
Abstract
Objective:
This systematic review synthesizes factors related to nicotine replacement therapy (NRT) use among adolescents seeking to quit smoking, using the social–ecological model as a guiding framework.
Data Source:
Searches of PubMED, ProQuest, EBSCOhost, and ERIC were conducted in July 2016.
Study Inclusion and Exclusion Criteria:
Original studies of cigarette smokers younger than 18 years that discussed NRT were included.
Data Extraction:
Two reviewers individually extracted study purpose, sample, design, and results.
Data Synthesis:
Factors were categorized by social–ecological model level and summarized.
Results:
A total of 103 907 articles were identified during initial search. After narrowing to peer-reviewed articles in English and eliminating reviews and adult-only studies, we reviewed 51 articles. These 51 articles identified factors from studies at each level of the social–ecological model: intrapersonal (k = 20), interpersonal (k = 2), organizational (k = 7), community (k = 11), and public policy (k = 14).
Conclusion:
Findings provide insight into the applicability of NRT for adolescent smoking cessation, and factors by social–ecological model level highlight areas for additional research. Future adolescent NRT studies should assess factors at the interpersonal, organizational, and community levels, as well as the interactions between levels.
Introduction
Tobacco use remains the leading preventable cause of disease and death worldwide. 1 Despite decades of tobacco prevention efforts, 3200 adolescents initiate smoking each day, many of whom will become lifetime users. 2 Adolescents are more susceptible to the addictive chemicals within combusted cigarettes and, therefore, more likely to become addicted despite sporadic smoking habits. 3 Furthermore, successful quit attempts among adolescent smokers are rare, perhaps due partly to the lack of best practice guidelines for this population. 3
Nicotine replacement therapy (NRT) is widely recommended for adult cessation as these medications can improve the odds of successfully quitting by 50%. 3 -6 The NRT is available in the form of gum, inhaler, nasal spray, transdermal patch, and lozenge, all of which increase adult tobacco abstinence rates. Although NRT has been found safe for adolescent use, it is not widely recommended due to the lack of evidence on the effectiveness of NRT among adolescents. 3 While some countries, including the United Kingdom and New Zealand, recommend NRT for individuals older than 12 years, the World Health Organization only includes it on the adult essential medications list, and many countries, including the United States and Canada, restrict it to individuals older than 18 years. 7 Compared to the vast amount of research among tobacco prevention and adult cessation, there is minimal literature related to NRT use among adolescents quitting smoking and thus hesitancy to recommend. While several authors 8 -11 have reviewed safety and efficacy studies related to NRT use among adolescents, no one yet has summarized additional factors related to NRT use, such as access, preferences, parental influence, and health-care influence. Identifying such factors may provide insight into why NRT has been ineffective among adolescents and provide information to improve future cessation efforts. Because NRT use for adolescent smoking cessation involves multiple levels of influence, a social–ecological framework was selected to synthesize information. Social–ecological approaches recognize that people participate in risky behaviors, such as tobacco use, because of a complex social system. 12 Therefore, researchers and practitioners are encouraged to use multilevel models to recognize the dynamics involved.
The social–ecological model (SEM) proposed by McLeroy et al 13 suggests behaviors result from influences at 5 levels: intrapersonal, interpersonal, organizational, community, and public policy (Figure 1). At the intrapersonal level are individual characteristics that influence behavior such as beliefs, attitudes, knowledge, and skills. At the interpersonal level are processes and groups that provide identity and support, including family, friends, and peers. For example, adolescents with parents who use NRT may be more likely to use themselves. 14,15 Within the organizational level are structures that constrain or promote behaviors such as schools, stores, and churches. Influences at the organizational level may include school health programs that provide adolescents NRT. The community level refers to broader social networks and community or cultural norms, which may include advertisements promoting NRT that may normalize NRT use. 16 Finally, the public policy level includes local, state, and federal policies and laws that regulate or support healthy practices and actions.
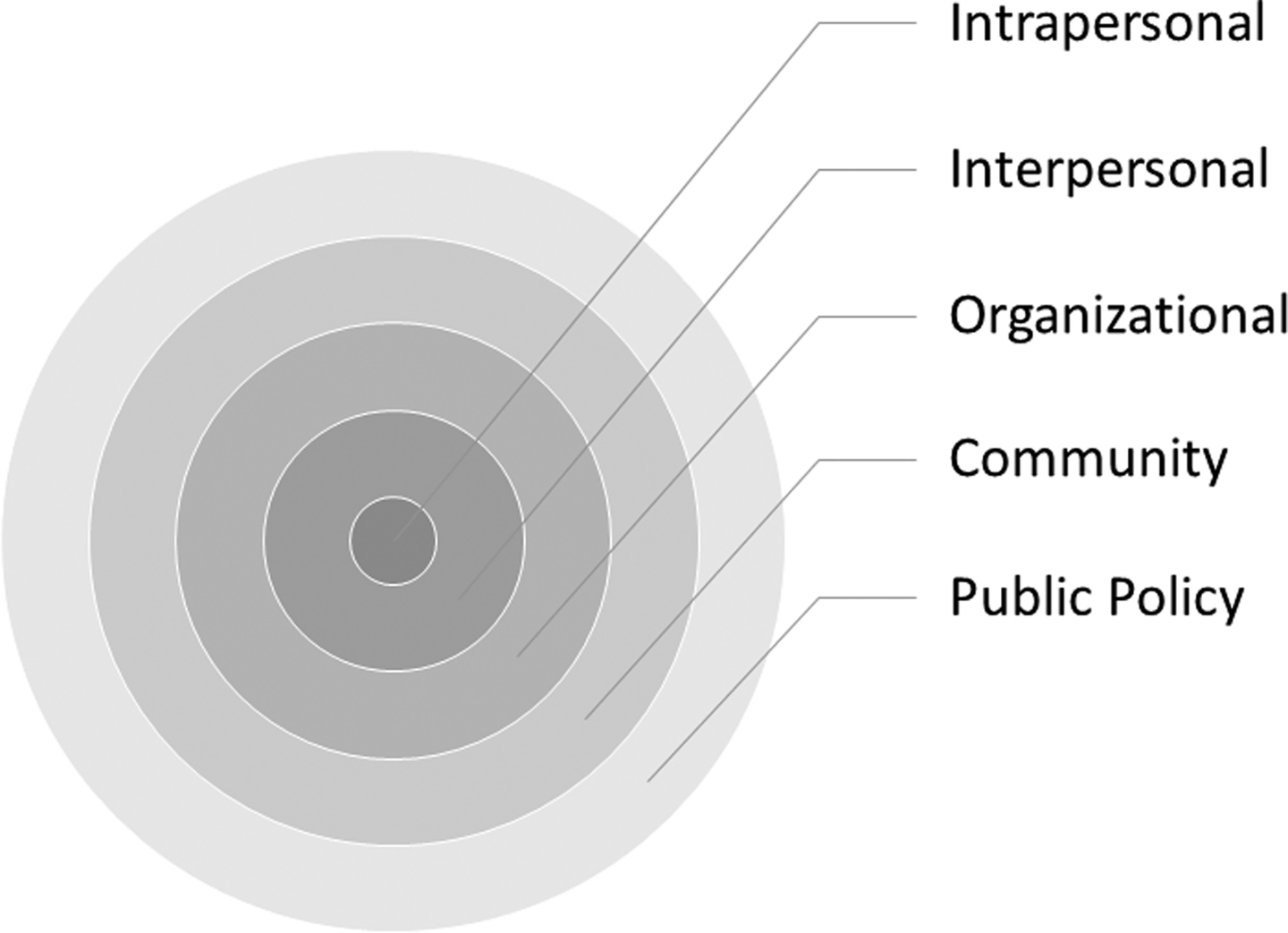
Social–ecological model.
The social–ecological perspective also emphasizes the interaction between, and interdependence of, factors within and across all levels of a health problem. Those who employ social–ecological approaches recognize that participating in risky behaviors such as tobacco use is the result of a complex social system. 12,17 Because individual behavior has multiple levels of influence and is shaped by and shapes the surrounding environment, it is necessary to identify and understand the factors within each level.
The purpose of this study was to systematically review the literature within the framework of the SEM to identify a comprehensive list of factors related to NRT use among adolescents seeking to quit smoking. For the purposes of this study, adolescent refers to any study which includes individuals younger than 18 years, due to NRT restrictions among this age-group in the United States. Further understanding of the factors related to adolescents using NRT for smoking cessation and the corresponding levels of influence may benefit clinicians working directly with this population as well as researchers and policy makers.
Methods
Data Sources and Extraction
The search process was initially conducted in January 2016, and then repeated in July 2016, to identify any additional published articles. Four databases (EBSCOhost, ERIC, ProQuest, and PubMed) were searched using the following keyword string: (adolescen* OR teens OR “young adults” OR students OR youth) AND (smoking OR cigarette OR tobacco OR nicotine) AND (NRT OR “Nicotine Replacement Therapy” OR Patch OR Gum OR Lozenge OR “Pharmacological treatment”). Initial search across all databases resulted in 103 907 articles, which were narrowed to peer-reviewed, full-text articles (7401 articles). Abstracts (164) and full texts (107) were reviewed to determine whether articles met the inclusion criteria (Figure 2). Broad inclusion criteria were used to ensure comprehensiveness. The inclusion criteria were (1) original research (no reviews or commentaries) that contained (2) information related to NRT for (3) adolescent smokers younger than 18 years of age.
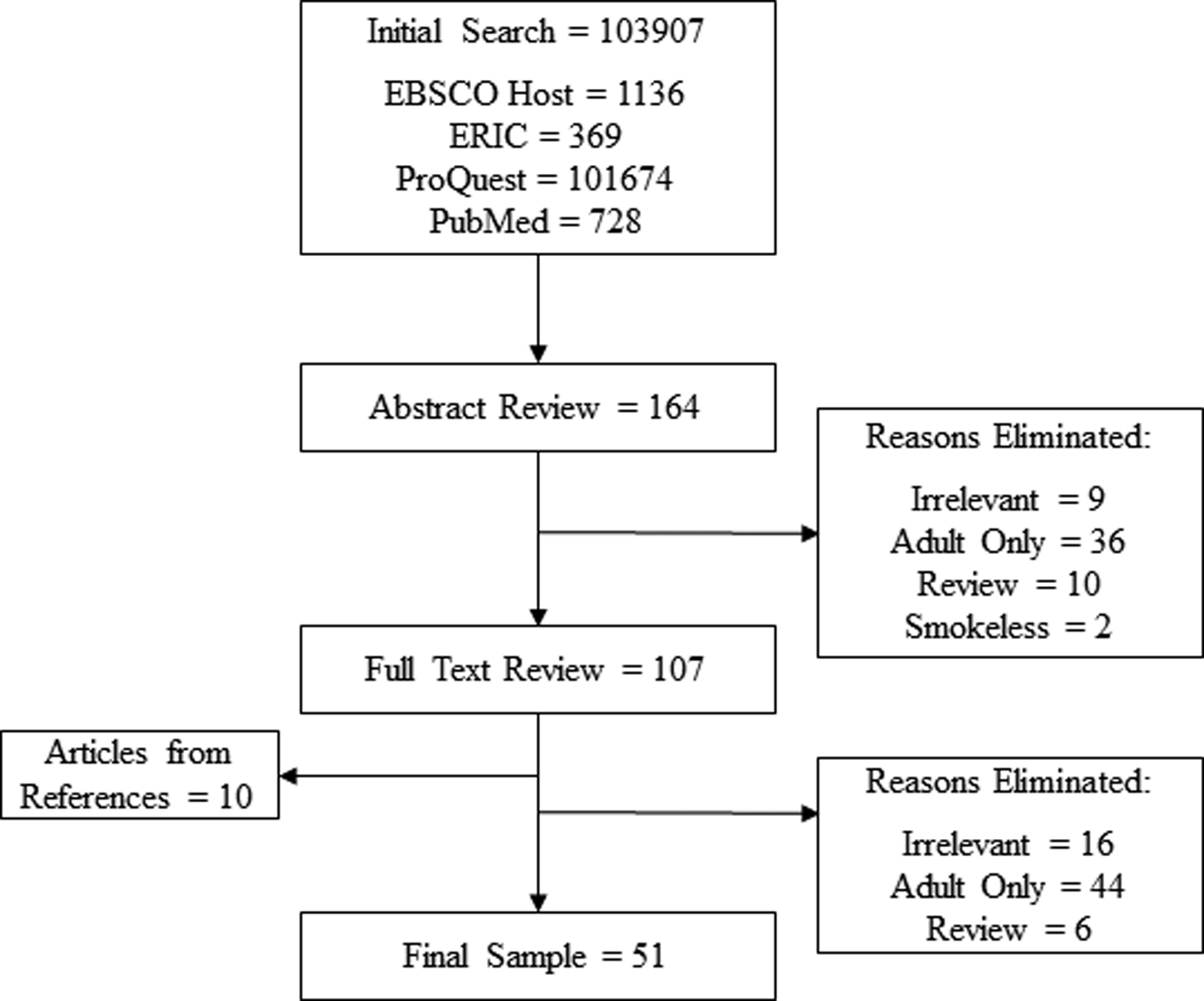
Article search process.
Data Synthesis
Two reviewers independently analyzed articles for factors related to adolescents using NRT for smoking cessation. Study purpose, sample characteristics, design, and results were extracted. Factors related to NRT were coded for the corresponding SEM level (intrapersonal, interpersonal, organizational, community, or policy). Because individual factors were coded as opposed to entire articles, some articles identified factors at multiple levels. Coders used past models on other public health topics, including smoking initiation, as examples for determining which factors fit within each level. 18,19 Within each SEM level, factors were grouped by topic areas and findings were compared and synthesized. Any disagreements were discussed and resolved with input from a third reviewer.
Quality assessment
We conducted quality assessments for each of the studies using 1 of 3 tools. These findings were used to provide an overall understanding of study quality and identify areas for improvement. For experiments and randomized trials, we used the Cochrane Risk of Bias tool which covers 6 areas of bias: random sequence generation, allocation concealment, performance bias, detection bias, attrition bias, and reporting bias. 20 For cross-sectional studies, we used the National Institute of Health’s Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies, a 14-item measure which covers selection bias, measurement bias, and confounders, resulting in a rating of good, fair, or poor quality. 21 For qualitative studies, we used the Critical Appraisal Skills Programme Qualitative Research Checklist, a 10-item tool which assesses whether qualitative methods, recruitment, data collection, and analysis were conducted appropriately. 22 Two reviewers independently assessed each of the studies and discussed discrepancies with a third reviewer.
Results
Fifty-one articles with factors related to NRT for adolescents younger than 18 years were analyzed for this study. Articles identified or assessed factors at each level of the SEM (Table 1), with most at the intrapersonal or policy level. Study methodologies included cross-sectional surveys, randomized controlled trials, focus groups, secondary analyses, nonrandomized trials, experimental studies, and qualitative interviews. Quality ratings varied by study type. Interventions and randomized trials were typically low risk of bias, with nonrandomized trials limited in areas of blinding and randomization. Most cross-sectional studies were rated fair and could be improved by controlling for potential confounding factors and better descriptions of measures used. Most qualitative studies were rated as good per the Critical Appraisal Skills Programme tool, with the most frequent areas for improvement in justifying which qualitative approach was selected and addressing potential bias of the researcher within the study. Factors are organized below by SEM level (Figure 3) following a brief overview of NRT prevalence.
Factors Related to Adolescent NRT Use by Social–Ecological Model Level.

Abbreviations: CASP, Critical Appraisal Skills Programme Qualitative Research Checklist used to assess qualitative studies, ratings include good, fair, or poor; CI, confidence interval; NRT, nicotine replacement therapy; NIH, National Institute of Health’s Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies used to assess cross-sectional studies, ratings include good, fair, or poor; OR, odds ratio; OTC, over-the-counter; ROB, Cochrane Risk of Bias tool used for interventions, ratings include low, high, or unclear risk of bias.
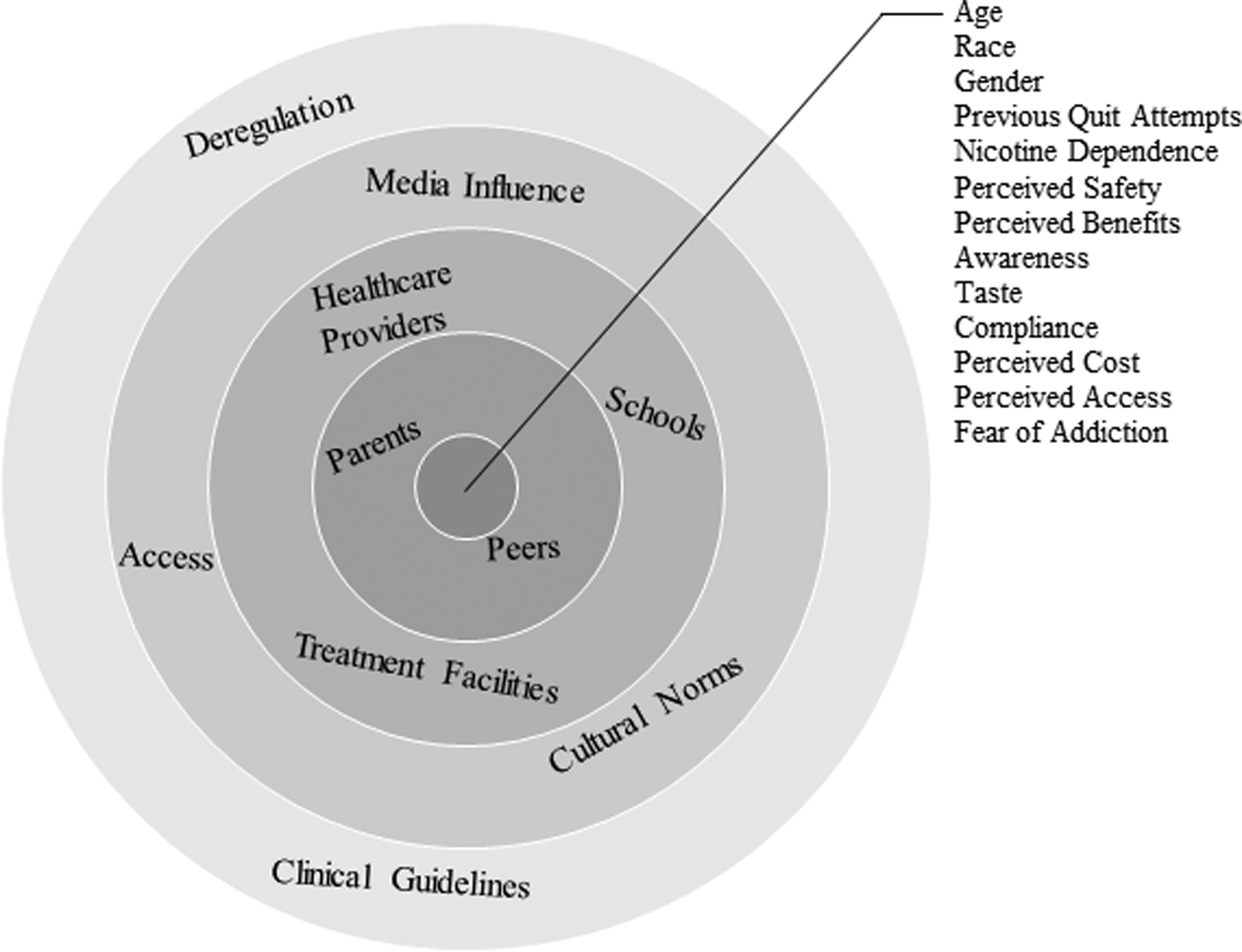
Factors at each social–ecological model level.
Prevalence of NRT Use
Twelve studies 23 -34 examined NRT prevalence among adolescents. These studies found between 2% 29 and 23.8% 30 of adolescents had ever used NRT. In demographic analyses, males were more likely to have used NRT than females, 23,26,27,30,31 older adolescents were more likely to have used NRT than younger adolescents, 29,32,33 and European Americans were more likely to have used NRT than African Americans. 26,33,34 Additionally, adolescents who had previously attempted to quit smoking were more likely to have used NRT. 32,34 The reasons adolescents used NRT included to quit smoking, as a substitute when smoking not possible, and to try it. 26,27,31,35
Factors at the Intrapersonal Level
Twenty articles identified factors at the intrapersonal level related to NRT use among adolescents (see Table 1). Factors included physiological effects such as withdrawal and cravings, awareness and knowledge of NRT, attitudes, preferences, compliance, perceived cost and availability, and addiction concerns.
Awareness, knowledge, and beliefs
Lack of awareness 29,36 and knowledge 37 -39 of NRT for smoking cessation were common among adolescents surveyed, as were misperceptions related to health consequences and safety. 37 However, Rainio and colleagues 29 found NRT awareness increased with age and was much greater among daily smokers than never smokers, suggesting lack of awareness may not be generalizable to all adolescents.
Beliefs related to perceived success were also identified as a factor for adolescent NRT use, both beliefs in effectiveness 40 and relevance. 15,37 Amos and colleagues 37 found adolescents believed NRT was for older or more addicted smokers and therefore lacked confidence in its relevancy. On the other hand, Al-Delaimy and colleagues 15 found younger adolescents were more likely than older adolescents to believe NRT helps people quit smoking. They also found never smokers were more likely than established or experimental smokers to believe NRT helps people quit, males were more likely than females to believe NRT helps people quit, and Hispanics and African Americans were more likely than European Americans to believe NRT helps people quit. 15
Preferences
Several articles discussed adolescent preferences for NRT, with some adolescents expressing great interest, 28,41,42 while others reported some 23,43 or no interest in NRT. 44 In other studies, students were as likely to use glucose and candy as an alternative to NRT. 45 Specific reasons given for such preferences were that adolescents did not like the taste 45,46 and they felt NRT did not adequately substitute for handling cigarettes. 46
Compliance
Compliance is an important factor for any medication use and was mentioned several times within the efficacy studies as well as some of the preference articles. 47 -50 Adolescents were noncompliant for a number of reasons, including forgetfulness, side effects, lack of effect, and wanting to smoke. 47,50 Factors associated with compliance included extraversion, higher education, and agreeableness. 50
Perceived barriers
Concerns with using NRT included cost, 37,38,43 access, 38,51 and addiction to NRT. 37 According to Lane and colleagues, 27 adolescents with increased spending money were more likely to use NRT, which may support adolescents’ reported cost concerns. However, the same study also found those with no disposable income were likely to use NRT, suggesting use may also be related to availability. 27
Physiological effects
Physiological effects refer to withdrawal, addiction, and cravings. Three studies addressed these factors in relation to NRT among adolescents. Raisamo and colleagues 30 found NRT users were more likely to perceive themselves as addicted to smoking, a finding also supported by heaviness of smoking. After identifying a correlation between nicotine dependence and withdrawal symptoms among adolescents, Prokhorov and colleagues 52 concluded NRT is important for adolescent cessation because nicotine dependence and withdrawal interfere with adolescents’ readiness to quit. Dickmann and colleagues 53 also examined adolescent withdrawal, within the context of craving systems in relation to gender. Dickmann and colleagues 53 found similar levels of withdrawal but higher craving in females, with females not using hormonal contraceptives experiencing the highest level of cravings. The overlap between withdrawal symptoms and premenstrual syndrome symptoms is lessened by hormonal contraceptives, but cravings are not impacted, which could explain why NRT is traditionally found to be less effective in women than men.
Factors at the Interpersonal Level
Two studies addressed interpersonal relationships and adolescent NRT use, both addressing the role of parents. Al-Delaimy and colleagues 15 found adolescents who lived with an adult who used NRT were more likely to think NRT is a sure way to quit, while Wyman and colleagues 54 found few parents of middle and high school students agreed the school should provide nicotine patches for students who are trying to quit.
Three articles, which were included within this study for their focuses on NRT at other SEM levels, mentioned interpersonal characteristics in adolescent preferences for smoking cessation. Although NRT use was not the main focus for the interpersonal characteristics mentioned, potentially related factors identified were advice from friends, 41 contracts with friends, 43 and seeking professional support with friends to eliminate the potential social cost related to participating in a cessation program. 51
Factors at the Organizational Level
Seven articles addressed factors related to adolescent NRT use at the organizational level, including an analysis of school characteristics related to NRT, and studies related to access to NRT prescriptions within schools, substance treatment facilities, mental health-care facilities, and general health-care settings.
Price and colleagues 55 assessed NRT availability within 250 school-based health centers and found most schools had not seriously thought about offering prescription services for NRT and few had provided NRT for a year or longer. School health-care center beliefs related to NRT were also assessed, with over half reporting they believed NRT increases the likelihood of quitting. Schools that did not provide NRT were more likely to believe that students would not use services, students would abuse NRT, parents would object to offering, staff did not have experience with NRT, and staff did not have the authority to provide NRT. Some of the specific reasons for not offering NRT were that the centers were run by nurses without prescriptive authority, lack of evidence to support recommending it, and high cost. 55
In a survey of 12 adolescent substance use residential treatment centers, Chun et al 56 found less than half of sites provided NRT to adolescents. In a similar study among mental health centers, Muilenburg et al 57 also found less than half of centers provided the nicotine patch, though the counselors stated pharmacotherapies were used by very few adolescents. Also surveying mental health-care providers, Morris and colleagues 28 found the professionals were split on their views regarding NRT, with half viewing medications as inappropriate for youth, whereas the other half asserted these cessation aids were not utilized enough.
Physicians were more likely to assist adolescent smokers if they had greater knowledge of and confidence using NRT, 58 though the majority of pediatricians had not prescribed NRT. 59 The most common reasons for prescribing NRT were request from adolescent, openness to quitting, or health problem exacerbated by smoking. 59
Factors at the Community Level
Four studies discussed media influence related to NRT use. Wakefield and colleagues 16 found public health antitobacco campaigns in the United States were matched or exceeded by tobacco and pharmaceutical cessation advertising. 16 Three studies looked at the effects of NRT and Zyban advertising on youth perceptions. 15,60,61 Although 2 of the studies found that NRT ads may influence youth perceptions on quitting, 15,61 long-term perceptions such as intention to smoke or health effects were not changed. 60,61
Five articles discussed access to NRT, with 1 reporting over half of adolescents having easy access. 26 Adolescents acquired NRT from friends and retailers. 29 In test purchases, NRT products were successfully obtained in most purchases by a minor buyer without proof of age. 62 If the minor was asked his age, the store was much less likely to sell NRT. Stores where the cash register gave an age prompt or where alcohol was sold were more likely to ask about age and less likely to sell NRT. 62 In Lane and colleagues’ 63 spatial analysis of school characteristics related to student NRT use, students in schools located near more pharmacies were less likely to use NRT.
While none of the studies directly assessed cultural norms related to NRT use, 3 studies did use geographic location, which is a primary contributor to norms, as a covariate. Price and colleagues 55 found schools in the Western part of the United States twice as likely as those in the South or Midwest to have offered prescription services. Wyman and colleagues 54 found parents of students in rural locations were more likely to agree schools should provide NRT, though Lane and colleagues 63 found students in schools within urban areas were more likely to use or have used NRT.
Factors at the Public Policy Level
Two studies looked at the effect of policy on NRT use and similarly found that NRT use rates among adolescents did not increase after deregulation. 29,35 Another study estimated the effects of the change in policy on NRT prescriptions to adolescents and found prescribing was highest among older adolescents and females, but there were no major differences after deregulation. 64
Eleven articles assessed the efficacy and/or safety of NRT for adolescent cessation. Although none of the studies found NRT to be unsafe for adolescents, efficacy results varied. Three studies 49,65,66 found promising results in assessing NRT, while the remaining studies concluded NRT was ineffective for adolescent smoking cessation. 67 -71 The methodologies and outcomes of these studies have been reviewed elsewhere. 8 -11
Discussion
This systematic review retrieved and analyzed 51 articles related to NRT for adolescent smoking cessation. The goal of this study was to identify factors related to adolescent use of NRT for smoking cessation within the framework of the SEM. According to the SEM, there are a number of factors influencing the use of NRT which exist at multiple levels. The 23 factors (Figure 3) identified within this study fit into each of the 5 SEM levels, though a majority were focused at the intrapersonal level, on individual factors.
At the intrapersonal level, 14 factors were identified including reasons for use, lack of knowledge, and preferences. While the majority of factors identified were at this level, there were few duplicate findings across studies. This may reflect the lack of funding for replication studies or indicate low interest in NRT for cessation. Additionally, many of the studies were focused on general cessation as opposed to NRT specifically and therefore contained limited relevant information. However, awareness, knowledge, and preferences do appear important factors for adolescent NRT use.
Only 2 studies focused on the interpersonal level, suggesting parental influence is important for adolescent NRT use. Peer influence related to NRT use among adolescents has not been studied, despite it being a major influence on smoking initiation. 72,73 Within smoking prevention literature, peer and parental influence are heavily cited factors, yet there is little interpersonal focus related to adolescent cessation. It is possible that medication and treatment are perceived more as individual decisions, and, therefore, peer influence is not important for cessation; however, this has not yet been determined.
There were also fewer studies at the community and organizational levels compared to the intrapersonal and policy levels. A few studies focused on the health-care perspective, finding that health-care providers did not provide adolescents NRT for a range of reasons, including lack of education. This is important when considering NRT is currently restricted to adolescents younger than 18 years in many jurisdictions, as, theoretically, the only way to obtain it would be through a doctor’s prescription. Additionally, studies thus far have only looked at whether NRT was prescribed and not at whether it was accompanied by diagnosis or education. Research indicates prescribing NRT in itself is not effective; NRT prescriptions should be accompanied with diagnosis, rational dosing, instructions and warnings, and follow-up. 74 At the community level, some articles mentioned cultural aspects but none directly studied cultural influences in using NRT. Cultural influences such as rural designation have been linked to tobacco use 2 and, as suggested by the limited findings within this review, possibly NRT. However, further analyses are needed to confirm and understand these potential differences.
Most articles at the policy level were related to efficacy and safety, which contribute to clinical guidelines and regulations. Clinical guidelines and regulations, while nested within the public policy level, impact all other levels within the SEM. For example, guidelines inform practitioners who then prescribe medications to adolescents. A few studies assessed these potential cross-level interactions. Specifically, increases in NRT abuse and prescriptions related to changes in regulations were identified as potential factors related to adolescent use. However, the studies reviewed found little change, whether in increased use or abuse or in prescriptions for NRT use relative to regulation. There was 1 other cross-level interaction study, parent perception of schools providing NRT. Additional research should explore interactions across levels, including what influences individual perceptions (eg, health-care advice, peer use). Understanding how factors across levels interact will provide greater context and will improve interventions to address such issues. In applying the findings to a real-world example, based on the factors identified and SEM theory which recommends addressing factors across levels, an intervention seeking to increase NRT use for adolescent smokers may seek to address individual factors such as perceived safety of the product through individual education as well as parent and health-care provider education.
Despite reviewing 51 articles for this study, there remains a sense of limited research regarding NRT for adolescent smoking cessation. One limitation, which may indicate a trend within the field, is the lack of studies on NRT directly related to adolescents, specifically those younger than 18 years of age. There were several potential factors that were discovered in articles that did not meet the adolescent age inclusion criteria that are likely applicable to this population, such as readability of NRT instructions. 75 Therefore, this cannot be assumed to be an exhaustive list of factors that contribute to adolescents using NRT. For example, several potential factors discussed within the reviewed studies were related to general smoking cessation strategies, as opposed to specifically NRT. Such factors include adolescent preferences which may be specific to NRT, such as confidentiality, 43 flexible programming, 51 and preferring resources not at school. 51 Finally, there are several limitations within the current study. First, authors reviewed only published literature, which introduces the possibility for publication bias. Additionally, the SEM tool as a framework has limitations, notably, factors may not clearly fit within a level. For example, some models suggest media at the community level, while others place it at the policy or macro level. Also, the studies reviewed may not have used SEM during design or analysis and therefore may not have considered multilevel or across-level interactions.
Despite these limitations, the factors identified provide insight into NRT for adolescent smoking cessation. While a number of factors have been identified at the adolescent and policy levels, additional research should be conducted at the interpersonal, organizational, and community levels to allow researchers, clinicians, and policy makers a more holistic understanding of NRT use among adolescents seeking to quit smoking.
So What?
Adolescent smoking remains an issue, yet there are no best practices for cessation. The NRT is widely recommended for adults, yet limited evidence exists for adolescent use. This review identified 51 articles related to NRT for adolescent smoking cessation and used a social–ecological model framework to identify factors that influence adolescents using NRT. The majority of factors were identified at the intrapersonal or public policy levels. Future research should explore factors at the interpersonal, organizational, and community levels, as well as interactions across levels in order to improve interventions utilizing NRT for adolescent cessation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.