
Abstract
Purpose:
The aim of the present study was to examine the influence of a supervised and regular program of aquatic activities throughout gestation on maternal weight gain and birth weight.
Design:
A randomized clinical trial.
Setting:
Instituto de Obstetricia, Ginecología y Fertilidad Ghisoni (Buenos Aires, Argentina).
Participants:
One hundred eleven pregnant women were analyzed (31.6 ± 3.8 years). All women had uncomplicated and singleton pregnancies; 49 were allocated to the exercise group (EG) and 62 to the control group (CG).
Intervention:
The intervention program consisted of 3 weekly sessions of aerobic and resistance aquatic activities from weeks 10 to 12 until weeks 38 to 39 of gestation.
Measures:
Maternal weight gain, birth weight, and other maternal and fetal outcomes were obtained by hospital records.
Analysis:
Student unpaired t test and χ2 test were used; P values ≤.05 indicated statistical significance. Cohen’s d was used to determinate the effect size.
Results:
There was a higher percentage of women with excessive maternal weight gain in the CG (45.2%; n = 28) than in the EG (24.5%; n = 12; odds ratio = 0.39; 95% confidence interval: 0.17-0.89; P = .02). Birth weight and other pregnancy outcomes showed no differences between groups.
Conclusion:
Three weekly sessions of water activities throughout pregnancy prevents excessive maternal weight gain and preserves birth weight.
Trial Registration:
The clinicaltrial.gov identifier: NCT 02602106.
A sedentary lifestyle and poor eating habits have been linked to metabolic, cardiovascular, and psychological diseases. 1 These diseases are suggested comorbidities to obesity with increasing prevalence in childhood. 2 -4 Physical exercise may stop the rising trend of childhood obesity and its comorbidities. 5
Developmental Origins of Health and Disease starts during pregnancy, and an adverse intrauterine environment could be a precursor for the development of future complications later in life. 6 Pregnancy modifies all systems in order to ensure adequate fetal growth and development creating constant adjustments and adaptations to the woman throughout gestation. 7 One of the most important adaptations from a metabolic point of view is the increasing insulin resistance that may progress to gestational diabetes mainly due to an inadequate diet and lack of physical exercise. 8,9 The scientific literature provides positive benefits for moderate and regular exercise during pregnancy to improve maternal and fetal well-being. 10
Over the past 20 years, the influence of exercise on maternal and fetal outcomes has been studied with interesting results. Exercise has been shown to have a positive influence on the process of pregnancy and childbirth. 11 -13 Maternal weight gain and birth weight have been examined by researchers in recent studies that report many beneficial effects of moderate exercise during pregnancy. 5,14,15 Prevention of excessive gestational weight gain and appropriate birth weight is a proxy for a healthy fetal environment. 10 Babies born large (macrosomic >4000 g) or small (<2500 g) are at risk for obesity and chronic disease later in life. 6
Many forms of exercise modalities are presented in intervention studies with a wide variety of designs and variations. Although most studies are based on land exercises, some studies have used a “swimming” intervention, 16,17 “aquatic activities” or “water aerobics,” 18 -24 and an “immersion” exercise session. 25 -27 Kamioka et al 28 reviewed the effects of aquatic exercise and concluded that there is insufficient evidence to report benefits for aquatic exercise due to poor methodological and reporting quality and heterogeneity of nonrandomized clinical trials.
The aquatic environment generates many alternatives that are usually not available to pregnant women using land-based exercise. Women participating in an aquatic exercise program report significantly less physical discomfort, improved mobility, and improved body image and health-promoting behaviors. 21 Buoyancy creates a feeling of physical comfort, improves mobility and postural balance, and facilitates the use of different muscle groups, which, in turn, decreases postexercise pain. 29 Therefore, there are several advantages to water exercise, particularly in pregnancy. 30
We believe that new studies are necessary and alternative forms of exercise using the aquatic environment during pregnancy are needed to promote healthy pregnancies. Indeed to better understand whether regular and supervised aquatic exercise can be used to promote maternal and fetal well-being is of clinical relevance and of public health interest.
The aim of the present study was to examine the influence of a supervised and regular program of aquatic activities throughout gestation on maternal weight gain and birth weight. We hypothesized that excessive maternal weight gain would be prevented, with more babies born with adequate weight in the intervention group compared to the control women.
Materials and Methods
Design
The present randomized clinical trial (RCT Registration: NCT02602106) was conducted between March 2013 and May 2015 following the ethical guidelines of the Declaration of Helsinki, last modified in 2000. The research protocol was reviewed and approved by the ethical committee of Universidad de Flores, and all women gave written informed consent.
Sample
We contacted a total of 184 pregnant women from a primary care obstetric medical center (Instituto de Obstetricia, Ginecología y Fertilidad Ghisoni, Buenos Aires, Argentina; Figure 1). The study participants were recruited by nurses during the first prenatal visit. Women were included if they had singleton and uncomplicated pregnancies. For practical reasons, women not planning to give birth in the same obstetric center and not under medical follow-up throughout the entire pregnancy period were not included in the study. In addition, women were not included if they had medical conditions that prevented them from exercising safely 31 such as:
heart disease,
thrombophlebitis,
pulmonary embolism,
cervical incompetence,
multiple pregnancy,
vaginal bleeding,
premature leakage of membranes,
intrauterine growth restriction,
preeclampsia,
risk of premature labor, and
prepregnant type 1 or 2 diabetes mellitus.
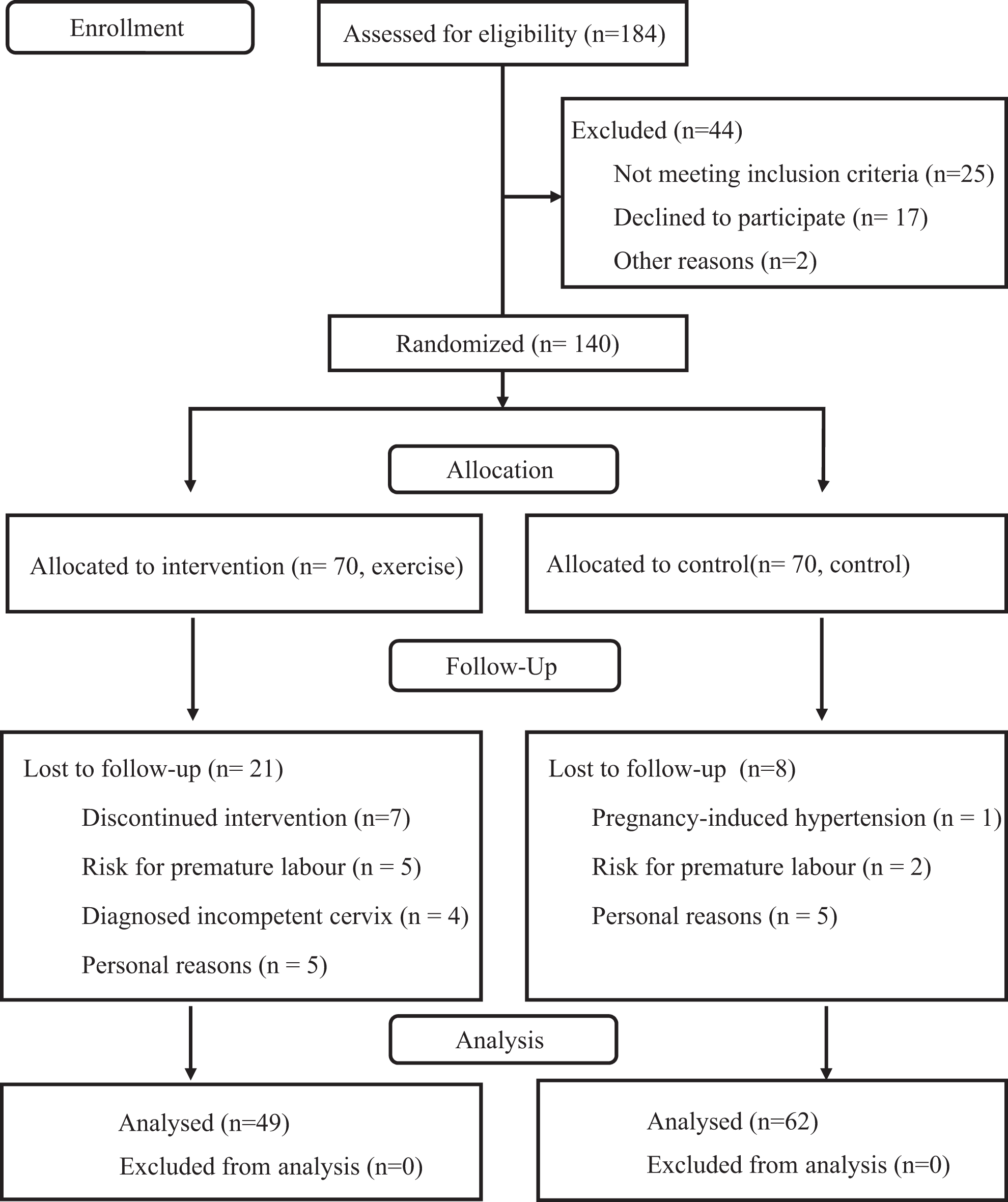
CONSORT 2010 flow diagram of the study participants.
Type of randomization
A simple randomization process was used to allocate the study participants. Regarding prerandomization evaluation, exclusion criteria were applied based on the clinical history of the all pregnant women and the first prenatal consult to identify contraindications for performing physical exercise. A computer-generated list of random numbers was used to allocate the participants into the 2 study groups (1:1 ratio) according to admission order and following the randomization list. To guarantee the concealment for the randomization procedure, each sequential number corresponded to a sealed opaque envelope containing information about the study group (exercise or control). Blinding of the study to the randomization arm was impossible due to the characteristics of intervention program (physical exercise).
The randomization blinded process (sequence generation, allocation concealment, and implementation) was performed by 3 different authors. The treatment allocation system was set up so that the researcher who was in charge of randomly assigning participants to each group did not know in advance which treatment the next person would receive, a process termed “allocation concealment.” Allocation concealment prevents researchers from (unconsciously or otherwise) influencing which participants are assigned to a given intervention group.
The women randomly allocated to the control group (CG; n = 70) received standard care from health professionals, and when asked by telephone interviews, they reported no regular exercise during their pregnancies. Women who were randomly allocated to the exercise group (EG; n = 70) received similar standard care and participated in a specific aquatic activities program. Women were excluded if they did not conform to the specifications of the allotted group.
Measures
Characteristics of women in both groups were recorded at the first prenatal visit (Table 1). Total maternal weight gain (kg), birth weight (g), and other maternal and fetal outcomes were obtained from hospital records.
Maternal Characteristics.a
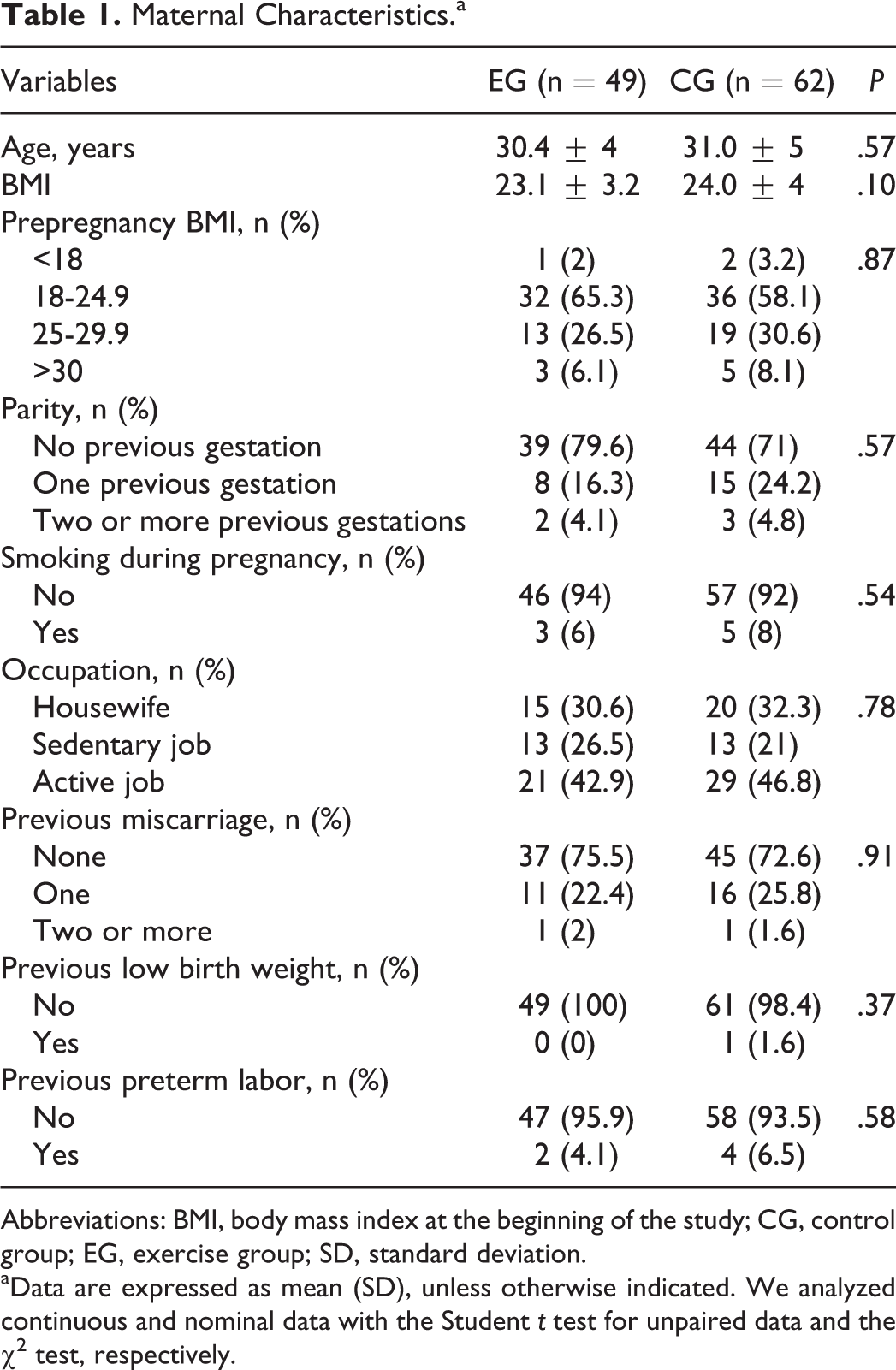
Abbreviations: BMI, body mass index at the beginning of the study; CG, control group; EG, exercise group; SD, standard deviation.
aData are expressed as mean (SD), unless otherwise indicated. We analyzed continuous and nominal data with the Student t test for unpaired data and the χ2 test, respectively.
Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in meters, and women were classified as underweight (BMI < 18.5 kg/m2), normal weight (BMI ≥ 18.5-24.9 kg/m2), overweight (BMI ≥ 25-29.9 kg/m2), or obese (BMI ≥ 30.0 kg/m2).
Primary outcomes
Total maternal weight gain during pregnancy (kg) and birth weight (g) were considered as primary outcomes. Gestational weight gain was calculated by the subtraction of weight measured at the first prenatal visit (representing pregravid weight) from weight measured at the last visit to the clinic before delivery. Gestational weight gain was classified as “adequate” or “excessive” according to the 2009 Institute of Medicine guidelines. 32 Recommended weight gains for underweight, normal-weight, overweight, and obese women are 12.5 to 18 kg, 11.5 to 16 kg, 7 to 11.5 kg, and 5 to 9 kg, respectively. Newborns were classified as having low birth weight or macrosomia when birth weight was less than 2500 g and greater than 4000 g, respectively. 33
Secondary outcomes
Gestational age (days), maternal blood pressure, infant length, head circumference, and Apgar scores were also recorded from medical records and analyzed.
Intervention
The exercise intervention program started at 8 to 11 weeks’ gestation and finished at 38 to 39 weeks’ gestation. The women exercised for an average of 25.8 ± 3.3 weeks, and a total of 85 sessions were planned for each participant. The women who did not meet the minimum required attendance of 80% of the sessions were excluded from the statistical analysis.
The exercise program was designed following the American College of Obstetricians and Gynecologists (ACOG) guidelines 31 to ensure safety and effectiveness. The exercise intensity was light to moderate according to Borg rating of perceived exertion scale 34 and ranged from 10 of 11 (“fairly light”) to 12 of 14 (representing “somewhat hard”).
The exercise program was performed in a swimming pool of different depths, depending on the type of exercise, 3 times per week on alternate days. Each session lasted between 55 and 60 minutes. All sessions were supervised by a qualified fitness specialist.
The structure of the exercise was the same in all of the sessions; the women started with a gradual warm-up that consisted of 8 to 10 minutes of walking at different intensities, static stretching of most muscle groups, and joint mobility exercises in the shallow area of the swimming pool.
The central part of the work was divided between:
aerobic exercises or dance (accompanied by music);
strength exercises and aquatic activities (propulsion exercises) in standing, supine, and ventral positions for 15 to 18 minutes; and
swimming lengths of the pool using all styles except butterfly for 8 to 10 minutes. Finally, a cooldown was performed for 10 to 12 minutes at the end of each session, including static stretching, relaxing, breathing, and flotation exercises.
Aquatic materials like foam rubber balls of differing sizes and swimming accessories such as floats, pull boys (buoyancy aiding devices), water noodles, armbands, and rubber rings were used. Swimming mitts were also provided for muscle conditioning and floating weights for resistance movement. Water temperature was 28.5°C to 29°C.
Statistical Analysis
We made power calculations for the primary outcome measures of excessive maternal weight gain considering a prevalence of ∼35% in the usual care group using previous studies conducted in the same population 5 and assuming a reduction of 25% in the intervention group. Under these assumptions, a 2-sample comparison (χ2) with a 5% level of significance and a statistical power of 0.80 gave a study population of ∼43 patients in each group. Assuming a maximum lost to follow-up of 10%, 47 women were needed for each group at baseline. 35
For treatment group comparisons, we analyzed continuous and nominal data with Student t test for unpaired data and χ2 tests, respectively. Data are shown as mean (standard deviation), and P values ≤.05 indicated statistical significance. Cohen’s d was used to determine the effect size in the mean comparisons and contingency coefficient in percentage comparisons. An effect size ranging from 0 to 0.20 was considered a small effect size, 0.20 to 0.50 was a moderate effect size, and >0.5 was a large effect size. 36 The odds ratio (OR) was used to calculate the effect of intervention on the likelihood of having excessive maternal weight gain. We conducted all statistical analyses using the Statistical Package for Social Sciences (version 18.0 for WINDOWS; SPSS Inc, Chicago, Illinois), and the level of significance was set to ≤.05.
Results
A total of 184 pregnant women were contacted at their first prenatal visit. Forty-four participants were excluded: 25 did not meet the inclusion criteria, 24 17 declined to participate, and 2 for personal reasons, leaving 140 healthy women randomized into 1 of the 2 groups. Twenty-one women in the EG were lost to follow up or excluded because of discontinued intervention (n = 7), risk of premature labor (n = 5), incompetent cervix (n = 4), and personal reasons (n = 5). A total of 8 participants in the CG were excluded from the study because of severe pregnancy-induced hypertension (n = 1), risk for premature labor (n = 2), and personal reasons (n = 5). Final analyses occurred on 111 healthy pregnant women, 49 in the EG and 62 in the CG (Figure 1).
The demographic characteristics of participants included in both training and CGs were similar (P > .5; Table 1). Adherence to training in the experimental group was >85%. No participant changed from the CG to the intervention group or vice versa.
Primary Outcome
The results showed no differences in total maternal weight gained (EG = 13.4 ± 10.8 kg vs CG = 13.2 ± 3.1 kg; P = .9) and birth weight (EG = 3259.4 ± 518.0 g vs CG = 3370.7 ± 339.0 g; P = .1); however, there was a higher percentage of women with excessive maternal weight gain in the CG (45.2%; n = 28) than in the EG (24.5%; n = 12; OR = 0.39; 95% confidence interval: 0.17-0.89; P = .02; Table 2).
Primary and Secondary Outcomes in Study Groups.a
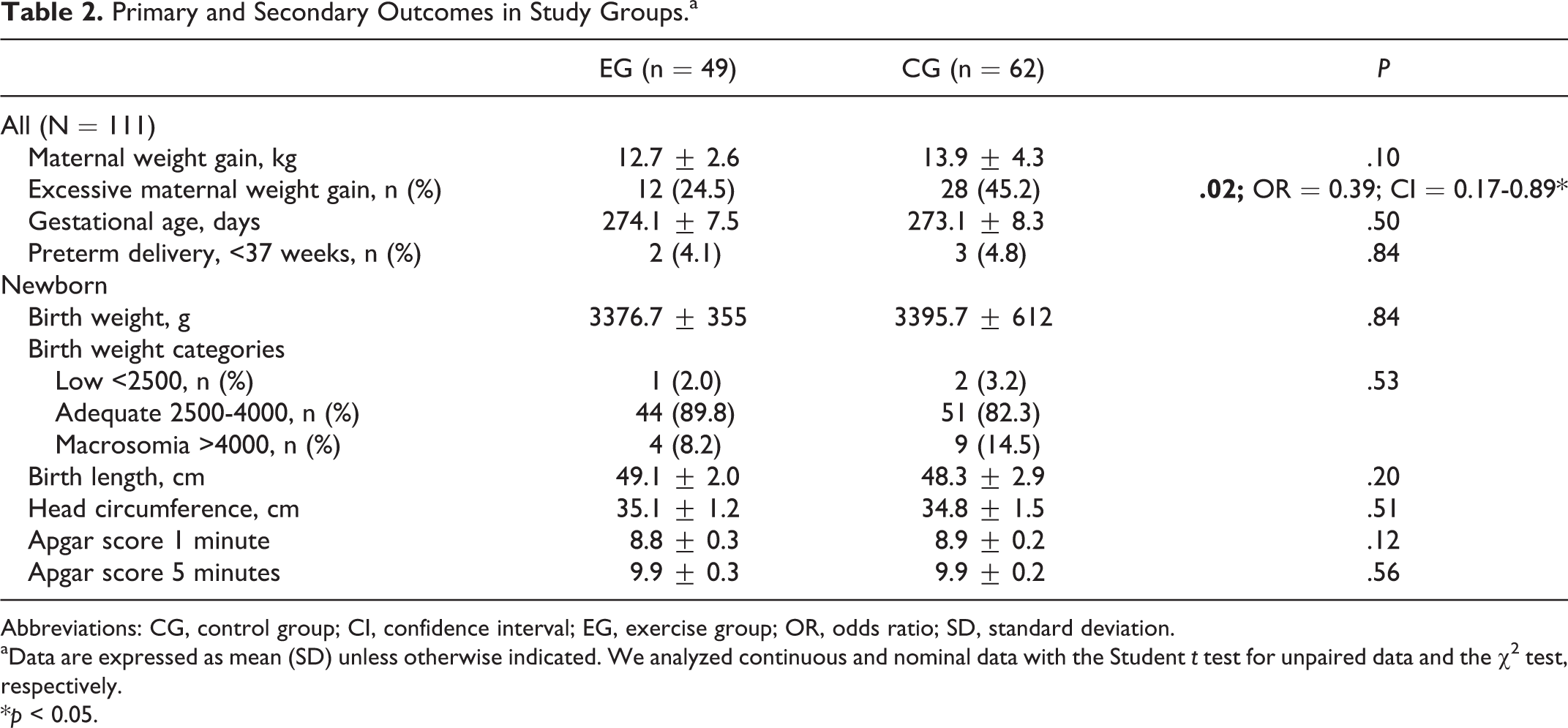
Abbreviations: CG, control group; CI, confidence interval; EG, exercise group; OR, odds ratio; SD, standard deviation.
aData are expressed as mean (SD) unless otherwise indicated. We analyzed continuous and nominal data with the Student t test for unpaired data and the χ2 test, respectively.
*p < 0.05.
Secondary Outcomes
The results of other pregnancy outcomes showed no differences between the study groups (Table 2).
Discussion
The aim of the present study was to evaluate the influence of a regular and supervised program of aquatic activities throughout pregnancy on maternal weight gain and infant birth weight. To our knowledge, this is the first RCT examining the effect of an aquatic intervention during pregnancy on maternal and newborn outcomes. The main novelty was to integrate into a program of water activities during pregnancy different types of exercises such as aerobic, resistance, stretching, propulsion, flotation, and so on. In addition, in the present study, swimming lengths were only a small part of the program sessions, while most of the activities were based on aqua exercises (including resistance exercise), giving a well-rounded approach to improving fitness. Our results showed the effectiveness of a structured aquatic program on the control of excessive maternal weight gain.
Few studies have used aquatic activities as part of an exercise intervention, and those that did presented positive results with no adverse effects for mother and fetus; however, only a small number used an RCT design. 18 -20 Furthermore, no studies examined the influence of an aquatics program on maternal weight gain and birth weight.
Baciuk et al 18 used an RCT to examine the influence of an aquatic exercise program on maternal cardiovascular capacity during pregnancy, labor, and neonatal outcomes (birth weight included); however, maternal weight gain was not measured. They found no differences between study groups for analyzed variables. Cavalcante et al 19 found no influence of a water aerobics program on maternal and newborn outcomes in 71 low-risk sedentary pregnant women using an RCT design. Granath et al 20 also used an RCT design and compared the influence of a land-based program versus water aerobics on low back or pelvic pain and sick leave in 390 healthy pregnant women. The intervention was performed once a week, and they found that water aerobics reduced pregnancy-related low back pain and sick leave.
Lynch et al 17 investigated the influence of a monitored swimming program during pregnancy on maternal fitness and fetal outcomes with a prospective observational study in 23 healthy sedentary pregnant women from 16 to 28 weeks of pregnancy. They evaluated the effects of swim-training on maternal heart rate, blood pressure and fetal heart rate, and umbilical artery systolic/diastolic ratio. The authors reported that a structured and well-supervised swimming program can improve maternal physical work capacity without untoward effects on fetal well-being. Smith and Michael 21 evaluated the effect of an aquatic exercise program on discomforts of pregnancy in 40 healthy pregnant women with a quasi-experimental (pretest/posttest) design. The authors found a positive association between the aquatic program during pregnancy with physical functioning, decreasing maternal discomfort, improving maternal body image, and improving health-promoting behaviors.
Juhl et al 16 examined the association between swimming during pregnancy and adverse maternal and fetal outcomes such as preterm birth, fetal growth measures, small for gestational age, and congenital malformations, especially regarding the use of disinfection by-products in swimming pool water. They studied 74 486 singleton pregnancies using self-reported exercise data (swimming, bicycling, or no exercise). The authors found that swimming in pool water was not associated with adverse reproductive outcomes.
A recent pilot study examined the effectiveness of a program of aquatic activities for high-risk, hospitalized pregnant women on bed rest as reflected by changes in blood pressure, amniotic fluid index, and the total length of gestation of pregnancy. The authors reported that women who received an aquatic exercise program had increased amniotic fluid index and length of gestation compared to controls. 22
Silveira et al 23 studied the impact of water aerobic exercise on cardiocirculatory fetal responses (cardiotocography patterns) by a nonrandomized controlled trial in 133 previously sedentary pregnant women. The authors reported no adverse effects of water activity–based exercise on any fetal responses.
Recently, Brearley et al 24 in an observational study examined the body temperature changes in pregnant women before, during, and after an aqua-aerobics class. The authors reported that maternal body core temperatures are maintained within safe limits during moderate-intensity aqua aerobic classes.
The main difference between our results and the literature cited above is the effectiveness of controlling maternal weight gain. Our program of aquatic exercise decreased the percentage of women with excessive weight gain. This may be due to the length of our program (19-20 weeks, ∼85 sessions) and time of the sessions (55-60 minutes), both of which are greater than the interventions used by other researchers. Land-based interventions may have more influence on birth weight, which may be due to the increased workload for pregnant women generated by land exercise compared to water activities.
Limitations
Limitations of the current study included no assessment of nutritional intake of the pregnant women, although they were all exposed to the same standard care. Future work should include assessment of dietary intake for both intervention and control women in an RCT design.
So What?
What is already known on this topic?
Comparative analysis between the present study and the other previous studies mentioned above becomes complicated due to the different study designs utilized. More RCTs are needed in this field to clarify current knowledge and generate new scientific evidence. The bottom line however, in examining the scientific literature with the necessary caution, would suggest that the result from our program of 3 weekly sessions of water activities throughout pregnancy is safe for mother and baby and prevents excessive maternal weight gain while preserving birth weight.
What does this article add?
New evidence regarding the benefits of regular water exercise during pregnancy now includes one of the most important pregnancy outcome measures, maternal weight gain as a modifiable risk factor for chronic disease. Excessive pregnancy weight gain can be prevented by a program of aquatic activities, without adverse maternal and fetal outcomes. After initial prenatal screening, pregnant women can start aquatic activities early and maintain an aquatic program until late pregnancy with no obstetrical complications, thus encouraging health-care practitioners to recommend aquatic activities throughout pregnancy.
What are the implications for health promotion practice or research?
It is known that excessive maternal weight gain is associated with important maternal (hypertension, gestational diabetes) and fetal (macrosomia) complications. From a clinical point of view, it is important to find new innovative strategies (for health professionals) to promote an adequate maternal weight for their clients. Supervised aquatic activities may be recommended to pregnant women as a safe and alternate program to land exercise that also encourages adherence because pregnant women appear to enjoy being active in water.
Footnotes
Acknowledgments
The authors would like to acknowledge the technical assistance of the Instituto de Obstetricia, Ginecología y Fertilidad Ghisoni (Buenos Aires), Argentina.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the Technical University of Madrid (AL16-PID-15), Spanish Ministry of Culture, Education and Sport (PRX15/00249), and University of Flores (Argentina).