
Abstract
Objective:
To determine: (1) What research has been done on health promotion interventions for low-wage workers and (2) what factors are associated with effective low-wage workers’ health promotion programs.
Data Source:
This review includes articles from PubMed and PsychINFO published in or before July 2016.
Study Inclusion/Exclusion Criteria:
The search yielded 130 unique articles, 35 met the inclusion criteria: (1) being conducted in the United States, (2) including an intervention or empirical data around health promotion among adult low-wage workers, and (3) measuring changes in low-wage worker health.
Data Extraction:
Central features of the selected studies were extracted, including the theoretical foundation; study design; health promotion intervention content and delivery format; intervention-targeted outcomes; sample characteristics; and work, occupational, and industry characteristics.
Data Analysis:
Consistent with a scoping review, we used a descriptive, content analysis approach to analyze extracted data. All authors agreed upon emergent themes and 2 authors independently coded data extracted from each article.
Results:
The results suggest that the research on low-wage workers’ health promotion is limited, but increasing, and that low-wage workers have limited access to and utilization of worksite health promotion programs.
Conclusion:
Workplace health promotion programs could have a positive effect on low-wage workers, but more work is needed to understand how to expand access, what drives participation, and which delivery mechanisms are most effective.
Objective
Workplace health promotion (WHP) programs offer unique opportunities for addressing workers’ health. 1 They build on existing structures at work, including work group norms, social identities, and employee time spent at work, to target a range of healthy behaviors (eg, physical activity, healthy eating, prevention, and/or smoking cessation) both on- and off-the-job. Previous reviews of the literature have already examined the programs’ content (ie, what makes them effective) 2 –5 ; its financial viability to organizations (ie, return on investment) 6,7 ; how to engage organizations of different types and size 8 ; and the relationship between health promotion programs and socioenvironmental factors. 9,10 However, they do not address the specific considerations of low-wage workers accessing or utilizing such programs. And yet, this is an important consideration in the United States, which has the greatest proportion of low-wage workers of 31 other developed countries 11 and high rates of poor health among low-wage workers.
Low-Wage Workers
The United States has a higher incidence of low-wage workers, defined as those with weekly earnings below 150% of the federal minimum wage for a 40-h week, 12 than 31 other developed countries. 11 Indeed, many of the fastest growing occupations in the United States are low-wage jobs, including food preparation ($10.60/h) and childcare work ($10.72/h), and tend to consolidate in the service sector. 13 Low-wage workers are more likely to work in part-time rather than full-time jobs and are less likely to have stable employment throughout the year.
Low-wage workers experience socioeconomic and racial disparities in health, including higher rates of morbidity and mortality, 14 greater exposure to physical and social hazards in the work environment, and a higher risk of chronic illness, such as heart disease or diabetes. 12 They are more likely to face precarious employment, 15 –17 job insecurity, 18 and exposure to job-related hazards that higher-wage workers can avoid. 19 One way that researchers and practitioners have tried to address these disparities is through targeted programs outside the workplace (eg, in low-income communities or health-care settings). 20 However, low-wage workers face unique challenges across both work and nonwork domains, including limited time and resources. Thus, interventions targeted at low-income neighborhoods alone may not address the challenges that low-wage workers face in balancing the demands of work and family and meeting their own health needs.
This article provides a scoping review to systematically compile this information. The objective of this scoping review is to address 2 primary research questions: (1) What research has been done on health promotion programs that target or include adult low-wage workers in the United States and (2) what factors have been associated with effective health promotion outcomes among low-wage workers?
Methods
We conducted a scoping review to systematically map the existing literature on health promotion programs for low-wage workers “in terms of the volume, nature, and characteristics of the primary research.” 21 The scoping review has emerged as a form of work that is distinct from traditional systematic reviews, which aim to determine the strength or quality of the evidence from empirical studies that use standardized research methods. Although both methods are systematic, the scoping review was the best fit for this domain, given the relatively small amount of literature and diverse research designs.
Data Source
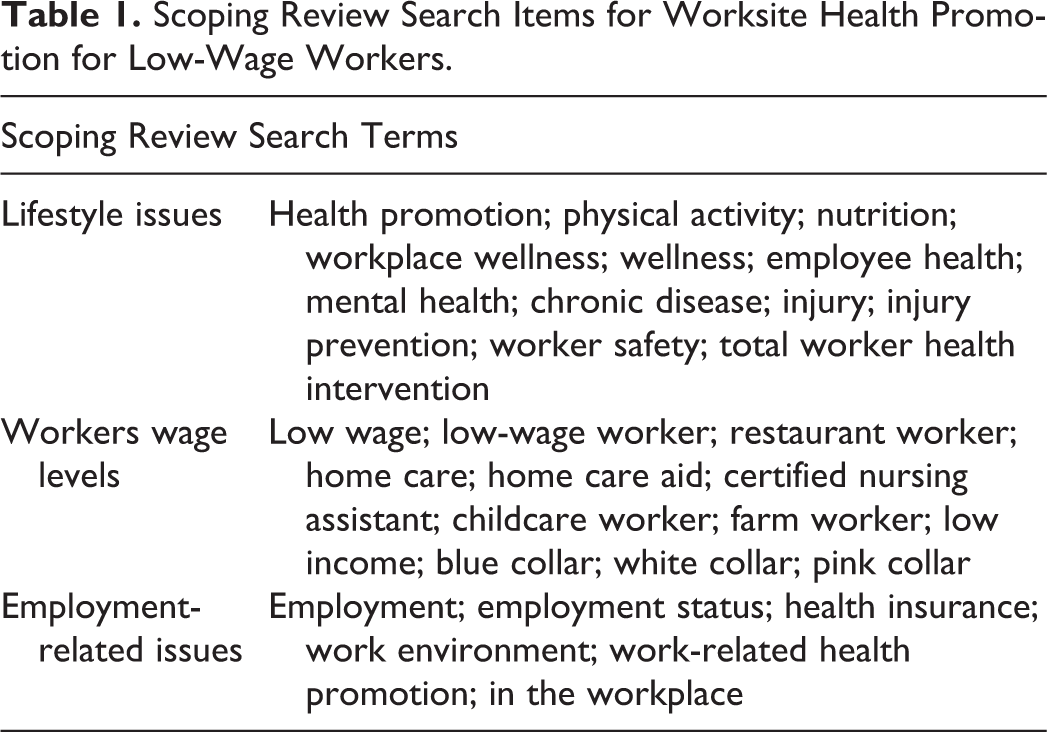
In January 2016, we searched PubMed and PsychINFO for articles around health promotion and low-wage workers. We followed the methods framework for searching, inclusion/exclusion, and data extraction from the literature that is explained in depth by Pham et al 21 and Gough et al 22 starting with the formation of a research team of members of the Workplace Health Research Network to inform each phase of the review. 23,24 Five articles that met our inclusion criteria came from an AHRQ literature review of Total Worker Health. 25 We updated the search in July 2016 to ensure inclusion of the emerging literature (all search terms are listed in Table 1).
Scoping Review Search Items for Worksite Health Promotion for Low-Wage Workers.
Study Inclusion and Exclusion Criteria
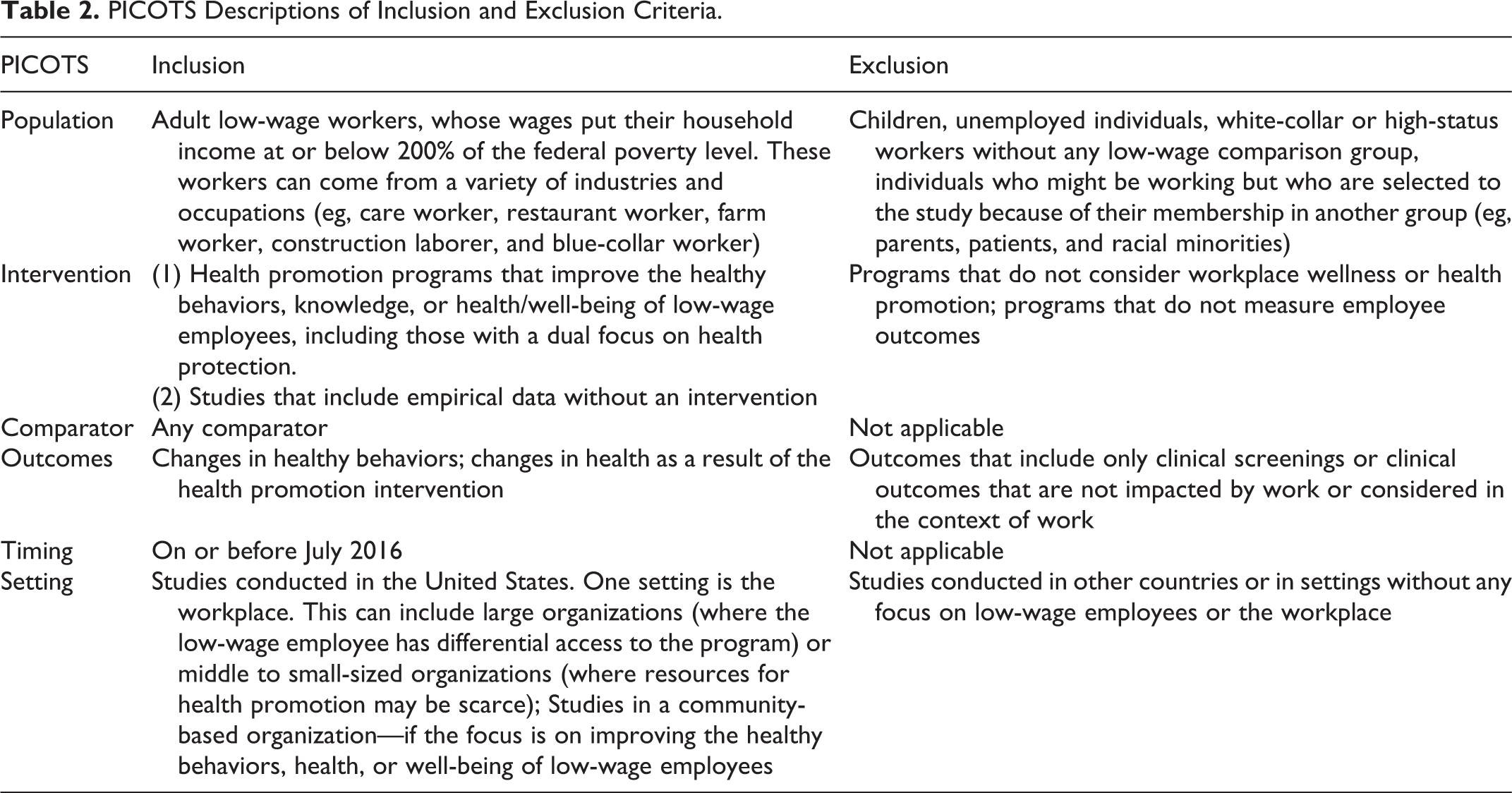
From the initial 1174 articles, 345 duplicates were removed (see Figure 1). The authors reviewed the titles of the remaining 829, removing any that did not meet the inclusion criteria. We use the populations, interventions, comparators, outcomes, timing, and setting (PICOTS) framework 26 to delineate our eligibility criteria (Table 2). To meet the inclusion criteria, studies had to (1) be conducted in the United States, (2) include intervention or empirical findings (either quantitative or qualitative) around health promotion, and (3) measure changes in health, healthy behavior, or well-being of adult low-wage workers. Articles not conducted in the United States (n = 224), those lacking empirical findings around health promotion (eg, reviews, commentaries, or theory-building articles; n = 84), or articles that were not relevant because they had only a child-focus (eg, how low parental wages affect the health of children), an employer or health-care focus (eg, patients’ adherence to clinical testing; n = 52), or did not include low-wage workers (n = 353) were excluded.
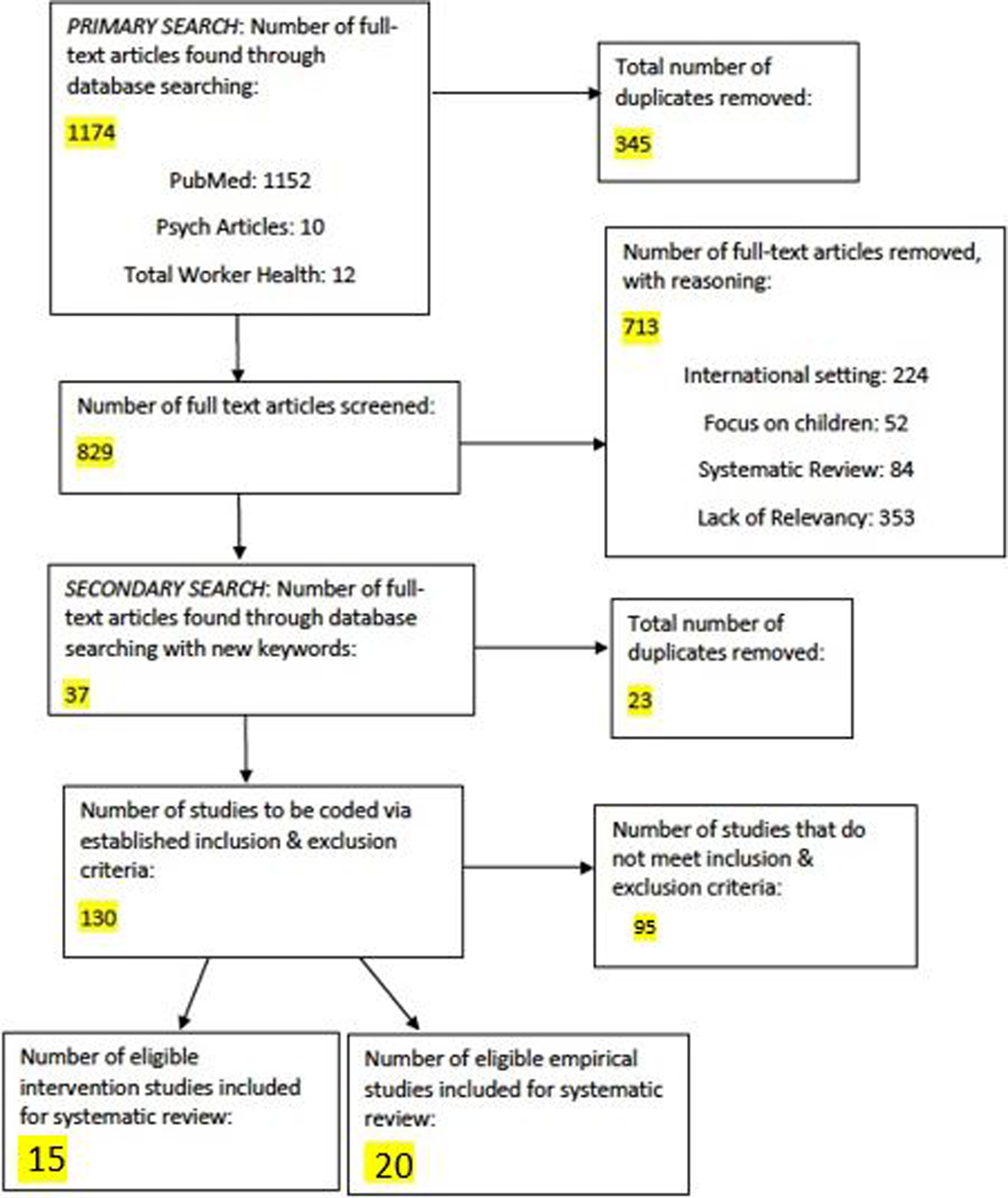
Disposition algorithm.
PICOTS Descriptions of Inclusion and Exclusion Criteria.
Data Extraction and Synthesis
The resulting articles were randomly divided among the authors for a review of abstracts and article content to verify that they met the inclusion criteria and to assist in developing codes for data extraction. The articles from the second, expanded search were reviewed in the same way. From the resulting 130 articles across both searches, 41 were identified as possibly meeting the eligibility criteria. The reviewers had shared agreement on the inclusion of 12 intervention studies and 20 empirical articles and the exclusion of 1 study that had a non-US sample (80% agreement across the 41 studies). For the remaining 8 studies, the reviewers discussed them to reach consensus on inclusion. Three of those articles were found to have a health promotion intervention and to meet the inclusion criteria, whereas 5 articles were excluded upon closer review. The final sample included 15 intervention studies and 20 nonintervention studies that reported empirical findings (see Figure 1). The research team discussed categories to be used for data extraction, based on their initial understanding of the articles. Articles were divided and assigned evenly among the coauthors to be coded around the following categories: theoretical foundation; study design; health promotion intervention delivery; intervention-targeted outcomes; sample characteristics; and work, occupational, and industry characteristics. After the first round of coding, they revisited the codes and discussed items that were confusing or did not fit. For instance, in the second round, the large set of health-related outcomes across the intervention studies were consolidated under 2 codes: diet and lifestyle, which included physical activity, prevention, and smoking cessation. Two reviewers then coded the rest of the intervention studies (see Tables 3 and 4). The nonintervention studies did not include intervention codes (see Table 5).
Intervention Study Model, Design, Outcomes, and Sample Characteristics.
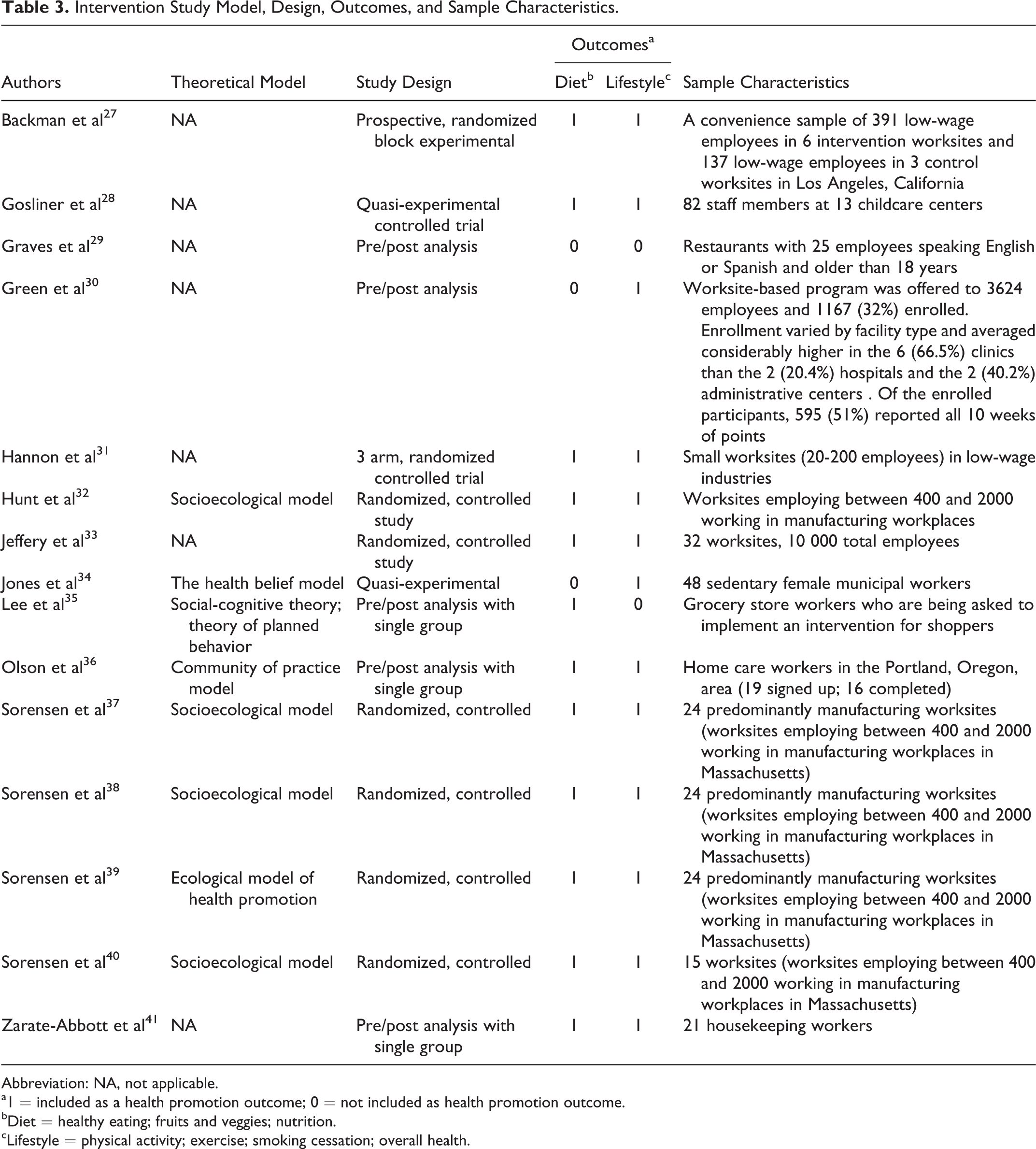
Abbreviation: NA, not applicable.
a1 = included as a health promotion outcome; 0 = not included as health promotion outcome.
bDiet = healthy eating; fruits and veggies; nutrition.
cLifestyle = physical activity; exercise; smoking cessation; overall health.
Intervention Study Delivery and Results.
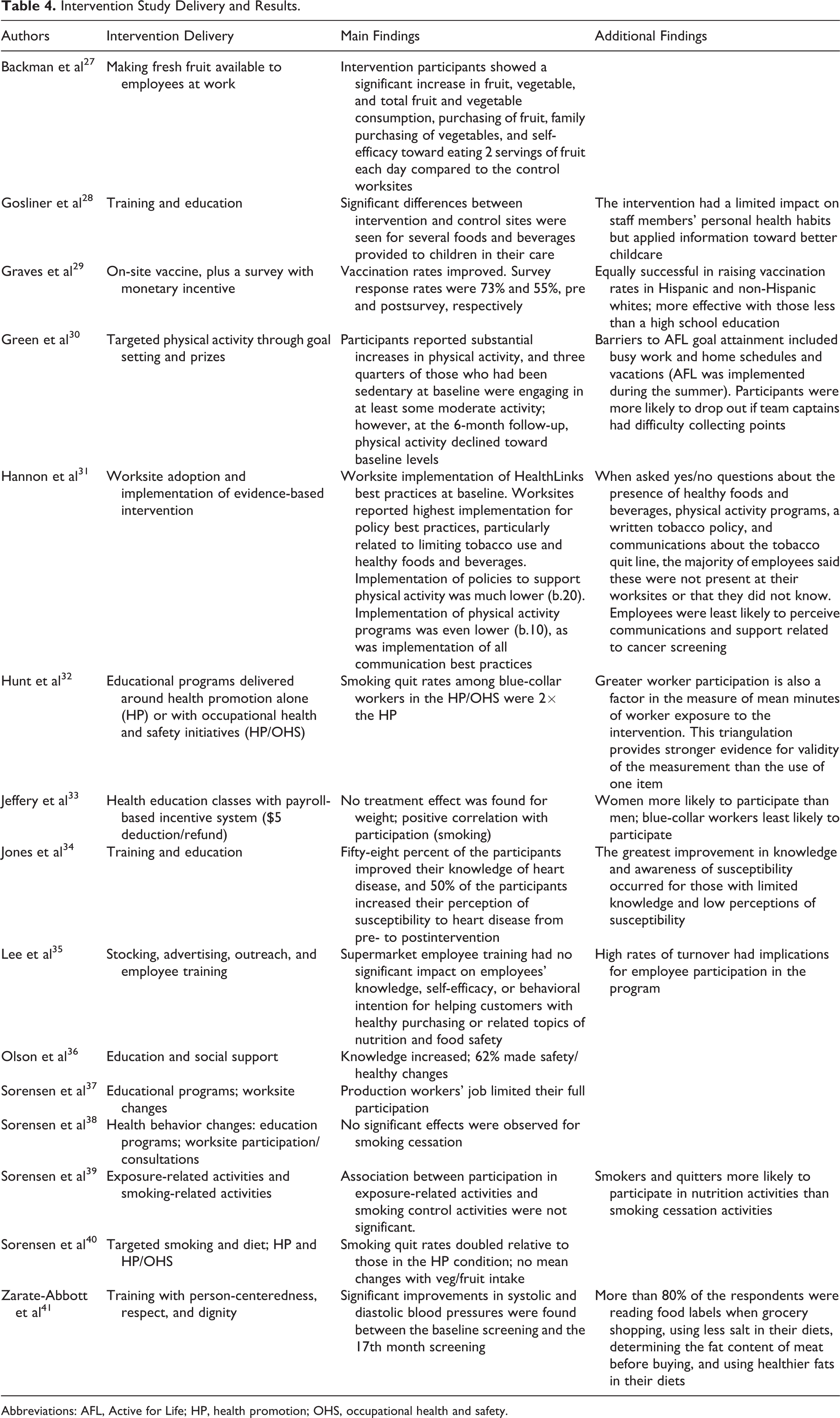
Abbreviations: AFL, Active for Life; HP, health promotion; OHS, occupational health and safety.
Nonintervention Study Design, Characteristics, and Sample Outcomes.
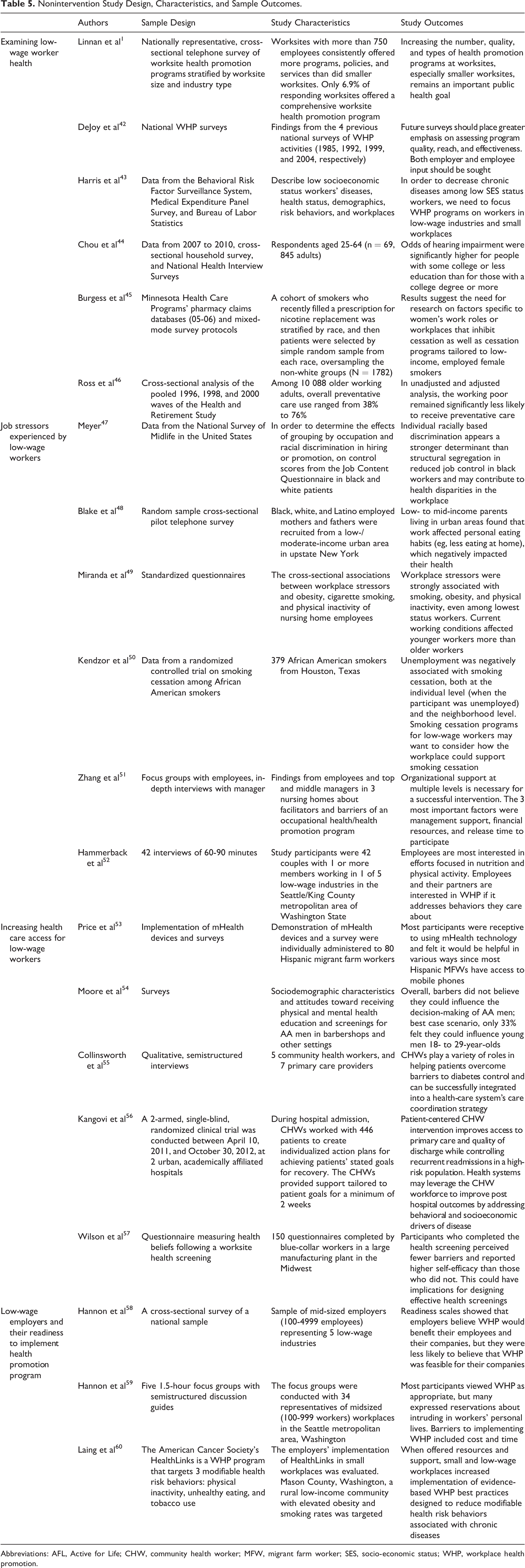
Abbreviations: AFL, Active for Life; CHW, community health worker; MFW, migrant farm worker; SES, socio-economic status; WHP, workplace health promotion.
Results
Study Design
Fifteen studies evaluated a health promotion intervention with low-wage workers, and 20 studies included empirical findings that addressed health promotion with low-wage workers but did not explicitly assess intervention outcomes. Instead, the 20 studies used a variety of methods including secondary data analysis, qualitative data analysis, and survey research.
Details About the Worksite Health Promotion Interventions
Population and sample
The intervention-based studies included participants from various industries (Table 3), most notably workers from low-wage occupations, such as blue-collar, hourly, supermarket, and childcare workers. Six of the samples included comparison groups of professional workers. 32,33,37 –40 About 42% of employees in the WellWorks studies were low-wage workers 37 but only 18% in the Healthy Worker Project study. 33
Theoretical frameworks
Four theoretical frameworks underlay 8 of these studies, whereas nearly half of the intervention studies did not explicitly specify a theoretical framework. The most frequently applied theory was the socioecological model, 61 –63 which suggests that one’s health is affected not only by individual characteristics but also by the environment (eg, peers, the workplace, family, or home). It is useful for studying low-wage workers’ health promotion because it frames the complex set of factors impacting their health and inhibiting their access to and utilization of health promotion programs. Social cognitive theory 64 was the second-most utilized framework, and introduces self-efficacy (eg, one’s belief about their ability to bring about a desired outcome) 65 to describe how people learn new health promotion behaviors. Although self-efficacy is important to learning, low-wage workers might have limited opportunities to build self-efficacy, 66 due to the lack of control they have over their work 47 and personal environments. 67 Third, the Health Belief Model (Becker & Maiman, 1975) 68 , which suggests that people are more willing to engage in preventive health behaviors when they perceive themselves at risk of health illness or injury, was noted in Jones et al. 34 Finally, the communities of practice model 69,70 describes how groups of people share information (eg, about health) through joint participation and engagement 69 and was applied in the COMPASS study. 36 This model was applied to low-wage workers because they are often isolated from sources of social support at work, including coworkers or managers, which potentially inhibits their ability to build supportive networks in their workplaces.
Characteristics of the intervention studies
Tables 3 and 4 provide an overview of the 15 intervention studies, including the study design, outcomes, and sample (Table 3), and the intervention types, delivery methods, and main findings (Table 4). Eight of the intervention studies were randomized controlled trials (RCTs), representing 5 distinct RCT projects. The remaining 7 intervention studies included 2 that used a quasi-experimental design 28,34 and 5 that used a 1-group, pre/postdesign to evaluate vaccine rates 29 and changes in employees’ knowledge and behaviors. 30,35,36
Fourteen studies addressed healthy diet or lifestyle programs and 1 highlighted a vaccine program. For low-wage workers, providing convenient access to these programs was associated with better health in some situations. For example, when fresh fruit was provided to low-wage workers in the workplace at no cost, 27 not only did workplace consumption of fresh fruit increase but also the low-wage workers with access to it reported higher personal consumption of fruits and vegetables, higher purchasing of fruit, and higher family purchasing of vegetables outside of work. 27 In the same way, restaurant workers, including both Hispanic and non-Hispanic whites, had higher vaccination rates when vaccines were provided in the workplace. 29 However, Jeffery et al 33 found no treatment effects for employees in organizations that offered interventions (ie, on-site classes and an incentive system around weight loss and smoking cessation) versus those that did not, although participation in the program overall was related with better weight loss outcomes. 33 In fact, the findings comparing low-wage workers (eg, craftsmen and laborers or blue-collar workers) to their professional colleagues consistently found that low-wage workers were less likely to participate in health promotion programs (participation ranged from 13%-36.9% for low-wage workers vs 43%-50.8% for professionals on nutrition/weight and from 18%-27.6% vs 37.3%-47% for smoking cessation). 33,39 It could be that the convenience of eating available fruit or receiving a 1-time flu shot are easier for low-wage workers to use than programs emphasizing continuous diet and exercise.
Education and training were the primary intervention delivery techniques. Among female municipal workers with known heart disease risk factors, education was especially effective for increasing knowledge and awareness of susceptibility among those who were unaware of their susceptibility for heart disease. 34 Some of the interventions for low-wage workers included combinations of tactics for encouraging participation in the program. For instance, 1 set of studies combined training (eg, weight loss or smoking cessation initiatives) and participation in occupational health and safety initiatives related to the training (ie, reducing exposure to particulates that contribute to lung damage) and found that it produced smoking quit rates twice as high as health promotion education alone. 32,40 Incorporating relationships was another tactic used in some studies. For instance, home care workers developed relationships during training that could be used to share information about avoiding injury in the future. 36 Similarly, for Hispanic female housekeepers, incorporating individual consideration, respect, and dignity (personalismo, respeto, and dignidad) into the training sessions seemed to increase their engagement with the trainers—the researchers suggest that the number of questions participants asked and their interest in their blood pressure readings increased throughout the training session. 41 However, these combinations did not guarantee changes in behavior. Following skill-based training with personalized consideration, more than 80% of the Hispanic female housekeepers above incorporated new knowledge about diet (eg, reading food labels), but fewer than half practiced the exercises they were taught. 41 It could be that reading labels was an easier task than exercising. It presents a dilemma around knowing how to be healthy and having the motivation to practice healthy behaviors.
At least 2 studies in this review were not designed with the employee’s health as the target, but rather, the customers that employees serve. In the first of these, 82 childcare workers received training around nutrition to examine whether they would alter the types of food options for children in their facility, 28 and in the second, grocery store workers were trained to examine whether their health knowledge would influence shoppers’ healthy purchasing. 35 The trained childcare workers versus controls were indeed more likely to offer fresh fruit instead of sweets at events and parties for the children in their facilities and reported greater confidence in their ability to talk to parents about the children’s health. 28 In terms of their own behavior, reported changes were minimal, the only statistically significant difference being a decrease in the consumption of sweetened beverages, suggesting that the largest beneficiaries of the training were the children they watched. This creates a dilemma around health promotion aimed at the consumer, where the workers may have adopted a “do as I say, not as I do” mentality to health. The trained grocery store clerks, though, did not impact customers’ behaviors nor did they change their own behaviors. 35 This might, however, be a reflection on the content of the training. Since a growing number of low-wage workers interact directly with customers especially in the food services sector, the value provided by their organizations is directly related to the service the workers provide and may provide opportunities for mutual benefits. 71
Nonintervention Studies Around Low-Wage Workers and Health Promotion in the United States
Secondary data to examine low-wage worker health
In addition to the intervention studies, other studies yielded further insight into the extent to which health promotion may be available for low-wage workers (see Table 5). Six studies examined the state of worksite health promotion using secondary analysis of panel data sets, including the national survey of health promotion, 42 the Behavioral Risk Factor Surveillance System, 43 the National Health Interview Surveys, 44 and the Minnesota Health Care Program pharmacy claims data. 45 They examine the state of worksite health promotion in the United States and correlates of health and wellness for low-wage workers in specific occupations or organizations. These studies found that low-wage workers are less likely to engage in preventative care or health promotion than their higher-wage counterparts, 43,46 although rates for vaccinations are not significantly different between the 2 groups. At the same time, the National Worksite Health Promotion Survey data collected in 2004 found that only about 7% of all worksites had comprehensive worksite health promotion programs, 1 which varied with the size of the employer. Larger worksites (more than 750 employees) were 6.7 times as likely as smaller worksites (50-99 employees) to offer a comprehensive health promotion program. 1 This is significant since low-wage workers tend to be concentrated in smaller organizations. 43 Moreover, a lower income level—even after adjusting for higher risk occupations, such as farming, service, and blue-collar jobs—was associated with increased risk of sensory impairment, including hearing loss. 44 At the same time, low-wage workers were found to be less likely to engage in preventative health screenings 46 or report high levels of physical activity. 43
Job stressors experienced by low-wage workers
Five studies examined job stressors associated with low-wage work, including work-life balance and on-the-job discrimination that can impact health. For example, 1 empirical study of low- to mid-income parents living in urban areas found that work affected personal eating habits (eg, less eating at home), which negatively impacted their health. 48 Another study used a national survey to examine how discrimination mediates the relationship between a person’s education and their job control and subsequently their health. 47 Framing the analysis using the job demands, job control mode, 72 Meyer 47 found that due to individual racial discrimination, black workers had less job control than white workers, and this lack of job control was associated with poorer self-rated health. Workplace stress impacts aspects of health, including obesity, smoking, and physical activity. 49 At the same time, employed African Americans had a better chance of abstaining from smoking than unemployed African Americans. 50 Finally, barriers to participating in health promotion programs can come from different levels and vary with organizational and managerial support. 51 In a qualitative study of low-wage workers, researchers found that while most employees were excited about the idea of worksite health promotion, especially programs centered on diet and exercise, they were skeptical about whether their employer would want to offer them. 52
Increasing health-care access for low-wage workers
Five studies examined strategies for increasing low-wage workers’ access to health-care services, either through new technologies, new domains for targeting health, or the incorporation of additional staff to increase the reach of programs. 53 –57 Although low-wage workers can be difficult to reach, especially part-time or temporary employees with little stability in their jobs, most have access to mobile devices. A survey of 80 migrant farm workers suggest that these mobile devices could be used to monitor low-wage workers’ health and manage or prevent chronic diseases across worksites. 53 Another strategy looked at increasing access to health care by expanding the involvement of community health workers (a group of workers who typically meet low-wage criteria) into care teams, which improved access to care and health outcomes among other low-wage individuals through community-based, but not worksite, settings. 55,56 In a similar way, Moore et al 54 examined the feasibility of expanding the delivery of health education or screenings to barbershops. Although they found that African American men preferred to obtain health education and screenings in clinical offices first, this was followed by barbershops and churches. The authors suggest that these nontraditional settings could be useful future targets for influencing health literacy or health perceptions in partnership with traditional health-care settings. 54
Low-wage employers and their readiness to implement health promotion programs
Finally, a growing number of studies focus on small- or mid-sized employers’ readiness to implement health promotion programs because these employers are likely to employ low-wage workers. 58,59 Using qualitative focus groups of human resources professionals representing these workplaces, these studies find that many workplaces want to increase access to worksite health promotion but face a number of barriers to doing so. 59 Some representatives expressed concern that the employees would find it intrusive, in addition to concerns about finding the time and money to make it effective. 59 This stream of research identifies strategies for increasing the adoption of worksite health promotion among these employers. 60
Conclusions
This scoping review summarizes the results of 15 intervention studies and 20 nonintervention studies that examine the state of health promotion activities for adult low-wage workers. As noted previously, the use of the scoping review provided rich results in an area where research is still relatively new, by including a variety of studies that use diverse methods and designs which may have been excluded from the traditional systematic review. Our primary finding is that while there is growing interest in understanding the health needs of low-wage workers and opportunities for addressing those needs in the workplace, the findings in this area are only beginning to shed light on how to most effectively integrate health promotion into workplaces for low-wage workers. We highlight a few key findings below to guide future research.
Greater Health Risks
First, low-wage workers have greater health needs than professional workers given their higher likelihood of working in more hazardous workplaces and living in communities with fewer health promoting resources. 12,14 They are less likely to have access to preventative care or health promotion, 43,46 especially those who are part time, temporary, or working multiple jobs, making them ineligible or unable to participate. They also face different barriers to health in the work context, 47,66 including heavy job demands, race-based discrimination, 47 and even exposure to hazardous materials. 32 Thus, from a public health perspective, worksite health promotion programs could be especially beneficial for addressing the health of this underaddressed group.
Improving Access to Health Promotion
Low-wage workers, especially those who are part time, temporary, or have multiple jobs, tend to have less access to health promotion programs, either because the organization does not offer them 8 or because they are ineligible or unable to participate. However, these barriers make health promotion even more necessary. From a public health perspective, finding innovative ways to address low-wage worker health in the workplace could deliver a bigger “bang for the buck” than comparable programs for professional workers. To improve low-wage worker access, the reviewed studies identify the potential use of new technologies, 53 new staffing models, 55,56 or new settings. 54 Two of the reviewed studies directly increased access by increasing convenience—delivering fresh fruit or providing vaccinations in the workplace. 27,29 The convenience of access may have increased employees’ willingness to utilize them. More work is needed to understand how to increase low-wage worker access to health promotion programs, especially through alternative approaches that might provide greater community access and acceptability, such as was illustrated through the use of community barbershops or community health workers.
Improving Utilization of Health Promotion
Even with access, employees may not participate, given financial constraints or a lack of management support for the program. 51 Programs that ask employees to withhold small amounts from their paycheck—where the funds are returned (or lost to charity) when personal health goals are met (or not) 33 —may actually generate less participation than those who simply offer rewards for participation. 31 For low-wage workers, the risk of losing even a nominal amount of money if health goals are not met could be too great a burden to warrant participation. 73 At the same time, we mentioned that combining tactics for delivering training (eg, linking smoking cessation education with organizational initiatives to reduce exposure to hazardous particulates or linking training with relational support) could prove to be more effective than training alone. It is worth noting that in the studies that combined tactics, they did not always result in health behavior changes. More work is needed to understand the mechanisms through which low-wage workers make decisions around engaging in health promotion programs. It is necessary to consider the commitments required by the program (eg, time, initial investment, and convenience), the organizational support provided to low-wage workers, and also the impact of combining delivery tactics. One future direction for researchers developing WHP programs for low-wage workers would be to use the National Health and Nutrition Examination Survey to identify specific health issues facing low-wage workers and to develop health promotion programs that will target and address those issues.
Differences by Worker Characteristics
Only 4 studies analyzed their data by subgroups. The analysis consistently demonstrated that low-wage workers were less likely than professional workers to participate in health promotion programs. Similarly, individuals living below the poverty line were less likely to engage in physical activity during their leisure time than those at or above the poverty line. 18 As is the case for many health promotion interventions, women were more likely than men to participate in health promotion programs. 33 Caucasian men and women were more likely to engage in leisure time physical activity than other racial/ethnic groups, whereas Mexican American men and women were least likely to participate. 18 Future work should further explore the underlying factors leading to disparities in program accessibility and/or acceptability across worker populations to improve program effectiveness and health promotion utilization.
Aligning Health Promotion for Employees With Value for Customers
Finally, the nature of work in a largely for-profit, consumer-driven society has prompted researchers to search for indirect means for providing benefits to workers. Although a business case for health promotion programs has been made with full-time employees in large organizations, 6,74 considering costs to the organization or absenteeism, productivity, and employer-based health care, the value proposition for low-wage workers has not been as clearly articulated. While some researchers are working to understand whether and how small- and mid-sized organizations can provide health promotion to their employees, 3,8,58 others are examining how to align the health of employees and customers to generate value and strengthen the case for health promotion in workplaces. For instance, some train-the-trainer models indirectly encourage employers to focus on low-wage workers’ health by tying it to the health of the customer. 75 The premise is that organizations employing low-wage workers may have an incentive to train their workers around health promotion if the initiative can be shown to improve the value (ie, quality, safety, or efficiency) of services to both employees and customers. Future interventions require a better understanding of the motivations driving employer behavior, to align low-wage worker health with employer initiatives.
Limitations
Our review does have some limitations. First, given the understudied nature of low-wage workers, we included some studies that did not explicitly focus on the demographics of their population, even though the population is likely to fall into our definition of “low wage.” In at least 1 study, we included an occupational group (eg, childcare workers) that is notoriously poorly paid in the market (average hourly wage = $10.72). 76 However, the article did not focus on the low-wage aspect of the work. Second, given the science related to health promotion among low-wage workers is just emerging, the scope of this review precluded performing quantitative comparisons across study findings. Third, self-reported data on health promotion outcomes might have reflected participants’ desire to please interventionists rather than reflect actual behavior. We expect these limitations will be addressed as more research is conducted in this area. In the meantime, this review provides a summary of the types of studies, frameworks, and findings conducted to date related to health promotion among specifically low-wage workers in the workplace; highlights the potential public health benefits of targeting this group; and provides recommendations for advancing research in this area.
So What?
What is already known on this topic?
Existing research suggests that workplace health promotion (WHP) programs, when appropriately designed and implemented can be effective.
What does this article add?
This article shifts the focus of WHP programs to low-wage workers, who are less likely to have access to or to utilize these programs but who could benefit significantly from them.
What are the implications for health promotion practice or research?
Through a broad assessment of the WHP research, this review highlights the potential public health impact of targeting low-wage workers. It calls for more research around how to increase WHP access and utilization for this group. These include initiatives to understand what drives employer participation and which delivery mechanisms are most effective for this group. It also calls for more research on how to align employee health promotion with customer well-being to improve organizational investments in such programs.
Footnotes
Acknowledgments
The authors recognize the Workplace Health Research Network, including members of the coordinating and collaborating centers, for its support in developing this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by the Grant U48DP005010-01S1 SIP 14-031: “Workplace Health Research Network Collaborating Center for Underserved Workers,” funded by the Centers for Disease Control and Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention of the Department of Health and Human Services.