
Abstract
Sport is frequently positioned as a context for positive development. However, athletes may face unique risks for interpersonal violence in coach–athlete and authority–athlete relationships alongside adverse experiences outside of sporting contexts. Given that little quantitative research considers both sources of trauma in relation to athlete mental health, the current study was designed to explore how coach violence, authority violence, and adverse childhood experiences (ACEs) contribute to mental health symptomology. Drawing on attachment theory, athlete mental health is recognized to be shaped by both prior developmental adversity and ongoing relational dynamics within sport. To examine these connections, participants (N = 341, Mage = 21.72 years, SDage = 4.56, 80.4% female) were a mixture of current and former athletes, with the majority identifying as White women from a Western region of the United States. Robust multiple regression analyses highlighted that coach violence, authority violence, and ACEs were associated with depression, post-traumatic stress disorder (PTSD), and dissociation. Interactions between coach violence and ACEs were associated with anxiety, depression, and dissociation, while a three-way interaction among coach violence, authority violence, and ACEs was associated with PTSD. These findings support the view that athletes are not blank slates upon entering sport; instead, pre-existing trauma and histories may shape their vulnerability to further harm and influence how they respond to relational dynamics within the sport environment. Rather than viewing sport participation as uniformly protective, results underscore the need to consider how developmental histories and interpersonal dynamics jointly shape athlete well-being. By integrating developmental theory and trauma-informed principles, this research provides insights into how practitioners can recognize signs of trauma, minimize re-traumatization, and create emotionally safe environments to promote mental health and relational safety in sport.
Keywords
Introduction
Despite a pervasive narrative about the inherent goodness of sport (Coakley, 2015), sport settings can be a site of substantial harm for some athletes (Alexander et al., 2023; Kerr et al., 2020). Sport is characterized by pronounced hierarchical power structures in which coaches and other authority figures exert substantial influence over athletes’ development, performance, and well-being (Alexander et al., 2023, 2024). Within these power dynamics, interpersonal violence (IV) perpetrated by coaches and authority figures (e.g., trainers, sport administrators, or other sport personnel) towards athletes represents a particularly distressing source of relational adversity, given that these individuals often occupy roles marked by trust, dependence, and emotional salience. Such authority- and coach-perpetrated IV is concerning, given qualitative links to lasting mental health effects and broader developmental harm (Alexander et al., 2023; Battaglia et al., 2017; Gervis & Godfrey, 2013; Gervis et al., 2016). Despite the relational harm caused by harsh and abusive behavioral practices, such behaviors have been culturally normalized due to their perceived links to winning, talent development, and mental toughness (Kerr & Stirling, 2017; Kerr et al., 2020; Owusu-Sekyere & Gervis, 2016).
Drawing on attachment theory and trauma-informed perspectives, the impacts of such exposures become increasingly complex given that athletes enter sport with existing exposure to adverse life events, yet minimal research to date explores how early trauma experienced outside of sport and relational trauma within sport may differentially interact to shape mental health outcomes. Examining how distinct contexts of adversity relate to athlete outcomes is critical, as this would inform individualized intervention and holistic prevention mechanisms (Alexander et al., 2024) that are grounded in different victim experiences (Berring et al., 2024; Ford et al., 2015). Therefore, this study was designed to explore how coaching violence, authority violence within the sport context, and adverse childhood experiences (ACEs) are associated with current mental health symptomology. Attachment theory is utilized to provide guiding relational and developmental perspectives, while trauma-informed approaches are included to highlight applied implications for promoting athlete well-being.
Violence as a Form of Trauma in Sport
One major form of trauma in sport is IV, which includes patterns of abusive behaviors that may or may not lead to observable or quantifiable harm to the victim. IV occurs in relationships where one party serves in caregiving and supervisory capacities and can be especially distressing for athletes because these perpetrators hold unique and substantial power over them (Alexander et al., 2024; A. E. Stirling & Kerr, 2008). Some of the most common critical relationships in sport include coach–athlete and authority figure–athlete relationships. Sport scholars categorize IV in terms of physical, psychological-neglectful, and sexual forms of behaviors and refer to a variety of possible perpetrators (e.g., parents, coaches, teammates, spectators; Parent et al., 2019). Experiences of coach and authority violence have been qualitatively linked to shame, social difficulties, anxiety, trauma-related symptoms, and other psychopathological symptoms (Alexander et al., 2023; Battaglia et al., 2017; Gervis & Godfrey, 2013; Gervis et al., 2016; Tuakli-Wosornu et al., 2024). Concerningly, these exposures are also qualitatively linked to self-injurious behaviors, including intentional self-harm (e.g., cutting, scratching), suicide, substance abuse, disordered eating, and disordered weight management techniques (Boudreault et al., 2022; Mountjoy et al., 2016; Willson et al., 2025). Violence perpetrated by coaches and other authorities has the potential to negatively impair emotion regulation, athletic performance, and holistic identity development (Aron et al., 2019; Daignault et al., 2023), indicating a breadth of potential deleterious consequences for athletes.
ACEs as a Form of Trauma Outside of Sport
Many individuals are shaped by ACEs, which include forms of violence, neglect, and household dysfunction experienced in youth (Bennett, 2022; Brown et al., 2020). While few works examine prevalence and impacts of ACEs in athletic populations, it is clear that athletes bring personal histories with them into sport. Emerging research suggests ACE prevalence is similar between athletic and non-athletic populations (Brown et al., 2020; Powless et al., 2025), yet little is known about whether ACEs manifest differently in athletic versus non-athletic populations or how sport-specific demands shape their long-term impact. In more generalized populations, ACEs have been consistently linked to negative psychological symptoms and emotion regulation difficulties (Cole & Diaz, 2024; Miu et al., 2022; Thurston et al., 2023) and are associated with increased likelihoods for chronic health problems in adulthood (Bennett, 2022; Cole & Diaz, 2024). Scholars have additionally started to include other forms of adversities experienced in youth (i.e., social isolation, discrimination, and peer bullying) when examining ACEs given that these factors can have lasting negative impacts on health (Almeida et al., 2021; Lei et al., 2021; Lereya et al., 2015). It is important to further consider how ACEs manifest in athletic populations since sport is a unique context that could strengthen resiliency and/or be a site for increased adversities.
Attachment Theory and Trauma-Informed Care as Heuristics
Attachment theory provides a relational framework for understanding how interpersonal experiences shape athletes’ responses to adversity across development. The theory posits that early caregiving relationships influence life-long internal working models for safety, trust, and emotion regulation (Bowlby, 1982; Doyle & Cicchetti, 2017). IV in sport and ACEs are related to disruptions in caregiving relationships, so the theory provides a powerful framework for understanding how relational trauma can disrupt development and contribute to insecure attachment styles and mental health concerns in athletic populations (Davis et al., 2021; Finch et al., 2024; Salim & Winter, 2022). It is highly applicable to sport since coaches and other authorities serve in critical, caregiving relationships with athletes and are some of the most influential members of the athlete’s developmental environment (Alexander et al., 2023; Shaver & Mikulincer, 2007; Zogg et al., 2024). These relationships play a pivotal role in shaping athletes’ relational patterns and sense of identity in the sport domain (Davis et al., 2013) and profoundly shape their worldview and self-concept (Zogg et al., 2024), with emerging research highlighting that athletes with insecure authority relationships reported poorer well-being than those with secure attachments (Davis & Jowett, 2014; Davis et al., 2021). Moreover, attachment theory provides a framework for understanding athlete personal histories related to ACEs, including the roles of existing attachment styles and responses to later adversity in sport (Finch et al., 2024; Szeifert et al., 2025).
Trauma-informed care (TIC) is referenced in this study as a guiding, applied perspective given that scholars have called for systematic approaches to address IV in sport (Gattis & Moore, 2022; Kerr et al., 2019). TIC builds on attachment theory’s relational perspective by providing a systems-level framework that emphasizes how relational and organizational environments can either exacerbate or buffer the effects of trauma by promoting safety, trust, peer support, collaboration, empowerment, and cultural responsiveness (Huang et al., 2014). When viewed through an attachment-informed lens, TIC principles offer a way to translate relational theory into practical considerations for fostering positive, ethical, and effective relationships in sport, attending to athletes’ varied histories of adversity and supporting both performance and holistic well-being (Hussey et al., 2023; Shaikh et al., 2021). Within this study, TIC offers guidance to sport authority figures and organizations on implementing practices that are sensitive to athletes’ trauma histories and reduce the risk of relational traumatization within sporting environments. This combined use of attachment theory and TIC create a powerful framework for viewing an individual’s well-being and developing protocols to promote safety for trauma victims (Fflur et al., 2024; Zinn, 2020).
The Current Study
Athletes face unique risks for trauma both inside and outside of the sporting context, including coach violence, authority violence, and ACEs. Although an emerging body of literature has examined maltreatment, abuse, and trauma in sport, much of this work has relied on qualitative methodologies or has focused on singular sources of adversity (e.g., coach-perpetrated abuse) without empirically distinguishing between multiple trauma contexts. At the same time, broader maltreatment and ACEs research often fails to consider sport as a distinct relational environment characterized by unique power dynamics and authority structures. As a result, limited empirical work has examined how diverse sources of trauma experienced both in and out of sport may differentially relate to athlete mental health outcomes.
Given that athletes often enter sport with pre-existing trauma histories and may be exposed to additional relational harm within sport settings, there is a critical need to examine how combinations of prior and sport-based adversities are uniquely and additively associated with mental health symptomology. To fill this gap, the current study explores how overall experiences of coaching violence, authority violence, and ACEs are associated with current mental health symptomology. Mental health symptoms investigated in the current study included anxiety, post-traumatic stress disorder (PTSD), depression, and dissociation given their prior linkages with traumatic events experienced in and out of sport settings. It was hypothesized that each form of adversity would be positively associated with mental health symptoms, and interactions were explored to consider how symptom severity may differ based on different levels of sport-based violence and number of ACEs. Moreover, attachment theory and TIC are both utilized to provide relational and systematic implications of findings.
Method
Participants
Participants were 341 current and former athletes (Mage = 21.72 years, SDage = 4.56, 80.4% female) who were over 18 years of age, had dedicated a significant amount of time to sport, and had a meaningful coach–athlete relationship during their athletic participation. They primarily identified as heterosexual (78.0%) and White (87.1%), with a family income generally above $150,000 (24.3%). On average, participants participated in 19.77 (SD = 8.46) hours of sport per week, across 10.02 months per year (SD = 2.52).
Procedure
Approval for this research was granted by the Utah State University institutional review board as part of a larger funded study designed to examine trauma, mental health symptomology, and neuroimaging in athletes. Informed consent was obtained online prior to survey completion, and convenience sampling was used to recruit participants. These potential participants were informed of the study through in-person university classes, in-person recruitment at adult sport organization events, and online through social media postings shared with nonprofit sport organizations. All participants were prompted to independently take surveys online via RedCap (Harris et al., 2009; 2019).
Measures
Violence Towards Athletes
The Violence Toward Athletes Questionnaire (VTAQ; Parent et al., 2019) was used to measure lifetime reports of physical, psychological-neglectful, and sexual forms of violence directed towards athletes. This 36-item measure utilizes a 1–4 Likert scale response system where 1 indicates never, 2 indicates rarely (1–2 times), 3 indicates sometimes (3–10 times), and 4 indicates often (more than 10 times). Two items relating to aggressive conduct (e.g., asking athletes to injure opponents or behave aggressively) were removed prior to data collection given potential non-relevance for athletes that partake in non-contact sports, so 34 items from the VTAQ were adopted in the current study. Versions of the VTAQ-coach (VTAQ-C) and VTAQ-authority (VTAQ-AU) were utilized to screen for reported lifetime prevalence of physical, psychological-neglectful, and sexual forms of violence. Coaches included head, assistant, strength and other types of coaches, while authorities included any non-coach person occupying positions of power in sport (e.g., medical professionals, therapists, administrators). The two scales are identical in nature and differ only as a function of the question stem used at the start of the survey. Sum scores are used in the present study as recommended as an option for severity per guidance of Parent et al. (2019). In the present study, MacDonald’s Omega was calculated alongside Cronbach’s Alpha and offered adequate support for the instrument reliability for both the coach (ω = .96, α = .93) and authority scales (ω = .92, α = .91; Hayes & Coutts, 2020).
Adverse Childhood Experiences
A measure of ACEs experienced outside of the sporting context was created by summing scores of 13 items that were pulled from both the traditional ACEs scale (Felitti et al., 1998) and a revised and broader measure of adversities (Karatekin & Hill, 2019). Nine items measured traditional forms of ACEs (i.e., abuse, neglect, household dysfunction), and four additional items measured social isolation (1 item), discrimination (2 items), and peer bullying victimization (1 item; Felitti et al., 1998; Karatekin & Hill, 2019). Instructions were altered to ensure that participants only reflected on experiences outside of the sporting context (e.g., in this section, please do not include your experiences in sport). Although the traditional measure of ACEs includes 10 total items, one item on child sexual abuse was excluded from the current study because of potential legal implications around institutional guidelines for reporting child sexual abuse. The additional four items were included to create a measure that represented a wider range of adverse experiences. MacDonald’s Omega and Cronbach’s Alpha offer support for the reliability of the measure (ω = .85, α = .79).
Generalized Anxiety
The Generalized Anxiety Disorder scale (GAD-7) was used to measure generalized anxiety disorder (Spitzer et al., 2006). It is a 7-item scale where participants score themselves on a 0–3 Likert scale. A choice of 0 reflects not at all, 1 indicates several days, 2 indicates more than half the days, and 3 indicates nearly every day. The scale includes items such as “. . . not being able to stop or control worrying,” and “being so restless that it is hard to sit still.” The GAD-7 demonstrates acceptable levels of reliability (ω = .91, α = .82).
Post-Traumatic Stress Disorder
PTSD was measured via the International Trauma Questionnaire using 12-items for symptomology (ITQ; Cloitre et al., 2018). This portion of the survey instrument utilizes a 5-point Likert scale from 0 not at all to 4 extremely for items such as “. . . having upsetting dreams that replay part of the experience of are closely related to the experience,” and “. . .avoiding external reminders of the experience (for example, people, places, conversations, objects, activities, or situations).” The sum score scale demonstrated acceptable reliability to be included in present analyses (ω = .93, α = .84).
Dissociation
The Brief Dissociative Experiences Scale (DES-B; Dalenberg & Carlson, 2010) was used to measure dissociative symptoms. It is an 8-item scale that assesses severity and experiences of dissociation in adults across the past 7 days. A 5-point Likert scale that ranges from 0 not at all to 4 more than once a day allows participants to identify their experiences. The total sum score is used to capture an adult’s dissociation severity. In the present study, this scale demonstrated acceptable reliability (ω = .94, α = .86).
Depression
The Patient Health Questionnaire (PHQ-9) was used to measure depression in our sample (Kroenke et al., 2001). The PHQ-9 is a 9-item scale that utilizes a 4-point Likert scale where 0 represents not at all and 3 represents nearly every day. Participants self-score themselves on items such as “. . . little interest or pleasure in doing things,” and “. . . feeling bad about yourself – or that you are a failure or have let yourself or your family down.” Participant scores are summed to give a final value. MacDonald’s Omega and Cronbach’s Alpha offer support for the reliability of the measure (ω = .91, α = .82).
Data Analysis
All data cleaning and analyses were conducted using R version 4.5.0 (R Core Team, 2025) with the assistance of tidyverse, psych, furniture, and apaTables (Barrett & Brignone, 2017; Revelle, 2021; Stanley, 2021; Van Buuren & Groothuis-Oudshoorn, 2011; Wickham et al., 2019). In line with the recommendations of Tabachnick and Fidell (2014), descriptive statistics were calculated and examined prior to any inferential analyses. To preserve participant data, and, therefore statistical power, missing data were replaced through predictive mean matching (PMM) multiple imputation in the MICE package (Little, 1988; Van Buuren & Groothuis-Oudshoorn, 2011). This method, using type 1 matching, has been shown to perform well when imputing non-normal variables (Lee & Carlin, 2017). In addition, we elected to use a smaller nearest neighbor value (2.22, as opposed to the default setting of 5) in line with Kleinke’s (2017) recommendation for working with smaller sample sizes. A total of five iterations were imputed as any iterations beyond this have been shown to produce similar results (He et al., 2010). The results of the imputation were inspected using the MICE package’s densityplot() function. When computing Cronbach’s Alpha, MacDonald’s Omega, and Means with Standard Deviations, the mean values across all five imputed datasets were used and reported.
Due to the nature of the variables included in the present study, there were large numbers of outliers (e.g. coach and authority violence scores ≥80) which had potential to be influential observations in the modeling procedure. This is likely because violence, relatively, is not the normal experience in sport—however, due to the nature of the study, these observations were retained as they reflect the lived experiences of participants in our sample and are therefore representative outliers that are correctly measured (Quintano et al., 2010). To quantify this, we calculated and reported Cook’s distance for each model with the cut off set to 4/n (Arimie et al., 2020). We then fit ordinary least squares linear regression models which will be described below.
Measures of VTAQ-C, VTAQ-AU, and ACEs were predictors of interest in the present study. We centered the two VTAQ scores and the ACEs scale prior to including them in any interaction terms to mitigate potential multicollinearity issues (Afshartous & Preston, 2011). Four regression models were fit, with each having a different dependent variable: depression, dissociation, PTSD, or generalized anxiety. Each of these models included a three-way interaction term between violence toward athletes from coaches, violence toward athletes from authority figures, and ACEs. Each model was fit for each imputed dataset, the results of which were then pooled using the pool() function. Any significant interaction term was probed using the Johnson-Neyman method to identify potential regions of significance, revealing if there is a specific point at which the moderator becomes a significant influence on the slope of the independent variable or if this is consistent across all values. Covariates included the effects of weekly hours and months out of the year participants were active in sport to control for time spent in these domains since increased time in sport increases risks of violence. R2 statistics are reported along with adjusted values. Model diagnostics were checked using Q-Q plots, non-normality of residual plots, and variance inflation factors.
Results
Descriptive Statistics
Upon inspection, 12.9% of data were missing and missingness varied from 0.88% (months per year in sport) to 37.54% (items 7, 8, and 9 on the ITQ). Once missing data had been imputed at the item level, missingness was 0.0%, and no variables had concerning levels of kurtosis or skewness. Alpha and Omega were calculated and reported for all scales (Hayes & Coutts, 2020). Table 1 displays the means, standard deviations, and bivariate correlations across all study variables.
Means, Standard Deviations, and Correlations With Confidence Intervals.
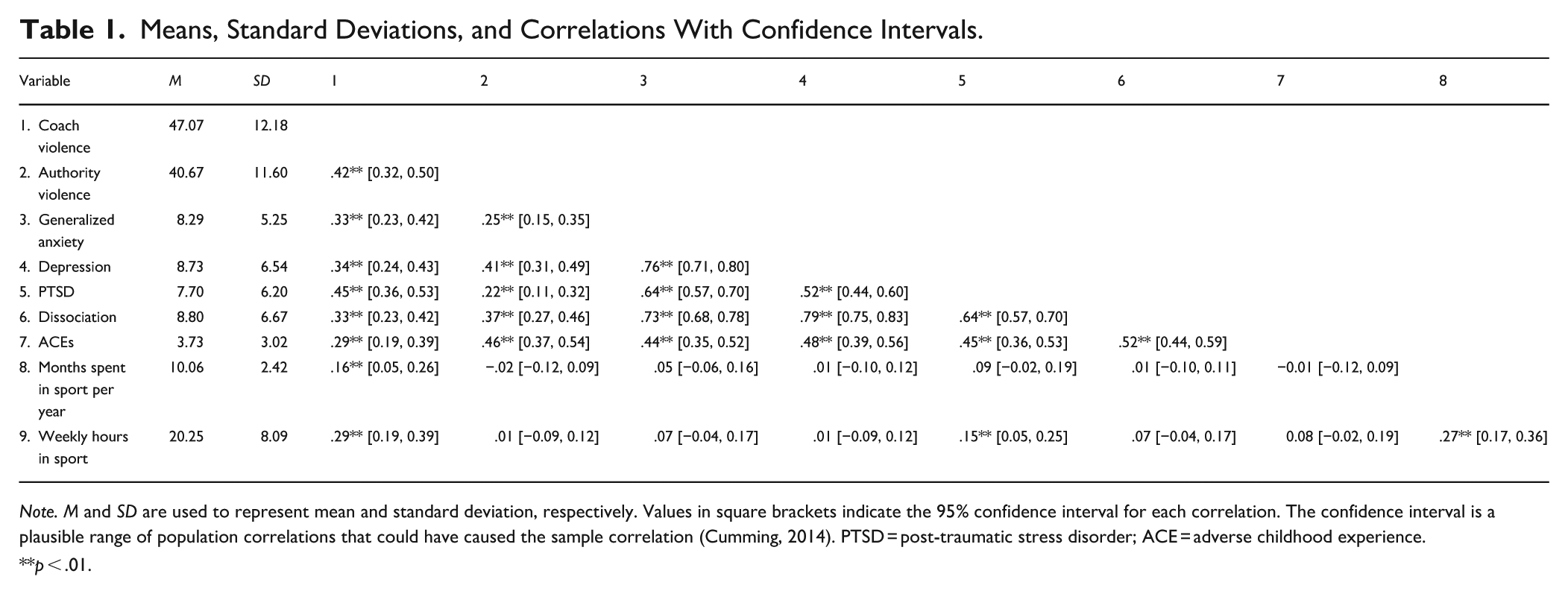
Note. M and SD are used to represent mean and standard deviation, respectively. Values in square brackets indicate the 95% confidence interval for each correlation. The confidence interval is a plausible range of population correlations that could have caused the sample correlation (Cumming, 2014). PTSD = post-traumatic stress disorder; ACE = adverse childhood experience.
p < .01.
Inferential Statistics
Full results of all models can be found in Table 2. Regarding generalized anxiety as the outcome, 25 influential cases of the total 341 observations were identified using Cook’s distance. As noted earlier, due to the nature of the study topic, these observations reflect the lived experiences of study participants and were therefore retained. This model identified coach violence (b = 0.11, 95% CI [0.06–0.17], SE = 0.03, p < .001), authority violence (b = 0.10, 95% CI [0.03–0.17], SE = 0.03, p = .004), ACES (b = 0.64, 95% CI [0.43–0.86], SE = 0.11, p < .001), and the interaction between coach violence and ACES (b = 0.02, 95% CI [0.01–0.04], SE = 0.01, p = .010) as significant predictors.
All Robust Regression Analyses.
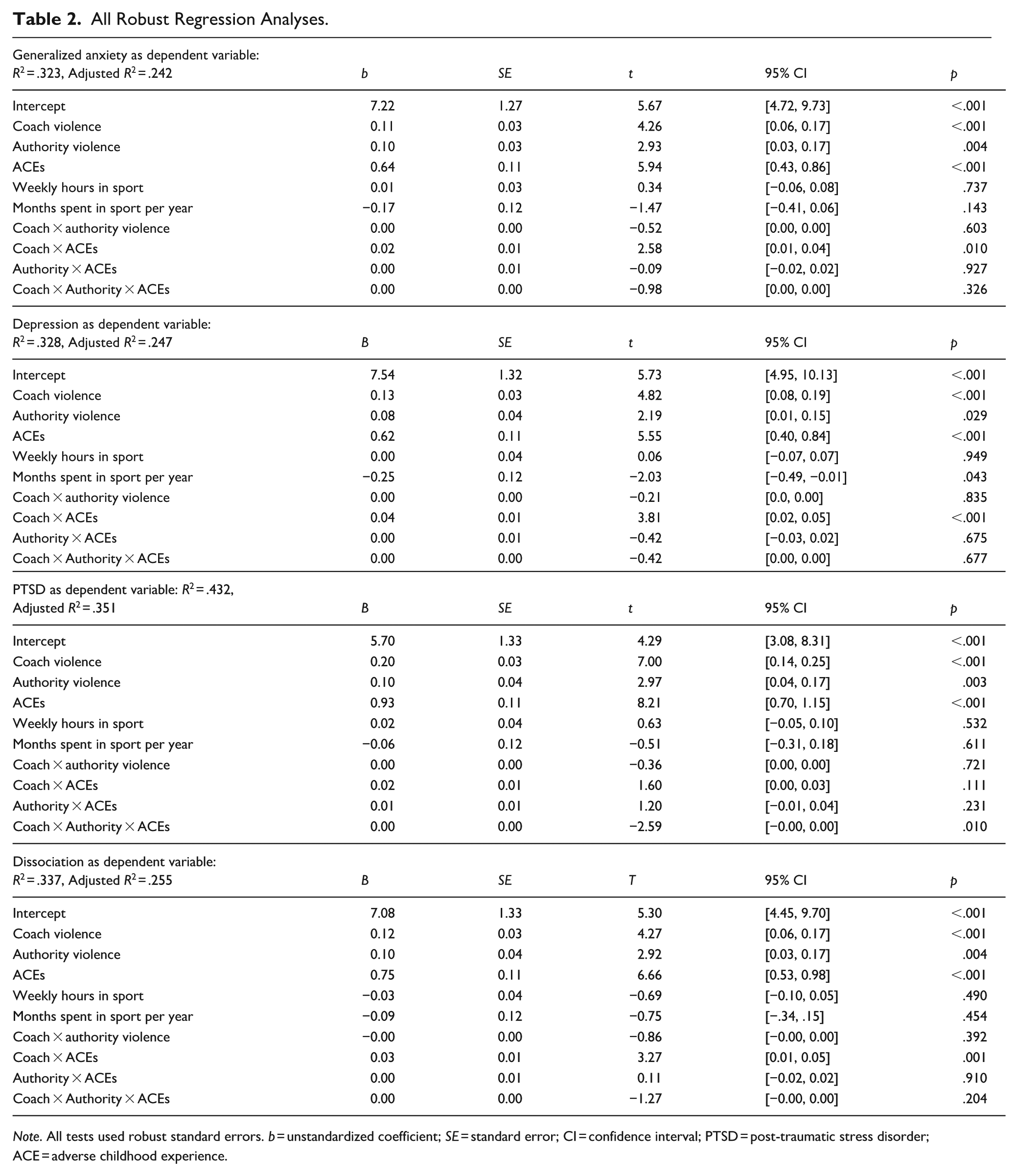
Note. All tests used robust standard errors. b = unstandardized coefficient; SE = standard error; CI = confidence interval; PTSD = post-traumatic stress disorder; ACE = adverse childhood experience.
With regards to depression, 20 influential cases were identified using Cook’s distance and retained in analyses. Model results showed that coach violence (b = 0.13, 95% CI [0.08–0.19], SE = 0.03, p < .001), authority violence (b = 0.08, 95% CI [0.01–0.15], SE = 0.04, p = .029), ACEs (b = 0.62, 95% CI [0.40–0.84], SE = 0.11, p < .001), the number of months per year spent in the sport context (b = −0.25, 95% CI [−0.49 to −0.01], SE = 0.12, p = .043) significantly predicted depression. In addition, there was a significant two-way interaction between coach violence and ACES (b = 0.04, 95% CI [0.02–0.05], SE = 0.01, p < .001).
When examining PTSD as the outcome, 16 influential observations were identified using Cook’s distance and retained in analyses. Coach violence towards athletes (b = 0.20, 95% CI [0.14–0.25], SE = 0.03, p < .001), authority violence (b = 0.10, 95% CI [0.04–0.17], SE = 0.04, p = .003), and ACEs (b = 0.93, 95% CI [0.70–1.15], SE = 0.11, p < .001) were positive predictors. There was also a three-way interaction between coach violence, authority violence, and ACES (b = 0.00, 95% CI [−0.00 to 0.00], SE = 0.00, p = .010).
Finally, when testing dissociation as the outcome, 18 influential observations were identified using Cook’s distance and retained in analyses. We observed that coach violence towards athletes (b = 0.12, 95% CI [0.06–0.17], SE = 0.03, p < .001), authority violence (b = 0.10, 95% CI [0.03–0.17], SE = 0.04, p = .004), and ACEs (b = 0.75, 95% CI [0.53–0.98], SE = 0.11, p < .001) were all significant predictors. Additionally, we observed a two-way interaction between coach violence and ACEs (b = 0.03, 95% CI [0.01–0.05], SE = 0.01, p = .001) that was subsequently probed with the Johnson-Neyman technique (see Figures 1–4).
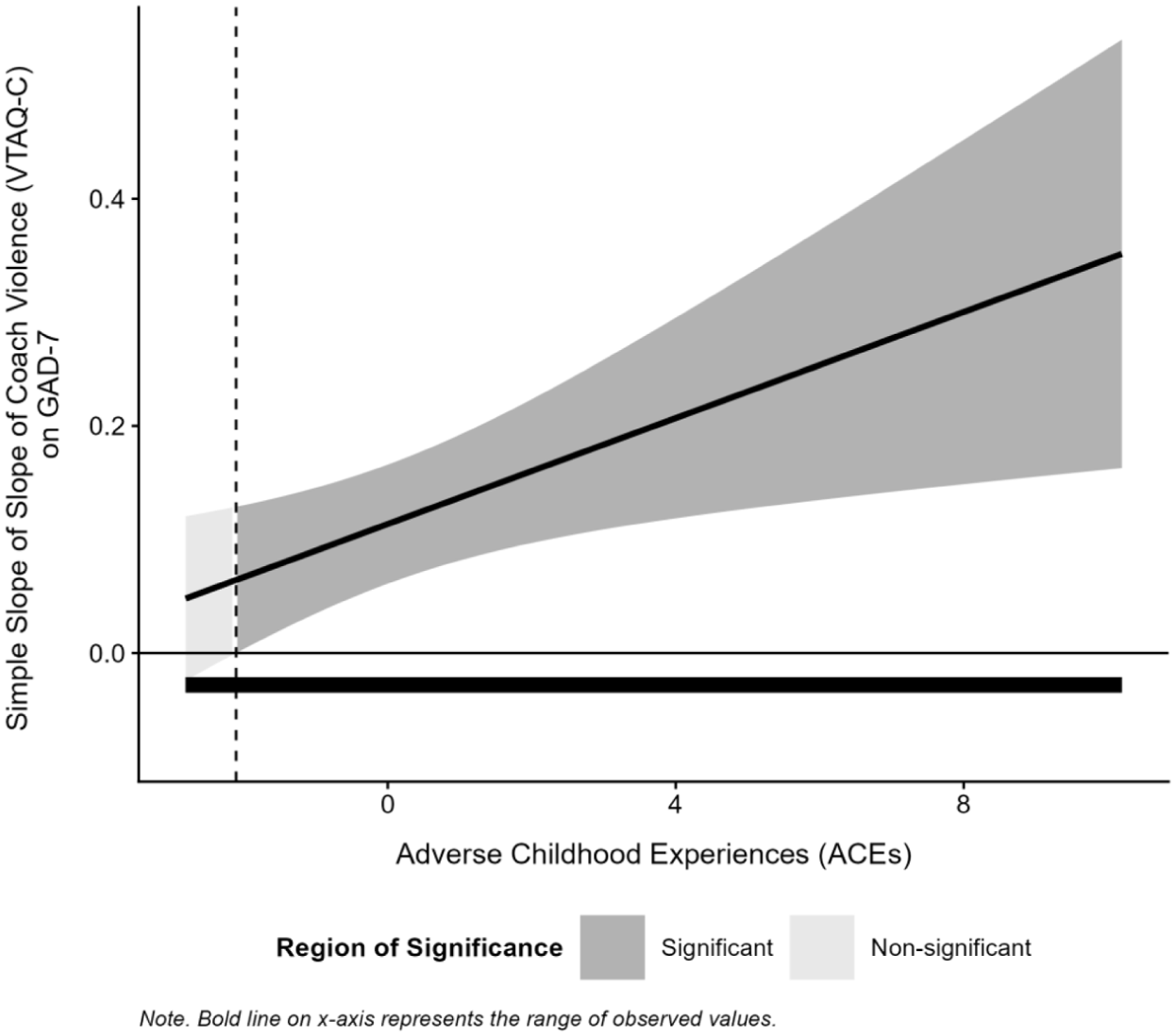
Interaction of coach violence and adverse childhood experiences on anxiety.
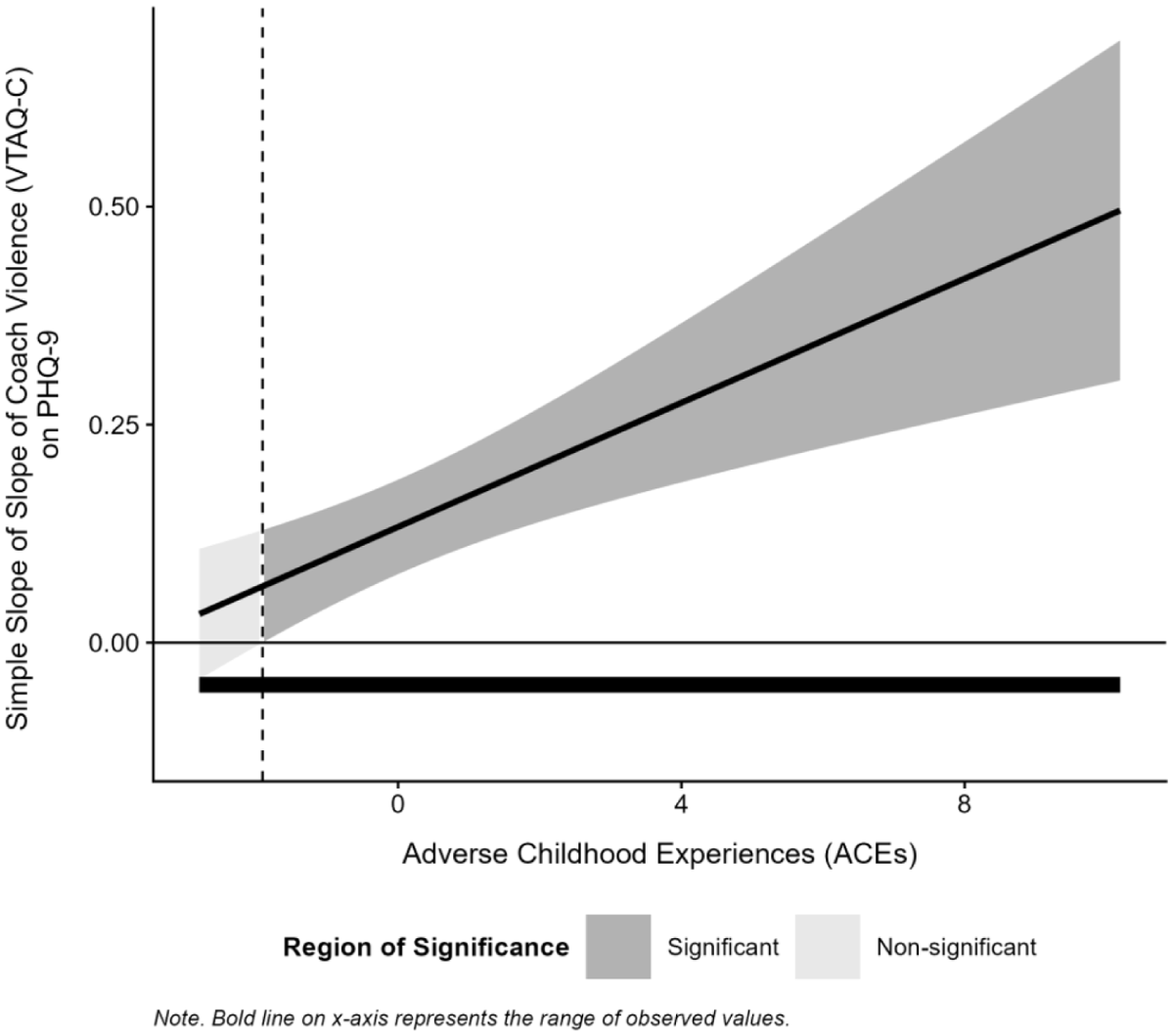
Interaction of coach violence and adverse childhood experiences on depression.
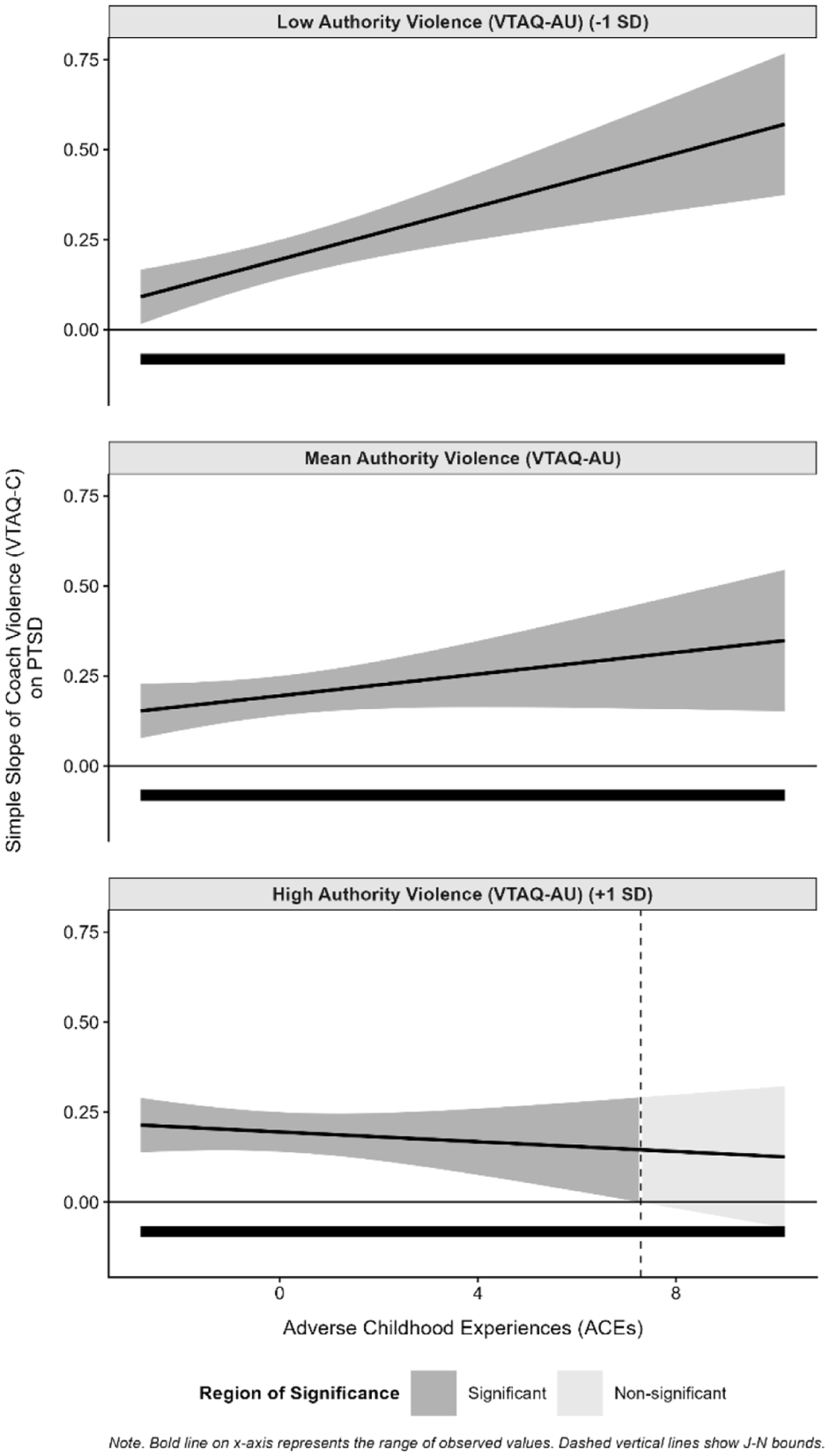
Interaction of coach violence, authority violence, and adverse childhood experiences on PTSD.
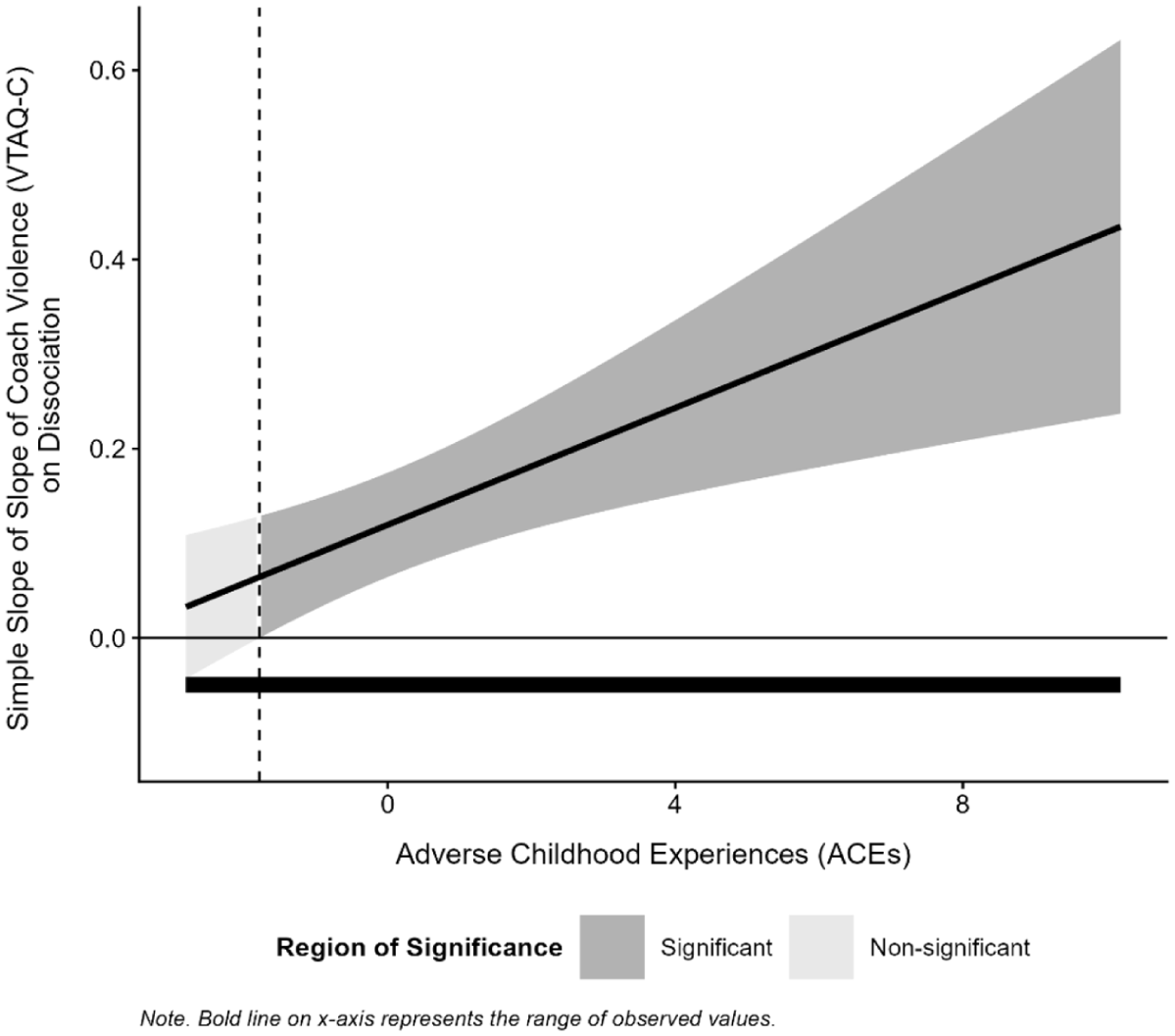
Interaction of coach violence and adverse childhood experiences on dissociation.
Discussion
While current scholarship on the topic of abuse in sport highlights the issue of mistreatment in sport, there is substantive gaps related to quantitative associations between traumatic events in and out of sports and mental health symptoms in U.S. athletic populations. Therefore, this study was designed to explore how coaching violence, authority violence, and ACEs were associated with current mental health symptomology. Findings suggest that ACEs, coaching violence, and authority violence were differentially and additively associated with athletes’ mental health symptoms. Subsequent sections interpret these findings primarily through an attachment-based lens to underscore the significance of relational trauma within athletic populations, with TIC referenced selectively in the discussion of applied and more systematic implications.
Coach–Athlete Violence as a Form of Trauma in Sport
Coaching violence was positively associated with anxiety, depression, PTSD, and dissociation symptoms. This finding aligns with previous qualitative research suggesting that abusive coach–athlete dynamics can be psychologically damaging to athletes (Alexander et al., 2023; Battaglia et al., 2017; Kerr et al., 2020; Salim & Winter, 2022). Furthermore, these results underscore the necessity of viewing sport through a relational lens. The coach–athlete relationship is inherently asymmetrical and developmentally salient, which positions coaches as central figures in shaping athletes’ experiences of safety and trust (Alexander et al., 2023; A. E. Stirling & Kerr, 2008). As such, this relational dynamic holds substantial power for harm, with our findings indicating that such experiences are associated with lasting impacts on athlete mental health.
From an attachment theory perspective, coach-perpetrated violence may establish or reinforce insecure attachment patterns by undermining relational security and failing to meet an athlete’s psychological needs, which can in turn reduce relationship quality and overall athlete well-being (Davis & Jowett, 2014). Given that prior experiences of coaching violence were associated with current mental health symptoms in the present study, it is evident that the coach–athlete relationship can maintain its own attachment pattern and that these relationships can uniquely influence an athlete’s well-being. Ultimately, coaches hold substantial relational power, and harm experienced in this relationship is not simply confined to sport but instead shapes athletes’ broader internal working models, interpersonal functioning, and long-term mental health (Alexander et al., 2024; Battaglia et al., 2017; A. E. Stirling & Kerr, 2008).
It is crucial that issues of coach–athlete violence are addressed at a systemic level (Gattis & Moore, 2022; Kerr et al., 2019; A. Stirling & Kerr, 2016). TIC and similar approaches provide coherent frameworks for addressing concerns of IV in organizations. TIC can specifically provide insights into proactive practices that reduce coercion, enhance predictability, and prioritize athlete psychological and relational safety (Huang et al., 2014). Organizations may reduce instances of IV and prevent outcomes related to relational harm by setting explicit behavioral standards for acceptable and unacceptable coaching practices and engaging in athlete-centered practices to facilitate safer coach–athlete relationships (Alexander et al., 2023; Bennett, 2024; Kerr et al., 2020). TIC frameworks focus on the development of positive relationships, and sport policies that focus on developing and maintaining positive coach–athlete relationships would be especially useful. Furthermore, athletes could receive education on coaching violence and trauma and those working with athletes could be required to complete continuing education on topics related to athlete violence and emotional safety (Alexander et al., 2023; Davis & Jowett, 2014; Salim & Winter, 2022).
Authority Violence
Authority violence was significantly and positively associated with anxiety, depression, PTSD, and dissociation symptoms. This study is among the first to quantify the relation of authority violence and mental health, and these preliminary findings provide empirical evidence that these distal authority–athlete relationships warrant greater attention within research literature. Moreover, these findings extend current research by demonstrating that relational harm in sport is not limited to the coach–athlete dyad but is also systemically embedded in broader relational imbalances often inherent to sport, including relationships that athletes have with sport administrators, medical professionals, and others (Gattis & Moore, 2022).
Several possible theoretical, conceptual, and empirical components may be driving findings in the current study. One theoretical explanation is that authority figures have meaningful and emotionally intimate interactions with fewer athletes compared to coaches, yet these interactions may still exert substantial influence on mental health outcomes for these athletes. Attachment theory suggests that the salience, frequency, and emotional intimacy of relationships affect the extent to which relational harm influences mental health outcomes. Therefore, authority figures who occupy caregiving positions (e.g., medical professionals, administrators) can function as secondary or conditional attachment figures, particularly when athletes rely on them for care, protection, or access to resources (e.g., athletic trainers aiding injury rehabilitation, administrators protecting athletes from coaching abuse; Haynes, 2023; Hooper et al., 2012; Salmoiraghi & Zarotti, 2025; Salmon & Young, 2009). Authority–athlete dynamics consequently influence an athlete’s sense of self, trust, and fulfilment of needs (Davis et al., 2021), and current findings provide empirical evidence that these relationships are meaningfully embedded within athletes’ attachment systems.
Conceptually, findings align with prior works that emphasize the role of sport systems in shaping athlete experiences and outcomes, including concerns related to power imbalances between athletes and authorities, establishing a culture of silence, and a tendency for bystander (in)action in the presence of IV (see Kerr et al., 2019; Roberts et al., 2020). While many sport authorities operate within rigorous and specific codes of conduct and training requirements (e.g., Health Insurance Portability and Accountability Act and ethical codes for medical professionals in U.S. contexts, American Counseling Association Code of Ethics for therapists), such safeguards may not fully mitigate risks of relational harm due to unique sporting constraints and pressures. Specifically, practitioners may become passive bystanders or even perpetrators of harm when accountability structures are weak or poorly enforced and within self-governed and performance-driven sport systems (Hartill & Rulofs, 2025). TIC is particularly well-suited to address these systemic vulnerabilities and offer guidance for translating more abstract awareness of relational power into concrete institutional practices. For example, sport organizations may implement mandatory, role-specific training for authority figures (e.g., medical staff, administrators) that explicitly address relational power, boundary-setting, and recognition of trauma-related distress in athletes (Mountjoy et al., 2016; Willson et al., 2021). Trauma-informed sport systems should also ensure access to independent, confidential reporting mechanisms that operate outside of performance hierarchies, thereby reducing fears of retaliation or career repercussions (Tak et al., 2024). Embedding routine health check-ins during periods of injury, rehabilitation, or transition—when psychological vulnerability and influence by authority figures may be heightened (Weiß et al., 2024)—offers a targeted strategy for reducing risks of authority–athlete IV.
One final alternative explanation for current results is empirical and includes the novelty of the scale utilized and the uniqueness of current sample characteristics. As the first published work to utilize the authority version of the VTAQ, these results provide initial empirical support for its utility in capturing authority-perpetrated violence yet indicate a need for further psychometric validation. Additionally, the composition of this sample may limit the robustness of these findings: many participants were from less competitive sport settings, and these athletes have fewer contacts with staff such as trainers or administrators (Kuhn et al., 2021). A majority of studies currently rely on more elite and Olympic-affiliated athlete samples when examining issues of violence and trauma (Aron et al., 2019; Rice et al., 2016; Willson et al., 2025), and the present findings extend the literature by demonstrating that authority violence is relevant across a broader range of sport contexts and athlete experiences.
ACEs and Mental Health
In the current study, ACEs explained the most variance in anxiety, depression, PTSD, and dissociation symptoms, which highlights the importance of recognizing that athletes often enter sport with trauma histories that can affect relational and psychological well-being. This aligns with robust literature demonstrating long-term mental health consequences of ACEs in general population samples (Haczkewicz et al., 2024; Hajat et al., 2020). Attachment theory provides a useful framework for interpreting these findings: early adversities may disrupt the development of secure internal working models related to safety, trust, and emotion regulation, thereby increasing vulnerability to later relational distress and mental health symptomology (Haczkewicz et al., 2024; Howard et al., 2023). Collectively, these findings indicate that athletes are not uniformly resilient and instead enter sport contexts with pre-existing relational vulnerabilities, emphasizing the need for sport environments to actively and explicitly support psychological safety.
Given that athletes enter sport with unique vulnerabilities, sport systems should adopt principles of TIC that avoid reinforcing powerlessness or shame. Trauma-informed practices may help buffer the effects of early adversity by promoting relational stability, emotional safety, and trust (Ortiz, 2019), thereby supporting secure relational attachments. Such approaches include establishing predictable routines, supporting athlete choice, and fostering emotionally safe environments (Berger et al., 2024; Whitley & Bartlett, 2023). Emotionally safe team environments should be built on compassion, consistency, and positive relationships since this can help counter the lasting effects of ACEs (Hambrick et al., 2019; Whitley & Bartlett, 2023). Moreover, trauma-informed principles can be utilized to create safe environments by normalizing and not stigmatizing mental health conversations, framing help-seeking in positive ways, and consistently using supportive communication styles (Cosh et al., 2023; Huang et al., 2014). Together, these practices offer practical strategies for reducing the reactivation of trauma-related distress among athletes with significant adversity histories.
Interactions Between Sport Violence and ACEs
Current analyses included significant and positive two-way interactions between coach-perpetrated violence and ACEs for anxiety, depression, and dissociation symptoms and a positive three-way interaction among coach IV, authority IV, and ACEs for PTSD symptoms. These findings suggest that the effects of sport-related violence on mental health are shaped by athletes’ prior relational histories and the broader relational contexts in which harm occurs, and that different patterns of experiences may be related to different mental health outcomes.
Affect and Mood
Two-way interactions indicated that athletes with a history of ACEs reported elevated affect and mood-based symptoms (e.g., anxiety, depression, dissociation) in the presence of coach-perpetrated violence. One way to interpret the implications of these findings is to consider how ACEs might sensitize individuals to subsequent relational stressors. Attachment theory postulates that early adversities disrupt the development of emotion regulation capacities and internal working models of relationships, thereby altering coping capabilities and increasing susceptibility to later interpersonal harm (Cole & Diaz, 2024; Kascakova et al., 2025; Miu et al., 2022). As such, it is possible that exposures to coach-perpetrated violence reinforce or reactivate earlier relational disruptions and contribute to heightened affective and dissociative symptomology.
Reports of ACEs may also represent a pattern of instability and inaccessibility to resources in the current sample, meaning that those that reported ACEs had less access to support and resources when facing coaching abuse. This could reflect differences in athletes’ broader social and structural contexts. For example, emerging research in maltreatment and intimate partner violence literatures suggests that mental health outcomes vary based on perpetrator and child characteristics, rather than being reflective of simple cumulative exposure (Ayer et al., 2016; Giesbrecht et al., 2025; Li et al., 2024). Within sport, disparities in access to mental health services, medical care, or protective relationships could further influence how ACEs and coaching violence translate into psychological distress. Given that these sociodemographic and relational variables (e.g., gender, race, relationship quality) are likely to shape how athletes experience and respond to both early and later adversity, future research should consider how to assist athletes with different risk and experiential profiles.
Trauma Symptomology
While smaller in magnitude compared to two-way interactions for anxiety, depression, and dissociation symptoms, a three-way interaction was exhibited for PTSD symptoms and is discussed given potentially unique empirical and practical implications. A combination of increased ACEs and increased coach-perpetrated violence was specifically associated with higher PTSD symptoms at lower levels of authority-perpetrated violence. Notably, the steepest increases in PTSD symptoms and coaching violence with ACEs were observed among athletes reporting the lowest levels of authority violence, and the flattest increases in PTSD symptoms and coaching violence with ACEs were observed among those athletes reporting the highest levels of authority violence.
This finding may be due to characteristics of the current sample and the distribution of authority-perpetrated violence. Athletes reported being involved in less elite sport settings compared to samples seen in other research studies (Aron et al., 2019; Rice et al., 2016; Willson et al., 2025), and less than one-third of the sample reported ever experiencing any form of authority violence. As such, athletes reporting higher levels of authority violence may represent a distinct subgroup embedded in more structured sport systems (e.g., collegiate athletics) where interactions with multiple authority figures were more common. Additionally, these environments may provide greater access to resources (e.g., medical care, mental health services), which could mitigate or buffer the psychological impact of cumulative trauma exposure (Bany-Mohammed et al., 2025; Schneider et al., 2020). In contrast, athletes that experience ACEs and coach-perpetrated violence but that had limited exposure to authority figures may have lacked comparable access to support, resulting in a stronger association with PTSD symptoms.
Current preliminary findings suggest that PTSD symptoms may be related to contextual dynamics inherent to sport, and this means it is important to consider how sport systems contribute to risks of coach and authority violence. Unlike anxiety, depression, and dissociation—which often reflect broader affective distress or coping responses—PTSD symptoms are inherently trauma-specific and are characterized by symptoms of re-experiencing the traumatic event (e.g., flashbacks, nightmares) (American Psychiatric Association, 2022; Jongedijk et al., 2023). More complex or prolonged cases of PTSD can also include symptoms related to affective dysregulation, negative self-concept, and relational disturbances (Giourou et al., 2018). As such, PTSD includes trauma-specific symptoms and detrimental impacts to coping, identity, and relationships; these symptoms are likely to be more strongly influenced by whether athletes have access to advanced, trauma-informed support and opportunities to recognize and process their trauma. More research is needed to better understand the role of broader structural and contextual factors, including access to resources and the organization of sport systems, in shaping PTSD and other symptoms. Taken altogether, findings suggest a need to consider the nuanced, contextual aspects of cumulative adversity and the resources available to athletes who face increased vulnerabilities.
Limitations and Future Directions
Despite the contributions of the current study, several limitations should be acknowledged. First, the cross-sectional design prevents causal conclusions and limits interpretation of temporal relationships. Future work should consider employing longitudinal designs to better understand how violence affects mental health symptomology and how timing may play a role in shaping experiences and outcomes for athletes. Second, the study relied on self-report data, which requires participants to more invariantly know and understand aspects of coaching violence, authority violence, and ACEs. This is challenging due to the requirement of recognition and the sensitive nature of such a topic. Although some research suggests that many adult athletes can recognize certain forms of violence that occur in sport (Adams et al., 2024; Alexander et al., 2023), there may be differences in the ways that they interpret severity and behaviors across sport and non-sport contexts. Furthermore, topics related to violence/trauma are sensitive, and there are challenges to ethically recruiting participants. Future work should assess how athletes may understand concepts related to violence in and outside of sport environments and should also consider how to best and most ethically recruit participants. Third, the sample was predominantly White and female, which may limit generalizability across genders/sexes, and racial/ethnic groups. This limitation is additionally discussed in the diversity statement subsection. Given the gender composition of the sample (80.4% women), gender-specific analyses were not conducted, which limits conclusions regarding potential gender differences. Future research should consider how prevalence rates and associations of traumatic events and mental health outcomes differ based on participant demographics. Ultimately, continued theoretically informed research is needed to understand the issue of trauma in athletes and to evaluate the effectiveness of trauma-informed practices in sport organizations.
Diversity Statement
The current sample was composed primarily of White, heterosexual, former and current female athletes from higher-income families in the Western United States. Therefore, these findings are limited in their generalizability to more diverse athlete populations. Experiences of trauma and mental health symptomology may vary substantially based on race, ethnicity, socioeconomic status, nationality, gender identity, and sexual orientation. Future research should consider intentional and ethical ways to recruit more diverse and representative samples since this better captures the experiences of athletes across intersecting identities.
Conclusion
The current study was designed to explore the impact of life-long trauma in and out of sport on current mental health symptomology in current and former adult athletes while utilizing attachment theory and TIC as guiding heuristics for understanding findings. The results provided partial support for our hypotheses. Specifically, experiences of coaching violence, authority violence, and ACEs were strongly and positively associated with current reports of depression, anxiety, PTSD, and dissociation symptomologies. Two-way interactions between coach-perpetrated violence and ACEs were associated with anxiety, depression, and dissociation symptoms, and a three-way interaction among coach IV, ACEs, and authority-perpetrated violence was identified for PTSD symptoms. These findings emphasize that athletes enter sport with their own vulnerabilities and that experiences in sport can impact mental health and well-being across all life domains. Attachment theory and TIC highlight the need for sport organizations to recognize the role of relationship dynamics in facilitating post-traumatic growth versus exposing athletes to further violence and harm. Accordingly, organizations should establish standards for coaches and other authority figures, taking active steps to promote athlete autonomy and safety. Future research should employ longitudinal designs across more diverse samples to further clarify these associations and to guide evidence-based approaches for prevention and intervention in sport contexts. Ultimately, advancing trauma-informed sport systems is essential for protecting athletes and fostering environments where performance and well-being can coexist.
Footnotes
Acknowledgements
No acknowledgments are applicable for this manuscript.
ORCID iDs
Ethical Considerations
The study was approved by the Utah State University Institutional Review Board (#13257) and was initially approved on April 11, 2023. Claude Artificial Intelligence was utilized to provide technical assistance in troubleshooting coding for the Johnson-Newman function in R during data analysis; all analytic decisions, interpretation of results, and reporting were conducted by the authors.
Consent to Participate
All participants provided online, written informed consent prior to participating.
Consent for Publication
Not applicable, as no individual responses are being shared.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: This research study is a part of a larger project that was – in part – supported by the Utah State University Graduate Research and Creative Opportunity (GRCO) grant offered by the Office of Research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Data Availability Statement
Data are available for request by the second author.