
Abstract
Suicide rates have increased notably in Spain, particularly among the migrant population, where mortality by suicide rose by 25% between 2018 and 2021. Migrants are exposed to cumulative stressors, including socioeconomic adversity, acculturative challenges, and adverse childhood experiences (ACEs) that may heighten the risk of suicidal behavior. This study aimed to examine and compare the risk factors associated with suicide attempts among foreign-born and native-born individuals in Spain, with particular emphasis on the role of ACEs. A sample of 754 patients assessed 15 days after a suicide attempt (73.1% female; M = 40.23, SD = 15.72) from the SURVIVE study was used. Sociodemographic, clinical, and psychological variables, including ACEs, were measured using validated instruments. Group comparisons and multigroup regression analyses were conducted to explore factors associated with suicidal outcomes based on migration status. Foreign-born patients were significantly younger and more likely to report emotional abuse, physical abuse, sexual abuse, and physical neglect during childhood than native-born individuals. They also exhibited higher psychological distress and greater acquired capability for suicide. In multivariate models, different predictors of suicidal ideation and behavior emerged across groups. In multivariate models, different predictors of suicidal ideation and behavior emerged across groups. For native-born individuals, suicidal ideation intensity was associated with greater psychopathology severity, more diagnosed mental disorders, higher acquired capability, and a history of suicide attempts. For migrants, higher acquired capability, lower impulsivity, and a history of suicide attempts were associated with greater ideation intensity. Migrant populations in Spain demonstrate a different profile of suicide risk, marked by increased ACEs and psychological burden. These findings highlight the need for culturally sensitive suicide prevention strategies that incorporate early trauma screening and address structural vulnerabilities. Prevention protocols should prioritize trauma-informed care and social integration to mitigate suicide risk in this vulnerable population.
Introduction
In 2023, 4,116 people died by suicide in Spain, making suicide the leading cause of non-natural death, surpassing traffic accidents (Instituto Nacional de Estadística [INE], 2024). Spain has historically maintained one of the lowest suicide mortality rates among European Union and other high-income countries (Organization for Economic Co-operation and Development, 2023). However, a concerning upward trend has emerged in recent years. Although this figure reflects a slight decrease compared to 2022 (4,227 deaths), the cumulative increase since the prepandemic years remains notable. The national suicide rate rose from 7.58 deaths per 100,000 inhabitants in 2018 to 8.80 in 2022, an increase of over 16% in just 4 years (INE, 2024). This rise is especially concerning among vulnerable populations such as migrants (de la Torre-Luque et al., 2024; López-Cuadrado et al., 2022).
In 2023, more than 720,000 individuals migrated to Spain, contributing to a foreign-born population exceeding 8.7 million people (INE, 2024). Of the suicide deaths registered in 2022, 455 involved individuals of foreign origin (9.29%), representing a 25% increase compared to 2018 (de la Torre-Luque et al., 2024). These figures point to a growing mental health crisis among migrant communities, who are often exposed to a wide range of cumulative psychosocial stressors. In the Spanish context, migrant populations are highly heterogeneous and include economic migrants, asylum seekers, refugees, and individuals undergoing family reunification. Most originate from Latin America, North Africa, and Eastern Europe, with each group facing specific structural vulnerabilities and psychosocial challenges (Aran et al., 2023; INE, 2024). This diversity underscores the importance of disaggregating data and avoiding overgeneralizations when examining mental health risks in migrant populations.
While migration is often motivated by aspirations for safety, education, or economic improvement, it frequently involves a complex constellation of adversities legal insecurity, job precariousness, social exclusion, discrimination, acculturative stress, loss of support networks, and limited access to healthcare services (Aran et al., 2023; Forte et al., 2018; Henkelmann et al., 2020; Kosidou et al., 2012; Pasch et al., 2006; Lai et al., 2017). These migration-related stressors intersect with established suicide risk factors, such as hopelessness, unemployment, and social isolation, which were exacerbated during the COVID-19 pandemic (Amiri, 2020; World Health Organization, 2023). Suicide attempts, recognized as the strongest predictor of completed suicide, are significantly more prevalent among migrants than among native-born individuals (Hollander et al., 2020; López-Cuadrado et al., 2022). In Spain, recent data indicate that the rate of suicide attempts among migrants is approximately 1.5 times higher than in the native population (López-Cuadrado et al., 2022), a disparity that may be partially explained by migrants’ disproportionate exposure to traumatic events, including forced displacement, violence, and abuse, both prior to and during the migratory process (Henkelmann et al., 2020; Peña et al., 2008). A recent meta-analysis by Henkelmann et al. (2020) identified poor working conditions, language barriers, and lack of social support as key predictors of mental disorders among migrants, including depression, posttraumatic stress disorder, and suicidal ideation. These findings highlight the need to consider trauma exposure as a central, differential risk factor in suicide prevention strategies targeting migrant populations.
One critical factor underlying the increased vulnerability of migrants is their disproportionate exposure to early-life trauma. Adverse childhood experiences (ACEs), and particularly child maltreatment (including emotional, physical, and sexual abuse, as well as emotional and physical neglect), are consistently associated with elevated risks of mental illness and suicidal behavior (Angelakis et al., 2020; Danese & McEwen, 2012; Felitti et al., 1998; Sami & Hallaq, 2018; Zatti et al., 2017). A meta-analysis of 23 longitudinal studies revealed that ACEs triple the likelihood of developing mental disorders in adulthood, highlighting the relevance of parental loss, emotional abuse, and neglect in this process (McKay et al., 2021). Psychiatric comorbidity further amplifies suicide risk: the co-occurrence of two or more disorders can increase risk by 3 to 10 times (Gili et al., 2019; Too et al., 2019).
In addition to their impact on psychopathology, early experiences of maltreatment can shape enduring psychological traits such as impulsivity and pain desensitization, both of which are implicated in suicide risk (Joiner, 2005; Ribeiro et al., 2014; Termorshuizen et al., 2012). A recent meta-analysis has demonstrated that impulsivity functions as a mediator between childhood maltreatment and suicidal behavior, suggesting that exposure to early traumatic experiences disrupts normative neurobiological, cognitive, and affective development. This, in turn, may lead to increased impulsivity, which is associated with a greater risk of suicidal behavior (Pérez-Balaguer et al., 2022). Furthermore, according to the Interpersonal Theory of Suicide, childhood maltreatment may contribute to suicide risk by increasing thwarted belongingness, heightened perceived burdensomeness, and greater acquired capability for suicide (Ratkowska & De Leo, 2013). These three constructs jointly elevate the risk of engaging in lethal or near-lethal suicidal behavior (Joiner, 2005; Van Orden et al., 2010). However, empirical evidence for these mechanisms remains heterogeneous, partly due to differences in how suicidal ideation and behaviors are conceptualized and measured across studies (Allbaugh et al., 2017; Schönfelder et al., 2021; Serebriakova et al., 2025). Nevertheless, there is robust evidence that ACEs are associated with an earlier age of first suicide attempt, even after controlling for psychiatric diagnoses, suggesting that maltreatment may directly increase suicide vulnerability (Hoertel et al., 2015). These experiences may promote greater pain tolerance and contribute to lethal capability for suicide (Smith & Cukrowicz, 2010), further elevating risk, especially in the context of impulsivity and unresolved trauma.
Despite the well-established relevance of these factors, few studies in Spain have examined how ACEs, socioeconomic stressors, psychiatric diagnoses, and psychological traits interact to influence suicidal behavior and whether these patterns differ between native-born and migrant populations. Understanding these interactions is critical for designing culturally sensitive and evidence-based prevention and intervention strategies tailored to the needs of these vulnerable groups. The aim of our work is to analyze the risk factors of the migrant population in Spain compared to the native population. Moreover, it intended to analyze the relationship between risk factors and suicide outcomes according to migration status.
Methods
Participants
A sample of 754 adults (73.1% females; M = 40.23 years, SD = 15.72) from the “Suicide Prevention and Intervention Study (SURVIVE)” (Pérez et al., 2023) was used. All patients were recruited from the psychiatric emergency department of seven public, general, and university hospitals throughout Spain (Universidad Complutense de Madrid, Hospital Clínic; Corporació Sanitària Parc Taulí; Parc de Salut Mar, Hospital Clínico San Carlos; Hospital Universitario La Paz, Hospital Universitario Araba-Santiago, Hospital Universitario Virgen del Rocio, and Hospital Universitario Central de Asturias). As inclusion criteria, patients should have been admitted to an emergency department due to a suicide attempt. Assessments were conducted approximately 15 days after hospital admission to ensure clinical stabilization and enable reliable participation in the baseline evaluation, in accordance with the SURVIVE protocol, which specifies baseline assessments within 10 days of the suicide attempt once informed consent is feasible. All patients had to be able to understand the study procedures and sign an informed consent form. Exclusion criteria were (1) being in a state of low level of consciousness; (2) inability to give informed consent, (3) lack of fluency in Spanish, and (4) participation in another suicide prevention study or psychotherapy.
The study was conducted in accordance with the Declaration of Helsinki (World Medical Association, 2013) and following the principles of good practice. All the protocols of this study were approved by a human research ethics committee at each of the recruiting centers.
Measures
An ad hoc interview was conducted to collect sociodemographic data, including sex, age, migration status (born in Spain or abroad), educational attainment (i.e. primary or none, secondary, and tertiary), marital status (i.e. partnered or married and unpaired), and employment status (i.e. non-active or active). In the case of inactive individuals, it was recorded whether they were receiving any type of pension.
The Mini International Neuropsychiatric Interview (MINI; Ferrando et al., 2016) was administered to assess the presence of current psychiatric disorders based on DSM-5 diagnostic criteria (American Psychiatric Association, 2013). The MINI is a structured diagnostic interview with demonstrated reliability and validity for clinical and research use in psychiatric populations.
Self-perceived health was evaluated using the EuroQol Visual Analog Scale (EQ-VAS) from the EQ-5D-5L version. This vertical visual analog scale ranges from 0 (The worst health you can imagine) to 100 (The best health you can imagine) (Balestroni & Bertolotti, 2012). The EQ-VAS has been widely validated as a measure of general health perception and has shown good test–retest reliability.
Suicidal ideation and behavior were assessed using the Columbia-Suicide Severity Rating Scale (C-SSRS; Posner et al., 2008), validated in Spanish by Al-Halabí et al. (2016). This clinician-administered scale evaluates the presence, severity, and intensity of suicidal ideation, as well as suicidal behavior. The C-SSRS has demonstrated strong inter-rater reliability and predictive validity for suicide-related outcomes. To assess acquired capability for suicide, the Acquired Capability for Suicide Scale, Fearlessness about Death (ACSS-FAD; Ribeiro et al., 2014) was used. This 7-item self-report questionnaire is rated on a 5-point Likert scale from 0 (Not at all like me) to 4 (Very much like me). The ACSS-FAD has demonstrated good internal consistency (Cronbach’s α = .73 in our sample) and construct validity.
Depressive symptoms were evaluated using the Patient Health Questionnaire-9 (PHQ-9) (Kroenke & Spitzer, 2002), which measures the frequency of depressive symptoms over the previous 2 weeks on a scale from 0 (Not at all) to 3 (Nearly every day). The PHQ-9 has excellent internal consistency (Cronbach’s α = .84 in our sample) and convergent validity with clinician diagnoses. Anxiety symptoms were assessed with the Generalized Anxiety Disorder-7 (GAD-7; Spitzer et al., 2006), a 7-item scale rated similarly to the PHQ-9. The GAD-7 has demonstrated high internal consistency (α = .85 in our sample) and good diagnostic validity.
Impulsivity was measured using the Barratt Impulsiveness Scale-11 (BIS-11; Patton et al., 1995), a 30-item self-report questionnaire with demonstrated internal consistency (α = .84 in our sample) and factorial validity. In this study, the total score was used, with higher scores indicating greater impulsivity.
Psychological distress was evaluated through the Brief Symptom Inventory (BSI; Derogatis & Melisaratos, 1983; Ruipérez et al., 2001). The BSI provides three indices: Global Severity Index (GSI), Positive Symptom Distress Index, and Positive Symptom Total (PST). It is a widely used screening tool with strong psychometric properties, including high internal consistency and factorial validity. In our sample, the Cronbach’s alpha was .96.
ACEs were assessed using the Childhood Trauma Questionnaire—Short Form (CTQ-SF) (Bernstein & Fink, 1998), validated in Spanish by Hernandez et al. (2013). This 28-item self-report instrument evaluates five types of maltreatment: emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect. The CTQ-SF has demonstrated excellent internal consistency (Cronbach’s α ranging from .79 to .94 across subscales) and good test–retest reliability. In the present study, the total score (sum of the five subscales) was used.
Data Analysis
All variables (including individual scores on demographic, clinical, and measures of suicidal behavior and childhood trauma) were compared between native and immigrant patients using the χ2 test for categorical variables and t tests for continuous variables. The Fisher’s exact correction of null hypothesis rejection probability (p value) was applied when the expected cell count was less than 5. Cramer’s V statistic (for categorical variables) and Hedges’ g (for continuous measures) were used as effect size estimates. Multigroup multivariate regression was used to study the relationship between the sociodemographic (sex, age, years living in the city, employment status, and pension benefits) and clinical risk factors (number of diagnosed mental disorders, antidepressant prescription, severity of psychopathology symptoms, impulsivity, acquired capability for suicide, history of traumatic experiences, number of previous attempts, and the presence of non-suicidal self-injury) and suicide outcomes (i.e., C-SSRS ideation intensity, number of suicide behaviors, medical damage derived from the index attempt), according to patient origin. Nationality (native- vs foreign-born patients) was used as a multigroup (mediating) factor. Multigroup regression allows for estimating group-specific relationship coefficients using the same structural model of relationships. The B coefficient was used as a relationship estimate. The diagonally weighted least squares estimation method was used due to outcome violations in terms of normality. The adjusted R squared (R2adj) was used to account for group-specific explained variance of each outcome. All the analyses were conducted using the R software (package lavaan, broom, and effsize).
Results
Of all the participants, a total of 754 patients (73.1% female; M = 40.23 years, SD = 15.72) were finally analyzed because the remaining participants did not complete the CTQ-SF questionnaire. Table 1 shows the results of the comparison of clinical and sociodemographic variables and outcomes related to suicidal behavior and ACEs between native-born and foreign-born patients. Almost three-quarters of patients were native-born (74.5%). Most foreign-born patients came from Latin American countries (74%), followed by those coming from European countries (16.6%), African countries (5.2%), Asian countries (3.1%), and Oceanian countries (1%). Most foreign-born patients had Spanish as a mother tongue (77.6%). In terms of mobility, 44.8% of native-born patients reported having moved from another city. Mean years living in the city were significantly higher for native-born patients (M = 40.37, SD = 16.82) in comparison to foreign-born patients (M = 18.09, SD = 5.41), t (633.57) = 15.81, g = 1.51.
Demographics, Clinical Variables, and Measures of Suicidal Behavior and Childhood Trauma of Native and Foreign-Born Patients.
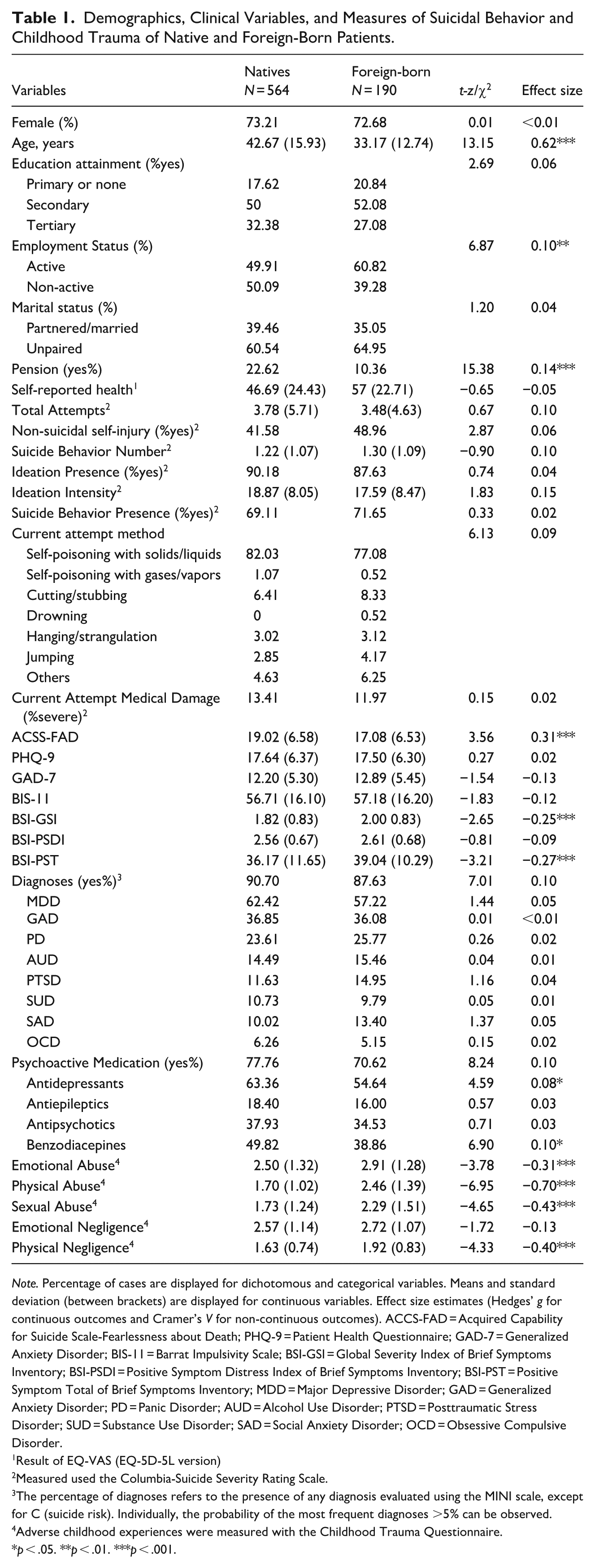
Note. Percentage of cases are displayed for dichotomous and categorical variables. Means and standard deviation (between brackets) are displayed for continuous variables. Effect size estimates (Hedges’ g for continuous outcomes and Cramer’s V for non-continuous outcomes). ACCS-FAD = Acquired Capability for Suicide Scale-Fearlessness about Death; PHQ-9 = Patient Health Questionnaire; GAD-7 = Generalized Anxiety Disorder; BIS-11 = Barrat Impulsivity Scale; BSI-GSI = Global Severity Index of Brief Symptoms Inventory; BSI-PSDI = Positive Symptom Distress Index of Brief Symptoms Inventory; BSI-PST = Positive Symptom Total of Brief Symptoms Inventory; MDD = Major Depressive Disorder; GAD = Generalized Anxiety Disorder; PD = Panic Disorder; AUD = Alcohol Use Disorder; PTSD = Posttraumatic Stress Disorder; SUD = Substance Use Disorder; SAD = Social Anxiety Disorder; OCD = Obsessive Compulsive Disorder.
Result of EQ-VAS (EQ-5D-5L version)
Measured used the Columbia-Suicide Severity Rating Scale.
The percentage of diagnoses refers to the presence of any diagnosis evaluated using the MINI scale, except for C (suicide risk). Individually, the probability of the most frequent diagnoses >5% can be observed.
Adverse childhood experiences were measured with the Childhood Trauma Questionnaire.
p < .05. **p < .01. ***p < .001.
Significant differences were observed between native and foreign-born Spanish regarding age and employment status. Native patients were significantly older than foreign-born individuals (t = 13.15, p < .001), and a higher percentage were unemployed (χ2 = 6.87, p < .01). Furthermore, among patients who were not currently working, foreign-born individuals were less likely to receive pension benefits. Regarding attitudes toward suicide-related death, native patients showed significantly higher scores on the ACSS-FAD (t = 3.56, p < .001), indicating lower levels of fear associated with dying by suicide. Conversely, foreign-born patients reported a significantly greater number of psychological symptoms as measured by BSI-PST (t = −3.21, p < .001) and showed higher levels of global psychological distress on the BSI-GSI (t = −2.65, p < .001). No significant differences were obtained in the variables related to suicidal behavior, depressive symptomatology, anxious symptomatology, and impulsivity. In relation to ACEs, foreign-born patients reported significantly more trauma exposure in several dimensions of the CTQ. Specifically, they scored higher in emotional abuse (t = −3.78; p = <.01; g = −0.31), physical abuse (t = −6.95; p =< .01; g = −0.70), sexual abuse (t = −4.65; p =< .01; g = −0.43) and physical neglect (t = −4.33; p =< .01; g = −0.40).
Regarding the relationship between the suicide risk factors and suicide-related outcomes, the multigroup regression models revealed satisfactory levels of explained variance across outcomes and groups (R2adj ≥ .17), except on the medical damage outcome for native-born patients (see Table 2). In terms of suicidal ideation intensity, risk factors significantly associated with the outcome for the native-born patients were: the number of diagnosed mental disorders (B = 0.39, p < .01), the severity of psychopathology symptoms (B = 1.85, p < .01), acquired capability for suicide (B = 0.11, p < .01) and the history of previous attempts (B = 0.08, p < .01). Thus, higher ideation intensity was associated with higher number of diagnosed mental conditions, psychopathology symptoms, acquired capability and more previous suicide attempts. In contrast, higher ideation intensity was associated in foreign-born patients with being female (B = −1.21, p < .05), lower impulsivity (B = −0.07, p < .05), higher acquired capability (B = 0.14, p < .01) and more previous suicide attempts (B = 0.37, p < .01). Regarding the number of suicide behaviors for the native-born patients (Table 2), the lack of necessity of receiving pension benefits (B = −0.13, p < .05), the number of diagnosed mental disorders (B = 0.11, p < .01), the severity of psychopathology symptoms (B = 0.28, p < .01), lower impulsivity (B = −0.01, p < .05) and the presence of non-suicidal self-injury (B = 0.33, p < .01), was associated with higher ideation intensity. Only the history of previous suicide attempts was associated with more suicide behaviors in foreign-born patients (B = 0.09, p < .01). Finally, two risk factors were associated with higher medical damage of the index suicide attempt in native-born patients: lower levels of psychopathology symptom severity (B = −0.27, p < .05) and more previous suicide attempts (B = 0.02, p < .05). Being younger (B = −0.88, p < .01) and more years living in the current city of residence (B = 0.89, p < .01) were associated with the medical damage of the index attempt in foreign-born patients.
Suicide Outcomes and Related Risk Factors According to Nationality.
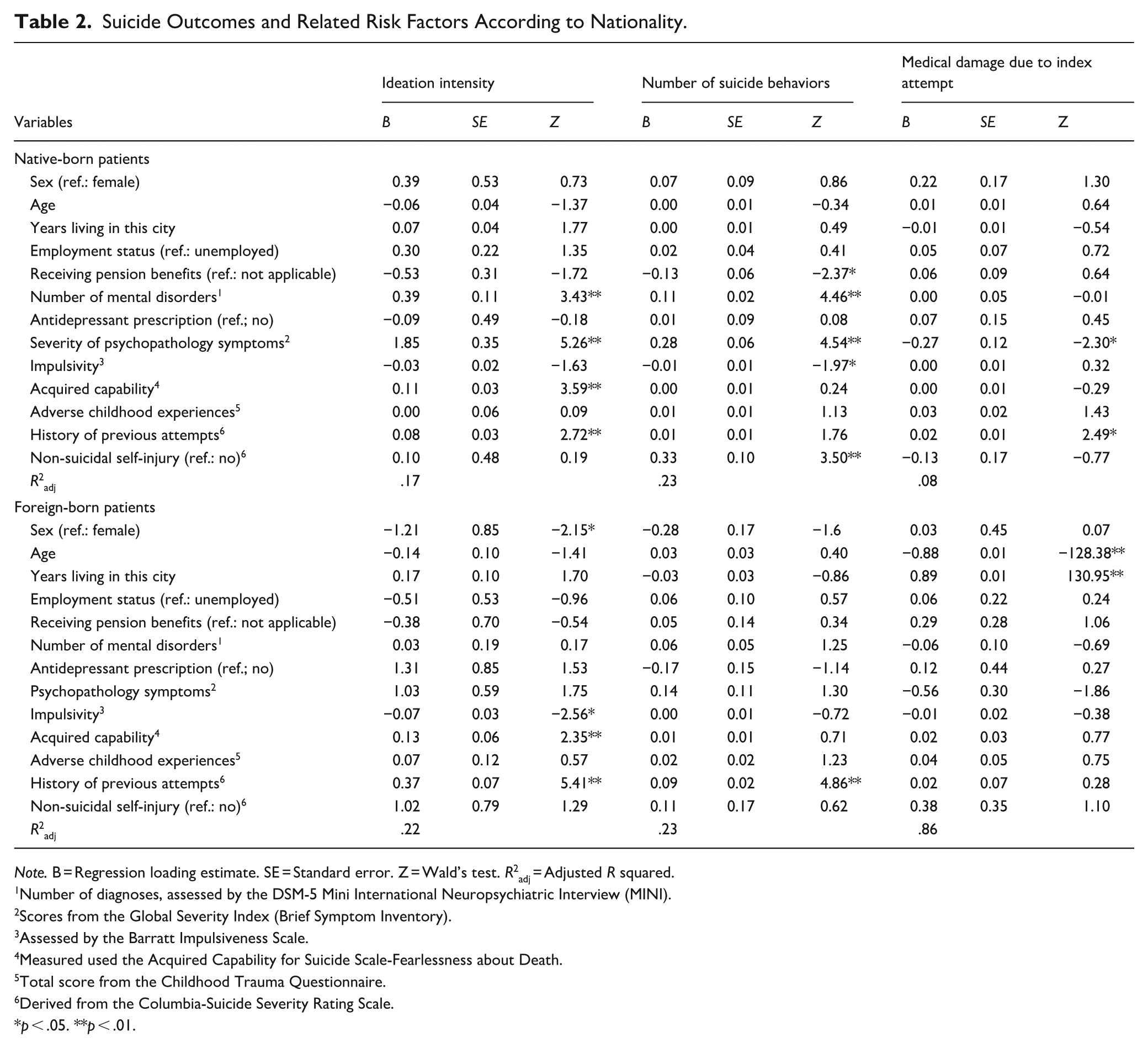
Note. B = Regression loading estimate. SE = Standard error. Z = Wald’s test. R2adj = Adjusted R squared.
Number of diagnoses, assessed by the DSM-5 Mini International Neuropsychiatric Interview (MINI).
Scores from the Global Severity Index (Brief Symptom Inventory).
Assessed by the Barratt Impulsiveness Scale.
Measured used the Acquired Capability for Suicide Scale-Fearlessness about Death.
Total score from the Childhood Trauma Questionnaire.
Derived from the Columbia-Suicide Severity Rating Scale.
p < .05. **p < .01.
Discussion
The present study aimed to examine the risk factors associated with suicide attempts in the immigrant population compared to the native population in Spain, with a specific focus on the impact of ACEs. The analysis utilized sociodemographic, clinical, suicidal behavior, and childhood trauma data to identify significant differences between these two groups and to underscore the role of childhood traumatic experiences as a pivotal risk factor for suicidal behavior. Our study is the first to report notable differences between native-born and foreign-born individuals who had attempted suicide in Spain. These differences were observed in key variables, including age, employment status, receipt of economic benefits, and psychological distress, specifically in the BSI-GSI and BSI-PST subscales. Moreover, significant disparities were found in childhood trauma, particularly emotional, physical, and sexual abuse, as well as physical neglect.
Importantly, 68.4% of the foreign-born participants in our sample reported experiencing more than one type of childhood maltreatment, compared to 51.9% of native-born individuals. This supports previous evidence that maltreatment tends to occur cumulatively rather than in isolation, amplifying the risk of adverse outcomes (Dong et al., 2004). The elevated levels of psychological distress among foreign-born individuals, reflected in higher BSI scores, suggest a compounded mental health burden. Contributing factors may include trauma exposure, acculturative stress, and economic precarity. Although more foreign-born participants reported being employed, they were significantly less likely to receive pension benefits, indicating greater engagement in informal or temporary labor markets. This aligns with research linking precarious employment to increased risk of depression, anxiety, and suicidality (Ornek et al., 2022). While our results reaffirm prior findings on the association between childhood maltreatment and suicidal behavior (Hughes et al., 2017; Zatti et al., 2017), some findings warrant further reflection. Despite higher trauma exposure, there were no significant differences between native and foreign-born participants regarding current suicidal behavior (ideation, plans, or attempts), suggesting possible protective cultural or community factors moderating this relationship. In addition, we found a negative association between the severity of psychopathological symptoms and suicide attempts. This counterintuitive result may reflect the cross-sectional nature of our design, variations in symptom reporting, or potential underreporting due to stigma in migrant groups (Lindert et al., 2009). Future longitudinal research is needed to clarify these dynamics.
Another critical factor potentially influencing suicidal behavior among migrants, especially recent arrivals, is limited access to healthcare services. Structural barriers such as administrative obstacles, lack of health insurance, and unclear legal status can restrict migrants’ ability to seek timely mental health support (Priebe et al., 2016; Satinsky et al., 2019). Linguistic and cultural differences, as well as a lack of culturally competent care, further reduce help-seeking behavior (Forte et al., 2018). Moreover, recent migrants may be unaware of their rights to healthcare access in Spain or fear that seeking care could negatively affect their immigration status. These barriers may contribute to underdiagnosis of psychiatric conditions and delayed intervention, heightening the risk of suicidal crises (World Health Organization, 2019). Stigma related to mental health and cultural interpretations of psychological suffering also play a role in discouraging treatment-seeking behaviors (Priebe et al., 2016). Integrating this dimension into suicide prevention efforts is crucial to ensuring that migrant populations, especially those in the early phases of resettlement, receive adequate support.
Regarding acquired capability for suicide, foreign-born participants scored significantly higher on the ACSS-FAD. Although this may indicate desensitization to pain due to repeated trauma exposure, recent studies have questioned the scale’s predictive validity for suicide attempts (Smith & Cukrowicz, 2010). It is therefore crucial to interpret these findings with caution and in context with other psychological and behavioral indicators. The consequences of childhood maltreatment also extend to relational domains. Loss of primary social ties due to migration, combined with pre-existing insecure attachment patterns, may exacerbate feelings of isolation and disconnection in host societies, recognized risk factors for suicide (Goldsmith et al., 2014; Kim et al., 2022). In addition, intergenerational acculturation conflicts may further strain familial bonds and mental well-being, particularly among adolescents and young adults (Bursztein Lipsicas & Henrik Mäkinen, 2010; Suárez-Orozco et al., 2018).
Another relevant issue is the nature of trauma captured in our study. The CTQ-SF measures maltreatment within the family context but does not include broader adversity such as war, displacement, or political violence. These forms of trauma, prevalent among many migrants, have unique psychological sequelae and differential associations with suicidality (Conway & Lewin, 2022; Ertanir et al., 2023). Thus, our findings may underestimate the full scope of adverse experiences in the foreign-born group. In this regard, we have adopted the term child maltreatment throughout the manuscript, as it more accurately reflects the specific types of abuse and neglect measured by the CTQ-SF, distinguishing them from broader conceptualizations of “childhood trauma.” Moreover, it is important to note that the composition of the foreign-born sample was predominantly Latin American (74%), with limited representation from other key migrant populations in Spain, such as individuals from North Africa, particularly Morocco. This underrepresentation restricts the generalizability of our findings across all migrant subgroups and highlights the need for future research that includes more diverse cultural and regional backgrounds. Cultural stigma and varying attitudes toward mental health care across different migrant communities may influence both help-seeking behaviors and mental health outcomes. For instance, research has shown that migrants from North African countries, particularly Moroccan communities in Europe, often face higher levels of stigma toward mental illness and are less likely to seek professional psychological support compared to Latin American migrants (Belhadj Kouider et al., 2014). These differences may result in underutilization of services and underreporting of mental health needs in certain subgroups. Therefore, understanding these cultural differences is essential for designing inclusive and effective mental health policies and interventions.
Our study contributes novel insights to the understanding of suicide risk in Spain by integrating epidemiological context with in-depth psychological profiling of vulnerable populations. In addition to highlighting the nationwide rise in suicide rates, particularly among migrants, we show that both native-born and foreign-born individuals who attempt suicide report alarmingly high levels of childhood maltreatment. However, our results also indicate that foreign-born individuals present a distinct pattern of suicide risk, characterized by greater psychological distress and a unique combination of predictors for suicidal ideation severity, including higher acquired capability, lower impulsivity, and previous suicide attempts. These findings suggest that the pathways to suicidality may differ by migration status and that social determinants such as labor instability and lack of social protection play a critical role. The identification of modifiable psychosocial stressors reinforces the importance of public policies and clinical approaches aimed at early intervention and social integration. In doing so, this research supports a shift toward comprehensive, trauma-informed prevention strategies that account for the social context of migrant populations.
Conclusion
Suicide is a major public health concern that requires continued research and evidence-based prevention strategies. Although it affects the general population, certain vulnerable groups, including migrants, face distinct risk factors that warrant targeted attention. Our study highlights the relevance of childhood maltreatment as a potential risk factor for suicidal behavior, particularly among foreign-born individuals. While we did not observe significant differences in current suicidality between native and foreign-born participants, the latter exhibited higher levels of psychological distress, greater exposure to multiple forms of child maltreatment, and elevated scores on acquired capability for suicide.
Given these findings, it is essential to implement resilience-promoting interventions for migrant youth, with a focus on mitigating acculturative stress and strengthening social integration. Institutional measures should aim to facilitate the post-migration experience—through inclusive immigration policies, access to mental health services, and the promotion of community-based support networks. These strategies may help reduce morbidity and mortality in this population by fostering connectedness and psychological well-being (Aran et al., 2023). Rather than assuming uniform effectiveness of culturally tailored suicide prevention programs, we suggest that such interventions should be contextually adapted, evidence-based, and responsive to the specific needs and experiences of different migrant subgroups.
Nonetheless, several limitations must be acknowledged. The foreign-born sample was predominantly Latin American, limiting the generalizability of our findings to other migrant populations in Spain, such as those from North Africa, who may face distinct cultural stigma and barriers to mental health care. In addition, the cross-sectional design prevents causal inferences, and the reliance on self-reported data may introduce recall and reporting biases. These methodological constraints call for cautious interpretation of the results. Future studies should include more culturally and regionally diverse samples and adopt longitudinal designs to better capture the complex interplay between early adversity, migration-related stressors, and suicidal behavior.
Footnotes
Acknowledgements
The following are members of SURVIVE: Adriana García-Ramos, Ainoa García-Fernández, Alba Toll, Andrea García González, Anna Pedrola-Pons, Beatriz Orgaz, Beatriz Rodriguez Vega, Carlos Schmidt, Daniel García, Eduard Vieta, Elena García Ligero, Elisa Seijo-Zazo, Enrico La Spina, Fernando Corbalán, Giovanna Fico, Guillermo Juarez, Guillermo Cano-Escalera, Idoia Gómez Grávalos, Irene Canosa, Itziar Leal Leturia, Javier Curto, Jennifer Fernández-Fernández, Joaquím Punti, Julia Rider, Lady Gonzalez-Agudelo, Lara Suárez-López, Laura Comendador, Lorea Mar Barrutia, Manuel Couce Sánchez, María Teresa Muñoz, María Fe Bravo, Marta Melero González, Miguel Ruiz Veguilla, Miguel Velasco, Mireia Vázquez, Natalia Angarita, Nathalia Garrido Torres, Pablo Reguera-Pozuelo, Purificación López Peña, Sara Martín, Veronica Fernandez-Rodrigues.
The authors would like to acknowledge the support of the research participants, who helped to make this work possible.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Instituto de Salud Carlos III-FIS research grants(PI19/00236, PI19/00569, PI19/00685, PI19/00941, PI19/00954, PI19/01027, PI19/01256, PI19/01484, PI20/00229 and PI23/00147, PI23/01483, PI23/00822, PI23/00614, PI23/00085, PI23/00707, PI23/0127, PI23/01469, PI23/01277, PI23/01367, PI23/01066) and S2022/BMD-7216 AGES 3-CM, S2017/BMD-3740 AGES-CM2-CM, co-funded by the European Regional Development Fund (ERDF) “A Way to Build Europe” and by the European Union grant numbers: COV20/00988, PI17/00768, PI20/01113, Horizon 2020 research and innovation programme Societal Challenges grant number: 101016127. This work was partly supported by the Government of the Principality of Asturias (Ref. PCTI 2021-2023 IDI/2021/111), “la Caixa” Foundation (Ref. HR23-00421 CaixaResearch Health 2023), CIBERSAM—Consorcio Centro de Investigación Biomédica en Red Salud Mental- (CB/07/09/0020 Group), Instituto de Salud Carlos III, Ministerio de Ciencia e Innovación and Unión Europea—European Regional Development Fund. However, the funding sources had no influence on this study. AGP thanks the support of the Spanish Ministry of Science, Innovation and Universities, integrated into the Plan Nacional de I+D+ I y cofinanciado por el ISCIII-Subdirección General de Evaluación y el Fondo Europeo de Desarrollo Regional (FEDER (PI18/01055; PI21/00713) CIBERSAM, the Basque Government 2022111054, and the University of the Basque Country IT1631-22. PLP thanks the support of the Spanish Ministry of Science, Innovation and Universities, integrated into the Plan Nacional de I+D+ I y cofinanciado por el ISCIII-Subdirección General de Evaluación y el Fondo Europeo de Desarrollo Regional (FEDER) PI19/00569, PI23/01367. IG has received support from the Secretaria d’Universitats i Recerca del Departament d’Economia i Coneixement (2021 SGR 01358), CERCA Programme / Generalitat de Catalunya, as well as the Fundació Clínic per la Recerca Biomèdica (Pons Bartran 2022-FRCB_PB1_2022).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AGP has received grants and served as consultant, advisor or CME speaker for the following entities: Janssen-Cilag, Lundbeck, Otsuka, Pfizer, Sanofi-Aventis, Alter, Angelini, Exeltis, Novartis, Rovi, Takeda, the Spanish Ministry of Science and Innovation (CIBERSAM), the Ministry of Science (Carlos III Institute), the Basque Government, and the European Framework Program of Research. IG has received grants and served as a consultant, advisor, or CME speaker for the following identities: Adamed, Angelini, Casen Recordati, Esteve, Ferrer, Gedeon Richter, Janssen-Cilag, Lundbeck, Lundbeck-Otsuka, Luye, SEI Healthcare, Viatris, outside the submitted work. She also receives royalties from Oxford University Press, Elsevier, and Editorial Médica Panamericana. In the last 5 years, IZ has received contributions in the form of registration fees for courses, congresses, and speakers from the following industries: Janssen-Cilag, Lundbeck, Otsuka, Pfizer, Angelini, Novartis, Rovi, and Takeda. PLP in the last 5 years has received collaborations in the form of registration fees for courses and congresses from the following industries: Janssen-Cilag, Lundbeck, Otsuka, Pfizer, Angelini, Novartis, Rovi, and Takeda. PAS has been a consultant to and/or has received honoraria or grants from Adamed, Alter Medica, Angelini Pharma, CIBERSAM, Ethypharm Digital Therapy, European Commission, Government of the Principality of Asturias, Instituto de Salud Carlos III, Johnson & Johnson, Lundbeck, Otsuka, Pfizer, Plan Nacional Sobre Drogas, Rovi, Servier, and Viatris España outside the submitted work.