
Abstract
Intimate partner violence (IPV) has been linked to substantial physical, social, and mental health concerns across the lifespan. Health impacts of IPV are linked to economic and housing instability. Emergency shelter is primarily focused on the safety and stabilization of the most vulnerable IPV survivors. Despite frequent use of shelter interventions, little is known about the health service experiences of IPV survivors in shelters, including the extent to which these services are perceived as helpful. To address these gaps, we surveyed 214 IPV shelter residents in a Southern state. We asked socioecological and economic questions, and health conditions including food insecurity, physical health status, mental health (e.g., post-traumatic stress disorder [PTSD], depression, somatic symptoms). We asked participants about seven IPV shelter health services use and perceived helpfulness. We used bivariate and regression analysis to examine study queries. In our racially and ethnically diverse sample of mostly (95%) women, over 40% self-report a disability. Over 63% of participants met criteria for probable PTSD, 43.9% met criteria for probable depression, and 40.2% reported severe somatic symptoms. Over 59% reported very low food security. Both food insecurity and PTSD were associated with economic, sexual and physical IPV before shelter. Participants used an average of five health services in shelter, with advocacy being perceived as most helpful. Participants with poor health and/or depression were less likely to find key health services helpful. This study demonstrated the ongoing need for health services for survivors of IPV residing in emergency shelter environments. While most services are perceived as helpful, substantial gaps prevent holistically addressing survivor health concerns.
Introduction
Intimate partner violence (IPV), including physical, sexual, and psychological abuse (Lacey et al., 2012) has been consistently and robustly linked to substantial health concerns over the life course (Stockman et al., 2015). In addition to injuries like bruises, fractures, and death, physical consequences of IPV include traumatic brain injury, long-term physical disability (Loxton et al, 2017; Potter et al., 2021), cardiovascular disease, hypertension, gastrointestinal problems, reduced physical functioning, and overall poor quality of health (Loxton et al., 2017; Stockman et al., 2015). Physical and sexual IPV experiences also lead to reproductive health concerns including STIs and HIV, chronic vaginal pain, and unintended pregnancy (Fanslow, 2017). All forms of IPV are associated with mental health concerns including depression, anxiety, chronic stress and post-traumatic stress disorder (PTSD; Dokkedahl et al.., 2022; Potter et al., 2021). IPV is linked to a range of other trauma sequalae including somatic symptoms and substance misuse (Mehr et al., 2023; Ogden et al., 2022). Further, there is some evidence to suggest that a survivor may experience differential impacts based on the type of IPV (physical, sexual, psychological). Indeed, Lacey et al. (2012) found that survivors of physical IPV were at higher risk of alcohol abuse, while those experiencing psychological violence had higher rates of substance misuse and depressive symptomology. They also note the increased impact of polyvictimization (e.g., physical and sexual IPV) on a number of health outcomes.
IPV is closely linked to social isolation (Loxton et al., 2017; Potter et al., 2021) and challenges with accessing support, as well as disability due to physical or mental health conditions stemming from IPV, which furthers these impacts (Ballan et al., 2024). Additionally, disrupted social networks, lack of community support, and inadequate resources contribute to the overlapping physical and mental health challenges for survivors of IPV (Stylianou et al., 2021). Indeed, alongside their IPV-induced health complaints, survivors face economic challenges, including and perhaps especially, housing insecurity (e.g., inability to pay rent/mortgage, homelessness; Daoud et al., 2016). Other economic consequences of IPV include food insecurity and missing work or the inability to find and maintain employment due to physical or mental health challenges (Strenio, 2022; Waterman et al., 2024). Making matters worse, poor mental and physical health (often resulting from IPV) makes survivors particularly vulnerable to revictimization, which, in turn, intensifies health impacts and contributes to chronic conditions (Ørke et al., 2018). As an example, PTSD has been linked to IPV revictimization among survivors who sought out shelters (Johnson et al., 2016).
IPV Shelter
Emergency shelter, typically offered for 30 to 90 days (Stylianou & Pich, 2021) is primarily focused on safety and stabilization of the most vulnerable IPV survivors; that is, those with significant safety risks from abuse and housing insecurity. In one single day in 2024, over 50,000 survivors and their children were residing in IPV housing, with shelters being the most frequently provided service in nearly 2000 programs (National Network to End Domestic Violence [NNEDV], 2025) across the United States. The emergency shelter model is used globally to house survivors and provide comprehensive services post-violence (Sullivan et al., 2008). Shelter is more frequently used by survivors from racial and ethnic minorities, those who have experienced high levels of IPV, people who have poor mental health, and survivors living in areas with a high cost of living (Galano et al., 2013; Grossman & Lundy, 2011; McFarlane et al., 2015). Despite IPV shelter being the primary service for many survivors across the country, relatively little is known about sheltered survivors’ health conditions and outcomes. In the last 2 decades, work by both Sullivan and colleagues (Bybee & Sullivan, 2005; Sullivan & Virden, 2017) and McFarlane et al. (2014, 2015) identified sustained reductions in victimization over a 2-year period post shelter. Importantly, Bybee and Sullivan (2005) found issues linked to revictimization risk, including reduced social support, lack of resources, recent violence, and difficulty with service access. In a study of IPV shelter residents, Lyon et al. (2008) found strong satisfaction with staff and available services, which was associated with increased hope, improved self-efficacy, and greater empowerment (Sullivan & Virden, 2017). While previous scholarship indicates that shelter can be impactful at reducing revictimization risks, the health conditions and needs of residents are less known, which represents a significant gap in knowledge to inform programming and high-impact service approaches.
Health Services in IPV Shelter
Given the complex medical and mental health needs of survivors seeking shelter, many programs offer some health-related supports. These services are typically focused on immediate stabilization and reduction of re-victimization risks, including homicide prevention through safety planning (Rivas et al., 2016), food access (Brandhorst & Clark, 2022) and longer-term support to address ongoing health needs (Grace et al., 2020). Consistent with Anderson’s behavioral model of health service use (Aday & Andersen, 1974), contextual and individual predisposing, enabling, and need-based factors all cyclically influence health behaviors, healthcare access, and societal health outcomes (Krzyż et al., 2023). In the context of IPV shelters, this model highlights economic and health needs, service availability, survivor demographics, previous experience with help and health seeking, and acute and chronic experiences with violence, all shape health care access and ultimately survivor health outcomes. This model further identifies places where breakdowns in support can occur (e.g., lack of access, mistreatment from providers), which highlights the need for a range of services to meet the complex circumstances of trauma survivors, and how IPV programs can address referrals and health needs.
Health services in shelters are typically offered in a low-barrier format to enable access through case management or advocacy, and include referrals, linkage to community resources, and help accessing medication. Occasionally, onsite medical help is provided in partnership with another agency (Voth Schrag et al., 2022; Wadsworth et al., 2018). Advocacy services holistically assess survivors’ physical and mental health needs by (1) building supportive connections to reduce feelings of isolation; (2) connecting survivors with medical and substance misuse services in the community; (3) helping survivors access prescription drugs to address health symptoms; (4) facilitating support for chronic and acute conditions; and (5) providing preventative and health support treatment and evaluation (Rivas et al., 2016; Wadsworth et al., 2018; Wood et al., 2020). Further, to address survivors’ mental and behavioral health, many IPV shelters provide individual and group counseling, evidence-based therapeutic treatments, substance use interventions and support groups (Allen et al., 2021; Johnson et al., 2021). For example, trauma-focused interventions have been identified as effective approaches for reducing trauma symptoms and addressing PTSD among IPV survivors residing in shelters (Warshaw & Zapata-Alma, 2020). Similarly, shelter-based support groups have been found to enhance survivor empowerment, address isolation, and enhance well-being (Allen et al., 2021), while individual mental health interventions have been shown to reduce depression and enhance self-efficacy among survivors (Arroyo et al., 2017).
The Current Study
Prior research has shown some promise in addressing mental health and has emphasized the need for and services offered to shelter residents, yet little is known about survivors’ perceived benefits of these services (Jonker et al., 2015). Further, the extant literature is largely outdated and lacks a comprehensive assessment of health-related needs. To address these gaps in understanding, we assessed residents of IPV emergency shelter programs, including both shelters and hotel placements administered by IPV programs guided by Andersen’s behavioral model of health service use to investigate the following research questions:
(1). What are the health conditions of shelter residents, and how are IPV experiences related to health experiences?
(2). What health services do survivors use in shelter, and what do they think about those services?
(3). What are the associations of health conditions with IPV experiences and service use?
Guided by Andersen’s behavioral model of health service use, we conceptualized length of stay as an enabling factor that may facilitate engagement with available services and promote health stabilization. We hypothesized that those with longer stays would report greater service utilization and lower odds of probable PTSD and very low food security compared to shorter stays.
Methods
In a statewide collaboration to improve IPV services, we worked with coalition partners to first build an evaluative approach for non-residential IPV services (Voth Schrag et al., 2022) and then to adapt assessment tools for IPV shelter residents based on survivor advisors, interviews with former shelter residents, and staff expertise. We then worked alongside coalition partners to (1) create an online survey to assess health, safety, and economic needs typically associated with IPV victimization, as well as experiences with shelter services and (2) identify IPV shelters throughout the state based on geographic and residential diversity to field the survey.
Data Collection
A total of 25 IPV shelters in the study state agreed to share our study materials with their residents. Shelter programs shared the study opportunity with residents via print and electronic fliers, text messages, and email. We conducted online meetings with shelter sites to discuss the study, survey questions, and eligibility criteria. Shelter sites shared the opportunity by posting in common areas, announcing the study in house meetings, and through individual reach outs and meetings with clients. Participants were eligible for the survey if they were (1) 18 and older; (2) currently or recently (within 30 days) residing in an IPV shelter or a hotel provided by an IPV program; and (3) able to complete the survey in English or Spanish. Potential participants took a brief eligibility assessment, allowing us to identify ineligible and potentially duplicative entries. We sent eligible participants a web link to the survey in their preferred and safe contact format (e.g., text or email). The survey was programmed in secure software (e.g., Qualtrics), with the consent form preceding the survey questions. Of the 25 IPV shelters who agreed to participate, we received surveys from residents from 19 IPV shelters. On average, participants completed the survey in 20 min. Participants were provided a gift card as a thank you for completing the survey.
Measures
Socioecological Items
We assessed participant age, gender identity, race/ethnicity, sexual orientation, education, and self-disclosed disability or mental health condition. To allow for meaningful comparisons across the sample, we categorized age into four quartile-based groups (18–27, 28–35, 36–43, and 44 or older) with approximately equal numbers of participants per group. We asked participants to self-report their monthly income, employment status, access to reliable transportation, and the number of times they had experienced homelessness. Lastly, we asked participants about the parenting status of minor children.
Shelter Experiences Assessment
We developed and refined programmatic experiences assessments through two previous statewide surveys developed with advocates and survivors (Voth Scrag et al., 2022). For the purposes of this study, we defined “health-related services” broadly to include both direct clinical services (e.g., counseling, psychiatric prescription assistance, health referrals) and health-enabling advocacy services (e.g., safety planning, case management). This definition reflects the interconnected nature of safety, mental health stabilization, and physical health access within IPV emergency housing settings, guided by our previous qualitative work (Voth Schrag et al., 2022; Wood et al., 2020). We assessed utilization of health-related services, including mental health, in shelter by asking participants to report their use of seven different services, including (1) advocacy (case management), (2) support groups, (3) psychiatric prescription access assistance, (4) mental health referrals, (5) counseling, (6) referral for physical health services, and (7) safety planning. For each service, we asked participants to indicate whether they had used it (yes/no) and rated its helpfulness on a scale from 1 (very helpful) to 5 (not at all helpful). For analyses, perceived helpfulness was dichotomized into “helpful” and “not helpful.” We created a composite variable to reflect the total number of services used. Additionally, we created a categorical variable to group participants based on service usage: three or fewer services, four to five services, or six or more services.
Intimate Partner Violence
We used behaviorally specific items (n = 24) adapted from the National Intimate and Sexual Violence Survey (Kresnow et al., 2021) to assess IPV before coming to shelter. Specifically, we assessed physical violence (6 items), psychological abuse (4 items), sexual assault (3 items), economic abuse (4 items) and stalking (7 items).
Food Security
We assessed household food security using the six-item USDA Food Insecurity Scale (2012). We summed the total number of affirmative responses to generate a raw score ranging from 0 to 6, with 0–1 indicating high or marginal food security, 2–4 indicating low food security, and 5–6 indicating very low food security, the most severe category. Accordingly, we created a binary variable in which households with very low food security (raw score 5–6) were coded as 1, and all others were coded as 0.
Posttraumatic Stress Disorder
We assessed PTSD symptoms using the PTSD Checklist for DSM-5 (Blevins et al., 2015). Participants endorsed symptoms based on their experiences, with responses indicating the presence of PTSD symptoms. A probable PTSD classification was assigned to individuals who endorsed at least four out of five key symptom criteria. For analysis, we created a binary variable in which individuals meeting the threshold for probable PTSD (≥4 symptoms) were coded as 1, and all others were coded as 0.
Depression
We assessed depression using the eight-item version of the Patient Health Questionnaire (PHQ-8) (Kroenke et al., 2008). Participants reported how often they had experienced depressive symptoms over the past 2 weeks, with response options of “not at all” (0), “several days” (1), “more than half the days” (2), and “nearly every day” (3). Total scores ranged from 0 to 24, with higher scores indicating greater depression severity. Following recommendations from the Rapid Variable Selection method, we used a cutoff score of 10 to identify probable depression (Wu et al., 2020).
Severe Somatization Symptoms
We assessed somatic experiences using the 15-item Patient Health Questionnaire (PHQ-15). Participants reported the frequency of experiencing various physical symptoms, with response options of “not at all” (0), “several days” (1), and “more than half the days” or “nearly every day” (2). Total scores ranged from 0 to 30, with higher scores indicating greater somatization severity. A cutoff score of 15 was used in the current study to identify severe levels of somatization (Kroenke et al., 2002).
Physical Health Perception
We assessed physical health status using a single-item measure, which asked participants about their overall physical health since staying at the shelter. Response options ranged from 1 (Excellent) to 5 (Poor). For analyses, a binary variable was created, grouping responses into “Excellent/Very Good/Good” and “Fair/Poor” to distinguish better versus worse perceived physical health (Ware et al., 2000).
Current Health Insurance Status
We assessed health insurance by asking participants a single item. For analyses, responses were treated as a binary variable, with “yes” indicating insured and “no” indicating uninsured.
Data Analysis
A total of 241 participants completed the survey. Missing data were minimal across survey responses, ranging from 0% to 4.56% across included analytic variables (n = 11). We used listwise deletion to handle missing data, resulting in a final analytic sample of 214 participants. We first conducted bivariate analyses to examine associations between health needs and socioecological factors. Next, we used bivariate analyses to explore survivors’ utilization of and perceived helpfulness of IPV-related health services by health needs. Key variables identified in these analyses were included in two hierarchical logistic regression models examining the association between socioecological and service-related factors with two health outcomes: PTSD and food insecurity. Multivariable analyses focused on probable PTSD and very low food security due to their high prevalence in shelter populations and their strong theoretical relevance as trauma-related and material hardship outcomes. In these models, Block 1 included socioecological variables, and Block 2 incorporated IPV-related health service variables. To ensure proper model specification, we performed link tests. Socioecological variables that were not significantly associated with health outcomes in bivariate analyses were excluded from subsequent hierarchical regression models. Housing type was examined descriptively but not included in multivariable models due to limited statistical power and high similarity in service access across housing types.
Results
A total of 214 participants were included in analysis. As shown in Table 1, most participants (95.3%) identified as women and were racially and ethnically diverse, mirroring the study state. Participants were 18 to 61 years old, with approximately one-third aged 39 years or older (36.0%). Most participants (83.7%) identified as heterosexual or straight. A slight majority of participants had minor children (57.5%). Over 40% of participants self-reported having a diagnosed disability or impairment, with 11% reporting two or more diagnosed disabilities. The most frequently reported disability was a mental health condition (29.8%). Participants also had extensive histories of IPV victimization, with nearly all (97.2%) reporting experiencing at least one type of IPV prior to entering the shelter. Economic challenges were pervasive, with 67.3% of participants reporting a monthly income of less than $500 and 72.9% reported being unemployed. Approximately 40% of participants indicated that they rarely or sometimes had reliable transportation. A large majority (87.4%) of participants reported experiencing homelessness or having to stay in a shelter, outside, or with friends and family at least one time. Most had been in shelter for 1 to 3 months (50.0%), followed by less than 1 month (36.5%) and 4 or more months (13.6%). See Table 1 for more information.
Key Demographic Characteristics (n = 214).
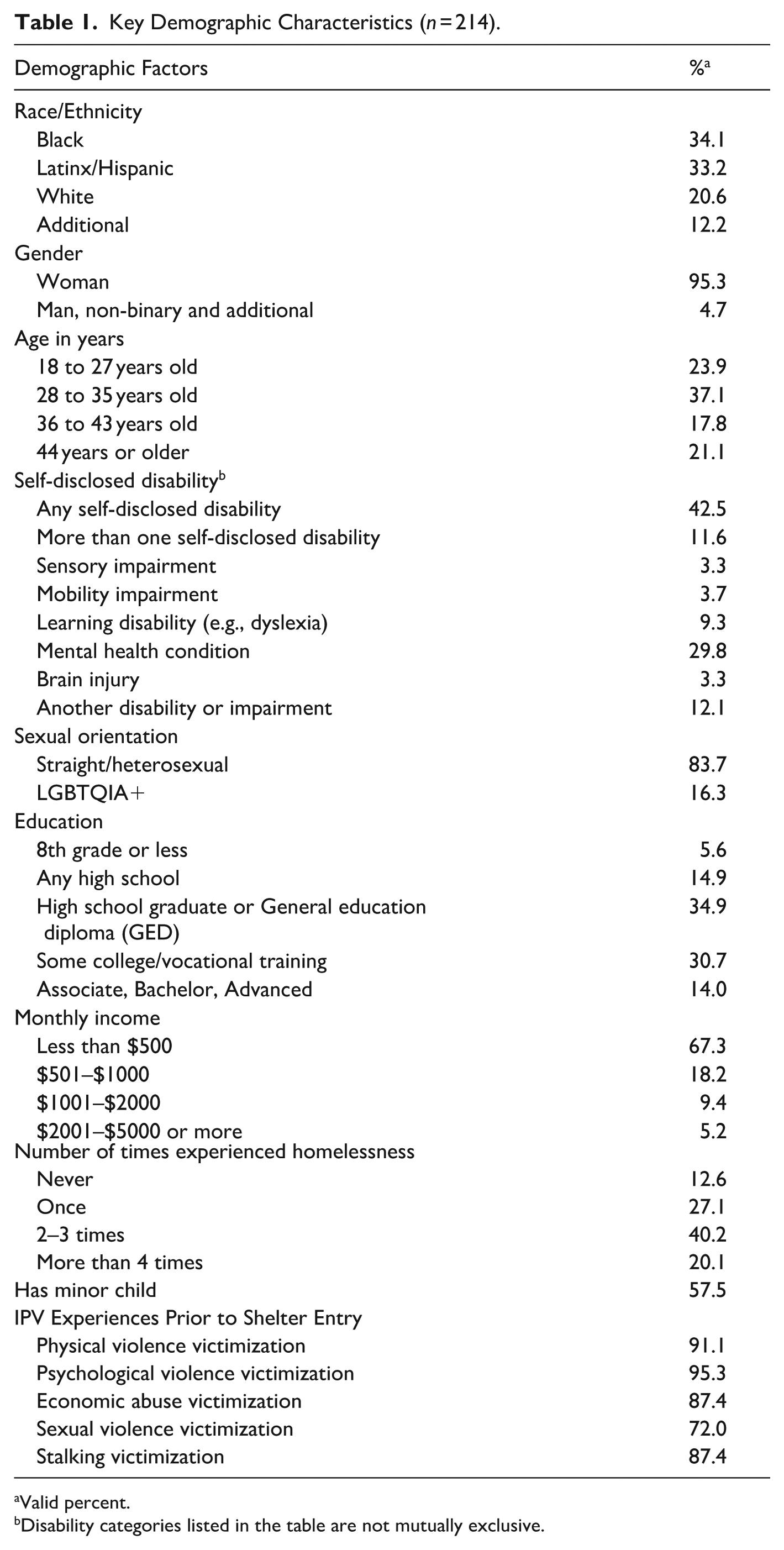
Valid percent.
Disability categories listed in the table are not mutually exclusive.
Health Conditions of IPV Shelter Residents
As shown in Table 2, 63.6% of participants met criteria for probable PTSD, 43.9% met criteria for probable depression, and 40.2% reported severe somatic symptoms. A sizable minority of participants were likely comorbid for both PTSD and depression (36.9%), and PTSD, depression, and somatic complaints (24.8%). Additionally, 35.1% of participants reported poor or fair physical health since entering the shelter, while 59.1% reported very low food security. See Table 2 for more on health conditions. Very low food security affected 58.9% of participants, indicating severe material hardship even while residing in a shelter. Severe somatic symptoms were reported by 40.7%, and 35.1% described their overall physical health as fair or poor. Less than half of participants (44.4%) reported having current health insurance.
Health Conditions by Socioecological Factors (N = 214).
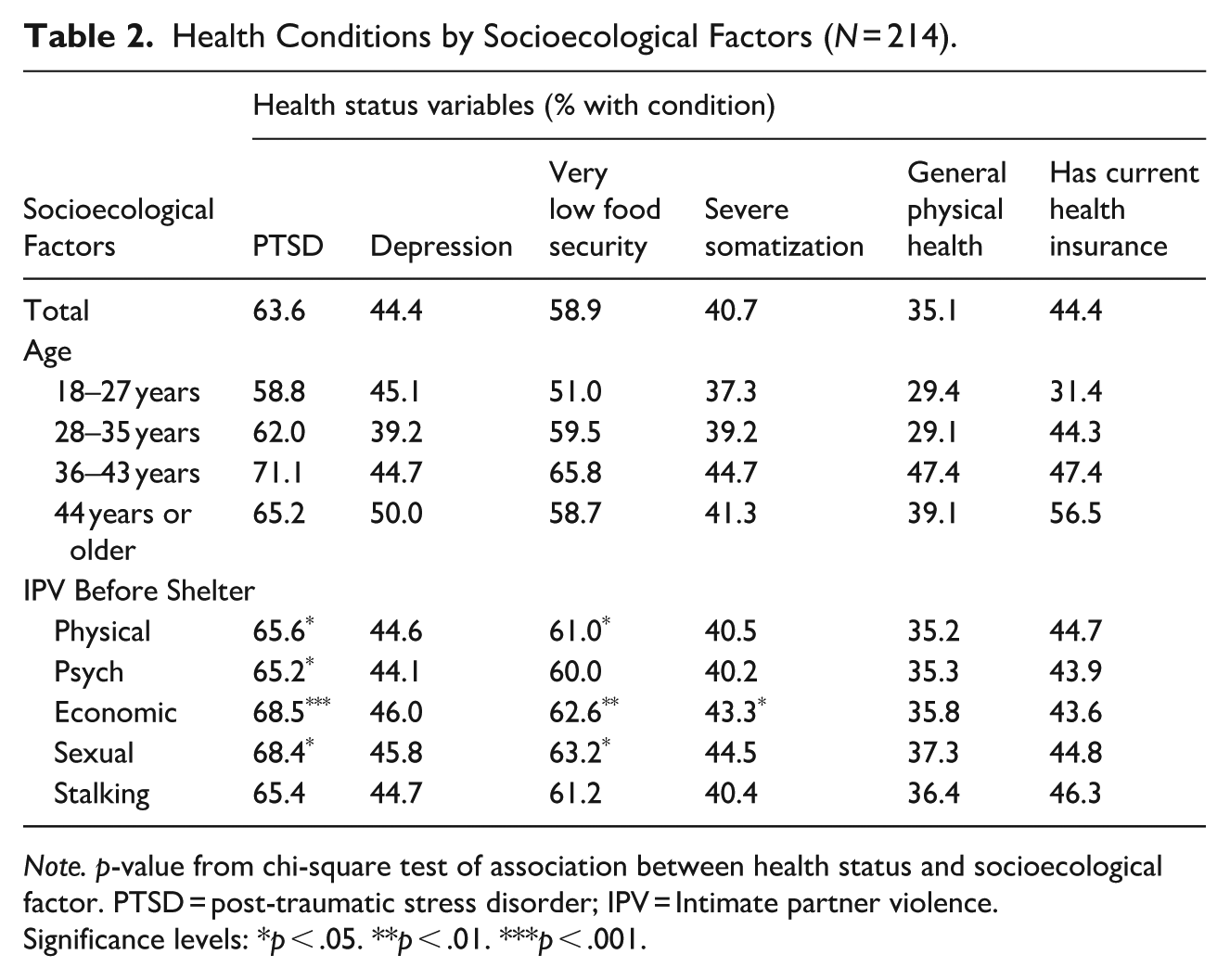
Note. p-value from chi-square test of association between health status and socioecological factor. PTSD = post-traumatic stress disorder; IPV = Intimate partner violence.
Significance levels: *p < .05. **p < .01. ***p < .001.
Rates of PTSD and food insecurity were consistently higher among those reporting economic abuse prior to shelter entry (68.5% and 62.6%, respectively). Economic abuse demonstrated the most consistent and strongest associations across health outcomes relative to other forms of IPV.
IPV Experiences and Health Conditions
As shown in Table 2, PTSD symptoms and food insecurity were significantly associated with IPV victimization prior to shelter entry. Participants with probable PTSD were significantly more likely to have experienced economic IPV (68.5% vs. 31.6%, p < .001), psychological IPV (65.2% vs. 34.8%, p < .05), physical IPV (65.6% vs. 34.4%, p < .05), and sexual IPV (68.4% vs. 31.6%, p < .05) prior to shelter entry compared to those without probable PTSD. Similarly, participants who reported significantly higher rates of very low food security had significantly higher rates of economic abuse (62.6% vs. 37.4%, p < .01), sexual IPV (63.2% vs. 36.8%, p < .05), and physical IPV (61.0% vs. 39.0%, p < .05) prior to shelter entry compared to those with greater food security. Participants with severe somatization also reported significantly higher rates of economic abuse compared to those without severe somatization (p < .05). It is important to note that there was significant overlap in previous violence experiences, with 93.0% of participants experiencing two or more types of IPV prior to entering shelter. Depression, general physical health, and health insurance status were not significantly associated with any form of IPV victimization prior to shelter entry.
Extent of Health Service Utilization
As shown on Tables 3 and 4, participants used between 0 and 7 health services (M = 5; SD = 1.97). Case management (advocacy) was the most frequently utilized health service (87.9%), with a vast majority of residents (83.0%) reporting it as helpful. Participants in poor or fair health were less likely to perceive case management as helpful compared to those in good or excellent health (30.8% vs. 69.2%, p < .05). Safety planning was used by 85.0% of participants, with 79.1% finding it helpful. Participants with probable depression reported less use of safety planning services compared to their non-depressed counterparts (43.1% vs. 59.9%, p < .001). Counseling was used by 82.7% of participants, with 76.8% finding it helpful. Individuals in poor or fair health (26.5% vs. 73.5, p < .001) and participants with depression (40.4% vs. 59.6, p < .05) who utilized services were less likely to find counseling services helpful.
IPV Shelter Health Service Matrix and Health Conditions (PTSD, Depression, Food Security, Somatic Symptoms, Health, and Health Insurance Status).
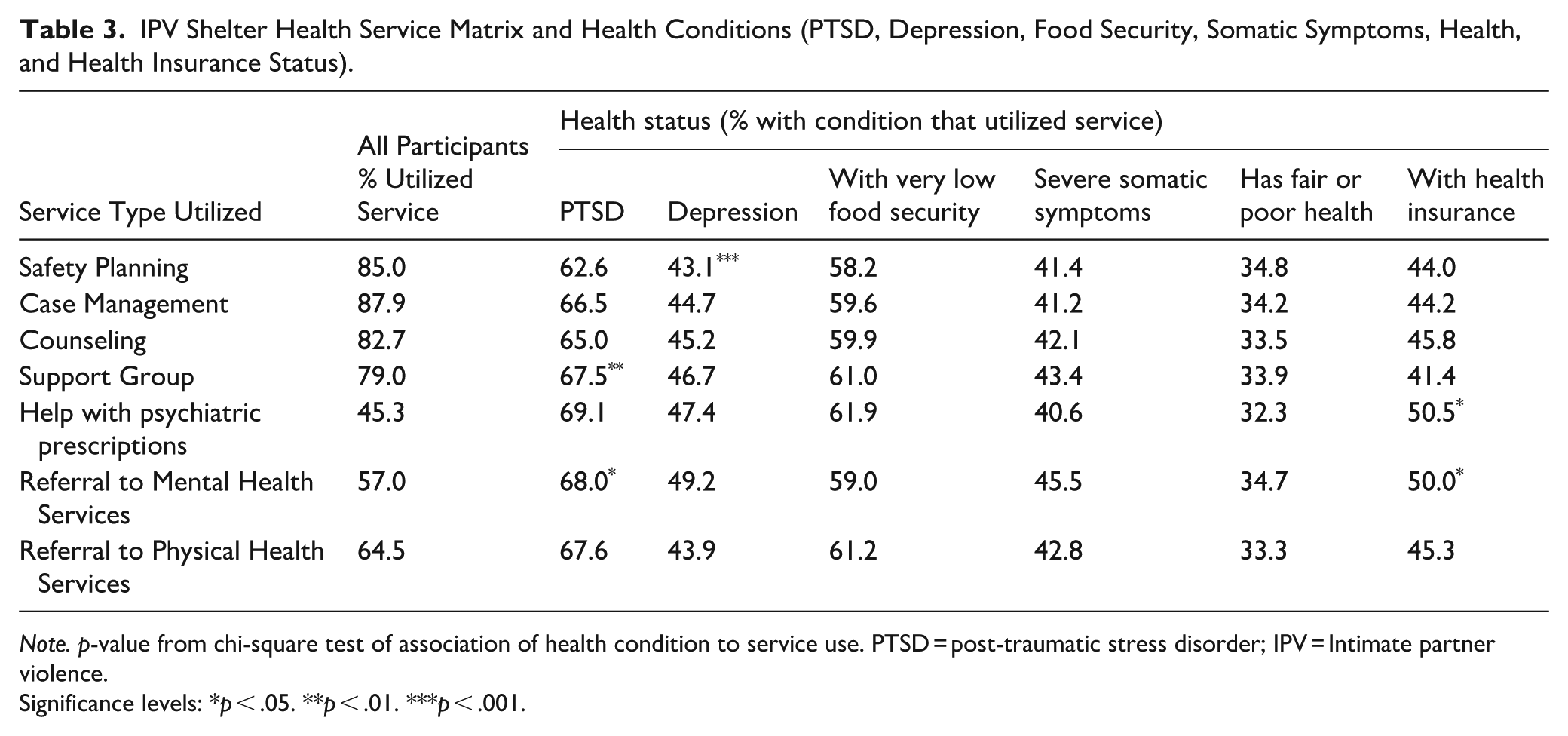
Note. p-value from chi-square test of association of health condition to service use. PTSD = post-traumatic stress disorder; IPV = Intimate partner violence.
Significance levels: *p < .05. **p < .01. ***p < .001.
Perceived Helpfulness of IPV Shelter Health Services and Health Conditions (PTSD, Depression, Food Security, Somatic Symptoms, Health, and Health Insurance Status).
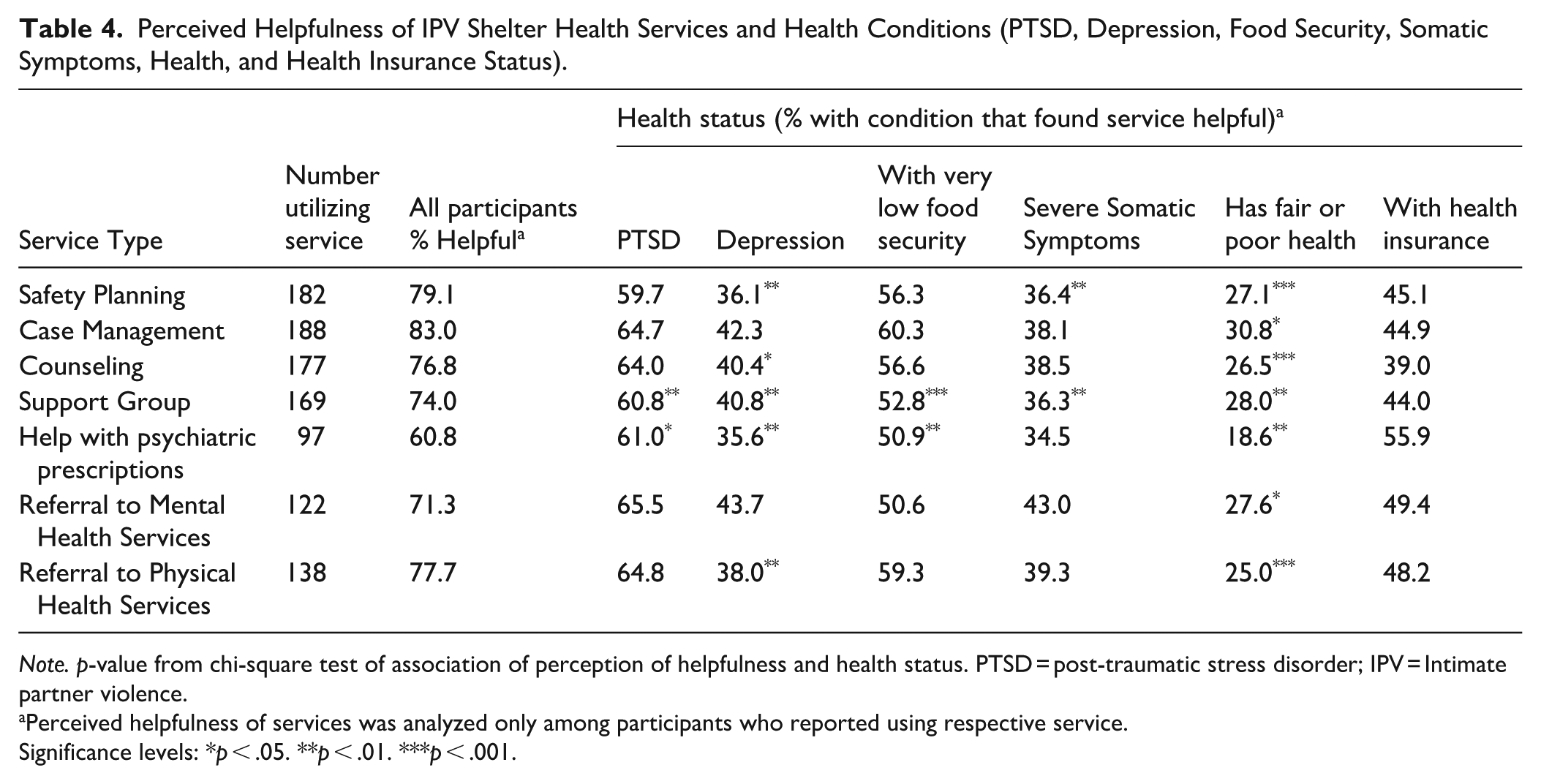
Note. p-value from chi-square test of association of perception of helpfulness and health status. PTSD = post-traumatic stress disorder; IPV = Intimate partner violence.
Perceived helpfulness of services was analyzed only among participants who reported using respective service.
Significance levels: *p < .05. **p < .01. ***p < .001.
Support group services were used by 79.0% of participants, with 74.0% reporting them as helpful. Participants with probable PTSD had significantly greater use of support group services compared to those without probable PTSD (67.5% vs. 32.5%, p < 0.01) and were also significantly more likely to perceive them as helpful (60.8% vs. 39.2%, p < .01). Similarly, survivors in IPV shelters experiencing very low food security were more likely to report support groups as helpful compared to those with greater food security (52.8% vs. 47.2%, p < .001). In contrast, participants with depression (40.8% vs. 59.2%, p < .01) and severe somatic symptoms (36.3% vs. 63.7%, p < .01) who utilized services were less likely to find support group services helpful. Additionally, individuals in poor or fair health were less likely to perceive support group services as helpful compared to participants in better health (28.0% vs. 72.0, p < .001).
Psychiatric prescription access assistance was utilized by 45.3% of participants, with 60.8% reporting it as helpful. Participants with PTSD were more likely to find this service helpful compared to those without PTSD (61.0% vs. 39.0%, p < .05). However, individuals with depression compared to those without depression (35.6% vs. 64.4%, p < .01) reported lower perceived helpfulness of psychiatric prescription assistance.
Referrals for mental health services were utilized by 57.0% of participants, with 71.3% finding them helpful. Referrals for physical health services were accessed by 64.5% of participants, with 77.7% reporting them as helpful. Survivors without depression were more likely to find these referrals helpful compared to those with depression (62.0% vs. 38.0%, p < .01).
Overall, survivors with probable PTSD reported greater use of health-related services in IPV shelter—particularly support groups and psychiatric prescription assistance—and generally found these services helpful. In contrast, those with probable depression, poor or fair health, or very low food security reported lower perceived helpfulness of several health services, including case management, support groups, counseling, and mental health referrals. Importantly, high utilization rates were observed across nearly all health conditions, suggesting that shelters are actively engaging survivors with varying health profiles in available services.
Associations of Health Conditions With Prior IPV Experience and Service Use
PTSD
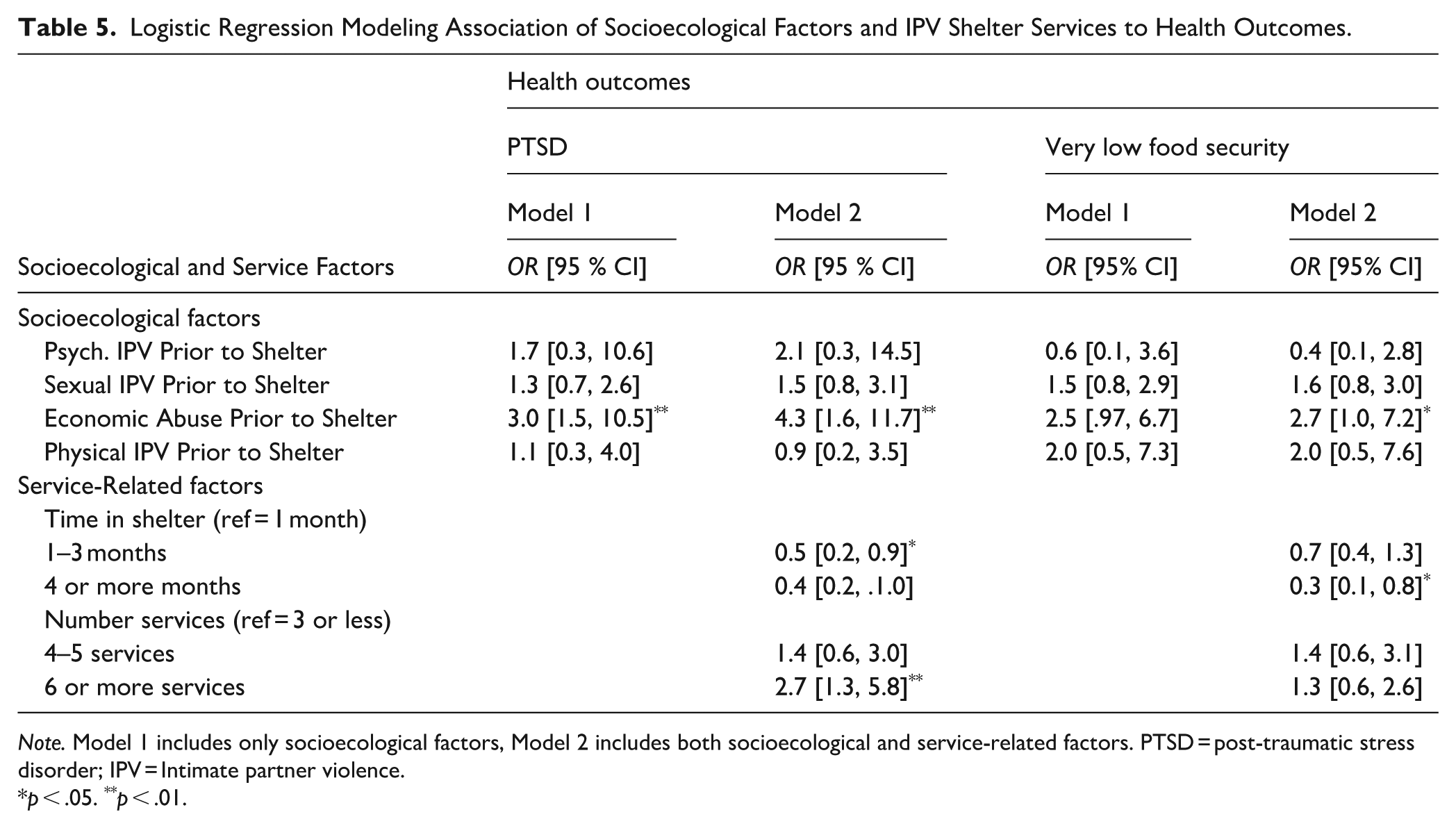
Given the high overall levels of service engagement and perceived helpfulness, regression analyses were conducted to explore whether specific IPV experiences or patterns of service use were associated with key health outcomes (PTSD and very low food security). Regression results are presented in Table 5. The first step included previous victimization variables. Experiencing economic abuse prior to coming to shelter (OR = 3.00; 95% CI [1.49, 10.54], p < .05) was associated with higher odds of probable PTSD. The second and final step added IPV health service variables to the overall model and was significant: χ2(8) = 28.45, p < .001. In this model, prior economic IPV remained significant. High levels of service use (i.e., using 6 or more services) was associated with higher odds of probable PTSD compared to those who with lower levels of service use (i.e., 3 or fewer services; OR = 2.73 [1.28, 5.84], p < .05). Staying in shelter for 1 to 3 months was associated with lower odds of probable PTSD compared to those who stayed in shelter less than 1 month (OR = 0.49 [0.24, 0.97], p < .05).
Logistic Regression Modeling Association of Socioecological Factors and IPV Shelter Services to Health Outcomes.
Note. Model 1 includes only socioecological factors, Model 2 includes both socioecological and service-related factors. PTSD = post-traumatic stress disorder; IPV = Intimate partner violence.
p < .05. **p < .01.
Very Low Food Security
We used logistic regression analysis to examine associations between key socioecological factors and IPV shelter health services and food security (see Table 5). The first step included previous victimization variables. In this step, none of the variables was significantly associated with very low food security. For the second and final step, we added IPV shelter health service variables to the overall model. In this model, experiencing economic abuse prior to coming to shelter was associated with very low food security (OR = 2.71, 95% CI [1.02, 7.24], p < .05). Staying in shelter for 4 or more months compared to less than 1 month was associated with decreased odds of reporting very low food security (OR = 0.32 [0.13, 0.80], p < .05).
Discussion
In our diverse sample of IPV shelter residents, health-related services are frequently accessed. Over 87% used advocacy or case management services, 82.7% counseling, and 64.5% received referrals to physical health services. Of the seven health services we assessed, all were considered helpful by the majority of participants, with case management/advocacy, safety planning, and counseling having the highest rates of perceived helpfulness. Surprisingly, in this study, length of time was not associated with service access, indicating that shelters are engaging survivors on their health needs at all parts of their stay. Extending Anderson’s model, this suggests survivors may have shifting health-related needs throughout the shelter stay that drive health service access. Advocacy was unsurprisingly considered the most helpful of health-related services while in shelter. This finding matches previous research indicating the salient role of advocates in addressing the multifaceted needs of survivors (Grace et al., 2020; Wood et al.,2020), through a model focused on voluntary engagement of survivor-driven needs (Goodman et al., 2016; Wood et al., 2020). Our findings suggest that survivors choose to engage on their health needs specifically while in shelter, and frequently with the assistance of an advocate. This finding underscores the importance of what Goodman et al. (2016) have referred to as “the alliance” or the connection between staff and survivors in IPV-focused agencies to assess and address needs. This connection is associated with reduced depression and PTSD symptoms (Goodman et al., 2016) and more needs being met (Wood et al., 2022).
We found high rates of probable depression (43.9%) and PTSD (63.6%), as well as fair or poor physical health (35.1%). Survivors with probable PTSD, relative to those without, reported more economic, sexual, physical, and psychological IPV and used more health-related services in IPV shelter—both directly and by referral. Shelter stays of 1 to 3 months were associated with lower odds of probable PTSD relative to stays under 1 month. However, length of stay is influenced by multiple contextual factors—including housing availability, safety risk, and programmatic policies—and therefore should not be interpreted as causally reducing PTSD symptoms. It may instead reflect stabilization processes or survivor circumstances that facilitate engagement with services In line with Anderson’s behavioral model of health services, access to support (via longer shelter stays and factors like mental health support, support groups, and medication assistance) may be a factor contributing to this enhanced mental health stabilization and increased safety (Fernández-González et al., 2019; Wood et al., 2022; Yakubovich et al., 2022). Promoting low-barrier access to health resources has been identified as a critical component of effective public health approaches in low-resource settings (Jacobs et al., 2012). It is possible that longer shelter stays (or accessible transition to other longer-term housing models) may facilitate trauma recovery and promote consistent engagement with mental health support and coping strategies, all of which are protective against future revictimization.
Economic IPV was linked to two core health outcomes, probable PTSD and food insecurity, indicating the pervasive nature of IPV with financial instability. Notably, IPV shelter is an intervention primary for survivors experiencing both financial insecurity and safety concerns, comprising a specific high-risk subset of victims. A crucial finding related to effective health service engagement is that over half the sample (55%) did not have health insurance and had a monthly income (67%) under $500. Without income or insurance coverage, preventative and indicated treatments are difficult to obtain, which subsequently results in worsening physical and mental health. Transportation access, a significant issue for participants of this study, likely impacts access to medical care. This reality underscores the role of broader economic and systemic barriers that constrain survivors’ ability to effectively engage with healthcare. Indeed, Letourneau et al. (2022) posit that increased health insurance coverage could reduce IPV by increasing health services, reducing health-related financial stressors, and increasing care access, and thus IPV identification and response. This same notion can be applied to IPV shelter residents (i.e., increased access to healthcare can serve to prevent revictimization). Addressing the impact of economic IPV should include health assessment and care access.
Food insecurity, a seldom-addressed issue among IPV survivors, was a significant concern for the majority of study participants as it was associated with economic, sexual, and physical IPV. Coupled with the economic and housing insecurity in our shelter sample, these findings highlight not only the impact of economic IPV, but the interconnected and detrimental impact of financial insecurity and food access on survivors’ health status. Studies have begun to show interconnections between food insecurity, health, and IPV (Brandhorst & Clark, 2022; Waterman et al., 2024), especially for survivors of color who are economically disadvantaged and for those living with HIV (Fedina et al., 2022). Services in shelter focused on access to housing, nutrition assistance, food bank linkage, flexible financial assistance, and employment support can contribute to both positive economic and health outcomes for IPV survivors.
Survivors reported high rates of severe somatization, underscoring the link between survivors’ mental and physical health, and emphasizing the need to holistically respond to survivor health in the shelter context. Previous studies have demonstrated that survivors of IPV have higher rates of physical somatic complaints (e.g., pain or fatigue) than their non-victimized counterparts, as well as higher levels of somatic-cognitive complaints (e.g., issues with attention, forgetfulness; Machorrinho et al., 2025). Advocacy focused on accessing and negotiating health systems (sometimes called navigation) could support the engagement of IPV survivors with health services while in shelter, including those focused on their mental health needs (Drouin et al., 2023), and address both physical and cognitive somatic concerns. Culturally specific services and trauma-informed services can also positively impact traumatic somatic experiences (Serrata et al. 2020).
Limitations and Future Research Needs
While our study has many strengths, including a focus on health conditions and services in a high-risk sample of IPV survivors, there are several important limitations to note. First, the cross-sectional nature of the study limits our ability to observe temporality in health changes and service use. Future studies should examine the long-term impact associated with health service use in IPV shelters. As other scholars have noted (Klein et al., 2021; Yakubovich et al., 2022) there is dearth of longitudinal assessment related to IPV shelter stays. Future mixed methods longitudinal work would allow us the ability to examine Anderson’s model more robustly, including the cyclical nature of predisposing characteristics, resources, and need factors. Second, the study could be improved with qualitative interviewing to add explanation to why services were (or were not) helpful based on different health needs. Third, future studies will benefit from a greater degree of physical health data, as well as a wider geographic diversity. Indeed, the availability and depth of service response varies from state to state (NNEDV, 2025), meriting a national look. Fourth, given the high level of polyvictimization in this sample, statistical independence among IPV categories was limited, which may have reduced our ability to detect unique effects of specific IPV types in multivariable models; although several IPV forms were associated with PTSD and food insecurity at the bivariate level, only economic IPV remained significant in adjusted analyses and the study may have been underpowered to detect smaller independent effects. Finally, our study is limited by the inherent challenges of self-report data.
Implications and Conclusions
This study demonstrated the ongoing need for health services for survivors of IPV residing in emergency shelter environments. High rates of mental health challenges, trauma symptoms, somatization, lack of health care access, and income and food insecurity point to overlapping health and well-being challenges that influence long term survivor and societal outcomes.
This study strongly supports the need for clinical mental health support in IPV shelters and community agency partners. By embedding effective individual and group supports and building community referral pathways, shelters can overcome gaps in the larger mental and physical health response system, including factors like lack of insurance or financial capacity to access services. By implementing interventions that have been demonstrated to reduce trauma symptoms and increase survivor-wellbeing, IPV shelter programs could overcome critical barriers to long-term health and wellbeing.
Additionally, our findings indicate that IPV shelter residents with symptoms of depression may need additional engagement on health issues. While PTSD symptoms may drive health service engagement both in shelter and by referral, our results indicate that probable depression and poor physical health may be associated with less health service engagement and less perceived helpfulness of key services (e.g., safety planning, support groups, case management), that are associated with reductions in revictimization and improved health. IPV shelter staff may benefit from additional strategies to engage residents struggling with depression and poor physical health, including trauma-informed counseling, psychoeducation, and skill-building sessions. These services should be provided in culturally responsive and language accessible formats, including support groups to reduce isolation and build resilience, and complementary and somatic therapies (e.g., yoga, mindfulness, expressive therapies), which can work in tandem to build resilience, and reduce trauma symptomology (Vroegindewey & Sabri, 2022). Study findings highlight the importance of embedding responsive physical health and mental health supports and economic interventions within shelter systems to promote health, safety, economic stability, and empowerment.
Without access to effective supports to ensure immediate safety and address factors contributing to their long-term economic stability, revictimization risks remain elevated and cycles of poverty and trauma persist. While we found robust engagement on addressing mental health needs, physical health concerns may merit more focus in IPV shelter service provision. Traditionally, IPV services focus on physical health by addressing post-assault injury and risk for homicide, but with less of a focus on longer-term health needs. Further, survivors report disengagement from medical care due to discrimination, negative experiences, and minimization of abuse impacts (Hargrave et al., 2024). The need for more health care focus in shelter services (Mantler et al., 2020) and for more partnerships between shelters and healthcare providers (Jagasia et al., 2023) have been documented. Given reports of disability, poor physical health, and potential impacts of food insecurity, a focus on health conditions could help to improve survivor stability, prevent revictimization, and facilitate a higher quality of life.
Footnotes
Acknowledgements
The authors wish to thank the shelter programs, state coalition, and study participants who offered their time and expertise.
Ethical Considerations
In accordance with the standards set forth in the Belmont Report, this study was approved by the corresponding author’s IRB at the time of data collection, the University of Texas Medical Branch. The corresponding author is currently at the University of Texas Health Science Center in Houston.
Consent to Participate
All study participants provided their consent for participation.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: This project was funded by the Center for Violence Prevention/ Violence and Injury Prevention Research Center.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to partnership agreements and confidentiality protections.