
Abstract
The aim of this study is to measure the effectiveness of an acceptance and commitment therapy (ACT)-based group intervention program on post-traumatic stress (PTS) symptoms, psychological inflexibility, and self-compassion in intimate partner violence (IPV) survivor university women. The research was conducted at a state university in İstanbul, Türkiye. Participants consisted of 22 IPV survivor university women with 10 in the treatment group and 12 in the waitlist-control group. Participants were assigned to groups based on their preferences. The treatment group participated in a 12-session ACT intervention group, each lasting 120 to 150 min. During this period, no intervention was applied to the waitlist-control group. At the end of the treatment, the intervention group’s average PTS symptom scores and psychological inflexibility scores significantly decreased, while their self-compassion scores significantly increased. This effect persisted during the 1-month follow-up period. On the other hand, no changes were observed in the PTS, psychological inflexibility, and self-compassion levels of the control group. When comparing the treatment group with the control group, it was observed that the treatment group had significantly lower levels of PTS and psychological inflexibility and significantly higher levels of self-compassion in both the post-test and follow-up assessments. Consequently, the results revealed the effectiveness of the program on PTS, psychological inflexibility, and self-compassion among a group of IPV survivor university women. Thus, we concluded that ACT may serve as an effective therapy for addressing IPV among university women and that it is culturally applicable to the Turkish context.
Keywords
Introduction
Violence against women is a human rights violation and a public health issue that affects women of different age groups worldwide. The World Health Organisation’s (WHO, 2024) draft of the 14th General Programme of Work for 2025 to 2028 emphasizes that women continue to be disadvantaged in terms of gender inequality, violence, and particularly intimate partner violence (IPV). In the global fight against IPV, empowering IPV survivor university women is particularly important because, as noted by Straus (2004), IPV experiences during this period can establish patterns that endure throughout one’s lifetime. Furthermore, a great deal of research indicates that IPV is notably prevalent among university women. Although research provides varying results regarding gender differences in IPV victimization and underlines its bidirectional nature (Rubio-Garay et al., 2017) it is a fact that female university students experience all kinds of IPV at high rates (e.g., Harned, 2002; Rennison & Addington, 2018; Spadine et al., 2022; Straus, 2004).
Studies conducted in Türkiye reveal high rates of IPV victimization among female university students, similar to findings from other countries. In their study, Toplu and Hatipoğlu-Sümer (2011) reported a prevalence of 46% for physical violence and 85% for psychological violence among female university students. In another study, Toplu-Demirtas et al. (2013) reported that 79.5% of female university students experienced at least one instance of physical, sexual, and/or psychological violence. Schuster et al. (2016) noted that 77.6% of female university students were sexually victimized, primarily by their current or ex-partners.
Research has demonstrated that exposure to IPV is associated with a variety of mental health problems both among women and university students. A recent meta-analysis study revealed the association of IPV victimization to depression, anxiety, post-traumatic stress disorder (PTSD), and suicidal ideation among women (White et al., 2024). Pengpid and Peltzer (2020), in their study with 18,335 university students from 25 countries, found that IPV victimization was associated with depression, PTSD, sleeping problems, loneliness, and addictive behaviors. In a recent study conducted with female university students in Türkiye, women who were exposed to IPV were found to have significantly higher levels of post-traumatic stress (PTS) symptoms compared to those who were not exposed (Yılmaz, 2023).
In addition to all these mental health problems, research also reveals the relationships between IPV victimization, PTS symptoms, psychological inflexibility (PI), and self-compassion (SC). For example, Palm and Follette (2011) reported the relationship between experiential avoidance, an indicator of psychological inflexibility, and PTS symptoms among female survivors of interpersonal violence. Mclean et al. (2018) found a negative relationship between psychological inflexibility and self-compassion among female survivors of interpersonal violence. Komlenac et al. (2023) reported that higher interpersonal violence victimization including IPV was associated with lower self-compassion among women (see the Supplemental Material of the article). In light of all these studies, it can be inferred that reducing psychological inflexibility and increasing self-compassion would be effective in alleviating PTS symptoms in women exposed to IPV. In this context, Acceptance and Commitment Therapy (ACT), which is based on psychological flexibility and self-compassion, emerges as an ideal method.
ACT, Trauma, and IPV Interventions
ACT is a third-wave Cognitive-Behavioral Therapy that posits psychological inflexibility as the core underlying all psychological problems. Psychological inflexibility refers to behavior that is guided by unwanted inner experiences (e.g., thoughts, feelings, bodily sensations, memories, images related to a traumatic event) rather than personal values (Bond et al., 2011). Consistent with the theory, psychological inflexibility is associated with mental health issues, such as depression, anxiety, eating disorders, substance use disorders, and PTSD (Levin et al., 2014). PTS symptoms are particularly relevant for psychological inflexibility (Walser & Westrup, 2007). Psychological inflexibility involves efforts to avoid and control internal experiences. Among PTS symptoms, there is also an effort to avoid internal experiences related to trauma (DSM–5; American Psychiatric Association, 2013). On the other hand, when individuals try to control their internal experiences related to trauma, this effort can have the opposite effect, leading them to experience trauma-related internal experiences more intensely (Walser & Westrup, 2007). Therefore, reducing psychological inflexibility, or in other words, increasing psychological flexibility, could be an effective way to alleviate trauma symptoms.
ACT offers a systematic approach to addressing trauma-related issues, designed to assist clients in discovering a meaningful life that transcends their traumatic experiences (McLean & Follette, 2016). The therapy process is based on a six-stage psychological flexibility model, which includes self as context, defusion, acceptance, contact with the present moment, values, and committed action (Hayes et al., 2006). The goal of ACT is to enhance psychological flexibility by developing skills in these six areas. ACT inherently incorporates self-compassion (Harris, 2021). It also utilizes mindfulness exercises but places present-moment awareness in a distinct context separate from spiritual mindfulness (Hayes et al., 2004).
The effectiveness of ACT in reducing PTS symptoms has been demonstrated through both case studies (e.g., Burrows, 2013) and group intervention studies (e.g., Boals & Murrell, 2016). Although ACT interventions specifically targeting IPV are not yet widespread, studies involving both IPV perpetrator men and IPV survivor women demonstrate the effectiveness of ACT. For instance, Zarling et al. (2019) assessed ACT’s effectiveness in reducing domestic violence among male perpetrators, finding that those receiving ACT had significantly fewer new charges, including domestic assault and other violent offenses, compared to those undergoing the Duluth Model and CBT. Baberi et al. (2022) found that ACT was effective in reducing domestic violence exposure among women experiencing emotional divorce. Fiorillo et al. (2017) reported initial evidence supporting the effectiveness of a web-based ACT intervention in alleviating psychological inflexibility, depression, anxiety, and PTSD in women who have encountered various forms of interpersonal violence, including IPV. Nikparvar et al. (2023) found that ACT was effective in reducing symptoms of depression and stress, as well as enhancing resilience in married women who have reported experiencing ongoing IPV.
Current Study
The most recent nationwide state-supported study on violence against women in Türkiye was conducted in 2014. The data from 2014 highlighted the high rates of violence against women with 33% reporting physical IPV, 11% reporting sexual IPV, 44% reporting psychological IPV, and 30% reporting economic IPV (HUIPS, 2015). As we estimate from the number of cases brought to court and women seeking help through social media, violence against women has increased in the last 10 years. However, we do not know the exact nationwide rate of this increase. As we do not know the extent of the increase in violence over the past decade, intervention programs aimed at healing the wounds of violence and empowering women survivors of violence are not receiving the necessary attention from policymakers and mental health researchers. When it comes to university women, the high rates of IPV among university students in Türkiye highlight the need for such intervention programs.
An analysis of IPV intervention programs in Türkiye reveals a scarcity of research focused on married women or those residing in shelters (e.g., Emirza, 2023; Yıldırım, 2019). When examining programs specifically developed for university students in Türkiye, only a few prevention programs are found, primarily aiming to increase awareness of IPV and change attitudes toward it (e.g., Göz & Dokuzcan, 2023; Toplu-Demirtaş & Aracı-İyiaydın, 2025; Üstünel, 2020). Recently, a study examining the effectiveness of ACT in a mixed group of female and male university students who experienced IPV was published (İlyas, 2024). The aim of this study was to enhance psychological flexibility and develop coping skills to deal with violence. However, there are no intervention programs that are designed for female university students, aim to reduce the negative effects of IPV and contribute to positive mental health, with experimentally proven effectiveness. Therefore, this study was designed with careful consideration of a significant need. The purpose of the study is to evaluate the effectiveness of a 12-session ACT-based group intervention program developed for IPV survivor university women on PTS symptoms, psychological inflexibility, and self-compassion.
Methods
Recruitment
The program announcement was communicated to all university students via email and through posters displayed in various locations across the university where the study was conducted. Students accessed the application form including the informed consent form and the pre-test measurement scales through the announcement link and the QR code on the poster. The inclusion criteria specified in the informed consent form were as follows: not having received any psychiatric diagnosis, currently not using any psychiatric medication, currently not receiving any psychotherapy/counseling, having experienced at least one type of psychological, physical, and/or sexual violence in an intimate relationship, and having had at least 1 month passed since the complete termination of that relationship. As part of assessing the complete termination of the relationship, participants were also asked whether they had any form of contact with their former partners, experienced stalking, or received any kind of threats. We established the final criterion mentioned to eliminate the 1-month risk period for acute stress disorder (ASD). ASD is characterized by stress responses that arise between 3 days and 4 weeks following a traumatic event and typically subside after 1 month (DSM–5; American Psychiatric Association, 2013). Including participants in this phase could threaten the internal validity of the study by raising doubts about whether the reduction in traumatic stress symptoms was due to the intervention or natural healing. Consequently, we set the ASD risk period as an exclusion criterion.
Applicants who met all the criteria were invited for a preliminary interview to receive more detailed information about the study and to sign the written consent. A total of 45 female university students filled in the application form. Among them, 26 met the inclusion criteria and were invited for a preliminary interview. All of them agreed to participate in the study and signed the written consent. Due to the varying class schedules, the program’s timing was not suitable for all participants. Therefore, participants were allocated to either the treatment or waitlist-control groups based on their preferences. This resulted in 12 participants in the treatment group and 14 in the control group (Figure 1).
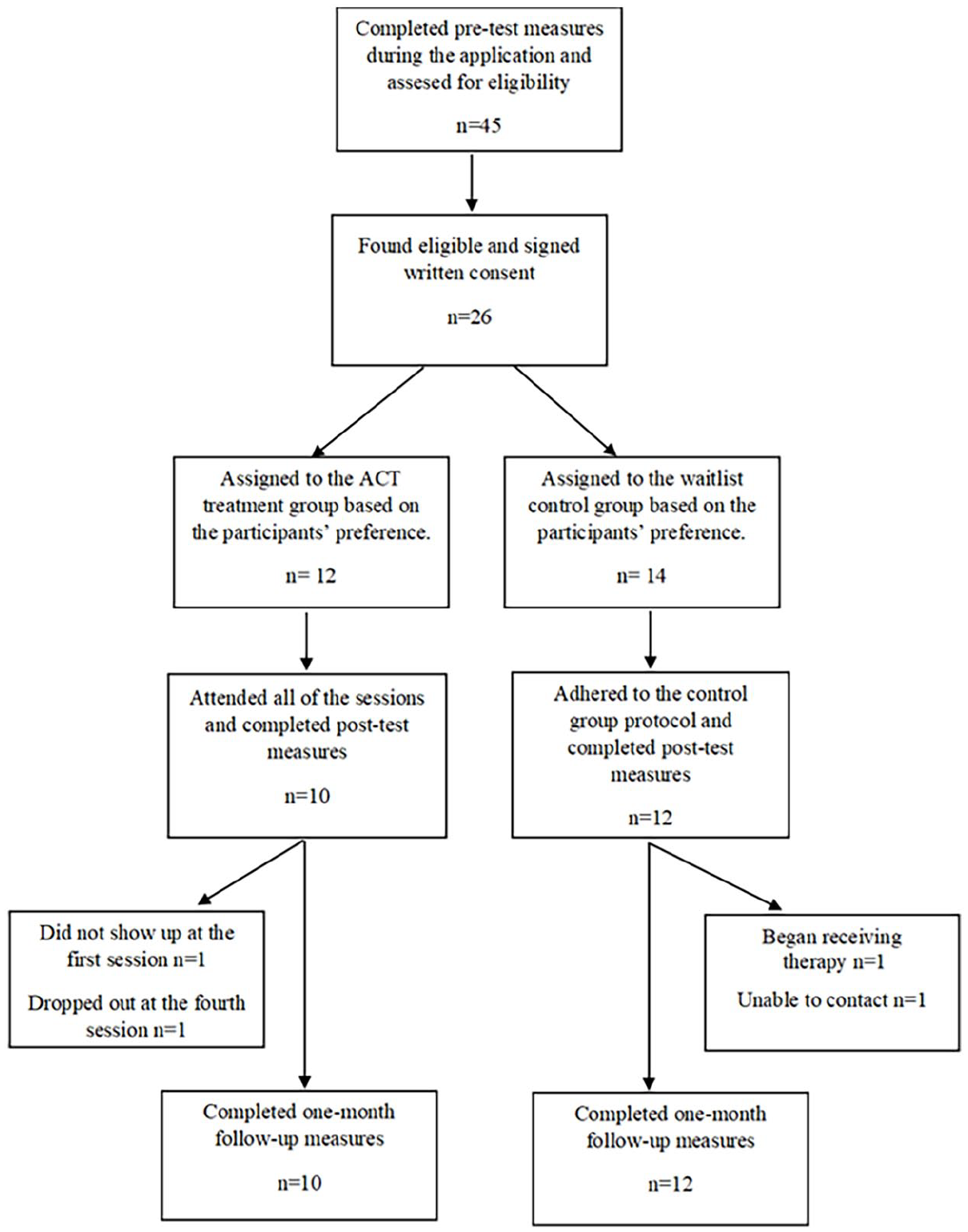
Participants’ flow diagram.
In the treatment group, one participant did not attend the first session and later informed us that she had decided to withdraw from the study. Another participant dropped out in the fourth session due to difficulties in managing both her part-time job and the group sessions. In the control group, one participant was unreachable for the post-test measurement, and another participant indicated that she had started another therapy process before the post-test measurement. Consequently, two participants from the treatment group and two from the control group were excluded from the study. The final sample consisted of 10 participants in the treatment group and 12 participants in the control group.
Participants and Procedure
The participants consisted of a total of 22 IPV survivor female university students, with 10 in the treatment group and 12 in the control group. The average age of participants in the treatment group was 23.20 (SD = 3.55), while the average age of participants in the control group was 22.50 (SD = 2.64) (Table 1).
Participants’ Characteristics.

The participants completed the pre-test measures during the application process. The treatment group participated in a 12-session ACT-based group intervention program. Sessions were held face-to-face on the university campus, twice a week for 6 weeks. Each session lasted 120 to 150 min. During this period, no intervention was applied to the waitlist-control group. The post-test measurement was conducted immediately after the sessions ended, and the follow-up measurement was conducted 1 month later using Google Forms.
Upon the completion of the research process, we re-engaged with the participants from the waitlist-control group. We extended an invitation for them to participate in the ACT group intervention program, which had previously been administered to the experimental group. We communicated to the participants that the scheduling of the sessions would be collaboratively determined. However, all participants declined our invitation. When we asked participants why they declined the invitation, they provided responses such as not currently wanting to seek help or being unable to allocate time for such a program due to the demands of their academic schedules. In response to this, we organized a 2-hr online workshop, facilitated by the first author of the study. During the workshop, we provided comprehensive information regarding the various forms of IPV, potential warning signs indicative of a partner’s propensity for violence, the characteristics of a healthy romantic relationship, and strategies for establishing and maintaining boundaries within intimate relationships. Finally, we informed participants about the counseling services provided by the university’s psychological counseling center and those conducted under supervision training by the department of psychological counseling. We encouraged them to utilize these resources to seek psychological help if needed.
Group Leader
The first author of the study led the sessions. She completed both undergraduate and master’s education in psychological counseling and is currently at the dissertation stage of a doctoral program in the same field. She has approximately 14 years of experience working in the field of psychological counseling. She has completed basic and advanced ACT training at the Turkish branch of the Association for Contextual Behavioral Science. Additionally, she has received theoretical and supervision training in psychological trauma. She works as a research assistant in the Department of Psychological Counseling at a state university in Istanbul and provides counseling services to trauma survivors.
The ACT-Based Group Intervention Program
The ACT-based group intervention program consists of 12 face-to-face sessions, each lasting 120 to 150 min. Various ACT books were consulted to prepare the program (Follette & Pistorello, 2007; Harris, 2022; Hayes & Smith, 2005; Stoddard & Afari, 2014; Walser & Westrup, 2007; Westrup & Wright, 2017). The techniques implemented in the program were specifically adapted to focus on women and IPV. The program employed various forms/worksheets for recording emotions, thoughts, bodily sensations, and behaviors both during sessions and as homework exercises between sessions. Audio recordings of ACT-specific acceptance and defusion techniques and mindfulness techniques used in the sessions were provided to participants as homework exercises to be practiced between sessions. Participants were sent forms via email to record their home exercises. They submitted the completed forms to the group leader via email 1 day before each session. At the beginning of each session, the group leader provided feedback to the participants regarding the home exercises they performed. The feedback addressed the skills that participants found challenging and discussed how they could improve their performance. For example, if a participant identified a “value-based behavior” that was challenging for them, strategies such as breaking the behavior down into smaller steps or teaching and testing a new “differentiation” technique if the original one was ineffective were employed. The follow-up on between-session exercises ensured that participants’ commitment to the process and their progress were regularly monitored.
The first session of the program included members’ introductions, identifying the purposes for joining the group, and an introduction to the psychological flexibility model. In the second and third sessions, participants shared their experiences with violent relationships and how these relationships had impacted their current lives. The fourth session was dedicated to the Creative Hopelessness and Willingness intervention, a specific ACT technique. This session aimed to demonstrate the ineffectiveness of the experiential avoidance strategies participants use to cope with unwanted internal experiences related to their violent relationships and to encourage willingness to make room for those experiences. The dimensions of ACT—self as context, cognitive defusion, acceptance, values, and committed action—addressed in subsequent sessions. Mindfulness/being present practices were incorporated into each session, rather than having a separate session dedicated specifically to mindfulness. Between the fifth and eighth sessions, participants evaluated their past relationships and internal experiences from an ACT perspective and learned skills for experiencing the contextual self, acceptance, and cognitive defusion. These skills aim to help participants reinterpret their internal experiences within the ACT framework. In the ninth session, participants identified their values in different life domains (e.g., mental health, family, education, romantic relationships) and determined actionable steps aligned with these values within the mental health domain. In the program, the mental health domain was defined as “my relationship with myself.” The 10th session focused on discussing the challenges they faced while implementing the value-based steps and the extent to which they were able to apply the acceptance and defusion skills they had learned to cope with these challenges. Additionally, this session included a discussion on the characteristics of a healthy romantic relationship and the warning signs that a potential partner may be prone to violence. Participants were encouraged to reflect on the signs indicating that their past partners were prone to violence, helping them gain awareness. It was emphasized that ending a relationship with a violent partner is challenging, making early recognition and avoidance of such relationships a better strategy. In the 11th session, there was again an evaluation of the committed actions undertaken and encouragement for future actions. Additionally, to ensure participants have a roadmap for their value-oriented future goals after the group concludes, they break down their selected short-term, medium-term, and long-term goals into achievable action steps. Finally, considering their values in the domain of romantic relationships and the discussion from the previous session, participants defined the boundaries they wish to maintain in future relationships. In the 12th session, the group evaluated their overall progress and shared their feelings about concluding the program, culminating in farewells (see the Supplemental Material for the ACT-Based Intervention Program Outline).
Pilot Study and Program Revision
The single-arm pilot feasibility study of the intervention program (Bektaş-Aydın & Yüksel-Şahin, 2025) was conducted with eight IPV survivor university women. The sessions were conducted face-to-face on the university campus. At the end of the pilot study, significant improvements were observed in participants’ PTS symptoms, psychological inflexibility, and self-compassion scores. The improvements were sustained at the end of a 1-month follow-up period. Feasibility and acceptability measures revealed that the program had high feasibility and acceptability rates.
While the pilot study demonstrated the initial feasibility and acceptability of the program, we decided to make some updates to the program based on our experiences gained from the pilot study. When designing the program, we allocated one session for an introduction, one session for taking the violence story, one session for the creative hopelessness-willingness intervention, which is a preparatory intervention specific to ACT, one session for each of the six phases of ACT (since present moment awareness was incorporated into each session, no separate session was allocated for it), one extra session for developing acceptance, defusion, and self-compassion skills, and one session for termination. This structure resulted in a total of 10 sessions for the program. At the end of the pilot study, we decided to add two more sessions to the program. To obtain more in-depth information about participants’ experiences of violence and to provide them with more opportunities for expression, we doubled the number of “violence story” session. Additionally, we doubled the number of “committed action” session to enable participants to work more on their value-based behaviors. Consequently, the number of sessions in the pilot study increased from 10 to 12. We also adjusted the sequence of sessions by moving the “values” session from fourth position to immediately before the first session on “committed action” to ensure thematic coherence. By incorporating content on recognizing danger signs of a violence-prone partner, the characteristics of a healthy romantic relationship, and identifying boundaries to protect in line with personal values, we have endowed the committed action sessions with protective and preventive qualities.
Intervention Fidelity
The researchers developed a program manual that detailed the content and techniques to be applied in each session step by step. A pilot study of the research was recorded, and the second author checked the sessions’ content for alignment with the manual. In the pilot study, the intervention showed over 95% adherence to the manual. In this study, the sessions were not recorded. The group leader was the same person as in the pilot study and conducted the process in the same manner. Additionally, to ensure consistency with the manual, the group leader kept a researcher journal, where she took notes on the process at the end of each session. The consistency of the sessions’ content with the manual was checked by comparing the researcher journal with the program manual, and again, over 95% adherence was observed.
Measures
Personal Information
We developed a personal information form to obtain certain demographic information from participants and determine their suitability for participating in the study. The form collected information regarding participants’ gender, age, education level, sexual orientation, duration of the violent relationship, time since the relationship ended completely, presence of psychiatric diagnosis, use of psychiatric medication, and current engagement in psychotherapy/counseling.
IPV Victimization
We measured IPV victimization using the Turkish version (Aba & Kulakaç, 2016) of the Conflict Tactics Scales-Revised (CTS2; Straus et al., 1996). CTS-2 simultaneously measures victimization and perpetration of IPV. In this study, we used the subscales of Psychological Aggression (PsyA), Sexual Coercion (SCO), Physical Assault (PhyC), and Injury (INJ) under the victimization dimension. These sub-scales collectively comprise 33 items. PsyA consists of eight items and measures behaviors such as insulting, yelling, and accusing (e.g., “My partner accused me of being a lousy lover.”). SCO consists of seven items and measures behaviors such as using threats or force to make a partner have sex (e.g., “My partner used threats to make me have sex”). PhyC consists of 12 items and measures behaviors such as kicking, beating up, and choking (e.g., “My partner kicked me.”). INJ consists of six items and measures severe situations such as breaking of bones or intentional burning (e.g., “My partner burned or scalded me on purpose”). The scale employs two distinct scoring methods to assess both prevalence and chronicity. In this study, the scoring system designated for prevalence was employed. Under this protocol, occurrences of violence (ranging from response categories 1–7) were uniformly coded as 1, irrespective of frequency or time, whereas instances devoid of violence were coded as 0. The Turkish CTS2 translation study showed good validity and reliability. Aba and Kulakaç (2016) reported Cronbach’s alphas of the Turkish version of the subscales to be .85 for PsyA, .79 for SCO, .89 for PhyA, and .76 for INJ. Test-retest reliability coefficients of the scale and the sub-scales were between .97 and 1.00. To assess construct validity, the scores obtained by women and men on the overall scale and its sub-scales were compared using t-tests. The observation of a significant difference in the expected direction between these two groups was considered an indicator of the test’s construct validity. Content validity was assessed by six specialists, and the results indicated no significant differences among their evaluations (W = 0.247, p > .05).
Psychological Inflexibility
We measured psychological inflexibility using the Turkish version (Yavuz et al., 2016) of the Acceptance and Action Questionnaire-II (AAQ-II; Bond et al., 2011). AAQ-II has seven items (i.e., “My painful experiences and memories make it difficult for me to live a life that I would value”), rated on a 7-point Likert scale. Higher scores obtained from the scale indicate higher psychological inflexibility/lower psychological flexibility. The Turkish AAQ-II translation study showed good validity and reliability. Yavuz et al. (2016) reported Cronbach’s alpha for the Turkish version of AAQ-II to be .84. Test-retest reliability coefficient was .85. For concurrent validity, the scale was compared with the Beck Depression Inventory, the State-Trait Anxiety Inventory, the Panic Disorder Severity Scale, and the Padua Inventory-Washington State University Revision, which was developed to measure obsessive-compulsive disorder. The correlation coefficients between the Turkish version of AAQ-II and the other scales were found to be statistically significant: .63 for depression, .53 for anxiety, .67 for obsessive-compulsive disorder, and .67 for panic disorder. Regarding predictive validity, the scale was examined in both clinical and non-clinical groups, with the clinical group showing significantly higher mean scores. The effect size of the difference was determined to be medium (eta squared: .08).
Self-Compassion
We measured self-compassion using the Turkish version (Deniz et al., 2008) of the Self Compassion Scale (SCS; Neff, 2003). The Turkish version of SCS is a 5-point Likert-type scale comprising 24 items (i.e., “I try to be loving towards myself when I’m feeling emotional pain.”). The Turkish adaptation study revealed a unidimensional structure of the scale. Higher scores obtained from the scale represent higher self-compassion. Deniz et al. (2008) reported Cronbach’s alpha for the Turkish version of SCS to be .89. The test-retest reliability coefficient was .83. To assess the criterion validity of the scale, its relationship with self-esteem, life satisfaction, positive affect, and negative affect was examined. The correlation coefficients between the scale and the other variables were found to be statistically significant: .62 for self-esteem, .45 for life satisfaction, .41 for positive affect, and −.37 for negative affect.”
Post-Traumatic Stress
We measured PTS using the Turkish version (Boysan et al., 2017) of the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders (PCL-5; Weathers et al., 2013). The Turkish version of PCL-5 consists of a total of 20 items (i.e., “How much you have been bothered by repeated, disturbing dreams of the stressful experience?”) rated on a 5-point scale to assess experiences over the past month. Higher scores obtained from the scale indicate higher symptom severity. The Turkish PCL-5 translation study showed good validity and reliability. Boysan et al. (2017) found composite reliability to be .94 and .97 for a non-clinical/university student group and a clinical group respectively. The test-retest reliability coefficient was .80. To measure the construct validity, the relationship between the PCL-5 and the Trauma Symptoms Checklist-40 (TSC-40) was examined, and the correlation coefficient between the two scales was found to be .75.
Ethics
The study complies with the Declaration of Helsinki. The study procedures were approved by the institutional ethics committee (Report No. 20221101681). Additionally, all participants provided written consent. The written consent included an agreement to uphold mutual confidentiality. Since the participants were selected from individuals whose relationships had completely ended and who had no contact with their former partners, there was no significant safety risk. The university where the study was conducted was closed to visitors other than its own students, faculty, and their guests, and was safeguarded by private security personnel. Among the experimental group participants, two had former partners attending the same university. The safety of these participants was closely monitored during the process, and they were instructed to inform the group leader if they encountered any risky situations. Additionally, all participants were provided with information about official resources they could contact in case of an emergency. No such incidents occurred during the study.
Data Analysis
In nonrandomized studies of preexisting groups, ANOVA of change from baseline is less biased than ANCOVA (Van Breukelen, 2006). Therefore, we preferred ANOVA over ANCOVA. The study has a 2 × 3 factorial design (i.e., one treatment and one control group, three timeline measurements). In accordance with the study design, we run mixed-design repeated-measures ANOVAs for each of the three dependent variables to analyze the data. We used per protocol analysis and omitted individuals with missing post-test measurements from the analysis. Therefore, we reported the baseline statistics for the groups based on the 22 participants who completed all measurements. We used IBM SPSS 26.0 for data analysis.
Results
Preliminary Analyses
We conducted descriptive analysis, checked mixed-design repeated-measures ANOVA assumptions, and ran t-test to determine if there was a significant difference between the average baseline scores of the treatment and control groups. The skewness and kurtosis values for each variable were within the range of −3 to +3, and the Shapiro-Wilk test was insignificant, indicating that the data met the assumption of normality (Field, 2018). Due to its sensitivity to sample size, Mauchly’s test is not highly recommended for assessing whether the sphericity condition has been met (Field, 2018). Therefore, following Field’s recommendation, we disregarded the Mauchly’s test results and routinely reported the results from the Greenhouse-Geisser corrected lines. Box’s M results showed that homogeneity of variance-covariance matrixes assumption was met for PTS (F [6, 2613] = 0.55, p = .77), PI (F [6, 2613] = 0.13, p = .99), and SC (F [6, 2613] = 1.71, p = .12). The Levene’s test results were insignificant across all three time points for each outcome variable, with p-values ranging from .30 to .99, indicating that the assumption of homogeneity of variances was met. Therefore, we concluded that the data were suitable for conducting mixed-design repeated-measures ANOVA (see the Supplemental Material for the table of Descriptives and Normality Tests of the Study Variables for the Treatment and Control Groups).
We run t-test to determine if there were significant differences between the PTS, PI, and SC scores of the groups at baseline. The Bonferroni-adjusted results indicated that there were no significant differences in the PTS (t[20] = 0.24, p = .81), PI (t[20] = 0.50, p = .62), and SC (t[20] = 1.14, p = .27) pre-test scores between the treatment and control groups.
The Effectiveness of the Treatment on PTS
The mixed-design repeated-measures ANOVA results revealed a significant main effect of group on average PTS scores (F [1, 20] = 8.42, p < .01, ηp2 = .30). The main effect of time on PTS scores was found significant (F [1.98, 39.51] = 23.11, p < .001, ηp2 = .54). However, this effect was accompanied by a significant time × group interaction (F [1.98, 39.51] = 9.67, p < .001, ηp2 = .33) (Figure 2).
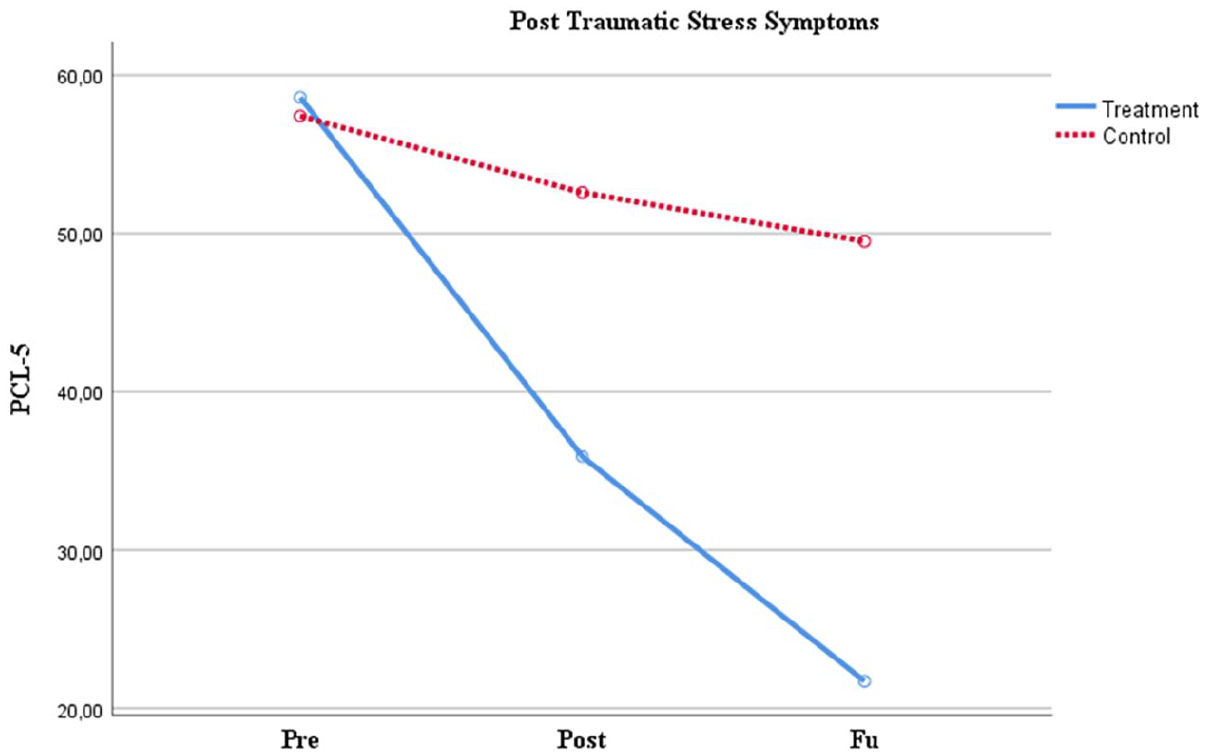
Mean change of PTS across groups for the three time points.
The interaction means that change in PTS scores over time depends on group membership. To break down this interaction, we conducted a series of simple effects tests (Pallant, 2011). Simple effects tests using the Bonferroni correction indicated a significant decrease in the PTS scores of the treatment group from pre-test to post-test (MD = 22.70, p < .01), pre-test to follow-up (MD = 36.90, p < .001), and post-test to follow-up (MD = 14.20, p < .05). On the other hand, the control group showed no statistically significant change in PTS scores across the three time points (see Table 2). The treatment group exhibited significantly lower PTS scores compared to the control group on both the post-test (MD = −16.68, p < .05) and follow-up (MD = −27.80, p < .001).
Bonferroni-Adjusted Pairwise Comparisons for Mean Differences Across Three Time Points.

Note. PCL-5 = PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders; AAQ-II = Acceptance and Action Questionnaire-II; SCS = Self Compassion Scale; MD = mean difference.
The Effectiveness of the Treatment on PI
The mixed-design repeated-measures ANOVA results indicated a significant main effect of group on average PI scores (F [1, 20] = 10.54, p < .01, ηp2 = .35). The main effect of time on PI scores was found significant (F [1.40, 27.98] = 36.86, p < .001, ηp2 = .65). On the other hand, this effect was qualified by a significant time × group interaction (F [1.40, 27.98] = 18.98, p < .001, ηp2 = .49) (Figure 3).
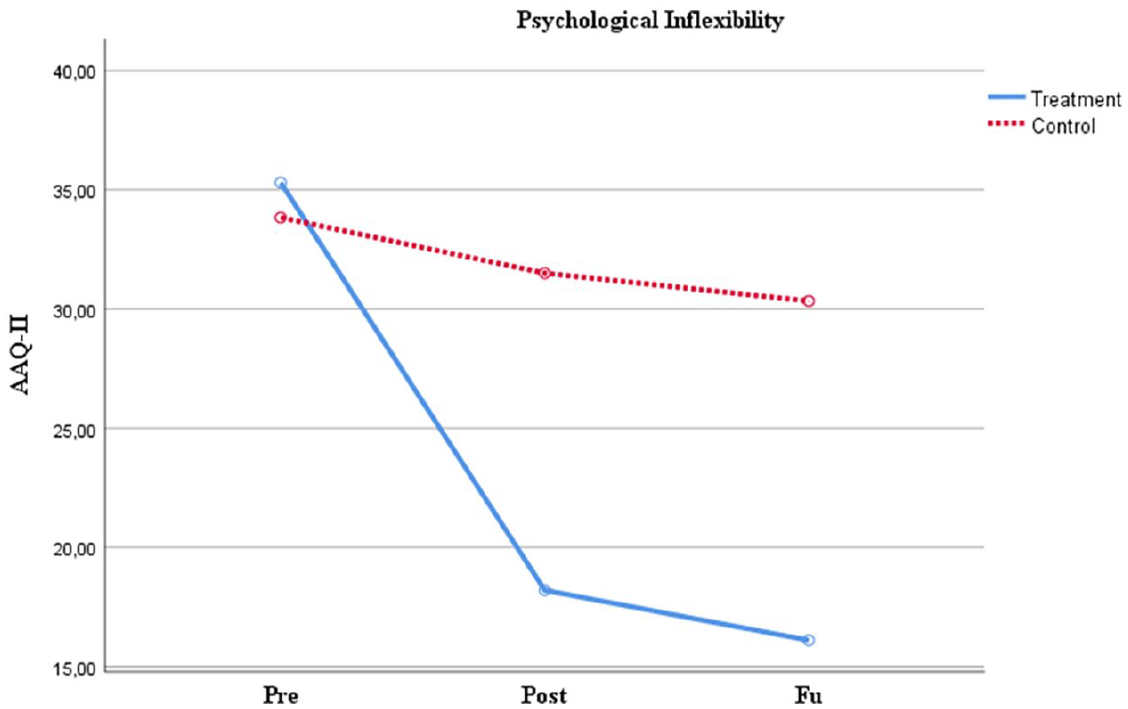
Mean change of PI across groups for the three time points.
Simple effects tests using the Bonferroni correction revealed a significant decrease in the PI scores of the treatment group from pre-test to post-test (MD = 17.10, p < .001) and pre-test to follow-up (MD = 19.20, p < .001). On the other hand, the control group showed no statistically significant change in PTS scores across the three time points (see Table 2). The treatment group exhibited significantly lower PI scores compared to the control group on both the post-test (MD = −13.30, p < .01) and follow-up (MD = −14.23, p < .001).
The Effectiveness of the Treatment on SC
The mixed-design repeated-measures ANOVA results indicated a significant main effect of group on average SC scores (F [1, 20] = 21.86, p < .001, ηp2 = .52). The main effect of time on SC was significant (F [1.45, 29.03] = 32.46, p < .001, ηp2 = .62). However, there was also a significant time × group interaction for SC (F [1.45, 29.03] = 27.94, p < .001, ηp2 = .58). Simple effects tests using the Bonferroni correction revealed a significant increase in the SC scores of the treatment group from pre-test to post-test (MD = −34.60, p < .001) and pre-test to follow-up (MD = −23.30, p < .001) (Figure 4).
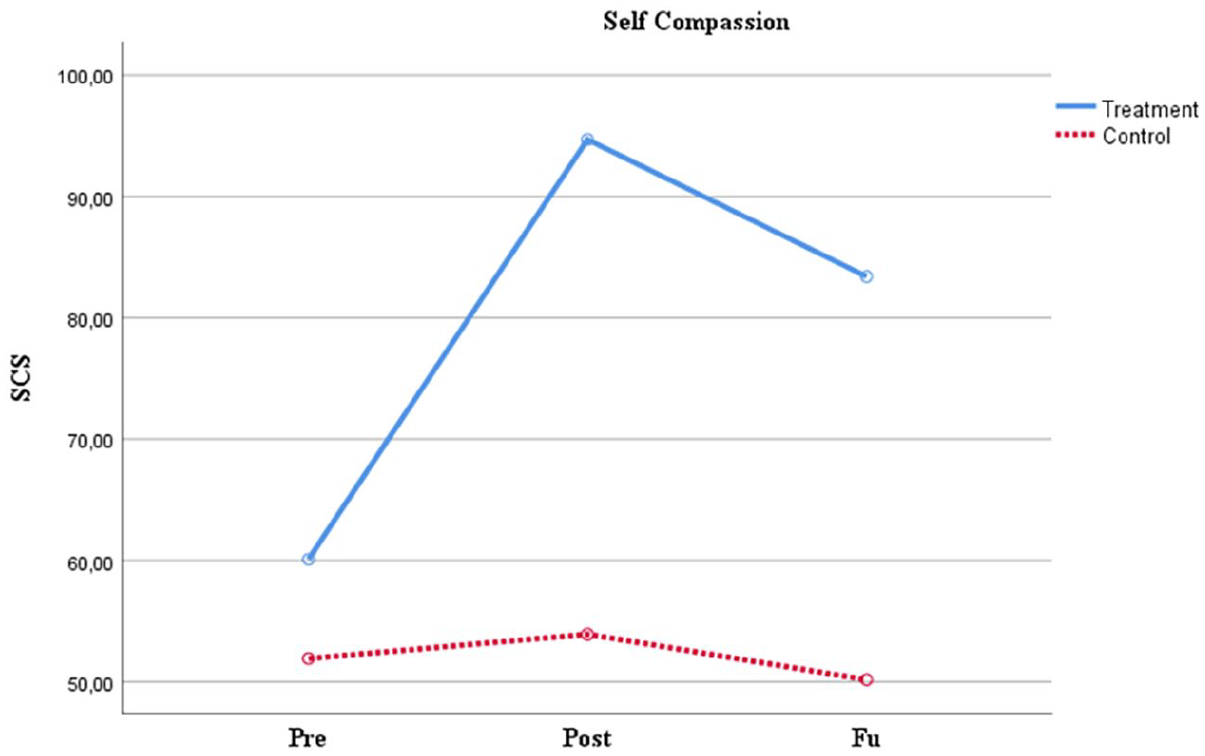
Mean change of SC across groups for the three time points.
A significant decrease from post-test to the follow-up (MD = 11.30, p < .001) was also noted. On the other hand, the progress achieved compared to baseline was maintained at follow-up. The control group showed no statistically significant change in SC scores across the three time points (see Table 2).
When comparing the treatment and control groups, the treatment group had higher SC scores than the control group in both the post-test (MD = 40.78, p < .001) and follow-up (MD = 33.23, p < .001).
Discussion
This study aimed to determine the effectiveness of an ACT-based group intervention program on PTS symptoms, psychological inflexibility, and self-compassion among IPV survivor university women. At the end of the program, the intervention group’s average PTS scores and psychological inflexibility scores significantly decreased, while their self-compassion scores significantly increased. This effect persisted during the 1-month follow-up period. On the other hand, no changes were observed in the PTS, psychological inflexibility, and self-compassion levels of the control group. When comparing the treatment group with the control group, it was observed that the treatment group had significantly lower levels of PTS and psychological inflexibility and significantly higher levels of self-compassion in both the post-test and follow-up assessments. Consequently, the results revealed the effectiveness of the program on PTS, psychological inflexibility, and self-compassion among this group of IPV survivor university women. We did not come across any other studies evaluating the effectiveness of ACT in IPV survivor university women. Along with this, the program’s effectiveness on PTS, psychological inflexibility, and self-compassion are consistent with the results of ACT studies conducted with women exposed to interpersonal violence and university students having IPV or another trauma history (e.g., Fiorillo et al., 2017; İlyas, 2024; Nikparvar et al., 2023; Yadavaia et al., 2014). The concurrent changes in IPV survivors’ PTS, psychological inflexibility, and self-compassion at the end of the treatment are consistent with previous research. Yadavaia et al. (2014) identified psychological flexibility as a significant mediator in the changes observed in self-compassion, depression, anxiety, and stress at the end of an ACT intervention. Moreover, they found that ACT intervention had a greater effect on self-compassion, depression, anxiety, and stress among those who had a trauma history.
The acceptance interventions included in the program encourage confronting unwanted internal experiences, being exposed to them for a while, and ultimately making room for them. Interventions involving exposure and acceptance are known to be effective in coping with PTS. Because they foster the capacity to endure distressing personal and situational stimuli, facilitate the reattribution of perceived danger or negative consequences associated with such stimuli, and enhance the awareness of the transient nature of even the most overwhelming psychological experiences (Lynn et al., 2012). The program incorporated various cognitive defusion techniques specific to ACT, equipping participants with the skills to use these techniques independently when needed. Research has shown that cognitive defusion techniques reduce emotional distress associated with thoughts and decrease avoidance behaviors (e.g., Barrera et al., 2015; Healy et al., 2008; Luciano et al., 2014). In this study, cognitive defusion interventions likely contributed to a reduction in PTS symptoms by decreasing participants’ avoidance of trauma-related memories and thoughts, as well as alleviating the emotional burden associated with those thoughts. Trauma can immobilize individuals, and experiential avoidance in traumatic experiences often manifests not only as an attempt to escape unwanted internal experiences but also as an avoidance of living a value-based meaningful life. In ACT, the processes of values and committed action are central to motivating clients to take action to live a life aligned with their values (Hayes et al., 2006). Engaging in value-based behaviors becomes easier for clients who have developed acceptance and cognitive defusion skills, as they learn to relate to their internal experiences differently rather than fighting against or avoiding them. Research indicates that engaging in committed action is related with lower psychological symptomology and higher well-being (e.g., Terhorst et al., 2020; Trindade et al., 2018). In this study, after working on acceptance and cognitive defusion skills, participants were encouraged to apply these skills in areas where they struggled to engage in committed action. Throughout the process, participants were observed transitioning from experiential avoidance to implementing value-based behaviors they had chosen. This progression is likely a significant factor contributing to the study’s findings.
The program is the first group intervention prepared for IPV survivor university women in Türkiye. Thus, it was also the first time it was proven that this specific group in Türkiye could benefit from a group intervention. While cultural, internal, and anticipated stigma act as barriers to help-seeking among IPV survivors (Overstreet & Quinn, 2013), the fact that young women were able to overcome these barriers, participate, and benefit from a group setting where they opened up sincerely is remarkable. The program is designed to provide ample opportunities for group interaction and includes techniques that involve members working together. Group interaction plays an important role in helping women who are survivors of interpersonal trauma normalize their abusive experiences and heal from trauma (Chouliara et al., 2020). Therefore, delivering ACT in a group format and enabling group interaction may have contributed to the gains achieved by the treatment group. A recent study (İlyas, 2024) found that ACT was effective in increasing psychological flexibility and positive coping skills for dealing with violence in a mixed group of female and male university students exposed to IPV. Our study, along with the results of this recent research, strengthens the evidence that ACT could be an effective therapy for university students exposed to IPV. Although there is no study evaluating the effectiveness of ACT among women exposed to IPV in Türkiye, Emirza (2023) showed that a mindfulness-based intervention program was effective in enhancing self-compassion and coping with stress in women staying in shelters due to IPV. This study, along with Emirza’s work, has demonstrated the cultural appropriateness of a therapy incorporating mindfulness elements for Turkish women who have experienced IPV.
Limitations and Future Directions
The most significant limitation of the study is that random assignments to groups were not possible. However, the inclusion criteria ensured that the groups had similar characteristics, and comparing the pre-test results also demonstrated that the groups were statistically equivalent in terms of study variables. Since participants were assigned to groups based on their own preferences, researcher bias was not a threat to the assignment process. Nonetheless, ensuring randomization in future studies is important for the generalizability of the results. Another limitation of the study is its small sample size. Perhaps because IPV tends to remain hidden in Türkiye, the number of applications to the program was notably lower compared to studies conducted in other countries. Therefore, increasing the sample size with new studies is important for enhancing the generalizability of the results. Due to the small sample size, mediation analysis could not be performed, and factors affecting change at the end of the treatment were not investigated. Future studies could explore factors affecting change by maintaining a larger sample size. Additionally, future studies could investigate ACT’s effectiveness on IPV survivor women with varying levels of education and from different sexual orientations. Psychological inflexibility is related to the risk of interpersonal violence revictimization (Fiorillo et al., 2013). Conversely, reducing psychological inflexibility by the program may decrease the likelihood of IPV revictimization. Therefore, future studies could test ACT’s effectiveness on revictimization.
The program is planned to be made available as a user manual to IPV mental health researchers in Türkiye, allowing its effectiveness to continue to be tested. Therefore, we would like to offer some recommendations for them. As mentioned above, group therapy is an effective method for women who are trauma survivors. However, future studies could test the effectiveness of the program in an individual therapy format. Additionally, ACT could be delivered in an online group therapy format. Currently, the program includes several techniques that require face-to-face interaction with multiple participants. On the other hand, ACT has a vast repertoire of techniques and metaphors (see Stoddard & Afari, 2014), and future researchers could easily update the program by replacing the mentioned techniques with new ones to fit their desired format. Consequently, they can evaluate the effectiveness of individual and online formats of the program among IPV survivor university women through pilot feasibility studies followed by experimental designs. Given the workload of psychological counseling centers at universities in Türkiye (Erkan et al., 2011), it is important for mental health professionals working in these centers to benefit from evidence-based group intervention programs, both to enhance the quality of services provided and to reduce the centers’ workload. Therefore, we suggest and hope that the effectiveness of the program continues to be tested on IPV survivor university women studying at different universities and in other cities of Türkiye. This may improve the generalizability of the findings related to the program’s effectiveness on IPV survivor university women. Consequently, the program could be implemented by university psychological counseling centers, thereby enabling them to offer more effective support to IPV survivor university women. Furthermore, other institutions and organizations that provide support to IPV survivor university women could benefit from the program. We hope that this study will inspire many future intervention studies and contribute to breaking the cycle of violence through the empowerment of young women in Türkiye.
Conclusion
The effectiveness of the ACT-based group intervention program developed for female university students who have experienced IPV was examined using a mixed-design repeated measures ANOVA. At the end of the program, the treatment group’s PTS symptoms and psychological inflexibility (PI) scores significantly decreased, while their self-compassion (SC) scores significantly increased. In contrast, no significant changes were observed in the PTS, PI, and SC scores of the control group. Although there were no significant differences in the PTS, PI, and SC scores between the two groups at baseline, by the end of the treatment and at the 1-month follow-up, the treatment group had significantly lower PTS and PI scores and significantly higher SC scores compared to the control group. In conclusion, the ACT-based group intervention program was found to be effective in reducing PTS symptoms and psychological inflexibility, and in increasing self-compassion among a group of female university students who have experienced IPV.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605251318283 – Supplemental material for Effectiveness of Acceptance and Commitment Therapy on Post-Traumatic Stress Symptoms, Psychological Inflexibility, and Self-Compassion in IPV Survivor University Women
Supplemental material, sj-docx-1-jiv-10.1177_08862605251318283 for Effectiveness of Acceptance and Commitment Therapy on Post-Traumatic Stress Symptoms, Psychological Inflexibility, and Self-Compassion in IPV Survivor University Women by Ceren Bektaş-Aydın and Fulya Yüksel-Şahin in Journal of Interpersonal Violence
Footnotes
Acknowledgements
We would like to express our sincere gratitude to the participants of this study. Their willingness to share their experiences and engage in the group process made this research possible. We hope that this study, made possible by them, will inspire and encourage many future IPV intervention studies that promote healing, empowerment, and hope for young women survivors of violence in Türkiye.
Author Note
This study is a part of the PhD dissertation research conducted by the first author under the supervision of the second author. The primary data have not been published previously nor accepted for publication.
Data Availability
The dataset analyzed during the current study is available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.
Ethics Approval and Informed Consent
The study was carried out in accordance with the Helsinki Declaration. In addition, the study was approved by Yildiz Technical University Scientific Research and Ethical Review Board (Report No. 20221101681). Informed consent was obtained from all the participants.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.