
Abstract
The transgender population experiences disproportionate rates of sexual assault (SA) compared with the cisgender population. Sexual assault nurse examiners (SANEs) have specialized education to provide care to victims of SA across the lifespan; however, training related to the care of transgender individuals following sexual assault is not always represented in SANE education. This leads to a lack of knowledge and confidence in providing care to transgender victims and can result in inequitable care and poor outcomes. To explore forensic nurses’ knowledge and confidence in the care of the transgender population following SA, a descriptive, cross-sectional survey design was employed and distributed to two professional forensic nursing organizations. A total of 240 survey responses were received. The majority of participants reported that content related to transgender sexual assault (TGSA) was not part of their SA education. Nearly 60% perceived their knowledge and confidence in providing TGSA care as “beginner” or “developing” and almost all “agree” or “strongly agree” that additional TGSA education would be beneficial to them. As over half of participants have provided care to a TGSA patient and more than 80% expect to provide care in the future, it is imperative include standardized content related to TGSA care as part of core SANE curriculum and to offer continuing education to address the gap in current SANE TGSA knowledge and practice.
In the United States, nearly half of all women (43.6%) and a quarter of all men (24.8%) will experience some form of contact sexual violence during their life (Smith et al., 2018). There are close to 335 million people in the United States (United States Census Bureau, 2023) with 1.6 million persons 13 and older identifying as transgender; 0.6% of the population; 39% are transgender women, 36% are transgender men, and 25.6% are gender nonconforming (Williams Institute, 2022). Transgender, or “trans” for short, is a term used to describe persons whose gender identity is different from the gender they were assigned at birth (National Center for Transgender Equality, 2023). Despite trans individuals accounting for a small portion of the country’s population, they endure disproportionately higher rates of sexual assault (SA); with a lifetime prevalence of 47% to 64% (Drescher et al., 2019; Henry et al., 2018). Transgender people experience a 2.5-fold increase in sexual violence compared to cisgender people, and compared with cisgender women, transgender women are five times more likely to be the victim of sexual abuse (Das et al., 2021). Additionally, in trans persons who are sexually assaulted, almost 75% experience repeat acts of such violence (FORGE, 2016).
Sexual assault nurse examiners (SANEs) are registered nurses who are specially educated and trained to provide comprehensive care to individuals following SA (Office of Victims of Crime[OVC], n.d.). SANEs conduct a medical-forensic examination; offer medications to prevent sexually transmitted infections, human immunodeficiency virus, and pregnancy; and recommend support and follow-up services to assist patients in addressing immediate and long-term health and legal consequences of SA (OVC). Because of the disproportionately higher rates of SA in trans persons, SANEs will likely encounter and provide care to a transgender patient at some point in their career. Despite this, it has been identified that SANEs require additional specific education to enhance knowledge and confidence in providing gender-affirming care to trans patients (Du Mont et al., 2019; Mackler et al., 2023).
Background/Significance
Barriers to Accessing Healthcare
Support services within healthcare, social/advocacy, and/or the criminal justice system are available to victims following SA. Yet, victims may choose to not disclose, report, or seek services as a result of shame, fear of disbelief, or feeling that their assault was “not serious enough” to warrant help (Anderson & Overby, 2020; Pijlman et al., 2023). Victims may believe that services will not be helpful, and in fact, could be harmful, contributing to retraumatization from victim blaming or having to retell/relive their assaultive experience. Further, structural barriers include lack of awareness of available resources or inability to access services due to location, time constraints, and perceived cost (Anderson & Overby, 2020; Pijlman et al., 2023).
Trans individuals may have additional barriers that contribute to avoiding and/or delaying services following SA as almost 80% did not access support such as healthcare, law enforcement, or the crisis center following their victimization (Rymer & Cartei, 2015). Reasons included fear of discrimination as a consequence of their gender identity (40%) and feelings of shame (21%). Of those who did access support services, almost all (92%) reported that their gender identity had an impact on their experience of support (Rymer & Cartei, 2015).
Fear of discrimination in healthcare is a common theme for trans persons. In a study of almost 3,500 transgender participants, close to 30% stated that they postponed treatment or did not seek healthcare related to fear of discrimination (Jaffee et al., 2016). Discrimination related to being identified as transgender, whether through assessment or because their identity must be disclosed, are significant deterrents in obtaining care (Kcomt et al., 2020; Seelman et al., 2017). Fear of abuse, hostility, rejection, and harassment are also concerns along with being outed, intentionally or accidentally, or denied services (FORGE, 2016).
Clinician Knowledge of Transgender Care
Fear of being welcomed, accepted, and treated in a culturally competent manner by clinicians who are educated and skilled in providing trans-affirming care remains a challenge (FORGE, 2016). This is impacted by clinician knowledge and comfort which is poor across many levels of practice and specialties (Du Mont et al., 2019; Stroumsa et al., 2019). In fact, the odds of an individual seeking and delaying healthcare was four times greater if they needed to educate their clinician about transgender people (Jaffee et al., 2016).
The 2015 US Transgender Survey was used to extrapolate data to evaluate trans patient perceptions of their healthcare provider’s knowledge about transgender health. Over 23,000 participants responded; 24.6% reported that their provider knows “almost everything about transgender care,” 17.5% know “most things,” 14.8% know “some things,” and 11.5% know “almost nothing”; 31.5% were “unsure” (Miller et al., 2023, p. 5). Additionally, as provider knowledge decreased, participant self-rated health decreased and severe psychological distress increased (Miller et al., 2023). Transgender persons were also found to have the highest prevalence of not being satisfied with the healthcare they received compared with cisgender individuals (Ferrucci et al., 2021).
Dissatisfaction with their provider could be related to receiving care from clinicians who have not received the necessary education to provide equitable care for transgender patients (Carabez et al., 2016). In a study of multiple OBGYN departments across the United States, 80% of physicians received no education on the care of transgender patients during medical school. Practice experience did not correlate with increased knowledge with 29% to 35.3% of providers uncomfortable caring for trans patients (Unger, 2015). Similarly, less than 50% of primary care providers reported receiving formal education on the care of transgender patients despite the fact that almost half had previously provided care to a patient who was transgender. Even in physicians who received some education, this education did not correlate with increased provider knowledge (Stroumsa et al., 2019). Nurses also expressed discomfort when working with trans patients reporting confusion and frustration about pronoun use, patient room assignment, bathroom use, and understanding terminology. As a result of their discomfort, these nurses reported avoiding/refusing care, gossiping/laughing about, and isolating transgender patients (Carabez et al., 2016).
SANE Education of Transgender Patients Following Sexual Assault
As care of transgender patients is not routinely part of healthcare provider education, it is critical that content be included within specialty curriculum to ensure that clinicians understand key considerations related to encountering trans patients within their specialty of care, cultivating an environment where health equity is possible. SANEs provide specialized care to patients who have experienced SA. In order to become certified as a SANE through the Commission for Forensic Nursing Certification, nurses must successfully complete a course that incorporates the International Association of Forensic Nurses (IAFN) SANE Education Guidelines. Nurses who receive education based on these guidelines should thus be prepared to implement evidence-based standards when conducting the medical-forensic exam with the ability to consider “developmental, cultural, racial, ethnic, gender identity, sexual, and socioeconomic diversity” (International Association of Forensic Nurses [IAFN], 2022, p. 1).
The SANE Education Guidelines provide “Key Target Learning Topics” that dictate curriculum to be included in any basic SANE course for nurses new to this subspecialty within forensic nursing. Content related to the care of transgender patients can be found in “Topic I: Overview of Forensic Nursing and Sexual Violence.” This standard specifies that the SANE educational offering must include content related to the unique healthcare challenges as well as best practice recommendations for improving forensic nursing care to underserved and vulnerable patient populations, including but not limited to “GLBTQIA (gay, lesbian, bisexual, transgender, questioning/queer, intersex, agender/asexual)” (IAFN, 2022, p. 19). “Topic II: Victim Responses and Crisis Intervention” requires the inclusion of content specific to psychosocial issues associated with underserved sexual violence patient populations and “Topic IV: Medical Forensic History Taking” suggests learners are educated on techniques for establishing rapport and facilitating disclosure while considering the patient’s gender identity. SANE guidelines offer broad topics to be covered within a training with the expectation that faculty delivering the course tailor content specific to the community of practice. This flexibility can contribute to a lack of content standardization and be further impacted by the expertise of the faculty teaching the course (Mackler et al., 2023).
In Ontario, Canada, there are 35 Sexual Assault/Domestic Violence Treatment Centres. These centers house forensic nursing programs where SA nurses, registered with the College of Nurses of Ontario, provide comprehensive care to adults who have recently been sexually assaulted. Some of these nurses have undergone formal SANE training in Ontario (Du Mont et al., 2019); “however, this training does not include comprehensive information on how to respond to transgender (trans) survivors of sexual assault” (Du Mont et al., 2020, p. 2). In a study examining the perceived level of competence and need for additional education, close to 75% reported little to no experience caring for transgender patients following SA and almost all (95.7%) reported they would benefit from additional training (Du Mont et al., 2019).
A follow-up study was conducted to determine the efficacy of trans-specific curriculum on forensic nurse competence in providing care to trans patients following SA (Du Mont et al., 2020). Sixty-six percent of respondents had not received previous education related to care of the trans patient, and in those who had (43.8%), it was most commonly self-directed. Following participation in the training, perceived level of expertise related to care of trans patients following SA improved significantly (M = 1.89, SD = 0.84 vs. M = 3.47, SD = 0.62, p < .001). These results are supported by a quality improvement project that sought to increase SANE self-perceived competence in caring for trans victims of SA. Less than 20% reported receiving trans-specific content in their SANE training despite almost three-quarters of respondents stating they previously provided care to a trans patient. Further, over 90% of participants agreed or strongly agreed that they would benefit from additional training (Mackler et al., 2023). Aside from the aforementioned Canadian studies, little research has been conducted on the care of transgender patients following SA, specifically on clinician/SANE knowledge and confidence in providing trauma-informed, gender-affirming care to this specific population.
Purpose
The purpose of this study was to explore factors that affect SANE self-reported knowledge and confidence in providing care to transgender patients following SA. The study further aimed to examine whether participants reported that their SANE education and training included content on the care of trans patients. The research questions were as follows: (a) to what extent is education on the care of transgender patients included in SANE training; and (b) what aspects of education and experience most significantly impact SANE knowledge and confidence in providing care to trans patients following SA.
Methods
Design and Data Collection
This study utilized a descriptive, cross-sectional research design to explore the research questions and was approved by the Oakland University Institutional Review Board (Rochester, MI). Based on a review of the literature and the researchers’ SANE education and practice experience, an internet-based survey was developed using Qualtrics software (Provo, UT). For the purposes of this study, “transgender” refers to any person who identifies as a gender that is different from the sex they were assigned at birth. This includes those who identify as transgender male, transgender female, nonbinary, or genderqueer, regardless of transition status. “Sexual assault” refers to attempted or completed nonconsensual penetration of the vagina, mouth, or anus or nonconsensual touching of the breasts, buttocks, or genital area. Eligibility criteria for this study included being a registered nurse (RN) or other healthcare provider over the age of 18.
Participants were recruited by distributing the survey to two professional forensic nursing organizations, the Academy of Forensic Nursing (AFN) and the IAFN. The AFN has approximately 1,000 members and more than 6,000 forensic nurses and allied professionals comprise IAFN membership, including 2,135 certified SANEs (IAFN, 2021). The survey was posted within each organization’s online community members’ forum and emailed directly to IAFN members.
Upon clicking the link to the survey, an information sheet explaining the study purpose, eligibility, risks and benefits, principal investigator contact information, and IRB approval was displayed. Participation in the study was voluntary, and informed consent was acknowledged by the participant clicking “yes” to advance the survey. Responses were anonymous. Data were collected from October 2022 through February 2023.
Demographic and professional items included gender identity, race, ethnicity, age range, highest level of education, years of practice as a RN, and timing of SANE training. Frequencies for these items are included in Table 1. Participants were asked whether content related to the care of transgender sexual assault (TGSA) patients was included in their SANE training and whether they had participated in any other training on the topic of caring for TGSA patients. Participants were also asked whether they had provided care to TGSA patients, the frequency of this care, and if they anticipated providing care to TGSA patients in the future.
Sample Characteristics.
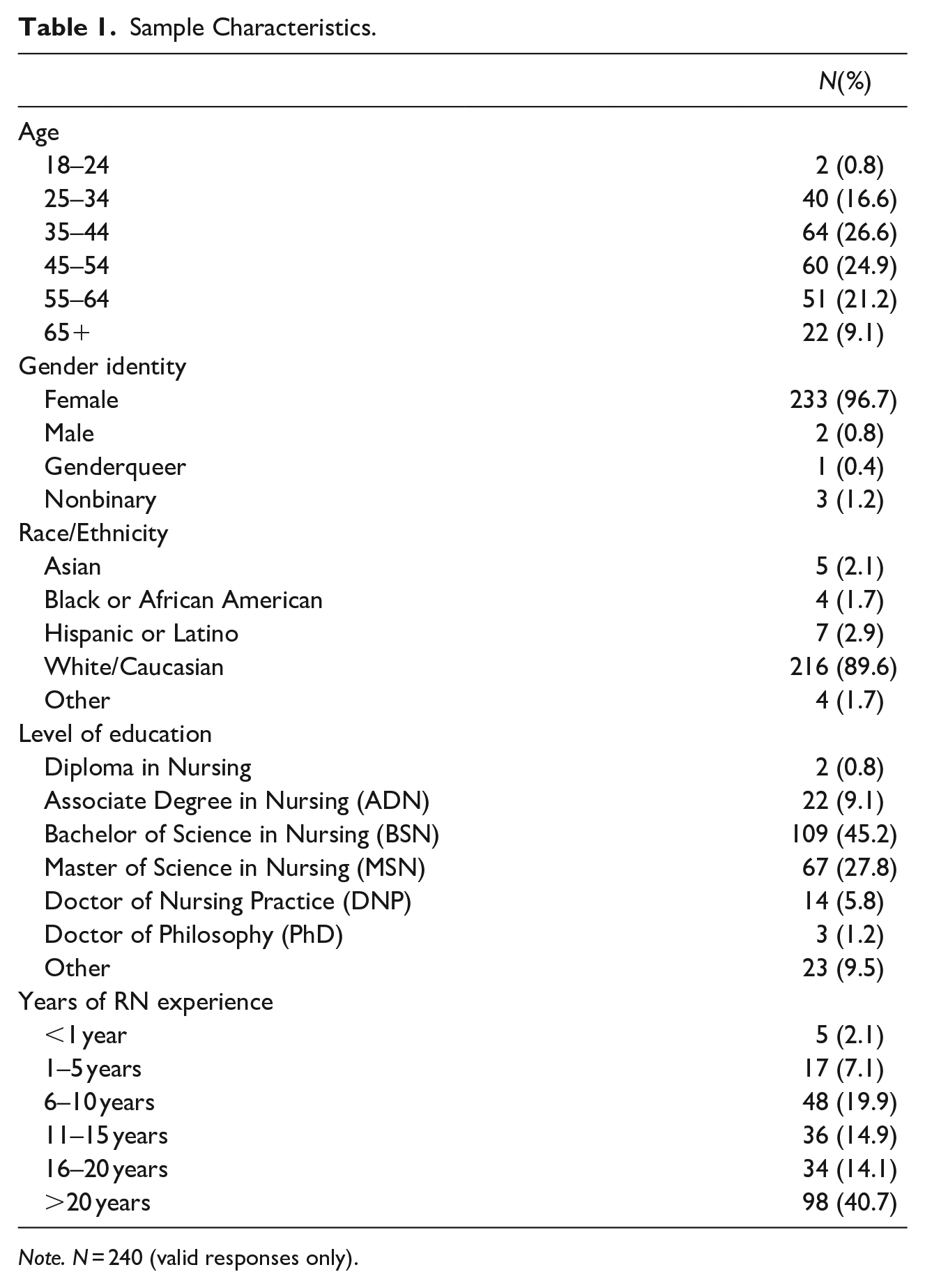
Note. N = 240 (valid responses only).
The study’s two dependent variables were participants’ self-rated knowledge of TGSA care and self-rated confidence in providing TGSA care. Knowledge was scored on a four-point Likert scale where 1 = beginner: this concept/topic is brand new to me, 2 = developing: I have a basic understanding of this concept/topic, 3 = proficient: I have above-average knowledge about this concept/topic and could explain it to others, and 4 = expert: I have immense knowledge of this concept/topic and could teach it to others. Confidence was also scored on a four-point Likert scale where 1 = beginner: not confident at all, 2 = developing: somewhat confident, 3 = proficient: confident, and 4 = expert: very confident. Cronbach’s alpha for the survey section measuring Knowledge and Confidence was good at ⍺ = .876.
Participants also rated their agreement with the statement: “I would benefit from additional education on the provision of care to transgender patients who have been sexually assaulted” on a four-point Likert scale from 1 = strongly disagree to 4 = strongly agree. Interest in future educational offerings was rated on a three-point Likert scale where 0 = not interested/needed, 1 = somewhat interested/needed, and 2 = extremely interested/much needed. Responses that included two ratings (i.e., “not interested/needed” and “somewhat interested/needed”) were recoded to a new variable reflecting the higher of the two levels of interest.
Data Analysis
Data was analyzed using IBM SPSS Statistics for Windows, version 29 (IBM Corp., Armonk, NY). Responses with significant missing data were excluded from analysis. Frequencies and descriptive statistics were explored for all study variables and are presented in Tables 1 to 3. Dummy variables were created for all categorical variables to test the assumption of proportional odds. This assumption was met, as assessed through a full likelihood ratio test which compared the fit of the proportional odds location model to a model with varied location parameters, χ2(40) = 23.209, p = .984. A cumulative odds ordinal logistic regression was conducted to examine the effect of RN education level, years of practice, SANE education timing, TGSA content in SANE education, additional TGSA education, and experience providing care to TGSA patients on SANE level of knowledge and confidence in providing care to TGSA patients.
Transgender Sexual Assault Education.
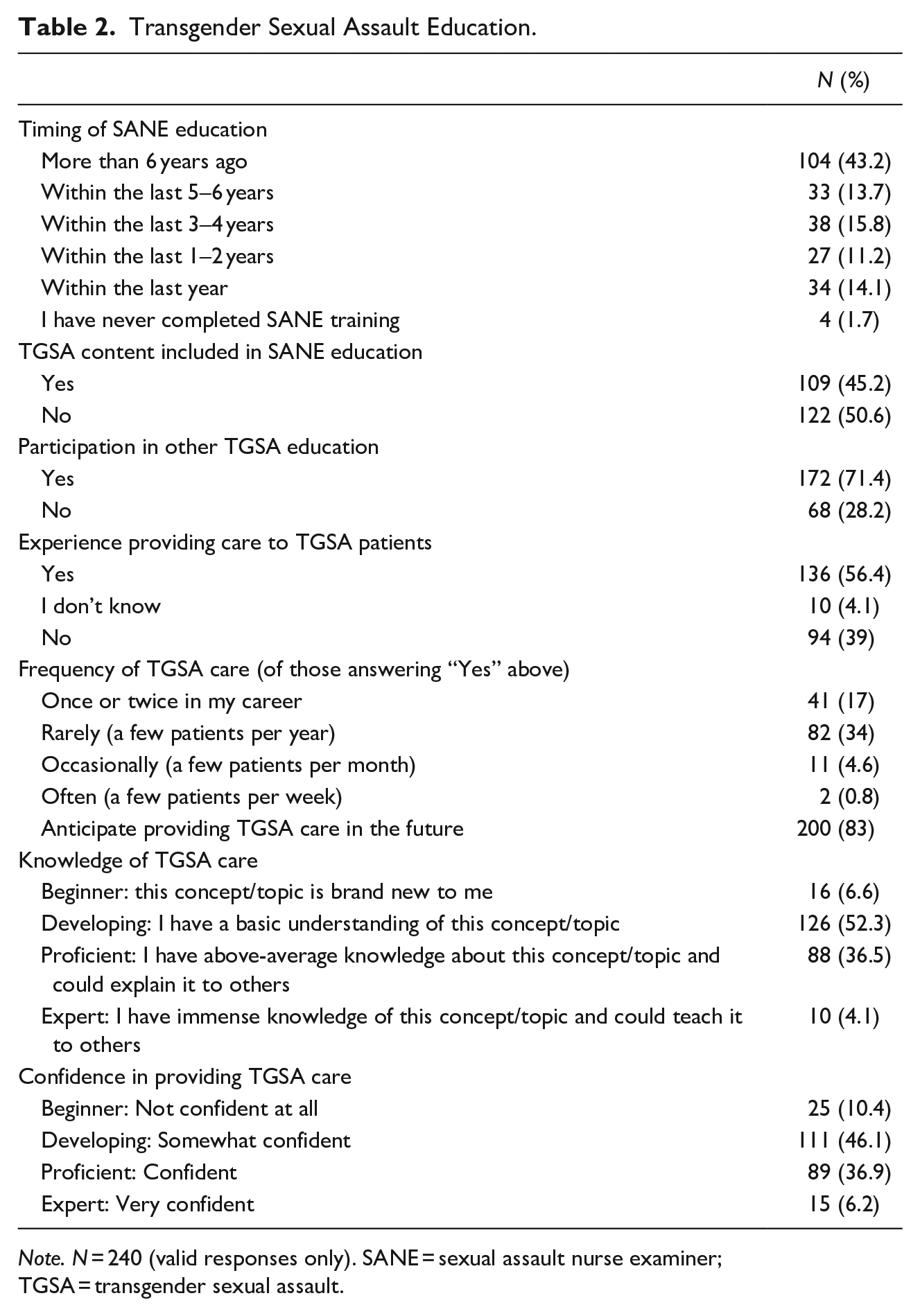
Note. N = 240 (valid responses only). SANE = sexual assault nurse examiner; TGSA = transgender sexual assault.
Level of Interest in Educational Topics.
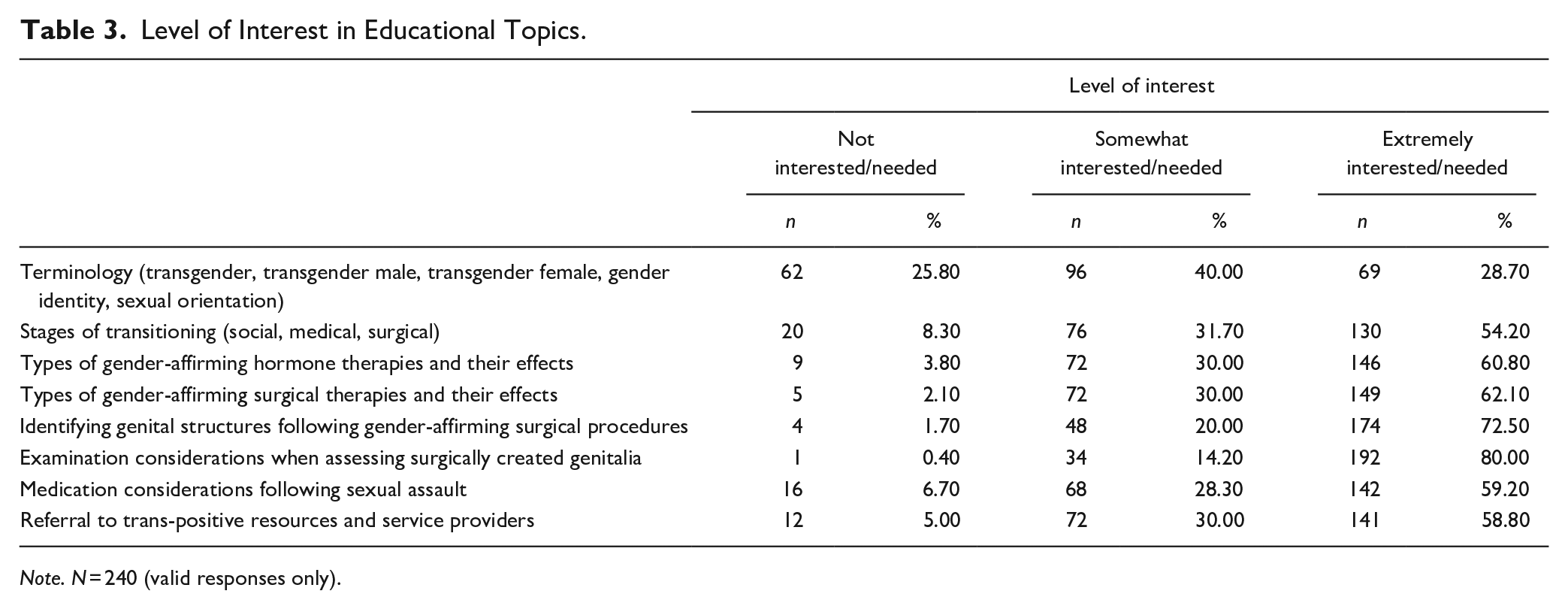
Note. N = 240 (valid responses only).
Results
Of the 240 healthcare professionals who completed the survey, 219 (91.3%) held a degree in nursing. About half of the participants fell into the age ranges of 35 to 44 (26.6%) and 45 to 54 (24.9%), and the majority identified as female (96.7%) and white (89.6%). Most had a Bachelor of Science in Nursing degree (45.2%) and had practiced as a RN for more than 20 years (40.7%) (Table 1).
Results related to the timing and content of SANE training revealed that 43.2% of respondents participated in SANE training more than 6 years ago; 50.6% indicated that content related to the care of TGSA patients was not included in their SANE education; and 71.4% sought additional TGSA education in the form of professional development such as webinars, conference sessions, or seminars. Most participants stated they have experience providing care to TGSA patients (56.4%) and anticipate providing TGSA care in the future (83%). Of those with experience, approximately one-third stated they provide care to only a few TGSA patients annually. Fifty-two percent of participants rated their level of knowledge in providing care to TGSA patients as “Developing,” and 36.5% rated their knowledge as “Proficient.” Most participants (46.1%) rated their level of confidence as “Developing,” and 36.9% rated their confidence as “Proficient” (Table 2).
Respondents indicated an interest in and the need for expanded options for TGSA education. The majority either strongly agreed (60.2%) or agreed (36.9%) that they would benefit from additional education. Educational topics of highest interest/need were exam considerations when assessing surgically created genitalia (94.2%); identifying genital structures following gender-affirming surgical procedures (92.5%); types of gender-affirming surgical therapies and their effects (92.1%); and types of gender-affirming hormone therapies and their effects (90.8%) (Table 3).
The deviance goodness-of-fit test showed that the models for both knowledge (χ2[18] = 22.865, p = .196) and confidence (χ2[18] = 18.060, p = .452) were a good fit to the data. Both final models were statistically significant, over and above the intercept-only models, in predicting the dependent variables of self-rated knowledge and confidence in providing care to TGSA patients, χ2(3) = 73.967, p < .001 and χ2(3) = 79.080, p < .001, respectively. The odds ratio of reporting higher levels of knowledge was 2.446, 95% CI [1.372, 4.361] for nurses who received education on the care of TGSA patients during their SANE training versus those who did not, and 5.593, 95% CI [2.522, 12.404] for SANEs who participated in additional training on the care of TGSA patients as compared to those who did not; both with statistically significant effects, χ2(1) = 9.187, p = .002, and χ2(1) = 17.943, p < .001 respectively. Similarly, nurses whose SANE training included education on the care of TGSA patients were 1.790, 95% CI [1.035, 3.098] times more likely to report higher levels of confidence than those whose SANE training did not include TGSA content (χ2[1] = 4.332, p = .037), and SANEs who participated in additional TGSA training were 5.725, 95% CI [2.688, 12.192] times more likely to report higher levels of confidence than those who did not, χ2(1) = 20.4657, p < .001. For nurses with experience providing care to TGSA patients, as compared to those without experience, the odds ratio of reporting higher levels of knowledge was 5.898, 95% CI [2.995, 11.616] and higher levels of confidence was 5.702, 95% CI [2.973, 10.935], also with statistically significant effects of χ2(1) = 26.335, p < .001 and χ2(1) = 27.451, p < .001, respectively.
Predictors of higher levels of knowledge were TGSA content in SANE training, Wald χ2(2) = 13.956, p < .001; Additional TGSA training, Wald χ2(2) = 9.854, p = .002l; and Experience Providing TGSA Care, Wald χ2(2) = 17.132, p < .001. The same factors also statistically significantly predicted higher reported levels of confidence, Wald χ2(2) = 8.628, p = .004, Wald χ2(2) = 8.067, p = .005, and Wald χ2(2) = 18.543, p < .001, respectively. Educational level, RN years of experience, and timing of SANE training were not statistically significant predictors of either dependent variable (Tables 4 and 5).
Ordinal Logistic Regression for Knowledge of TGSA Patient Care.
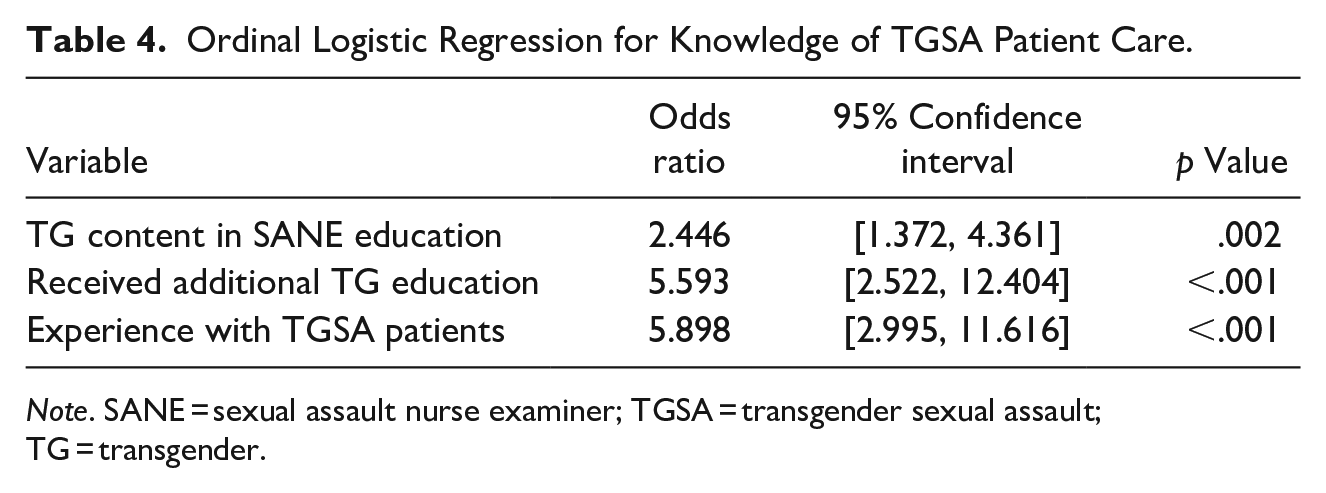
Note. SANE = sexual assault nurse examiner; TGSA = transgender sexual assault; TG = transgender.
Ordinal Logistic Regression for Confidence in Providing TGSA Patient Care.
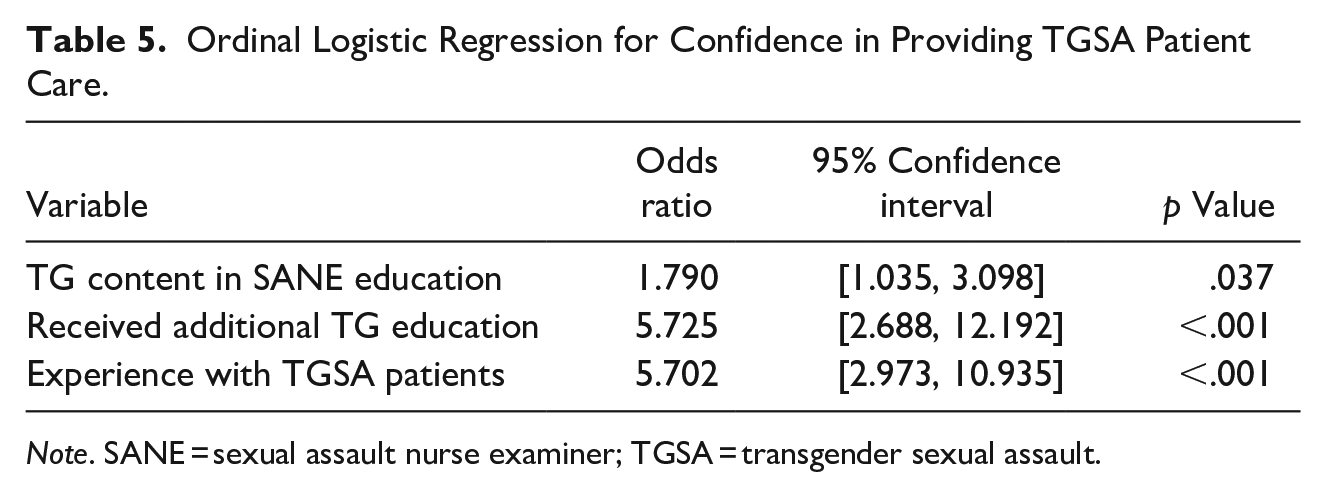
Note. SANE = sexual assault nurse examiner; TGSA = transgender sexual assault.
Discussion
For most participants, content related to TGSA was not part of their SANE education despite it being “a minimum recommended requirement of training” to function and seek certification as a SANE (IAFN, 2022, p. 3). This correlates with the fact that almost 60% of study participants perceived their knowledge and confidence in providing TGSA care as beginner or developing and almost all (97.1%) agree or strongly agree that additional TGSA education would be beneficial to them. Results support findings in the Canadian study, which found that comprehensive TGSA content was not consistently provided in SANE training (Du Mont et al., 2020), and nearly all study participants reported they would benefit from additional TGSA education (Du Mont et al., 2019). Participants in the current study who either received TGSA content during their SANE training or sought additional TGSA training were significantly more likely to report higher levels of knowledge and confidence in providing care to TGSA patients.
A contributing factor to the reported lack of TGSA education may be that most respondents completed their SANE training five or more years ago (56.9%), and integration of TGSA content may not have been as prevalent then. Importantly, over half of participants reported they have provided care to a TGSA patient and more than 80% anticipate providing this care in the future. These findings emphasize the importance of including standardized content related to TGSA care as part of SANE curriculum and in continuing education offerings to address the gap in current SANE knowledge and practice.
The study’s limitations include a low overall response rate, a largely homogenous sample, and potential response and selection bias. Just before the start of the study, the IAFN changed its web platform, which required all members to create a new account and opt-in to receive email updates related to the different community forums. This may have limited the number of members who received study information. AFN members had less exposure, as the study information was posted in a community forum on the organization’s website and not automatically distributed via email.
Regarding the sample, most survey respondents identified as White females (limiting the generalizability of findings). Another limitation is potential selection bias related to the education and practice demographics of nurses who are members of professional organizations, and those who then choose to participate in research studies. Close to 35% of participants reported having a graduate degree in nursing (MSN, DNP, PhD), which is significantly higher than the 2020 national average of 17.1% (American Association of Colleges of Nursing, 2022). Further, almost 70% of participants had at least 11 years of practice, with 40.7% having over 20 years of experience. This level of education and experience may not reflect overall SANE demographics.
Furthermore, this study did not address the healthcare experiences of TG individuals following SA. Therefore, the relationship between SANE knowledge and confidence and actual TG patient experiences following sexual assault was not explored.
Recommendations
It is proposed that SANE curriculum include best practice recommendations related to the care of TGSA patients (IAFN, 2022). Lack of standardization on what constitutes best practice lends to inconsistent educational offerings, deficient SANE knowledge and confidence, and clinicians unable to meet the needs of transgender individuals seeking healthcare following SA. The incorporation of standardized, evidence-based TGSA content into SANE curriculum will help address the knowledge gap of new SANEs. Continuing education offerings must also be developed to address the gap in current SANE knowledge and practice as 56.4% of respondents reported previously providing care to a TGSA patient and 83% expect to do so in the future.
The World Professional Association for Transgender Health (WPATH) is composed of over 3,000 members involved in healthcare, social scientists, and legal professionals. WPATH develops standards of care (SOC) which offers clinical guidance for healthcare providers serving trans and gender diverse patients as well as evidence-based recommendations that impact education, research, and public policy surrounding trans issues. Topics within the SOC include: Terminology; Assessment of Adults, Adolescents, Children, Nonbinary, Eunuchs, Intersex Individuals, and those living in Institutional Environments; gender-affirming treatments such as Hormone Therapy, Surgery and Postoperative Care, Voice and Communication, Primary Care, Reproductive Health, Sexual Health, and Mental Health (Coleman et al., 2022). Researchers also support that quality gender-affirming care requires that the provider be knowledgeable about: gender and sexual orientation terminology; completing an anatomical inventory; hormone therapy, interactions, and adverse effects; and gender-affirming surgical procedures (Klein et al., 2018; Rosendale et al., 2018). The current study helps inform what SANEs perceive as necessary content to include in curriculum related to TGSA. Beyond terminology and gender-affirming treatments, SANEs specifically request education on identifying genital structures, exam considerations when assessing surgically created genitalia, medication considerations post-SA, and referral to trans-positive resources and services.
Future research must evaluate what transgender individuals perceive as important for clinicians and SANEs to consider when offering and providing medical-forensic exams following SA as they are the ultimate expert in what constitutes trans-affirming care. The combined results of WPATH recommendations, SANE perspectives, and patient considerations, will provide a comprehensive foundation to inform best practice recommendations for TGSA content in SANE curriculum. An outcome could be the increased likelihood of trans individuals seeking and receiving gender-affirming care following SA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.