
Abstract
Although women of all ages are at risk of being killed by an intimate partner, little attention has considered intimate partner homicide (IPH) against older women. Existing research suggests IPH characteristics differ between younger and older women, but no work has considered whether these characteristics vary across older women by age. Current work is hindered by the tendency to define “older women” using a single age category (such as over age 50). This practice implicitly equates women in their 50s with those 80 or older and likely masks key differences. This brief note uses incident data from the National Violent Death Reporting System to explore whether characteristics of IPH against older women vary across age subgroups. Findings obtained from descriptive statistics highlight clear distinctions between women in their 50s and 60s and those over 70. IPH against women in their 50s and 60s was more likely to involve prior intimate partner violence as compared to incidents involving women over age 70. In contrast, IPH against women over age 70 was more likely to involve a homicide-suicide or an intimate partner who was a caregiver as compared to women in their 50s or 60s. While firearms were used in a majority of IPH incidents for all age subgroups, the proportion of firearm-involved IPH increased with age. Overall, the findings emphasize the need to incorporate age in studies of IPH against older women. To illustrate opportunities for such work, this brief note discusses avenues for future research to investigate these findings and IPH risk factors with age subgroups in mind.
Introduction
Women are at a greater risk of being killed by an intimate partner than by any other perpetrator (Bureau of Justice Statistics, 2022; Campbell et al., 2007). Despite extensive research devoted to understanding intimate partner homicide (IPH), little attention has focused on victims who are older women (MacPherson et al., 2020; Roberto et al., 2013; World Health Organization [WHO], 2024). This work is needed as women over 50 represent one of the fastest growing demographics in the United States (Vespa et al., 2020), and older women remain at continued risk of IPH (Dawson, 2021). Studies also suggest that IPH characteristics differ between older and younger women (MacPherson et al., 2020; Salari & Maxwell, 2016). For example, a history of intimate partner violence (IPV) is observed less often in IPH against older as opposed to younger women (MacPherson et al., 2020). 1 In contrast, IPH against older as compared to younger women is more likely to involve intimate partners who are the victim’s caregiver (MacPherson et al., 2020) and intimate partner homicide-suicides (IPHS; Salari & Sillito, 2016). While firearm-involved IPH is observed for both younger and older women, firearms are commonly used to commit IPH against older women and almost exclusively used in IPHS involving older women (MacPherson et al., 2020).
A challenge in studying IPH against older women is how “older women” are defined. No age demarcation consistently identifies who is an older adult (Addington, 2013). As a result, various ages between 50 and 65 have been used to define older women (Crockett et al., 2015). Recent IPV studies have started to converge around age 50 to identify postmenopausal women (Meyer et al., 2020) and to rectify the frequent exclusion of women over 50 in health research (WHO, 2007). No matter what age demarcation is used, researchers typically group older women into a single category (i.e., all women over age 50; Salari & Maxwell, 2016). This practice results in a measure that implicitly equates women in their 50s with those 80 or older and masks age-based patterns (Addington, 2013; MacPherson et al., 2020).
This brief note seeks to explore whether previously identified characteristics of IPH against older women vary across age subgroups. To date, no research has considered this issue despite the likelihood that age-related differences influence these characteristics (Salari & Maxwell, 2016). The goal of this study is to generate foundational knowledge regarding age subgroup patterns to guide research on the characteristics and risk factors associated with IPH against older women. Identifying this future work is important as it could ultimately inform prevention efforts tailored to the experiences of older women as opposed to current strategies that focus on risks associated with younger women (Salari & Maxwell, 2016).
Methodology
Data
The current study used 3 years (2017–2019) of pooled data from the restricted-use National Violent Death Reporting System (NVDRS; Centers for Disease Control and Prevention [CDC], 2023). These specific years were selected as part of a larger research project examining fatal and nonfatal violence against older women. The NVDRS is the Centers for Disease Control and Prevention’s incident-based surveillance system of homicides and other violent deaths (CDC, 2022). NVDRS quantitative variables are derived from details gathered by trained data abstractors using death certificates, coroner or medical examiner records, and law enforcement reports (CDC, 2022). The NVDRS is well suited for this study as it identifies IPH against older women and relevant characteristics. In particular, the NVDRS’s public health orientation results in the inclusion of details such as a history of abuse between the victim and perpetrator and the occurrence of a homicide-suicide. These details are not captured by other sources used to study IPH such as the Federal Bureau of Investigation’s Uniform Crime Reporting System in either its Supplemental Homicide Report or National Incident-Based Reporting System (Addington, 2022).
Case Selection
To be eligible for the present study, IPH incidents needed to involve victims who were women age 50 or older and intimate partner perpetrators who could be men of any age. Intimate partners were defined as current or former spouses or dating partners. Only incidents involving one victim and one perpetrator were selected, which is consistent with prior IPH studies (Addington & Perumean-Chaney, 2014). For this study, intimate partners were limited to opposite-sex couples as the small number of same-sex couples prevented additional analyses of these cases. Applying these selection criteria resulted in a total of 660 IPH incidents against women age 50 or older.
Variables
This study used victim age subgroup and incident characteristic variables. Victim age subgroups were measured using decade categories (50–59, 60–69, 70–79, and 80 plus). Decade categories allowed for the identification of age patterns while minimizing small cells that trigger data privacy concerns for the restricted-use NVDRS data. The incident characteristics were selected based on previous studies of IPH against older women including (1) prior IPV, (2) an intimate partner who was the victim’s caregiver, (3) IPHS, and (4) the use of a firearm. The prior IPV characteristic was measured using the NVDRS “history of abuse” variable that includes physical, psychological, sexual, or other violence committed by a former or current intimate partner (CDC, 2022). The intimate caregiver characteristic used the NVDRS variable that indicates whether the perpetrator was the victim’s caregiver (CDC, 2022). The IPHS characteristic used the NVDRS variable that indicates whether the perpetrator died by suicide within 24 hours of committing the homicide (CDC, 2022). Firearm use was based on “firearm” responses to the NVDRS variable that identifies the primary weapon used to kill the victim (CDC, 2022). 2 All incident variables were coded as dichotomies of whether the characteristic was present or not.
Analysis
To explore how incident characteristics of IPH against older women might vary across victim age subgroups, this study used joint frequency distributions with Chi-square tests. Although the American University Institutional Review Board determined this study to be exempt from IRB review, the restricted-use NVDRS data were accessed pursuant to a data agreement with the CDC to prevent possible identification of individuals. The findings presented abided by this agreement, which included a requirement to suppress cells with fewer than 10 cases.
Findings
For IPH characteristics, clear patterns emerged between older women in their 50s and 60s and those over 70 (Table 1). For incidents with a history of IPV, a greater proportion of victims in their 50s (21.1%) and 60s (18%) experienced prior IPV than the older age subgroups. For IPH involving caregivers, this pattern was reversed. IPH committed by a caregiver occurred primarily in incidents involving victims in their 70s (16.1%) and over 80 (29.3%). While IPHS incidents were observed across all age subgroups, they increased by age with the greatest proportion observed in the oldest age subgroups. Almost two-thirds (66.9%) of incidents against victims in their 70s and slightly over three-quarters (75.9%) of those against victims 80 or older involved IPHS as compared a third (32.2%) of victims in their 50s and 44.9% of victims in their 60s. While firearm-involved IPH was the only characteristic that appeared in a majority of incidents for all ages, variations occurred across age subgroups. The proportion of incidents involving a firearm increased by victim age where 53% of IPH against victims in their 50s were killed with a firearm as compared to nearly 85% of victims 80 or older. Analyses not presented here indicated that three-quarters of the firearms used were handguns, and the proportion of handgun use was consistent across age subgroups.
Characteristics of IPH against Older Women by Age Subgroups, 2017–2019 NVDRS Restricted-Use Data.
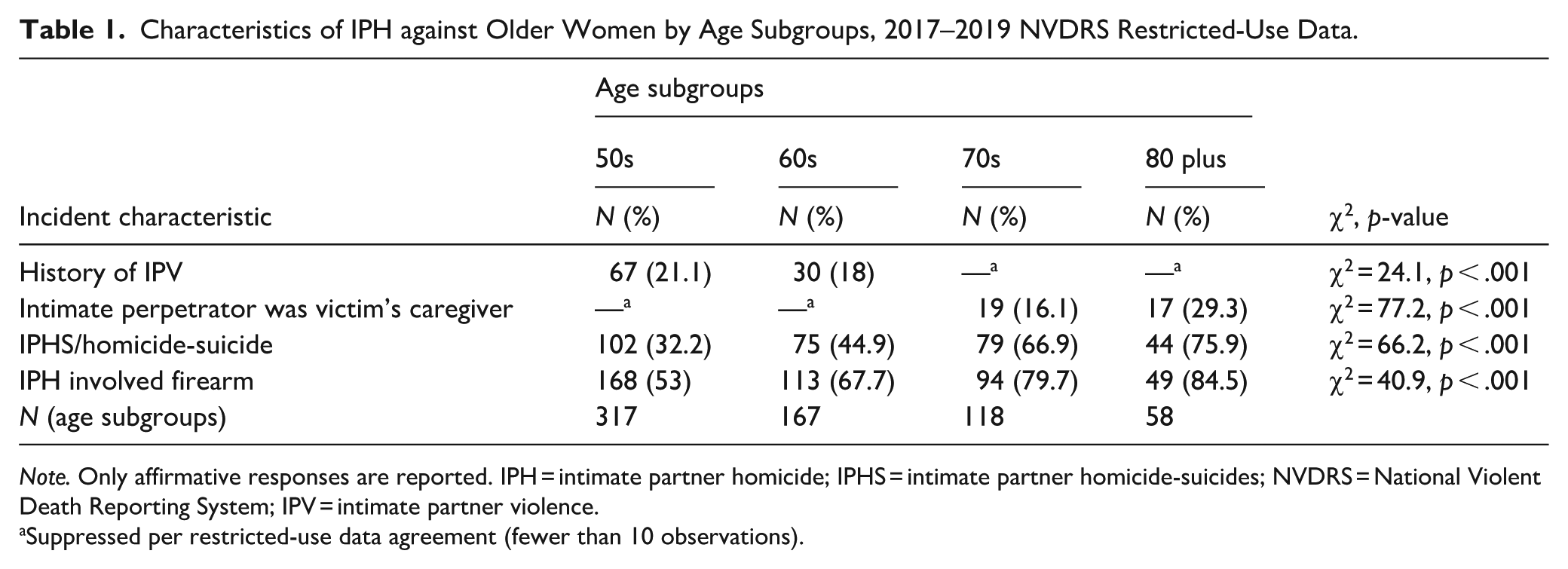
Note. Only affirmative responses are reported. IPH = intimate partner homicide; IPHS = intimate partner homicide-suicides; NVDRS = National Violent Death Reporting System; IPV = intimate partner violence.
Suppressed per restricted-use data agreement (fewer than 10 observations).
Discussion
While previous research identified characteristics of IPH against older women, it was unknown how these might vary with age. This study found IPH characteristics differed between victims in their 50s and 60s as compared to those over 70. These findings highlight the need to consider age when studying IPH against older women. To illustrate opportunities for such work, the following discussion considers each of the four characteristics with examples for investigating the findings obtained and possible IPH risk factors with age subgroups in mind.
The present study confirmed research that IPH against older women typically does not involve a history of IPV. This study also brought nuance to previous work by finding prior IPV was more common among victims in their 50s and 60s than those over 70. Investigation of these age-related patterns suggests research opportunities. One avenue could explore characteristics of the IPV that precedes IPH for women in their 50s and 60s, particularly how these experiences might compare with those of women under 50. Gaining this information could determine the applicability to older women of current IPH prevention strategies that utilize IPV risk factors such as danger assessments (Campbell et al., 2007). Another example could examine whether the patterns observed by this study were due to differences in IPV experiences or reporting for women in their 50s and 60s as opposed to those over 70. Previous work found that IPV is often underreported by older women due to age-related reasons (Crockett et al., 2018; Roberto et al., 2013). For example, older women tended to experience nonphysical violence such as coercive control but were unlikely to report because they did not interpret it as IPV. Older women also appeared reluctant to report due to economic dependency on their partners’ retirement income or health insurance. In addition, generational views of IPV as a private matter contributed to underreporting. No study has explored whether underreporting varies by age for older women. Understanding patterns of IPV and underreporting across age groups could inform the risk for IPH against older women with a history of IPV.
IPH incidents perpetrated by intimate partner caregivers occurred almost exclusively against women over 70. This finding confirmed prior research and extended it by identifying this age pattern. This pattern appeared to be consistent with women over 70 being at a greater risk to experience a serious illness and need for care as compared to women in their 50s and 60s (DiJulio et al., 2017). Future work could confirm the relationship between health, age, and caregiver IPH. Additional research could delve into circumstances that may increase the likelihood of IPH by a caregiver, particularly factors that might explain the increased proportion of victims over 80. For example, studies could explore differences between victims in their 70s and 80s including variations in the level and type of caregiving. Research also could consider the effect on IPH of changes in demographic factors such as the effect of financial constraints on caregiving and changes in the caregiver’s own health. Currently little is known about any association with these characteristics and IPH by a caregiver.
With regard to IPHS, this study confirmed previous work that indicated the frequency of IPHS involving older women (Salari & Sillito, 2016) and provided additional detail by highlighting the increased proportion of IPHS for victims over 70. Prior research on IPHS involving older adults suggested that suicidal (rather than homicidal) motivations by older male partners was more common than with IPHS among adults under 50 (Salari & Sillito, 2016). It is unknown whether these motivational patterns vary across age subgroups for older women. Given the age-related patterns identified by this study, different motivations might occur between IPHS victims in their 50s and 60s and those over 70. Variation across age subgroups would be important to explore. Additional research could focus on the two oldest age groups that had the greatest proportion of IPHS. It is unknown how characteristics of IPHS might vary between women in their 70s and those over 80 and how these affect risk.
The final characteristic was firearm-involved IPH. While firearms were used in a majority of IPH incidents across all age subgroups, their use increased with age. Over three-quarters of IPH against women over 70 involved firearms as compared to about half of IPH against women in their 50s. Future work could consider characteristics that might explain the increased use of firearms with victim age. One avenue for further exploration would be to build on the firearm and IPHS patterns identified by this study. Both IPHS and firearm use increased substantially for IPH against women over 70. These findings were consistent with prior research that indicates the frequency of firearm use in both suicide deaths of older men (Garnett et al., 2023) and IPHS against older women (Salari & Sillito, 2016).
Limitations
While these findings offered an initial understanding of how characteristics of IPH against older women might vary across age subgroups, study limitations suggest caution in interpreting and extending the results. One limitation concerned this study’s reliance on the NVDRS variables. The NVDRS variables are limited to information available to the data abstractors. If details were not mentioned in official coroner or police records, they would not be captured in the NVDRS and could result in an undercount. The impact of this issue likely varied across the variables used in this study. The prior IPV measure could be subject to greater undercounting than other variables if underreporting prevented this information from being captured by official records. In contrast, information on IPHS or use of a firearm could be less subject to undercounting as these details would likely be part of a homicide investigation and official record. Second, this study opted to focus on age subgroup variations and did not include additional covariates. This decision was based on this study’s goal to ascertain whether age-related distinctions were present and outline research needed to fully investigate such patterns. Finally, the incident characteristic patterns across the age subgroups do not distinguish whether the differences reflected increased risk conditional on age or mechanical changes in demographic exposure. Future research could delve into the nature of these patterns. Despite these limitations, the present study provided insights on age variations not previously identified and ways to improve the understanding of IPH against older women.
Conclusion
Although older women remain at the greatest risk for being killed by an intimate partner, few studies have examined their IPH. Existing research suggested that IPH characteristics appear to differ between younger and older women, but no work had considered whether these characteristics vary across older women of different ages. Findings obtained from this study highlighted distinctions between IPH against women in their 50s and 60s and those over 70. These findings also provided guidance for ways that research can incorporate age subgroups in future studies that investigate characteristics and risk factors associated with IPH against older women and ultimately inform prevention efforts tailored to these distinctions.
Footnotes
Acknowledgements
This project utilizes information from the NVDRS, which is administered by the Centers for Disease Control and Prevention and participating NVDRS states. The findings and conclusions of this study are those of the author alone and do not necessarily represent the official position of the CDC or participating NVDRS states.
Ethical Considerations
The Institutional Review Board of American University determined that this research met one or more of the criteria under Code of Federal Regulations Title 45 §46.101(b) and was exempt from IRB review (Protocol #: IRB-2021-334).
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported, in part, by Award No. 15PNIJ-21-GG-02801-REVA, awarded by the National Institute of Justice, Office of Justice Programs, U.S. Department of Justice. The opinions, findings, conclusions, and recommendations expressed in this publication are those of the author and do not necessarily reflect those of the U.S. Department of Justice.
Declaration of Conflicting Interests
The author declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the Centers for Disease Control and Prevention, but restrictions apply to the availability of these data, which were used under license for the current study, and are not publicly available or available from the author.