
Abstract
Purpose:
To evaluate a healthy eating and physical activity intervention for immigrant families, derived through community-based participatory research.
Design:
The Healthy Immigrant Families study was a randomized controlled trial with delayed intervention control group, with families as the randomization unit.
Setting:
US Midwest city.
Participants:
Participants were recruited by community partners from Hispanic, Somali, and Sudanese immigrant communities.
Intervention:
Family health promoters from participating communities delivered 6 healthy eating modules, 4 physical activity modules, and 2 modules synthesizing information in 12 home visits (60-90 minutes) within the first 6 months. Up to 12 follow-up phone calls to each participant occurred within the second 6 months.
Measures:
Primary measures were dietary quality measured with weekday 24-hour recall and reported as Healthy Eating Index score (0-100) and physical activity measured with accelerometers (14 wear days) at baseline, 6, 12, and 24 months.
Results:
In total, 151 persons (81 adolescents and 70 adults; 44 families) were randomly assigned. At 12 months, significant improvement occurred in Healthy Eating Index scores for adults in the intervention group compared with controls (change, +8.6 vs −4.4; P < .01) and persisted at 24 months (+7.4 from baseline; P < .01). No differences were observed for adolescents and no significant differences occurred between groups for physical activity.
Conclusion:
This intervention produced sustained dietary quality improvement among adults but not among adolescents. Program outcomes are relevant to communities working to decrease cardiovascular risk among immigrant populations.
Keywords
Purpose
Immigrants and their descendants will make up the majority of US population growth in the coming decades. 1 Across many studies that have included a range of health measures, immigrants and refugees arrive to the United States healthier than the general population. 2 However, residency in North America is associated with accumulation of cardiovascular risk, including increasing rates of obesity, 3,4 hyperlipidemia, 5 hypertension, 6 diabetes mellitus, 7 and cardiovascular disease. 8,9 Furthermore, children of immigrants living in the United States may be at higher risk of obesity and its associated complications than persons who arrive to the country as adults.
Unhealthy dietary behaviors and low levels of physical activity are associated with each aforementioned risk factor. 10 –12 Populations that immigrate to high-income nations generally have less healthy behaviors than the nonimmigrant majority populations. 13 –16 Despite calls for intervention to address nutrition and physical activity among immigrant populations, 17 –19 few interventions have been reported. Systematic reviews published in 2010 20 and 2013 21 identified only 8 studies targeting dietary quality or obesity in immigrant populations; results from these studies suggest that tailored interventions may result in more success than general interventions applied to an immigrant population.
One barrier to designing healthy eating and physical activity interventions is that factors contributing to suboptimal behaviors among immigrant groups are multiple, complex, and not well understood. 22,23 The identified factors include disproportionate social, economic, and environmental vulnerabilities that are compounded by the heterogeneous impacts of acculturation, low health literacy, and other migration-specific effects on health. 24 Community-based participatory research is an intervention approach designed to collaboratively investigate health topics, in which community members and academic professionals partner in an equitable relationship through all research phases. 25 –27 Community-based participatory research has been effective in addressing health topics among immigrant and refugee populations. 28 –35 Although studies are underway, 36,37 no results have been published on interventions of nutrition or physical activity, or both, for immigrant populations resulting from a community-based participatory research approach.
The Healthy Immigrant Families (HIF) study is a product of Rochester Healthy Community Partnership (RHCP), a community-based participatory research (CBPR) partnership with a mission “to promote health and well-being among the city population through community-based participatory research, education, and civic engagement to achieve good health for all.” 38 Since its inception in 2004, RHCP effectively has designed and implemented several interventions with immigrant and refugee populations. 28,39 Community and academic partners have conducted every aspect of research together.
The purpose of HIF was to leverage the experience of this CBPR partnership 40 to cocreate and evaluate a socioculturally appropriate intervention to enhance dietary quality and improve physical activity with and for immigrant and refugee families living in the Midwest city. Social cognitive theory 41 formed the conceptual base of intervention development. The theory acknowledges the interaction between individual factors (eg, self-efficacy to eat a healthful diet) and social environmental factors (eg, social support) on behavior change. Low self-efficacy is an important barrier to eating a healthful diet 42 and to being physically active. 43 Furthermore, a socially supportive family environment has important positive influence on health behaviors among families of low socioeconomic position. 44
We have previously reported the results of formative research to inform intervention development. 45 –47 We have previously detailed the accounts of participatory recruitment processes, 48 study methods, 49 baseline measurements, 49 association of distress with health behaviors, 50 and training of interventionists 51 for the trial. In this study, we report the results of the HIF study.
Methods
The study design was a randomized controlled trial with families as the unit of randomization and a delayed intervention control group. The assessments were done at baseline and at 6, 12, and 24 months after intervention initiation (Figure 1). The respective institutional review board and the public school district approved the trial on behalf of community partners. The trial is registered at ClinicalTrials.gov NCT01952808.
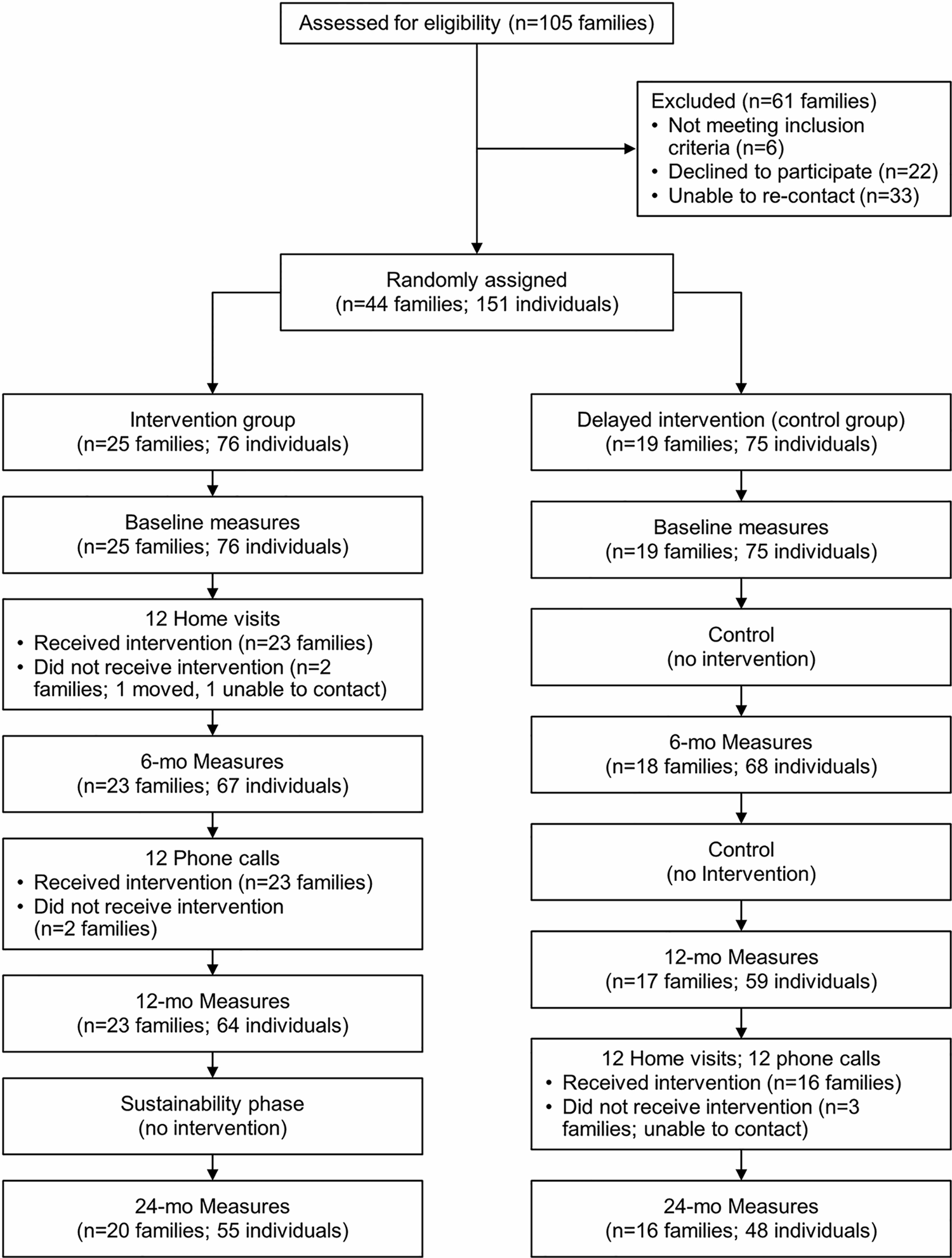
Flowchart of Healthy Immigrant Families study overview.
Study Setting and Participants
Participants were recruited by RHCP partners from the Hispanic, Somali, and Sudanese communities in the Midwest city. These partners completed RHCP-developed human subjects protection training 52 before recruitment, which was accomplished through in-person contact and word of mouth with adult members of households throughout the community. Partners identified families who may meet eligibility criteria, explained the study, and gauged interest in participation. Partners obtained permission from an adult family member of an interested household (man or woman) to forward their contact information to a study staff member. A language-congruent study staff member then called the family and performed telephone screening. Eligible families (all adult and adolescent members) were invited to a study event at a community partner location, where full eligibility screening and informed consent were conducted. Additional details of the community-led recruitment processes for this trial are described elsewhere. 48
Because this was a family-based intervention, eligibility criteria were available for both families and individuals. Eligibility criteria for families were a household with at least 1 adult and at least 1 adolescent aged 10 to 18 years (ie, no less than 2 participants per family). Adolescents were targeted instead of younger children on the basis of perceived need in the community and the enhanced rigor of assessment tools for the primary outcomes among adolescents compared with younger children. Inclusion criteria for individual participants (adults and adolescents) included (1) not planning to move from the area for the next 2 years, (2) willing and able to participate in all study aspects, and (3) able to provide oral informed consent or assent. The 4 individual exclusion criteria were self-reported pregnancy, self-reported insulin-dependent diabetes mellitus, self-reported diagnosis of cancer within the past 3 years, and a “yes” answer to the question “Do you know of any reason why you should not do physical activity?”
Randomization and Blinding
Each participant completed consent, enrollment, randomization, and baseline measurements at a community setting from February through March 2014. Randomization of family clusters (stratified as Hispanic, Somali, or Sudanese community) was achieved using software that allocated participants to either an early or delayed intervention group. Randomization status was revealed to participants and research staff only after completion of baseline measurements. Intervention group assignments could not be masked to interventionists and participants because of the logistical need for coordination among families. However, group assignments were masked to data managers and analysts throughout the study.
Intervention
The HIF work groups with community and academic membership developed the intervention framework and content over 2 years. Details of participatory intervention development and implementation of this trial are described elsewhere. 49 The study team of community and academic partners created an intervention manual with 12 content modules: 6 for healthful eating (increasing fruit and vegetable consumption, healthful beverages, reducing dietary fats, healthful snacks, portion control, and smart shopping strategies), 4 to address physical activity (increasing physical activity, muscle strength, and flexibility, reducing screening time, and overcoming barriers to physical activity), and 2 to synthesize and reinforce the content (exercise/food/work–life balance and celebrating accomplishments). Physical activity content was adapted from Active Living Every Day, 53 an evidence-based guide to incorporating more physical activity into busy lifestyles, and from the LEARN Program for Weight Management. 54 Nutrition content was partially adapted from the Simply Good Eating for English Language Learners 55 curriculum for immigrants and refugee families with low English language literacy. Newsletters were written to underscore the central messages of each module and to incorporate success stories from community members.
Language-congruent family health promoters were trained to deliver the intervention to participants within a participant’s respective community. A working group of multidisciplinary health professionals derived the family health promoter training curriculum, which included the following constructs: community-based participatory research partnership orientation, HIF project orientation, protecting human research participant training, principles of community-based participatory research, social cognitive theory–based behavior change principles, motivational interviewing principles, family-focused communication, physical activity principles, nutrition principles, mastery of intervention guide content, and training on the intervention delivery. Approximately 250 hours of training were conducted with each family health promoter, which included practicing all of the modules with families and role-playing, including a combined 64 sessions under direct observation. 51
The family health promoters delivered the intervention through 12 home visits (30-90 minutes each) over 6 months, followed by phone calls every 2 weeks (up to 12 calls total) during the next 6 months. At each visit, family health promoters assessed content knowledge and current behaviors related to each module topic, delivered the information, engaged in an interactive activity (eg, working with food models), discussed barriers and potential solutions with the family, and engaged in individual (with each participating adult and adolescent) and family goal setting. Family health promoters included counseling strategies consistent with social cognitive therapy, including role modeling, feedback, reinforcement, and social support to enrich self-efficacy and behavior change. Furthermore, family health promoters modeled healthful behaviors with the families. An important aspect of this intervention involved family health promoters working with participants to adapt solutions for each family.
Following the completion of home visits, family health promoters began biweekly 15-minute telephone calls to each family (up to 12 calls within 6 months). During these calls with an adult family member, family health promoters obtained a verbal progress report regarding the family’s diet and physical activity relative to their stated goals. They ended each call with a content summary related to 1 of 12 modules.
Treatment Adherence
A content module was considered to be successfully delivered if it were provided to at least 1 participating adult and 1 adolescent family member. Participants were categorized as receiving adequate intervention dose after they received at least 9 of 12 home visits and 9 of 12 phone calls (75% each). A telephone call was counted toward the total if completed by 1 adult participating family member.
Measures
Primary outcomes
Dietary quality was assessed by a single 24-hour dietary recall collected from each participant through the Automated Self-Administered 24-hour (ASA24) recall system, a National Cancer Institute web-based tool. 56 Respondents were guided through the recall interview with a modified version of the US Department of Agriculture (USDA) Automated Multiple-Pass Method. This tool performs well relative to true dietary intake and traditional interviewer-administered dietary recalls. 57,58 The ASA24-Kids system was used for adolescent participants. Recalls were supervised by study staff trained in use of the instrument, including a registered dietician. The tool was available in English and Spanish. Study staff and interpreters completed the recall with participants who spoke other languages. Many ethnic foods are included in the tool, and language-congruent study team members who were experienced with the tool assisted participants with food substitutions when needed. Automated Self-Administered 24-hour data files produced nutrient estimates for each participant based on the USDA Food and Nutrient Database for Dietary Studies, from which we calculated the Healthy Eating Index-2010, as well as intake of fruits, vegetables, and sugar. The Healthy Eating Index, derived directly from the ASA24, is a valid and reliable measure of overall diet quality according to the 2010 Dietary Guidelines for Americans. 59 The Healthy Eating Index is reported on a linear scale of 0 to 100, where a higher score reflects a more healthful diet.
Physical activity was measured for each participant with the Kinetic Activity Monitor accelerometer (Kersh Health, Plano, TX). 60,61 Participants were instructed to wear the accelerometer at the waist for 14 consecutive days while awake. No feedback was provided to participants from the accelerometer. An assessment was considered valid when participants wore the accelerometer at least 12 hours per day for 5 days. The data collected included sedentary time, as well as time spent performing mild, moderate, and vigorous physical activity.
Secondary outcomes
Weight was measured to the nearest 0.1 kg with a single digital floor scale (model 876; Seca, Hamburg, Germany) and height to the nearest 0.1 cm with a single stadiometer (model 213; Seca). Overweight was a body mass index (BMI) of 25.0 to 29.9 kg/m2 for adults and in the 85.0 to 94.9 percentile for adolescents; obesity was a BMI of 30.0 kg/m2 or greater for adults and in the 95.0 percentile for adolescents. 62,63 Waist circumference was measured twice to the nearest 0.1 cm with a tape measure at the narrowest part of the torso between the ribs and the iliac crest after removing excess clothing and smoothing the remaining clothes. A third measurement was taken when the difference between the 2 measures exceeded 2.0 cm; the average of the 2 closest measurements was used in the analysis. Systolic and diastolic blood pressures were measured using a mechanical device on the right arm after each participant sat quietly for 5 minutes. 64 The average of 2 blood pressure readings (1 minute apart) was used for analysis. Health-related quality of life was measured by single-item linear analog scale assessments of physical and emotional health. 65
Treatment fidelity
To document fidelity of intervention delivery, family health promoters electronically recorded assessments immediately after each encounter with a family (module delivery and telephone call) using a checklist of key delivery points for each module and call. Protocol deviations were also recorded. These assessments were reviewed by study team members throughout the intervention interval, and difficult scenarios were incorporated into regular directly observed role-playing sessions that continued throughout the intervention. Additional details of treatment fidelity assessment among family health promoters for this study have been described elsewhere. 51
Sample Size Considerations
Preliminary data indicated that a moderate effect size could be detected in the outcome variables, 40 where a moderate effect size is defined as a half standard deviation (SD) difference between groups. 66 The study had power to detect at least a moderate effect size for the primary outcomes of dietary quality and physical activity between the 2 groups. A sample of 64 persons per group (128 persons in total) provided 80% power for a 2-sample t test to detect differences in the mean changes from baseline of 50% times the SD of dietary improvement or physical activity with a 2-sided alternative and a 5% type I error rate. Additional persons were accrued to account for cancellation, protocol violations, and incomplete cases.
Analysis
Primary analyses of dietary and physical activity data were compared between groups with a single 2-sample, 2-sided t test and 5% type I error rate. The supplementary analysis of primary outcomes included repeated-measures analysis of variance modeling to assess the effect of baseline measures and clustering on subsequent values. We used the individual person as the analysis unit because of the impractically large sample size that would have been required for use of a family as the unit. Therefore, we adjusted for the clustering nature of our sample by including the family as an effect. Analyses of secondary outcomes were conducted either with 2-sample t tests supplemented by mixed-effects modeling when the studied variable was continuous in nature or with Fisher exact test comparing relative incidence rates of each outcome supplemented by logistic regression to assess the effect of covariates on univariate results, with the family as an effect in the model. We performed additional subgroup analysis to evaluate outcomes separately for adults and adolescents. Missing data were managed with simple imputation methods, including last, minimum, average, or maximum value carried forward, followed by multiple imputation methods to assess the robustness of study results when data were missing. All analyses were performed using statistical software (SAS version 9.3; SAS Institute Inc).
Results
Participants
Target enrollment was achieved with 151 persons (81 adolescents and 70 adults) from 44 families undergoing randomization. Of these, 25 families (76 persons) were in the early intervention group and 19 families (75 persons) were in the delayed intervention (control) group. No significant demographic differences or baseline differences were found between the 2 groups for any primary or secondary outcome measure, with the exception of more Hispanic adolescents in the early intervention group (23 in the early intervention group vs 15 in the delayed intervention group; P = .04). 49 Baseline characteristics of the study population are shown in Table 1.
Baseline Characteristics of the Healthy Immigrant Families Study Population of 151 Persons.
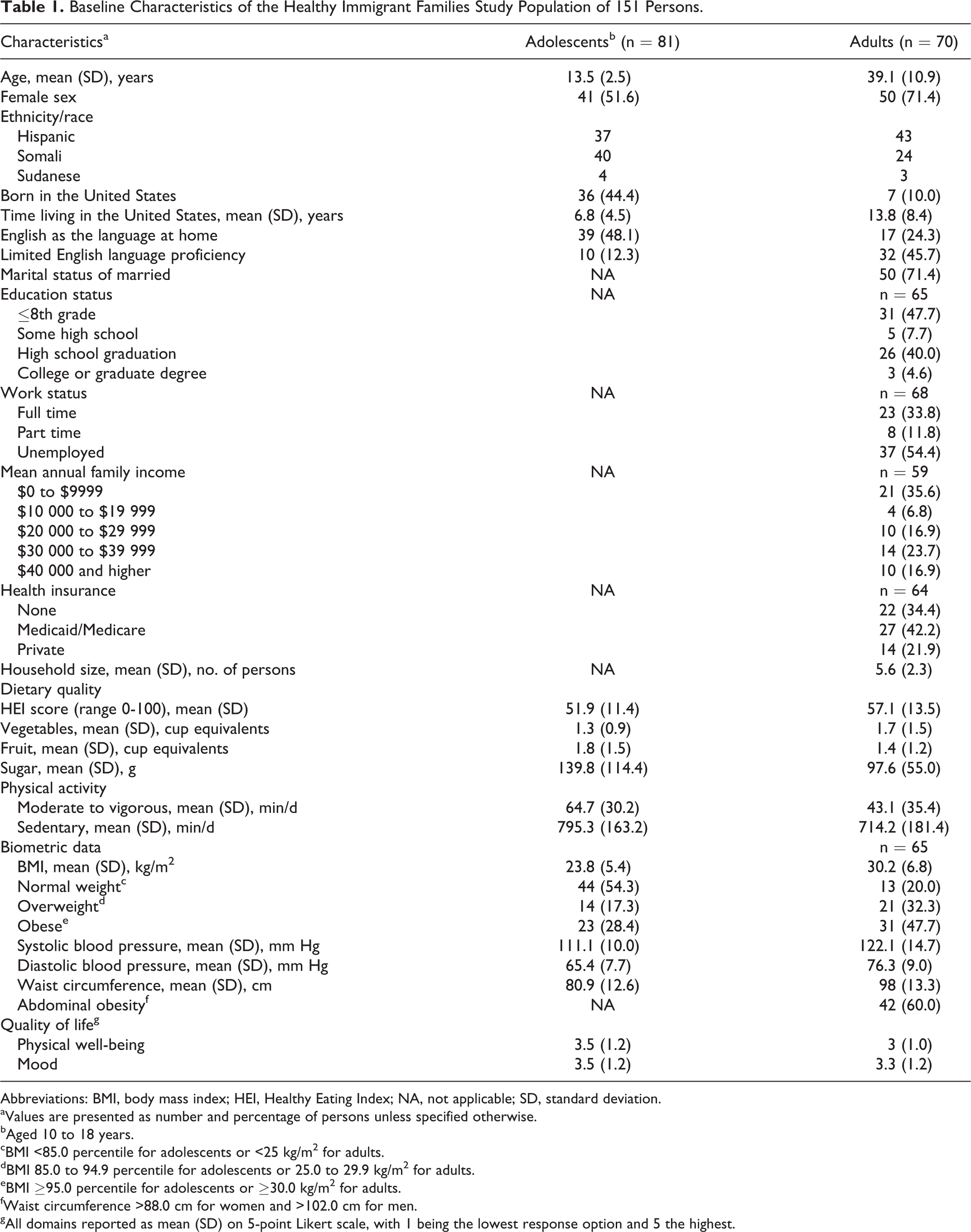
Abbreviations: BMI, body mass index; HEI, Healthy Eating Index; NA, not applicable; SD, standard deviation.
aValues are presented as number and percentage of persons unless specified otherwise.
bAged 10 to 18 years.
cBMI <85.0 percentile for adolescents or <25 kg/m2 for adults.
dBMI 85.0 to 94.9 percentile for adolescents or 25.0 to 29.9 kg/m2 for adults.
eBMI ≥95.0 percentile for adolescents or ≥30.0 kg/m2 for adults.
fWaist circumference >88.0 cm for women and >102.0 cm for men.
gAll domains reported as mean (SD) on 5-point Likert scale, with 1 being the lowest response option and 5 the highest.
Of the 25 families allocated to the early intervention arm, 23 (92%) received the intervention (2 families were lost to follow-up before intervention initiation). Of the initial 151 persons, loss to follow-up was 16 (11%) at 6 months, 28 (19%) at 12 months (the primary end point), and 48 (32%) at 24 months (Figure 1). The family health promoters completed documentation for 294 (98%) of the 301 sessions. Visits lasted a mean (SD) period of 50.7 (12.2) minutes (range, 20-90 minutes). For treatment adherence, 100% of the participating families met the predefined criteria for treatment adherence, and every family had at least 1 individual receiving the entire intervention (12 visits). Most visits included at least 1 adult (91%) and 1 adolescent (88%). The mean treatment fidelity related to intervention delivery was between 82% and 89% for each domain. 51
For all data reported, we found no statistically significant differences between the 3 racial/ethnic groups. Therefore, all data are reported in aggregate.
Dietary Quality
At baseline, moderate dietary quality was demonstrated with the Healthy Eating Index. Mean (SD) scores were 57.1 (13.5) for adults and 51.9 (11.4) for adolescents (Table 1). At 12 months, a significant improvement was seen in the Healthy Eating Index score for adults in the intervention group compared with controls (change of +8.6 vs −4.4, P < .01) that persisted at 24 months (+7.4 from baseline, P < .01). This change was mediated by statistically significant improvements in the so-called empty calories (reduction in calories from solid fats, alcoholic beverages, and added sugars; P < .05), increased greens and beans (P ≤ .005), and decreased refined carbohydrates (P < .05), as well as nonsignificant increases in overall intake of fruits and vegetables at 12 months. Similarly, 47% of adults achieved the goal of no sugar-sweetened beverages (eg, regular soda, sports drink, fruit drink) at 12 months, compared with 10% of controls (P < .005; Table 2).
Healthy Immigrant Families Study Outcomes.
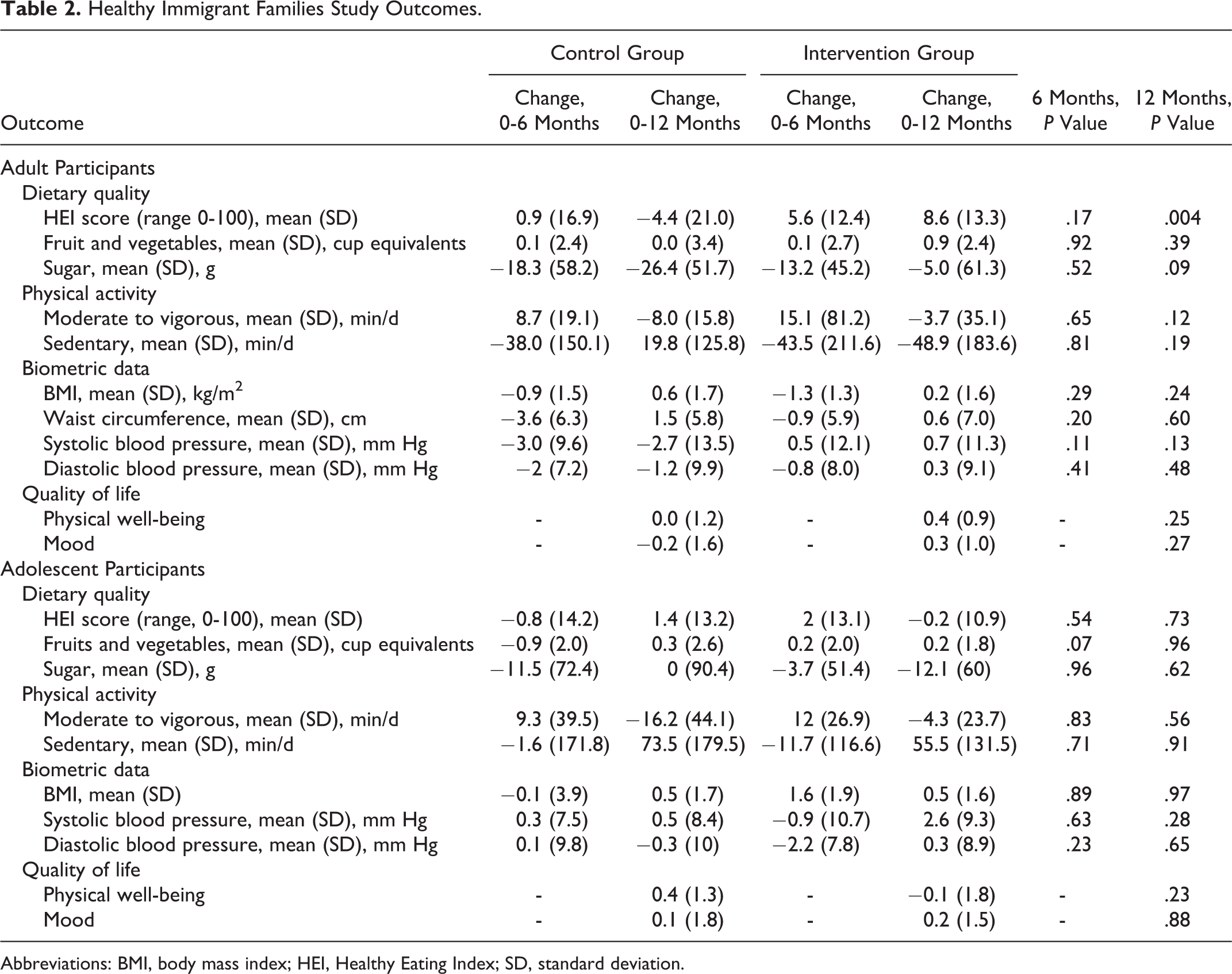
Abbreviations: BMI, body mass index; HEI, Healthy Eating Index; SD, standard deviation.
Finally, improvement in Healthy Eating Index score for adults was replicated in the delayed intervention group at 12 months (+9.8 from baseline, P ≤ .01; Table 3). Adolescents had nonsignificant improvements in the Healthy Eating Index score, fruit and vegetable consumption, and sugar intake at 6 months in the intervention group compared with controls (Table 2). However, these findings were not sustained at 12 months.
Results of 24-Month Measures for Healthy Immigrant Families, Adult Participants.
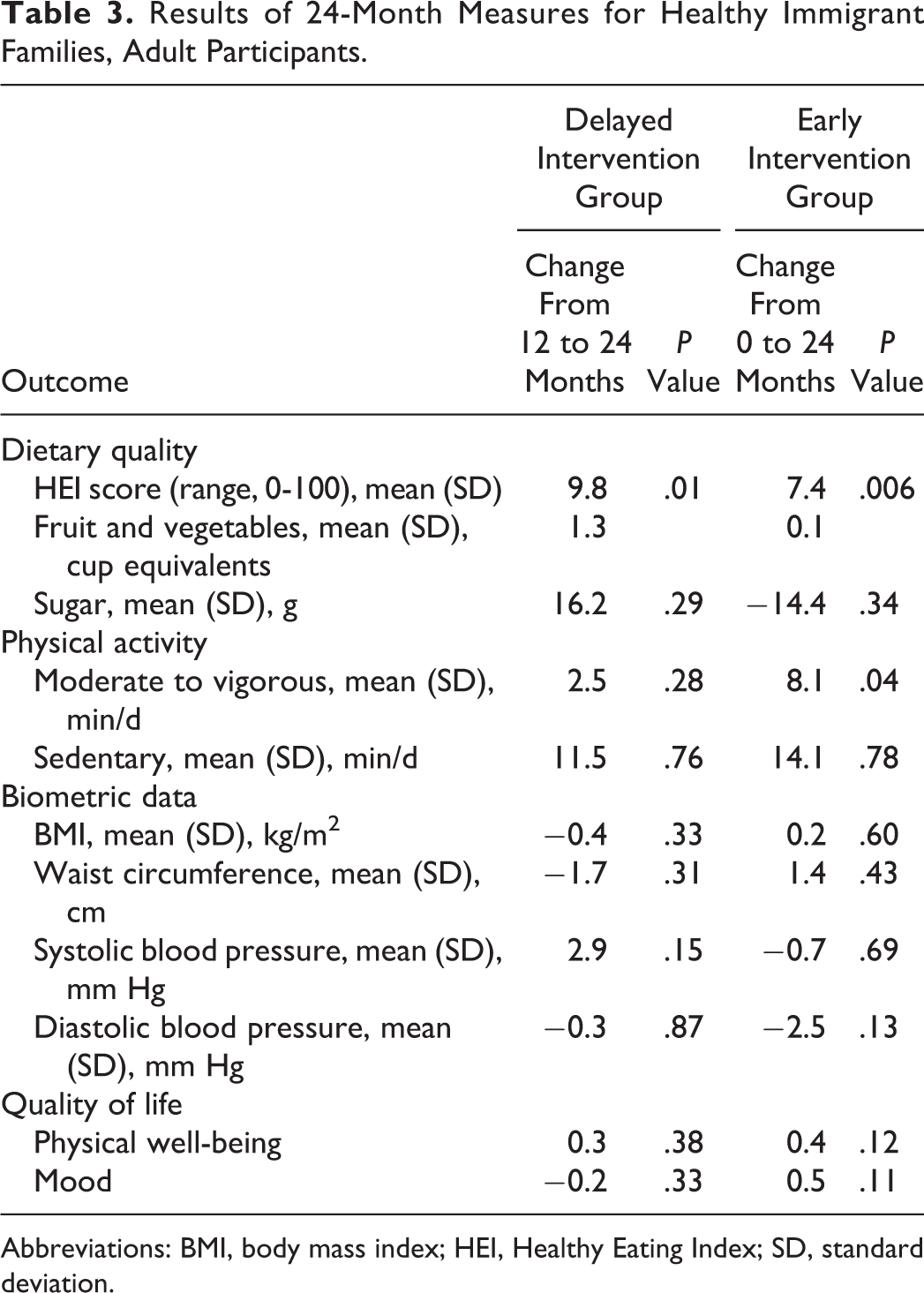
Abbreviations: BMI, body mass index; HEI, Healthy Eating Index; SD, standard deviation.
Physical Activity
At baseline, data from accelerometers were collected for 148 (98%) participants. Accelerometers were worn for a mean (SD) time of 11.9 (4.8) hours per day for 11.4 (6.4) days, and the predetermined threshold for valid data was achieved by 117 (77%) participants. Baseline physical activity values were relatively high; mean (SD) time spent per day in moderate to vigorous physical activity was 64.7 (30.2) minutes for adolescents and 43.1 (35.4) minutes for adults (Table 1).
No statistically significant differences were seen at 6 and 12 months between the intervention group and controls for moderate to vigorous physical activity or sedentary time among adults or adolescents (Table 2). Nonsignificant trends toward improvements in physical activity measures were found for adults and adolescents compared with controls at 6 months, but these findings were not sustained at 12 months.
Secondary Outcome Measures
Baseline biometric measurements showed that 37 (45.7%) adolescents and 52 (80.0%) adults were overweight or obese (Table 1). At 6 and 12 months, no significant differences were found in BMI, waist circumference, or blood pressure in the intervention group compared to the control group overall or for participants who were overweight or obese at baseline (Table 2).
For quality-of-life measures, nonsignificant trends toward improvement in physical well-being and mood were found among adults at 12 months in the intervention group compared with controls and were sustained at 24 months (Tables 2 and 3). Adolescents showed no significant changes in either of these domains following the intervention (Table 2).
Discussion
In this intervention of healthful eating and physical activity derived through a community-based participatory research approach with and for immigrant families, intervention participants had sustained improvements in dietary quality among adults but not among adolescents. No significant improvements occurred in physical activity level among adults or adolescents. A key finding is the high rate of intervention adherence and study retention among participating families, demonstrating the feasibility of conducting a randomized controlled trial in these immigrant communities. Other strengths are high intervention fidelity among family health promoters and community leadership through every study phase, which highlights the fact that rigorous study procedures can be sustained by incorporating participatory approaches in research. This trial is among the first reported community-based interventions to use a community-based participatory research approach to address decreases in dietary quality and physical activity in populations after immigration to the United States.
Among adults in the intervention group, dietary quality improved in a substantive and consistent manner at 12 months compared with controls, and the improvement was sustained through the 24-month measures—a finding replicated in the delayed intervention control group. This change was mediated by improvements in intake of empty calories, of fruits and vegetables, and of refined carbohydrates. This clinically significant behavior change reflects the content of the intervention modules and the goals established by most of the families.
Physical activity is associated with positive physical and mental health; thus, we find it disappointing that the intervention did not improve physical activity levels. In looking to explain this lack of effect, we found that in contrast to seeking to improve their dietary quality, most participating families and individuals in this study did not cite improvement in physical activity as a goal. In addition, baseline objective levels of physical activity were high, 49 creating a potential ceiling effect. These baseline findings are similar to data among racial/ethnic minority groups in the United States, in which the physical activity level objectively measured with an accelerometer is higher than physical activity levels in the general population. 67,68 These 2 factors—physical activity improvements as lower priorities for participating families and high baseline objective levels of physical activity—likely accounted for the lack of improvement in physical activity in this study.
Obesity is an important health problem among immigrant populations, and 80% of adults in the present study were overweight or obese at baseline. The difference in BMI reduction between intervention adults and control adults did not achieve statistical significance. However, the relatively large effect at 6 months suggests a possibility of clinically meaningful reduction in BMI among adults as a result of the intervention that was not sustained at 12 or 24 months. Although this study was not intended as a weight loss intervention, future research is warranted to test the addition of dietary weight loss principles (eg, calorie restriction, tracking daily intake, planning meals, managing urges for overeating) to the existing intervention modules to promote weight loss and weight loss maintenance among immigrants who are overweight or obese. Past research findings suggest that these interventions may be most successful when they are implemented within 10 years of immigration to the United States. 3
For adolescents in the early intervention arm, no improvement was seen for either primary outcome. This result may reflect factors of intervention dose and implementation audience strategy. Delivery of each module required participation of at least 1 adult and 1 adolescent. Although treatment fidelity related to delivery of the intervention was high, most participating families included more than 1 adolescent, such that individual participation in modules was inconsistent for the specific study adolescents compared with the enrolled study adults. 51 Family health promoters reported difficulties with adolescents being unable to participate in counseling sessions because of after-school activities. For this reason, the modules tended to be delivered for the more engaged adult audience members. Furthermore, analysis of baseline data showed a positive association between mood and healthful behaviors, 50 suggesting that mood management strategies should be included as a component of future interventions with adolescent participants. Future development of family-based interventions among these immigrant populations will require more intentional engagement of adolescents during the planning and implementation phases.
Limitations
The study has several important limitations. Although the randomized study design was optimal, a risk existed of indirect intervention dissemination to the control group through social networks among these immigrant communities in a single small city, a phenomena common to behavior change interventions. 69 The observed improvements in several variables among the control group, despite no significant improvement in secular trends, suggest that intervention diffusion to the control group occurred in this study. For logistical reasons in this community-based study, only a single 24-hour dietary recall measure was obtained for each participant at every measurement point. Therefore, only group-level changes can be inferred from these data. For practical reasons, individuals were used as the unit of analysis, even though families were used as the unit of randomization. These individuals may not represent the results of the entire family, and results for individuals within the same family may be correlated. Although the analyses were adjusted for a family effect, the study results would have been more robust with a larger sample size, thereby allowing the use of families as the unit of analysis. Finally, although treatment conditions were masked to the investigators and data analysts, it was not practical to maintain blinding for the interventionists (family health promoters) with direct participant contact.
Significance
Healthy Immigrant Families is a multicomponent intervention, cocreated by community and academic partners, which resulted in the successful enrollment and study completion of adult and adolescent immigrants and produced sustained improvement in dietary quality among adults, but not among adolescents, in this Midwest city. It was feasible to conduct a randomized controlled trial in the participating immigrant groups, indicating substantial community support for this approach. Program outcomes are relevant to other communities working to reduce the accumulation of cardiovascular health risk among these adult and adolescent immigrant populations.
So What? Implications for Health Promotion Practitioners and Researchers
What is already known on this topic?
Immigrants to the United States often have escalating cardiovascular risk after arrival. Barriers to healthy eating and physical activity are important contributors to this risk.
What does this article add?
This multicomponent intervention, cocreated by community and academic partners, resulted in the successful enrollment and study completion of adult and adolescent immigrants and produced sustained improvement in dietary quality among adults but not among adolescents.
What are the implications for health promotion practice or research?
Outcomes are relevant to other communities working to reduce the accumulation of cardiovascular health risk among these adult and adolescent immigrant populations.
Footnotes
Authors’ Note
J. A. Levine provides advice to Kersh Health, inventor of the accelerometer used in this study. The contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH. The funding bodies played no role in study design, in the collection, analysis, and interpretation of data, writing of the manuscript, and in the decision to submit the manuscript for publication.
Acknowledgments
The authors thank the RHCP partners who contributed to the organization, implementation, and dissemination of this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by National Institutes of Health (NIH) grant no R01 HL 111407 from the National Heart, Lung, and Blood Institute, by National Center for Advancing Translational Science grant no UL1 TR000135, and by the Mayo Clinic Office of Health Disparities Research.