
Abstract
HIV phylogenetics is a powerful tool for elucidating HIV transmission dynamics, but ethical concerns have been raised about its use. We conducted a cross-sectional online survey among HIV professional stakeholders in Uganda to explore their knowledge of HIV phylogenetics and associated ethical considerations. Thirty-two participants completed the survey. 87% correctly defined HIV phylogenetics, but some were unable to recognize potential individual harms associated with HIV phylogenetic research (HPR). The most common individual and societal harms of HPR recognized were identification as an HIV transmission source 25 (78%; 95% CI, 61–89%) and marginalization of certain groups 27 (84%; 95% CI, 68–93%), respectively. Most strongly agreed that obtaining community assent 17 (53%; 95% CI, 36–69%) and specific informed consent for viral sequences used in HPR 20 (63%; 95% CI, 45–77%) were critical. Risks associated with HPR appear to be incompletely understood, underscoring the need to raise awareness of them among various professional stakeholders.
HIV phylogenetic analysis is a powerful tool for understanding HIV transmission dynamics and viral evolution. By analyzing viral genetic sequences from individuals living with HIV, it is possible to infer relationships between viral strains, track transmission pathways, and gather critical epidemiological insights. 1 However, HIV phylogenetics involves ethical challenges, particularly when drawing inferences about transmission. 2 Phylogenetic clusters can include individuals linked within a transmission network but are not definitive transmission chains, raising the risk of misinterpreting phylogenetic analysis results, 3 which can lead to individual and societal harms, as well as misguided public health interventions.
We conducted a cross-sectional survey on knowledge and ethical considerations of HIV phylogenetics among professional stakeholders involved in HIV research, prevention, and policy, as well as research ethics in Uganda. An electronic, quantitative survey was administered via Qualtrics between November 2018 and August 2019. Participants were recruited through snowball sampling, utilizing peer referrals. Initial seed participants were actively engaged in ethics and/or HIV research. The instrument comprised 21 items, with survey domains covering basic knowledge of HIV biology and phylogenetics, perceptions of the ethical aspects of HIV phylogenetic research (HPR), and demographic information. Questions related to individual and societal risks were informed by a publication from a multidisciplinary working group examining ethical issues in global HPR. 2 Survey responses were recorded anonymously.
This study was approved by the Johns Hopkins Medicine IRB (IRB00160117) and the Uganda Virus Research Institute Research Ethics Committee (GC/127/18/05/652). After reviewing the study information online, participants provided electronic consent before completing the survey.
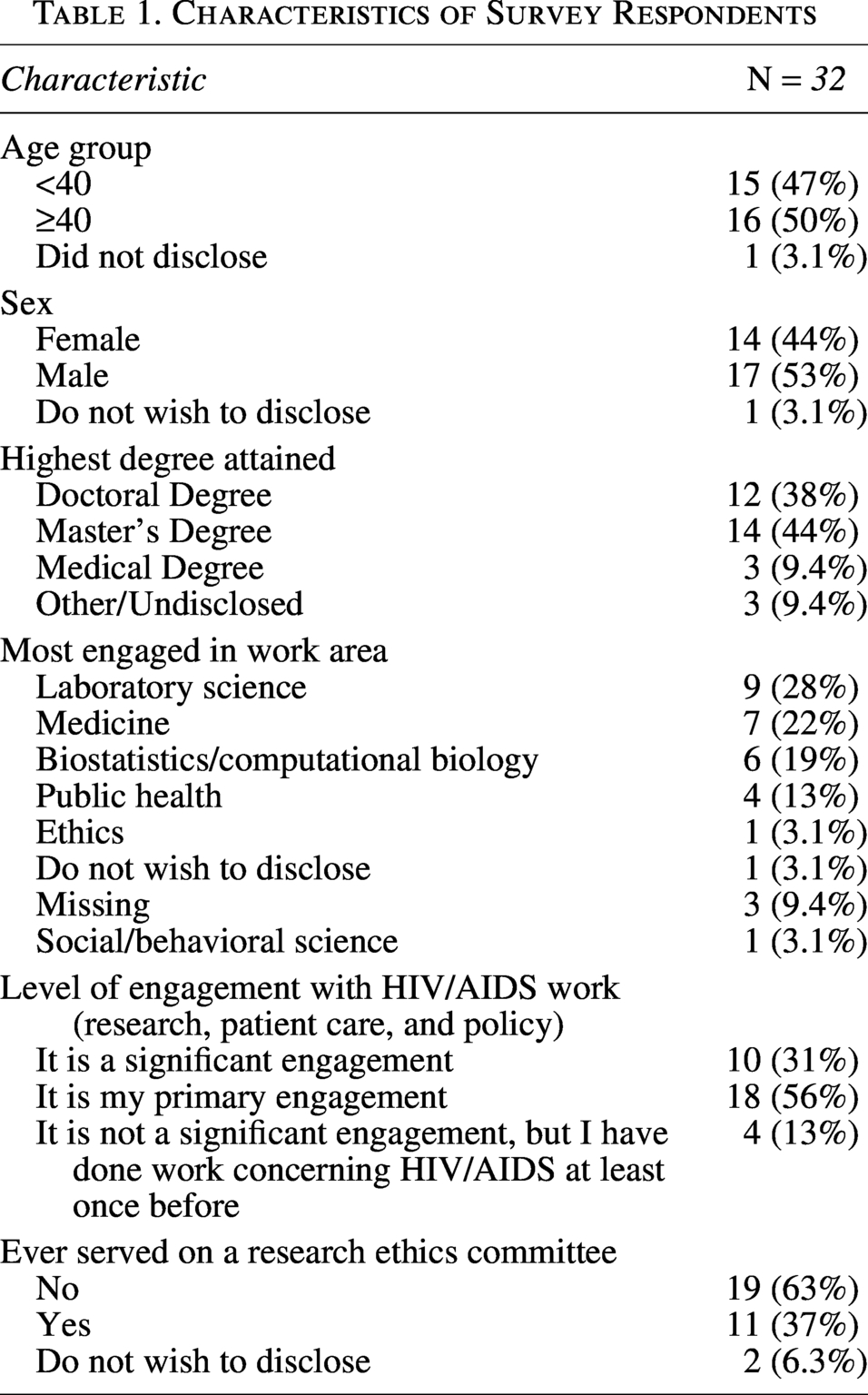
Of the 32 participants included in this analysis, 16 (50%) were 40 years or older (Table 1). Most were male (n = 17, 53%) and highly educated, with only six individuals (19%) not holding either a master’s or doctoral degree. Respondents primarily worked in laboratory science (n = 9, 28%), medicine (n = 7, 22%), biostatistics/computational biology (n = 6, 19%), public health (n = 4, 13%), and one each in ethics and the social and behavioral sciences (n = 2, 6%); the remainder were missing or not disclosed. Overall, 18 participants (56%) reported that HIV/AIDS work was their main professional focus; for 10 (31%), it was significant; and the remainder had previously done such work. Most (n = 19, 63%) had no prior experience on a research ethics committee.
Characteristics of Survey Respondents
While most respondents (87%) correctly identified the definition of HIV phylogenetics (“the study of HIV genomes and their evolutionary patterns”), potential individual-level harms of HPR were less well recognized. The most frequently cited individual harm of HPR (Fig. 1A) was being identified as a source of HIV transmission 25 (78%; 95% CI, 61–89%), closely followed by being linked to a transmission event (the transmission of HIV from one person to another) 23 (72%; 95% CI, 55–84%); being linked to a particular HIV-related risk behavior (e.g., drug use, sexual behavior) 18 (56%; 95% CI, 39–72%); being identified as HIV positive 14 (44%; 95% CI, 28–61%); and incarceration 11 (34%; 95% CI, 20–52%). A minority either reported no potential harms 1 (3%; 95% CI, 1–16%) or did not know 2 (6%; 95% CI, 2–20%).
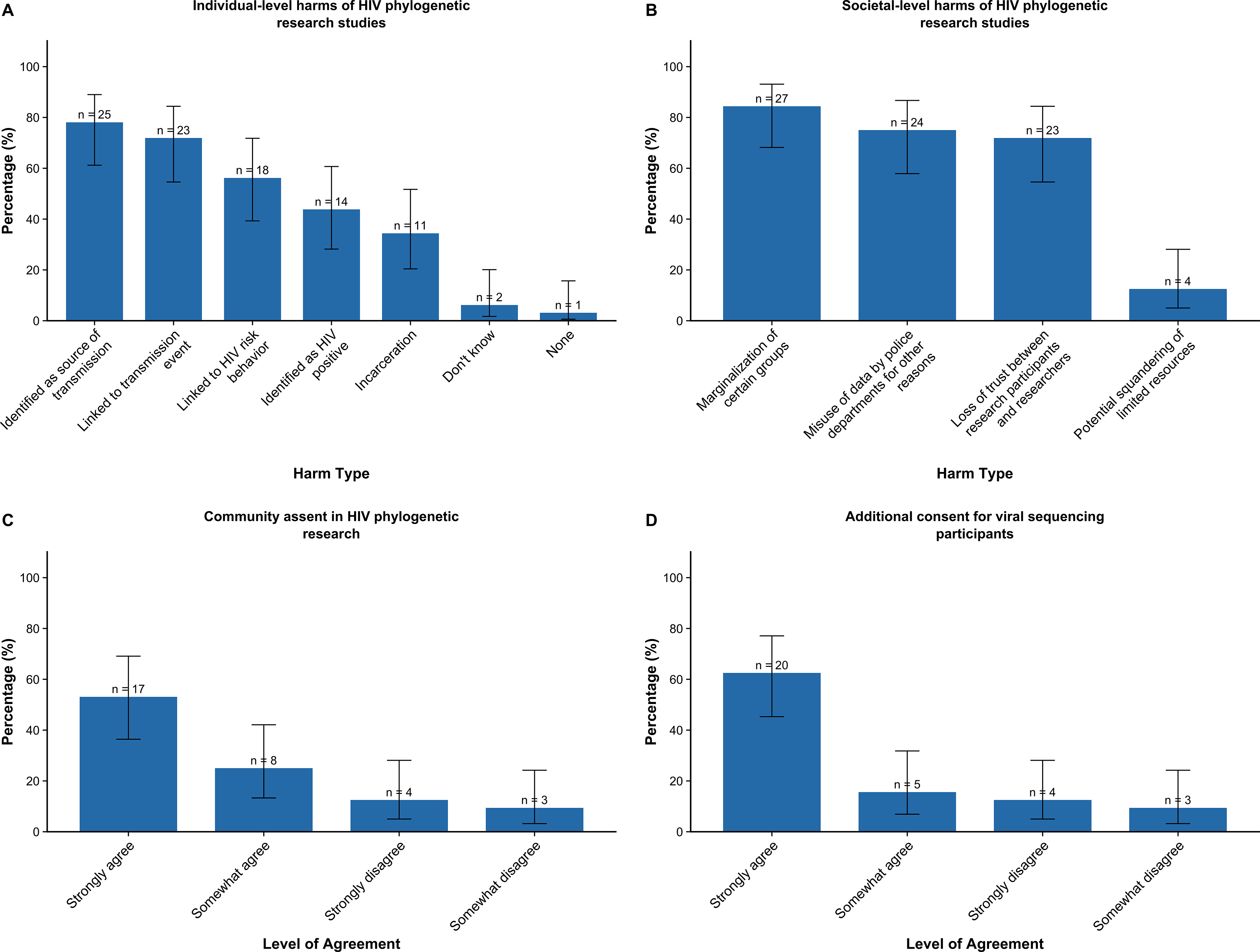
Figure 1 includes participants’ perceptions on
The most frequently selected societal level harm (Fig. 1B) was marginalization of certain groups 27 (84%; 95% CI, 68–93%), followed by misuse of data by police departments for other reasons 24 (75%; 95% CI, 58–87%), and loss of trust between research participants and researchers 23 (72%; 95% CI, 55–84%). The potential squandering of limited resources was cited by the fewest number of respondents 4 (13%; 95% CI, 5–28%).
Participants were asked to what extent they agreed with the statement: “Community assent is necessary prior to beginning HIV phylogenetic studies” (Fig. 1C). Most agreed, specifically: Strongly agree 17 (53%; 95% CI, 36–69%); Somewhat agree 8 (25%; 95% CI, 13–42%); Somewhat disagree 3 (9%; 95% CI, 3–24%); and, Strongly disagree 4 (13%; 95% CI, 5–28%).
We also asked participants to evaluate the extent to which they agreed with the statement that individuals whose viral sequences would be used in phylogenetic studies should undergo an additional informed consent process (i.e., a separate consent procedure for participants in a clinical trial for inclusion in a phylogenetics sub-study). Most agreed, specifically (Fig. 1D): Strongly agree 20 (63%; 95% CI, 45–77%); Somewhat agree 5 (16%; 95% CI, 7–32%); and Somewhat disagree 3 (9%; 95% CI, 3–24%).
Overall, most participants perceived at least one individual-level and one societal-level harm stemming from HPR. Concerns included privacy and confidentiality, stigma related to certain behaviors, potential legal consequences, data misuse, and loss of trust. A nontrivial minority (9%) reported uncertainty or the absence of perceived individual harms, underscoring heterogeneity in risk perceptions among this educated sample that was mostly engaged in HIV/AIDS-related work. Nevertheless, 91% recognized that HPR could expose individuals to harm—for example, by identifying someone as a potential source of HIV infection, linking them to a marginalized group, or enabling misuse of data by police. Consistent with these concerns, 78% supported obtaining both community assent (a community’s informed collective agreement to participate in or permit research) and additional individual consent for HPR.
Potential societal-level harms posed by HIV phylogenetic studies have been raised, including criminalization and marginalization of specific population sub-groups.4–6 However, these risks must be carefully weighed against the benefits, including deeper epidemiological insights that can inform more effective public health interventions. Currently, there is no established framework for understanding the scope of benefits from molecular epidemiology, which complicates such evaluations.
Despite increasing recognition of the value of obtaining community assent in genomic research, both its role and the processes for obtaining it remain underdeveloped. 7 Similarly, despite the importance of consent,8,9 evidence remains limited regarding whether specific individual consent processes meaningfully improve participants’ understanding of the risks entailed in using HIV genomic data for research in African contexts.
Our study was limited by sample size and only surveying one country. This limits the generalizability of our findings. It may also overestimate risk knowledge, since the survey participants were provided a list of particular risks that are not typically available during actual protocol reviews.
Furthermore, as a study focused on professionals, the survey did not elicit the perspectives of other key stakeholder groups—community representatives, advocacy groups, people living with HIV, and beneficiaries of HIV services. Without these voices, the study’s findings may not fully reflect community-specific concerns, and interpretations of risk, acceptability, and appropriate safeguards for HPR may be incomplete or skewed toward professional rather than lived experiences of those most affected by HPR. The survey was conducted before the enactment of the Anti-Homosexuality Act in Uganda and the COVID-19 pandemic; stakeholders’ perceptions may have shifted following these events.
At the time of data collection, scholarship on the ethics of HIV phylogenetics—particularly empirical evidence of actual harms—was extremely limited, making it impossible to assess the reality of respondents’ perceived risks. Nevertheless, as background, in Uganda, intentional and attempted transmission of HIV is criminalized with penalties including fines and imprisonment up to 10 years through the HIV and AIDS Prevention and Control Act of 2014. 10 However, in this survey, participants were not asked about their awareness of HIV-specific laws in Uganda or the legal implications of HPR. This gap highlights an area for future research.
Despite the study’s limitations, our findings have important implications for practice, education, and future research. There is a clear need for education about HPR as well as rigorous ethical safeguards, transparency, and participant-centered approaches in the design, conduct, and regulation of HPR in the region. Educational modules on the ethics of HPR could be designed and tailored for different stakeholders, including researchers, regulators, and members of institutional review boards and community advisory boards. It is unclear how research ethics guidelines and researchers are currently addressing the potential risks of HPR and whether these measures are sufficient to mitigate them. A regional study on current practices for HPR could help address such uncertainties.
As the body of evidence in this area grows, future research could systematically assess how perceived risks of HPR studies align with real-world experiences to strengthen the empirical basis for ethical guidance. Others could explore whether—and in what ways—community assent and robust individual consent procedures might help protect individuals and communities from the potential risks associated with HPR. Furthermore, it will be important to understand participants’ preferences regarding the amount and type of information they find useful during HPR consent, as lengthy or complex consent processes may create unwarranted research burdens.
Further research is also needed to understand how different settings—such as variations in ethical and legal frameworks, HIV epidemiology, community norms, and public health infrastructure—shape both the actual risks of HPR and stakeholders’ perceptions of those risks. Comparative or multi-site studies could also clarify how such contextual factors influence the feasibility and effectiveness of potential risk-mitigation strategies, including consent processes and community engagement approaches. Such data promise to facilitate the protection of individuals and communities included in the HPR.
Footnotes
Author Disclosure Statement
J.S. is a consultant to Merck KGaA, Merck, Moderna, Thermo Fisher, and Fujifilm; and was previously a member of Aspen Neurosciences Clinical Advisory Committee. None of these activities are related to the work described in this article. No other authors have provided disclosures.
Funding Information
This research was supported in part by the Intramural Research Program of the