Abstract
Cost-utility analyses use the quality-adjusted life-year (QALY) as a measure of health benefit. Normally, they treat every QALY gain equally, that is, attach the same weight (or value) to each QALY gained. However, it appears that this practice does not reflect the distributional preferences of the general public nor of health care professionals. Maximizing the QALY gain from a given budget is not the only aim in priority setting. This article presents a study into such distributional preferences of general practitioners (GPs) for prioritization at the patient level in Hungary. Given the special position GPs have in many health care systems, including the Hungarian, more knowledge of their preferences is important. The authors used a discrete choice experiment to study these preferences, focusing on factors related to the characteristics of the patients, the disease, and treatment effects. Results show that the most important factors influencing the GPs’ decision were the age of the patient, the mortality of the disease, the impact of the disease on patients’ quality of life, and the potential for the full restoration of the previous health status. The treatment of patients without comorbidities was preferred to that of patients with comorbidities. Importantly, these preferences in GPs may steer the actual distribution of health care.
Cost-utility analysis, using Quality-Adjusted Life-Years (QALYs) as the measure of benefit, is often recommended as the appropriate type of economic evaluation in the field of health care. 1 However, the implicit distributional weights attached to QALY gains in the common operationalization of cost-utility analyses, that is, all QALY gains receive equal weight, has aroused quite some debate in the health economic literature. 2 The general public, health care decision makers, and medical professional may not share this value judgment but may rather attach unequal weights to different QALY gains. 3 Commonly, people favor gaining QALYs in the young rather than in the old and in people in a worse health state rather than someone in a better health state. Different values are thus attached to different QALY gains depending on relevant characteristics of beneficiaries (age, socioeconomic status, lifestyle, comorbidity, having dependents) and the disease (prevalence, disease severity, etc.). 4
Such distributional preferences will probably exist among medical professionals as well. This is important in two ways. First, they may be considered an informed group of people to elicit distributional preferences in, as they are relatively knowledgeable. Second, perhaps even more important, if and when these professionals are in the position to influence the distribution of health care, they may do so in a way that is consistent with their own distributional preferences. In that case, it is important to know these (and how they might differ from others’ preferences or other norms).
In this study we opted for general practitioners (GPs) to be interviewed, as GPs may be an especially interesting group in this respect. First, they are familiar with patient-level decision making and have autonomy in their decisions. Second, our research question did not focus on any specific illness, patient group, or therapy. This approach is mostly in line with the practice of GPs who deal with many different types of patients. Also, patients usually are registered with the same GP for a longer period, which allows these GPs to follow them over time and have a more holistic view on their health. Third, due to the governmental regulations of the referrals, GPs have a gatekeeper function in the Hungarian health care system with the possibility to distribute health care.
We therefore set out to investigate the distributional preferences of Hungarian GPs, for a selection of relevant factors, using a discrete choice experiment. To our knowledge, this is the first time this has been done in Hungarian context and it is also a relatively underexplored topic internationally, though similar research has been done, for example, in Finland. 5 This article reports on our study. First we will describe the methodologic issues of this study, the next section will present the results of our model, and then we discuss our findings.
Methods
A discrete choice experiment (DCE) was used to elicit the preferences of GPs for patient level prioritization. DCE is a stated preference technique rooted in the random utility theory 6 and Lancaster’s theory on goods 7 and is increasingly used in health care. 8 A DCE typically describes two options using relevant attributes and levels and asks respondents to choose the option (scenario) they prefer. In choosing, respondents have to consider several attributes simultaneously, which is close to real-world choice situations. The properties of a DCE are described elsewhere. 9
Identifying Attributes and Levels
We identified many factors in the literature that reflect social value judgments in allocating health care resources (e.g., age of the patients, severity of the disease, potential for benefit from the treatment). 10 In order to avoid overburdening the respondents, the number of factors were limited to eight in the DCE. We decided not to include attributes on socioeconomic status and lifestyle factors, although they can be influential in this context. 11 The phrasing of the choice tasks was kept as simple as possible, and concepts were used that GPs were familiar with.
The eight attributes selected in this study are shown in Table 1.
Attributes and Levels
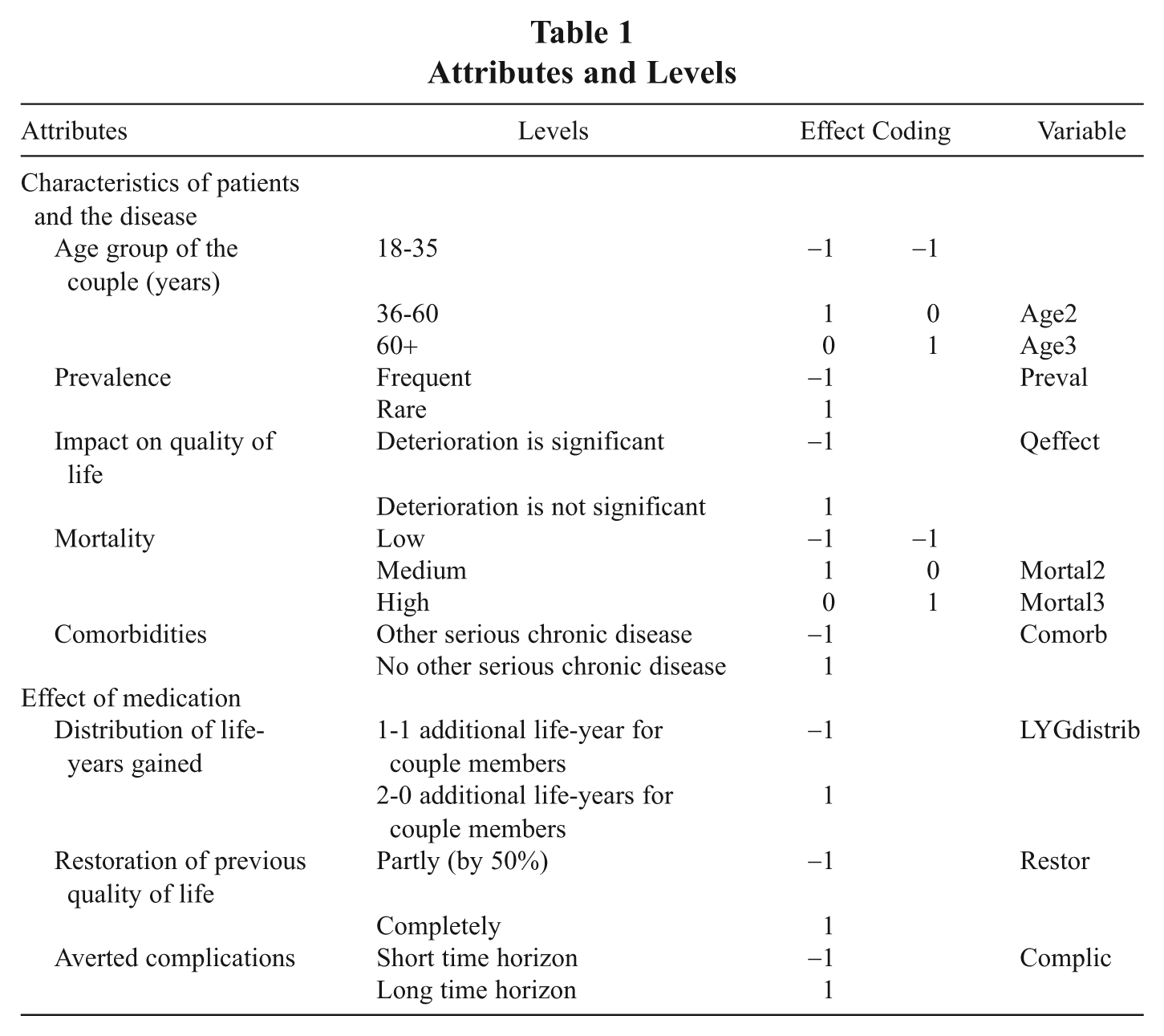
The age of the patients is one of the central concepts, extensively discussed in the literature. 12 The prevalence of the disease may also play a role (e.g., the treatment of rare diseases may be considered relatively more important). 13 Previous studies suggest that priority is normally given to treatment of patients in a worse condition before the treatment. 14 In our study, the severity of the disease was captured by mortality and the impact of the disease on the quality of life. The health status after the treatment is also addressed in previous studies, 15 although the evidence regarding its influence is mixed so far. Also, unsurprisingly, the size of the health gain matters in the allocation of resources. 16 In our study, the existence of comorbidity is to present a difference in the available end status and the potential for restoring previous quality of life is a measure of how much the patient can benefit from the treatment. In the literature, egalitarian tendencies are observed and people do not prefer to give all the health gains to one patient group. 17 We investigated whether the respondents prefer equal distributions of life years gained or not. To frame this in an understandable way, we used scenarios in which the treatment of couples was studied. Respondents were instructed that, except for the attributes on the vignettes, the couples were perfectly identical. Finally, time preference (or sense of urgency) may be of importance in treatment decisions. The final attribute therefore indicated whether the complications caused by the disease would occur after a short period of time or rather a long period of time.
Experimental Design
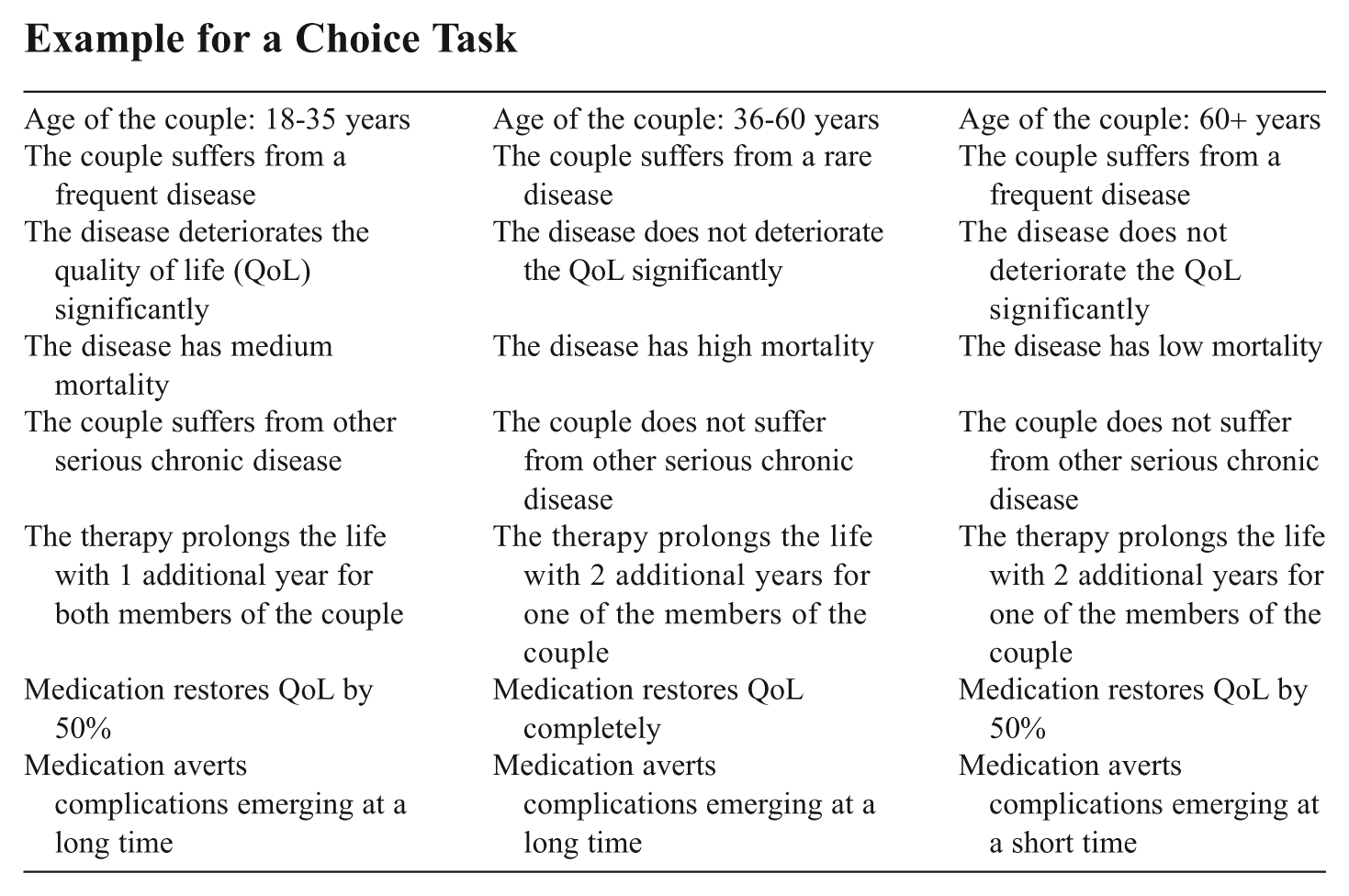
The attributes and levels presented in Table 1 result in 576 possible scenarios (26 × 32). Fractional factorial design was used to reduce the number of presented scenarios. In our paper-and-pencil survey, four versions of the questionnaire were generated with Sawtooth® Software to enhance the number of observed decision making situations. The design of the DCE was constructed in Sawtooth with the balanced overlap method, that is, a random design that keeps track of the co-occurrence of all pairs of attribute levels but allows some degree of overlap. 18 All four versions of the questionnaire consisted of fifteen choice tasks, and each choice task described three concepts (GPs were presented with three options). We did not include an “opt out” option, as complete denial of the treatment was considered to be implausible. An example for a choice task is shown in the appendix.
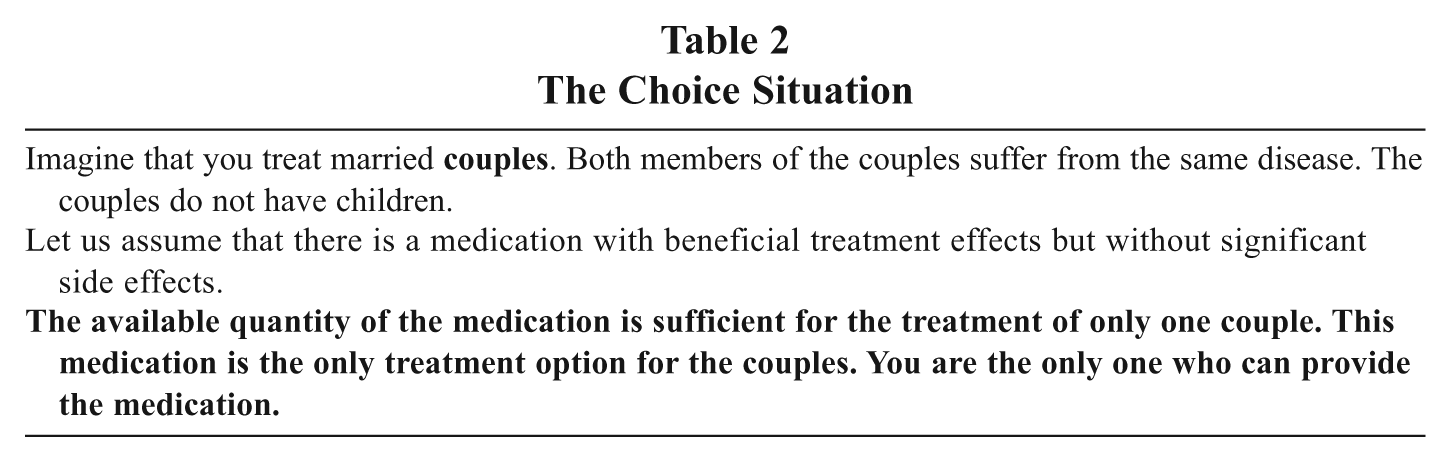
A small pilot survey with three medical doctors was conducted to ensure that interviewees understood the choice situation (Table 2) and were completing the questionnaire as instructed. In the pilot, respondents indicated to have no difficulties with interpreting the choices and attributes; nor did they consider completing the questionnaire particularly burdensome. Changes were made to the introductory text to emphasize that prioritization was forced by insufficient resources and there was no other treatment for the couples. The respondents moreover did not report any difficulties with making choices between couples.
The Choice Situation
Subjects and Data Collection
Hungarian GPs with adult enrollees were randomly sampled from a market research database with stratification by gender and the location of the practice. Subjects were contacted via telephone to ask for their consent to take part in the study. As our research fund was limited, the number of subjects was set to two hundred. GPs received a financial incentive to complete the questionnaire. Questionnaire versions were randomly allocated so that each of the four versions was filled out by fifty respondents. Information was collected on respondent’s gender, the year of graduation (serving as a proxy for the age of the GP), the number of years working as a GP, and the number of enrollees. Face-to-face interviews took place in April and May 2006 with the assistance of skilled interviewers.
Data Analysis
We used a random parameter logit (RPL) or mixed logit model to analyze the data. The mixed logit model incorporates random taste variations and correlations in unobserved factors by allowing the regression coefficients of observed variables to vary randomly over the respondents rather than being fixed. 19 A parameter is considered random if the standard deviation parameter estimate is statistically significant, so taste variation exists. Data were analyzed in NLOGIT 4.0.
Categorical variables were effect coded; that is, the regression coefficients are estimated in a special manner so that the sum of the corresponding category-effects are required to be zero. As a consequence, the estimated category-regression coefficients must be interpreted as compared with the predicted value based on all other predictors in the model rather than with a fixed reference category. We tested for and investigated preference heterogeneity by studying correlation between random parameters. If these were correlated, we used the Cholesky decomposition matrix to decompose the standard deviation into an attribute-specific component and an attribute-interaction component. 20
Internal validity of the DCE was investigated through a priori expectations based on rational behavior that maximizes health benefits. We expected respondents to prefer younger patients, diseases with high mortality and affecting the quality of life significantly, and to treat those patients who can recover fully from the disease and have no comorbidities and the avoidance of complications at a shorter time scale. For the prevalence of the disease and the distribution of life-years gained, had we no a priori expectations.
Tests were carried out to determine if respondents showed dominant preferences, that is, the GP always chose the scenario with the “best” level of an attribute, irrespective of other characteristics. 21 Independent-samples t-tests were calculated to investigate whether respondent groups by questionnaire versions were similar.
Results
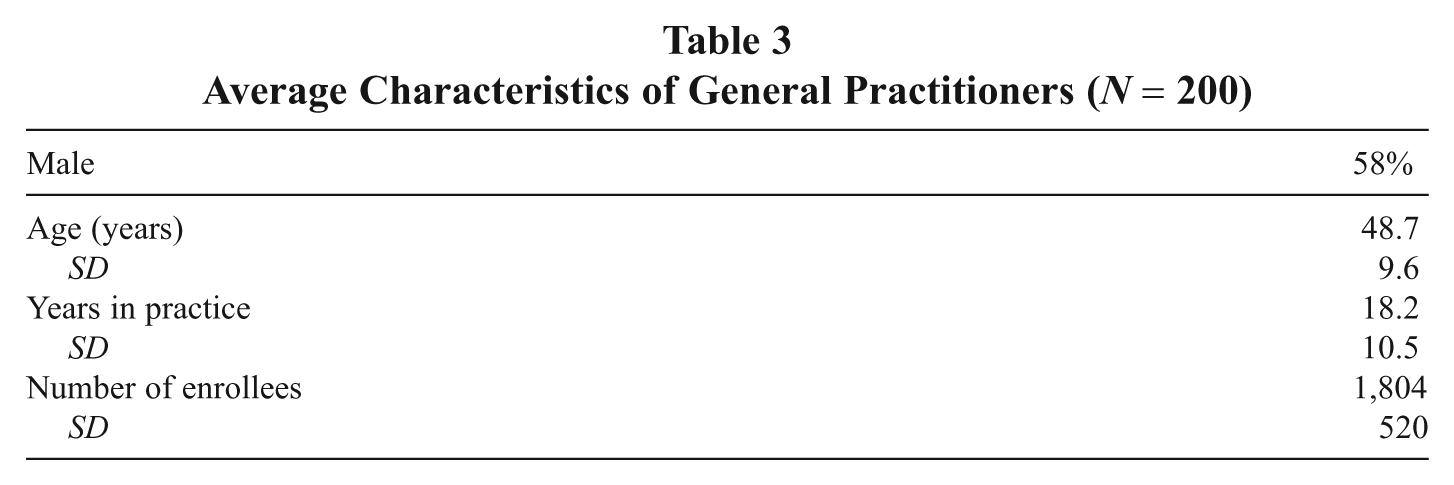
Table 3 gives the background information regarding our respondents. Pair-wise comparisons of respondent groups by the four questionnaire versions showed that the mean age of respondents, years in practice, and the average number of enrollees were similar in these groups. Independent-samples t-tests were insignificant (p-values ranged from .069 to .92). Unsurprisingly, years in practice and the age of the GP showed a Pearson correlation of .78 (p < .01). Due to face-to-face interviews, all the two hundred questionnaires were completed. None of the GPs showed dominant preferences for the youngest age group, for high mortality, to treat the disease that deteriorates quality of life significantly, or for full restoration of previous health status.
Average Characteristics of General Practitioners (N = 200)
A number of models (not presented here) were investigated to identify random parameters and to explore taste variations among our respondents. After testing various possible distributions, the normal distribution of random parameters was chosen. Halton sequences were used in simulations with five hundred replications. Since we found relatively high correlation between our random parameters (i.e., .71, .71, and .50 for Qeffect:Mortal2, Qeffect:Mortal3, and Mortal2:Mortal3, respectively), we investigated the Cholesky decomposition matrix.
The results of the final RPL model is shown in Table 4. The model was statistically significant with a χ2(18) = 848.6 (p = .000). Compared to the standard multinomial logit model (MNL) with twelve parameters, the likelihood ratio test produced a χ2(6) = 30.42 (p = .005). 22 This measure of improvement indicated that the goodness-of-fit of the RPL model was significantly better, and suggested that heterogeneity in GPs’ preferences was an important phenomenon.
Results of the Random Parameter Logit (RPL) Model
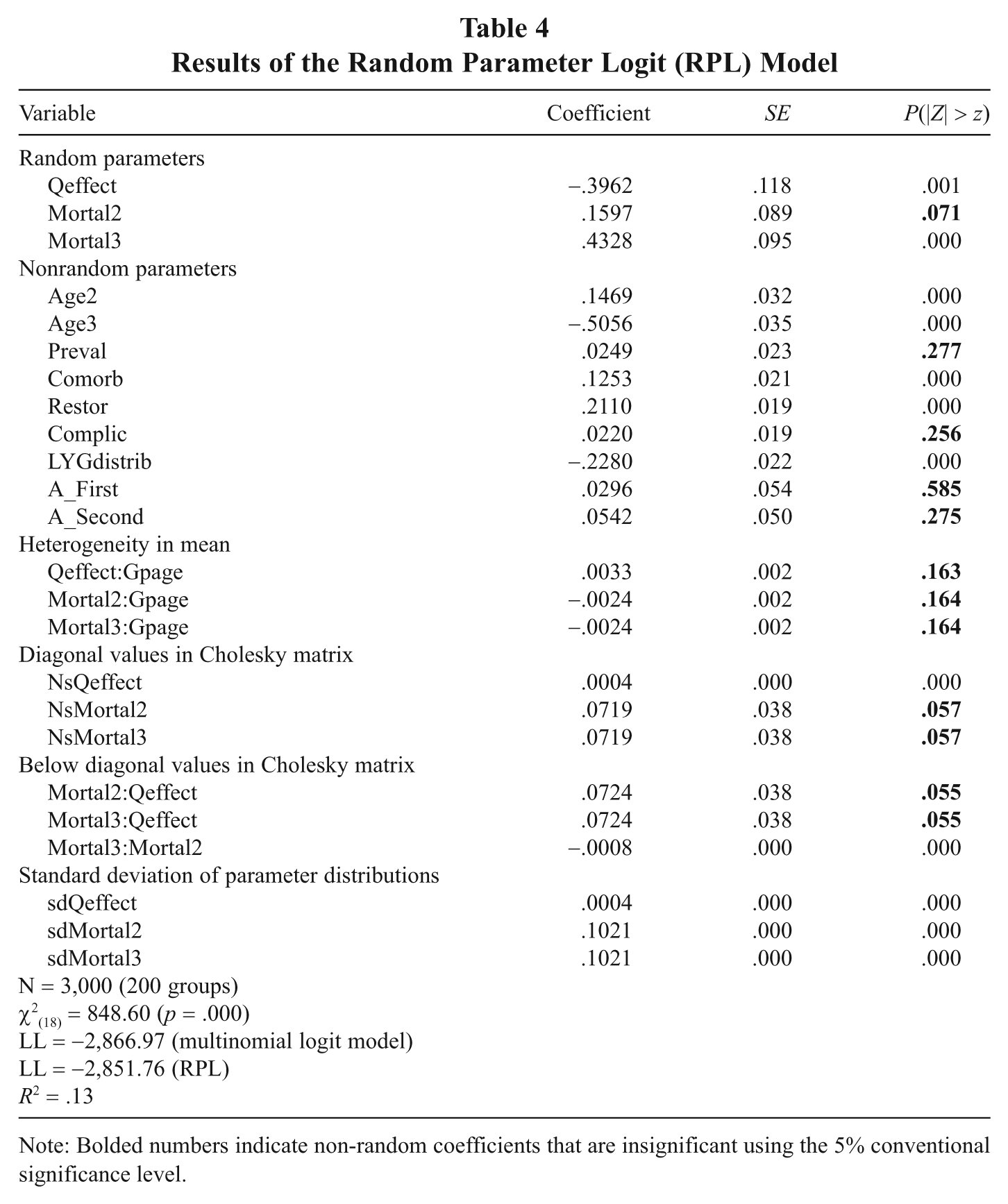
Note: Bolded numbers indicate non-random coefficients that are insignificant using the 5% conventional significance level.
The results show that many of the coefficients were statistically significant at a 5 percent level and had the expected signs. Ceteris paribus and given the levels of the attributes used, GPs preferred to treat the youngest patients and those diseases that affect patients’ quality of life most. Treatment was increasingly preferred when the mortality related to the disease increased. GPs were more likely to prefer treatment of patients without comorbidities and those who had the potential to fully restore their previous health status. They also showed a preference for distributing life-years gained equally between the members of the couple. Neither the prevalence of the disease nor the time horizon of available complications played a significant role in the decisions. The insignificance of the (alternative specific) constants (i.e., A_First and A_Second) indicates that GPs, as would be expected, did not prefer one couple over the other when the differences in attribute (levels) were accounted for. Nevertheless, constant terms were included in the model as a test for specification error. 23
After thorough investigation, we found that two attributes, that is, effect on quality of life and mortality, could not be sufficiently described by single parameter estimates. The mean random parameters of quality of life effect and high mortality were statistically different to zero at a 5 percent level of significance. The attribute-specific standard deviations (diagonal values in Cholesky matrix) were significant at a 5.7 percent level, indicating that GPs’ preferences for quality of life effect and for diseases with high mortality were, indeed, heterogeneous. To determine the potential sources of taste variations among the respondents (e.g., older GPs show less strong preferences for the treatment of diseases with high mortality than younger GPs), it is common to introduce interactions of the random parameter and other variables. All possible interactions with the observed characteristics of the GPs were investigated. (The results with GPs’ age as explanatory variable are shown in Table 4.) Unfortunately, none of these interactions were significant, indicating that the characteristics of the GPs collected in the study were not able to explain the taste variations.
Discussion
We investigated the preferences of Hungarian GPs for a set of criteria that might affect patient level prioritization with a DCE. The direction and the strength of preferences for different attributes (given the specified levels) seem to be plausible, and findings showed that GPs were willing to trade-off these attributes. The importance of these criteria is widely discussed in the literature, although the preferences of health care professionals have been elicited only in few studies.
Ryynänen et al. investigated the prioritization attitudes of doctors and nurses in Finland, using a number of attributes comparable to those in our study. 24 Treatment of children was found to be preferred in that study. Old age in itself was not a reason for lower priority, but treatment of demented and institutionalized patients was less preferred due to comorbidities in old age. In our study only adult patients were included in the scenarios, and we find a preference for treating younger patients. Relative discrimination against the old is controversial also in the literature. These preferences may depend on the characteristics of respondents and cultural issues. 25 In line with international studies, 26 we found no relationship between age of the respondents and preferences for treatment on the basis of age of the patients.
Our finding that respondents preferred treatment of patients with diseases associated with high mortality and those with a negative impact on quality of life is also in line with the study by Ryynänen et al. 27 Moreover, he found that both patients with a poor prognosis and those with a good prognosis did not receive priority in treatment. (While this result may be considered counterintuitive, this need not be the case if respondents understood good prognosis as a situation in which patients will recover without treatment as well, while patients with poor prognosis were considered to be “beyond help” or for whom the health state after treatment would still be poor.) In our study, the improvement in health was explicitly related to medical treatment. Unsurprisingly, GPs preferred to treat people with a higher capacity to benefit from the treatment. The importance of the magnitude of the health gain in our study is in line with previous studies (in the general public). 28
Earlier studies suggest that after-treatment health status has a limited relevance in allocating resources, although it was stressed that eliciting these preferences may be highly sensitive to framing effects. 29 Ubel and colleagues also found that the general public gave equal priority to patients with and without preexisting health conditions that influence the possible after-treatment health status. 30 Our respondents appear to hold other preferences. One of the potential explanations is that we did not ask respondents to choose between patients in life-threatening conditions. The “rule of rescue” might mitigate the importance of factors like after-treatment health. Moreover, subjects from the general public might feel more uncomfortable with making such discriminatory choices than medical professionals. 31 The study by Ryynänen et al. provide some support for this hypothesis, as treatment of patients with comorbidities were less preferred by nurses and doctors in that study as well. 32
The time horizon of avoidable complications was not significant. GPs are likely to consider other attributes more important and did not focus on events that might occur in the future. Also, the interpretation of complications (e.g., severe or not) was left to the respondents, which may be considered a limitation of this study.
Life-years gained were preferred to be distributed equally between the members of the couple, even if the magnitude of the difference was not so remarkable. This sort of egalitarian tendencies are also observed elsewhere, 33 and we assume it to be more prevalent if differences in gains were more significant.
A number of limitations of our study deserve mentioning. First, more attributes than here considered may be relevant in the investigation of social value judgments in the allocation of health care resources. We narrowed the scope of the study to avoid overburdening our respondents, in such a way as to focus on general concepts that were considered to be able to characterize the patient, the disease, and treatment effect in a broad sense. Further research is encouraged to study the role of socioeconomic factors, the lifestyle of the patients, and so forth in prioritization decisions. Also, collecting more background information of respondents (e.g., health state) may contribute to explaining taste variations.
Second, we sought to determine attributes and levels in a way that all the possible combinations correspond to a disease in real life; nevertheless, some of the scenarios were more realistic than others. (For example, a disease with high mortality and low impact on quality of life might seem unrealistic at first sight, but myocardial infarction can be thought of in this case.)
Third, in this study we investigated only the main effects, but the possibility of interaction effects cannot be excluded. Also, the generalizability of our results is limited by the fact that survey of other medical professionals, the general public or of health policy decision makers might lead to different results, and preferences can be determined by country-specific and cultural factors.
Interestingly, our findings suggest that GPs’ choices were reasonably in line with QALY maximization. However, our study was not designed to separate maximizing behavior from other considerations, so we cannot be conclusive in this respect. Still, often, respondents preferred those levels of the attributes that can be considered as the ones that generate more health gain. For example, GPs preferred treating the youngest age group. In general, young people have a larger capacity to benefit because of longer life expectancy. Obviously, it is possible that respondents was considering other age-related aspects as well (e.g., the productivity of the patient or, indeed, a simple distributional preference to treat the young). An exception in this respect is the distribution of life-years gained. Maximizing health gains, one would not make a distinction between how the gains were distributed. Still, GPs clearly preferred to give equal gain for both members of the couple, showing that equality carried additional value for them. A limitation in this context is the fact that this preference for equality may also be induced by broader well-being considerations. For example, prolonging the life of only one member of the couple may be considered to be less valuable (given the grief involved in being the “last living”).
Conclusions
This article is one of the first to study distributional preferences of GPs treating patients, in terms of characteristics of the patients (age, presence of comorbidities) and of the disease (prevalence, mortality, impact on quality of life), as well as the potential effect of available treatments (restoration of quality of life, time horizon of averted complications, distribution of life-years gained between two treated persons). GPs prefer to treat older patients without serious chronic comorbidities, less severe diseases (with low impact on quality of life and low mortality), and disorders for which effective treatments are available. GPs’ characteristics collected in the study, such as age, gender, and years in practice, did not have an effect on the results.
Our results demonstrate that discrete choice experiment is a feasible method to analyze health professionals’ preferences in this context. GPs clearly differentiate according to disease and patient characteristics. Still, it cannot be excluded that their preferences are reasonably in line with QALY maximization. Especially given the important role of GPs in many health care systems, more research in this interesting area, as well as further exploration of preference heterogeneity in GPs, seems warranted.
Footnotes
Appendix
Example for a Choice Task
| Age of the couple: 18-35 years | Age of the couple: 36-60 years | Age of the couple: 60+ years |
| The couple suffers from a frequent disease | The couple suffers from a rare disease | The couple suffers from a frequent disease |
| The disease deteriorates the quality of life (QoL) significantly | The disease does not deteriorate the QoL significantly | The disease does not deteriorate the QoL significantly |
| The disease has medium mortality | The disease has high mortality | The disease has low mortality |
| The couple suffers from other serious chronic disease | The couple does not suffer from other serious chronic disease | The couple does not suffer from other serious chronic disease |
| The therapy prolongs the life with 1 additional year for both members of the couple | The therapy prolongs the life with 2 additional years for one of the members of the couple | The therapy prolongs the life with 2 additional years for one of the members of the couple |
| Medication restores QoL by 50% | Medication restores QoL completely | Medication restores QoL by 50% |
| Medication averts complications emerging at a long time | Medication averts complications emerging at a long time | Medication averts complications emerging at a short time |