
Abstract
During sexual assault (SA), victims commonly experience tonic immobility (TI), a state of involuntary paralysis and motor inhibition that occurs in response to extreme stress. TI often includes being unable to move or vocalize during the event (e.g., freezing, being unable to say “no”). Despite its efficacy as an evolutionary survival mechanism that may serve to prevent fatal injury, SA survivors who experienced TI are often blamed for the assault due to the false belief that lack of resistance during assault equates to consent. Self-blame and victim-blame by others are associated with more severe symptoms of posttraumatic stress disorder (PTSD). Prior research has not yet examined whether self-blame and victim-blame explain more severe PTSD among SA survivors who experienced TI. The current study tested the hypothesis that self-blame and victim-blame would mediate the relationship between TI and PTSD. All students from a public liberal arts college were asked to complete an online survey if they had a history of unwanted sexual contact. Among participants who completed all survey measures (N = 76), self-blame, but not victim-blame, mediated a link between TI and PTSD. This study highlights the need for interventions, such as cognitive processing therapy (CPT), that address cognitive distortions, including the survivor’s belief that they should have done more to stop the assault. Thus, CPT may be a particularly promising therapy for SA survivors who blame themselves for the assault because of their experience of TI.
Introduction
Sexual assault (SA), defined as any sexual contact occurring without explicit and enthusiastic consent (e.g., a clear, continuous “yes”) of the victim, is a pervasive problem among colleges and universities (Rape, Abuse and Incest National Network [RAINN], 2023). SA affects approximately one in five female and TGQN (transgender, genderqueer, nonconforming) students, as well as one in sixteen male students (Bell et al., 2023; Cantor et al., 2015). SA can have negative psychological consequences, including the development of posttraumatic stress disorder (PTSD; RAINN, 2023). Survivors commonly experience severe PTSD symptoms (Dworkin et al., 2021), which are frequently accompanied by feelings of intense shame and isolation that significantly impair their ability to cope with stress and thrive in an academic environment (Dworkin et al., 2021; Tipps et al., 2014). Although SA is associated with more severe PTSD compared to other traumatic events (Dworkin et al., 2021), SA survivors do not all experience PTSD symptoms to the same degree. The survivor’s behavior during the assault has been identified as one factor that predicts more severe PTSD symptoms, though reasons for this effect are unclear (deMello et al., 2022; Möller et al., 2017). The current study examined two potential mediators linking the survivor’s behavior during the assault to PTSD symptom severity.
Survivors’ behavior during a traumatic event, referred to as their peritraumatic response, encompasses a variety of stress responses, many of which may not fit societal expectations of how the survivor “should” have behaved (deMello et al., 2022). The “fight-or-flight” response is commonly used to describe the body’s reaction to extreme stress, and refers to the ways in which a person’s sympathetic nervous system mobilizes energy to either attack the threat (the “fight” response) or evade the threat (the “flight” response) (American Psychological Association [APA], 2023). However, peritraumatic responses can be more complex and include behaviors that do not fit the description of physical resistance or attempted escape. One such response is the “freeze” response which has been found to be uniquely associated with severe PTSD symptoms (deMello et al., 2022; Möller et al., 2017).
The freeze response, referred to as tonic immobility (TI), is an involuntary response to extreme stress in which an individual experiences a catatonic-like state, unable to vocalize, physically resist, or escape (Humphreys et al., 2010; Marx et al., 2008). TI is common during SA, reported by as many as 70% of female survivors (Möller et al., 2017). While a lack of resistance seems counterintuitive since it increases the likelihood of assault completion (Tark & Kleck, 2014), it can serve as an adaptive survival mechanism, reducing the risk of physical injury when resistance is perceived to be futile (Carli & Farabollini, 2022). Indeed, despite some mixed evidence, the majority of research supports a link between active resistance and greater physical injury (see Wong & Balemba, 2018 for a systematic review and meta-analysis). Additionally, in situations where the survivor perceived the perpetrator as physically stronger or armed, the sympathetic nervous system may have triggered TI as a defense mechanism (Bachman et al., 2002; Volchan et al., 2011). However, while TI may increase the chances of survival during an assault, it is linked to more severe PTSD symptoms, particularly in relation to symptoms of avoidance and re-experiencing (Coimbra et al., 2023; Hagenaars, 2016).
The association between TI and PTSD symptom severity has been well-documented (de la Torre Laso, 2023). Women who experience TI during SA are twice as likely as those who do not experience TI to develop PTSD (Möller et al., 2017). The consistent finding that TI is associated with more severe PTSD underscores a need to understand why TI leads to more severe symptoms. Although prior research links TI to PTSD symptoms through posttraumatic guilt and shame (Bovin et al., 2014), no study has examined the mediating effects of self-blame, a cognitive distortion based on the false belief that a lack of resistance indicates consent (Burgin, 2019; Young et al., 2021).
Despite TI’s effectiveness as a survival mechanism, societal rape myths, or false and harmful beliefs about how survivors “should” have responded, persist, leading many survivors to blame themselves for not resisting more forcefully to prevent the assault (Ullman et al., 2014). The myth that a victim must physically fight back or say “no” repeatedly for the assault to be classified as SA is widespread (de la Torre Laso & Rodriguez-Diaz, 2022). However, there is no singular or “correct” response to victimization, and lack of repetitive, forceful resistance does not indicate consent (RAINN, 2023). In reality, only a minority of survivors report having engaged in physical resistance during the assault (Kaysen et al., 2005), and even those who did sometimes face blame based on the timing or intensity of their resistance (Rusinko et al., 2010). Victim-blaming culture and societal expectations regarding how a survivor should have behaved can reinforce self-blame and worsen PTSD symptoms (Salim et al., 2023).
In addition to more severe PTSD among survivors who blame themselves for the assault, survivors may also experience more severe PTSD symptoms when they are blamed by others (O’Neal, 2019). Various studies have demonstrated associations between victim-blaming responses from others and increased risk of PTSD symptoms after an assault (Dworkin et al., 2021; Ullman et al., 2017; Wilson et al., 2022). Researchers theorize that when survivors are blamed by others, they experience exacerbated feelings of shame and secondary victimization, and are also more likely to engage in maladaptive coping and social withdrawal following disclosure (e.g., Bhuptani & Messman, 2023; Lee et al., 2023; Relyea & Ullman 2015). Better understanding the role of both self-blame and victim-blaming from others following TI during SA could have notable implications for the improvement of clinical interventions and educational programs designed to support survivors of SA.
The current study examined whether blame mediates the association between TI and PTSD symptom severity. We hypothesized that TI during SA would be associated with greater self-blame and victim-blame from others, which in turn would be associated with more severe PTSD symptoms. We also hypothesized that there would be a significant indirect effect of TI on PTSD symptoms through self-blame and victim-blame. Understanding these mediators is crucial for refining interventions that reduce the psychological toll of SA and enhance survivor support. By exploring the role of blame in PTSD symptom severity, this study aims to inform educational programs on sexual violence and consent, as well as treatment approaches for reducing negative psychological outcomes for survivors.
Method
Participants
The study was conducted in the fall of 2024 at a public college in the Northeastern United States. Students (ages 18 and older) were recruited through an online survey distributed via email to all students enrolled at the college. The email instructed students to only complete the survey if they had experienced unwanted sexual contact since entering the college. Although 790 students responded, 33 were excluded for failing quality control questions assessing participants’ attention and response accuracy (e.g., “If you are still reading this, please select ‘moderately’”). Of the remaining 757 respondents, only 123 (16.64%) reported a history of sexual assault victimization by indicating they had experienced unwanted sexual contact through either (a) physical force (n = 57, 7.5%), (b) by pressuring, coercion, or threat (n = 89, 12.5%), and/or (c) while they were unable to provide consent or stop what was happening because they were passed out, drugged, drunk, incapacitated, or asleep (n = 49, 6.5%). Participants who responded yes to any of the three questions and completed all survey measures were included in the study. If participants did not respond yes to any of the three questions, they were exited from the survey. Assessment of potential attrition bias indicated that participants who completed the full survey (N = 76, 38% attrition rate) were older (M = 20.60, SD = 1.91, Mdifference = −0.68, t (123) = −2.04, p < .05) and more likely to identify as a member of a sexual minoritized group (26.0% of attritors vs. 53.9% of survey completers, χ2 (1, N = 126) = 9.62, p < .01). To account for potential attrition bias, we controlled for sexual minoritized identity and age when testing the study hypotheses. The final sample consisted of 80.3% cisgender women, 11.8% cisgender men, 2.6% transgender men, and 5.3% nonbinary students. Participants were 73.7% White, 21.1% Hispanic/Latino, 9.2% Asian, 7.9% Black/African American, 1.3% American Indian/Alaskan Native, and 3.9% who chose to self-describe. Regarding sexual orientation, 46.1% of participants identified as straight, 34.2% as bisexual/pansexual, 7.9% as gay/lesbian, 5.3% as queer, 3.9% as unsure/questioning, and 2.6% chose to self-identify. Participants also consisted of 10.5% first years, 11.8% sophomores, 34.2% juniors, and 42.1% seniors.
Procedure
Study procedures were approved by the Institutional Review Board at the College. Students received an email with a link to the online survey conducted through the online survey platform Qualtrics. The link directed the students to an informed consent form where they were asked to indicate their consent to participate in the anonymous survey. Students who did not consent to participate were exited from the survey. Those who provided consent could exit the survey at any time, and all the questions were optional. At the end of the survey, participants were directed to a form where they could provide their email address to enter a raffle to win one of twenty $50 Amazon gift cards. Email addresses were not linked to survey responses in any way.
Measures
Tonic Immobility
TI was assessed using the 7-item physical immobility subscale of the Tonic Immobility Scale Adult-form (TIS-A; Forsyth et al., 2000). Items were rated on a 7-point scale from 0 (not at all) to 6 (extremely). Sample items included whether the participant felt paralyzed, cold, or numb during the assault and whether they were unable to call out or scream during the assault. Total sum scores ranged from 0 to 42 (>21 representing significant immobility, ≥28 representing extreme immobility). The current sample demonstrated good internal consistency of the physical immobility items (α = .87).
Self-Blame
Self-blame was assessed using the 5-item self-blame subscale of the Rape Attribution Questionnaire (RAQ; Frazier, 2003). Participants were asked to rate how often they had different thoughts about their assault from 1 (never) to 5 (very often). Sample items include “This happened to me because I should have resisted more” or “This happened to me because I used poor judgment.” Items from the self-blame subscale were summed, such that higher scores indicated greater endorsement of self-blame. The current sample demonstrated good internal consistency of the self-blame items (α = .85).
Victim-Blame
Participants completed the Social Reactions Questionnaire-Shortened version (SRQ-S; Ullman et al., 2017), a 16-item questionnaire that measures social reactions to disclosures of sexual assault. Participants completed the SRQ-S separately for reactions received from informal support (e.g., family and peers) and formal support (e.g., police and Title IX staff); however, because so few participants reported disclosing to formal support (n = 15), we combined responses by taking a mean of informal and formal reactions for each item. Consistent with prior research, we used two items from the victim-blame subscale: “Told you that you were irresponsible or not cautious enough,” and “Told you that you could have done more to prevent this experience from occurring” (Wilson et al., 2022). Participants were asked to indicate how often they had experienced each of these reactions upon disclosing their SA to others on a 0 (Never) to 4 (Always) scale. We used a mean of both items, such that a higher score indicated more victim-blame (rsb = .85).
PTSD Symptoms
PTSD symptoms were assessed using the 20-item PTSD Checklist for the DSM-5 (PCL-5; Weathers et al., 2013). Items were rated on a 5-point scale from 0 (Not at All) to 4 (Extremely). Items were summed to obtain a symptom severity score ranging from 0 to 80. Scores above 31 to 33 are consistent with a probable PTSD diagnosis (Bovin et al., 2016). Sample items include “In the past month, how much were you bothered by: ‘Repeated, disturbing, and unwanted memories of the stressful experience’, and ‘Avoiding memories, thoughts, or feelings related to the stressful experience’.” In the current sample, the PCL-5 demonstrated good internal consistency (α = .95).
Data Analytic Plan
Analyses were conducted using IBM SPSS Statistics version 29. Preliminary analyses included descriptive statistics and bivariate correlations among study variables. Given the use of bootstrapping in mediation analyses, we did not transform the PTSD symptom or victim-blame variables to correct for positive skew. The mediation model depicted in Figure 1 was tested using the PROCESS macro for SPSS, Model 4 (Hayes, 2017) with 5,000 bootstrap samples to account for violations of normality (Hayes, 2022). TI was entered as the predictor variable, self-blame and victim-blame as mediator variables, and PTSD symptoms as the outcome variable. We considered the indirect effect to be statistically significant if the confidence interval did not include zero. The mediation model had adequate statistical power (80%) to detect a medium indirect effect (Fritz & MacKinnon, 2007).
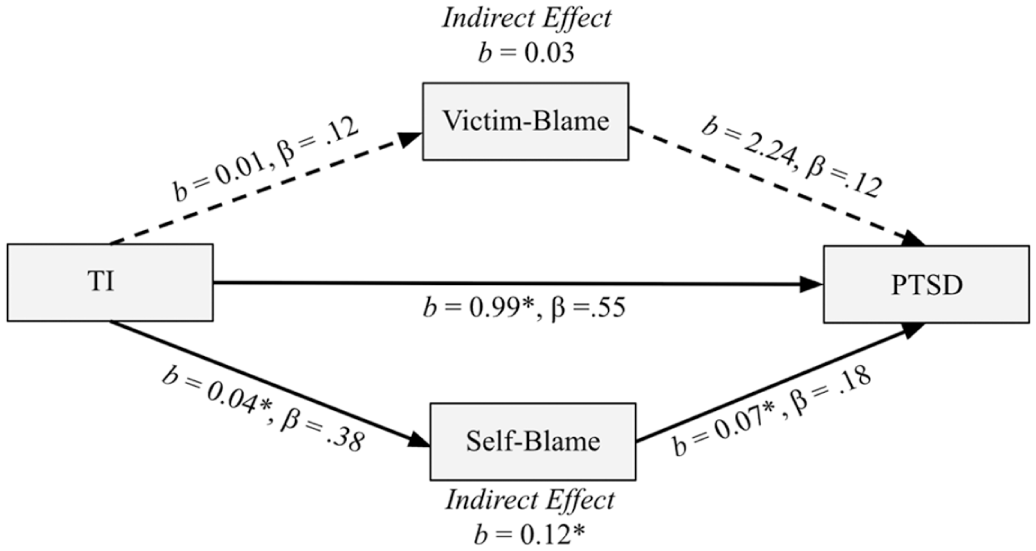
Mediation model.
Results
Preliminary analyses included descriptive statistics and bivariate correlations for all study variables. Of the participants, 18.9% reported significant TI and an additional 13.8% reported extreme TI (M = 18.15, SD = 10.19). In addition, 30.4% of participants reported scores above the cutoff score of 31 for clinically significant PTSD symptoms on the PCL-5 (M = 25.07, SD = 18.39). On average, participants endorsed occasional to moderate self-blame (M = 16.38, SD = 5.66), but they generally reported experiencing victim-blame from others “never” or “rarely” (M = 0.78, SD = 0.97). As expected, there were positive correlations between TI and self-blame (r = .39, p < .01), TI and PTSD (r = .63, p < .01), self-blame and victim-blame (r = .49, p < .01), self-blame and PTSD (r = .45, p < .01), and victim-blame and PTSD (r = .24, p < .05). The correlation between victim-blame and TI was positive but not significant (r = .12, p = .29). Mediation analysis assessed whether self-blame and victim-blame from others mediated the relationship between TI and PTSD (see Figure 1 for standardized and bootstrap coefficients). TI significantly predicted self-blame and PTSD symptoms; however, TI was not a significant predictor of victim-blame from others. Self-blame significantly predicted PTSD symptoms, and the indirect effect of TI on PTSD through self-blame was significant. The effect of victim-blame from others on PTSD symptoms was not significant, and there was no indirect effect of TI on PTSD symptoms through victim-blame.
Discussion
The purpose of this study was to evaluate whether TI predicted PTSD symptom severity through the pathways of self-blame and victim-blame from others. Consistent with prior research, TI significantly predicted PTSD symptom severity. To our knowledge, this is the first study to demonstrate TI as a significant predictor of self-blame. We also found that self-blame mediated the link between TI and PTSD, but our hypotheses regarding victim-blame were only partially supported. Specifically, victim-blame did not emerge as a significant mediator when accounting for the effect of self-blame.
Our findings align with previous studies demonstrating that TI is a common response during SA and is associated with more severe PTSD symptoms (de la Torre Laso, 2023; Möller et al., 2017). These results underscore the potential role of self-blame in understanding how TI may contribute to PTSD severity and highlights the need for educational and clinical interventions that address both TI and self-blame in SA survivors. We extend the literature by demonstrating that self-blame is a mediator of the link between TI and PTSD symptoms. Previous research has shown that societal rape myths often contribute to self-blame in survivors, as they may believe that their nonresistance during an assault implied their consent (O’Neill & Kerig, 2000; Salim et al., 2023). Our study supports that survivors who experienced TI during the assault are more likely to engage in self-blaming attributions, which, in turn, is associated with more severe PTSD symptoms (Bhuptani & Messman, 2021; Kline et al., 2021).
Survivors who experienced TI were not more likely to report victim-blaming reactions from others. One explanation for this finding is that survivors may not disclose to others that they experienced TI during the assault. Even if survivors did disclose their TI to others, they might have been met with more compassion and empathy than they showed themselves. For instance, others may not blame the victim if they perceive them as having less control in preventing the assault from occurring because they understand that TI prevented the victim from being able to resist. Thus, education may be particularly important in ensuring survivors receive adequate support from others. Although victim-blame was not associated with TI, it was associated with more PTSD symptoms, which is consistent with prior literature demonstrating the harm of negative social reactions to disclosures of SA (Ullman & Peter-Hagene, 2016). However, the effect of victim-blame on PTSD symptoms was not significant in the full mediation model, when accounting for the effects of self-blame. With self-blame in the model, the statistical power may have been too low to detect relatively small effects for victim-blame. Future research should continue to explore the role of victim-blame in the PTSD response, particularly in larger, more diverse samples. Longitudinal studies should also use serial mediation to test whether self-blame is at least partially a result of experiencing victim-blaming reactions from others (Morris & Quevillion, 2021; Ullman & Najdowski, 2011) or vice versa (Hassija & Gray, 2012).
Additionally, only 16.6% of the sample reported experiences of SA, which is lower than prevalence rates typically reported on college campuses. Notably, SA was not assessed using the revised Sexual Experiences Survey (SES-SFV; Koss et al., 2007), a widely used measure that provides behaviorally specific definitions of rape, attempted rape, and other forms of unwanted sexual experiences. Instead, SA was assessed using a single item asking whether participants had experienced “unwanted sexual contact through force, coercion, or incapacitation.” Although similar single-item definitions have been used in prior research (Ullman et al., 2017), the relatively low prevalence of SA observed in this study may be attributable, in part, to the lack of a more detailed and behaviorally specific assessment.
While findings regarding the relationship between TI and self-blame are compelling, the cross-sectional nature of this study presents a considerable limitation in the ability to draw causal inferences. Although we were unable to test the direction of effects between the study variables, the temporal ordering was based on longitudinal evidence from prior literature that supports the proposed direction of effects. For instance, prior longitudinal research shows that the development of PTSD symptoms occurs after the experience of TI and similar peritraumatic responses such as dissociation (Birmes et al., 2003; Möller et al., 2017). Additionally, dysfunction in posttraumatic cognitions about the self contributes to the development and maintenance of PTSD symptoms over time (Dalgleish, 2004; Ehlers & Clark, 2000; Resick et al., 2002). More specifically, self-blame for behavior during the assault has been found to influence the later onset of PTSD symptoms (Kline et al., 2021). Unfortunately, the current study’s cross-sectional model precludes us from replicating the direction of effects between blame and PTSD. It is possible that self-blame occurs as a result of PTSD (Kline et al., 2021). Indeed, persistent negative beliefs about oneself following a traumatic event is a symptom of PTSD (American Psychological Association [APA], 2013). Future longitudinal studies should establish more robust evidence for our mediation model.
Another important limitation of the correlational design is that it prevents us from being able to rule out alternative explanations for the observed effects. For instance, TI might be associated with more severe PTSD because survivors who experienced TI felt helpless during the assault (Hagenaars, 2016; Möller et al., 2017). In fact, many survivors who experienced TI indicate that the most traumatic aspect of the assault was that they were unable to move or resist verbally (Gbahabo & Duma, 2021). Thus, perceived helplessness associated with TI provides an alternative explanation for the association between TI and PTSD symptoms. Additionally, survivors may have experienced a co-occurrence of TI and peritraumatic dissociation, which has been associated with disruption in memory encoding, potentially exacerbating PTSD symptoms (Bedard-Gilligan & Zoellner, 2012; deMello et al., 2022). Trauma-related shame (TRS) related to TI might also explain more severe symptoms of PTSD, as TRS may be a byproduct of falsely attributing nonresistance to consent. Finally, it is possible that TI occurs as a result of prior victimization (Tannahill et al., 2023). Future studies should compare the effects of TI that occurs during a first assault versus subsequent revictimization. Thus, these additional factors offer alternative explanations for why PTSD symptoms are more severe among survivors who experienced TI. Future research should clarify their role in the posttraumatic response of sexual assault survivors.
Despite these limitations, preliminary findings, in combination with prior findings from clinical intervention research, may inform trauma-focused therapy for SA survivors (Schumm et al., 2015). The higher prevalence of self-blame among survivors who experienced TI emphasizes the need to restructure maladaptive cognitions related to self-blame (e.g., “nonresistance implied consent”) for those survivors. Cognitive processing therapy (CPT) is an effective therapeutic intervention for survivors of SA that improves PTSD symptoms by targeting self-blaming cognitions (O’Doherty et al., 2023; Miles et al., 2024; Schumm et al., 2015; Wilson et al., 2022). Thus, CPT could be a particularly effective treatment for survivors of SA who experienced TI. Therapists should also promote a better understanding of TI as an involuntary and adaptive biological response to trauma. As such, these findings may serve to educate survivors, their support networks, and clinicians about the biological nature of TI as an involuntary response to extreme threat, and subsequently reduce self-blame, promote self-compassion, and improve PTSD treatment outcomes (Bhuptani & Messman, 2021; Hamrick & Owens, 2018; Kearney et al., 2013).
Moreover, public awareness campaigns should also inform the general public about TI, emphasizing that a lack of resistance does not imply consent nor does it invalidate an experience as assault. For instance, the common experience of TI observed in our study may have notable implications for the judicial system where reports of SA are often considered false by law enforcement in the absence of physical resistance (O’Neal, 2019). Currently, perpetrators are convicted in as little as 3% of reported assaults, and survivors consistently experience secondary victimization due to victim-blaming from law enforcement (Campbell et al., 2021). Notably, research shows that when common indicators of physical resistance (e.g., cuts or bruises) are not present, police officers are more likely to question victim credibility and doubt that an assault occurred (O’Neal, 2019). Given the tendency of law enforcement to not always believe the survivor, it is no surprise that only a small percentage of SA survivors in the current study reported their assault to formal authorities. This is consistent with prior studies in which survivors describe not reporting to the police out of fear of non-belief, judgment, and secondary traumatization, as well as a lack of trust in the judicial system (Johnson, 2017; Jones et al., 2009). As such, a shift in understanding of TI as both an involuntary and adaptive defense mechanism may allow for a better understanding of why victims do not resist to promote empathetic, evidence-based approaches to handling cases of sexual assault (Lorenz et al., 2019).
The current study provides novel insights into the relationship between TI, self-blame, and PTSD symptoms among survivors of SA. Findings reinforce the notion that survivors’ experience of TI during SA is associated with more severe PTSD symptoms and demonstrates that self-blame mediates this relationship. Increasing awareness of TI as a common biological defense mechanism and challenging the false belief that nonresistance indicates consent may have important implications for therapists, as well as members of law enforcement. Specifically, targeting self-blaming cognitions related to TI may protect survivors from severe PTSD symptoms. Considering that TI is particularly common among survivors of SA, future longitudinal studies should examine whether self-blame is a mechanism that explains increased PTSD symptom severity related to TI.
Footnotes
Ethical Considerations
The Institutional Review Board at The College of New Jersey approved the study procedures. Study participants were treated in acccordance with APA ethical standards.
Consent to Participate
The study participants provided written informed consent.
Funding
The authors received no financial support for the research and/or authorship of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Data Availability Statement
The participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the research supporting data is not available.
Diversity Statement
Data was collected as part of a series of survey studies conducted at a public college to evaluate the experiences of diverse groups of students. Though participants were more likely to identify as members of a sexually minoritized group, the sample lacked racial and gender diversity with a majority identifying as White, and women.