
Abstract
Children’s exposure to violence is a significant public health issue associated with heightened trauma symptoms. Children exposed to multiple types of violence may develop beliefs that there is something about them or their actions to blame for their experiences, which in turn increases distress. We examined how the number of violence exposures and self-blame related to trauma symptoms among children referred to the United States Navy’s Family Advocacy Program for family violence. Participants were recruited as part of a larger study on families reported to the Family Advocacy Program due to allegations of child physical abuse (48%), sexual abuse (20%), or intimate partner violence (32%). Children (N = 195) were 63% female and aged 7 to 17 years old (Mean age = 12.17). We investigated the relation between child self-reports of violence exposure and self-blame within 2 to 6 weeks of the referral and trauma symptoms reported by children and a non-offending caregiver 9 to 12 months later. The number of violence exposures (b = 2.93, p < .001) and self-blame (b = 1.22, p < .001) predicted higher levels of child-reported trauma symptoms. Self-blame mediated the association between the number of violence exposures and child-reported trauma symptoms, indirect effect = 0.70, 95% Confidence interval [0.18, 1.22]. These effects did not emerge for caregiver reports. Results highlight the importance of broad assessments of violence and self-blame among children referred for family violence.
Introduction
Children’s exposure to violence is a major public health concern, with more than 70% of children in North America experiencing violence in their lifetime (Cyr et al., 2013). Exposure to violence can involve child physical or sexual abuse, physical assault, intimate partner violence, or community violence (Finkelhor et al., 2015). Children exposed to one type of violence are nearly four times more likely to experience multiple types of violence (Chan et al., 2021). Exposure to any type of violence is associated with heightened trauma symptoms, including posttraumatic stress disorder, anxiety, and depression (Alisic et al., 2014; Vibhakar et al., 2019), and exposure to more types of violence substantially increases the risk of adjustment problems (Haahr-Pedersen et al., 2020). However, many children exposed to violence do not develop significant distress. This variability has stimulated a large body of research attempting to understand the range in outcomes (Spearman et al., 2023; Valle & Silovsky, 2002), some of which has highlighted the importance of understanding children’s appraisals of violence.
In response to stressful events, children form appraisals to try to explain why the event occurred (Weiner, 1985). Consistent with attribution theory, in the context of abuse and violence, both the transactional model and the traumagenic dynamic framework suggest that specific kinds of appraisals can contribute to subsequent adjustment problems (Finkelhor & Browne, 1985; Spaccarelli, 1994). Self-blame appraisals have been identified as particularly important following exposure to violence (Aaron, 2012; Celano, 1992) and are defined as attributing the cause of the violence to oneself or one’s actions or accepting fault for the violence occurring. In some conceptual models, self-blame is viewed as an attributional process that grants a sense of control or agency over violent experiences (Janoff-Bulman, 1979) or provides cautionary lessons on how to avoid future violence (Mills, 2005); more often, however, self-blame appraisals are conceptualized as harmful, negative beliefs about the self (Aaron, 2012). These maladaptive cognitions are posited to foster the development of a negative self-image, low self-esteem, and/or guilt that can contribute to higher levels of trauma symptoms. Indeed, greater self-blame has been robustly associated with higher levels of trauma symptoms among children exposed to violence (Alix et al., 2020; De Champlain et al., 2023; Jouriles et al., 2025; Tanzer et al., 2021). However, the vast majority of these studies only consider cross-sectional associations and focus on children’s exposure to a single type of violence (Evans et al., 2022; Valle & Silovsky, 2002).
Few studies consider how children’s self-blame appraisals may contribute to adjustment problems in the context of multiple types of violence exposures over time. Exposure to multiple types of violence may foster children’s beliefs that there is something about them or their actions that causes them to continue to experience violence. Recent findings support this, suggesting that experiencing multiple types of violence, including exposure to intimate partner violence, sexual abuse, and physical abuse, is associated with higher levels of self-blame appraisals (Klebanov et al., 2023; Rancher et al., 2024). It seems plausible that, in turn, this heightened self-blame contributes to the development of trauma symptoms (Finkelhor & Browne, 1985; Spaccarelli, 1994). In other words, self-blame appraisals may partially explain the association between children’s exposure to violence and their subsequent trauma symptoms. Numerous studies have found that self-blame appraisals mediate the association between children’s exposure to a single type of violence and child adjustment (Evans et al., 2022; Rhoades, 2008). It seems plausible this pattern would similarly emerge following exposure to multiple types of violence.
On the other hand, it may be that exposure to violence does not have a dose-response on self-blame appraisals. Aggregating a total number of heterogeneous types of violence experiences may erroneously suggest that these experiences are all equal (Negriff, 2020). Experiencing even a single type of violence can be detrimental to child’s adjustment. For example, severe, chronic sexual abuse can have a significant impact on the development of self-blame appraisals and trauma symptoms (Alix et al., 2020; De Champlain et al., 2023). Children who experience multiple types of violence may also develop psychological numbing or habituation to the experience of victimization (Tarabah et al., 2016), which may attenuate the effect of self-blame appraisals as a mediator of adjustment problems. Ultimately, it is unknown whether the findings that self-blame can mediate the association between experiences of violence and child adjustment generalize to children who have experienced multiple types of violence.
It also may be important to consider whether the relation between exposure to violence and self-blame differs for boys and girls. For instance, beliefs around masculinity and gender role socialization may cause boys to experience higher self-blame if they believe that they were unable to protect themselves or did not do enough to stop the violence (De Champlain et al., 2023). On the other hand, girls tend to develop more self-conscious criticisms and negative self-evaluations, which may in turn, increase their vulnerability to developing beliefs that they are responsible or at fault for the violence (Hards et al., 2020). In literature examining differences in self-blame across boys and girls exposed to violence, conflicting findings emerge. Some have found boys report higher self-blame (Grych et al., 2000; Rancher et al., 2024; Schacter & Juvonen, 2017); some have found girls report higher self-blame (Miller et al., 2014; Ullman & Filipas, 2005); and some have found no difference (Jouriles et al., 2025; Quas et al., 2003; Tanzer et al., 2021). Ultimately, more research is needed to see if experiencing multiple types of violence may relate to self-blame differently for boys and girls; such a finding has important clinical implications for directing interventions that address social experiences.
Current Study
The present study provides a novel examination of how exposure to violence and self-blame appraisals relate to trauma symptoms among children referred to the United States Navy’s Family Advocacy Program due to allegations of family violence. Military families often experience unique stressors, including relocations, separations, and elevated rates of parental trauma exposure, all of which may increase family stress and, in turn, children’s vulnerability to violence exposure (Blamey et al., 2019). Military families are also provided with resources, including employment, health care, subsidized housing, and counseling services that can mitigate many daily stressors (Leskin et al., 2025). Understanding the links between violence exposure, self-blame, and trauma symptoms has important implications for supporting the well-being of military families. In contrast to much of the existing cross-sectional literature, the current study uses longitudinal data to examine self-blame appraisals reported within 2 to 6 weeks of the violence referral (T1) and trauma symptoms reported at a follow-up assessment 9 to 12 months later (T2). Longitudinal data is critical to establishing temporal relations between variables. We also examined trauma symptoms reported by both children and a non-offending caregiver. There is evidence that parent and child report of child adjustment rarely converges (De Los Reyes et al., 2015). Children have different insight into their emotions, experiences of distress, and the cognitive components of symptoms than their parents – highlighting the benefits to considering multi-reporter ratings of adjustment (see De Los Reyes & Kazdin, 2005, for discussion).
First, we examined the associations between the number of violence exposures, self-blame appraisals at T1, and trauma symptoms at T2. Consistent with the transactional model and traumagenic dynamic framework, we hypothesized that (H1) the number of violence exposures would be positively associated with self-blame appraisals, that (H2) the number of violence exposures would be positively associated with trauma symptoms, and that (H3) self-blame appraisals would be positively associated with trauma symptoms.
Second, we examined whether self-blame appraisals partially explain the association between violence exposure and trauma symptoms. We hypothesized (H4) that greater self-blame at T1 would mediate the association between the number of violence exposures (that occurred pre-T1) and trauma symptoms reported at T2 (Figure 1). Finally, we explored whether the hypothesized mediation model differed between boys and girls, that is, we explored whether child gender moderated the association between the number of violence exposures and self-blame. Given the contradictory findings on self-blame among boys and girls, we made no directional hypothesis for this effect. As children who have been exposed to violence are at greater risk for exposure to additional violence, we controlled for new violence exposures between T1 and T2 in our analyses. Previous research also suggests that children exposed to multiple types of violence are disproportionately older (Finkelhor et al., 2015), as they may have had more opportunities to experience violence; therefore, we also controlled for child age.
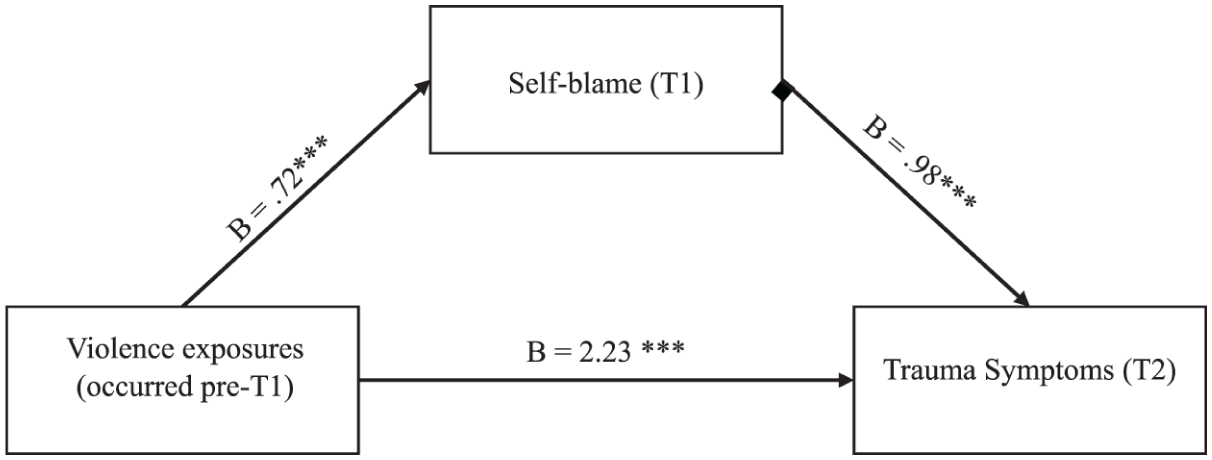
Mediation model predicting child report of trauma symptoms.
Methods
Participants and Procedures
Participants were recruited as part of a larger study on families reported to the United States Navy’s Family Advocacy Program due to allegations of child physical abuse (48%), sexual abuse (20%), or intimate partner violence (32%). The Family Advocacy Program is analogous to civilian Child Protective Services and provides support for families of military personnel who are suspected of having experienced maltreatment or violence. For the original study, eligibility criteria included two adults and a child who had been cohabitating for at least 6 months, one adult was an active Navy service member, and the family was referred for suspected child abuse (physical or sexual) or intimate partner violence. Due to the volume of referrals, members of the research team randomly selected families referred for child physical abuse or intimate partner violence. All families referred for child sexual abuse were contacted to participate. The Institutional Review Boards at the University of New Hampshire, Wellesley College, and the Medical University of South Carolina approved all study procedures. Adult caregivers provided consent, and children provided assent. Children aged 7 years and older completed self-report assessments. Trained members of the research team, independent of the Family Advocacy Program, conducted the semi-structured interviews. All families had access to mental health services as part of the Family Advocacy Program.
Of the 530 families included in the larger study, 285 (54%) had children old enough to complete the child assessment (i.e. >7 years old). Among these eligible children, approximately 70% (195) participated. There were no differences in child age, gender, or race in those who completed the T1 assessment (195), compared to those children who did not participate (90), ps > .05. Families referred for intimate partner violence were less likely to have a child complete the T1 assessment, p = .013. The final sample at the T1 assessment included 195 children aged 7 to 17 years old (M = 12.17, Standard deviation [SD] = 3.11). Children reported their gender was either female (63%) or male (37%). Most children identified their race as White (52%); with 30% reporting African American, 4% Filipino, 2% Asian American, 3% Hispanic/Latino, and 9% Biracial.
The T1 assessment took place within 2 to 6 weeks of the referral to the Family Advocacy Program. Of the N = 195 families who completed the T1 assessment, 70% (136) completed the T2 follow-up assessment 9 to 12 months later. There was no difference in child age, gender, race, the referring incident, number of violence exposures, or self-blame at T1, between those who completed both assessments compared to those who only completed the T1 assessment, ps > .05.
Measures
Exposure to Violence (T1 and T2)
Children completed a semi-structured interview used in the National Survey of Adolescents on their violence exposure (Kilpatrick et al., 2003). Children were asked multiple questions about each type of violence, including sexual abuse (7 items), physical abuse (7 items), physical assault (5 items), witnessing community violence (6 items), and exposure to domestic violence (7 items). At T1, children were asked whether they had ever experienced each type of violence (e.g. “Has any parent ever spanked or hit you so hard it caused bad marks, bruises, cuts, or welts on you”) on a dichotomous scale (0 = no, 1 = yes). Responses were aggregated and coded dichotomously for each type of violence (e.g. 0 = no history of physical abuse, 1 = yes, physical abuse). Items were summed to create a total number of violence exposures score. Detailed description of the survey development and measurement properties can be found in previous methodological reports (Kilpatrick & Saunders, 2000).
At the follow-up assessment (T2), children completed the same semi-structured interview but were asked whether each item had occurred since the first assessment. Responses were aggregated to create a dichotomous score for new violence exposure: 0 = no, 1 = yes.
Self-Blame Appraisals (T1)
Children completed the 4-item Personal Attributions for Negative Events subscale of the Children’s Attributions and Perceptions Scale (CAPS; Mannarino et al., 1994). Responses to items (e.g. “If something bad happens, are you usually responsible (is it your fault)?”) are made on a 5-point scale (1 = neve to 5 = always) and summed to create a total score. Self-blame appraisals measured on the CAPS have been positively correlated with adjustment problems (Mannarino & Cohen, 1996). In the current sample, the coefficient alpha was .78.
Trauma Symptoms (T2)
Caregivers completed the internalizing symptoms subscale of the Child Behavior Checklist (CBCL; Achenbach, 2000). Caregivers reported on their child’s symptoms (e.g. “can’t get mind off certain thoughts”) on a 3-point scale (0 = not true to 2 = very true or often true). Items were summed and converted into T-scores. Clinically significant levels of symptoms are indicated by T-scores > 64 (Pandolfi et al., 2012). CBCL internalizing symptom T-scores have been positively correlated with self-blame appraisals for interparental conflict (Grych et al., 2000). The CBCL has demonstrated robust internal consistency across several diverse samples with a coefficient alpha ranging from .63 to .97 (Achenbach & Rescorla, 2001).
Children reported on their trauma symptoms using the 10-item posttraumatic stress subscale from the Trauma Symptom Checklist for Children (TSCC; Briere, 1996). Responses to items (e.g. “Can’t stop thinking about something bad that happened to me”) are made on a 4-point scale (0 = never to 3 = almost all of the time). Items were summed and converted to T-scores. Clinically significant levels of symptoms are indicated by T-scores > 65 (Briere, 1996). Trauma symptoms measured on the TSCC have been positively correlated with self-blame appraisals (Rancher et al., 2022). In the current sample coefficient alpha was .89.
Data Analysis
Data were primarily missing due to attrition from the first assessment (T1) to the follow-up assessment (T2), with 2.1% of data missing on self-blame appraisals at T1. Exposure to violence at T1 and child age had complete data. We managed missing data using multiple imputation with R’s multivariate imputation by chained equation package (Zhang, 2016). Multiple imputation has fewer stringent assumptions and can manage item-level missingness across categorical and continuous variables (Enders, 2017). We created 20 imputed datasets using predictive mean matching for the numeric data and examined pooled results.
To test hypotheses 1 to 3, we conducted a series of linear regression models. For H1, we entered the number of violence exposures as the independent variable and self-blame at T1 as the dependent variable. For H2, the number of violence exposures was the independent variable, and trauma symptoms at T2 were the dependent variable. For H3, self-blame at T1 was the independent variable, and trauma symptoms at T2 were the dependent variable. We conducted separate models examining caregiver and child reports of trauma symptoms. Each model included new violence exposures between T1 and T2 (0 = no, 1 = yes) and child age as covariates.
To test our fourth hypothesis, we examined the indirect effect of the number of violence exposures (independent variable) on trauma symptoms (dependent variable) through self-blame (mediator) in a single model using R’s lavaan package with 95% confidence intervals and boot-strapping estimation (n = 500) (Rosseel, 2012). We conducted separate models for caregiver and child reports of trauma symptoms. We controlled for new violence exposures and child age. Finally, to explore whether child gender moderated the hypothesized associations, we entered the interaction between the number of violence exposures × child gender in the “α path” of the model predicting self-blame at T1. We examined the indirect effect separately for boys and girls. We interpreted significant effects as a 95% confidence interval that does not include zero.
We conducted a priori power analyses to determine the sample size needed to detect a small-to-medium sized effect, with alpha set at .05, and .80 power. For hypotheses 1 to 3, the program G*Power 3.1.9.7 indicated that a sample size of 138 was needed to detect a small-to-medium effect size (f2 = 0.09) (Kang, 2021). For hypothesis 4, simulation data indicated that with alpha set at .05, power at .80, and analyses using bias-corrected boot-strapping to assess for mediation, a sample size of 148 was needed to detect a small-to-medium indirect effect (α = .26 and β = .26) (Fritz & MacKinnon, 2007).
Results
Descriptive Statistics
Table 1 depicts the means, standard deviations, and correlations among study variables. At T1, children reported a range of 0 to 5 types of violence exposures, with nearly 70% reporting they had been exposed to two or more types of violence. Nearly half of children, 46%, reported they had a new violence exposure between T1 and T2. At T1, girls reported experiencing a higher number of violence exposures (M = 2.55, SD = 1.49) than boys (M = 1.77, SD = 1.14), t(193) = 3.86, p < .001, d = 0.57. There was no difference in self-blame appraisals across girls (M = 7.32, SD = 3.17) and boys (M = 7.05, SD = 3.26), t(193) = 0.56, p = .58. Results indicated that, at T2, caregivers reported 18% of children were exhibiting clinically significant trauma symptoms, and 10% of children reported clinically significant trauma symptoms.
Means, SDs, and Correlations Among Study Variables (N = 195).
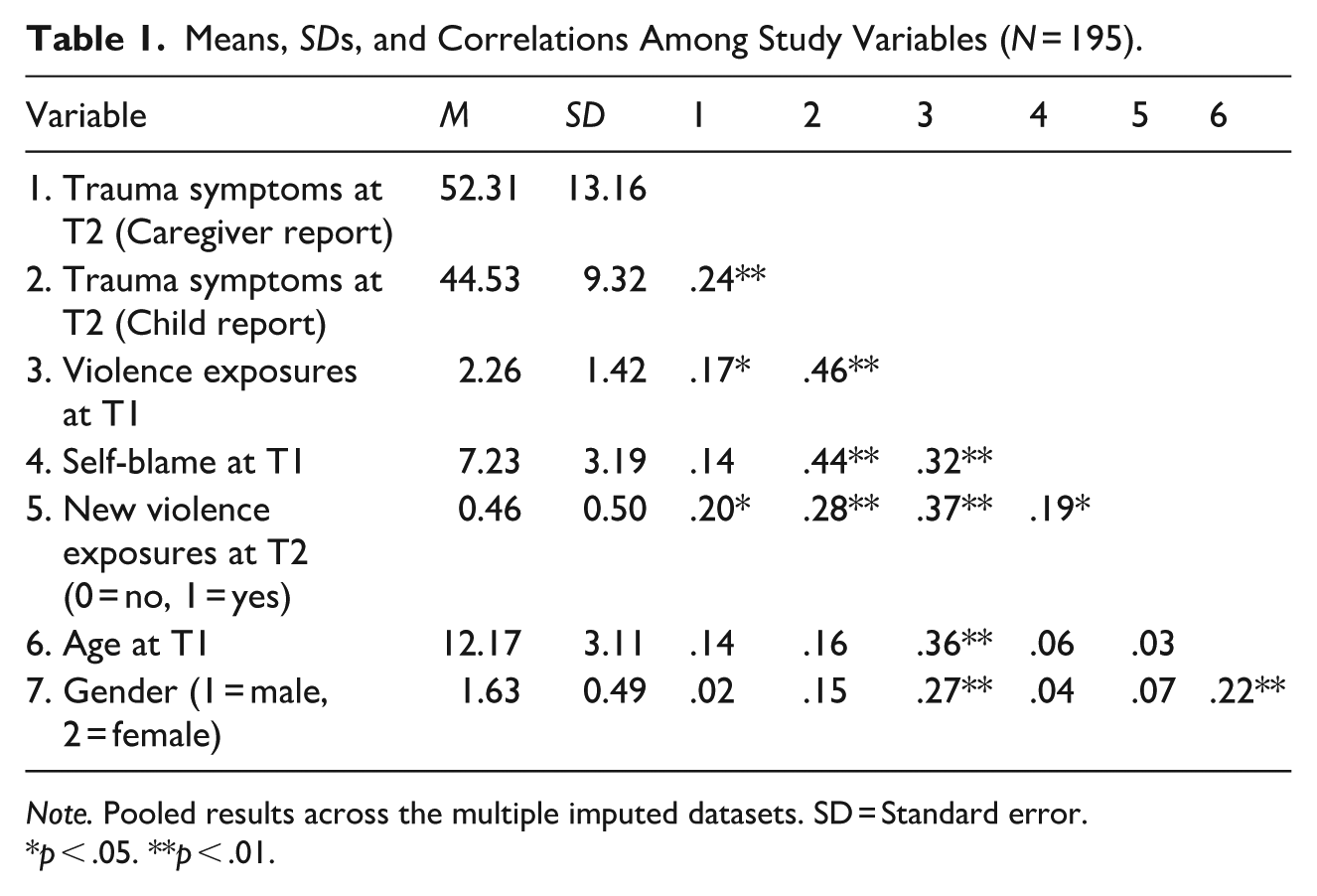
Note. Pooled results across the multiple imputed datasets. SD = Standard error.
p < .05. **p < .01.
Results of the Regression Analyses (Hypotheses 1–3)
Table 2 depicts the results of the regression analyses examining hypotheses 1 through 3. Consistent with the first hypothesis, the number of violence exposures was positively associated with self-blame appraisals after accounting for new violence exposures and child age. In partial support of the second hypothesis, the number of violence exposures was positively associated with child report of trauma symptoms at T2 but not associated with caregiver report of trauma symptoms at T2 after accounting for new violence exposures and child age. Similarly, partially consistent with the third hypothesis, self-blame at T1 was positively associated with child report of trauma symptoms at T2, but not associated with caregiver report of symptoms.
Regression Models Predicting Self-blame and Trauma Symptoms (N = 195).
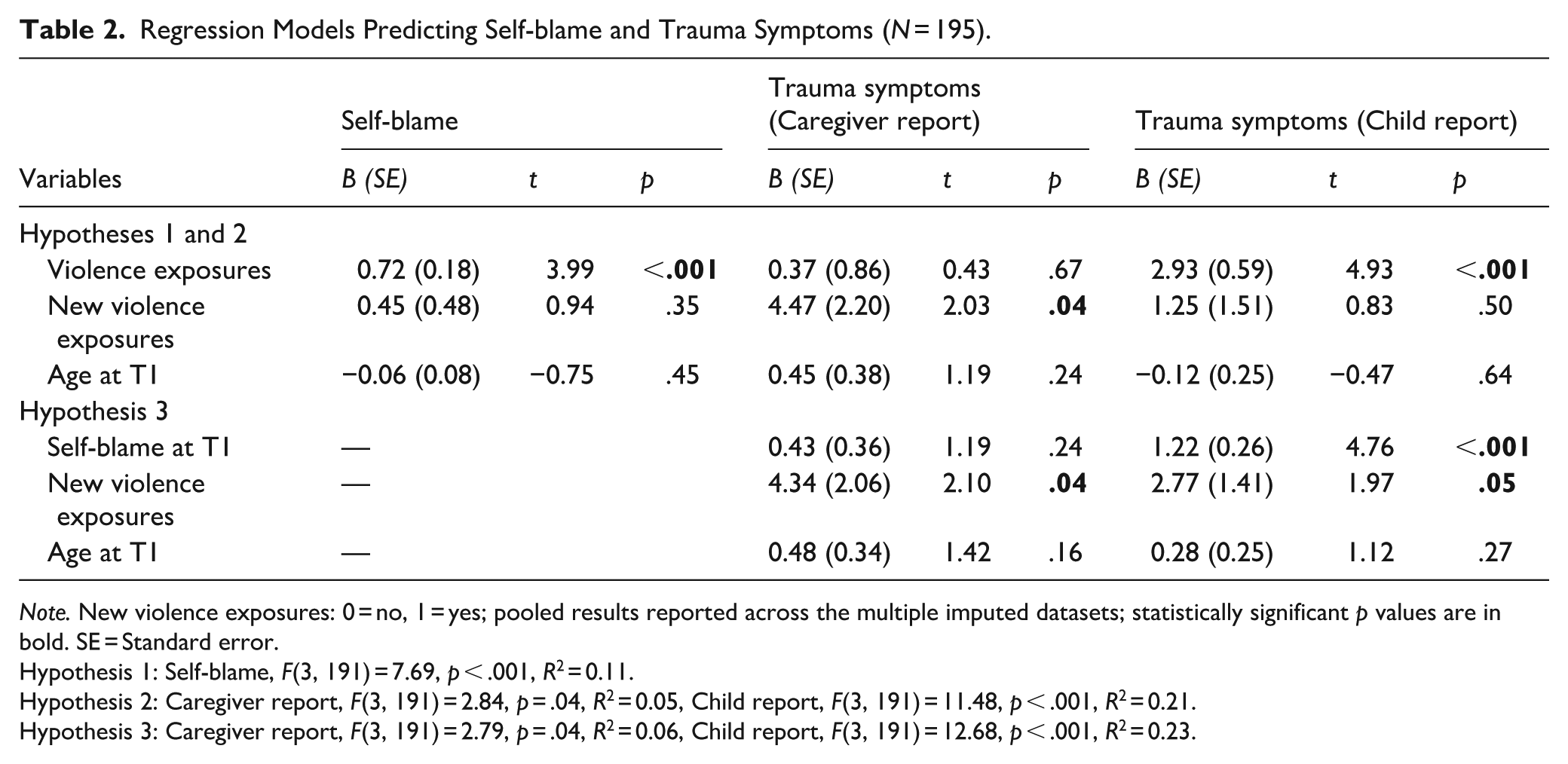
Note. New violence exposures: 0 = no, 1 = yes; pooled results reported across the multiple imputed datasets; statistically significant p values are in bold. SE = Standard error.
Hypothesis 1: Self-blame, F(3, 191) = 7.69, p < .001, R2 = 0.11.
Hypothesis 2: Caregiver report, F(3, 191) = 2.84, p = .04, R2 = 0.05, Child report, F(3, 191) = 11.48, p < .001, R2 = 0.21.
Hypothesis 3: Caregiver report, F(3, 191) = 2.79, p = .04, R2 = 0.06, Child report, F(3, 191) = 12.68, p < .001, R2 = 0.23.
Sensitivity analyses indicated that those with clinically significant levels of child report of trauma symptoms at T2 reported higher levels of self-blame at T1 (M = 8.92, SD = 3.45) compared to those without clinically significant trauma symptoms (M = 6.86, SD = 2.91), t(132) = 2.39, p = .009, d = 0.70. There was no difference in self-blame across those with and without clinically significant levels of caregiver report of trauma symptoms, p > .05.
Examining Self-Blame as a Mediator (Hypothesis 4)
Our fourth hypothesis was partially supported. We found that self-blame mediated the association between violence exposures and child report of trauma symptoms, indirect effect = 0.70, Standard error [SE] = 0.26, 95% CI [0.18, 1.22]. The results of this model are depicted in Figure 1. Self-blame did not mediate the association between violence exposures and caregiver report of trauma symptoms, indirect effect = 0.30, SE = 0.27, 95% CI [−0.23, 0.83].
Exploring Child Gender and Moderated Mediation
Results indicated that child gender moderated the association between the number of violence exposures and self-blame. This interaction is depicted in Figure 2. For girls, the number of violence exposures was positively associated with self-blame, b = .88, p < .001. For boys, the number of violence exposures was not associated with self-blame, b = .29, p = .37. In the mediation model, results indicated that self-blame mediated the association between violence exposures and child report of trauma symptoms for girls, indirect effect = 0.76, SE = .36, 95% CI [0.06, 1.46], but not for boys, indirect effect = 0.28, SE = 0.46, 95% CI [−0.61, 1.18]. Self-blame did not mediate the association between violence exposures and caregiver report of trauma symptoms for either girls, indirect effect = 0.30, SE = 0.33, 95% CI [−0.36, 0.96], or boys, indirect effect = 0.11, SE = 0.26, 95% CI [−0.39, 0.62].
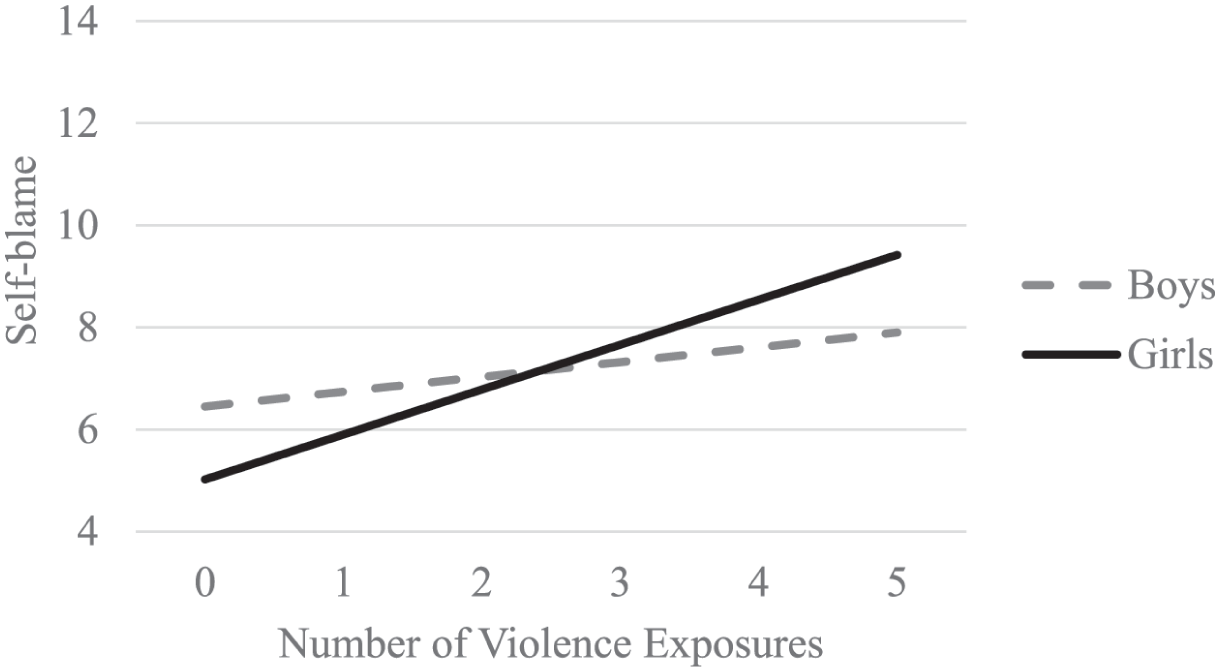
Relation between self-blame and violence exposure by gender.
Discussion
The current study examined how the number of violence exposures and self-blame appraisals relate to trauma symptoms among children referred to the United States Navy’s Family Advocacy Program due to allegations of family violence. We found evidence supporting our first hypothesis in that the number of violence exposures was positively associated with self-blame appraisals (r = 0.32); this finding emerged even after accounting for other possible sources of variance. This is consistent with previous research suggesting that exposure to multiple types of violence may lead to heightened self-blame appraisals (Klebanov et al., 2023; Rancher et al., 2024). Children exposed to multiple types of violence may be more susceptible to developing attributional beliefs that they are responsible for the violence occurring. Given the prevalence of children’s exposure to violence in general population studies (Cyr et al., 2013) and risk for repeated violence exposure (Chan et al., 2021), this has important implications for those working with children referred for family violence. These findings highlight the importance of assessing for violence exposure beyond the referring incident and the need for continued assessment.
It is also interesting to consider how rates of exposure to violence in this sample of military families compare to those in civilian populations. We observed that nearly 70% of children reported they had experienced two or more types of violence at the T1 assessment, with almost half of the sample (46%) experiencing new violence exposure in the subsequent 9 to 12 months. These prevalence rates align with prior findings from a sample of 5,058 civilian youth referred for services following trauma exposure that found nearly 89% reported experiencing two or more types of violence (Hodgdon et al., 2018). Further, work by Finkelhor and colleagues (2015) suggests that nearly 70% of civilian children report exposure to at least one potentially traumatic event in their lifetime and 50% report experiencing multiple types of violence. Overall, these findings are consistent with research suggesting children’s exposure to violence is equivalent across military and civilian populations (Rentz et al., 2006). Although military families face unique stressors such as frequent relocations and parental combat deployment (Campbell et al., 2011), they may experience violence at comparable rates to civilian families.
Our second and third hypotheses were partially supported, in that the number of violence exposures and self-blame appraisals were positively associated with child report of trauma symptoms, but not caregiver report of symptoms. We observed positive correlations between the number of violence exposures and both reports of trauma symptoms (see Table 1), but after accounting for child age and new violence exposures at T2, the number of violence exposures at T1 was no longer associated with caregiver reports of trauma symptoms. This pattern of results may be attributed to several factors. It may be that more recent exposures to violence, those new incidents that occurred between the T1 and T2 assessments, have a stronger effect on adjustment at T2. However, it may also be important to consider the reporter of symptoms. Consistent with research suggesting parent and child reports of adjustment rarely converge (De Los Reyes et al., 2015), child report and caregiver report of trauma symptoms were only moderately correlated (r = 0.24, see Table 1). It may be that children have different insights into their thinking patterns and emotional distress, while caregivers are referencing observed behaviors or estimating how they believe their child may be feeling. It is also worth considering the effect of common method variance; we may be observing stronger associations between self-blame appraisals and child reports of trauma symptoms, because they were both child self-report measures. Importantly, caregivers and children also completed measures on slightly different symptoms. The TSCC (child report) was developed to assess trauma symptoms; the CBCL Internalizing Scale (caregiver report) assesses a broader range of symptoms. Finally, demand characteristics may also be influencing caregiver reports of symptoms in this sample of military families referred to the equivalent of Child Protective Services. Caregivers may have felt pressured to respond in a certain manner, consciously or not, to avoid any consequences to their connected service member. Ultimately, these findings highlight the importance of considering multiple reporters of children’s adjustment problems among those referred for family violence.
Partially consistent with our fourth hypothesis, we found that self-blame appraisals mediated the association between the number of violence exposures and trauma symptoms. Our exploratory analyses found evidence for moderated mediation, suggesting this association may be particularly relevant for girls. These findings converge with ample research suggesting self-blame can mediate the association between exposure to violence and adjustment (Evans et al., 2022; Rhoades, 2008) but offer a nuanced examination of this pattern following exposure to multiple types of violence. As noted above, exposure to multiple types of violence may increase children’s vulnerability to blaming themselves for negative events, which, in turn, contributes to the development of heightened trauma symptoms. One implication of these findings is the clinical need to assess for self-blame appraisals among children referred for family violence. Such an assessment could help identify those children at higher risk for developing significant distress, facilitating timely referrals and triaging of supportive services to those most in need.
It is noteworthy that child gender moderated the association between the number of violence exposures and self-blame. Specifically, we observed that there was a positive association between the number of violence exposures and self-blame appraisals for girls, but not for boys. These findings converge with developmental literature suggesting girls are more vulnerable to developing self-critical beliefs than boys (Hards et al., 2020). In the present sample, we also observed that girls reported higher numbers of violence exposures (M = 2.55) than boys (M = 1.77). This is consistent with decades of research suggesting that girls experience higher rates of violence compared to boys (Kilpatrick et al., 2003). Thus, it may be that this is a difference in the range of experiences; the restricted range of boys’ exposure to violence may limit the association with self-blame. However, it is worth noting there was no difference in the mean levels of self-blame appraisals for girls (M = 7.32) and boys (M = 7.05). This finding is consistent with previous research that has found no differences in self-blame across gender (Jouriles et al., 2025; Quas et al., 2003; Tanzer et al., 2021) and suggests there may be some unmeasured variables driving boys’ self-blame appraisals. While outside the scope of the present study, it may be that beliefs around masculinity or characteristics of the violence may influence how boys’ exposure to violence relates to the development of self-blame appraisals.
Finally, it is interesting to consider that while the number of violence exposures in this sample was high, caregivers reported only 1 in 5 children had clinically significant levels of trauma symptoms, and only 1 in 10 children reported clinically significant symptoms. This is an important reminder that not all children exposed to violence develop significant adjustment problems, thus highlighting the need for researchers, clinicians, and child-serving agencies to broaden their assessment of child functioning to include factors – such as self-blame appraisals – that may indicate risk, beyond a strict definition of clinical levels of adjustment problems.
Several limitations of the present study should be acknowledged. First, data for this study were drawn from two time points, which can limit our conclusions about mediation. Although we can establish some temporal precedence – the number of violence exposures occurred prior to the T1 assessment, children reported on their current self-blame appraisals at T1, which occurred 9 to 12 months prior to the T2 assessment of trauma symptoms – this research would be further strengthened by additional longitudinal data. Second, there was notable attrition across the two assessments. Although we did not observe any differences between those who completed both assessments compared to those who only completed the T1 assessment, it may still be possible that the data were biased by unmeasured third variables.
It is also worth noting some limitations to the generalizability of our findings, given this sample was composed of military families. Because of their involvement with the United States Navy, these families were guaranteed to have at least one parent employed with a high school education, and likely had access to housing, income, and medical care. Furthermore, military families often have access to support services – including programs designed to address violence (Dodge et al., 2025; Leskin et al., 2025). As noted above, this affiliation and referral to the Family Advocacy Program may also have resulted in caregivers experiencing some demand characteristics, where consciously or not, they completed measures in a way that could minimize any consequences to the connected service member. Research on military families is important for policy and clinical intervention, still, this sample may have experienced different pressures and adversities than a civilian sample, and future research with more representative samples is warranted. Finally, our examination of children’s exposure to violence did not include an assessment of exposure to racism, racial trauma, or other race-related potentially traumatic events. In the absence of this measurement, we may be underreporting the experiences of violence in this population. This is an important area for future research.
In conclusion, among military families referred for family violence, we found that self-blame appraisals may partially explain the association between exposure to violence and trauma symptoms. This study replicates findings that both violence exposure and self-blame appraisals are positively associated with children’s trauma symptoms. In addition, we found this association may be particularly salient for girls. Nevertheless, our results should be interpreted with some caution, as we found this association only when examining the child report of trauma symptoms, not the caregiver report. This research highlights the importance of conducting broad assessments of violence exposure as well as examining self-blame appraisals among children referred for family violence to identify those most at risk of developing adjustment problems.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by U.S. Department of the Navy through contracts #N001040-01-C-N662 and #N00600-96-C3145.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Disclaimer
Points of view expressed in this document are those of the authors only and do not necessarily reflect the position or polices of the U.S. Department of the Navy.