
Abstract
Experience and exposure to Intimate Partner Violence (IPV) are reported worldwide across various age groups. However, little is known about resilience and its associated factors, such as anger management and social integration, among the victims of IPV at universities in low- and middle-income countries, particularly in Tanzania. We employed a cross-sectional design to examine 276 students (41.7% female; MAge range = 22–24 years, SDAge range = .695) randomly chosen from a university in Tanzania. Descriptive results showed a high prevalence of IPV among university students, with over 91% (M = 44.40, SD = 59.546, Range: 1–396) reporting having experienced at least one instance of IPV in the past year. Likewise, students reported a high mean score for resilience and social integration, yet a lower mean score for anger management. Findings of a hierarchical linear regression model revealed a good model fit at step 1 (adj. R2 = .047, F (2, 248) = 7.189, p < .001; Cohen’s f2 = .050) and step 2 (adj. R2 = .055, F (3, 247) = 5.884, p = .002; Cohen’s f2 = .060) with greater social integration and improved anger management both significantly associated with resilience at step 1 and step 2 (p < .05). IPV victimization was not a significant moderator on the association of social integration and anger management with resilience (p > .05). The model-independent variables accounted for 26% of the variability in the association with resilience. Our findings reveal the prevalence of IPV victimization in the understudied population of university students and settings in Tanzania. We recommend a review of existing policies to eradicate IPV within the university community and to familiarize individuals with the available psychosocial support services for IPV victims, thereby protecting them from potential psychological and academic risks of victimization.
Introduction
Intimate partner violence (IPV) refers to any behavior within an intimate relationship that causes physical, psychological, or sexual harm to the individuals involved (Krug et al., 2002). It encompasses physical aggression such as slapping and hitting; psychological abuse involving intimidation and constant belittling; coerced intercourse and other forms of sexual coercion; as well as controlling behaviors such as isolating an individual from their family and friends, monitoring their movements, and restricting their access to information or support (Krug et al., 2002). Reports indicate that young adults (especially those aged between 18 and 24) are more likely to experience higher levels of IPV (Winstok & Straus, 2014), often reported among university students (Spencer et al., 2021) and perpetrated by both male and female students, resulting in consequences for well-being. In the USA, for instance, between 17% and 38% of university students have experienced IPV (Spencer et al., 2021), and 43% of tertiary students in South Africa have experienced some form of IPV (Spencer et al., 2016), while 40% and 30% of Chinese university students reported having perpetrated and been victims of physical IPV, respectively (Kamimura et al., 2016).
Among the risk factors for IPV include cultural norms and approving attitudes toward violence (Nabors & Jasinski, 2009; Straus et al., 2004; Wilson & Smirles, 2022), low collective efficacy in neighborhoods, for example, the low willingness of neighbors to intervene when they see violence (Niolon et al., 2022), childhood experience of violence and exposure to IPV in families (Capaldi et al., 2012; Mulawa et al., 2018), substance use, personality disorder, conduct problems, anger, and hostility (Capaldi et al., 2012, 2022) while age, gender/gender roles, socioeconomic status (Capaldi et al., 2012, 2022; Mulawa et al., 2018) may act as both risk and protective factors. Other protective factors for IPV include anger management (Straus et al., 2010), social integration, spirituality and community cohesion, and ethnic identity (Howell et al., 2018).
Global reports of IPV in college settings show varied findings. For instance, the International Dating Violence Survey indicates that between 4% and 20% of college students have experienced severe forms of violence from a romantic partner (Straus et al., 2004). In the United States, 31% of female students reported experiencing at least one incident of IPV victimization since starting university. (Wood et al., 2020). However, 7.3%, 3.7%, and 19.4% of heterosexual and sexual minority undergraduate students who completed the National College Health Assessment IIb reported being victims of sexual assault, physical assault, and verbal threats, respectively. (Brewer et al., 2018). Once more, a report by Kamimura et al. (2016) indicated that 40% of Chinese college students reported committing physical IPV, whereas 30% reported being victims of it.
In Tanzania, IPV is illegal and a criminal offense under Article 13 of the 1977 constitution, the Law of Marriage Act (LMA), Cap. 29, and Penal Code Cap. 16 (Tanzania Women Lawyers Association, 2014). Despite legal protection, reports indicate that IPV prevails higher, particularly among women (Kapiga et al., 2017; Kinyondo et al., 2021). For instance, about 61% of women reported having ever experienced physical and or sexual IPV in North-western Tanzania (Kapiga et al., 2017). Again, 42% of women reported having experienced physical and/or sexual IPV, as reported from the Tanzania Demographic and Health Survey secondary data (Mahenge & Stöckl, 2021).
Resilience and IPV
Research acknowledges an increasing interest in studying resilience among survivors of violence, including IPV. While there is no agreed definition of resilience, Moeller-Saxone et al. (2015) define it as a dynamic process in which psychological, social, environmental, and biological factors interact to enable individuals at any stage of life to develop, maintain, or regain their mental health despite exposure to adversity. It is also defined as “the maintenance of healthy/successful functioning or adaptation within the context of significant adversity or threat and is better characterized as a dynamic process since individuals can be resilient to specific environmental hazards or resilient at one time but not another”. It is argued that despite the various definitions of resilience, two major components characterize it: (a) exposure to a significant threat, severe adversity, or trauma; (b) the achievement of positive adaptation despite major assaults on the developmental process. In this study, we employ the fundamental definition of resilience to refer to positive adaptation or the ability to maintain or regain mental health despite experiencing adversity (Herrman et al., 2011). This is because we hypothesize that students who are victims of IPV essentially develop positive self-adaptation after the IPV event (referring to any act of IPV experienced by a university student in the past year in this study) for a better self and interaction with others.
Considering that exposure to IPV has multiple effects on an individual, including developed Post-traumatic Stress Disorder (PTSD) symptoms and murder (Spencer et al., 2016), depression symptoms, (Hines & Douglas, 2022), lowered self-esteem, harmful alcohol use, and fatal injuries (World Health Organization, 2013), the victims’ possession of positive psychological adaptation to such an event is necessary. However, understanding what escalates resilience among survivors of IPV is very important. For instance, Tsirigotis and Łuczak (2018) found that the type of perpetrator of IPV determined the level of resilience among women survivors of domestic violence, and Howell et al. (2018) reported that spirituality, higher social support, and fewer violent relationships determined resilience among women survivors of IPV. Among the college students’ sample, particularly in the countries where violence, particularly IPV and violence against children, are considered a norm, no evidence of a study has explored the protective factors of anger management and social integration as associates of resilience among survivors of IPV in college settings.
Anger Management and Resilience
It is reported that the insufficient ability to recognize and manage emotions in general, and anger in particular, among adolescents may frequently result in aggression, bullying, and other disruptive behaviors (Anjanappa et al., 2020). One strategy that can assist an individual in abstaining from engaging in aggressive and disruptive behavior is the ability to manage anger (anger management). While anger management is ideally regarded as a skill-based training outcome, it is undeniably true that individuals, regardless of their exposure to anger management interventions, therapy, or programs, differ in how they respond to anger when faced with emotionally triggering situations, events, or trauma. The assumption underlying the association between anger management and resilience is that an individual endeavoring to cope with a stressful event or trauma may employ various strategies, including anger management. Implicitly, a person with higher anger management skills is more resilient, as supported by Harris et al. (2011). Therefore, understanding the association between anger management and the resilience of victims of IPV in university settings is essential, as most of them are also navigating turbulent and stressful years, as noted by developmental psychologists. (Arnett, 1999).
Social Integration and Resilience
The concept of “social integration” results from the Social Integration Theory. The theory proposes that social ties, such as marriage, family, and friends, can protect individuals from engaging in risky behaviors such as suicide, aggression, and addictive behaviors such as substance abuse, as well as suicidal ideation and harm (Selin & Lind, 2023). Ellison and Anderson (2001) found that lower social integration was linked to a rise in domestic violence. In education, it is also reported that sintegration plays a crucial role in student retention and persistence, with effective integration into appropriate socialization contexts being regarded as a protective factor. (Johnson & Goldman, 2023). This is also linked to social integration arising from the need for relatedness, such as being part of a group (Ryan & Deci, 2000). The sense of integration nurtures positive self-perceptions as a valuable and cherished individual. This protects against engaging in risky behavior, such as violence perpetration, as argued by Selin and Lind (2023). Reports suggest a link between individual social support and resilience in survivors of traumatic events (Mancini & Bonanno, 2009) because of the sense of connectedness in social networks (Davis, 2002). The association between social integration and resilience, particularly among university students who are victims of IPV, is missing in Tanzania. Our argument is that individual students who are victims of IPV and possess higher social integration are more likely to be resilient after the event than those with lower social integration. Thus, examining this association is crucial, given the elevated rates of IPV, particularly GBV, among women in the country. This is because the lack of higher social integration during stressful events may impact the physical and psychological health of the victims, deteriorate their academic performance (Brewer et al., 2018; Brewer & Thomas, 2019), and promote risky behaviors, including IPV perpetration (Selin & Lind, 2023).
The Current Study
Although rates of IPV are said to be high among teenagers and young adults in other regions (Straus et al., 2004), research remains unclear about its prevalence among university students in the Sub-Saharan African context, especially in Tanzania. This is partly due to the social approval of violence, including IPV, which may significantly impact its underreporting. In addition, cultural and societal norms surrounding sexuality and intimate relationships in these contexts may lead university students to refrain from reporting their experiences of IPV to protect their self-image among family members and society. They are raised to view engagement in intimate sexual relationships before marriage and at a younger age as taboo. The lack of scientific data on IPV among this age group limits our understanding of the problem’s magnitude, potential risks, and protective factors for IPV. It also affects their development and well-being, such as academic performance, barriers to leaving a violent relationship, and the coping strategies university students employ when dealing with violent partners. Grasping these components is essential for developing and implementing interventions to safeguard university students from IPV in a country where incidents of violence, particularly gender-based violence, are widely reported and generally receive social approval (Kapiga et al., 2017). Consequently, if IPV among university students is not well understood, it will be challenging to support the victims and assist offenders in overcoming such behaviors while believing they are normal. A lack of understanding regarding the associates of IPV poses a risk to students’ academic and physical well-being and jeopardizes institutions’ efforts to foster a violence-free learning environment.
Hypothesis
a. A high percentage of university students are victims of IPV.
b. Resilience in IPV victims is associated with their anger management and social integration, and the level of IPV victimization moderates the association.
Methods
Design, Sample, and Sampling
We used a cross-sectional research design to inform our objectives. Two hundred seventy-six (276) second and third-year students at a university in Tanzania were selected. The selection of the university was twofold: one, all researchers are based at the college, and two, the college has scientific evidence of psychosocial support services utilization by university college students (reference omitted for review purposes), which again triggered the need to understand how resilient students are when they face health-related challenges including violence by their intimate partners.
We obtained a list of second and third-year students who studied the compulsory Curriculum and Teaching courses in their first and second year of studies from the Faculty of Education examination office. The principal investigator sorted the obtained second and third-year lists based on academic programs offered by the college (i.e., Bachelor of Arts with Education, Bachelor of Science with Education, Bachelor of Education in Arts, and Bachelor of Education in Science). Second-year and third-year students were sorted into their respective programs. In addition, we also reached out to Postgraduate Diploma in Education students during their regular class sessions. Again, we sought a list of students studying for a Bachelor of Arts in Disaster and Risk Management (who do not take the university-wide courses) from the college undergraduate studies office. Having obtained and sorted the list for each program, we further sorted students (except for postgraduate diplomas in education students) based on their sex for representativeness and diversity. From each list, the nth number was specified to select our estimated sample size.
Based on a prior power analysis using G*Power version 3.1 (Verma & Verma, 2020) with an effect size (f2 = .015, p = .05, actual power = .950), a sample size of 138 participants was required to determine the effect of the association of our predictor variables. Considering the dropout rate of 10%–20% and broader representativeness of our students’ sample based on their academic programs, we selected and contacted 400 participants assuming a lower to moderate response rate as the timing of the assessment was close to the end of the first semester, and is characterized with tests, assignments, and preparations for the semester examination.
Participants
The study sample consisted of 276 (41.7% [n = 105] females, with an MAge range of 22 to 24 years and an SDAge range of .695) university college students. Table 1 presents further detailed descriptive demographic characteristics of the study participants.
Population’s Descriptive Demographic Characteristics (N = 276).
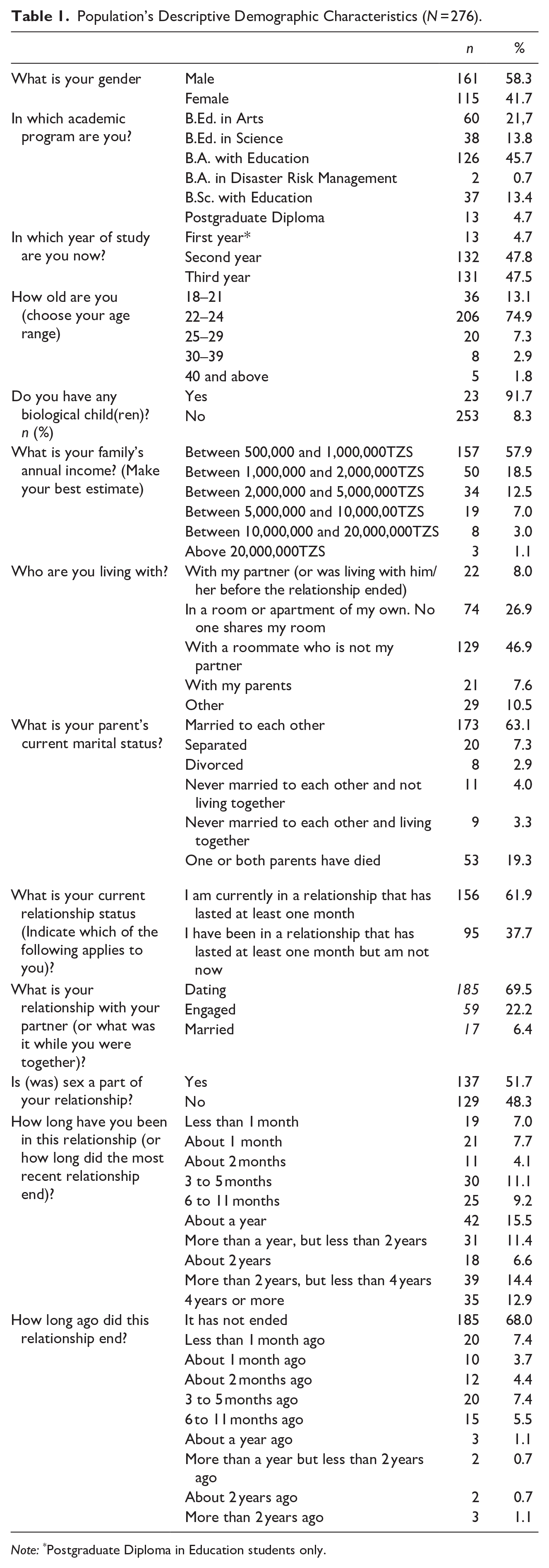
Note: *Postgraduate Diploma in Education students only.
Procedures
The study was conducted from January to February 2024. Having selected the study sample, we recruited two research assistants with experience in research and data assessment to support data assessment. The research team contacted the academic minister of the university student organization, who introduced the research assistants to the representatives of each program offered at the college. Information regarding the project was then shared with the students during their classes and through WhatsApp groups, where a list of all selected students was shared with instructions on how to meet the research team. A total of 276 students (a response rate of 69%) out of 400 appeared for assessment. This was twice the targeted sample size! Before commencing with assessments, the research assistants introduced the project to the participants in a one-on-one session, asked for their written consent to participate in the study, and assured them of confidentiality and anonymity of their data before they were handed a questionnaire to fill out. All 276 participants who appeared for assessments agreed to take part by signing the informed consent form before they were issued with a questionnaire form. Having signed the consent form, participants were handed in a questionnaire to fill in at their convenience. All questions were in English. The average questionnaire return time was between 1 and 2 days. Those who returned the completed filled-in questionnaire were given an appreciation token of 2000TZS (less than 1$) for a drink (water/tea/coffee). The study was conducted per the authors’ university’s ethical approval and research permit.
Measures
Demographic Variables
We assessed participants’ age, sex, partner’s sex, marital status, family income, relationship duration, and academic program using the modified background information presented in Straus et al.’s manual for the personal and relationship profiles (2010).
Intimate Partner Violence
We assessed students’ past years’ experience of IPV using the Relational Behavior Scales of the CTS2 (Straus et al., 1996). The scale consists of 39 items (eight assessing psychological aggression, 12 assessing physical assault, seven assessing sexual coercion, six assessing injuries, and six assessing negotiations) answered with a 7-point point Likert scale format ranging from 0 (Never) to 6 (More than 20 times). For scoring purposes, the answer categories are recorded as 0 = 0, 1 = 1, 2 = 2, 3 = 4, 4 = 8, 5 = 15, 6 = 25, and 7 = 0 (when the experience of violence is beyond the specified time frame) (Straus et al., 1996). The original CTS2 scale has good validity and an internal consistency ranging from .79 to .95 Cronbach’s alpha value. In this study, the 33 items assessing the participants’ reports of experience of violence by their partners were used. The total score can range from 0 to 825, and the scale had an internal consistency of .85 Cronbach’s alpha value in this study.
Resilience
Resilience was assessed using the Ego Resiliency Scale (ER89) (Block & Kremen, 1996), consisting of 14 items. The scale is answered with a 4-point Likert scale ranging from 1 (Strongly disagree) to 4 (Strongly agree). Sample items include “I am generous with my friends” and “I usually think carefully about something before acting.” The total score can range from 14 to 56. The original scale used in a sample of 18 to 23 years olds had an internal consistency of a .76 coefficient. In this study, the scale had an internal consistency of .80 Cronbach’s alpha value.
Anger Management
We assessed anger management using the nine items of the 20-item short form of the Anger Management Scale (Stith & Hamby, 2002) as presented in Straus et al.’s manual for the personal and relationship profile (2010). The scale is answered with a 4-point Likert scale ranging from 1 (Strongly disagree) to 4 (Strongly agree). Sample items include “I can calm myself down when I am upset with my partner” and “Before I let myself get mad at my partner, I think about what will happen if I lose my temper.” Three items (3, 5, and 9) are reverse coded. The total score can range from 9 to 36. The scale had an internal consistency of .70 Cronbach’s alpha value. In this study, the scale had an internal consistency of .48 Cronbach’s alpha value.
Social Integration
We assessed social integration using the 10-item short form of the Social Integration Scale as presented in Straus et al.’s manual for the personal and relationship profile (2010) and appears in Ross and Straus (1997). Answer categories range from 1 (Strongly disagree) to 4 (Strongly agree). Sample items include “I share my thoughts with a family member” and “To get ahead, I have done some things that are not right.” The total score can range from 10 to 40. The internal consistency of the 10-item short-form scale is low at .65 Cronbach’s alpha value. However, Ross and Straus (1997) argue that the validity of the short-form scale remains the same as the full scale. We relied on the established validity of the short-form scale. Again, according to Hair et al. (2003), preliminary studies have considered a low-reliability level acceptable.
Data Analysis
Preliminary analysis using descriptive statistics frequency indicated that 25 (9%) out of 276 students had never experienced violence by their intimate partner in the past year and were excluded from further analysis. Missing values were detected listwise in each of the later analyses. We used the total sum scores of our independent and dependent variables for the bivariate and multivariate analyses. Bivariate correlation analysis using Pearson correlation coefficient (r) was used to test the correlation between the independent variables. The correlation coefficient (r) values of .01, .03, and .05> at p < .05 were considered small, moderate, and high correlations, respectively. Similarly, the effect sizes (Cohen’s d) of 0.2, 0.5, and 0.8 were considered small, moderate, and high effect sizes (Cohen, 1992), respectively. Furthermore, we used an independent sample t-test to test any significant difference between male and female students on the study variables (p > .05). Using hierarchical linear regression analysis, we moderated the association of our model-independent and dependent variables with the moderating variable IPV (IPV*Anger management*Social integration). We tested for possible outliers using the standardized scores of IPV victimization, anger management, social integration, and resilience using a ±3/2 standard deviation. Only IPV victimization had six outliers that we retained in the multivariate models, as IPV is a rare event. All conditions for linear regression, including multicollinearity, were met. The range for multicollinearity, using VIF, was <2. Effect sizes (Cohen’s f2) of 0.02, 0.15, and 0.35 were considered small, middle, and high, respectively (Cohen, 1992).
Results
Descriptive Results
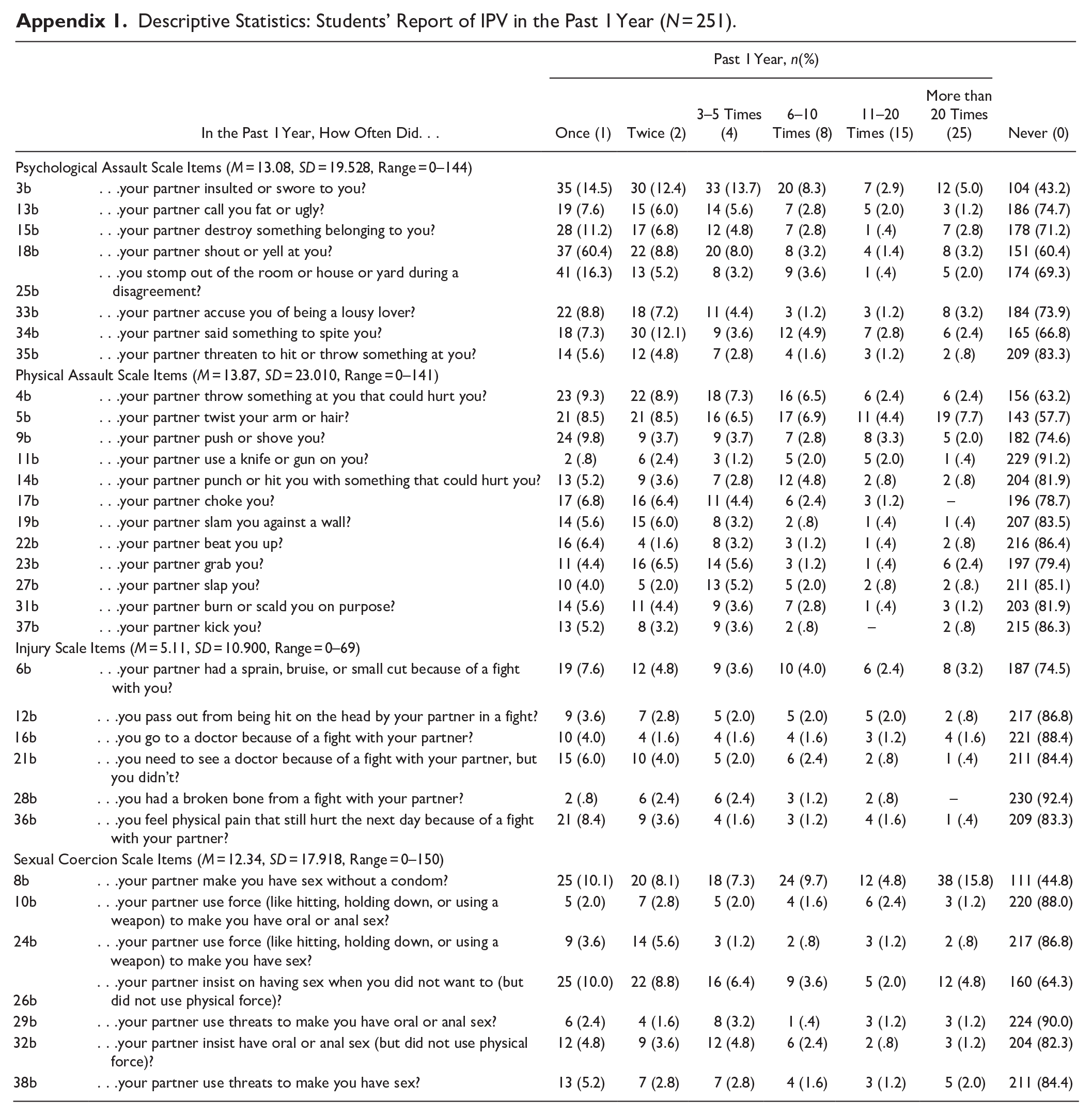
This study included only students with at least one or more reports of acts of IPV in the past year. A total of 251 students (91%; M = 44.40, SD = 59.546, Range: 1–396) out of 276 reported having experienced violence by their intimate partner and were included in further analysis. Descriptive results of students’ scores on each scale item are appended in Appendix 1. A mean score of 41.20, SDresilience = 5.037; range = 20 to 54 was found for resilience, while a mean score of 25.63, SDanger management = 3.605; range = 16 to 57 and 30.43, SDSocial integration = 3.442; range = 21 to 39 were found for anger management and social integration, respectively.
Bivariate Correlation, Independent Sample t-test, and Linear Regression Model Results
Bivariate correlation results indicated a significant correlation between the independent variables: anger management (r = .191, 95% CI: .069 to .307, p = .002) and social integration (r = .189, 95% CI: .067 to .306, p = .003) with resilience. In addition, a significant correlation was found between the independent variables (r = .315, 95% CI: .199 to .422, p < .001). No significant correlation was observed between the moderating variable (IPV) and resilience (p > .05). An independent sample t-test was employed to assess any significant difference between male and female students regarding the study variables. No significant difference (p > .05) was found (see Table 2). The model results in step 1 were significant with a good fit (adj. R2 = .047, F (2, 248) = 7.189, p < .001; Cohen’s f2 = .050), with higher social integration (ß = .143, 95% CI: .015 to .271, p = .029) and improved anger management (ß = .146, 95% CI: .018 to .274, p = .026) significantly associated with resilience. The model-independent variables explained 6% of the variability in the association with resilience. When the moderator variable was entered in step 2, the model fit was significant (adj. R2 = .047, F (3, 247) = 5.080, p = .002; Cohen’s f2 = .060) with higher social integration (β = .146, 95% CI: .018 to .274, p = .026) and more anger management (β = .166, 95 % CI: .031 to .301, p = .016) significantly associated with resilience. IPV experience was not a significant moderator on the association of social integration and anger management with resilience (p > .05). Figure 1 provides the results of the moderating model. The model-independent variables explained 6% of the variability in the association with resilience. We also tested for possible differences in the association between anger management and social integration with students’ resilience based on their sex. Only anger management was significantly associated with female students’ resilience (β = . 226, 95% CI: .021 to .338, p = .027) at step 1 (adj. R2 = .077, F (2, 102) = 5.313, p = .006; Cohen’s f2 = .083), and IPV experience moderated the association of social integration and anger management with resilience (β = . 189, 95% CI: .030 to .392, p = .023) at step 2 (adj. R2 = .049, F (3, 142) = 3.526, p = .018; Cohen’s f2 = .052) in the male’s model. Social integration was not significantly associated with resilience in both the female and male models.
Independent Samples T-test Results of the Study Variables Based on Students’ Sex (N = 251).

IPV = Intimate Partner Violence; CI = Confidence Interval; LL = Lower Limit; UL = Upper Limit.
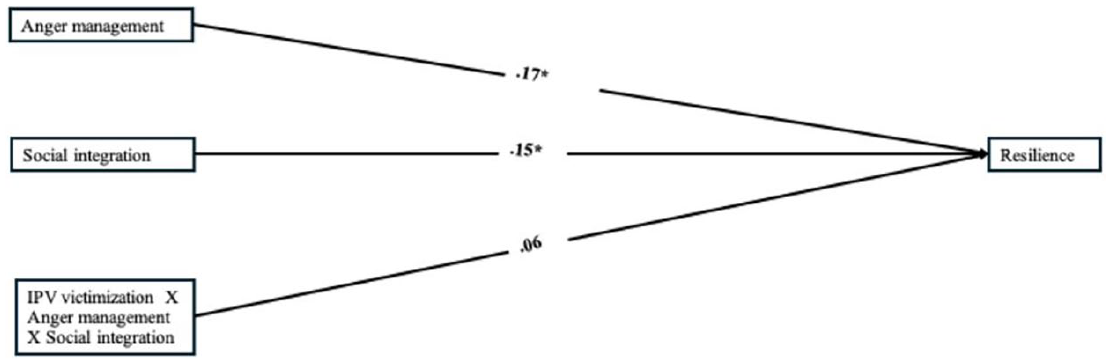
Regression results of the moderating effect of IPV victimization on the association of anger management and social integration with resilience.
Discussion
While associations between violence, including IPV, and resilience have been reported in other studies, this research provides essential evidence regarding the prevalence of IPV, especially among the vulnerable and previously unstudied group of university students. It also explores the relationship between resilience, anger management, and social integration, as well as the moderating effect of IPV experience on these associations within a sample of college students, particularly in lower-income countries such as Tanzania, where IPV is highly prevalent and widely normalized. Our findings confirm the increased prevalence of IPV in the Tanzanian context, as reported in other studies (Kapiga et al., 2017; Kinyondo et al., 2021; Mahenge & Stöckl, 2021). However, no significant differences in IPV were found between female and male students, nor among age groups. Our findings suggest that, regardless of gender and age, university college students in this setting are all at risk of experiencing IPV victimization in various forms. Given the higher prevalence of GBV in the country, university college students, regardless of age or gender, may have learned through modeling or observation of their caregivers, friends, or other community members in response to these elevated prevalence reports and widespread societal approval (Kapiga et al., 2017).
Similarly, our findings showed higher average scores for resilience and social integration among university students who are victims of IPV compared to anger management. However, our findings indicated that anger management and social integration were significantly associated with the resilience of university student victims of IPV. Although the independent and moderating variables of the models demonstrate a smaller effect size, the associations observed can be explained in various ways. First, owing to the elevated prevalence of IPV highlighted in the study and the normalization of violence, especially GBV, within the Tanzanian context (Kapiga et al., 2017; Kinyondo et al., 2021; Mahenge & Stöckl, 2021), Students may have long developed resilience to cope with traumatic, violence-related events through normalization. Second, students in these environments demonstrate positive social integration, as shown in the results, enhancing their resilience when encountering IPV. An individual’s resilience to IPV is likely to depend on their social network, as argued by Selin and Lind (2023). Third, the association between anger management and resilience suggests that unless an individual possesses higher anger management skills, the likelihood of being less resilient in the face of a stressful or traumatic event increases, thereby exacerbating the risk of engaging in risky behaviors such as suicide, feelings of revenge, substance misuse, and PTSD. (Capaldi et al., 2012, 2022), school dropout, and poor academic performance (Brewer et al., 2018; Brewer & Thomas, 2019). In this study, we found that university student victims of IPV had average anger management skills, which may have contributed to their resilience, although the association was minimal (β = .17).
Our study indicated that anger management and social integration may contribute to resilience among university student victims of IPV. However, this can further be tested in longitudinal cause-effect association studies. Anger management was significantly positively associated with female students’ resilience in the aftermath of IPV experience. We attribute this to the fact that in Tanzania, women and girls are at a higher risk of experiencing IPV than men because of power relation norms (Vyas & Jansen, 2018). Men’s aggression toward women is leveraged by societal norms and gender norms, which may exaggerate anger when encountering an IPV risk factor from their partners and lower their resilience. Our findings on anger management and resilience may speak for and intensify the need for gender transformative interventions to engage men in IPV and gender-based violence prevention in Tanzania and other similar settings where societal norms and gender norms promote violence (Lees et al., 2021). In addition, our findings imply that students should be advised of the role of integrating with family, peers, friends, and any other social support systems and sharing their feelings or reporting any signs of violence from their partners. It is through their social integration that they can get support and strategies on how to deal with a violent partner. Utilizing social support services such as spirituality and social support (Howell et al., 2018) is necessary, as religion forms a large part of social life in the country. Again, interventions targeting intimate relationships should form part of the universities’ strategies. Public awareness campaigns on the available university or college psychosocial support services should be made. Equally important is reaching out to the victims’ violent partners. We know that anger is a risk factor that attracts violent acts from partners and that there is a need for the university or college deans of students or directors of student services offices in the country to establish seminar sessions in which safe and healthy relationships will be discussed and strategies such as anger management and social integration will be discussed. Also, universities/colleges should familiarize their community, including students, with their sexual harassment code and the available strategies against a violent partner as stipulated in the policy documents.
Future research should examine the direct and indirect associations between resilience and other related outcome variables of violence, including physical and mental health, as well as academic performance. This is essential as resilience has long been linked to anxiety, a component of mental health that is associated with lower academic performance. Given that over 90% of our study sample reported experiencing IPV victimization and considering that violence is related to mental health issues, it is crucial to connect the outcome variables of violence to design interventions that broadly enhance the physical and psychological health of IPV victims in college settings.
The study reveals violence among a neglected group of college students, who may be at high risk of experiencing IPV due to their age, with the majority being teenagers and likely entering or already involved in their first relationship. Furthermore, it highlights that IPV extends beyond the family setting, where country-specific reports indicate a high prevalence of IPV regarded as normative. Undeniably, these individuals are prospective parents and couples, and their experiences of IPV during college illuminate the next generation of parents. This also signals that much work needs to be done to break the cycle of violence, particularly IPV, at the earliest stages of development. Our findings emphasize the necessity of extending interventions beyond the family context to ensure that both IPV and domestic violence are openly addressed and discouraged from the grassroots level, including in schools, colleges, and universities.
Limitations
One significant challenge of our study is the absence of demographic characteristics and socioeconomic status concerning our sampled students’ partners. For instance, information such as whether their current partners (the referred violent ones) are fellow students (enrolled at the same university or others) would have facilitated a better understanding of the nature of our students’ intimate relationships and what might have driven violence from their perpetrators. This would have offered a stronger foundation for developing interventions to reduce IPV among our university students. Furthermore, while other studies have indicated an association between spirituality and resilience in IPV, particularly among women, we limited our testing for such an association because religious issues have multiple connotations in Tanzania, where Christianity and Islam are the two predominant beliefs. Such findings may ignite debates or provoke violence, particularly as violence, especially IPV, is a critical public health issue. In addition, we recognize that there may be individual differences in IPV experiences based on ethnic groups; Tanzania hosts more than 120 ethnic groups, yet our sample included fewer than half of them. Moreover, the study was conducted at a university in the country’s major economic city, among over 50 universities and colleges. The socioeconomic disparities among university students, based on the geographical location of their institutions, may influence their experiences of IPV and resilience compared to areas where economic pressures are lower. Therefore, it is essential to expand the investigation of IPV experiences, resilience, and associated factors among university students to encompass more universities and colleges, and interpretations of the results should be approached with caution. Lastly, due to the cross-sectional nature of our data, the cause-effect relationships between predictors (anger management and social integration), the moderator (IPV victimization), and the criterion variable (resilience) cannot be generalized for causal direction.
Conclusion
This study investigated the prevalence of IPV among university students in Tanzania. Founded on reports of high prevalence rates of violence against children and gender-based violence in the country, assessing the prevalence of IPV among university students, their resilience toward IPV, and the factors associated with their resilience was important. Our findings indicated a high prevalence of and resilience to IPV in our study sample. Students’ resilience to IPV was associated with their anger management and their social support. Based on this study’s findings, we highlight the urge for universities to possibly review their existing policies to end IPV in their community and, if possible, establish teaching sessions to equip students with skills that will enable them to identify risk and protective factors for IPV such as anger management and ensure that they socially integrate. Again, universities must familiarize students with the available psychosocial support services to support them in coping with IPV.
Footnotes
Appendix
Descriptive Statistics: Students’ Report of IPV in the Past 1 Year (N = 251).
| In the Past 1 Year, How Often Did. . . | Past 1 Year, n(%) | Never (0) | ||||||
|---|---|---|---|---|---|---|---|---|
| Once (1) | Twice (2) | 3–5 Times (4) | 6–10 Times (8) | 11–20 Times (15) | More than 20 Times (25) | |||
| Psychological Assault Scale Items (M = 13.08, SD = 19.528, Range = 0–144) | ||||||||
| 3b | . . .your partner insulted or swore to you? | 35 (14.5) | 30 (12.4) | 33 (13.7) | 20 (8.3) | 7 (2.9) | 12 (5.0) | 104 (43.2) |
| 13b | . . .your partner call you fat or ugly? | 19 (7.6) | 15 (6.0) | 14 (5.6) | 7 (2.8) | 5 (2.0) | 3 (1.2) | 186 (74.7) |
| 15b | . . .your partner destroy something belonging to you? | 28 (11.2) | 17 (6.8) | 12 (4.8) | 7 (2.8) | 1 (.4) | 7 (2.8) | 178 (71.2) |
| 18b | . . .your partner shout or yell at you? | 37 (60.4) | 22 (8.8) | 20 (8.0) | 8 (3.2) | 4 (1.4) | 8 (3.2) | 151 (60.4) |
25b |
. . .you stomp out of the room or house or yard during a disagreement? | 41 (16.3) | 13 (5.2) | 8 (3.2) | 9 (3.6) | 1 (.4) | 5 (2.0) | 174 (69.3) |
| 33b | . . .your partner accuse you of being a lousy lover? | 22 (8.8) | 18 (7.2) | 11 (4.4) | 3 (1.2) | 3 (1.2) | 8 (3.2) | 184 (73.9) |
| 34b | . . .your partner said something to spite you? | 18 (7.3) | 30 (12.1) | 9 (3.6) | 12 (4.9) | 7 (2.8) | 6 (2.4) | 165 (66.8) |
| 35b | . . .your partner threaten to hit or throw something at you? | 14 (5.6) | 12 (4.8) | 7 (2.8) | 4 (1.6) | 3 (1.2) | 2 (.8) | 209 (83.3) |
| Physical Assault Scale Items (M = 13.87, SD = 23.010, Range = 0–141) | ||||||||
| 4b | . . .your partner throw something at you that could hurt you? | 23 (9.3) | 22 (8.9) | 18 (7.3) | 16 (6.5) | 6 (2.4) | 6 (2.4) | 156 (63.2) |
| 5b | . . .your partner twist your arm or hair? | 21 (8.5) | 21 (8.5) | 16 (6.5) | 17 (6.9) | 11 (4.4) | 19 (7.7) | 143 (57.7) |
| 9b | . . .your partner push or shove you? | 24 (9.8) | 9 (3.7) | 9 (3.7) | 7 (2.8) | 8 (3.3) | 5 (2.0) | 182 (74.6) |
| 11b | . . .your partner use a knife or gun on you? | 2 (.8) | 6 (2.4) | 3 (1.2) | 5 (2.0) | 5 (2.0) | 1 (.4) | 229 (91.2) |
| 14b | . . .your partner punch or hit you with something that could hurt you? | 13 (5.2) | 9 (3.6) | 7 (2.8) | 12 (4.8) | 2 (.8) | 2 (.8) | 204 (81.9) |
| 17b | . . .your partner choke you? | 17 (6.8) | 16 (6.4) | 11 (4.4) | 6 (2.4) | 3 (1.2) | – | 196 (78.7) |
| 19b | . . .your partner slam you against a wall? | 14 (5.6) | 15 (6.0) | 8 (3.2) | 2 (.8) | 1 (.4) | 1 (.4) | 207 (83.5) |
| 22b | . . .your partner beat you up? | 16 (6.4) | 4 (1.6) | 8 (3.2) | 3 (1.2) | 1 (.4) | 2 (.8) | 216 (86.4) |
| 23b | . . .your partner grab you? | 11 (4.4) | 16 (6.5) | 14 (5.6) | 3 (1.2) | 1 (.4) | 6 (2.4) | 197 (79.4) |
| 27b | . . .your partner slap you? | 10 (4.0) | 5 (2.0) | 13 (5.2) | 5 (2.0) | 2 (.8) | 2 (.8.) | 211 (85.1) |
| 31b | . . .your partner burn or scald you on purpose? | 14 (5.6) | 11 (4.4) | 9 (3.6) | 7 (2.8) | 1 (.4) | 3 (1.2) | 203 (81.9) |
| 37b | . . .your partner kick you? | 13 (5.2) | 8 (3.2) | 9 (3.6) | 2 (.8) | – | 2 (.8) | 215 (86.3) |
| Injury Scale Items (M = 5.11, SD = 10.900, Range = 0–69) | ||||||||
| 6b | . . .your partner had a sprain, bruise, or small cut because of a fight with you? | 19 (7.6) | 12 (4.8) | 9 (3.6) | 10 (4.0) | 6 (2.4) | 8 (3.2) | 187 (74.5) |
| 12b | . . .you pass out from being hit on the head by your partner in a fight? | 9 (3.6) | 7 (2.8) | 5 (2.0) | 5 (2.0) | 5 (2.0) | 2 (.8) | 217 (86.8) |
| 16b | . . .you go to a doctor because of a fight with your partner? | 10 (4.0) | 4 (1.6) | 4 (1.6) | 4 (1.6) | 3 (1.2) | 4 (1.6) | 221 (88.4) |
| 21b | . . .you need to see a doctor because of a fight with your partner, but you didn’t? | 15 (6.0) | 10 (4.0) | 5 (2.0) | 6 (2.4) | 2 (.8) | 1 (.4) | 211 (84.4) |
| 28b | . . .you had a broken bone from a fight with your partner? | 2 (.8) | 6 (2.4) | 6 (2.4) | 3 (1.2) | 2 (.8) | – | 230 (92.4) |
| 36b | . . .you feel physical pain that still hurt the next day because of a fight with your partner? | 21 (8.4) | 9 (3.6) | 4 (1.6) | 3 (1.2) | 4 (1.6) | 1 (.4) | 209 (83.3) |
| Sexual Coercion Scale Items (M = 12.34, SD = 17.918, Range = 0–150) | ||||||||
| 8b | . . .your partner make you have sex without a condom? | 25 (10.1) | 20 (8.1) | 18 (7.3) | 24 (9.7) | 12 (4.8) | 38 (15.8) | 111 (44.8) |
| 10b | . . .your partner use force (like hitting, holding down, or using a weapon) to make you have oral or anal sex? | 5 (2.0) | 7 (2.8) | 5 (2.0) | 4 (1.6) | 6 (2.4) | 3 (1.2) | 220 (88.0) |
| 24b | . . .your partner use force (like hitting, holding down, or using a weapon) to make you have sex? | 9 (3.6) | 14 (5.6) | 3 (1.2) | 2 (.8) | 3 (1.2) | 2 (.8) | 217 (86.8) |
26b |
. . .your partner insist on having sex when you did not want to (but did not use physical force)? | 25 (10.0) | 22 (8.8) | 16 (6.4) | 9 (3.6) | 5 (2.0) | 12 (4.8) | 160 (64.3) |
| 29b | . . .your partner use threats to make you have oral or anal sex? | 6 (2.4) | 4 (1.6) | 8 (3.2) | 1 (.4) | 3 (1.2) | 3 (1.2) | 224 (90.0) |
| 32b | . . .your partner insist have oral or anal sex (but did not use physical force)? | 12 (4.8) | 9 (3.6) | 12 (4.8) | 6 (2.4) | 2 (.8) | 3 (1.2) | 204 (82.3) |
| 38b | . . .your partner use threats to make you have sex? | 13 (5.2) | 7 (2.8) | 7 (2.8) | 4 (1.6) | 3 (1.2) | 5 (2.0) | 211 (84.4) |
Acknowledgements
We acknowledge the two research assistants, Thomas Masatu Nyasaira and Godfrey Mushi, and Dorothea Clement for their dedication to the success of our study. Thank you to all the participating students.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for this article’s research and/or authorship.