
Abstract
Past research has established trauma and posttraumatic stress disorder (PTSD) as important risk factors for intimate partner violence (IPV) perpetration, focusing on hyperarousal and cognitive biases as explanatory mechanisms. The current study investigated whether experiential avoidance (EA), the tendency to avoid unwanted private experiences, helps explain the association between PTSD symptoms and IPV perpetration. Seventy-four men receiving IPV intervention services completed assessments of trauma exposure, PTSD symptoms, and IPV perpetration, and responded to hypothetical distressing relationship situations by rating: (1) anticipated experience of negative emotions, (2) motivation to avoid those emotional experiences, (3) the expectation that various aggressive and nonaggressive responses would reduce negative emotions, and (4) perceived likelihood of engaging in those responses. PTSD symptoms were associated with higher levels of dispositional EA, anticipation of negative emotions during distressing relationship situations, EA during difficult relationship situations, and anticipated reduction in negative emotion from engaging in abusive behaviors. EA significantly mediated the association between PTSD symptoms and emotional abuse perpetration, but not physical assault or sexual coercion. Partner abusive men experiencing higher PTSD symptoms report greater experiential avoidance of negative emotions during difficult relationship situations and higher anticipation that abusive and aggressive actions will repair their uncomfortable emotional state. The results highlight EA as an important treatment target for trauma-informed IPV intervention, particularly with respect to emotionally abusive behavior.
Introduction
An extensive body of research indicates that posttraumatic stress disorder (PTSD) is an important risk factor for perpetration of intimate partner violence (IPV). For example, a lifetime PTSD diagnosis is associated with a two-to-three-fold increased risk of perpetrating physical IPV (Hahn et al., 2015), and meta-analysis has found consistent associations between PTSD and perpetration of both physical and psychological relationship abuse with effects in the medium range of magnitude (Taft et al., 2011). Among men in treatment for IPV perpetration, PTSD symptoms are associated with more extensive IPV (Semiatin et al., 2017) and higher risk for continued violence after treatment (Creech et al., 2017; Miles-McLean et al., 2019).
The predominant explanations for this risk association focus on trauma-related alterations in social cognition, including heightened threat sensitivity and thematic concerns involving mistrust and a need for control (Chemtob et al, 1997; Taft, Murphy et al., 2016). Studies using the Social Information Processing (SIP) model (Crick & Dodge, 1994; Lemerise & Arsenio, 2000) have indicated that PTSD may increase risk for IPV by altering the encoding and interpretation of social cues as reflected in general mistrust of others, an inclination to perceive others as angry or hostile, a tendency to assume that others have negative intentions, and faster processing of shame information (LaMotte et al., 2016; Sippel & Marshall, 2011; Taft et al., 2008). Additionally, PTSD has been associated with a tendency to generate and select less socially competent and more harmful responses to relationship conflict situations (LaMotte et al., 2017).
Efforts to examine emotional factors in this process have found that the associations between posttraumatic cognitions and physical and psychological IPV were mediated by both anger misappraisal (the tendency to incorrectly identify non-angry speech audio as angry) and emotion dysregulation (Marshall et al., 2011). Surprisingly, however, research in this area has generally not included the role of emotions (cf., Marshall et al., 2011; Sippel & Marshall, 2011), This is notable because PTSD can have profound effects on the frequency and intensity of negative mood states (Gillihan et al., 2014), and because contemporary SIP models indicate that socially competent behavior often requires an ability to sustain interpersonal goals in the face of emotional arousal (Lemerise & Arsenio, 2000; Murphy, 2013).
Experiential avoidance (EA) is a way of relating to one’s emotions that may help further elucidate the associations among trauma exposures, PTSD symptoms, and IPV perpetration. EA refers to the unwillingness to stay in contact with present private experiences in order to avoid uncomfortable or distressing thoughts, emotions, memories, and physical sensations (S. C. Hayes et al., 1996). Whereas some forms of short-lived EA can be healthy, long-term reliance on EA as a coping mechanism can result in negative consequences (S. C. Hayes et al., 2012). Through the experience of trauma, individuals may learn that their changing internal bodily sensations in relation to their ongoing context (i.e., interoception) provide important and reliable indicators of danger, as this is generally the case during traumatic events. As a result, stopping or reversing those bodily changes as quickly as possible serves as a reliable indicator that the potential threat has been neutralized, and this becomes a generalized process across a range of different situations. This type of avoidance is believed to be a key mechanism through which PTSD symptoms are maintained and the affected person’s life begins to feel smaller and more restricted (Walser & Hayes, 2006).
Along these lines, when applied to challenging relationship situations, trauma and PTSD symptoms would promote a tendency to prioritize and focus on the goal of immediately altering/preventing emotional experience at the expense of the more pro-social considerations that are involved in maintaining healthy intimate relationships. This prioritization of EA may even influence one’s internal calculus of which strategies are likely to serve this goal most effectively. However, to date, the intricacies of this type of decision-making in the context of PTSD symptoms and difficult relationship situations has not been sufficiently examined.
Research has supported the connection between PTSD symptoms and a general strategy of EA. For example, PTSD is associated not only with avoidance of specific trauma-related cues and emotional triggers but also with a general tendency to avoid unwanted emotional experiences (Frewen et al., 2008). Among military veterans, PTSD was strongly associated with the frequency (r = .58) and intensity (r = .70) of effortful withholding of emotional expression (Roemer et al., 2001). In addition to the fear involved in re-experiencing symptoms, PTSD has been shown to be associated with an increase in a range of negative mood states, including anger, shame, guilt, and disgust (McLean & Foa, 2017). This tendency to avoid a wide range of uncomfortable emotions, even within contexts that are not directly related to the trauma, may prove very important when considering how experiential avoidance may increase risk for IPV perpetration among individuals with PTSD symptoms.
Consistent with the concept of EA, the anger avoidance model (AAM) maintains that the avoidance of anger and other closely associated emotions can result in maladaptive reactions such as aggression (Gardner & Moore, 2008). Although anger is a natural human emotion that is adaptive in many contexts, the perception of anger as intolerable, along with subsequent efforts to avoid it, can result in problematic behavioral manifestations. Studies indicate that people are more prone to use aggression when they believe it will help repair their negative mood state, supporting the theoretical assertion that avoiding the experience of anger is a motivating factor in human aggression (Bushman et al., 2001; Shorey et al., 2014). Moreover, a study examining PTSD symptoms, EA, and general aggression together found that both experiential avoidance and emotional inexpressivity independently mediated the relationship between PTSD symptoms and general aggression (Tull et al., 2007). Given that this past study examined general aggressive tendencies, and not relationship-specific patterns of abusive behavior, more research is needed to examine whether EA may mediate the association between PTSD and aggression in the context of intimate relationships.
The AAM is also supported by research that has assessed the connection between EA and IPV perpetration. For example, one study found that reporting high levels of both threat appraisal and repressed emotion was associated with 3.5 times greater odds of IPV perpetration among men (Umberson et al., 2002). Similarly, another study found that men’s EA was associated with both IPV perpetration and victimization (Reddy et al., 2011). Previous research has also shown EA to be associated at the bivariate level with psychological, physical, and sexual PV perpetration, and significantly predictive of psychological and sexual IPV when controlling for age, relationship satisfaction, and alcohol use (Shorey et al., 2014). Overall, these studies indicate that a greater tendency to avoid aversive internal experiences is associated with increased frequency of IPV perpetration. By extension, individuals who experience PTSD symptoms may be at increased risk for partner violence because they experience a strong drive to quickly reduce or avoid uncomfortable emotion states brought on by relationship challenges.
However, there are several important limitations of past research on EA and IPV. First, most prior studies in this area measured EA using the Acceptance and Action Questionnaire (AAQ; S. C. Hayes et al., 2004) and its revision (AAQ-II; Bond et al., 2011). This measure has been shown to have suboptimal discriminant validity with measures of neuroticism and negative affect, and suboptimal convergent validity with other constructs at the foundation of third-wave behavior therapies, such as dialectical behavior therapy, and acceptance and commitment therapy (ACT; Rochefort et al., 2018). Additionally, all reviewed studies on this topic have relied on self-report questionnaires of general EA. Although past research has indicated that anticipated change in emotion, rather than simply current emotional state, guides behavior (Bushman et al., 2001; DeWall et al., 2016), prior studies have not assessed anticipated change in emotions from engaging in aggression/abuse behaviors in an intimate relationship context. Finally, our literature review uncovered no prior studies that have examined EA as a mediating variable in the association between PTSD symptoms and IPV perpetration.
The current study aims to advance knowledge in this area by (1) using a more comprehensive self-report assessment of general EA, the Multidimensional Experiential Avoidance Questionnaire (MEAQ; Gámez et al., 2011); (2) assessing EA within the context of situations that are directly relevant to intimate relationship discord and IPV perpetration; (3) evaluating anticipated change in emotion from aggression/abuse perpetration in an intimate relationship context in addition to current emotional state, and (4) examining EA as a mediating variable in the associations between PTSD symptoms and IPV perpetration. The study was designed to test the following hypotheses:
Higher levels of lifetime trauma exposure and higher PTSD symptoms will be associated at the bivariate level with higher levels of anticipated negative emotion states in response to distressing hypothetical relationship scenarios.
Higher levels of lifetime trauma exposure and higher PTSD symptoms will be associated at the bivariate level with greater EA, assessed both via a trait measure and via avoidance-related responses to hypothetical relationship scenarios.
Participants will show a general tendency to rate aggressive/abusive responses to challenging relationship scenarios as more likely to reduce negative emotions, compared with nonaggressive/nonabusive responses.
EA, assessed both via a trait measure and via avoidance-related responses to hypothetical relationship scenarios, will mediate the relationship between PTSD symptoms and IPV perpetration, including physical assault, emotional abuse, and sexual coercion.
Methods
Participants
Participants were 74 men enrolled in the relationship abuse intervention program at House of Ruth, Maryland. Of 116 individuals who indicated initial interest in the study, 22 could not be reached to schedule a study appointment, 4 were no longer interested in participating, 3 could not be scheduled, and 13 failed to attend or reschedule their research visit. Table 1 displays sample background characteristics.
Sample Demographic Characteristics.
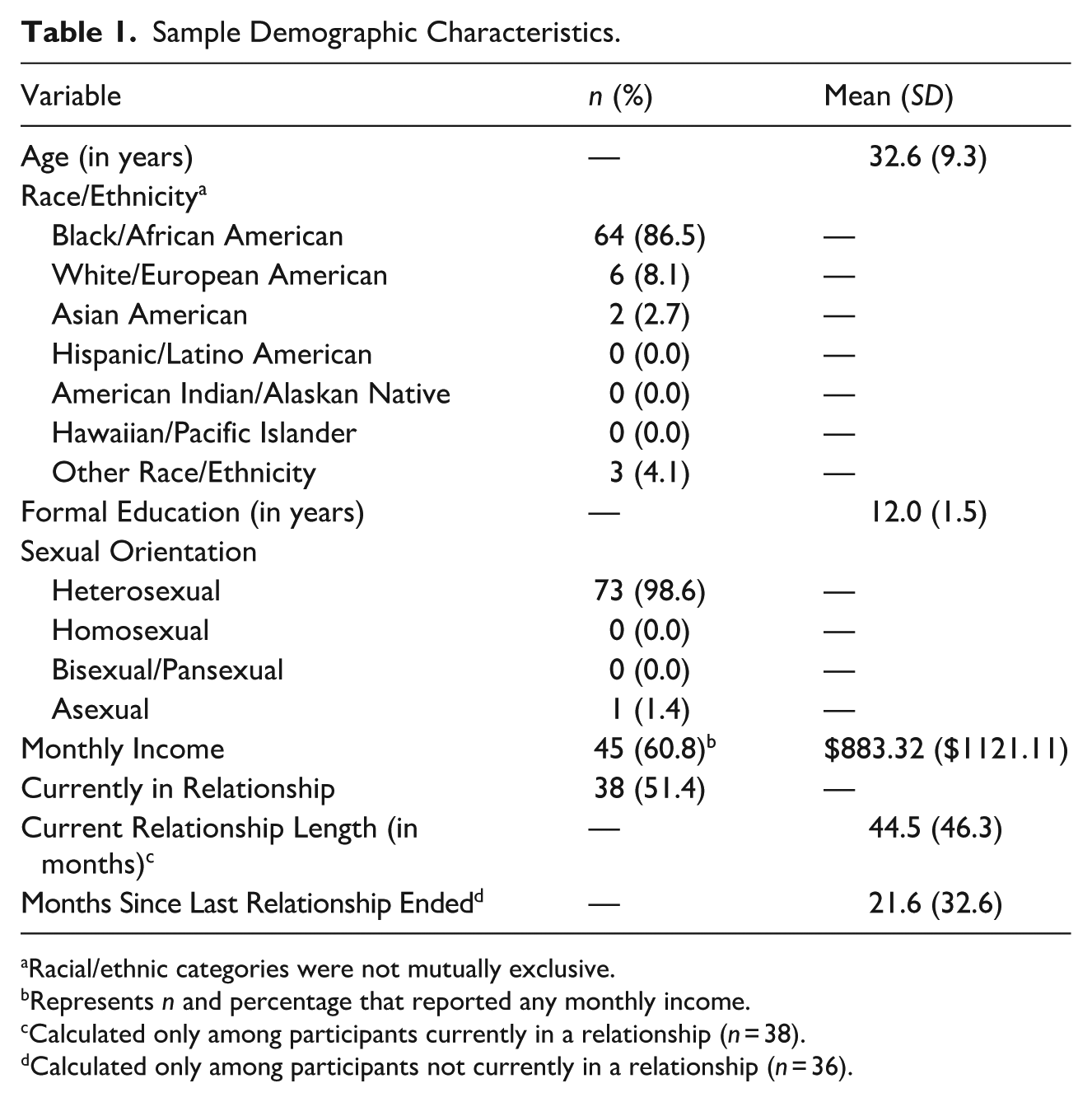
Racial/ethnic categories were not mutually exclusive.
Represents n and percentage that reported any monthly income.
Calculated only among participants currently in a relationship (n = 38).
Calculated only among participants not currently in a relationship (n = 36).
Measures
Multidimensional Experiential Avoidance Questionnaire
The MEAQ (Gámez et al., 2011) is a 62-item self-report assessment of EA, composed of six subscales: Behavioral Avoidance (11 items), Distress Aversion (13 items), Procrastination (7 items), Distraction and Suppression (7 items), Repression and Denial (13 items), and Distress Endurance (11 items). Response options are on a Likert scale ranging from 1 (strongly disagree) to 6 (strongly agree). The current study used the total sum of all item scores to represent EA as a generalized coping response style. Cronbach’s alpha for the total MEAQ scale score in the current sample was .86.
Experiential Avoidance in Relationship Situations
The Experiential Avoidance in Relationship Situations (EARS; LaMotte et al., 2025) assesses aspects of experiential avoidance in difficult relationships situations. Participants imagine themselves in five relationship scenarios that are expected to provoke uncomfortable emotions and are presented via narrated audio-recording. After each scenario, participants answer structured interview questions. First, they rate how much they would experience each of four negative emotions in the imagined scenario on a scale from 0 (not at all) to 10 (extremely): Anger, Jealousy, Sadness, and Anxiety. Next, they rate agreement with the following statements designed to assess motivation to avoid those emotions: “I would want to get rid of these emotions as soon as possible,” and “It would be difficult for me to tolerate these feelings for more than a short time” on a scale ranging from 0 (not at all) to 10 (completely). Participants are then presented with six behavioral responses for each scenario, and asked to rate how much each of these actions would help them to get rid of the negative anticipated emotions, and how likely they would be to engage in each action, with ratings provided on a scale from 0 (not at all) to 10 (completely). For each scenario, three response options represent aggressive/abusive actions, and three represent non-aggressive/non-abusive actions. Composite scores across scenarios assess total uncomfortable emotions, motivation to escape from those emotions, anticipated reduction in uncomfortable emotions from aggressive/abusive actions and from non-aggressive/non-abusive actions, and perceived likelihood of engaging in these responses. Psychometric details and descriptive data are presented in a separate paper (LaMotte et al., 2025).
Traumatic Events Questionnaire
The Traumatic Events Questionnaire (TEQ; Vrana & Lauterbach, 1994) is an 11-item assessment of exposure to traumatic events. Participants indicate whether they have experienced nine different categories of traumatic events, other very traumatic events, and other traumatic events that they are unwilling to describe. This study modified the TEQ by disaggregating childhood physical and sexual abuse into two items, adding an item inquiring about witnessing of parental abuse, and dropping probes about injury, life threat, and traumatization to reduce assessment burden. Participants indicated whether they had experienced each type of trauma never, once, twice, or three or more times. They also indicated the type of trauma that caused them the most distress, as well as their age when it began and ended. Those responses were used as the reference for a subsequent assessment of PTSD symptoms. The total number of traumatic events endorsed was calculated by summing the number of occurrences for each item (i.e., never = 0, once = 1, twice = 2, and three or more = 3). This scoring method has been found to correlate highly (r’s ranging from .80 to .92) with other scoring methods (e.g., number of trauma categories endorsed) in past research (LaMotte, 2021).
PTSD Symptom Checklist-5
The PTSD Symptom Checklist-5 (PCL-5; Weathers et al., 2013) is a 20-item self-report scale to assess DSM-5 symptoms of PTSD (American Psychiatric Association, 2013). Respondents rate how much they have been bothered by each symptom in the past month on a Likert scale from 0 (Not at all) to 4 (Extremely), with item scores summed to create a total PTSD symptom severity score. For the current study, participants reported symptoms in response to the traumatic experience that they reported was most distressing on the TEQ. Coefficient alpha was .91 for the PCL-5 total score in the current sample.
Revised Conflict Tactics Scales
The Revised Conflict Tactics Scales (CTS2; Straus et al., 1996) is a widely used assessment of IPV. The current study used the 12-item Physical Assault scale and the 7-item Sexual Coercion scale, eliciting frequency reports for the 6-months prior to study participation. For the current study, the lifetime variety scores were used (Moffitt et al., 1997). Each item is scored dichotomously as either 0 (never occurred) or 1 (occurred at least once before in lifetime), before summing across items. Cronbach’s alpha was .84 for the Physical Assault Lifetime Variety score, and .68 for the Sexual Coercion Lifetime Variety score.
Multidimensional Measure of Emotional Abuse, Short Form
The Multidimensional Measure of Emotional Abuse, Short Form (MMEA-SF; Maldonado et al., 2022) is a 16-item self-report scale that assesses four common forms of emotional abuse in adult intimate relationships: Restrictive Engulfment (e.g., “Tried to stop the other person from seeing certain friends or family members”), Hostile Withdrawal (e.g., “Acted cold or distant when angry”), Denigration (e.g., “Said or implied that the other person was stupid”), and Dominance/Intimidation (e.g., “Threw, smashed, hit, or kicked something in front of the other person”). The current study used an Emotional Abuse Lifetime Variety score, constructed using the procedures described above for the CTS2. Cronbach’s alpha was .89 for the Emotional Abuse Lifetime Variety score in the current sample. Confirmatory factor analyses have demonstrated good fit for the 4-factor model in both clinical and community samples, providing evidence for the structural validity of the MMEA-SF (Maldonado et al., 2022).
Procedures
Recruitment, Informed Consent, and Data Collection
Individuals were recruited during their first 6 weeks of participation in a 24-week Abuse Intervention Program, with 74% enrolling during an initial orientation session and 26% during Stage 1 group sessions This early phase of the program provides psychoeducation about partner abuse and encourages participants to recognize and acknowledge their abusive behavior. The intervention program uses a trauma-informed and oppression-sensitive approach, so it was deemed important to recruit participants early in the program before they had been extensively exposed to interventions that might alter the variables under investigation. Written informed consent was obtained in person, and all data were collected in a private room at the agency research site during a single study session which lasted approximately 1 hr. All assessments were administered via structured interview by the first author, and all data were collected in 2018–2019. Participants completed assessments in the following order: Demographic information, TEQ, PCL-5, EARS, MEAQ, CTS-2 Physical Assault and Sexual Coercion scales, and MMEA-SF. Finally, participants were debriefed, assessed for any adverse reactions, and paid $25 for participation. Study procedures were approved by Institutional Review at the University of Maryland, Baltimore County.
Data Analysis
After conducting descriptive analyses, the first two hypotheses were tested using Pearson’s correlations. The third hypothesis was tested using a dependent-means t-test comparing EARS anticipated reduction in uncomfortable emotions from aggressive/abusive actions versus non-aggressive/non-abusive actions. For the fourth hypothesis, mediation was tested with Model 4 of the SPSS PROCESS Macro (A. F. Hayes, 2017), using bias-corrected bootstrap 95% confidence intervals to determine the significance of indirect effects, as indicated by intervals that do not cross zero. Separate mediation analyses were conducted for the two measures of EA for each of the three forms of abusive behavior. Data were analyzed using IBM SPSS, version 25.
Results
Descriptive Analyses
Overall, the sample reported high rates of exposure to potentially traumatic events (PTEs) and high levels of PTSD symptoms. Participants reported experiencing, on average, 5.5 (SD = 2.4) unique categories of PTEs and 12.3 (SD = 6.9) total PTEs. All participants (100%) reported experiencing at least one PTE. Additionally, 34 participants (45.9%) had a PCL-5 score of 33 or higher, indicating a probable diagnosis of PTSD. Descriptive statistics for the measures of abusive behavior are presented in Table 2. On average, participants reported having engaged in 4 different physically assaultive behaviors, 9 emotionally abusive behaviors, and 0.2 sexually coercive behaviors. Notably, the Sexual Coercion score substantially deviated from normality (operationalized as skew greater than 2.0 and/or kurtosis greater than 7.0; Curran et al., 1996). Therefore, this variable was log-transformed for subsequent analyses.
Descriptive Statistics for the TEQ, PCL-5, EARS, MEAQ and CTS2.
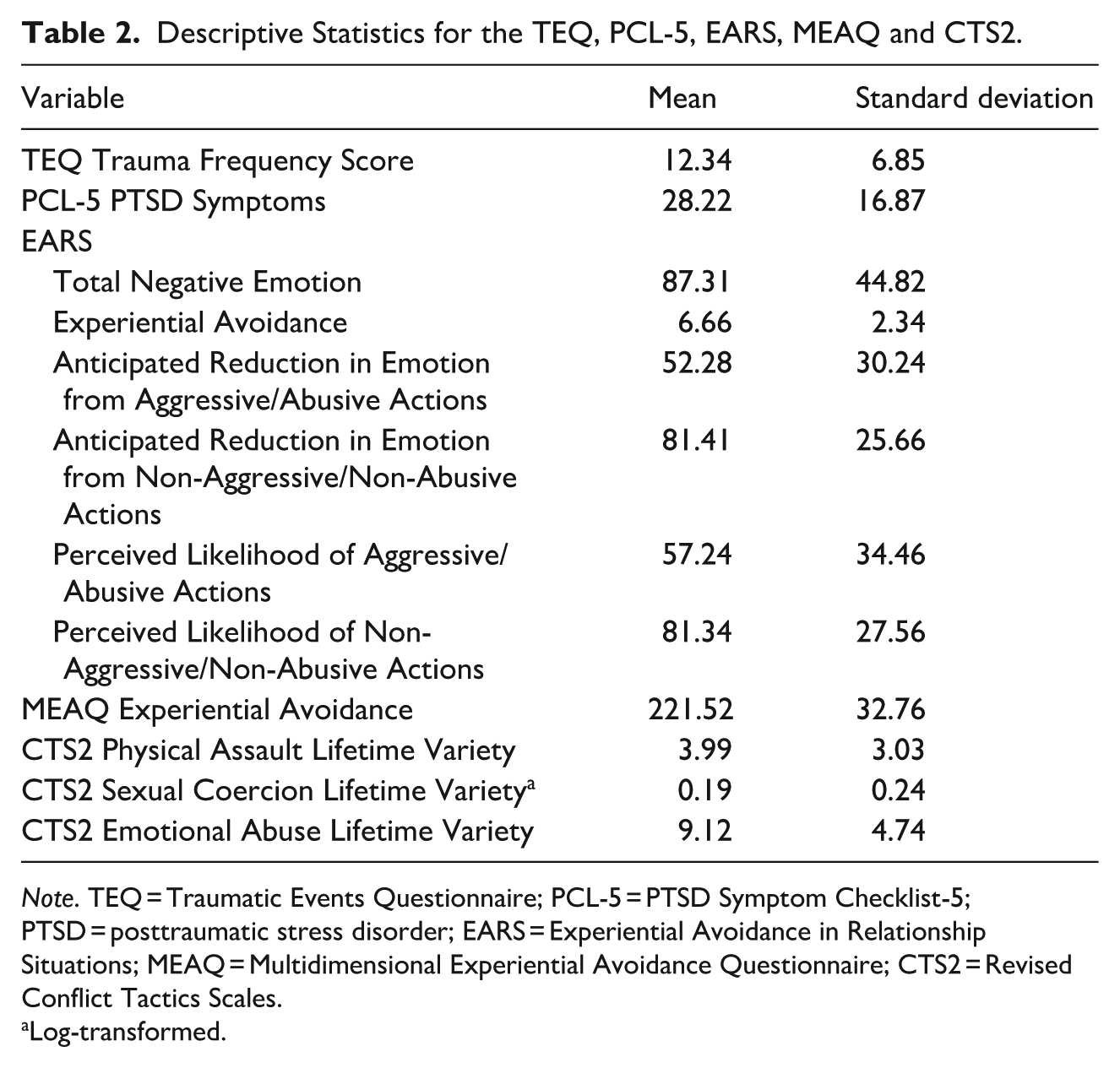
Note. TEQ = Traumatic Events Questionnaire; PCL-5 = PTSD Symptom Checklist-5; PTSD = posttraumatic stress disorder; EARS = Experiential Avoidance in Relationship Situations; MEAQ = Multidimensional Experiential Avoidance Questionnaire; CTS2 = Revised Conflict Tactics Scales.
Log-transformed.
Hypothesis Tests
Trauma Associations With Emotional Responses to Relationship Scenarios
The results support hypothesis one. As revealed in Table 3, both higher levels of lifetime trauma exposure and higher PTSD symptoms were significantly and positively associated with total anticipated uncomfortable emotions in response to challenging relationship scenarios. The correlation was in medium in magnitude for trauma exposure, and large in magnitude for PTSD symptoms.
Pearson Correlations Between Variables of Interest.
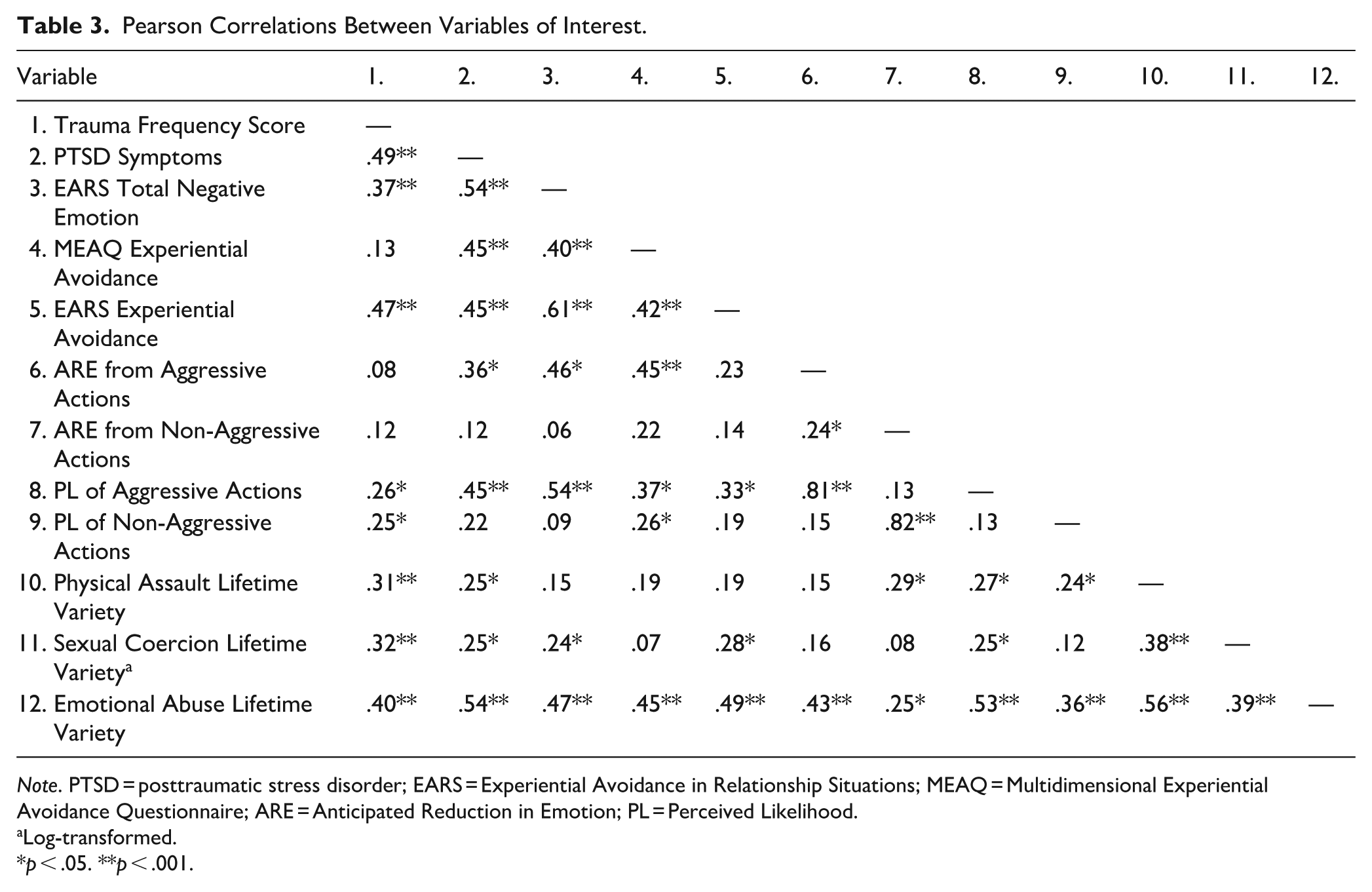
Note. PTSD = posttraumatic stress disorder; EARS = Experiential Avoidance in Relationship Situations; MEAQ = Multidimensional Experiential Avoidance Questionnaire; ARE = Anticipated Reduction in Emotion; PL = Perceived Likelihood.
Log-transformed.
p < .05. **p < .001.
Trauma Associations With Experiential Avoidance
Hypothesis two was supported by three of the four association tests. As revealed in Table 3, PTSD symptoms were significantly and positively correlated with greater trait experiential avoidance, as measured by the MEAQ, and with greater relationship-specific experiential avoidance, as measured by the EARS. Trauma exposure was significantly correlated with relationship-specific EA, but not with trait EA. All three significant correlations were in the medium range of magnitude.
Other Correlations With Experiential Avoidance
Trait EA, as measured by the MEAQ, was significantly and positively associated with anticipated reduction in uncomfortable emotions from aggressive/abusive actions, with perceived likelihood of engaging in aggressive/abusive actions, and with emotional abuse perpetration, all with medium effect sizes. There was a small and significant positive correlation between trait EA and perceived likelihood of non-aggressive/non-abusive actions. Relationship-specific EA, as measured by the EARS, was significantly and positively associated with perceived likelihood of aggressive/abusive actions and with emotional abuse perpetration, with moderate effect sizes, and with sexual coercion perpetration, with a small effect size.
Anticipated Reduction in Uncomfortable Emotions From Aggressive/Abusive Versus Nonaggressive/Nonabusive Responses
Across the five EARS scenarios, the mean endorsement for anticipated reduction in uncomfortable emotions was substantially higher for Nonaggressive/Nonabusive response options (M = 81.41, SD = 25.66) than for Aggressive/Abusive Response options (M = 52.28, SD = 30.24), t(73) = 7.25, p < .001, with a large effect size, d = 0.84. This result is directly counter to hypothesis 3.
Tests of Experiential Avoidance as Mediator of the Associations Between PTSD and IPV
Figure 1 depicts the general mediation model for the fourth hypothesis. In total, six mediation analyses were run, including both MEAQ and EARS measures of experiential avoidance as mediators, and perpetration of physical assault, sexual coercion, and emotional abuse as outcomes. Results of the mediation analyses are presented in Table 4 and significant mediation models are presented in Figures 2 and 3. As hypothesized, both relationship-specific and trait EA significantly mediated the association between PTSD symptoms and emotional abuse perpetration. In both cases, PTSD symptoms significantly predicted emotional abuse perpetration while controlling for experiential avoidance, indicating both direct and indirect effects. Contrary to the hypotheses, EA did not significantly mediate the associations between PTSD symptoms and perpetration of physical assault or sexual coercion. In summary, the hypothesis that experiential avoidance would account for the association between PTSD symptoms and abusive behavior was supported for emotional abuse, but not for physical assault and sexual coercion.
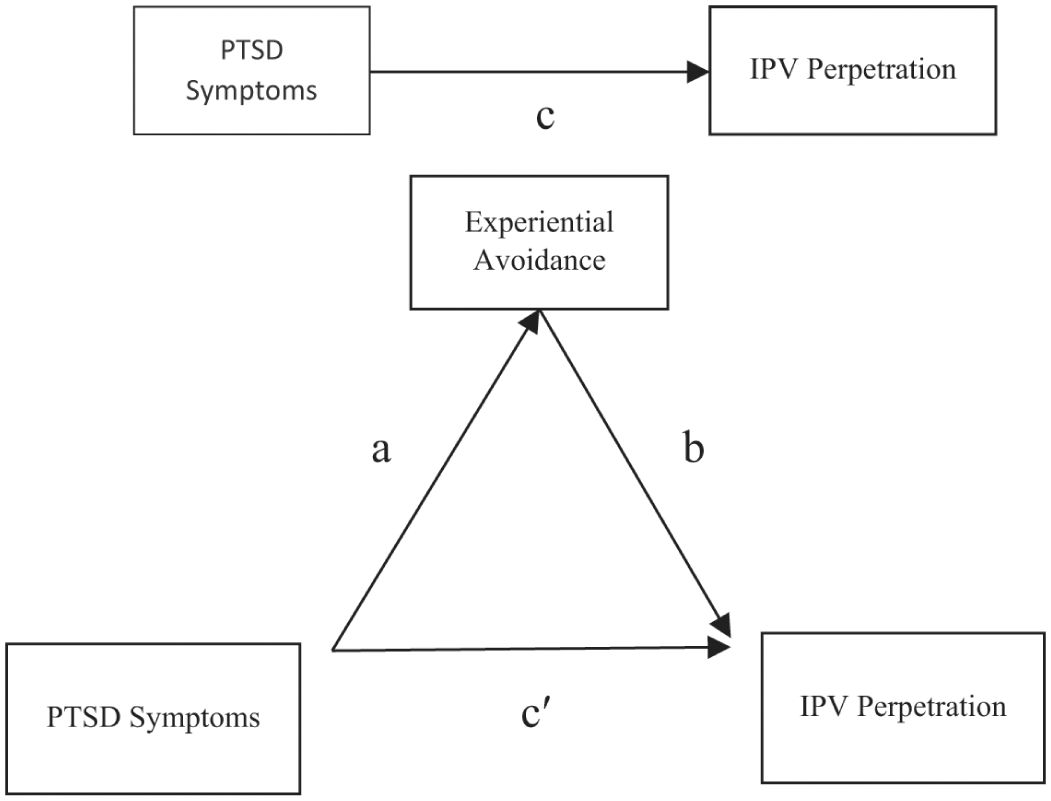
General mediation model with experiential avoidance as a mediator between PTSD symptoms and IPV perpetration.
Results of Mediation Analyses.
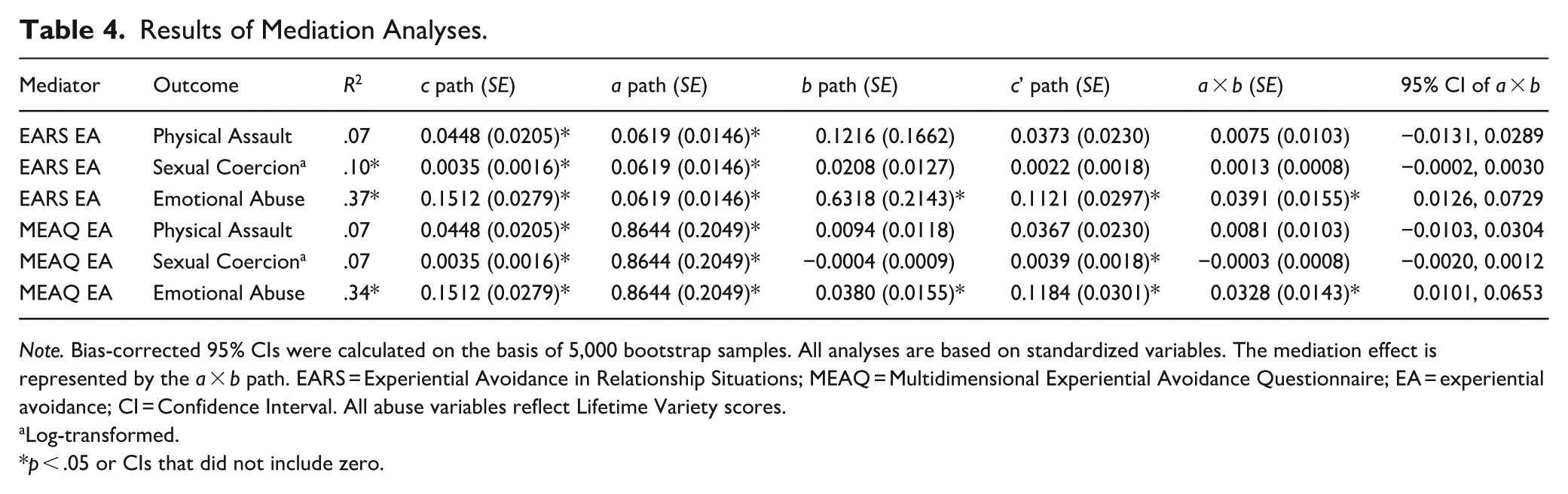
Note. Bias-corrected 95% CIs were calculated on the basis of 5,000 bootstrap samples. All analyses are based on standardized variables. The mediation effect is represented by the a × b path. EARS = Experiential Avoidance in Relationship Situations; MEAQ = Multidimensional Experiential Avoidance Questionnaire; EA = experiential avoidance; CI = Confidence Interval. All abuse variables reflect Lifetime Variety scores.
Log-transformed.
p < .05 or CIs that did not include zero.
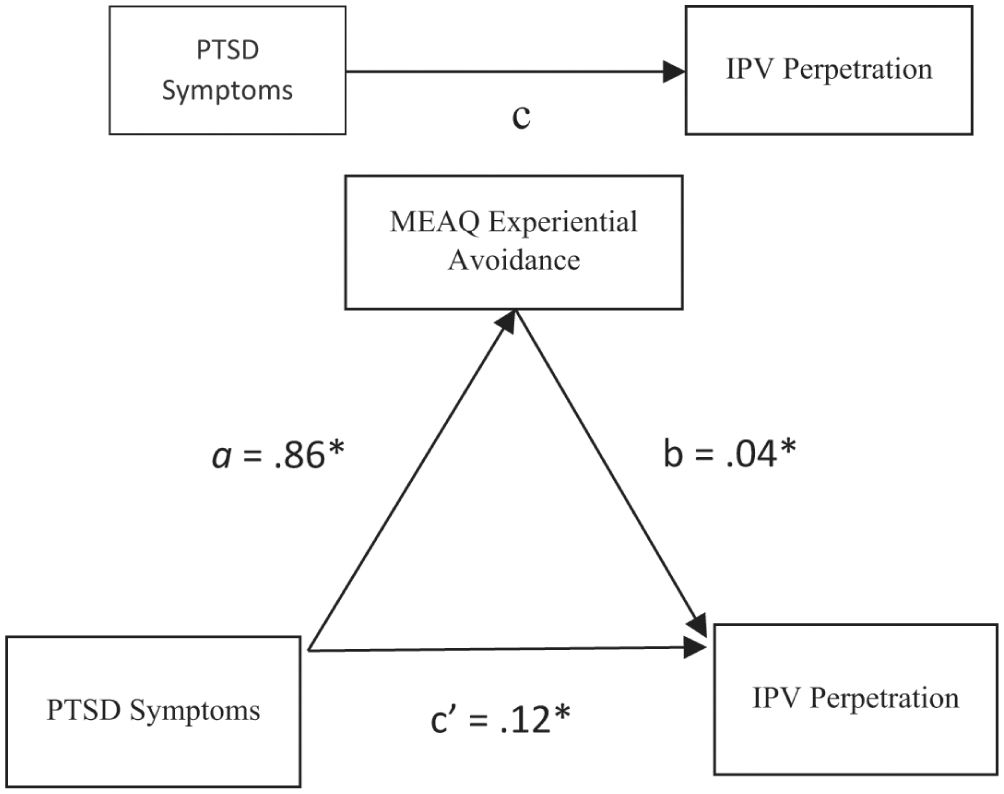
MEAQ Experiential avoidance as a mediator between PTSD symptoms and emotional abuse perpetration.
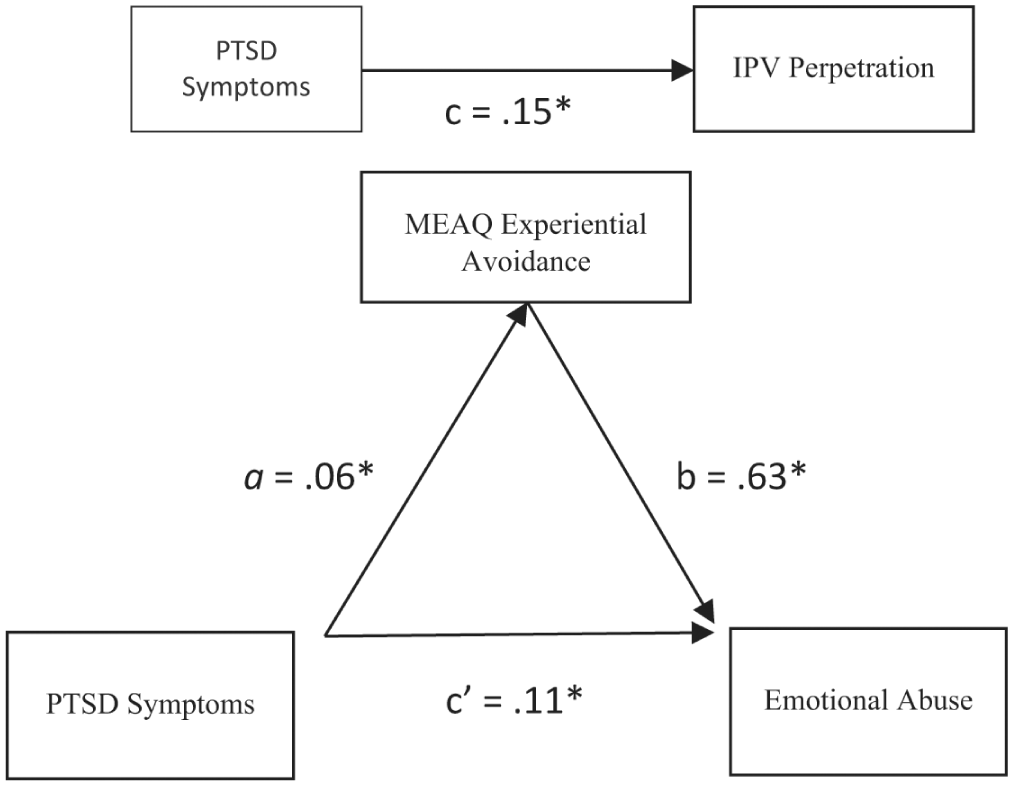
EARS Experiential avoidance as a mediator between PTSD symptoms and emotional abuse perpetration.
Sensitivity Analyses Adjusting for IPV Victimization
In light of the common finding that IPV perpetration is highly correlated with victimization, we conducted sensitivity analyses to determine whether PTSD symptoms predict abuse perpetration after adjusting for experiences of IPV victimization. A composite measure combining physical assault, sexual coercion, and emotional abuse victimization (using the same scoring method as for perpetration) was entered on the first step of a hierarchical multiple regression model followed by PTSD on the second step. IPV victimization explained 45.6% of the variance in physical assault perpetration (F = 60.42, p < .001). When PTSD was added to this model, it increased the explained variance by only 0.5% (ΔR2 = .005, F change = 0.64, p = .428), and was not significant in the final model (β = .035, p = .655). IPV victimization explained 53.4% of variance in emotional abuse perpetration (F = 82.58, p < .001). When PTSD was added to this model, it significantly increased explained variance by 5.2% (ΔR2 = .052, F(1, 71) = 8.84, p = .004), and remained significant in the final model (β = .256, p = .004, 95% CI [0.024, 0.120]). These results align with our mediation analyses showing that experiential avoidance mediated the PTSD-emotional abuse relationship but not the PTSD-physical assault relationship, and indicate that PTSD may convey unique risk for emotional abuse perpetration that does not appear to be explained solely by mutual patterns of aggression.
Discussion
As hypothesized, partner violent men with greater trauma exposure and higher levels of PTSD symptoms anticipate experiencing more uncomfortable emotions (anger, anxiety, sadness, and jealousy) in distressing relationship situations. In addition, those with higher levels of PTSD symptoms displayed higher levels of experiential avoidance, both when measured as a general (trait-like) coping strategy, and when assessed as the motivation to escape from uncomfortable emotions in difficult relationship situations. In addition, both relationship-specific and general experiential avoidance significantly mediated the association between PTSD symptoms and emotional abuse perpetration, but not physical assault or sexual coercion perpetration. Contrary to the prediction that participants would show a general tendency to rate aggressive actions as more likely than non-aggressive actions to reduce negative mood states in distressing relationship situations, participants reported the opposite. On average, they expressed the expectation that non-aggressive/non-abusive responses, such as cognitive reframing, deep breathing, and emotional expression, would be more likely to reduce their negative mood states.
The findings with regard to emotional abuse are consistent with the theory tested in this study that PTSD is associated, not only with hyperarousal and hostile bias in interpreting social cues (Chemtob et al., 1997) but also with deficits at the goals clarification stage of SIP (Crick & Dodge, 1994). Individuals with elevated PTSD symptoms tend to view immediate reduction of negative emotion as a primary goal during difficult relationship situations. This intention to repair one’s emotional state makes it more difficult to sustain other interpersonal goals, such as maintaining emotional connection while resolving disagreements or conflicts. The desire to escape from negative emotions can bias subsequent response selection toward abusive and controlling behaviors that are expected to help reduce those negative emotions, such as yelling, threatening harm, or violating the partner’s privacy or personal rights.
It may also be important to consider the role of EA relative to alexithymia, a related construct that was not measured in the current study. Alexithymia involves difficulties in identifying and labeling emotions and poor emotional awareness (Sifneos, 1972). Similar to EA, alexithymia has been associated with both traumatic stress exposure and IPV and is considered an important component of emotion regulation (Veggi et al, 2024). However, whereas alexithymia focuses primarily on emotion awareness, EA can involve a wide range of private experiences including unpleasant thoughts, images, impulses, and bodily sensations. In addition, alexithymia is often described as a character trait or skill deficit, whereas EA implies a motivated process of suppression, avoidance, or escape. It is therefore not surprising that EA may explain the association between alexithymia and distress and may provide a more robust target for clinical intervention (Torunsky et al., 2023).
Whereas the mediation results with emotional abuse supported predictions from the SIP model, results with physical assault and sexual coercion did not. Relatedly, the association with PTSD symptoms was stronger for emotional abuse perpetration than for physical and sexual IPV, which is consistent with prior research (Maguire et al., 2015; Semiatin et al., 2017). Participants reported lower overall levels of physical assault and sexual coercion in contrast to emotional abuse, and this restriction of variability may suppress associations. Alternatively, experiential avoidance, operating at the goals clarification stage, may be particularly relevant to emotional abuse perpetration, whereas deficits at other stages of SIP may be more relevant to other forms of IPV perpetration. For example, hyperactive threat perception at early SIP stages may be particularly relevant for impulsive physical aggression (LaMotte et al., 2016; Sippel & Marshall, 2011).
The finding that PTSD symptoms were associated with a stronger belief in the mood repairing properties of aggression/abuse is especially interesting, as this is an aspect of SIP that has received limited theoretical and research attention with respect to PTSD. One recent study (Miles-McLean et al., 2021) found that PTSD symptoms were associated with greater positive outcome expectancies of IPV perpetration among a sample of men presenting to an AIP. Some particular types of traumatic events, such as witnessing interparental abuse during childhood, may directly model aggressive responses. For example, Fite et al. (2008) found that adolescents who had witnessed greater inter-parental IPV in childhood generated more aggressive responses and evaluated aggressive responses more positively during social vignettes. Other potential explanations for this relationship have not been thoroughly explored. For instance, positive views of aggression may relate to hyperactive threat perception in PTSD (Chemtob et al., 1997), whereby mistrust of others’ intentions contributes to the general view that aggression is necessary in order to protect oneself. Additionally, as trauma can disrupt one’s prior beliefs about justice in the world (Resick et al., 2017; Tay et al., 2017), aggression may be viewed favorably by those with PTSD as a means to enact one’s own perceived justice and correct perceived injustice. It will be beneficial for future research to explore the over-valuing of aggression as an emotion-regulation strategy by people with PTSD, given that this study’s findings demonstrate its relevance to emotional abuse perpetration.
Limitations
The current findings should be interpreted in light of several study limitations. First, the reliance on participant self-reports of abusive behavior, trauma exposure, and PTSD may be subject to retrospective biases and socially desirable responding. Several practical barriers precluded the use of victim partner reports, including the fact that a sizable proportion of the sample (32.4%) were not in a current relationship at the time of assessment. Similarly, socially desirable responding may have influenced participant reports on the EARS, for example the desire to give “correct” responses when asked about the expected value of aggressive versus non-aggressive responses in repairing one’s emotion state. In addition, the temporal ordering of variables cannot be determined from the cross-sectional study design. Similarly, other correlated factors such as relationship adjustment, co-morbid personality or mental health problems, or stressful life circumstances may influence the associations between EA and IPV. Further research is needed to explore multi-factorial models involving EA in IPV. The relatively modest sample size in the current study precluded further analysis of more complex models. Finally, generalization of findings may be limited given that the sample came from one specific program in a large urban center. All participants were men, and most were African American (86.5%) and heterosexual (98.6%). Many of the study participants have been exposed to significant life challenges that may not be well represented in other research on partner abuse. For example, their rate of probable PTSD was over three times higher than the rates reported in IPV treatment samples in other contexts (Rosenbaum & Leisring, 2003; Semiatin et al., 2017).
Clinical Implications
The findings are consistent with several encouraging trends in recent research on the efficacy of partner violence interventions. The high level of trauma exposure and PTSD observed in the current sample is consistent with an increasing recognition of the importance of trauma-informed and anti-oppression practices in IPV intervention (Murphy et al., 2021; Taft, Murphy et al., 2016). Through creating an organizational culture that acknowledges the effects of trauma on the population served, trauma-informed IPV interventions use empathic and supportive relationships to prevent re-traumatizing clients, and employ treatment strategies that directly address the psychological sequelae of trauma (Elliott et al., 2005; Substance Abuse and Mental Health Services Administration, 2014). Trauma-informed intervention has been effective in reducing abusive behavior in controlled trial research with military veterans (Taft, MacDonald, et al., 2016) and uncontrolled research with court-referred men from the community (Taft et al., 2021). Similarly, consistent with the current finding that trauma exposure can influence IPV risk through experiential avoidance, trauma-informed IPV intervention has been associated with improvements in emotional processing, specifically reductions in the tendency to suppress and avoid emotions (Berke et al., 2017). Additionally, culturally-informed and oppression-sensitive IPV interventions may better address systemic barriers faced by marginalized communities while fostering accountability and long-term behavior change. Scholars (Emezue et al., 2021; Williams, 2008) and organizations such as the Oregon Coalition Against Domestic and Sexual Violence have highlighted the importance of addressing IPV within broader systems of oppression. Such frameworks emphasize the value of culturally tailored, community-centered strategies that align interventions with the lived experiences of diverse populations.
The current study helps to advance trauma-informed practice by identifying how emotional sequelae of PTSD symptoms are associated with abusive reactions to difficult relationship situations, further highlighting the importance of intervention strategies that target experiential avoidance for this population. The potential value of focusing on experiential avoidance in IPV Intervention has been supported through application of intervention strategies derived from ACT (Zarling & Berta, 2017). Several controlled trials have provided support for the efficacy of this approach (Lawrence et al., 2021; Zarling & Russell, 2022; Zarling et al, 2019), along with evidence that improved emotion regulation partially accounts for reductions in abusive behavior from ACT-based treatment (Zarling et al., 2015).
The current findings bolster the theoretical rationale for the application of third-wave CBTs for IPV by demonstrating the important role of experiential avoidance in abusive behaviors. Furthermore, trauma experiences and PTSD, which are highly prevalent in this population (Hoyt et al., 2012; Maguire et al., 2015; Rosenbaum & Leisring, 2003; Semiatin et al., 2017), accentuate this avoidance of uncomfortable emotion states. Therefore, it may be useful for treatment providers to help clients explore how their past traumatic experiences are associated with the desire to reduce uncomfortable emotion states, and how this process contributes to abusive and controlling behavior. Additionally, this study found that both PTSD symptoms and emotional abuse perpetration were associated with a greater tendency to anticipate that aggressive responses will reduce uncomfortable emotions. Some traditional IPV intervention models seek to alter clients’ decisional balance for IPV (i.e., weighing pros and cons) by highlighting the negative long-term consequences of IPV and by promoting alternative short-term strategies to reduce uncomfortable emotions without incurring these negative consequences. However, the current finding suggests that it may also be useful to challenge the pressing need to reduce uncomfortable emotion states by increasing emotional awareness and acceptance. Finally, an increased focus on community-informed and oppression-sensitive intervention approaches can help to contextualize the high rates of community and family violence exposure reported by the current sample, as well as social pressures to avoid and suppress emotional reactions to stress and trauma.
Footnotes
Authors’ Note
This article is based on a dissertation completed by the first author (LaMotte, 2021).
Funding
The authors received no financial support for the research and/or authorship of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.