
Abstract
This study examines the frequency of specific discrimination experiences by attribution and social identities (i.e., race, gender) and quantifies if both frequent discrimination experiences and different types of discrimination are associated with violence exposure (i.e., victimization, aggression) and its behavioral and mental health risk factors for violent injury (e.g., substance use). We analyzed baseline survey data from a multi-site longitudinal study of emerging adults aged 18 to 24 recruited from emergency departments in Seattle, Philadelphia, and Flint (n = 1,506). We examined the frequency and attribution of discrimination experiences and assessed associations with violence exposure and its relevant behavioral and mental health risk factors, including suicidal ideation, substance use, and anxiety/depression. Overall, 79.1% reported experiencing discrimination in daily life and 31.2% experienced it more than weekly. Reports of more-than-weekly discrimination were highest among multiracial (40%) and non-gender conforming individuals (41.5%). Race, gender, and age were the most cited reasons. Participants reporting ≥weekly discrimination were more likely to report suicidal ideation in the past 2 weeks, drug misuse, firearm victimization, and recent mental health symptoms (depression and anxiety symptoms in the past 2 weeks; post-traumatic stress disorder symptoms in the past month) compared to those with less frequent or no discrimination. Of note, discrimination related to being treated as inferior, unintelligent, or with less courtesy showed the strongest associations with mental health symptoms, while more static associations, across discrimination types, were found with regard to substance use and violence outcomes. Given that types of discrimination experiences may be more strongly linked to mental health symptoms, highlighting the need to consider the specific nature of these experiences. Moreover, discrimination was more pervasive among some minoritized groups (e.g., multiracial, gender non-conforming), underscoring the need for an intersectional lens to understand and address this stressor effectively.
Introduction
Violent injuries, including interpersonal injuries due to aggression and/or victimization and self-inflicted injuries, are the leading causes of death among emerging adults (ages 18–24, consistent with the definition of emerging adulthood; Arnett, 2000; Centers for Disease Control and Prevention [CDC], 2025). In recent national mortality data, suicide and homicide together account for roughly 30 deaths per day among emerging adults in the United States (e.g., ages 20–24), underscoring the significance of both self-directed and interpersonal violence in this age group (CDC, 2025). Interpersonal discrimination (hereafter, “discrimination”) is a significant psychosocial stressor pervasive in the lives of emerging adults, with a recent study showing that 93% of emerging adults reported experiencing discrimination on the basis of racial and ethnic identity or ancestry, sex, age, physical appearance, and other reasons (Lei et al., 2021).
Experiencing discrimination is associated with common risk factors for violent injury, including substance misuse (Lei et al., 2021), mental distress (Lee et al., 2020), and violent behaviors (Caldwell et al., 2004). Theoretically, the relationship between discrimination and violence exposure (hereafter, referring to violent victimization and aggression) can be understood through the Weathering Hypothesis (Geronimus, 1992), which suggests that chronic exposure to social discrimination erodes psychological and physiological health over time, contributing to risk factors linked with violent injury, such as substance misuse. Similarly, the Minority Stress Theory (Meyer, 2003), emphasizes the ways in which unique and compounding stresses experienced by individuals with marginalized identities deteriorates mental and physical health. Together, these and related theoretical models (e.g., stress and coping frameworks; Lazarus & Folkman, 1984), in conjunction with empirical studies (Emmer et al., 2024; Lee et al., 2020; Pascoe & Smart Richman, 2009; Schmitt et al., 2014), posit that routine experiences of discrimination impose a cumulative psychological burden that, over time, increases risk for maladaptive coping that puts individuals at-risk for violence toward oneself or others.
Discrimination also plays a critical role when considering the etiologies of persistent disparities in violent injuries (D. R. Williams & Mohammed, 2013). For example, researchers have documented that fatal and nonfatal firearm assault injuries are highest among Black males compared to males and females of other racial groups (CDC, 2025; Goldstick et al., 2021). There are higher suicidal ideation rates among LGBTQ+ emerging adults when compared to heterosexual peers (Ybarra et al., 2015). Scholars argue that these disparities reflect broader systems of oppression operating across both social processes (e.g., racial microaggressions, stereotypes, and implicit bias) and structural conditions (e.g., institutional policies and practices such as the school-to-prison pipeline; D. R. Williams & Mohammed, 2013). Importantly, discrimination and violence exposure may also co-occur rather than operate only through a downstream coping process. Overt manifestations of discrimination, such as being called a racial epithet or being physically threatened because of one’s race, may reflect forms of victimization rooted in prejudice (Díaz-Faes & Pereda, 2022). Thus, discrimination and violence exposure may arise from both prejudicial social environments, while discrimination may also contribute to violence-related risk through stress-related psychological and behavioral pathways (Lee et al., 2026; Lemke et al., 2022).
It is also important to recognize that victimization and aggression are often intertwined. Prior research documents substantial overlap between these experiences, making them difficult to treat as mutually exclusive categories (Goldstick, Carter, Whiteside, Delgado, & Cunningham, 2024; Jennings et al., 2012). For instance, Goldstick, Carter, Whiteside, Delgado, & Cunningham (2024) found that more than 90% of participants who experienced a firearm assault also reported firearm assault victimization. Discriminatory experiences may also heighten vigilance, retaliatory attitudes, and safety concerns (Copeland-Linder et al., 2012; Lee et al., 2022), which may increase risk for victimization and aggression by placing youth in more vulnerable environments or contributing to defensive responses, retaliation, or conflict escalation (Dong et al., 2020; Wiebe et al., 2015). Therefore, we examined violence involvement more broadly rather than stratifying analyses by victimization versus aggression.
In this study, we focus specifically on experiences of interpersonal discrimination in the lives of emerging adults. Interpersonal discrimination refers to unfair treatment enacted in social interactions (e.g., disrespect, harassment), whereas structural discrimination operates through institutional policies and broader social systems that shape unequal opportunities and exposures (e.g., residential racial segregation; Neblett, 2023). Structural forms of discrimination were not directly assessed in this study.
A substantial body of literature has established that discrimination is associated with poor mental health (Emmer et al., 2024; Schouler-Ocak & Moran, 2023; Shi et al., 2022), substance use (Lee et al., 2017; Rouhani et al., 2025), and other violent behaviors (Caldwell et al., 2004; Martin et al., 2011). This study seeks to extend this literature to violent injury-related risk factors by examining whether specific interpersonal discrimination experiences are associated with behavioral and mental health factors linked to violence involvement. This distinction is important because most studies in this area have relied on aggregated measures of discrimination, which may obscure whether particular types of discriminatory experiences are more strongly associated with risk. In addition, much of the firearm violence and injury literature has emphasized structural or place-based indicators of racism, with comparatively less attention to individuals’ lived experiences of interpersonal discrimination (Lee et al., 2026).
To date, few studies have examined discrimination and violent injury-related outcomes beyond the aggregation of multiple forms of discrimination, limiting insight into whether specific experiences relate to risk. Therefore, this study aims to: (1) characterize the prevalence of specific discrimination types, (2) examine attributions by race and gender, (3) examine the prevalence of more frequent (weekly) discrimination, and determine factors associated with more frequent discrimination experiences, and (4) evaluate if specific types of discrimination experiences relate to key behavioral and mental health risk factors for violence, including violence victimization and aggression.
Method
Study Design and Setting
Here, we present secondary data analysis from the Screening to Predict Young Adults at Risk for Firearm Violence (SPARK) study (Goldstick, Carter, Whiteside, Delgado, Stallworth, et al., 2024). Data for this study are from baseline assessments of a multi-site longitudinal study of risk factors that predict violence outcomes among emerging adults seeking treatment at four emergency departments that is, one in Seattle, one in Flint, and two in Philadelphia. The primary aim of SPARK was to externally validate the SaFETy score (Goldstick et al., 2017), the only clinical screening tool designed to assess risk for future firearm violence. Previous work from this study examined cross-sectional associations between the SaFETy score and firearm violence risk at baseline (Goldstick et al., 2024) and demonstrated the prospective predictive power of the SaFETy score with regard to firearm violence in the 12-month following baseline (Goldstick et al., 2026).
Eligible participants were those that were able to provide informed consent. Exclusions included sexual assault, psychosis, suicidal ideation, police custody, or—due to COVID-19 precautions—those requiring respiratory/droplet isolation. We selected these exclusion criteria because the goal of the study was to conduct prospective validation of a clinical screening tool for future firearm violence risk in a general sample of emerging adults presenting to the emergency department. Study staff used electronic health records to identify eligible patients and approached them in waiting or treatment areas. Consenting participants received $40 for completing the baseline survey and agreed to follow-up contact and 1-year chart review. The survey was self-administered and on rare occasions verbally administered by a research assistant. Participant recruitment began in Seattle, Philadelphia, and Flint sites on August 26, 2021; July 26, 2021; and January 24, 2022, respectively. Recruitment activities concluded on May 25, 2023 (Seattle), May 31, 2023 (Philadelphia), and May 9, 2023 (Flint). Overall, 25.4% refused/declined participation in the study. Additional recruitment details and the study flowchart are provided elsewhere (Goldstick, Carter, Whiteside, Delgado, Stallworth, et al., 2024). All study protocols were approved by the University of Michigan IRB.
Measures
We measured discrimination experiences using the Everyday Discrimination Scale (EDS; D. R. Williams et al., 1997). Participants rated the frequency of seven discriminatory experiences on a 6-point scale (1 = Never, 6 = Almost everyday). Items captured experiences such as being treated as less intelligent or receiving threats and experiencing harassment. The scale was slightly adapted for parsimony and to reduce redundancy: two items were combined (“treated with less courtesy or respect”) and another on name-calling was omitted. Participants reporting any discrimination also identified perceived reasons from a checklist of social identity categories, including ancestry/national origins, gender, race, age, religion, height, weight, some other aspect of physical appearance, sexual orientation, educational attainment, or other reasons.
In addition to demographic characteristics (age/gender/race), we measured violence experiences, mental health symptoms, and substance use outcomes. The modified conflict tactics scale separately measured past 6-month frequency of 11 violence behaviors, both as victim and aggressor; for this analysis, we collapsed the items to examine any violence, severe violence (e.g., weapon violence, beating up), and firearm violence (Straus et al., 1996), each stratified by victimization and aggression, and combined. We measured post-traumatic stress disorder (PTSD) symptoms in the past month using the PCL-17 (Lang & Stein, 2005), depressive symptoms in the past 2 weeks using the PHQ-9 (Richardson et al., 2010), and anxiety symptoms in the past 2 week using the GAD-7 (Spitzer et al., 2006); we determined positive screens using established clinical screening cut points of 10, 10, and 30, respectively. The Columbia Suicide Severity Scale measured past-2-week suicidal ideation (Posner et al., 2011). The NIDA-ASSIST measured the use of marijuana, illicit (e.g., cocaine, heroin, hallucinogens), and prescription (e.g., opioids, sedatives, stimulants) drugs, with a ≥4 score on any substance used as an indicator of drug misuse in the past 6 months (WHO ASSIST Working Group, 2002). The AUDIT-C (Bush et al., 1998) measured alcohol use frequency, with cut points of 3 and 4 indicating risky use in women, and men, respectively, in the past 6 months (Reinert & Allen, 2007).
Statistical Analysis
We descriptively summarized the frequency of each discrimination type in the sample; among those reporting ≥weekly discrimination, we examined reasons for discrimination, stratified by race and gender. Next, we contrasted those reporting ≥weekly discrimination with those who did not, by demographic characteristics, violence exposures, and substance use/mental health outcomes. Next, we used logistic regression to estimate odds ratios relating weekly discrimination to the binary indicators of violence exposure and substance use/mental health outcomes, adjusted for age, gender, race, and site. Finally, we examined whether each type of discrimination was associated with any violent aggression, violent victimization, and mental health/substance use outcomes, by estimating adjusted standardized mean differences (adjusted Cohen’s d) comparing participants who did and did not report each outcome, after controlling for age, gender, race, and site. We estimated adjusted Cohen’s d values as estimated marginal means, implemented in the R package emmeans. All analyses were completed using R version 4.4.1.
Results
Among 1,506 total participants across sites (61.3% female; 40.9% Black; 33.0% White), 79.1% reported experiencing discrimination. The most frequent experience was having other people act as though they are better than you, with 62.9% reporting having ever experienced it; 37.5% reported a history of discriminatory threats/harassment. Many (31.2%) participants reported experiencing discrimination more than weekly, with multiracial (40.0%) and non-gender conforming (41.5%) respondents reporting this most frequently. Table 1 presents discrimination frequencies by gender, and Table 2 presents discrimination experiences by race.
Frequency of Seven Different Types of Discrimination Among the SPARK Sample, Stratified by Gender.
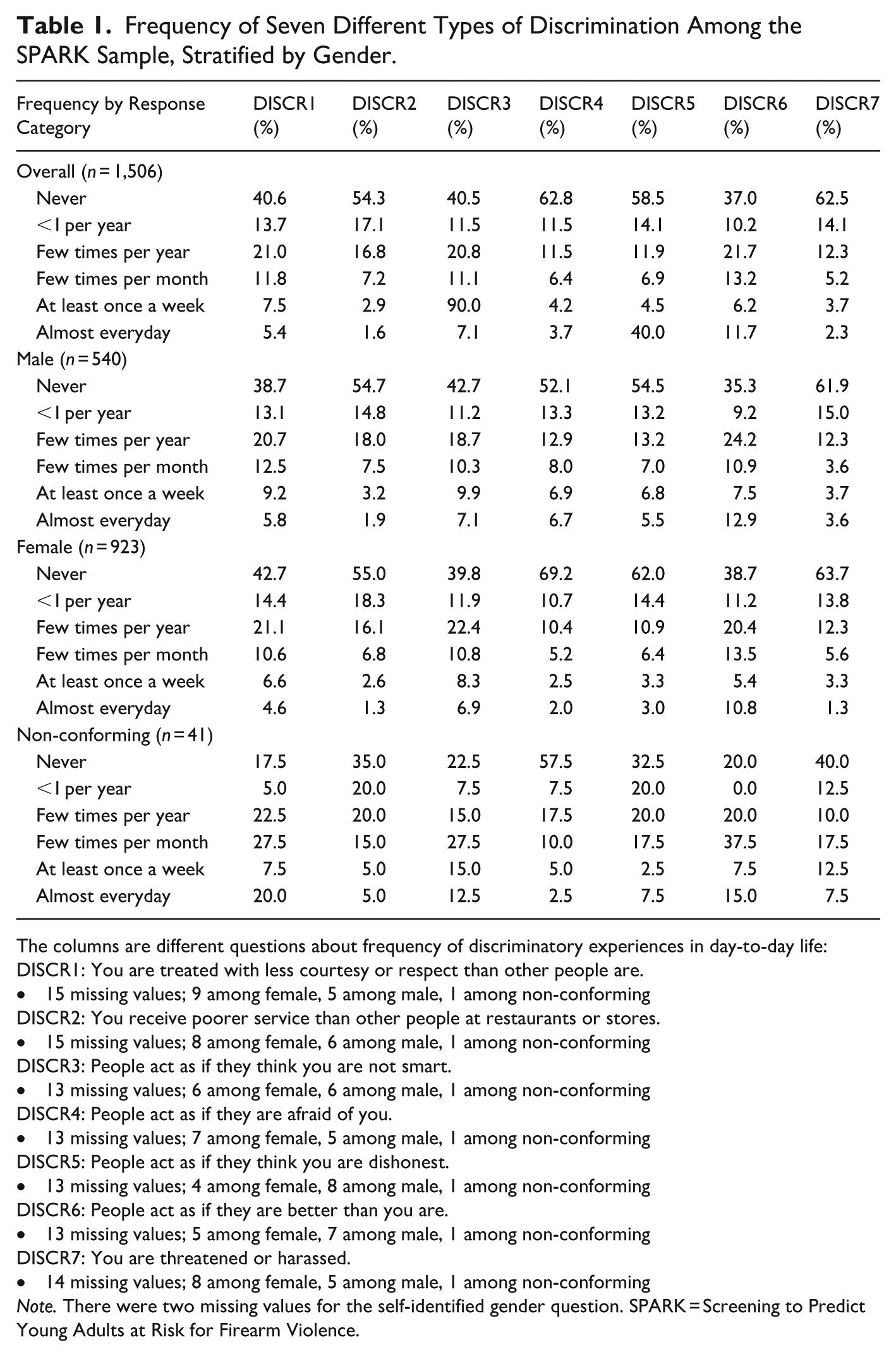
The columns are different questions about frequency of discriminatory experiences in day-to-day life:
DISCR1: You are treated with less courtesy or respect than other people are.
• 15 missing values; 9 among female, 5 among male, 1 among non-conforming
DISCR2: You receive poorer service than other people at restaurants or stores.
• 15 missing values; 8 among female, 6 among male, 1 among non-conforming
DISCR3: People act as if they think you are not smart.
• 13 missing values; 6 among female, 6 among male, 1 among non-conforming
DISCR4: People act as if they are afraid of you.
• 13 missing values; 7 among female, 5 among male, 1 among non-conforming
DISCR5: People act as if they think you are dishonest.
• 13 missing values; 4 among female, 8 among male, 1 among non-conforming
DISCR6: People act as if they are better than you are.
• 13 missing values; 5 among female, 7 among male, 1 among non-conforming
DISCR7: You are threatened or harassed.
• 14 missing values; 8 among female, 5 among male, 1 among non-conforming
Note. There were two missing values for the self-identified gender question. SPARK = Screening to Predict Young Adults at Risk for Firearm Violence.
Frequency of Seven Different Types of Discrimination Among the SPARK Sample, Stratified by Race.
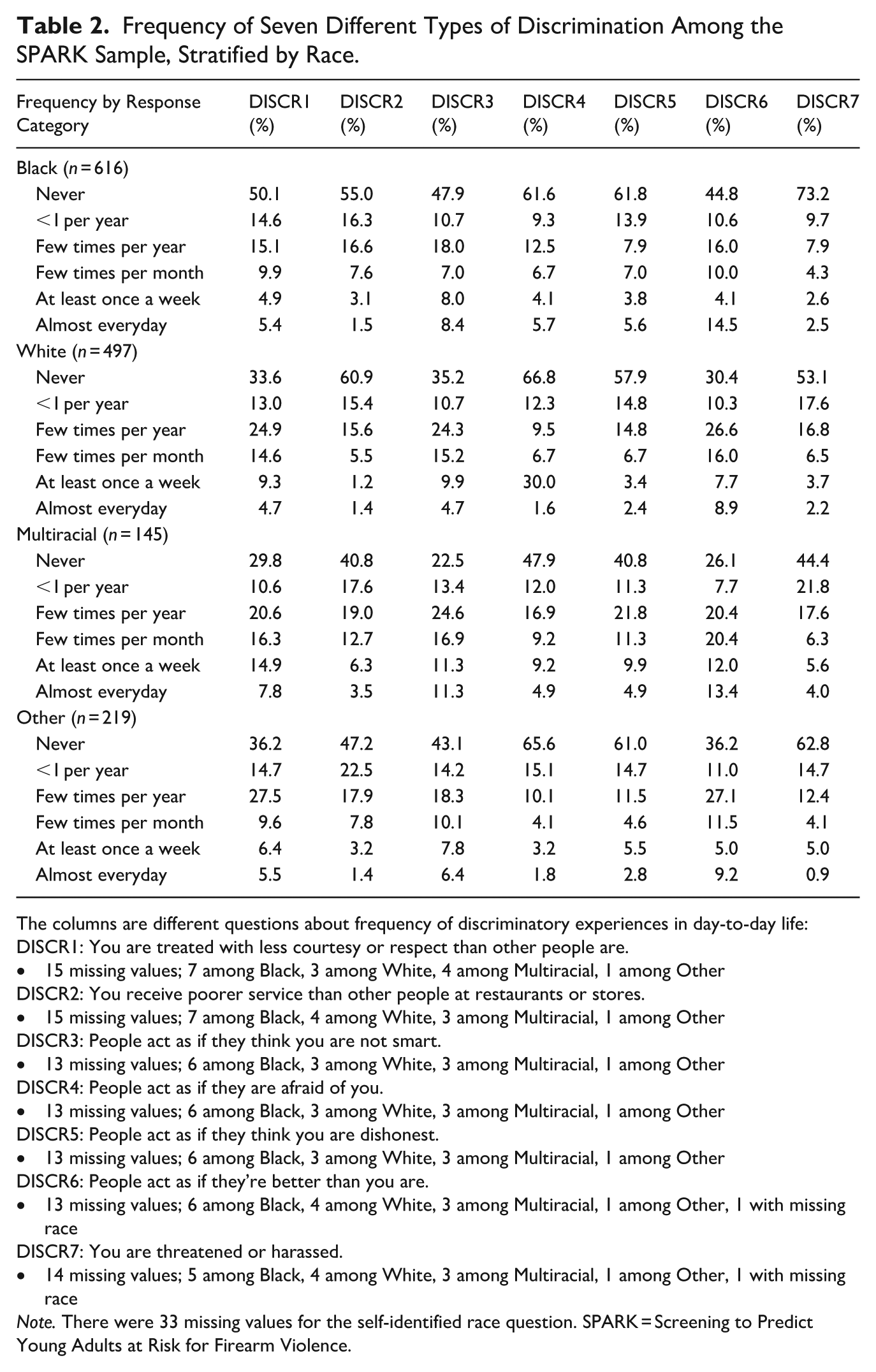
The columns are different questions about frequency of discriminatory experiences in day-to-day life:
DISCR1: You are treated with less courtesy or respect than other people are.
• 15 missing values; 7 among Black, 3 among White, 4 among Multiracial, 1 among Other
DISCR2: You receive poorer service than other people at restaurants or stores.
• 15 missing values; 7 among Black, 4 among White, 3 among Multiracial, 1 among Other
DISCR3: People act as if they think you are not smart.
• 13 missing values; 6 among Black, 3 among White, 3 among Multiracial, 1 among Other
DISCR4: People act as if they are afraid of you.
• 13 missing values; 6 among Black, 3 among White, 3 among Multiracial, 1 among Other
DISCR5: People act as if they think you are dishonest.
• 13 missing values; 6 among Black, 3 among White, 3 among Multiracial, 1 among Other
DISCR6: People act as if they’re better than you are.
• 13 missing values; 6 among Black, 4 among White, 3 among Multiracial, 1 among Other, 1 with missing race
DISCR7: You are threatened or harassed.
• 14 missing values; 5 among Black, 4 among White, 3 among Multiracial, 1 among Other, 1 with missing race
Note. There were 33 missing values for the self-identified race question. SPARK = Screening to Predict Young Adults at Risk for Firearm Violence.
Supplemental Appendix Figure S1 shows frequency of perceived reasons for discrimination, among those reporting ≥weekly discrimination, stratified by gender/race. Race (44.6%), gender (44.4%), and age (42.4%) were most frequently cited as perceived discrimination reasons. Racialized minorities more frequently cited race as a perceived reason, non-gender conforming individuals cited gender and sexual orientation, and women cited gender.
Table 3 presents unadjusted contrasts of those reporting, and not reporting, ≥weekly discrimination. Across our sociodemographic variables, Women, younger adults, and multiracial respondents more frequently reported ≥weekly discrimination; those from Seattle reported ≥weekly discrimination most frequently, and those from Philadelphia reported least frequently. Table 4 presents adjusted contrasts of those reporting ≥weekly discrimination for violence exposure, mental health symptoms, and substance use. Violence exposure rates were uniformly higher among those reporting ≥weekly discrimination, including >4× the risk of past-6-month firearm victimization. Self-reported mental health symptoms were most common among those who experienced ≥weekly discrimination, ranging from ~4× higher rates (depression) to >6× higher rates (PTSD). Moreover, past-2-week suicidal ideation was >5× higher (8.6%-vs.-1.7%) among those reporting ≥weekly discrimination. Alcohol misuse was more common among those experiencing ≥weekly discrimination (34.9%-vs.-31.3%), but there were no significant differences in the odds of risky alcohol use.
Contrasts Between Those Who Report, and Do Not Report, Weekly or Greater Discrimination Experiences on Demographics, Violence Experiences, and Mental Health and Substance Use Symptoms.
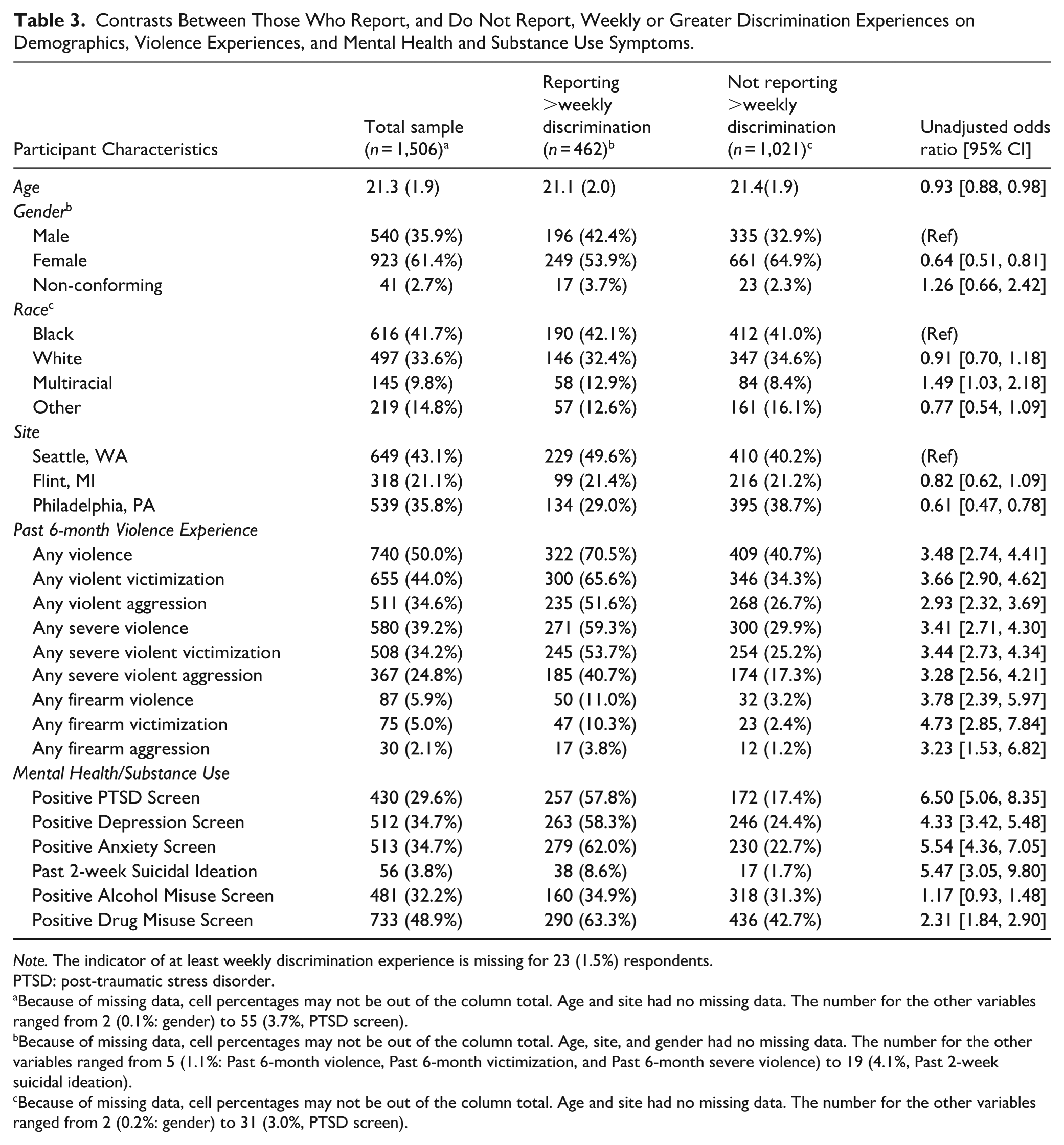
Note. The indicator of at least weekly discrimination experience is missing for 23 (1.5%) respondents.
PTSD: post-traumatic stress disorder.
Because of missing data, cell percentages may not be out of the column total. Age and site had no missing data. The number for the other variables ranged from 2 (0.1%: gender) to 55 (3.7%, PTSD screen).
Because of missing data, cell percentages may not be out of the column total. Age, site, and gender had no missing data. The number for the other variables ranged from 5 (1.1%: Past 6-month violence, Past 6-month victimization, and Past 6-month severe violence) to 19 (4.1%, Past 2-week suicidal ideation).
Because of missing data, cell percentages may not be out of the column total. Age and site had no missing data. The number for the other variables ranged from 2 (0.2%: gender) to 31 (3.0%, PTSD screen).
Odds Ratio, Adjusted for Age, Gender, Race, and Site, Relating Each Violence, Mental Health, and Substance Use Variable to Weekly (or Greater) Discrimination Experiences.
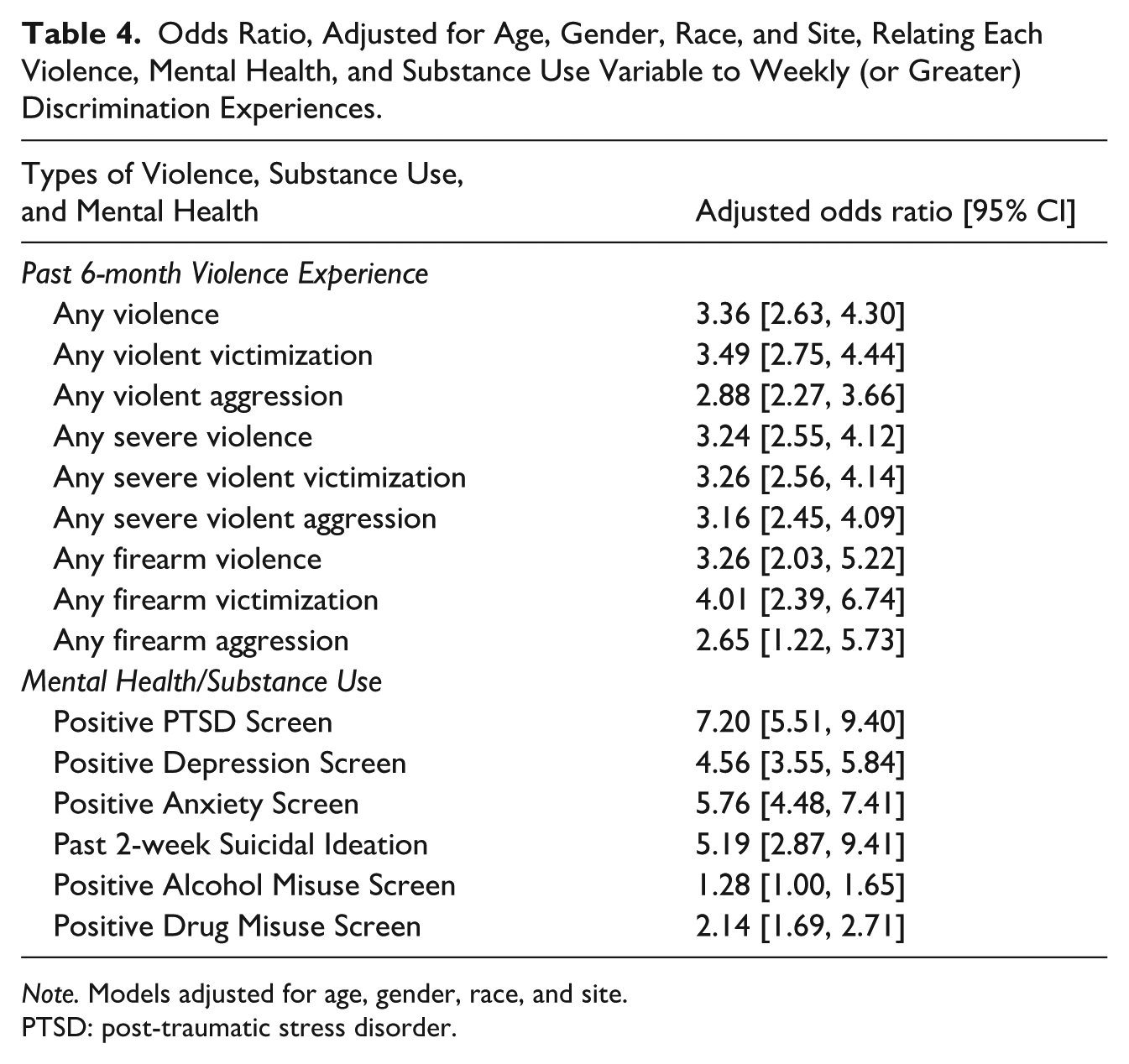
Note. Models adjusted for age, gender, race, and site.
PTSD: post-traumatic stress disorder.
Figure 1 shows adjusted Cohen’s d differentiating those with versus those without six behavioral and mental risk factors of violence, including violence, by each discrimination measure, controlling for gender, age, race, and site. Each type of discrimination showed similar effect sizes on drug misuse, risky alcohol use, violent victimization, and violent aggression, with overlapping confidence intervals indicating relatively small differences across discrimination types. Items on discrimination experiences related to perceptions of being treated less courteous, being treated as unintelligent, being treated as dishonest, and being treated as inferior showed larger effect sizes on anxiety and/or depression, and PTSD than items related to perceptions of others treating you as though they are afraid of you or giving you poorer service at stores/restaurants.
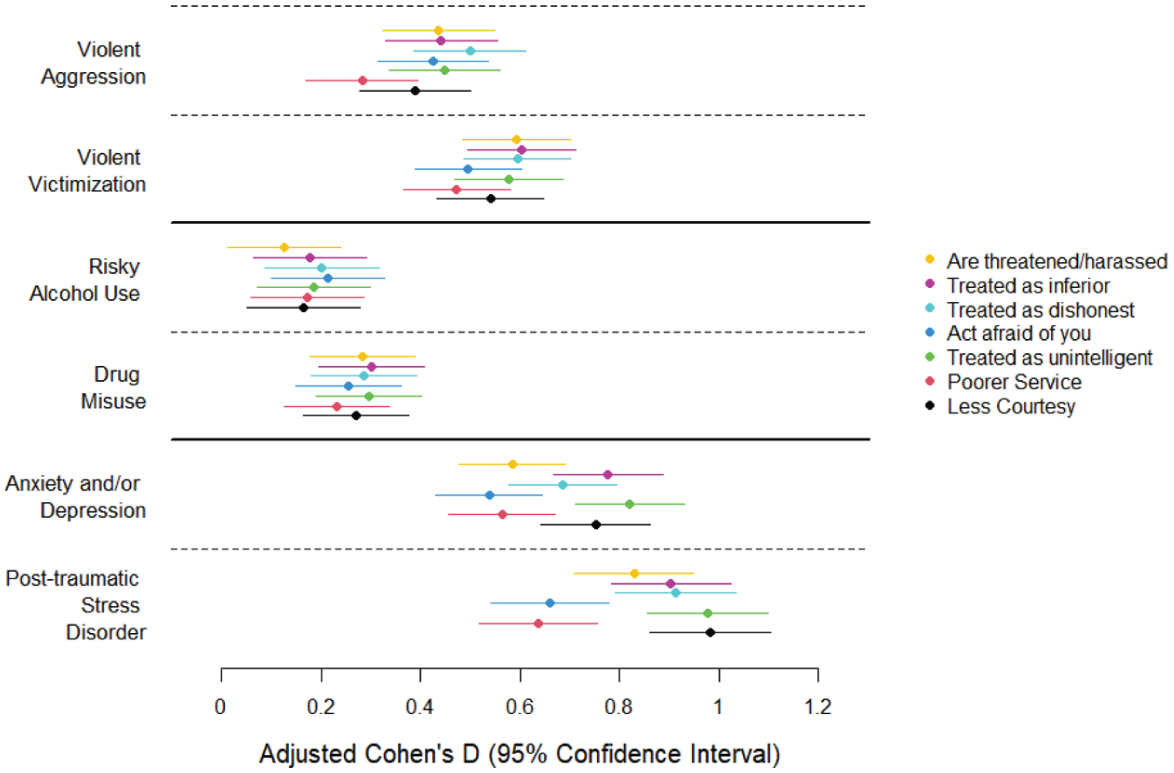
Standardized mean difference in each of seven discrimination scores between those who do versus do not report six psychosocial outcomes.
Discussion
Our findings, in conjunction with other studies, show that discrimination is a common stressor, with nearly 1-in-3 participants reporting at least weekly discrimination experiences, and is strongly associated with a history of firearm victimization, recent suicidal ideation, drug misuse and mental health symptoms (Clark et al., 1999; Lei et al., 2021; Mattingly et al., 2025; Pascoe & Smart Richman, 2009). Importantly, consistent with the biopsychosocial model for perceived racism (Clark et al., 1999), we found that all of the different discrimination types were associated with positive screening for mental health symptomology. That said, the size of the association varied depending on the type of discrimination experienced. Consistent, robust associations were found between different discrimination types and violence exposure after controlling for gender, age, race, and site. One possible explanation is that mental health outcomes are more proximal, reflecting the immediate psychological toll of discriminatory encounters (Clark et al., 1999; Lee et al., 2018; Pascoe & Smart Richman, 2009). Because distress is thought to vary with the nature of the stressor, the stress and coping theory (Lazarus & Folkman, 1984) suggests that the psychological impact of a stressor depends not only on whether the event occurred but also on how the event is appraised. Therefore, stressors appraised as more degrading or threatening may show stronger associations with depression, anxiety, or PTSD (Lee et al., 2020). By contrast, alcohol/drug misuse and violent involvement may represent downstream coping responses or contextual consequences of sustained exposure, making them less sensitive to discrimination type and more uniform across forms. For instance, as per the tension reduction theory (Cappell & Greeley, 1987), mental health symptoms may represent a more proximal, emotional response to discriminatory stress to degrading or threatening encounters. By contrast, alcohol/drug misuse and violent involvement may represent more distal outcomes that represent coping behaviors to alleviate negative emotional responses. Nevertheless, the findings suggest that interventions addressing discrimination experiences broadly may be beneficial, while in some cases greater efficiency may be achieved by tailoring strategies to the specific type of discrimination experienced. For example, experiences involving perceived inferiority, such as being treated as less intelligent or with less courtesy, were more strongly associated with depression and/or anxiety, and PTSD than experiences like being feared or receiving poor service. Experiences that communicate devaluation of competence or social worth may be particularly salient for internalizing symptoms because they directly challenge core aspects of identity and self-evaluation. Such experiences may also be difficult to dismiss or attribute to situational factors, and often occur in subtle, but chronic forms across everyday interactions, which may cumulatively contribute to depressive and anxiety-related symptoms (D. R. Williams et al., 2019). Taken together, the strong associations we observed suggest that addressing discrimination-related stressors by expanding access to responsive services—such as, culturally responsive and accessible mental health care that addresses racism-related stress and trauma (M. T. Williams et al., 2023)—may help emerging adults manage its socioemotional consequences of discrimination.
Discrimination was particularly frequent among multiracial and gender non-conforming individuals. Consistent with intersectionality frameworks, our findings indicate that discrimination is patterned across intersecting social positions, and participants’ attributions for unfair treatment often reflect multiple marginalized identities (Crenshaw, 1997; Lam et al., 2024). These findings underscore the need for targeted, intersectional strategies to prevent interpersonal discrimination among emerging adults. Potential approaches include revising institutional and organizational policies and protocols in settings where emerging adults commonly interact with institutions (e.g., schools, workplaces, and healthcare environments) to reduce discriminatory discretion based on marginalized social identities (e.g., race. gender and age), implementing routine training focused on bias toward multiracial and gender-diverse individuals, and establishing accountability and feedback mechanisms to allow and address reports of discriminatory treatment (Crenshaw, 1997; Hebl et al., 2015; Roberson et al., 2020). Such efforts must center lived experiences of those with multiple marginalized identities and engage them in shaping equity efforts (e.g., gendered racism; Erving et al., 2022). Thus, prevention efforts must acknowledge and address the multifaceted systems of power such as racism and sexism that operate in tandem to enable and reinforce interpersonal discrimination experiences in the first place (Crenshaw, 1997).
This study has several limitations. First, its cross-sectional design precludes causal inference. Yet, it is among the first to examine whether specific discrimination experiences relate to violence exposure and its behavioral and mental health risk factors. Second, we recruited our sample from four emergency departments across three urban centers, which may limit generalizability. Furthermore, we excluded individuals presenting with sexual assault, psychosis, active suicidal ideation, police custody, or other ineligible conditions due to COVID-19 precautions. Still, its geographic diversity (Philadelphia, Flint, Seattle) enhances relevance specifically to urban populations and highlights the need for broader demographic representation. Third, while the EDS was modified, the scale retained strong coverage of both implicit (e.g., being seen as unintelligent) and overt (e.g., harassment) discrimination. Future research should examine the impact of omitted or combined items and explore other forms of discrimination to better identify those most strongly linked to violent injury. Fourth, we combined Asian, Hispanic, and American Indian individuals into an “other” category due to limited sample sizes, preventing reliable inference. Future research should recruit larger samples to allow disaggregation and examination across racial/ethnic groups. Lastly, this study did not evaluate the composite score of the EDS, as has been done in prior work. Instead, we intentionally focused on item-level associations to provide an initial, descriptive examination of whether specific discrimination experiences show differential relationships with violent outcomes and its related behavioral and mental health risk factors. Future research should build on this work using measures of interpersonal discrimination that capture a broader range of experiences across multiple settings (e.g., work, school) to examine which forms of discrimination have distinct associations with violent injury risk. Such work can help inform tailored violent injury prevention efforts by pinpointing which discrimination experiences are most strongly linked to violent injury risk.
Social determinants such as discrimination are correlated with violence exposure and relevant behavioral and mental health risk factors. Violence prevention efforts, thus, should consider mitigating the psychological consequences of discrimination and implement policies and practices to prevent its many forms. Our disaggregated findings also suggest value in tailoring responses by discrimination type, depending on the behavioral and mental health risk factors targeted by those activities. Taken together, our findings clarify our understanding of whether discrimination relates to violent injury risk and highlight pathways to optimizing prevention.
Supplemental Material
sj-docx-1-jiv-10.1177_08862605261459046 – Supplemental material for Discrimination Experiences and Violent Injury Risk Among Young Adults
Supplemental material, sj-docx-1-jiv-10.1177_08862605261459046 for Discrimination Experiences and Violent Injury Risk Among Young Adults by Daniel B. Lee, Sara F. Jacoby, Eugenio Weigend Vargas, Patrick M. Carter, Arleen Lopez Cruz, Mucio Kit Delgado and Jason E. Goldstick in Journal of Interpersonal Violence
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: This research was supported by the National Center for Injury Prevention and Control R01CE003294 (PI: Jason E. Goldstick).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.