
Abstract
The link between intimate partner violence (IPV) and suicidality has been well-established in empirical literature; yet, these phenomena are typically measured independently and associated via statistical tests. The purpose of this study was to assess whether women reported suicidality directly due to their experiences of IPV victimization. Data were collected from 150 women who experienced IPV and were receiving civil legal services in a Midwest state in the United States. Women were asked if they ever had suicidal thoughts, made suicidal gestures, made a plan for suicide, or attempted suicide as a result of the abuse they experienced from their intimate partner. Women were also asked about suicidality as a result of childhood maltreatment, along with aspects of well-being. Nearly 45% of the sample (n = 67) reported some form of suicidality as a result of IPV. There were no group differences in women’s reports of suicidality (lifetime-only, past year/lifetime, none) with respect to any sociodemographic characteristics; however, physical IPV was greater among women who reported both past year and lifetime suicidality compared to women who reported no suicidality (p = .027). Group differences in suicidality were also associated with depressive and posttraumatic stress disorder (PTSD) symptoms, interpersonal support, and empowerment. The study findings demonstrate a more nuanced link between IPV and suicidality, which have implications for IPV and suicide prevention and future data collection efforts.
Introduction
Intimate partner violence (IPV) and suicide are both preventable public health crises that affect millions of individuals, families, and communities in the United States. An estimated 41% of women in the United States experienced contact sexual violence, physical violence, or stalking by an intimate partner during their lifetime and reported a related impact (Leemis et al., 2022). Women’s experiences of IPV victimization are associated with a wide range of health disparities, including physical health problems, mental health disorders, and parenting difficulties (Beydoun et al., 2012; Breiding et al., 2008; Chiesa et al., 2018; Dillon et al., 2013; Lagdon et al., 2014; Trevillion et al., 2012). IPV yields a population economic burden of nearly $3.6 trillion over victims’ lifetimes (Peterson et al., 2018) and jeopardizes the safety of whole communities.
Suicide is a leading cause of death in the United States, with over 49,000 deaths reported in 2023 (Centers for Disease Control and Prevention [CDC], 2025). In 2023, suicide was the second leading cause of death for people ages 10–14, 15–24, and 25–34, and it was the fourth and fifth leading cause of death among people ages 35–44 and 45–54, respectively (CDC, 2024). Annually, the number of people who think about or attempt suicide is significantly higher than the number of people who die by suicide. Among adults aged 18 or older in 2020, 4.9% (or 12.2 million people) had serious thoughts of suicide, 1.3% (or 3.2 million people) made a suicide plan, and 0.5% (or 1.2 million people) attempted suicide in the past year (Substance Abuse and Mental Health Services Administration [SAMHSA], 2021). In 2019, the economic cost of suicide deaths was highest among those aged 25–44 years ($167 billion) and 45–64 years ($174 billion; Peterson et al., 2021).
The association between IPV and suicidality (which includes ideation, plans, behaviors, and attempts) has been well-established in empirical literature. IPV victimization has been associated with suicidal ideation and suicide attempts among diverse samples of adults both within the United States and across the globe (Afifi et al., 2009; Chan et al., 2008; Devries et al., 2011; Kazan et al., 2016; McLaughlin et al., 2012). The extant literature also includes many variables that influence the relationship between IPV victimization and suicidality. For example, depression and posttraumatic stress disorder (PTSD) have been reported as key intervening factors in suicidality among women who experience IPV (Alhusen, et al., 2015; Devries et al., 2013; Dillon et al., 2013; Pico-Alfonso et al., 2006; Wolford-Clevenger et al., 2019). Social support, self-efficacy, and feelings of hopefulness have been found to serve as protective factors in the association between IPV victimization and suicidality (Meadows et al., 2005; Muyan & Chang, 2019; Yoon et al., 2022). Empowerment has been associated with less depression and PTSD symptoms among women who experience IPV (Wright et al., 2010); and research explorations on the overlap between IPV and suicidality should also include variables that may influence this association.
In addition to empirical research associations, IPV is a component within the interpersonal theory of suicide. According to the theory, when an individual’s need for belonging is unmet (referred to as thwarted belongingness), a desire for death may develop. Experiences of IPV can lead to social isolation and a lack of reciprocally caring relationships, which is a contributor to thwarted belongingness (Van Orden et al., 2010). In addition to constructs of thwarted belongingness and perceived burdensome, the interpersonal theory of suicide requires acquired capability for someone to die by suicide. The capability for suicidal behavior emerges, via habituation and activation of opponent processes, in response to repeated exposure to physically painful and/or fear-inducing experiences (Smith & Cukrowicz, 2010; Van Orden et al., 2010). To die by suicide, an individual must lose some of the fear associated with suicidal behaviors. People who experience violence, particularly physical and/or sexual violence over time, are more likely to experience the lowered fear of death and the elevated tolerance for physical pain required to acquire the capability for suicide. Along with IPV, child abuse is also a factor of acquired capability for suicide. There is robust empirical literature on the association between child maltreatment and suicidality in adolescence (Miller et al., 2013) and adulthood (Angelakis et al., 2019). Child maltreatment is also a well-established risk factor for IPV victimization (Li et al., 2019).
Measuring IPV Victimization and Suicidality
Despite the robust literature, few researchers have made intentional efforts to connect the occurrence of IPV victimization with the occurrence of suicidal thoughts and behaviors via measurement that directly joins the two experiences. In most research studies, these experiences are measured separately. Researchers often use standardized measures to assess women’s lifetime or recent (i.e., within the past year) IPV experiences (e.g., Revised Conflict Tactics Scale; Index of Spouse Abuse) and standardized measures (e.g., Suicide Resilience Inventory; International Classification of Diseases codes) or dichotomous items (‘Have you ever had thoughts of suicide?’; ‘Have you ever attempted suicide?’) to assess an individual’s history or recent experiences of suicidal ideation, behaviors, and attempts. Using measures that separately assess each phenomenon, the link between IPV victimization and suicidality is made via statistical tests of association rather than through measuring the role of violence in someone’s suicidal thoughts, plans, behaviors, and attempts. As such, the nature of the association (i.e., whether suicidality is a risk factor for IPV or a consequence of IPV) may not be as well-established as previously thought.
A review of published literature revealed eight studies in which the authors made attempts to connect IPV and suicide by measuring the two phenomena together (see Table 1). However, each study has limitations in how IPV and suicide were connected (e.g., focusing on conflict but not IPV; measuring suicide attempts but not suicidal thoughts or behaviors; not separating IPV from other forms of family violence; not providing the survey item or interview question used).
Publications in Which Authors Focused on Connecting IPV and Suicidality via Measurement.
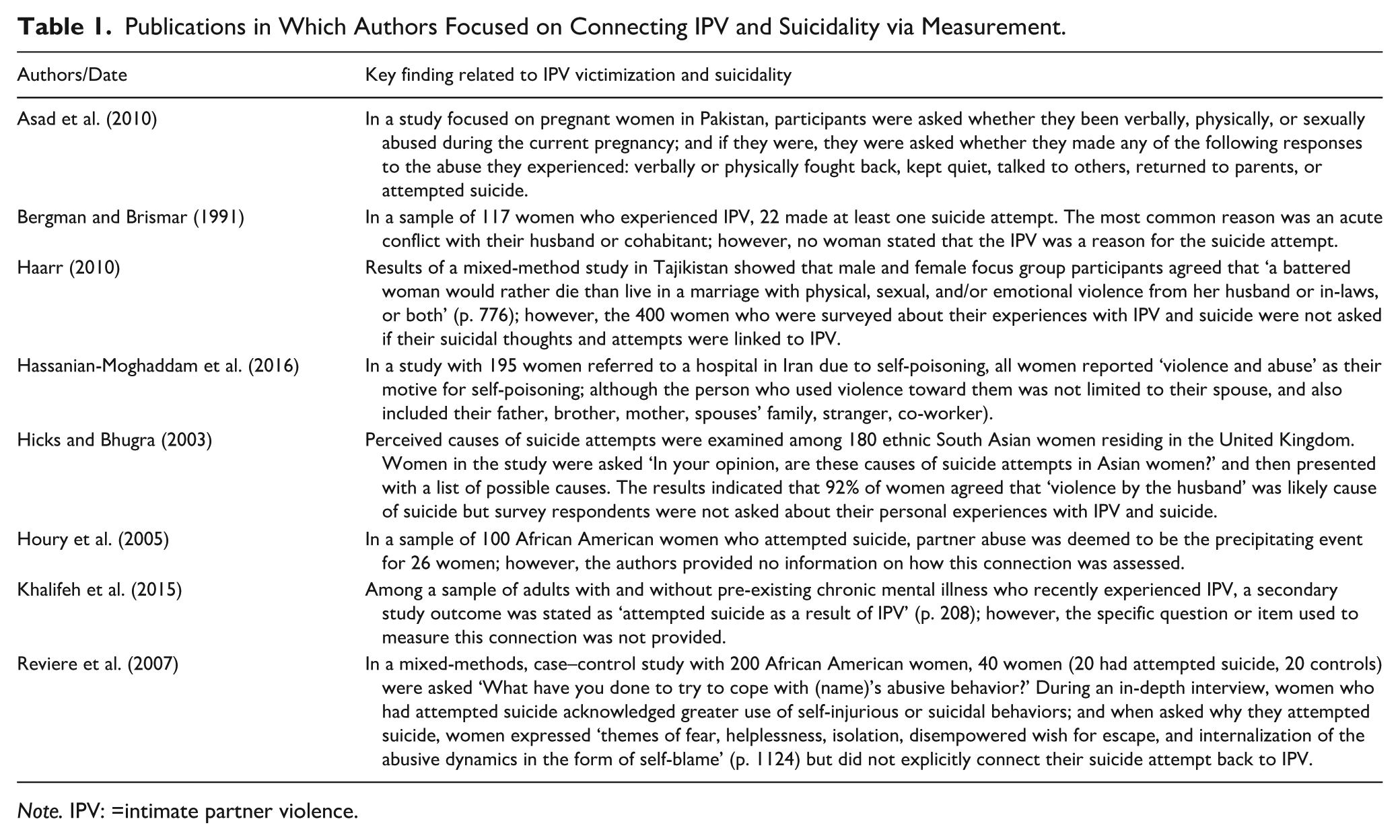
Note. IPV: =intimate partner violence.
The primary purpose of this study was to assess whether women reported suicidal thoughts, made suicidal gestures, developed a plan for suicide, or attempted suicide because of the IPV they experienced. Despite the robust literature linking IPV and suicidality, women who experience IPV are not often asked whether suicidality was directly attributed to the violence they experienced. Measuring suicidality among survivors of IPV in this manner is unique and fills a gap in the extant literature. This study may be one of the first to explicate this connection in this manner. As a secondary purpose of this study, women were asked whether they attributed any suicidality to their experiences of childhood maltreatment. This also contributes to the field, as child maltreatment and suicidality are also typically measured separately. Finally, analyses were performed to examine whether sociodemographic characteristics, types of IPV, and aspects of well-being were associated with women’s reports of suicidality. The findings highlight the connection between abuse and suicide in several unique ways, specifically by presenting the number of women who report suicidality as a direct result of their experiences of IPV and child maltreatment.
Method
Data Source
This study utilized baseline data from a larger, 2-year study of women who experienced IPV and received civil legal services. Potential participants contacted Iowa Legal Aid (ILA) for a civil legal matter and self-identified as having experienced IPV victimization. ILA is a non-profit organization that provides civil legal services to low-income Iowans in all 99 counties from offices located in 10 Iowa cities, averaging 20,000 cases per year. Recruitment for the study focused on women who had a history of IPV and contacted ILA for services related to a family law matter or a civil protection order (CPO), which are the two largest categories of services provided to women by legal aid offices.
Data Collection
The ILA intake staff assessed IPV victimization using a set of screening items focused on physical abuse (‘Has your spouse or partner ever physically abused or threatened to harm you or your children?’), sexual abuse (‘Has your spouse or partner ever forced you to have sex or unwanted sexual touching?’), stalking (‘Has your spouse or partner ever done anything to make you feel that you were being stalked, such as: following or spying on you; waiting for you outside of home/school/work; or making unwanted contact such as phone calls, mail, e-mails, or leaving gifts?’), and psychological abuse (‘Has your spouse or partner ever done any of the following: threatened or attempted to kill himself/herself; destroyed your personal belongings; kept you from friends and family; told you where you are allowed to go; made you afraid of him or her; stopped you from leaving your house; or hurt your pets?’). Once a woman met ILA’s initial screening criteria for receiving services (a ‘yes’ response to any of the screening items), the inclusion criteria for the larger study were applied. Potential study participants: (1) were female and 18 years of age or older; (2) had minor children in the home; and (3) ILA accepted their legal case for representation of a family law-related issue or a CPO.
Once ILA accepted the woman’s case, staff contacted her to inquire if she would be willing to share her contact information with the study researchers. Study recruitment and data collection took place between June 2012 and November 2015. Three-hundred eighty-three women agreed to learn more about the study during this period. ILA staff transferred contact information for these women to the researchers using a password-protected web file transfer service. A research assistant contacted women to explain the study and ask if they were interested in participating. Women who verbally agreed to participate were assigned to an interviewer in their geographic area of the state, who contacted them to schedule the first interview. Interviewers in 7 locations across the state conducted in-person interviews with participants using a structured interview guide. Interviewers conducted an initial interview (Wave 1), and up to 4 follow-up interviews at 6, 12, 18, and 24 months (Waves 2–5). Participants received a $75 gift card for the first interview and a $65 gift card for each follow-up interview (maximum of five interviews over 2 years). Women provided informed consent through a signed consent form at the first interview. The University of Iowa Institutional Review Board approved this study. A total of 150 women completed a baseline interview.
Sample
Table 2 presents sociodemographic statistics for the study sample (N = 150). The mean age of the respondents was 32.07 years (SD = 7.55). All the women had children, with an average of 2.59 children (SD = 1.47; range = 1–9). Most women identified as non-Hispanic White (n = 120; 80.0%), with 8.0% (n = 12) who identified as non-Hispanic Black and 8.67% (n = 13) who identified as Hispanic. Over 70% of the women had some post-secondary education (n = 106; 70.67%) and 57.33% (n = 86) of the women were working at least part-time.
Sociodemographic Characteristics for Women Who Reported No, Lifetime-Only, or Past Year/Lifetime Suicidality.
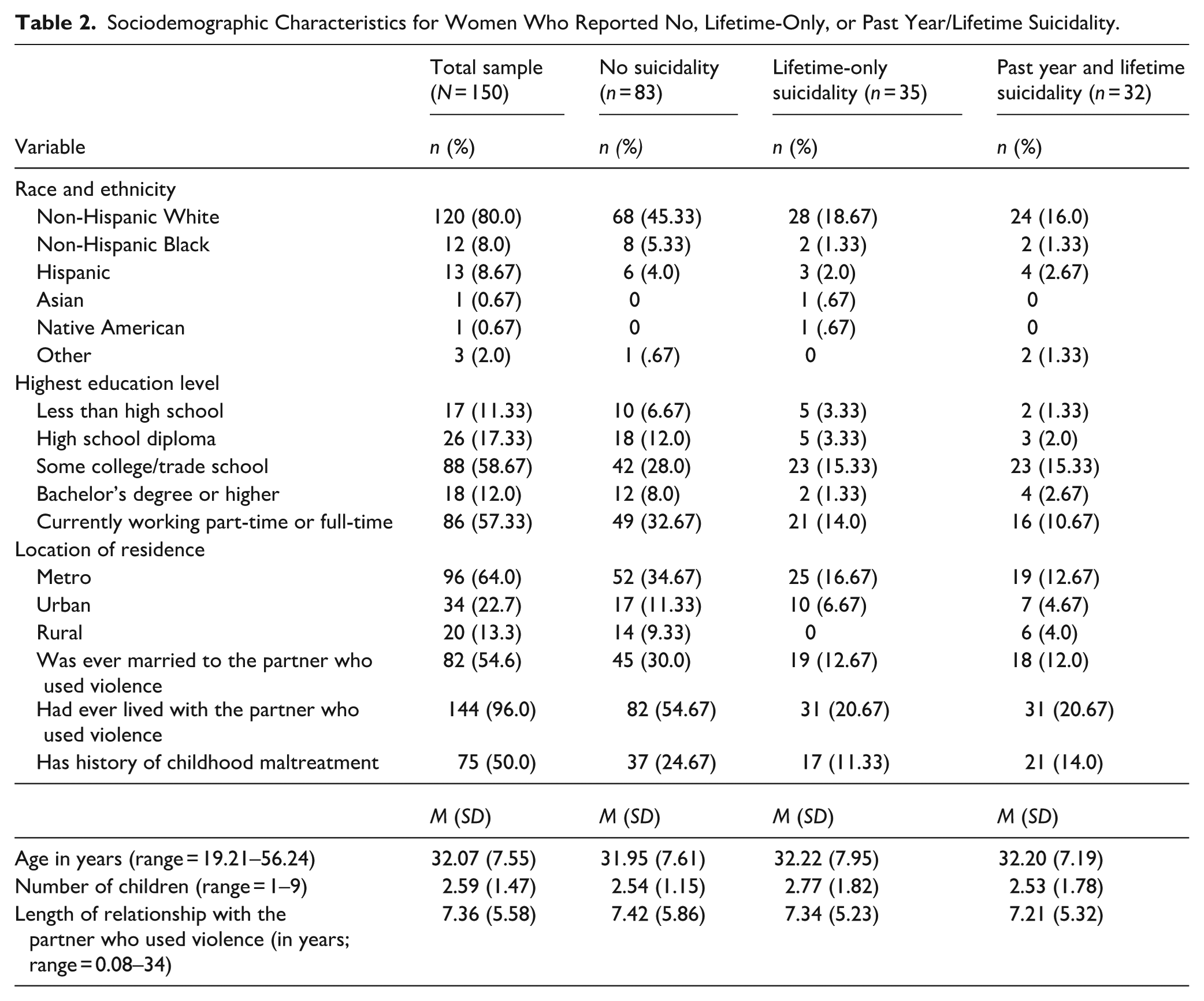
All the women in the sample experienced abuse by a male partner, although the use of violence by a male was not a study criterion. The average length of the relationship between a woman and her partner was 7.36 years (SD = 5.58). Most of the women reported having lived with the partner who used IPV at some point in their relationship (n = 144; 96.0%), and 54.67% were ever married to him (n = 82). Nearly two-thirds of women (n = 97; 64.67%) received assistance from ILA for a CPO, while approximately one-third (n = 53; 35.33%) sought services for a family law problem (e.g., divorce, custody). Women’s zip codes were used to discern their county of residence. Counties were then classified as metro, urban, and rural, based on Rural Urban Continuum codes. Over 20% of the women resided in urban (n = 34; 22.67%) and rural communities (n = 20; 13.33%), with 64% residing in metro areas (n = 96). Exactly half of the sample (n = 75) reported they experienced abuse or neglect as a child.
Measures
Intimate Partner Violence
Women in the study were already deemed to have experienced IPV as part of the ILA screening protocol. However, additional measures were used to gather more extensive information on the violence experienced by women in the study. Data on women’s experiences of IPV are presented in Table 3.
Self-Reported Lifetime and Recent Suicidality (N = 150).
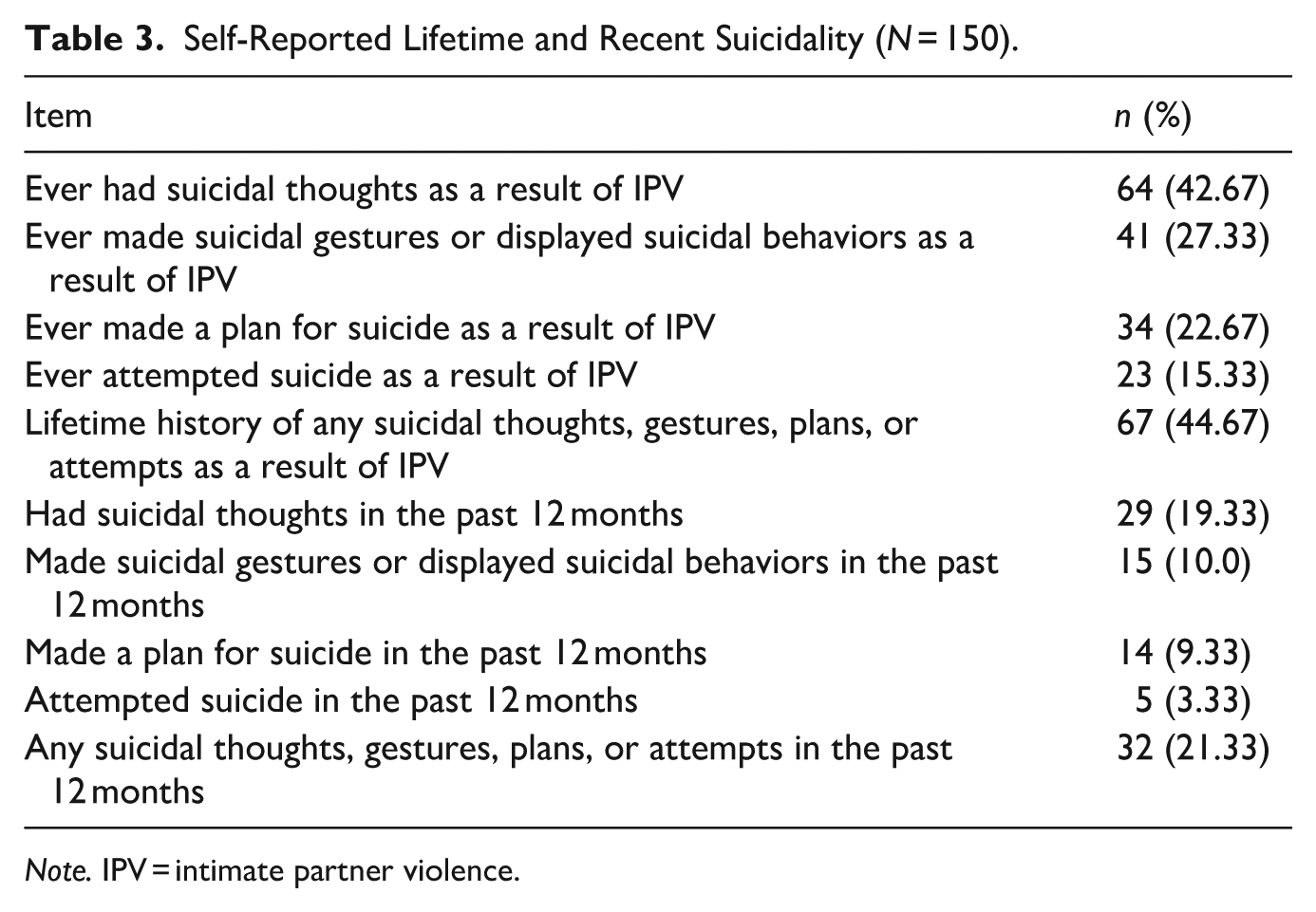
Note. IPV = intimate partner violence.
Women’s experiences of IPV were measured through the Index of Spouse Abuse (ISA; Hudson & McIntosh, 1981). The ISA is a 30-item self-report scale that measures 11 forms of physical abuse (ISA-P) and 19 forms of nonphysical abuse (ISA-NP). Women rated how frequently each item occurred during their relationship with their abuser using a 5-point scale that ranged from ‘never’ to ‘very frequently’. Physical violence items included: ‘He punched you with his fists, He threatened you with a weapon, He beat you so badly that you had to seek medical help, and, He made you perform sex acts that you did not enjoy or like’. Nonphysical violence items included: ‘He told you that you were ugly and unattractive, He became very angry if you disagreed with his point of view, He insulted or shamed you in front of others, and He felt that you should not work or go to school’. Items have varying weights, depending on the severity of the abuse, which is reflected in the scoring. Final scale scores may range from 0 to 100, with higher scores indicating a greater amount of abuse. The reliability coefficient for the sample was .79 for the ISA-P and .86 for the ISA-NP subscales.
The Women’s Experience with Battering scale (WEB; Smith et al., 1999) was used to measure the experiences or meanings women attached to their partner’s violence. Women rated the 10 items on the WEB using a 6-point scale from ‘agree strongly’ to ‘disagree strongly’ to indicate their general agreement with each statement as a description of their relationship. Items included: ‘He made you feel unsafe even in your own home, You tried not to rock the boat because you were afraid of what he might do, and He could scare you without laying a hand on you’. Total scores could range from 10 to 60, with higher scores indicating a greater presence of abuse. The WEB has good construct validity and accurately discriminates battered from non-battered women (Smith et al., 1999). The reliability coefficient for the sample was 0.90.
The short form of the Psychological Maltreatment of Women Inventory (PMWI; Tolman, 1999) was used to assess women’s experiences of psychological abuse. The dominance-isolation subscale (PMWI D/I) measures behaviors related to isolation from resources, demands for subservience, and rigid observances of traditional sex roles (e.g., monitored your time and made you account for your whereabouts; was jealous or suspicious of your friends; and tried to keep you from doing things to help yourself). The emotional-verbal subscale (PMWI E/V) measures behaviors related to verbal attacks, attempts to demean the partner, and withholding emotional resources (e.g., called you names; screamed and yelled at you; and treated you like an inferior). Women indicated how frequently they experienced each item during their relationship using a 5-point scale that ranged from ‘never’ to ‘very frequently’. Scores for each subscale could range from 7 to 35, with higher scores indicating more psychological abuse. The reliability coefficient for the sample was 0.86 for the dominance/isolation subscale and 0.87 for the emotional/verbal abuse subscale.
An adapted version of the 25-item Stalking Behavior Checklist (SBC; Coleman, 1997) was used to measure overt violent behaviors and harassing behaviors. The 32-item scale included in this study was adapted by the Nebraska Domestic Violence Sexual Assault Coalition and included the following seven additional items: (1) injured or killed a pet; (2) threatened violence to friends or family members; (3) threatened family members or friends; (4) electronic stalking (i.e., using computer, phone, electronic equipment); (5) attempted to get you in trouble or fired from a job by making false accusations; (6) attempted to have your children taken away from you by calling or contacting Child Protective Services (CPS) and making false report; and (7) attempted to contact the victim through friends/family members. This adapted scale captured additional stalking behaviors that are known to be used by people who use IPV but were not included in the original scale. Participants were asked to focus on unwanted contact by their abusive partner in the past 6 months and rate each item on a 6-point scale from ‘never’ to ‘once a day or more’. The two subscales were averaged and possible scores on each ranged from 1 to 5. The reliability coefficient for the sample was 0.84 for the overt violent behaviors subscale was 0.84 and 0.87 for the harassing behaviors subscale.
Child Maltreatment
Items from the Comprehensive Child Maltreatment Scale (Higgins & McCabe, 2001) and the Children’s Exposure to Domestic Violence Scale (Edleson et al., 2008) were used to assess retrospective reports of childhood experiences of abuse and neglect before age 18 (sexual abuse, physical abuse, psychological maltreatment, neglect, and witnessing family violence). Because the occurrence of any child maltreatment was of interest in this study rather than the type or frequency of child maltreatment, a dichotomous variable (yes or no) was used to capture each respondent’s history of childhood maltreatment.
Suicidality
Project-designed items were used to assess women’s lifetime and recent history of suicidal ideation, gestures, plans, and attempts. During the interview, women responded either ‘yes’ or ‘no’ to four items that asked if they ever had suicidal thoughts, ever made suicidal gestures or displayed suicidal behaviors (e.g., cutting, taking pills), ever made a plan for how they might attempt suicide, or ever attempted suicide ‘as a result of any abuse you experienced from your most recent partner or any other adult intimate partner’. Following each affirmative response, women were asked if the thoughts, gestures, plan, or attempt occurred in the past 12 months. Women responded either ‘yes’ or ‘no’ to these items.
Women who reported a history of child maltreatment were asked four questions about whether they had any suicidal thoughts, behaviors, plans, or attempts ‘as a result of any abuse or neglect you experienced during your childhood’. Women responded ‘yes’ or ‘no’ to each of the four questions.
Depressive Symptoms
Depressive symptoms were measured using the 20-item Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977). The CES-D captures the frequency of depressive symptomatology within the past 7 days. Items include ‘I felt I was just as good as other people’, ‘I felt that everything I did was an effort’, and ‘I had trouble keeping my mind on what I was doing’. Response options range from ‘rarely or none of the time’ to ‘most or all of the time’. Positive items were reverse coded, and all 20 items were summed. The total score could range from 0 to 60 with a higher score indicating greater levels of depressive symptoms. The CES-D has demonstrated high construct and concurrent validity when compared to clinical diagnostic criteria, as well as good internal consistency and test–retest reliability (Radloff, 1977). The reliability coefficient for the CES-D in this sample was .92.
Posttraumatic Stress Disorder
The Impact of Event Scale-Revised (IES-R; Weiss & Marmar, 1996) was used to measure subjective distress to traumatic events. The 22-item IES-R measures the level of symptomatic response to traumatic stressors in the last 7 days across three subscales: intrusion (8 items), avoidance (8 items), and hyperarousal (6 items). Items included ‘You were jumpy and easily startled’ and ‘You tried not to think about it’. Each item used a 5-point response option ranging from ‘not at all’ to ‘extremely’. Average scores were computed with possible ranges from 0 to 4. The IES-R had good reliability for all three subscales (reliability coefficients = 0.92, 0.84, and 0.89 for the intrusion, avoidance, and hyperarousal subscales, respectively).
Resilience
The Connor Davidson Resilience Scale (CD-RISC; Connor & Davidson, 2003) was used to measure women’s resilience. The CD-RISC is a 25-item, self-report scale that addresses psycho–social–spiritual aspects of resilience displayed in the last month (e.g., ‘I am able to adapt when changes occur’ and ‘I am not easily discouraged by failure’). Response options are based on a 4-point scale that ranges from ‘not true at all’ to ‘true nearly all the time’. Responses were summed to create a total score that could range from 0 to 100, with higher scores representing greater levels of resilience. The CD-RISC has been tested in the general population as well as clinical samples and has demonstrated sound psychometric properties (Connor & Davidson, 2003). The reliability coefficient for the CD-RISC in this sample was 0.93.
Support
The Interpersonal Support Evaluation List (Cohen & Hoberman, 1983; Cohen et al., 1985) is a 40-item scale that was used to measure women’s perceived availability of tangible assets support, appraisal support, self-esteem support, and belonging support. Tangible assets support captures the perceived availability of material aid; appraisal support is the perceived availability of someone to discuss issues of personal importance; self-esteem support is the perceived availability of others with whom one compares favorably; and belonging support is the perceived availability of others to interact with socially. All responses were given using a 4-point scale ranging from ‘definitely false’ to ‘definitely true’. Scores on each subscale could range from 0 to 30, with higher scores indicating greater levels of support. The measure has good reliability for all subscales in the sample, as reliability coefficients ranged from 0.85 (self-esteem support) to 0.91 (appraisal support).
Goal-Directed Thinking
The State Hope Scale (Snyder et al., 1996) is a 6-item measure of ongoing goal-directed thinking with an 8-point response scale ranging from ‘definitely false’ to ‘definitely true’. The total score is a sum of all six items, and two subscales are created to represent women’s agency (belief in self-capacity to initiate and sustain actions) and pathways (belief in self-capacity to generate routes) to reach their goals. The total score could range from 6 to 48, with each subscale score ranging from 3 to 24. Higher scores indicate greater degrees of goal-directed thinking. Reliabilities for the sample were acceptable, with alphas of 0.85 for the total measure, 0.82 for agency, and 0.72 for pathways.
Empowerment
The Personal Progress Scale-Revised (PPS-R; Johnson et al., 2005; Worell & Chandler, 1998) measured empowerment defined as the ability to access skills and resources to cope with current and future stress and trauma. The 26 items are rated on a 7-point scale based on the women’s perceptions of how true (‘almost never true’ to ‘almost always true’) each item is as it applies to her at the present time. The total score represents an average of all items, with a possible range of 1 to 7, with higher values indicating a greater sense of empowerment. The reliability coefficient for the PPS-R in this sample was 0.99.
Data Analysis Plan
Univariate analyses were performed to describe sociodemographic data for the sample, along with measures of IPV, child maltreatment, and their associated suicidality. Bivariate analyses focused on group differences in suicidality with respect to sociodemographic characteristics presented in the description of the sample (age, length of relationship, education level, race, history of child maltreatment, and geographic location), measures of IPV, and measures of well-being. Analyses were performed using three groups for comparison: no suicidality, lifetime-only suicidality, and both past year and lifetime suicidality. One-way analysis of variance (ANOVA) with post-hoc comparisons was used to examine group mean differences for continuous variables. Chi-square analyses were used with categorical variables. A p-value ≤ .05 was considered statistically significant.
Results
Over half of the sample reported no history of suicidality (n = 83; 55.33%) and 67 women (44.67%) reported any suicidality because of the IPV they experienced. Of these, 32 women (21.33%) reported suicidality in the past year and over their lifetime and 35 (23.33%) reported lifetime suicidality but not in the past year. Over their lifetime, 64 women (42.67%) in the sample reported suicidal thoughts because of the IPV they experienced. Over their lifetime, women also attributed making suicidal behaviors (n = 41; 27.33%), making a plan for suicide (n = 34; 22.67%), and attempting suicide (n = 23; 15.33%) to their experiences of IPV. Table 3 presents frequencies of women’s suicidality due to IPV over their lifetime and within the past year.
Exactly half (n = 75) of the women in the sample reported a history of child maltreatment. Of those, 44 (58.67%) reported attributed suicidal thoughts to the childhood abuse or neglect they experienced. Women also reported making suicidal behaviors (n = 37; 49.33%), making a plan for suicide (n = 30; 40%), and attempting suicide (n = 23; 30.67%) as a result of experiencing maltreatment during their childhood. Table 4 presents data on suicidality attributed to IPV and/or child maltreatment.
Self-Reported Suicidality as a Result of IPV and/or Child Maltreatment (N = 150).
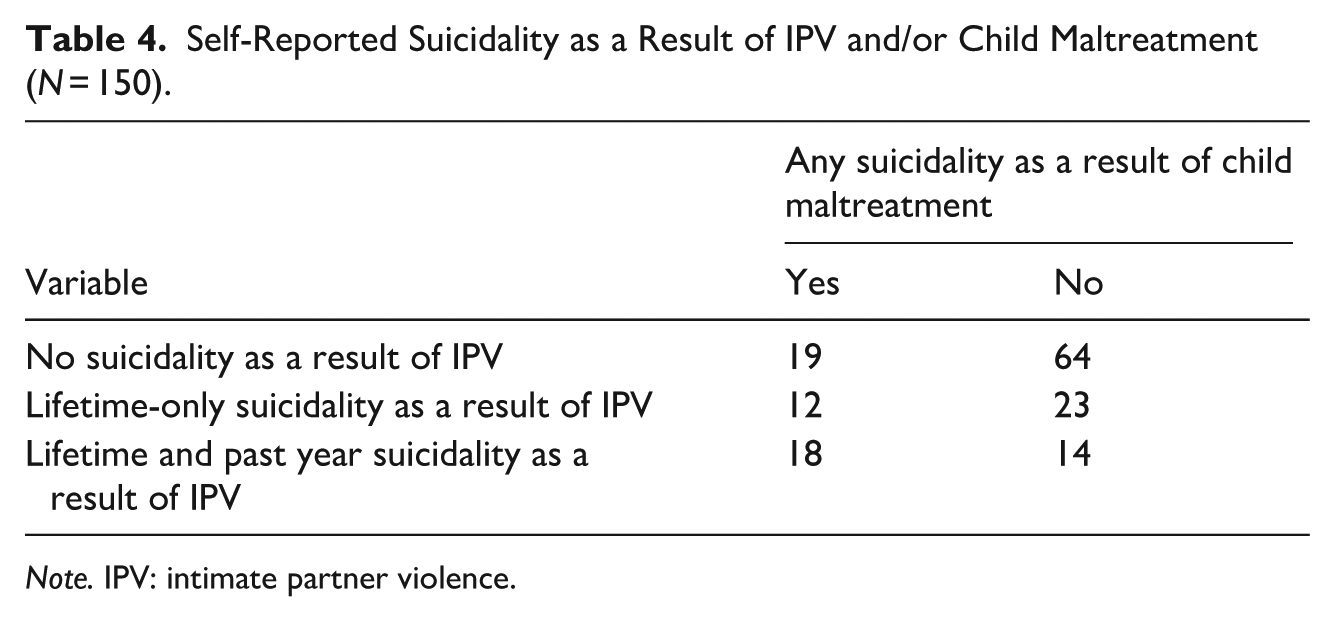
Note. IPV: intimate partner violence.
Measures of IPV Victimization and Suicidality
There were no group differences in women’s reports of suicidality (lifetime-only vs. past year/lifetime vs. none) with respect to any sociodemographic characteristics. Women in the sample reported high levels of physical IPV, psychological IPV, and stalking (see Table 5), and group differences among abuse-related variables were limited. A one-way ANOVA revealed a statistically significant difference in physical IPV between at least two groups (F[2, 149] = 3.40, p = .036). Tukey’s Honestly Significant Difference (HSD) test for multiple comparisons showed that the mean value of physical IPV was significantly different between women who reported both lifetime and past year suicidality and women who reported no suicidality (55.34 vs. 44.35, respectively; p = .027). There was no statistically significant difference between women who reported lifetime-only suicidality and women who reported no suicidality (p = .650). All other analyses indicated no statistically significant differences in types of IPV among the three groups.
Measures of IPV and Well-Being for Women Who Reported No, Lifetime-Only, or Past Year/Lifetime Suicidality.
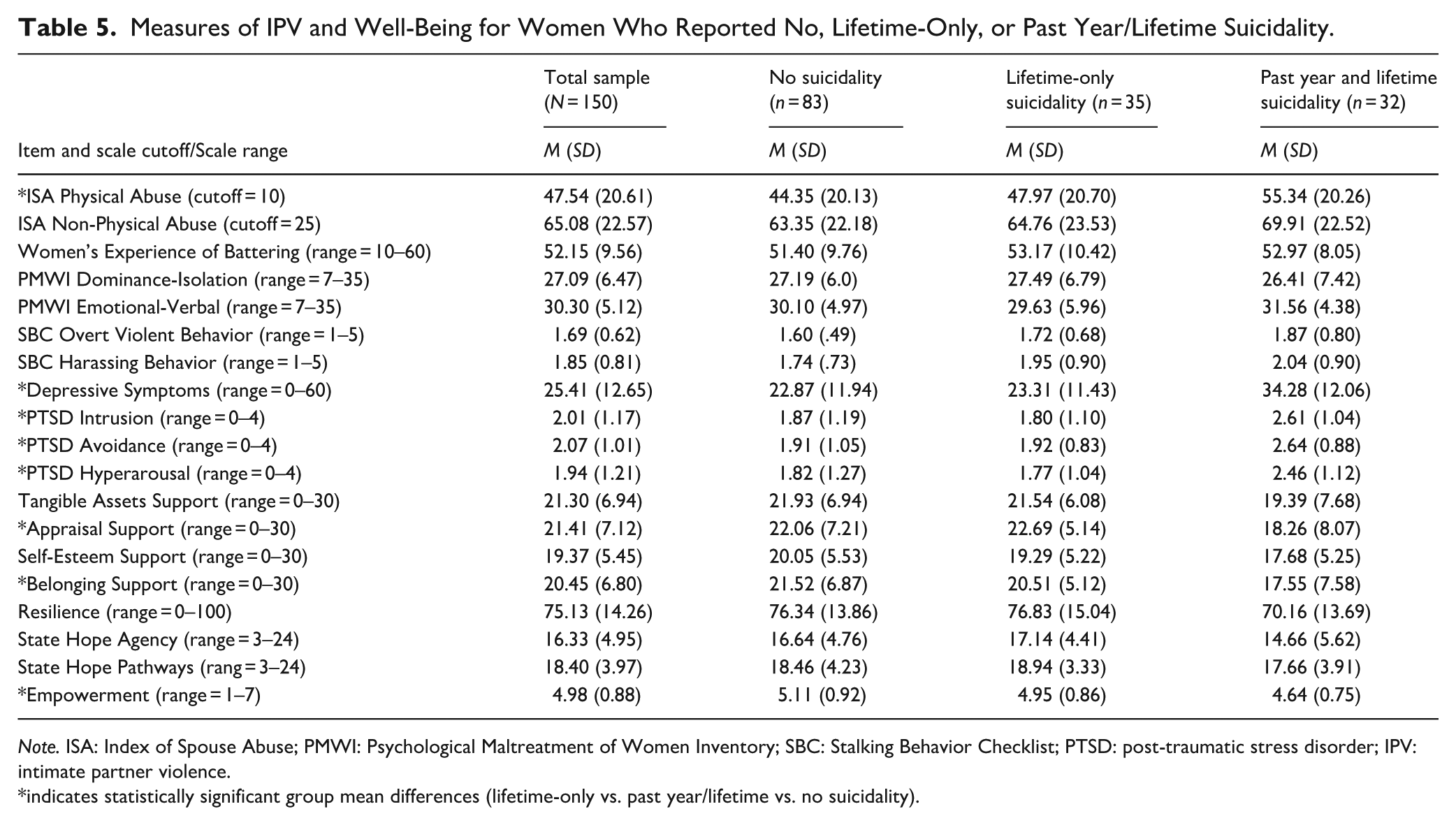
Note. ISA: Index of Spouse Abuse; PMWI: Psychological Maltreatment of Women Inventory; SBC: Stalking Behavior Checklist; PTSD: post-traumatic stress disorder; IPV: intimate partner violence.
indicates statistically significant group mean differences (lifetime-only vs. past year/lifetime vs. no suicidality).
Measures of Well-Being and Suicidality
Several group differences in suicidality emerged when examining well-being among the three groups (lifetime-only vs. past year/lifetime vs. none). A one-way ANOVA revealed a statistically significant difference in depressive symptoms between at least two groups (F[2, 149] = 11.42, p =< .001). Tukey’s HSD Test for multiple comparisons indicated that the mean value of depressive symptoms was significantly different between women who reported lifetime-only suicidality and women who reported no suicidality (p =< .001), and between women who reported both past year and lifetime suicidality and women who reported no suicidality (p =< .001).
With respect to PTSD, statistically significant group mean differences were found for all three subscales (F[2, 149] = 5.66, p = .004 for intrusion; F[2, 149] = 7.18, p = .001 for avoidance; F[2, 149] = 3.86, p = .023 for hyperarousal). The mean value for intrusion was significantly different between women who reported lifetime-only suicidality and women who reported no suicidality (p = .012), and between women who reported both lifetime and past year suicidality and women who reported no suicidality (p = .006). The mean value for avoidance was significantly different between women who reported lifetime suicidality and women who reported no suicidality (p = .007), and between women who reported both lifetime and past year suicidality and women who reported no suicidality (p = .001). The mean value for hyperarousal was significantly different between women who reported lifetime suicidality and women who reported no suicidality (p = .049), and between women who reported both lifetime and past year suicidality and women who reported no suicidality (p = .028).
Some group differences were found for women’s interpersonal support. Statistically significant differences were found for appraisal support, (F[2, 147] = 4.11, p = .018, and belonging support, F[2, 149] = 4.01, p = .020). The mean value for appraisal support was significantly different between women who reported lifetime suicidality and women who reported no suicidality (p = .030), and between women who reported both lifetime and past year suicidality and women who reported no suicidality (p = .029). The mean value for belonging support was significantly different between women who reported both lifetime and past year suicidality and women who reported no suicidality (p = .015). There was no statistically significant difference between women who reported lifetime-only suicidality and women who reported no suicidality.
There was also a difference between at least two groups in women’s empowerment, F(2, 149) = 3.36, p = .037. The mean value of empowerment was significantly different between women who reported both lifetime and past year suicidality and women who reported no suicidality (p = .029). There was no significant difference between women who reported lifetime-only suicidality and women who reported no suicidality. There were statistically significant group differences for measures of resilience or goal-directed thinking.
Discussion
Despite the robust literature linking IPV and suicidality, women are not often asked if their suicidality is directly attributed to the violence they experienced. It is important that researchers attempt to provide a more in-depth understanding of the relationship between IPV and suicidality, including the types of abuse experienced and their relative timing (McLaughlin et al, 2012). The findings from this study document the prevalence of suicidality among a sample of women who experienced multiple forms of IPV (and some with a history of childhood maltreatment), and did so within a unique context because women were asked whether they had suicidal thoughts, made suicidal gestures, developed a plan for suicide, or attempted suicide as a result of the IPV they experienced. As such, this study makes an important measurement contribution to the literature on IPV, suicidality, and the relationship between IPV and suicidality.
All 150 women in this study experienced IPV and 67 (44.67%) attributed their suicidality to their experience of IPV. In addition, 75 of the women in the sample reported a history of child maltreatment, and 44 (58.67%) of these women reported suicidal thoughts as a result of the childhood abuse or neglect they experienced. A unique component of this study was the focus on measurement and the decision to assess women’s perspectives on suicidality because of IPV and child maltreatment. Measuring the association between victimization and suicidality in this way is unique and contributes to the literature on family violence. It is important to note, however, that suicidality is associated with many risk factors. Even though women in this study attributed their suicidal thoughts, plans, behaviors, and attempts ‘as a result of’ the violence they experienced, there are a myriad of risk factors for suicide and a causal connection between IPV and suicidality cannot be drawn from this data. Still, this study offers insight into measurement limitations among most studies focused on the overlap between IPV victimization and suicide and offers suggestions for gathering more nuanced data to connect these phenomena.
The study findings also make a conceptual contribution to the literature. By experiencing acute and chronic trauma, women who experience IPV and/or child maltreatment may have greater tolerance for pain, less fear of injury or death, and a lowered sense of belongingness or social alienation, which aligns within the interpersonal theory of suicide. This study’s finding that physical IPV was greater among women who reported both past year and lifetime suicidality compared to women who reported no suicidality also resonates with this theory, as people who experience physical violence over time may be more likely to experience the elevated tolerance for physical pain required to acquire the capability for suicide.
Study Limitations and Suggestions for Future Research
Despite the intentional efforts to connect IPV and suicide via innovative measurement, this study is also not without limitations. First, there are limitations to the data collection. All data in this study were self-reported, subject to recall bias, and represented one point in time. Some scholars have found a dose–response relationship between IPV and suicidality (see review by McLaughlin et al., 2012), which is not accounted for in this study. Although this study included assessments of different types of IPV and the frequency of IPV, it did not account for the persistence or desistence of suicidality over time. In addition, suicidality was measured using project-specific items that were not validated. Future research on this topic should better account for the frequency and duration of violence and engage in more nuanced investigation of how these aspects of victimization relate to the presence, stability, and change in suicidality to better understand the link between the IPV and suicidality and the temporal relationship between them. Although a goal of this study was to highlight the need to measure the overlap between IPV and suicidality through survey items and/or interview questions that more intentionally connect the two phenomena, only this direct relationship was of focus. Future research on the association between IPV and suicidality should include variables that may mediate or moderate the relationship between these two phenomena.
Second, the sample was limited in diversity of sociodemographic characteristics that relate to experiences of IPV and suicidality. Women in the study sample primarily identified as White and were in heterosexual relationships at the time of data collection. People who identify as lesbian, bisexual, transgender, and queer experience IPV at high rates, while also facing additional experiences of discrimination and oppression (Chen at al., 2020; Harden et al., 2022; Scheer & Poteat, 2021). Some scholars have reported the consequences of IPV within the context of a same-sex relationship to be somewhat different than the consequences of IPV for people in a heterosexual relationship (Gehring et al., 2017); and adults who are lesbian or bisexual report higher rates of suicidal thoughts and attempts relative to their heterosexual counterparts (Hottes et al., 2016; Salway et al., 2019). Women who identify as Black and Native American also face greater risk for femicide and greater barriers to help-seeking (Rosay, 2016; Waller et al., 2022). Women in the sample also reported low-income levels. Lower socioeconomic status has been identified as a risk factor for suicide deaths but not suicidal thoughts or attempts (see meta-analysis by Huang et al., 2017), and the women in this sample were required to have incomes at or below 125% to 200% of the federal poverty guidelines to access legal aid services. Income or other socioeconomic factors could influence the relationship between IPV and suicidality among women in this sample in ways that may be different from other survivors of violence. Future research efforts on the overlap between IPV victimization and suicidality should include a more diverse sample to further explicate the link between these two public health crises.
Study Implications
The objective of this study was to bring awareness to current measurement limitations in the overlap between IPV victimization and suicidality and offer some suggestions for improvement. Despite the robust literature on suicidality among survivors of family violence, the overlap between IPV victimization and suicidality has not been established through the nuanced data collection efforts that are arguably required to explore this intricate connection. Few researchers have directly connected suicidality with IPV by asking women whether and how their suicidal thoughts, behaviors, or attempts were directly related to the violence they endured. In this study, women were asked if their suicidal thoughts, plans, behaviors, and attempts were due to the violence they experienced. Findings from this study demonstrate a clear overlap between victimization and suicidality, which has implications for IPV prevention efforts and highlights the need to tailor suicide prevention efforts for survivors of IPV.
Most concretely, the study findings suggest that interventions designed to reduce the occurrence, frequency, and chronicity of IPV could have the potential to directly reduce suicidality. Efforts to engage women in increasing their help-seeking strategies aimed to stop their victimization have the potential to improve their safety and well-being, which may reduce their risk of suicidality. Related, suicide interventions in the context of IPV must address women’s wider social and economic environments. Interventions with women who have recent and lifetime histories of IPV should include an evaluation of coping strategies, social supports, economic stability, and various other internal and external resources related to safety and well-being. As shown in this study, suicidality was associated with greater symptoms of depression and PTSD and lower levels of interpersonal support and feelings of empowerment. In addition, intervention efforts should pay attention to points in time that are critical to heightened risks for both IPV and suicide. For example, relationship separation is a prominent factor contributing to an increased risk for IPV (Rezey, 2020) and increased suicidality (Batterham et al., 2014; see also review by Kazan et al., 2016). Women who separate from an abusive partner are at a greater risk of intimate partner homicide (Kafonek et al., 2022), and they may also have an increased risk of self-harm. Intervention efforts must focus on utilizing formal and informal strategies to enhance women’s safety for both risk of re-victimization and risk of self-harm.
Finally, suicide prevention efforts are dependent on knowing the precipitating factors for suicidality (Brown & Seals, 2019), which directly speaks to how suicidality is experienced conjunction with IPV victimization. We know that IPV is associated with suicidality for many individuals, yet it remains unclear how often IPV precipitates suicide mortality. Inquiries among Domestic Violence Fatality Review teams and research using the National Violent Death Reporting System (NVDRS) are two examples of data-focused approaches to exploring IPV and suicide in tandem. The findings from an exploratory study in Washington state revealed that 13% of women who died by suicide in 1 year had a court-documented history of IPV victimization (Starr & Fawcett, 2006). Using NVDRS data from 43 states, Kafka et al. (2024) conservatively estimated that IPV was a precipitating factor for 7.1% or more of suicides in the United States; however, the researchers could not reliably record whether the person who died by suicide had previously experienced IPV or been the person who used violence against an intimate partner. Although these efforts cannot explain whether or how experiencing IPV contributed to women’s deaths, they do further document that there is an overlap between IPV victimization and suicide for many women. The findings from this study and the work of other scholars demonstrate that the overlap between IPV and suicidality needs to be better assessed and more meaningfully documented in all data collection efforts.
Footnotes
Acknowledgements
The author would like to thank all the staff and AmeriCorps workers at Iowa Legal Aid and the interviewers for their support and contributions to this project. The author would also like to thank all the women who participated in the project and shared their experiences; their strength and courage are remarkable.
Funding
The author disclosed receipt of the following financial support for the research and/or authorship of this article: This project was supported by Award No. 2010-WG-BX-0009, awarded by the National Institute of Justice, Office of Justice Programs, U.S. Department of Justice. The opinions, findings, and conclusions or recommendations expressed in this publication are those of the authors and do not necessarily reflect those of the Department of Justice.
Declaration of Conflicting Interests
The author declared no potential conflicts of interests with respect to the authorship and/or publication of this article.