
Abstract
Intimate partner violence (IPV) poses a significant public health concern for women in the United States. IPV among women is associated with deleterious consequences, such as heightened drug use and susceptibility to increased drug-related harm. Women experiencing IPV are also at increased risk for exposure to other forms of trauma, including community violence. Given that exposure to community violence confers heightened risk for drug use-related harm, it is imperative to identify factors that may help explain this association. The current study extends this line of research by exploring the role of posttraumatic stress disorder (PTSD) symptom severity in the association between exposure to community violence and drug use-related harm among women experiencing IPV. Participants were 169 women experiencing IPV (Mage = 40.42, 31.7% Black/African American) who were recruited from the community and completed validated measures of community violence, PTSD symptom severity, and drug use-related harm. To address the question of whether PTSD symptom severity underlies the association between differential exposure to community violence and drug use-related harm, two indirect effect analyses were conducted. Results provided support for significant indirect effects of witnessing and experiencing community violence, respectively, on drug use-related harm through PTSD symptom severity when accounting for physical, sexual, and psychological IPV; income; and employment status. Study findings align with prior research suggesting a positive association between community violence and PTSD symptom severity and outlining the robust positive relationship between PTSD and substance use. Findings underscore the importance of assessing the role of PTSD symptom severity in drug use-related harm among women experiencing IPV who have been exposed to community violence.
Keywords
Introduction
Intimate partner violence (IPV) is a major public health issue for women in the United States. IPV is characterized by physical violence, sexual violence, psychological aggression, and/or stalking within a romantic relationship (Centers for Disease Control, 2024a). IPV exposure (i.e., experiences of physical, sexual, and/or psychological victimization perpetuated by an intimate partner) disproportionately affects women, such that 41% of women experience IPV by an intimate partner during their lifetime, compared to 26% of men (Leemis et al., 2022). Empirical evidence suggests that IPV exposure is associated with substantial physical and psychological distress and impairment (Leemis et al., 2022). IPV exposure is associated with 1.4 to 3.5 times greater odds of physical illness (e.g., cardiovascular, endocrine, chronic, and infectious diseases), 1.8 times greater odds of depression, 2 times greater odds of anxiety, and 1.5 to 3.3 times greater odds of substance use (alcohol, tobacco, and illicit drugs; Bacchus et al., 2018; Stubbs & Szoeke, 2022). IPV-related contexts are among the most commonly reported interpersonal precipitating circumstances for suicidal and homicidal deaths (Liu, 2023). In addition, there are significant economic costs ($3.6 trillion) associated with IPV-related events (e.g., hospitalizations/medical costs, mental health costs, and rape-related pregnancy), resulting in a total of over $100,000 per woman experiencing IPV (Peterson et al., 2018). These alarming consequences underscore the significance of investigating factors that pose an increased risk for injurious public health outcomes among women experiencing IPV. One notable consequence is drug use-related harm. Prior research has highlighted the role of drug use-related harm as a common outcome of exposure to IPV in women (Mehr et al., 2023; Ogden et al., 2022). Women experiencing IPV are approximately three times more likely to engage in illicit drug use (e.g., heroin and crack/cocaine; El-Bassel et al., 2005; Gilbert et al., 2012) and are more likely to experience a drug use disorder (DUD; e.g., cocaine, cannabis, and opioid; Dichter et al., 2017; P. H. Smith et al., 2012). Additionally, prior work indicates that IPV exposure among women is associated with increased drug-related harm (e.g., occupational or relational problems, illegal activities, and regret; Flanagan et al., 2014; Ogden et al., 2022). These findings align with affective processing models of negative reinforcement of drug use, which suggest that individuals may use drugs in attempt to escape or avoid trauma symptoms and related distress (Hawn et al., 2020). While research that identifies the predictors (e.g., PTSD and emotion dysregulation) of drug use outcomes in women experiencing IPV is limited (Sullivan et al., 2020; Weiss et al., 2022), the current study adds to the increasing body of research on drug use-related harm among women who experience IPV (for reviews, see Cafferky et al., 2018; Ogden et al., 2022; R. Stone & Rothman, 2019) by examining the influences of community- (i.e., community violence) and individual- (i.e., PTSD symptom severity) level factors on drug use-related harm in this population.
Exposure to community violence may play an integral role in shaping the use of drugs and experience of related harm. Community violence is marked by acts between unrelated individuals that occur outside of the home (i.e., within one’s neighborhood and/or community) and threaten, or result in harm (e.g., assault, fights, shooting, and robbing; Centers for Disease Control, 2024b; Kennedy & Ceballo, 2014; Richters & Saltzman, 1990) and is associated with increased IPV exposure (Beyer et al., 2015; Raghavan et al., 2006). The prevalence of community violence is linked to deleterious consequences at the individual, community, and systemic levels (Burrell et al., 2021; Taylor & Patel, 2012). For instance, community violence is associated with significant economic costs, distrust of law enforcement and community leaders, and loss of social cohesion within the community (Taylor & Patel, 2012). Moreover, community violence creates a positive feedback loop, contributing to increases in community strain and subsequent violence over time (Burrell et al., 2021). Exposure to community violence also increases vulnerability to hazardous outcomes such as drug use-related harm (Brady, 2006; Löfving-Gupta et al., 2018; Motley et al., 2017; Thomas et al., 2020; Walker et al., 2024). However, there is limited knowledge of underlying mechanisms that may explain this association.
Posttraumatic stress disorder (PTSD) symptom severity is worth examining in this regard. PTSD is characterized by intrusions, avoidance, negative alterations in cognition and mood, and alterations in arousal and reactivity following exposure to a traumatic event (American Psychiatric Association, 2013), such as IPV (Dutton et al., 2006; Pill et al., 2017). Empirical studies have shown that PTSD symptom severity is positively associated with exposure to community violence (Fitzpatrick & Boldizar, 1993; Margolin & Gordis, 2000), yielding small to moderate effect sizes (Affrunti et al., 2018). While the association between PTSD symptom severity and drug use-related harm has been well-established (Haller & Chassin, 2013; Jacobsen et al., 2001; McCauley et al., 2012; Weiss et al., 2019), the relations among community violence, PTSD, and drug use-related harm remain unclear. Exposure to community violence may contribute to an increase in PTSD symptom severity due to an elevated risk of exposure to community-related traumatic events (Cole et al., 2020; Sargent et al., 2020). Additionally, increased community violence might reflect broader community issues such as diminished social cohesion (Kawachi & Berkman, 2000), which has been associated with elevated PTSD rates (Johns et al., 2012). Chronic community violence exposure also results in increased hyperarousal (e.g., hypervigilance; J. R. Smith & Patton, 2016; Phan et al., 2020), a key feature of PTSD, as a means of mitigating risk of violence exposure. Moreover, individuals affected by greater exposure community violence are also more likely to be characterized by lower socioeconomic status (APA, 2010) and may face unique barriers to access and utilization of mental health services (e.g., transportation, financial, and stigma; Hodgkinson et al., 2017). Consequently, community violence exposure may exacerbate risk for exposure to traumatic events, developing PTSD, and chronicity of PTSD due to diminished protective factors, shared consequences, and treatment barriers. In line with the affective processing model of negative reinforcement (Baker et al., 2004)—which posits avoidance of negative affect as a primary motive for drug use—individuals may subsequently use drugs to mitigate the severity of PTSD symptoms (Jaquier et al., 2015; Sullivan & Holt, 2008). PTSD symptom severity, under these conditions, may help explain the relation between exposure to community violence and drug use-related harm (Wamser et al., 2024).
Despite evidence suggesting positive relations between these variables, research in this area remains largely underexplored with respect to adults in the community, with most studies comprising children, adolescents, and young adults. Likewise, investigations of these relations among women experiencing IPV are scant, despite research suggesting empirical ties between IPV and exposure to community violence (Beyer et al., 2015; Raghavan et al., 2006), PTSD symptoms (Dutton et al., 2006; Pill et al., 2017), and drug use-related harm (Ogden et al., 2022) among women. Addressing these limitations, the current study is the first known study to examine the underlying role of PTSD symptom severity in the association between exposure to community violence and drug use-related harm in a sample of community women experiencing IPV. We hypothesized that exposure to community violence (both experiencing and witnessing) would be indirectly associated with drug use-related harm via PTSD symptom severity among women experiencing IPV. While not primary study variables, physical, sexual, and psychological IPV exposure were included as covariates in the analytic models given that the sample comprised women experiencing IPV and evidence that IPV is related to drug use-related harm (Ogden et al., 2022). Further, income and employment status were included as covariates given evidence that individuals with lower socioeconomic status backgrounds are more likely to live in areas with higher community violence (Markowitz, 2003) and are at higher risk for drug use-related harm (Baptiste-Roberts & Hossain, 2018).
Method
Participants
The present study utilized baseline data collected from a larger study examining the proximal role and temporal ordering of emotion dysregulation in substance use and HIV/sexual risk, and the role of PTSD (Weiss et al., 2023). Participants were recruited from 2018 to 2020 from the community in Providence County, Rhode Island online (e.g., local Craigslist) and through postings in laundromats, grocery stores, and stores; state offices including the Office of Housing and Community Development; and restrooms, waiting rooms, and city primary care clinics. Eligible participants were determined by an initial phone screen. Participants comprised women who experienced physical/sexual victimization by their current male partner in the past 30 days and used any number of drugs or alcohol in the past 30 days. Inclusion criteria were as follows: (a) age 18 or older, (b) fluent in the English language, and (c) current involvement in a relationship of at least 6 months’ duration with contact at least twice a week. Exclusion criteria encompassed: (a) current mania/psychosis, assessed at baseline through the Structured Clinical Interview for DSM-V (SCID-5; First & Williams, 2016), (b) current impairment in cognitive functioning, assessed at baseline through the Mini-Mental Status Exam (Folstein et al., 1975) and requiring a score >24, (c) self-reported current pregnancy (due to concerns that induction of negative affect during an experimental session in the parent study could induce distress that would have a subsequent negative effect on fetal development), (d) colorblindness (which would limit ability to complete study activities in an experimental session in the parent study), (e) cardiovascular disease (which could influence measurement of cardiovascular reactivity in an experimental session in the parent study), and (f) residence in a shelter or group home (which could limit opportunities for substance use during the experience sampling method [ESM] period in the parent study).
Procedures
All procedures were reviewed and approved by the [redacted] Institutional Review Board. As part of the larger study [redacted], participants underwent a baseline session, an experimental session, 30 days of ESM using interactive voice recording technology (i.e., phone technology that facilitates collection of data from participants via automated voice commands and keypad input), and a follow-up session. Community resources and any assistance with referrals were provided for participants. Participants were provided the contact information of the principal investigator, a licensed psychologist in the state of Rhode Island to ensure participant safety with trauma- and/or substance-related concerns. The present study utilized cross-sectional data collected at the baseline session.
Measures
Demographic Variables and IPV Characteristics
Participants reported their age, race, ethnicity, education, employment, income, and relationship status. Participants also reported whether they had experienced any physical, sexual, or psychological IPV in the past 30 days. Physical IPV instances were recorded using the 12-item Revised Conflict Tactics Scale (Straus et al., 2003). Sexual IPV exposure was captured by the 10-item Sexual Experiences Survey (Koss & Oros, 1982). Psychological IPV experiences were measured by 14 items from the Psychological Maltreatment of Women Inventory–Short Form (Tolman, 1999).
Community Violence
The Survey of Exposure to Community Violence–Brief (SECV-B; Rosenthal & Wilson, 2001) is an 18-item self-report measure, adapted from Richters and Saltzman (1990), used to assess the frequency of exposure to different forms of violent and threatening community events. Participants completed the SECV-B in response to the frequency of exposures to community violence over their lifetime. Responses options were rated on a nine-point Likert scale ranging from 1 (never) to 9 (almost every day). Subscale scores were calculated for witnessing and experiencing community violence. Higher scores indicated greater witnessing and experiencing community violence. The SECV-B-witnessing subscale scores ranged from 0 to 75. The SECV-B-experiencing subscale scores ranged from 0 to 47. The SECV-B has demonstrated acceptable psychometric properties (DeCou & Lynch, 2017). In the current study, the SECV-B witnessing (ω = .91) and experiencing (ω = .86) subscales, respectively, demonstrated excellent and good reliability.
PTSD Symptom Severity
The PTSD Checklist for the DSM-5 (PCL-5; Weathers et al., 2013b) is a 20-item self-report measure used to assess PTSD symptom severity. Participants responded to a series of questions that correspond to the DSM-5 criteria for PTSD based on the most distressing Criterion A event endorsed on the Life Events Checklist for DSM-5 (LEC-5; Weathers et al., 2013a), a 17-item self-report measure of lifetime trauma. Participants who endorsed “any other stressful event or experience” as their most distressing event on the LEC-5 (n = 2) were excluded from the analyses as we were unable to confirm that event they completed the PCL-5 in response to would meet criteria for a Criterion A event. Participants were asked to indicate how often they have been bothered by each of the symptoms over the past month. Responses options were rated on a five-point Likert scale ranging from 0 (not at all) to 4 (extremely). A total score was calculated by summing all the items, with higher scores indicating greater PTSD symptom severity. PCL-5 scores ranged from 0 to 80. The PCL-5 has shown good internal consistency and convergent and discriminant validity (Blevins et al., 2015; Forkus et al., 2023; Schick et al., 2024). In the current study, the PCL-5 demonstrated excellent reliability (ω = .97).
Drug Use-Related Harm
The Drug Abuse Screening Test (DAST; Skinner, 1982) is a 10-item self-report measure used to assess the presence of past-month problems related to drug use, such as medical and relational problems, illegal activities, or guilt. Participants were asked whether they experienced different types of drug-related harm. Responses options were rated on a binary scale ranging from 0 (no) to 1 (yes). Higher scores indicated greater drug use-related harm. DAST scores ranged from 0 to 10. The DAST has demonstrated good reliability and validity (Skinner, 1982). In the current study, the DAST demonstrated excellent reliability (ω = .90).
Data Analytic Plan
IBM SPSS Statistics Version 29 was utilized the analyze the data. First, data were assessed for violations to assumptions of normality. Next, descriptive data (i.e., frequencies, averages, and standard deviations) on study variables were conducted. To address the question of whether PTSD symptom severity underlies the association between differential exposure to community violence (i.e., witnessing and experiencing) and drug use-related harm (Figure 1), we conducted two indirect effect analyses (Preacher & Hayes, 2004) with the PROCESS SPSS macro (Model 4; Hayes, 2022). The PROCESS procedures use ordinary least squares regression and bootstrapping methodology, which confers more statistical power than do standard approaches to statistical inference and does not rely on distributional assumptions. Bootstrapping was done with 5,000 random samples generated from the observed covariance matrix to estimate bias-corrected 95% confidence intervals (CIs) and significance values (MacKinnon et al., 2002; Preacher & Hayes, 2004). Effects are deemed statistically significant if the 95% CI does not contain zero (Preacher & Hayes, 2004). Each model included physical, sexual, and psychological IPV; income; and employment status as covariates.
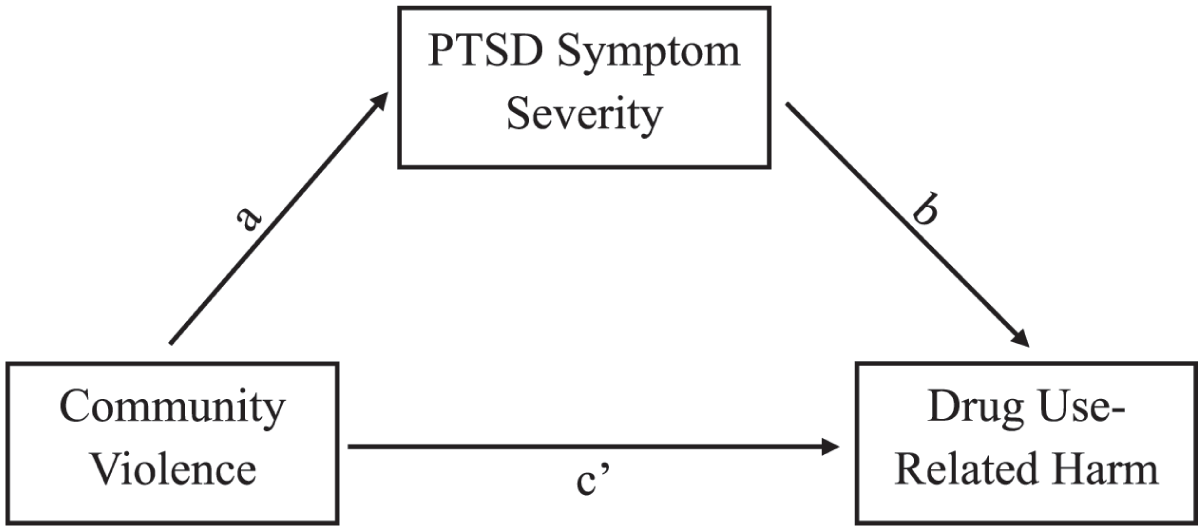
Conceptual model of the indirect effects of community violence exposure on drug use-related harm via PTSD symptom severity.
Results
Preliminary Analyses
The total sample included 169 women who participated in the baseline session. Demographic characteristics are summarized in Table 1. The majority of participants reported physical (67.7%) and psychological (93.8%) IPV, and over half (53.2%) reported sexual IPV. Most participants reported witnessing (87.3%) and experiencing (89.0%) community violence. Over half of participants met criteria for a probable PTSD (55.8%) and DUD (54.0%) diagnosis, respectively. See Tables 1 and 2 for descriptive and correlational statistics, respectively. All of the primary study variables were significantly positively intercorrelated (r values ranging from .177 to .756; p values ranging from <.001 to .041). Physical, sexual, and psychological IPV severity were significantly positively associated with witnessing and experiencing community violence and drug use-related harm (r values ranging from .230 to .411; p values ranging from <.001 to .006). There were no significant differences in drug use-related harm across demographics.
Sample Demographic Characteristics (N = 169).
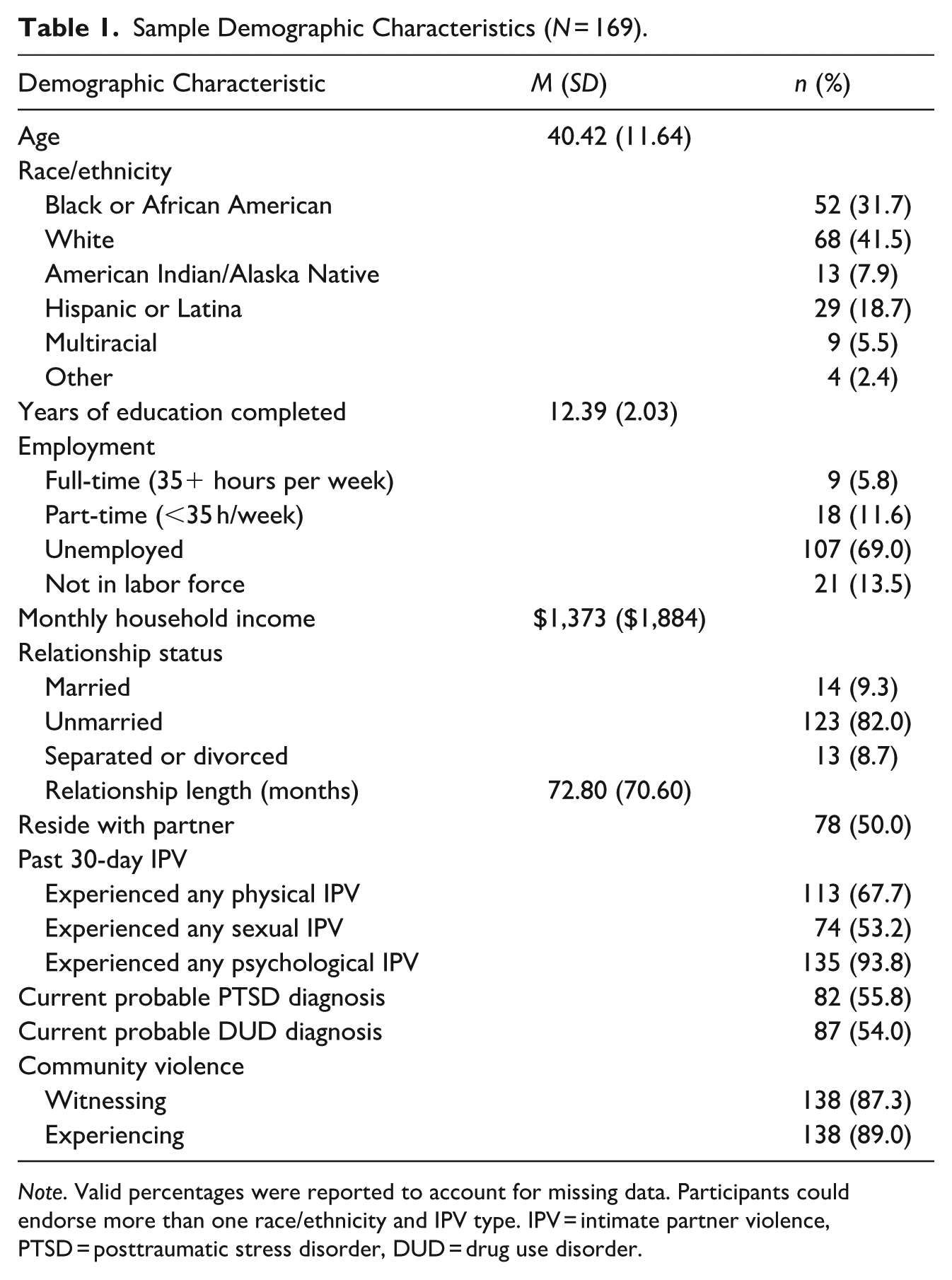
Note. Valid percentages were reported to account for missing data. Participants could endorse more than one race/ethnicity and IPV type. IPV = intimate partner violence, PTSD = posttraumatic stress disorder, DUD = drug use disorder.
Intercorrelations Among the Primary Study Variables.
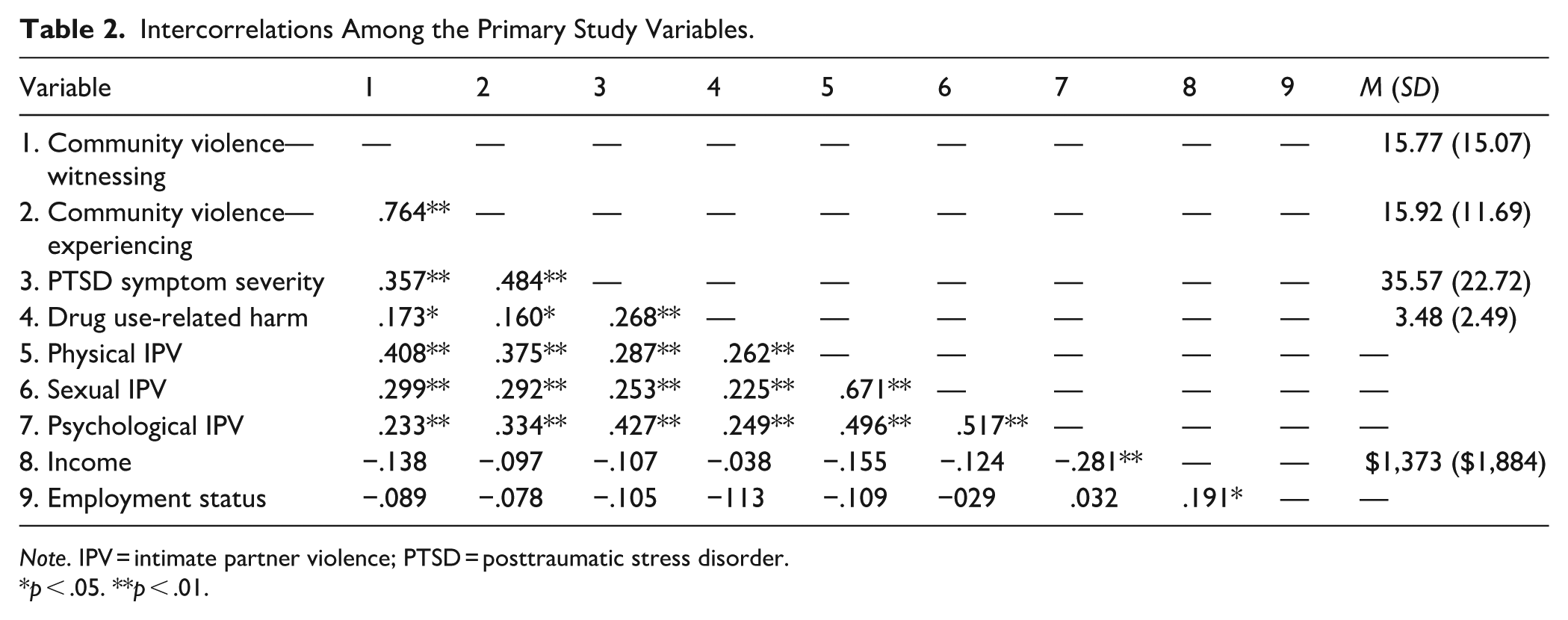
Note. IPV = intimate partner violence; PTSD = posttraumatic stress disorder.
p < .05. **p < .01.
Primary Analyses
Witnessing Community Violence
See Table 3 for a summary of indirect effect analyses. A significant indirect effect of witnessing community violence on past month drug use-related harm was found through PTSD symptom severity (b = 0.016, SE = 0.009, 95% CI [0.003, 0.037]) when controlling for physical, sexual, and psychological IPV; income; and employment status. Witnessing community violence was significantly associated with PTSD symptom severity (a path; b = 0.579, SE = 0.157, t = 3.677, p > .001 [0.266, 0.892]). There was a significant conditional main effect of PTSD symptom severity on drug use-related harm (b path; b = 0.028, SE = 0.012, t = 2.370, p = .020 [0.005, 0.051]), accounting for the effect of witnessing community violence. There was no significant direct effect of witnessing community violence on drug use-related harm when PTSD symptom severity was accounted for in the model (c′ path; b = 0.020, SE = 0.018, t = 1.063, p = .291 [−0.017, 0.056]). The strength and direction of findings did not change when physical, sexual, and psychological IPV were excluded from the model. 1
Analyses of Indirect Effects.
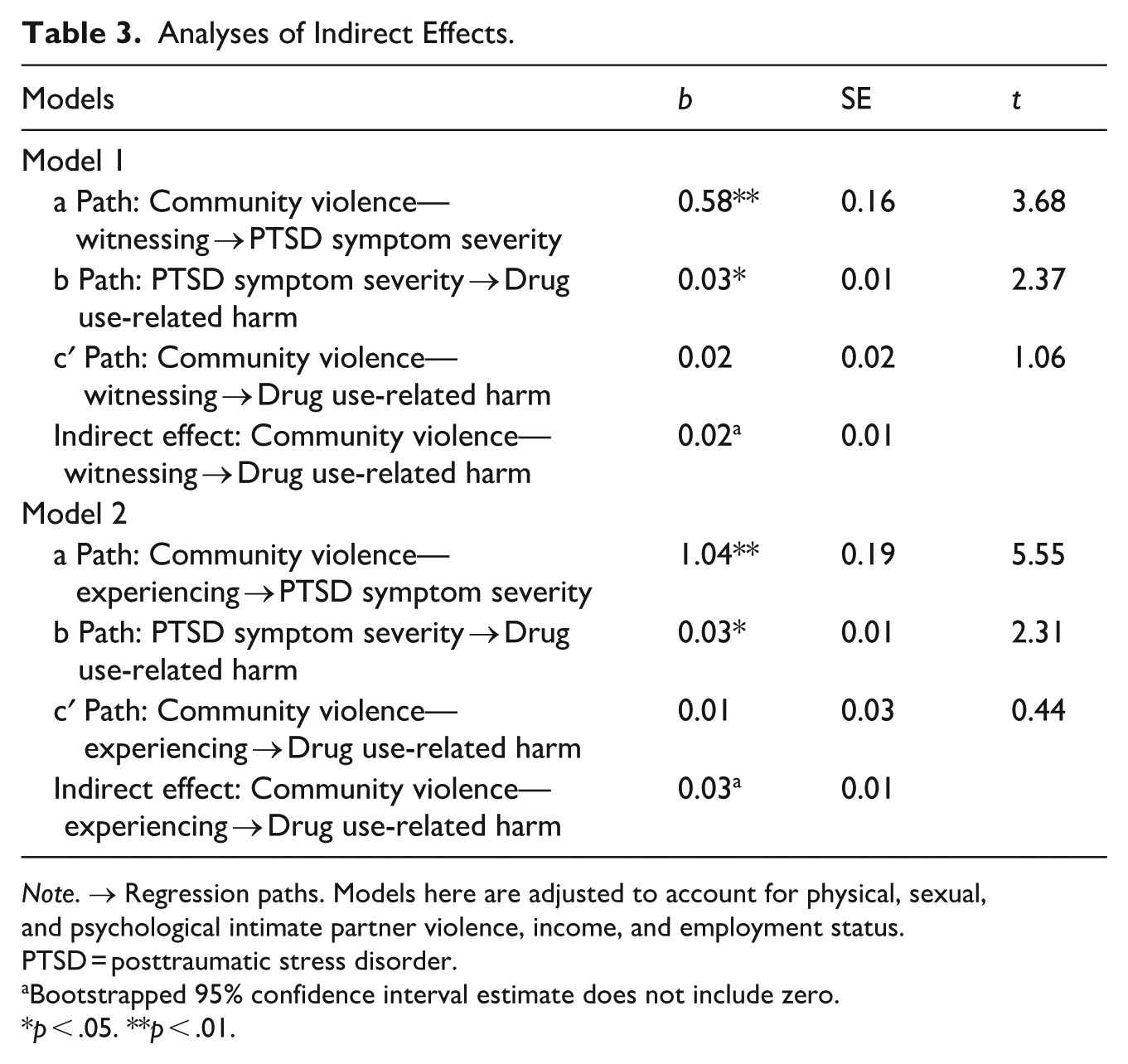
Note. → Regression paths. Models here are adjusted to account for physical, sexual, and psychological intimate partner violence, income, and employment status. PTSD = posttraumatic stress disorder.
Bootstrapped 95% confidence interval estimate does not include zero.
p < .05. **p < .01.
Experiencing Community Violence
A significant indirect effect of experiencing community violence on past-month drug use-related harm was found through PTSD symptom severity (b = 0.031, SE = 0.014, 95% CI [0.007, 0.063]) when controlling for physical, sexual, and psychological IPV; income; and employment status. Experiencing community violence was significantly associated with PTSD symptom severity (a path; b = 1.037, SE = 0.187, t = 5.549, p < .001 [0.665, 1.408]). There was a significant conditional main effect of PTSD symptom severity on drug use-related harm (b path; b = 0.030, SE = 0.013, t = 2.308, p = .024 [0.004, 0.055]), accounting for the effect of experiencing community violence. There was no significant direct effect of experiencing community violence on drug use-related harm when PTSD symptom severity was accounted for in the model (c′ path; b = 0.011, SE = 0.026, t = 0.440, p = .661 [−0.040, 0.063]). The strength and direction of findings did not change when physical, sexual, and psychological IPV were excluded from the model. 2
Discussion
The current study aimed to advance extant research on exposure to community violence, PTSD symptom severity, drug use-related harm, and their interplay within a community sample of women experiencing IPV. All primary study variables were significantly positively intercorrelated. Consistent with our hypothesis, PTSD symptom severity underlay the associations between witnessing and experiencing community violence, and drug use-related harm. Women who reported more experiences of witnessing and experiencing community violence exhibited greater severity of PTSD symptoms, which, in turn, was associated with more drug use-related harm when controlling for physical, sexual, and psychological IPV; income; and employment status. These findings are in line with prior research to suggest that individuals who are exposed to more community violence are at elevated risk for experiencing PTSD symptoms (Affrunti et al., 2018; Fitzpatrick & Boldizar, 1993; Margolin & Gordis, 2000; Resnick et al., 1993). Study findings highlight the relevance of PTSD symptoms to drug use-related harm among women experiencing IPV who also live in communities where they are exposed to community violence.
There are multiple potential avenues by which exposure to community violence may increase risk for greater severity of PTSD symptoms. For instance, individuals who live in environments with high exposure to community violence are more likely to be characterized by lower socioeconomic status, which may increase overall risk for poorer health outcomes (Centers for Disease Control, 2024b) such as PTSD symptom severity by limiting access to social, financial, and safety resources for buffering the effects of community trauma (Vincent, 2009). In the context of lower socioeconomic status, individuals exposed to community violence may also be less likely to seek out mental health services to address PTSD symptoms resultant from community trauma despite high need (Jaycox et al., 2004). This can be attributed, but not limited, to unique barriers to treatment, such as accessibility (e.g., cost, lack of transportation, and lack of childcare) and availability (e.g., lack of providers; Coombs et al., 2021; Steele et al., 2007). Moreover, frequent exposure to community violence may contribute to isolation, lower engagement within the community (Taylor & Patel, 2012), and subsequent weaken social support systems—a well-established protective buffer against the severity of PTSD symptoms (Reyes et al., 2022; Zalta et al., 2021). Finally, individuals who live in environments with heightened community violence may be more likely to experience criterion A traumatic events given overlap of event types (e.g., actual or threatened death and actual or threatened serious injury; American Psychiatric Association, 2013; Richters & Saltzman, 1990).
PTSD symptom severity may inform the relationship between community violence and drug use through the perspective of self-medication and negative reinforcement, and shared vulnerability models. According to affective processing models of negative reinforcement of drug use (Baker et al., 2004) such as the self-medication model (Khantzian, 1997), individuals may rely on drugs as means of tempering distress associated with experiencing PTSD symptoms. Within the scope of these models, exposure to community violence may trigger PTSD symptoms (e.g., hyperarousal; Phan et al., 2020; J. R. Smith & Patton, 2016), which then may prompt individuals to engage in increased drug use and experience subsequent drug-related harm. Alternatively, these relationships may be understood through the perspective of shared vulnerability, in which biological, psychological, and social factors that predispose individuals to disproportionate consequences of trauma exposure and drug use (e.g., PTSD and DUD; Elwood et al., 2009; María-Ríos & Morrow, 2020) are exacerbated by exposure to community violence. While theoretical and empirical evidence support these relations, much of the literature regarding community violence comprises youth and emerging adult samples. In addition, these relations are relatively understudied in samples of women experiencing IPV, despite existing research indicating that women experiencing IPV are at unique risk for experiencing community violence, PTSD, and drug use-related harm (Beyer et al., 2015; Dutton et al., 2006; Ogden et al., 2022; Pill et al., 2017; Raghavan et al., 2006). Indeed, it is necessary to acknowledge the potential amplification of victimization risk by virtue of exposure to violence both within the communities in which they reside (Raghavan et al., 2006; Stueve & O’Donnell, 2008) and within the home—where most acts of IPV occur (Catalano, 2006). This potential susceptibility to victimization may carry profound risk for heightened PTSD symptom severity, and the increase in utilization of drugs, in consequence, may increase risk for drug-related harm.
The present study has several research and clinical implications. While the positive relationship between PTSD symptom severity and drug use-related harm is well-documented (Haller & Chassin, 2013; Jacobsen et al., 2001; McCauley et al., 2012; Weiss et al., 2019), this study is the first known to examine these variables in relation to community violence and among women experiencing IPV. Findings provide preliminary support for PTSD symptom severity as an intermediary between exposure to community violence and drug use-related harm in a clinically relevant sample and extend accumulating research on health outcomes among women experiencing IPV. Extensions of this study may include repeated assessments of community violence exposure, PTSD symptom severity, and drug use-related harm within one’s natural environment to more accurately capture experiences and behaviors over time. Additionally, our findings contribute to a growing body of research aimed at identifying potential predictors of drug use-related harm among women who experience IPV (Sullivan et al., 2020; Weiss et al., 2022). Future investigations may examine community violence exposure and PTSD symptom severity in relation to other previously identified risk factors for drug use-related harm in this population, such as emotion dysregulation (Weiss et al., 2022), cortisol levels (Forkus et al., 2024), and avoidance coping (Flanagan et al., 2014).This may provide treatment providers with useful insight into relevant contextual, temporal, environmental, and social factors to inform treatment of PTSD symptoms and drug use in women experiencing IPV. With this insight, treatment providers may better pinpoint treatment targets unique to women experiencing IPV, with a concerted focus on individual-, interpersonal-, community-, and structural-level interventions (Raiford et al., 2013). Finally, beyond the scope of this study, findings may prompt further discussion regarding implications for policies that affect women in the community who experience IPV. The lack of consistent system-level policies for IPV screening in healthcare settings (Clark et al., 2020) poses a critical gap given the impact of IPV on overall physical and mental health. It is worthwhile to consider implementation of preventive and trauma-informed care that prioritizes expansion of IPV survivors’ roles and input and promotes stronger cross-sector advocacy and community relationships, with an orientation toward system-level social and economic factors that influence, and are influenced by, IPV (Kulkarni, 2019; Wathen & Mantler, 2022). That is, advancing streamlined pipelines of care (e.g., referral coordination and accessible patient education) across local and state community violence and domestic violence prevention initiatives, emergency and primary care settings, and behavioral health clinics, while leveraging the expertise of peer-specialists with lived experience may more effectively target these intersecting vulnerabilities.
Although this study demonstrates notable strengths, it is necessary to interpret its findings within the context of its limitations. First, the data were cross-sectional and correlational in nature, therefore precluding examination of the nature and direction of the proposed relationships and claims of causation. It is worthwhile for future studies to employ longitudinal assessment methods, such as ecological momentary assessment (EMA), to track behaviors and experiences within one’s natural environment and across time. EMA addresses limitations of cross-sectional designs, as it is less subject to memory decay/distortion (e.g., recall bias as influenced by context and one’s mental state) and heuristic (e.g., availability) bias (A. A. Stone & Shiffman, 1994; Shiffman et al., 2008). Next, the study solely relied on self-report measures. Future investigations would benefit from multimethod assessments, which may include clinical diagnostic interviews to more accurately screen for PTSD (Weathers et al., 2013a) and DUD (First et al., 2015) and comprehensively identify associated symptoms. Further, as the sample largely comprised participants who were low-income and unemployed, concerns of homogeneity of socioeconomic status across the sample may limit generalizability. Finally, while this study makes noteworthy contributions to the literature base regarding the associations between community violence, PTSD symptom severity, and drug use-related harm in a sample of historically underrepresented in research, study findings may not generalize across other (e.g., non-IPV) populations, additional subgroups characterized by IPV (e.g., individuals in same-sex relationships, men), and diverse contexts and settings (e.g., clinical, military, and college campus).
Notwithstanding these limitations, study findings extend research that identifies exposure to community violence and PTSD symptom severity as crucial factors in the development, maintenance, and intensification of drug use-related harm beyond the effects of physical, sexual, and psychological IPV. It also explores these outcomes in a clinically relevant sample of women in the community experiencing IPV. The study underscores the importance of furthering our knowledge of these concepts beyond the individual level to consider structural and systemic drivers of health disparities. Women experiencing IPV are not solely defined by their lived experiences, as these experiences do not exist in a vacuum. Therefore, enhancing our understanding of health disparities among women experiencing IPV necessitates attention toward the broader dynamic systems with which they interact to advance efforts toward dismantling structures that promote violence toward women.
Footnotes
Ethical Considerations
All procedures were reviewed and approved by the University of Rhode Island Institutional Review Board.
Consent to Participate
All participants provided written informed consent.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: This research was supported by National Institute on Drug Abuse Grant K23DA039327, awarded to Nicole H. Weiss. Work on this paper by Emmanuel D. Thomas was supported by the National Institute on Alcohol Abuse and Alcoholism Grants F31AA030502 and R25AA028464.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.