
Abstract
Purpose:
Studies have examined the independent and additive effects of health behaviors (e.g., physical activity, diet, sleep, and smoking) on systemic inflammation, but we know little about whether different pairs of these behaviors differentially influence inflammation, which was the purpose of this study.
Design:
Cross-sectional.
Setting:
The National Health and Nutrition Examination Survey (NHANES) 2005–2006.
Subjects:
A total of 2051 adults (≥20 years).
Measures:
A questionnaire/interview was used to assess sleep and dietary behavior; physical activity was assessed via accelerometry; smoking was assessed via cotinine levels; and a blood sample was taken to assess systemic inflammation (C-reactive protein; [CRP]).
Analysis:
Multivariable linear regression analysis.
Results:
Six health behavior pairs were evaluated: (1) active and healthy diet, (2) active and adequate sleep, (3) active and nonsmoker, (4) healthy diet and adequate sleep, (5) healthy diet and nonsmoker, and (6) adequate sleep and nonsmoker. After adjusting for age, gender, race-ethnicity, poverty level, and chronic disease, only active and nonsmoker (β = −.15) and healthy diet and adequate sleep (β = −.16) were associated with CRP.
Conclusion:
Regular physical activity and smoking avoidance and healthy eating and adequate sleep were the two health behavior pairs associated with less inflammation. This suggests that certain health behaviors may act synergistically on reducing systemic inflammation, whereas other health behavior combinations may not. Such knowledge may help to develop and implement tailored health behavior interventions.
Purpose
Health behaviors, including physical activity, 1 healthy eating, 2 adequate sleep, 3 and smoking avoidance, 4 are all independently associated with reduced systemic inflammation. Although less investigated, research also demonstrates an additive effect of these health behaviors on health, 5 in that those adopting more health behaviors tend to have better overall health than those adopting fewer health behaviors. However, we know less about the specific effects of different health behavior combinations on inflammation. Here, using cross-sectional data from the National Health and Nutrition Examination Survey (NHANES), six health behavior dyads (all possible dyad combinations) were evaluated: (1) active and healthy diet, (2) active and adequate sleep, (3) active and nonsmoker, (4) healthy diet and adequate sleep, (5) healthy diet and nonsmoker, and (6) adequate sleep and nonsmoker. Specific attention to health behavior dyads may be of particular importance from a health promotion standpoint as it may be much more realistic for unhealthy individuals to adopt two health behaviors as compared to simultaneous adoption of all health behaviors. For example, Reeves and Rafferty 6 used self-reported data from the Behavioral Risk Factor Surveillance System and reported that, for four health behaviors, only 3% of the population engaged in all health behaviors, with little variation among demographic-related (e.g., age, gender, race-ethnicity) subgroups (0.8%–5.7%). Further, several intervention studies have been ineffective in changing several health behaviors concurrently. 7 –9
The specific purpose of this applied research brief was to examine the association of these six health behavior dyads on systemic inflammation in a national sample of U.S. adults. Specific attention is focused on C-reactive protein (CRP) as the outcome of interest, as elevated CRP concentration is indicative of increased systemic inflammation, with increased systemic inflammation facilitating the development and progression of diabetes, 10 cardiovascular disease, 11 chronic kidney disease, 12 and various mental health disorders. 13
Methods
Design and Participants
Data from the present study were extracted from the 2005–2006 NHANES (only cycle with available data on all study variables), an ongoing survey conducted by the Centers for Disease Control and Prevention that uses a representative sample of noninstitutionalized U.S. civilians, selected by a complex, multistage, stratified, clustered probability design. The 2005–2006 NHANES study procedures were approved by the National Center for Health Statistics Ethics Review Board. Consent was obtained from all participants before any data collection. A total of 2051 participants provided data on the study variables.
Measurement of High-Sensitivity CRP Concentration
High-sensitivity CRP concentration was quantified by using latex-enhanced nephelometry. The coefficients of variation by lot ranged from 3.1% to 9.9%. Further details about the laboratory procedures and quality control are available elsewhere. 14
Health Behaviors
The six evaluated health behavior pairs are noted in the “Purpose” section. Physical activity was assessed by using an ActiGraph 7164 accelerometer (Pensacola, Florida) for 7 days, with only those providing at least 4 days of 10+ hours/day of monitoring included in the present study. Detailed information on the ActiGraph accelerometer and the protocol implemented in NHANES can be found elsewhere. 15 Participants were defined as active (≥150 min/wk of moderate to vigorous physical activity [MVPA]) or not active, with activity counts per minute ≥ 2020 defined as MVPA.
Using the average of the 2-day interview–determined health eating index (HEI) scores, participants at or above the 60th percentile of HEI scores in the population were categorized as adhering to the dietary guidelines or consuming a healthy diet. 2 The HEI was derived for each of the 24-hour recall days by using the MyPyramid Equivalents Database and following the methods and SAS code established by the U.S. Department of Agriculture Center for Nutrition Policy and Promotion. 16
Serum cotinine levels > 1.78 ng/mL for men and > 4.47 ng/mL for women were assessed to differentiate smokers from nonsmokers. 17
Adequate sleep was defined as 7 to 8 self-reported hours/night of sleep 18 ; otherwise, inadequate sleep.
Demographics/Covariates
Covariates included age, gender, race-ethnicity, poverty-to-income ratio, and comorbidity index. A comorbidity index variable (range of having 0–12 chronic diseases) was created from the physician diagnosis of the following chronic diseases/events: arthritis, asthma, chronic bronchitis, cancer, congestive heart failure, coronary artery disease, diabetes, emphysema, liver disease, stroke, hypertension, and overweight/obesity. Notably, hypertension was not self-reported but determined from measured blood pressure (≥140/90 mm Hg). Similarly, over-weight/obese was defined as >20% body fat for men and >30% body fat for women. 19 Total body fat percentage was estimated from whole-body dualenergy x-ray absorptiometry scans by using the Hologic QDR 4500A fan beam x-ray bone densitometer (Bedford, Massachusetts).
Analysis
All analyses accounted for the complex survey design used by NHANES when using Stata (v.12; StataCorp LP, College Station, Texas). Multivariable linear regression analyses were used to examine the association between the health behavior dyads and CRP (outcome variable). Significance was set at p < .05.
Results
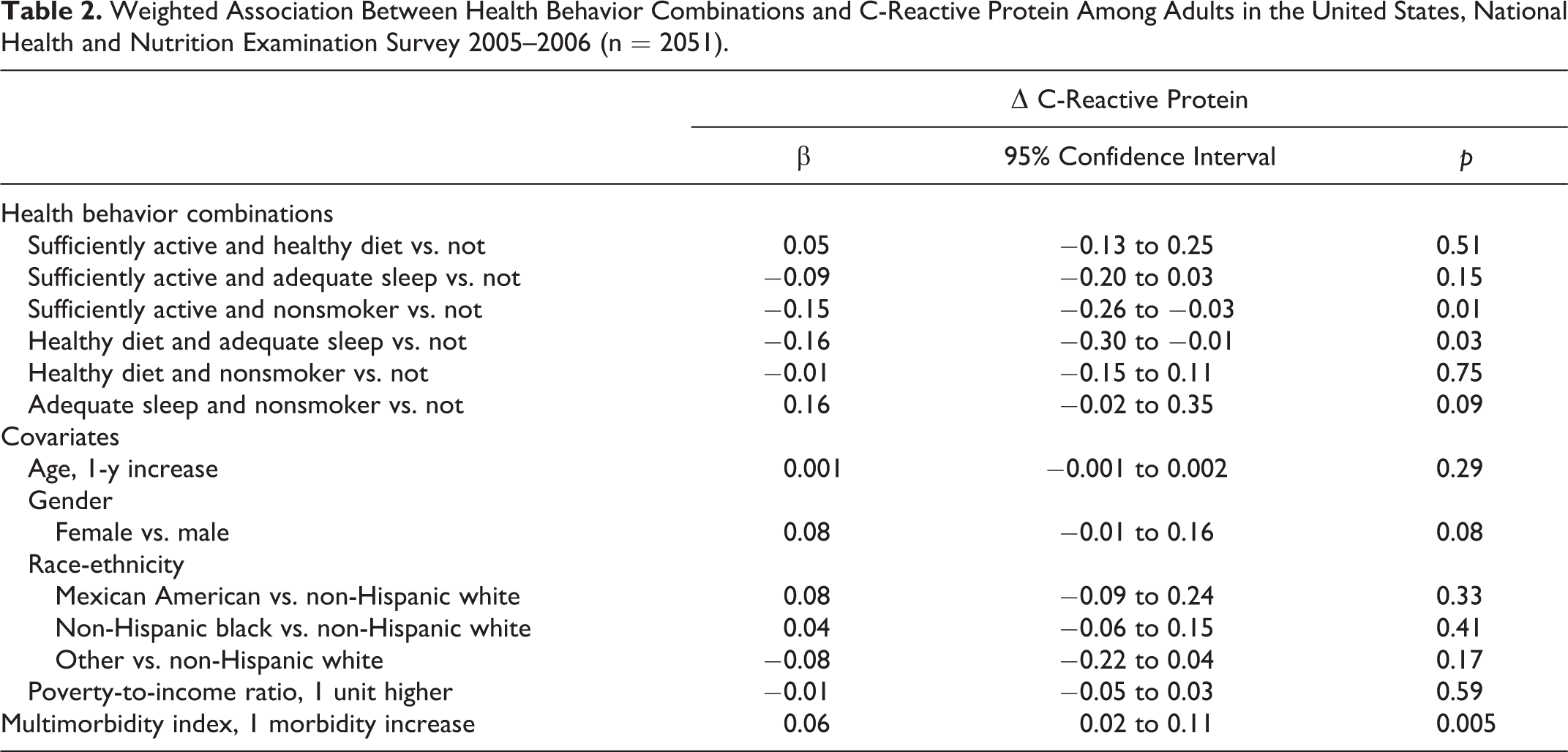
Table 1 reports the weighted characteristics of the analyzed sample. Six multivariable regression analyses were computed: one for each health behavior dyad along with covariates in each model. With the exception of those engaging in adequate sleep and not smoking (β = .01, p = .78), all other combinations (not shown in tabular format) were individually associated with CRP: active and healthy diet (β = −.14, p = .001); active and adequate sleep (β = −.12, p = .02); active and nonsmoker (β = −.14, p = .005); healthy diet and adequate sleep (β = −.11, p = .01); and healthy diet and nonsmoker (β = −.08, p = .01). Table 2 shows the results when each of these health behavior dyads was included in the same model. In this model, only active and nonsmoker (β = −.15) and healthy diet and adequate sleep (β = −.16) were associated with CRP (Table 2). In this model, there was no evidence of multicollinearity; the mean variance inflation factor was 1.7, the highest individual variance inflation factor was 2.5, and all tolerance statistics were >0.38.
Weighted Characteristics of the Analyzed Sample, National Health and Nutrition Examination Survey 2005–2006 (n = 2051).
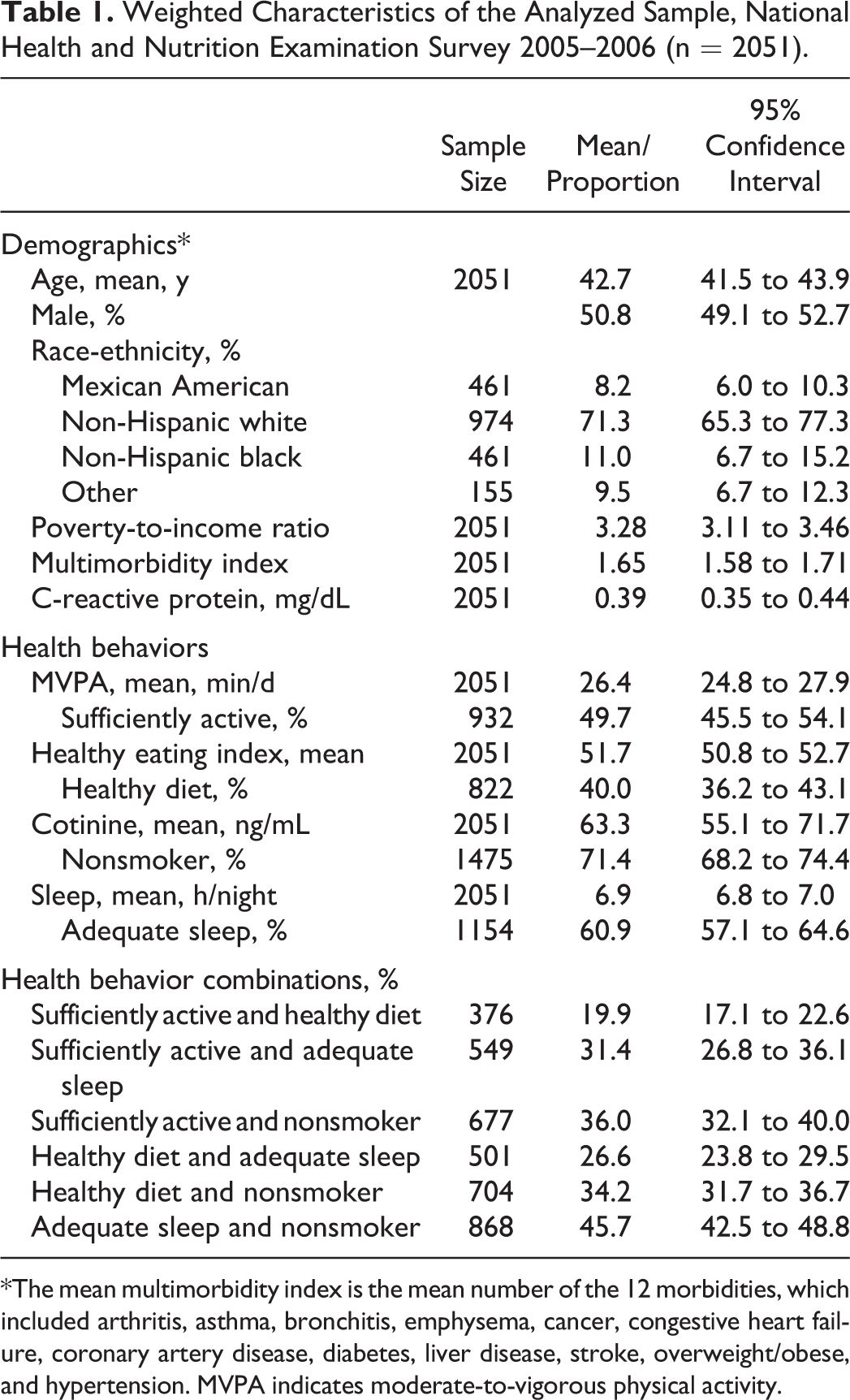
*The mean multimorbidity index is the mean number of the 12 morbidities, which included arthritis, asthma, bronchitis, emphysema, cancer, congestive heart failure, coronary artery disease, diabetes, liver disease, stroke, overweight/obese, and hypertension. MVPA indicates moderate-to-vigorous physical activity.
Weighted Association Between Health Behavior Combinations and C-Reactive Protein Among Adults in the United States, National Health and Nutrition Examination Survey 2005–2006 (n = 2051).
Discussion
Summary
Among the six health behavior combinations evaluated, only two were independently associated with CRP: active and nonsmoker and healthy diet and adequate sleep.
Limitations
Limitations of this study include the cross-sectional design, with the observed results noting statistical significant differences with little variation in the strength of the relationships. Further, sleep duration was subjectively determined as opposed to an objective assessment of sleep (e.g., polysomnographic assessment).
Significance
The differential association of health behavior combinations on inflammation suggests that some health behaviors may work synergistically to reduce inflammation. Identification of potential synergistic behaviors may provide informative information to health practitioners aiming to develop and implement tailored health behavior interventions.
SO WHAT? Implications for Health Promotion Practitioners and Researchers
What is already known on this topic?
Physical activity, diet, smoking, and sleep are independently and additively associated with inflammation. Elevated systemic inflammation (as determined here by elevated CRP levels) is of major concern, as it may facilitate the development and progression of various chronic diseases, including diabetes and cardiovascular disease.
What does this article add?
This cross-sectional analysis demonstrates different statistically significant combinations of health behaviors with systemic inflammation.
What are the implications for health promotion practice or research?
If confirmed by future prospective and experimental work, practitioners may wish to selectively promote health behaviors on the basis of their combined effect on inflammation. Further, research examining the potential independent or shared mechanisms of the dual health behaviors on inflammation is warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.