging and empowering supervision reduced the likelihood of DV advocates’ experience of STS (Slattery & Goodman, 2009), which was also found in Dworkin et al.’s (2016) study of the impact of frequency of supervision and client loads on STS (Dworkin et al., 2016). Lazarus and Folkman’s (1984) theory of stress and coping can once again help to contextualize these findings through their research on coping, which refers to the cognitive mastering of stressful demands by both regulating distress and managing the problem itself. Self-care practices may serve as a mechanism of coping through its focus of emotional regulation, while training and supervision provide opportunities for case management, professional support, and organizational knowledge-sharing.
In the existing literature, training programs focused on TIC improve skills and role satisfaction while also providing tools to create balance between the provider’s professional and personal lives (Baird & Jenkins, 2003). In the present study, with many employers requiring continuous education for healthcare providers, providers are kept up to date in the practices of TIC and can employ new strategies or perspectives with a diverse background of patients. There are several limitations to this research to be noted and considered in the interpretation of our results. All providers recruited for this research were women, with 95% being white. As such, our findings may not be applicable to providers of other genders or racial/ethnic backgrounds. Furthermore, our sample was comprised of many different types of providers who work in different organizational settings, and there are likely contextual factors unique to these settings that could impact provider experiences related to occupational stress. In future research, we hope to explore more in-depth, occupational experiences of specific categories of providers, such as doctors or DV advocates. Despite the limitations noted about the sample composition, a strength of this study was the inclusion of different types of TIC healthcare providers, including medical advocates, nurses, and therapists, which, in turn, allowed us to capture a broad range of experiences. In addition, every effort was made to maximize the credibility and dependability of the research during the data collection and analysis process using strategies such as collaborative coding, triangulation of the data by multiple investigators and review of literature from multiple disciplines, and audit trails. Furthermore, no new codes or themes were generated after analyzing the 20 interviews, suggesting sufficient information power of the sample size’s richness regarding our research question.
Implications
This qualitative study centered on the perceptions healthcare and mental health professionals who provide TIC to DV survivors have and explores, through qualitative research, manifestations, drivers, and mitigators of occupational stress among these participants. Within this study, the dynamic nature between these drivers and manifestations is revealed as one that requires attention that goes beyond the individual and extends to peer, departmental, and organization-level structures to combat and mitigate occupational stress specifically in the medical setting. The findings, which identify individual-, interpersonal-, and organizational-level factors as outlined in the socioecological model that can drive experiences of stress, can inform how DV providers’ employers and organizations can work to further support providers who work with DV survivors. In particular, it is critical to focus on fostering a workplace environment where self-care and support is institutionalized so that the burden does not fall on individual providers but rather that their health and well-being are also supported by policies, programs, and practices that address and meet their occupational needs. Strengthened training, supervision, and opportunities to practice self-care within and beyond the workplace should be evaluated in future research.
Conclusion
This study provides evidence of both risk and protective factors in a sample of healthcare providers who engage in therapeutic TIC work. As noted by Molnar et al. (2017), better understanding risk and protective factors for providers’ occupational stress can help inform the development of interventions and policies to mitigate this stress. Evidence gathered through this study suggests the importance of intervening, particularly at the organizational level, to mitigate risk factors and amplify protective factors associated with manifestations of occupational stress among healthcare providers who deliver TIC to DV survivors.
Footnotes
Acknowledgements
A sincere thank you to Tufts University, the Community Health Department, and the Undergraduate Research Fund for supporting this research. Most importantly, I would like to thank and applaud the research participants for the impactful work that they do for survivors of domestic violence.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The author received financial support for the research of this article through Tufts University’s Undergraduate Research Fund.