
Abstract
Transgender and nonbinary (trans) individuals experience high rates of intimate partner violence (IPV), contributing to elevated vulnerability to human immunodeficiency virus (HIV) and other sexually transmitted infections (STIs). While prior research has established associations between IPV and HIV risk, little is known about the mechanisms through which IPV affects engagement in HIV/STI prevention among trans populations. This study qualitatively explored how varied experiences of IPV may impact prevention behaviors, including pre-exposure prophylaxis (PrEP) use, condom negotiation, and HIV/STI testing, within the broader context of structural and interpersonal inequities. We conducted semi-structured interviews with 32 racially and ethnically diverse trans participants who reported IPV in a prior relationship and with 10 key informants who had experience working with this population. Interviews explored experiences of IPV, sexual health decision-making, and barriers to accessing sexual health services. Transcripts were analyzed using applied thematic analysis. Coding combined deductive and inductive approaches, and intercoder agreement was established through team consensus. Four major themes were identified: (1) partner directly interfering with HIV/STI prevention, in which abusive partners restricted access to PrEP, condoms, or HIV/STI testing as a form of control; (2) fear of partner reactions interfering with prevention engagement, where anticipated conflict or violence led survivors to avoid sexual health discussions or care; (3) structural barriers shaping sexual health and safety, highlighting how poverty, stigma, and lack of affirming care compounded IPV-related risks; and (4) gaps in services and suggestions for improvement, emphasizing the need for trauma-informed, gender-affirming, and community-driven interventions in this area. Findings illustrate how IPV may undermine HIV/STI prevention through both direct partner interference and indirect mechanisms rooted in fear, control, and systemic inequity. Addressing these barriers will require a combination of integrated, affirming, trauma-informed, and community-driven interventions that link IPV support with affirming sexual health services along with an expansion of existing IPV services to address the needs of trans people.
Keywords
Introduction
Transgender and nonbinary (trans) 1 individuals experience disproportionately high rates of intimate partner violence (IPV) compared to their cisgender peers (Anderson, 2020; Peitzmeier et al., 2020; Stephenson et al., 2020). Over half (54%) of trans people in the United States report having experienced some form of IPV, including psychological abuse, physical violence, or coercive control (James et al., 2016). IPV is strongly associated with increased HIV and sexually transmitted infection (STI) vulnerability, as well as reduced engagement in prevention behaviors such as pre-exposure prophylaxis (PrEP) use, condom use and HIV/STI testing (Becasen et al., 2019; Brennan et al., 2012; El-Bassel et al., 2022; Heintz & Melendez, 2006; Mimiaga et al., 2019). However, there remains a paucity of research on how IPV may influence sexual health and prevention behaviors among trans individuals, resulting in a lack of the understanding needed to implement effective interventions that integrate affirming IPV support with sexual health services.
The disproportionately high rates of IPV and HIV/STI burden among trans individuals reflect shared structural determinants of health (Baral et al., 2013; Becasen et al., 2019; Centers for Disease Control and Prevention [CDC], 2013; Hughto et al., 2015; Magno et al., 2019). HIV prevalence remains substantially elevated among trans populations, with laboratory-confirmed estimates of 14.1% among trans women and 3.2% among trans men in the United States (Becasen et al., 2019). The HIV burden is especially high among Black (44.2%) and Latina (25.8%) trans women (Becasen et al., 2019), reflecting intersecting impacts of racism, transphobia, and transmisogyny (Romero, 2019). These disparities are not solely the result of individual behaviors but are rooted in structural violence, including stigma, discrimination, and exclusion from health, legal, and economic institutions (Baral et al., 2013; Becasen et al., 2019; CDC, 2013; Hughto et al., 2015; Magno et al., 2019). Barriers such as limited access to gender-affirming care, economic marginalization, and medical mistrust can further reduce engagement in HIV/STI prevention (Maragh-Bass et al., 2024; Ogunbajo et al., 2021; Storholm et al., 2024; Sullivan et al., 2024), while experiences of trauma, homelessness, and survival economies can heighten vulnerability to both IPV and HIV/STIs (McCann & Brown, 2018; Ogunbajo et al., 2021; Yang et al., 2024).
IPV may undermine engagement across the HIV/STI prevention continuum for trans people, including HIV/STI testing, PrEP initiation and adherence, and condom negotiation, by inducing fear of retaliation, constraining autonomy, and limiting access to care (Becasen et al., 2019; Brennan et al., 2012; El-Bassel et al., 2022; Heintz & Melendez, 2006; Mimiaga et al., 2019). Trans survivors have reported concerns that initiating PrEP, carrying condoms, or seeking HIV testing may provoke suspicion or violence from a partner (Nieto et al., 2021; Sevelius et al., 2016; Wilson et al., 2015). Emerging evidence suggests that IPV may act as a barrier to PrEP uptake and adherence, but these relationships have not been fully explored among trans individuals (Sevelius et al., 2016; Wilson et al., 2015; Zamantakis et al., 2023). Additionally, structural conditions, such as stigma in healthcare settings, lack of trauma-informed care, and exclusion from prevention messaging, may further compound the effects of IPV (Marrow et al., 2024; Zamantakis et al., 2023). Yet despite growing recognition of these linkages, existing research has largely been quantitative, cross-sectional, and reliant on IPV measures designed for cisgender heterosexual populations, limiting the ability to capture the unique experiences of trans survivors (Marrow et al., 2024; Peitzmeier et al., 2020). As a result, critical questions remain regarding how power dynamics, gender affirmation, and partner control intersect to influence HIV/STI prevention within trans relationships. Qualitative research is essential to understand these complex interpersonal and structural mechanisms, amplify survivors’ perspectives, and identify actionable strategies to improve prevention and care.
Guided by syndemic theory (Brennan et al., 2012; Operario & Nemoto, 2010; Poteat et al., 2016; Singer, 1994) and the gender minority stress and resilience (GMSR) framework (Brooks, 1981; Goldenberg et al., 2020; Hendricks & Testa, 2012; Lefevor et al., 2019; Meyer, 2003; Rich et al., 2020; Testa et al., 2017), the present study conceptualizes IPV as both a relational and structural determinant of health. Syndemic theory posits that co-occurring psychosocial and structural conditions, such as trauma, depression, and discrimination, can interact to exacerbate vulnerability to health outcomes, including HIV (Singer, 1994; Stall et al., 2001, 2008). The GMSR framework extends this by highlighting the unique stressors associated with gender marginalization, while also acknowledging community strength and coping as protective factors (Meyer, 2015; Operario & Nemoto, 2010; Reisner et al., 2016; Testa et al., 2015). Together, these frameworks underscore that IPV, HIV risk, and structural inequities are mutually reinforcing processes that demand integrated, community-informed responses.
The current study draws on in-depth interviews with trans individuals who experienced IPV, and with key informants who have subject matter expertise, to understand better the mechanisms linking IPV and HIV/STI prevention. Specifically, we explored how IPV may influence engagement in prevention behaviors such as PrEP use, condom negotiation, and HIV/STI testing; how fear, control, and structural vulnerability might constrain sexual health autonomy; and how survivors and service providers envision pathways toward safer, more affirming prevention approaches. This article aims to deepen understanding of how IPV affects HIV/STI prevention engagement among trans people and to inform the development of trauma-informed, gender-affirming, and community-driven interventions.
Methods
Study Design
This qualitative study was conducted as part of Phase I of the RADIANT (Relationships And Dynamics—Improving Advocacy for Nonbinary and Trans) project, a national two-phase longitudinal cohort study examining the intersection of IPV and HIV/STI prevention among trans individuals (Storholm, Horvath, et al., 2025). Phase I employed a qualitative descriptive design using semi-structured interviews with trans participants and key informants to explore the relationship between IPV experiences, gender identity-specific stressors, and sexual health outcomes. Phase I was designed to inform the development of the Phase II quantitative survey and to guide culturally responsive recommendations for IPV and HIV/STI prevention interventions. Data collection and analytic procedures were grounded in trauma-informed, community-engaged research practices (Champine et al., 2022; DePrince et al., 2022; Restar et al., 2023) to ensure that findings reflected the priorities, language, and lived realities of the communities most affected by IPV and HIV disparities.
Forming the Community Advisory Board
A Community Advisory Board (CAB) composed of trans community leaders and advocates was established to ensure that the study was grounded in community priorities and lived experience. Fifteen CAB members were recruited nationally through word-of-mouth referrals and online outreach via Instagram and Facebook. Members were intentionally selected to reflect diversity across geography, age, gender identity, and racial/ethnic background, reflecting the trans communities affected by IPV and HIV.
The CAB met virtually on a monthly basis and members were compensated for their time. Throughout Phase I, the CAB played a central role in shaping study design and implementation. Members reviewed and refined the semi-structured interview guide, ensuring sensitivity and cultural relevance of questions related to IPV and sexual health. The guide was also grounded in the study’s theoretical frameworks. Consistent with syndemic theory, questions were designed to elicit how co-occurring and mutually reinforcing conditions—such as violence, stigma, structural marginalization, and HIV/STI risk—intersected in participants’ lives. Drawing on the GMSR framework, the guide included questions about identity-specific stressors, anticipated rejection or conflict, and sources of community connection, support, and coping. They also provided guidance on recruitment strategies and outreach materials to enhance safety, confidentiality, and inclusion of participants with varied lived experiences of violence.
Beyond the planning phase, CAB members contributed to study recruitment as well as the interpretation of preliminary findings, helping to validate and contextualize the results with community perspectives. CAB members were invited to contribute to study manuscripts, and one member elected to assist with the drafting of this manuscript and is listed as a co-author. Other members of the CAB are assisting with other manuscripts and will also assist with community dissemination efforts, including presentations and summaries for academic and nonacademic audiences. This participatory structure ensures that the entire research process is trauma-informed, culturally grounded, and community-driven.
Participant Recruitment
Data were collected between April and October 2024 as part of the Phase I qualitative component of RADIANT. A purposive sampling strategy was used to ensure diverse representation across gender identity, race, ethnicity, and geographic region. Eligibility criteria included: (1) identifying as transgender or nonbinary; (2) being aged 18–45; (3) having been in a romantic relationship within the past 5 years; (4) reporting experience of IPV in at least one of those previous relationships in the past 5 years; and (5) residing in the United States. Additional key informants were recruited, including physician assistants, medical doctors, program managers/directors, and therapists who had experience providing clinical and/or social services to trans clients affected by IPV.
Participants (n = 32) were recruited using online and venue-based methods (e.g., Grindr, Instagram, Facebook, and word-of-mouth referrals). Key informants (n = 10) were recruited through referrals and email outreach to relevant organizations. To identify key informants, the study team worked together with the CAB to generate a list of professionals working in the context of IPV and sexual health programs with trans persons through a combination of our professional networks and internet searches. We then emailed members of the list to ask if they would be willing to participate in an interview focused on IPV and sexual health services for trans individuals experiencing IPV.
Data Collection
Eligibility for participants was determined through an online screener that collected demographic information, relationship history, and prior IPV experience. IPV experience was assessed using a single self-identification item rather than a published screening scale; potential participants were asked, “Would you characterize any of your romantic relationships in the past 5 years as abusive or violent?” (yes/no), and those who responded “yes” met this eligibility criterion. Individual semi-structured interviews explored participants’ sexual and romantic relationships, experiences of IPV (including physical, sexual, and psychological forms), gender identity–specific stressors and their relationship to IPV, and the impact of IPV on sexual health and well-being. Example questions included: “Are there any unique ways that trans and nonbinary persons experience abuse or violence in their relationships?” “How might a person’s trans or nonbinary identity be used against them by their partner?”, and “How might an abusive or controlling partner impact your sexual health and well-being?”
Key informant interviews explored professional roles, client populations served, approaches to IPV screening and training, their experiences delivering IPV and sexual health services to trans clients, their awareness of service gaps, and recommendations for improving care. Example questions included: “Can you describe the services that your program provides?”, “Do you have suggestions on ways to improve services for trans and nonbinary individuals who have experienced violence?”, “In your experience, how has partner violence, control, or abuse affected trans/non-binary persons’ sexual health and safety?”, and “In your experience, how has partner violence, control, or abuse influenced trans and nonbinary persons’ ability to protect themselves sexually?”
All participant and key informant interviews were conducted virtually via Zoom by a research assistant trained in trauma-informed qualitative interviewing. Interviewers had lived experience and/or extensive prior work on IPV with trans populations. To maximize participants’ sense of safety and control, interviewers used a range of trauma-informed practices throughout each interview. They emphasized confidentiality and worked to build trust, asked permission before introducing sensitive topics, and prepared participants for upcoming questions by previewing them and explaining the rationale for asking. Interviewers used survivor-centered language and reminded participants that they could decline or skip any question, take breaks, or proceed at their own pace, and they normalized silence and unhurried pacing. Participants were offered relevant support resources during and after the interview, and interviewers were likewise provided with self-care resources and debriefing support. Interviews lasted approximately 1 hr and were audio-recorded with participant consent. Participants and key informants received a $100 gift card for their time. The San Diego State University Institutional Review Board approved all study procedures.
Qualitative Analyses
Audio recordings were transcribed verbatim, de-identified, and analyzed using applied thematic analysis (Guest, 2012). Three research assistants led data collection, coding, and analysis, meeting regularly to refine the codebook and ensure consistency. The principal investigator provided analytic oversight and participated in consensus discussions. Coding began with a deductive approach based on the interview guide and existing literature, followed by inductive refinement through close reading of transcripts (Guest, 2012). Intercoder agreement was assessed by two coders double-coding transcripts, discussing coding discrepancies, and updating the codebook accordingly. Once a minimum interrater reliability of >0.70 was obtained (Cohen, 1960; O’Connor & Joffe, 2020), coders began independently coding the remaining transcripts. Once all transcripts were coded, themes were developed iteratively through group discussions and refined through consensus (Creswell & Miller, 2000). Analyses were conducted using Dedoose qualitative software (SocioCultural Research Consultants LLC, 2017). The research team brought relevant lived experience and identities to data collection and analysis. All members of the research team identified as LGBTQ+, many identified as transgender or nonbinary, and the CAB was composed entirely of transgender and nonbinary community members; some members of the team also had personal experience of IPV. These shared identities and experiences supported reflexivity throughout coding and interpretation and helped ensure that findings remained grounded in the lived realities of the communities most affected by IPV and HIV/STI disparities.
Results
Participant Characteristics
A total of 32 trans participants completed qualitative interviews between April and October 2024. The sample reflected broad diversity in terms of age, gender identity, racial and ethnic background, and geographic region of the United States (see Table 1). Participants ranged in age from 19 to 40 years (M = 28.1). Gender identities for participants included transgender women (n = 12), transgender men (n = 11), and nonbinary individuals (n = 9). Most participants identified as Hispanic/Latinx (n = 10), White (n = 9), Multiracial (n = 7) and/or Black or African American (n = 5).
Participant Characteristics (N = 32).
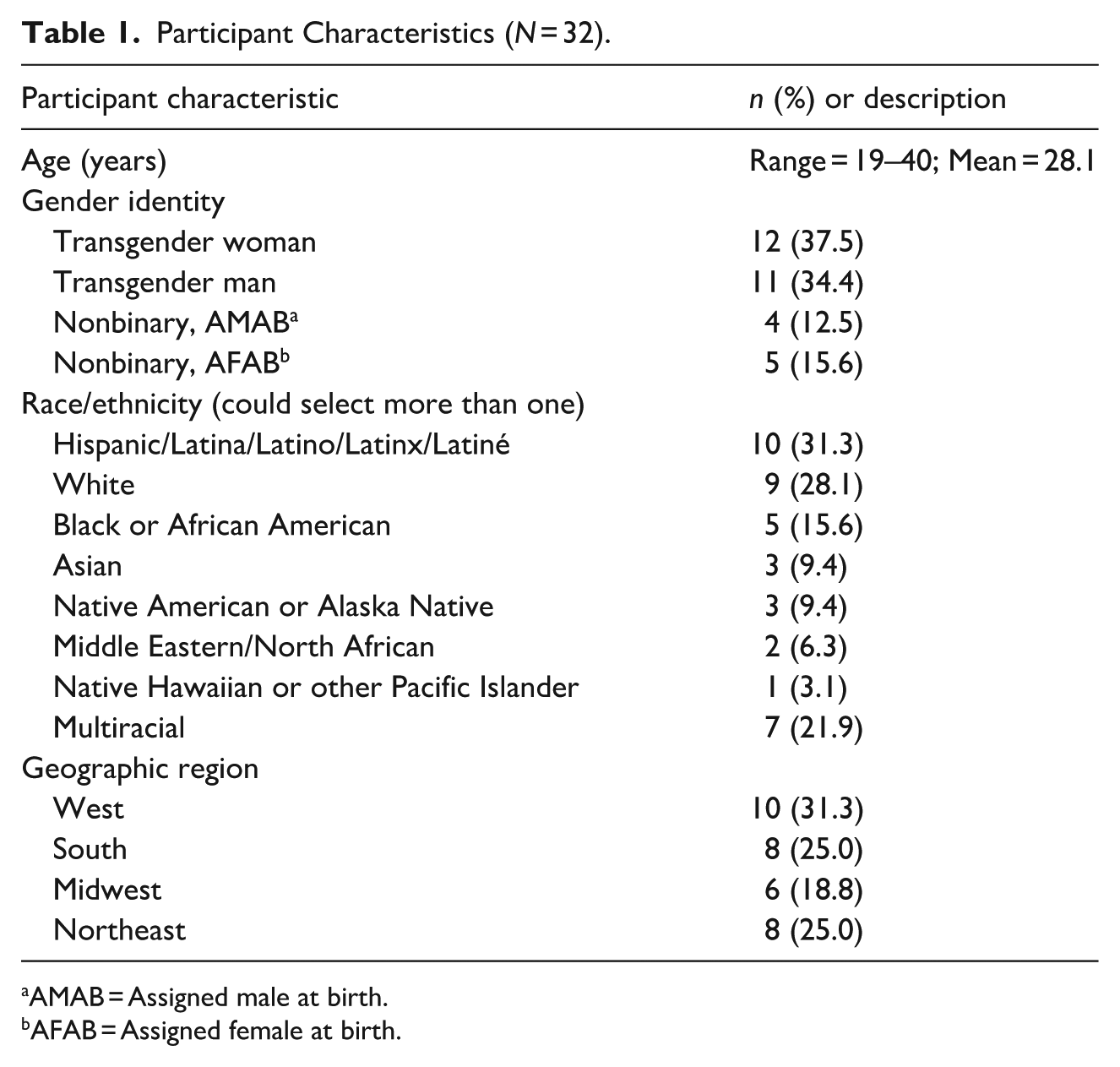
AMAB = Assigned male at birth.
AFAB = Assigned female at birth.
Key informants (n = 10) represented professional backgrounds including behavioral health, medicine, and community-based program management (see Table 2). Their roles included program directors, program supervisors, clinicians, and academic medical faculty specializing in HIV, infectious disease, reproductive health, and transgender health. Because key informants were recruited for their professional expertise, their demographic characteristics, including gender identity, and any personal experiences of IPV were not systematically collected. While these experiences of the key informants were not systematically collected, many identified themselves as trans and/or IPV survivors during their interviews. Accordingly, the two groups in this study, trans survivors of IPV and key informants who serve this population, are best understood as somewhat overlapping rather than wholly distinct, given that many key informants were motivated to work in the field based on their own lived experiences.
Key Informant Roles (N = 10).
Summary of Qualitative Results
Interviews with participants and key informants revealed complex, intersecting dynamics that influenced HIV/STI prevention engagement among trans individuals experiencing IPV. Table 3 illustrates the four overarching themes that were identified from the data through iterative coding and analytic consensus: (1) partner direct interference with HIV/STI prevention engagement, describing how abusive partners actively restricted access to prevention resources and healthcare; (2) fear of partner reactions interfering with HIV/STI prevention engagement, capturing how anticipated conflict, mistrust, or violence inhibited communication and care-seeking; (3) structural barriers shaping sexual health and safety, reflecting the ways that systemic inequities further influenced HIV/STI engagement; and (4) gaps in services and suggestions for improvement, emphasizing survivors’ and key informants’ calls for trauma-informed, gender-affirming, and peer-led prevention approaches. Together, these themes illustrate how interpersonal violence, structural exclusion, and institutional failures converge to shape trans individuals’ HIV/STI prevention experiences and outcomes. Alongside these barriers, participants’ and key informants’ narratives also surfaced forms of resilience and agency, persistence in accessing prevention through whatever channels available and a consistent emphasis on peer-led, community-based protective resources, which are described at the close of the results.
Themes, Analytic Summaries, and Example Illustrative Quotes.
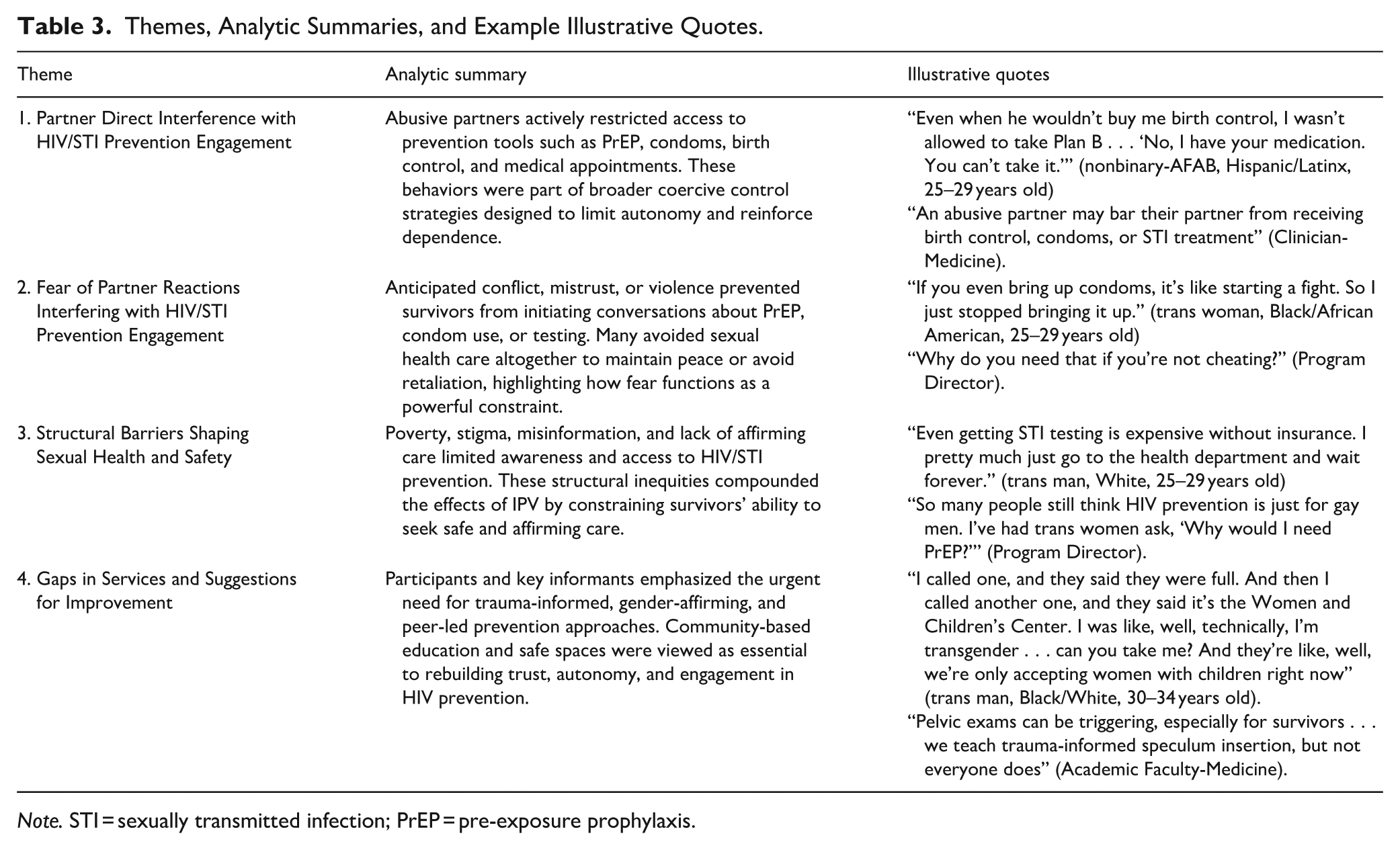
Note. STI = sexually transmitted infection; PrEP = pre-exposure prophylaxis.
Theme 1: Partner Direct Interference with HIV/STI Prevention Engagement
Across participant and key informant accounts, abusive partners were described as actively interfering with HIV/STI prevention efforts as part of broader patterns of control, coercion, and surveillance. This interference often extended beyond isolated incidents, functioning as a deliberate strategy to limit autonomy, manipulate trust, and assert power. Survivors recounted partners restricting access to prevention tools such as PrEP, condoms, and birth control, or preventing attendance at medical appointments. For some, medication was physically withheld or monitored, making it impossible to maintain adherence. As one participant explained, “Even when he wouldn’t buy me birth control, I wasn’t allowed to take Plan B afterward . . . They kept me from taking my PrEP prescription for, like, a week . . . ‘No, I have your medication. You can’t take it’” (nonbinary-AFAB, Hispanic/Latinx, 25–29 years old). Another participant similarly observed that “people in abusive relationships may have those resources not permitted to them” (nonbinary-AFAB, Hispanic/Latinx, 20–24 years old). A key informant similarly stated that “an abusive partner may bar their partner from receiving birth control, condoms, or STI treatment” (Clinician-Medicine).
Several participants described being coerced into condomless sex or experiencing condom refusal framed as a measure of loyalty or trust. In some cases, this coercion escalated to sexual violence or stealthing—the nonconsensual removal of condoms during sex. One participant recounted, “He just took the condom off without telling me. I thought we were having protected sex . . . then boom, we weren’t” (trans man, Black/White, 30–34 years old). Another noted, “He’d say, ‘I don’t like how it feels’ or ‘I’m allergic’ . . . always some excuse” (trans man, White, 25–29 years old). “They definitely want to prevent the use of a condom. They want to prevent you from protecting yourself,” explained one participant (nonbinary-AMAB, Black/White, 20–24 years old). Key informants echoed these experiences, observing how sexual coercion and misinformation were used to control prevention behaviors, “With clients doing sex work, it was condoms with everyone else, but not with the main partner. That was the one who had control” (Program Director).
Collectively, these dynamics reveal how IPV can directly undermine the ability to protect against HIV and other STIs. Control often extended to financial resources, transportation, and communication, making it dangerous to access prevention services. As one key informant described: “He told her she couldn’t go to the doctor. If she even tried, he’d accuse her of cheating. She stopped trying” (Program Supervisor/Manager). A participant also described how this can directly impact the use of PrEP: “Some stalking and controlling is just very sophisticated now . . . even getting PrEP becomes difficult” (trans woman, Middle Eastern/North African, 35–39 years old). As a key informant reflected, “The abusive partner knew all their doctor visits, where they got meds, everything, and used that to control them” (Program Director). These accounts underscore how IPV-related control mechanisms intersect with sexual health behaviors. By controlling access to medical care and prevention tools, abusive partners compromise both the physical and psychological safety of those seeking to protect their sexual health.
These narratives illustrate how IPV operates as a direct barrier to HIV/STI prevention, where control over sexual health behaviors becomes a mechanism of abuse. Interference with PrEP, condoms, and testing reflects both material and psychological domination, undermining autonomy and fostering fear around sexual health decision-making.
Theme 2: Fear of Partner Reactions Interfering with HIV/STI Prevention Engagement
Beyond direct interference, participants and key informants described the pervasive fear of abusive partner reactions, such as anger, accusations, or escalation of violence, as a powerful deterrent to engaging in HIV and STI prevention. Even in the absence of overt control, many survivors avoided conversations about PrEP, condom use, or HIV/STI testing because such topics were perceived as dangerous or destabilizing within abusive relationships. For some, raising issues of prevention immediately triggered suspicion or accusations of infidelity. One participant explained, “There’s people I know that have been accused of cheating because they wanted to get birth control or get tested . . . even using preventive measures” (trans man, White, 20–24 years old).
Participants and key informants emphasized that discussions about HIV prevention often provoked jealousy, suspicion, or accusations of infidelity. Attempts to initiate conversations about condoms or PrEP were described as emotionally charged or dangerous. As one key informant summarized, “People are afraid to say they want to get tested, because that turns into ‘What are you accusing me of?’” (Program Supervisor/Manager). Another key informant noted, “Conversations about PrEP or condoms would trigger jealousy or accusations like, ‘Why do you need that if you’re not cheating?’” (Program Director).
Requests to enact prevention strategies were often interpreted by abusive partners as challenges to trust or loyalty, reframing self-protection as betrayal. As one participant recalled, “Why are you taking PrEP? You don’t trust me?” (nonbinary-AMAB, Hispanic/Latinx, 25–29 years old), while another shared, “You trust me, right? So we don’t need to use protection” (trans man, White, 25–29 years old). Such dynamics forced many survivors into silence, prioritizing safety over sexual health. “If you even bring up condoms, it’s like starting a fight,” explained one participant. “So I just stopped bringing it up. Now I just go along with it, even though it scares me” (trans woman, Black/African American, 25–29 years old).
This pattern extended to HIV/STI testing as well, where even routine screenings were seen as acts of mistrust. “He said if I brought up testing again, he’d leave. So, I didn’t. Even when I was worried,” said one participant (trans man, White, 25–29 years old). A key informant reflected on this phenomenon, noting that “if they imply that getting tested is in conflict with trusting them, then that is going to make it harder for some people” (Program Supervisor/Manager). These interactions demonstrate how IPV can erode the capacity for open communication about sexual health, turning prevention into a relational risk. For some, avoidance became a learned survival strategy: “People are scared to even bring it up . . . they think it’ll cause a fight. So they don’t go [to the doctor],” (trans woman, Hispanic/Latinx, 30–34 years old). Another participant noted, “The doctors always want to test you [for HIV/STIs] when you’re trans. But when you’re in a relationship, you’re not going. You wait until your physical, and by then, it’s too late” (nonbinary-AMAB, Black/White, 20–24 years old).
Key informants echoed how these fears, coupled with stigma and misinformation, inhibit both prevention and disclosure. “They discovered [their partner] was on meds and didn’t disclose, and [they] left. There’s still so much stigma,” explained one key informant (Program Director). Another key informant summarized how fear of being perceived as promiscuous undermines care-seeking with an example of a statement an abusive partner may ask: “Why would your therapist talk to you about PrEP? Are you sleeping around?” (Clinician-Mental Health).
Taken together, these accounts illustrate how fear of partner reactions transforms HIV/STI prevention into a perceived act of defiance. Whereas Theme 1 described explicit control and interference with sexual health, here, the threat of possible emotional or physical retaliation exerts a subtler yet equally constraining form of control. Survivors learned to navigate sexual health decisions by anticipating danger, weighing the potential cost of protection against the risk of provoking abuse.
Theme 3: Structural Barriers Shaping Sexual Health and Safety
Beyond the immediate dynamics of IPV, participants described pervasive structural barriers that compounded risk and shaped the context in which HIV/STI prevention occurred. Across narratives, systemic inequities such as poverty, stigma, and medical mistrust created conditions where prevention tools like PrEP, post-exposure prophylaxis (PEP), antiretroviral therapy (ART), and routine testing were difficult to access even for those actively seeking care. For individuals experiencing IPV, these systemic challenges were intensified by interpersonal control. Survivors described situations in which partner surveillance, lack of transportation, financial dependence, and fear of outing or retaliation made it dangerous or impossible to access care. “There’s all these resources but no way to get to them,” (nonbinary-AMAB, Black/African American, 30–34 years old). “If your partner controls the car, the money, your phone . . . then what?” (nonbinary-AFAB, Native American/Asian, 40–45 years old). Another shared, “Even getting STI testing is expensive without insurance. I pretty much just go to the health department and wait forever” (trans man, White, 25–29 years old).
These barriers were not solely logistical but reflected broader structural exclusion and institutional neglect. Participants emphasized how structural inequities interact with gender- and identity-based stigma to further limit prevention engagement. Several highlighted the absence of affirming, trauma-informed services and prevention messaging that has historically centered cisgender gay men, leaving some feeling excluded or invisible: “Even in advertisements, its cis gay men taking PrEP . . . I feel like that deters [trans] people from knowing it’s even an option for them,” explained one participant (trans woman, Hispanic/Latina, 30–34 years old). A key informant also observed: “So many people still think HIV prevention is just for gay men. I’ve had trans women ask, ‘Why would I need PrEP?’” (Program Director).
Key informants also discussed how financial and institutional barriers intersect with these dynamics. “There’s a distrust of the healthcare system, the lack of financial independence, the inability to take time off work to get labs. . . all of that affects PrEP access,” said one key informant (Clinician-Medicine). Others described restrictive insurance policies and systemic obstacles that reinforce vulnerability: “In some places, if you want Medicaid to pay for your abortion after assault, you have to say you were raped. That’s a huge barrier” (Academic Faculty-Medicine).
These overlapping structural barriers functioned as powerful factors shaping sexual health and safety, amplifying the impact of IPV on HIV vulnerability. Survivors navigating abusive relationships faced a compounded burden: even when motivated to engage in prevention, external systems of inequity limited their ability to do so safely. As one key informant reflected, “PrEP is just catching up with the [trans] community . . . Hopefully we make it popular soon, but it’s not where it’s supposed to be” (Program Director). Together, these narratives from participants and key informants illustrate how structural and informational barriers create an additional layer of disempowerment and limit autonomy for trans individuals navigating IPV and sexual health decisions.
Theme 4: Gaps in Services and Suggestions for Improvement
Participants and key informants underscored a profound lack of trauma-informed, gender-affirming HIV/STI prevention services for trans individuals experiencing IPV. Clinical environments were frequently described as ill-equipped to meet the needs of survivors, with participants citing experiences of misgendering, invasive procedures, and limited awareness of trauma-sensitive practices. As one participant noted, “I avoided going to the doctor for years because . . . it was a nightmare for me as a trans person” (nonbinary-AMAB, Hispanic/Latinx, 25–29 years old). Another shared, “I’m always just like scared of going and then being treated like crap because I’ve had, like, plenty of experiences where it’s like they realize that I’m, you know, biologically female or whatever, and then they’re treating me like I’m like this specimen, which is super weird” (trans man, Hispanic/Latino/White, 25–29 years old). These interactions created conditions where survivors felt unsafe disclosing violence or engaging in sexual health care, often resulting in avoidance or delayed treatment. As one key informant explained, “Pelvic exams can be triggering, especially for survivors . . . we teach trauma-informed speculum insertion, but not everyone does” (Academic Faculty-Medicine).
Participants also described the limited availability of IPV or domestic violence services for trans people. Shelters often refused to accept individuals who were not cisgender women or children. One participant recounted, “I called one, and they said they were full. And then I called another one, and they said it’s the Women and Children’s Center. I was like, well, technically, I’m transgender . . . can you take me? And they’re like, well, we’re only accepting women with children right now” (trans man, Black/White, 30–34 years old). Others emphasized the gaps in knowledge among survivors’ advocacy groups, police, and criminal justice organizations. As one participant stated, “If you work in these kinds of fields . . . you should probably know a little bit more about transgender people” (nonbinary-AFAB, White, 25–29 years old).
Even when trauma-informed or gender-affirming services existed, participants and key informants noted their inconsistent implementation and limited reach. Some highlighted the potential of alternative models such as self-swab STI kits and mail-in PrEP labs. “Those could be game-changers for people experiencing IPV who can’t get to a clinic,” one key informant suggested (Academic Faculty-Medicine). Others noted that IPV screening remains irregular in gender-affirming care settings. “We should be asking everyone about IPV and sexual health, especially in gender care, but it’s not standardized, and we miss things,” a key informant explained (Clinician-Medicine). These gaps leave many survivors navigating fragmented systems that fail to recognize how trauma and gender identity shape access to prevention.
In response, both survivors and key informants emphasized the importance of peer-led, community-based interventions that promote safety, autonomy, and connection. Participants expressed a desire for accessible, affirming information about HIV prevention tools, such as PrEP and PEP, delivered in ways that reflect trans-specific experiences and risks. “We need real sex ed that centers trans bodies and trans risk—not just anatomy or porn myths,” explained one key informant (Program Director). A participant reflected, “I never had the chance to go back and have those conversations about healthy relationships . . . and I wish I had” (trans woman, Black/African American, 21–25 years old).
Peer-delivered education, support groups, and trans-led outreach were consistently described as promising models for overcoming clinical mistrust and avoiding retraumatization. “[There is a need for] comprehensive and wellness services in LGBTQ+ focused environments” (trans woman, White, in their 30s). These spaces create opportunities for shared learning, normalize diverse experiences, and foster healing through community connection. As one key informant observed, “Just having a partner in the room changes what people will say. They won’t disclose violence or sexual health concerns” (Clinician-Medicine), underscoring the need for confidential, survivor-centered alternatives. As one participant suggested, “[We] just need something where we can go . . . We just need information, STD tests, and somebody that talks. Because we all need somebody to talk to sometimes” (nonbinary-AMAB, Black/African American, in their 30s).
Persistence, Agency, and Collective Care in HIV/STI Prevention
Although participants’ accounts centered on the barriers described above, their narratives also revealed forms of resilience and agency exercised in the service of sexual health. Even under conditions of control and structural exclusion, some survivors persisted in seeking prevention through whatever channels remained available to them, such as low-cost public clinics or routine medical visits, rather than forgoing care entirely. Key informants similarly described clients who actively sought protection despite fear and constraint; as one reflected, “I had a patient ask for PEP but wouldn’t say why. After an hour, they disclosed a sexual assault. It took that long to feel safe” (Clinician-Medicine), illustrating both the patient’s agency in seeking prevention and the role of trauma-informed care in enabling disclosure. Participants and key informants also pointed to autonomy-preserving options, such as self-swab STI kits and mail-in PrEP labs, and repeatedly, to the importance of having peer-led, community-based, and trans-affirming spaces as protective resources that could help survivors maintain sexual health more safely. Consistent with the resilience dimension of the GMSR framework, these accounts suggest that collective care and community connection operate as meaningful, if often unmet, protective processes through which trans survivors navigate HIV/STI prevention amid IPV.
Discussion
The current study explored how IPV can shape HIV/STI prevention among trans individuals, a population disproportionately affected by both interpersonal violence and structural inequities in healthcare access. Findings reveal a constellation of relational, structural, and systemic barriers that undermine engagement in prevention behaviors such as PrEP use, condom negotiation, and HIV/STI testing. Across narratives, the impacts of IPV extended beyond physical or emotional harm, functioning as a mechanism through which sexual health autonomy was constrained. Survivors described both partners’ overt interference with prevention behaviors and the internalized fear that even attempting to protect oneself could provoke harm. Institutional failures, such as the lack of trauma-informed, gender-affirming services and limited community-specific education further compounded these relational and contextual barriers. Collectively, the results underscore that HIV prevention cannot be disentangled from safety, autonomy, and access to affirming care, highlighting the urgent need for integrated, community-driven, and trauma-informed approaches that address IPV, structural stigma, and HIV risk as co-occurring and mutually reinforcing conditions, consistent with syndemic theory (Operario & Nemoto, 2010; Poteat et al., 2016; Reisner et al., 2016).
Beyond noting that these findings are consistent with syndemic theory, the framework clarifies why single-issue approaches are likely to fall short. Syndemic theory holds that IPV, structural stigma, and HIV/STI risk are not merely co-occurring but interact and amplify one another, such that the harms of each are magnified by their clustering within contexts of marginalization. Viewed through this lens, partner interference, anticipatory fear, and structural exclusion are not separable problems but interlocking components of a single, mutually reinforcing system. This reframing carries a concrete implication for practice: rather than addressing IPV and HIV/STI prevention through parallel, siloed services, interventions should target the interactions among these conditions, integrating violence support, affirming sexual health care, and structural advocacy, so that progress in one domain is not undone by unaddressed harms in another.
Consistent with previous research linking IPV to reduced PrEP uptake, condom use, and HIV/STI testing among trans persons (Nieto et al., 2021; Ogunbajo et al., 2021; Sevelius et al., 2016; Storholm et al., 2023; 2024; Storholm, Horvath, et al., 2025; Wilson et al., 2015; Zamantakis et al., 2023), our findings demonstrate that for many participants, partner control extended to the deliberate restriction or sabotage of prevention behaviors. These actions reflected broader coercive dynamics in which health, sexuality, and bodily autonomy were weaponized to maintain dominance. At the same time, even when direct interference was absent, fear of a partner’s reactions, ranging from accusations of infidelity to threats of abandonment or violence, often silenced prevention discussions altogether. These findings echo studies showing that emotional and psychological abuse can create environments where self-protection becomes perceived as relational betrayal, reinforcing cycles of risk and control (Camp, 2022; Christensen, 2022). This anticipatory avoidance reflects core mechanisms of gender minority stress, wherein chronic vigilance, fear of rejection, and expectation of harm shape health-related decision-making even in the absence of overt control (Millar, 2025; Rood et al., 2016; Wood, 2024).
Importantly, this study highlights how structural barriers amplify these interpersonal dynamics. Participants’ accounts of limited access to affirming care, lack of active inclusive advertising about PrEP, and systemic exclusion from HIV/STI prevention efforts underscore how structural inequities shape IPV’s impact on health. These findings align with gender minority stress theory, which posits that stigma, discrimination, and institutional erasure generate chronic stress that constrains health-promoting behaviors (Tan et al., 2020; Testa et al., 2015; Turone et al., 2025). While prior HIV prevention interventions have largely targeted cisgender gay men, trans individuals, particularly those experiencing violence, remain underserved. Key informants in this study noted that even when biomedical prevention options were available, stigma, misgendering, and institutional mistrust discouraged engagement. These intersecting forces illustrate that HIV prevention for trans communities cannot be fully achieved without addressing the overlapping social and structural determinants that constrain autonomy and access.
Participants and key informants offered critical insights into how to bridge these gaps. Despite pervasive barriers, participants described strategies for navigating safety, preserving autonomy, and selectively engaging with prevention when trusted resources were available. These accounts reflect gender minority resilience processes, including community connection, peer support, and access to affirming spaces, which can buffer the health impacts of minority stress and violence (Perrin et al., 2020; Puckett et al., 2024; Testa et al., 2015; Turone et al., 2025). The consistent call for trauma-informed, gender-affirming, and community-based care reflects not only unmet needs but also community-driven protective mechanisms rooted in lived experience. Peer-led education, support groups, and outreach programs were viewed as essential for building trust, increasing prevention literacy, and fostering safety. These recommendations align with emerging models of integrated care that center survivor empowerment and recognize IPV as a key barrier to HIV prevention (Cavanaugh & Ward, 2021; El-Bassel et al., 2022; Marshall et al., 2018; Reynolds et al., 2024; Storholm, Nacht, et al., 2025).
Recommendations
At the clinical level, participants emphasized the importance of integrating routine IPV screening and safety planning into gender-affirming healthcare settings, accompanied by staff training on trauma-informed communication and practices (e.g., trauma-informed speculum insertion) and trans-inclusive sexual health counseling. For example, implementing brief, non-stigmatizing IPV screening tools, with a combination of trans-specific and universal IPV items, within primary care and PrEP programs could help identify survivors earlier while ensuring confidentiality. Clinics could also offer flexible service options, such as HIV/STI self-testing, mail-in PrEP labs, or telehealth consultations, to minimize risks for those monitored by abusive partners. Training trans affirming PrEP navigators in trauma-informed IPV response could further facilitate coordinated, survivor-centered care within existing HIV prevention frameworks.
At the social and community level, participants and key informants called for expanding peer-led interventions that normalize conversations about sexual health, IPV, and relationship safety. Programs such as peer navigation and PrEP mentorship, already effective in other trans community contexts (Storholm, Nacht, et al., 2025), can be adapted for trans persons experiencing IPV to promote engagement through trust and shared experience. Community-based organizations could host support groups and drop-in spaces co-facilitated by survivors and trained advocates, offering education on healthy relationships, consent, HIV/STI prevention, legal services, and harm reduction. In parallel, IPV organizations could strengthen their sexual health proficiency and build partnerships with gender-affirming and HIV/STI prevention key informants to more effectively support trans survivors. In addition, mobile outreach programs and collaborations with shelters, legal aid, and housing programs can ensure continuity of care for individuals who are unstably housed or leaving abusive relationships.
At the structural and policy level, participants’ narratives point to the need for broader attention to the systemic factors that shape both IPV and HIV/STI vulnerability among trans individuals. Increasing support for trans-affirming violence and HIV/STI prevention programs, along with expanding provider training on gender diversity and trauma-informed care, may help strengthen existing service systems. Some participants also described the importance of policies that promote safe, confidential reporting options and reduce discrimination in healthcare, housing, and employment. Additionally, efforts to better integrate IPV and HIV/STI considerations within public health and service planning, for example, through improved data collection on gender identity and IPV, could help inform resource allocation and highlight unmet needs.
Developing interventions that combine affirming, trauma-informed clinical practices with community-rooted, peer-driven support and policy advocacy may be particularly effective for reaching trans individuals whose safety concerns, medical mistrust, or lack of access keep them disconnected from traditional healthcare systems. Collectively, these multi-level strategies offer a framework for addressing IPV as both a public health and social justice priority within HIV/STI prevention efforts.
Limitations
This study has several limitations. Participants were recruited through online and community-based methods, which may have favored individuals already connected to networks of care or advocacy, potentially limiting the perspectives of those most isolated by IPV. The sample size and qualitative design do not allow for generalization but instead aim to provide an in-depth understanding of a variety of diverse lived experiences. Additionally, while efforts were made to ensure demographic diversity, findings may not capture the full spectrum of gender identities or regional contexts within trans populations. Finally, interviews were conducted virtually, which may have affected participant comfort or privacy, particularly for those currently living with controlling partners.
Future Research
These findings point to several directions for future research. As the qualitative foundation for the larger RADIANT study, this work has directly informed the Phase II quantitative survey, which can test the prevalence and strength of the associations described here among IPV, anticipated partner reactions, structural barriers, and engagement across the HIV/STI prevention continuum, in a larger, more representative sample. Future studies should also examine these dynamics within specific subgroups that may experience compounded risk, such as Black and Latina trans women, and across differing regional and policy contexts. Building on the resilience and collective-care processes identified here, subsequent research could investigate how peer-led, trans-affirming, and trauma-informed interventions, including low-barrier options such as self-testing and mail-in PrEP, shape prevention engagement among trans survivors of IPV. Finally, longitudinal and intervention research is needed to evaluate integrated models that link IPV support with affirming sexual health services and to identify which components most effectively restore sexual health autonomy over time.
Conclusion
This study contributes to growing evidence that IPV fundamentally shapes HIV and STI prevention engagement through both direct and indirect pathways. Among trans individuals, partner control, fear of retaliation, and structural inequities converge to undermine sexual health autonomy and access to prevention tools. Addressing these multilayered barriers requires more than individual-level interventions, it requires structural change, affirming care, trauma-informed clinical practices, and investment in community-led initiatives that center safety and empowerment. Integrating IPV screening and support within gender-affirming care, expanding peer-led education, and ensuring equitable access to prevention technologies are critical next steps toward reducing HIV vulnerability and promoting holistic well-being for those most impacted by IPV.
Footnotes
Acknowledgements
We would like to express our deep gratitude to the RADIANT Community Advisory Board members including Manav Lund, Pamuela Halliwell, Dionte Gill, Dean Amethyst Dvorak, Ethan Lee, Ramona Natachu, Preslee Thorne, and Chris Washington for their ongoing involvement and thoughtful contributions and careful review of every aspect of the study. Their insights have been essential to ensure that this work remains grounded in community knowledge and priorities. We also extend our heartfelt thanks to the RADIANT study participants, whose willingness to share their personal stories and lived experiences makes this research possible. We recognize that recounting traumatic experiences can be deeply vulnerable and emotionally difficult and we are humbled by the courage and trust shown by each participant. The voices of transgender and nonbinary persons matter, and we are fully committed to honoring these contributions by ensuring that the data shared are used meaningfully and responsibly to advance health equity and support the development of tailored resources for transgender and nonbinary persons.
Author Contributions
Erik D. Storholm: conceptualization, methodology, investigation, resources, writing, review and editing, supervision, funding acquisition.
Ruby Lucas: methodology, survey development, qualitative protocol development, data collection and analysis, review and editing.
Cleo Spencer: Development of recruitment materials, qualitative protocol development, data collection and analysis, review and editing.
Glenn J. Wagner: conceptualization, methodology, review and editing, funding acquisition.
Audren Bambilla: Qualitative protocol development, data collection and analysis, review and editing.
Preslee P. Thorne: Development of recruitment materials, qualitative protocol development, review and editing.
Ayden I. Scheim: methodology, survey development, investigation, review and editing.
Arjee Restar: methodology, survey development, protocol development, investigation, review and editing.
Adedotun Ogunbajo: conceptualization, methodology, investigation, review and editing, funding acquisition.
Keith J. Horvath: conceptualization, methodology, investigation, review and editing, funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: This project was funded by grant R01MH133484 (PI: Storholm) from the National Institute of Mental Health. The content is solely the responsibility of the research team and does not necessarily represent the official views of the National Institute of Mental Health or the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.