
Abstract
Purpose:
To examine associations of adolescent sugar-sweetened beverage (SSB) intake with parent SSB intake and parent and adolescent attitudes about limiting SSB and junk food (SSB/JF) intake.
Design:
Quantitative, cross-sectional study.
Setting:
The 2014 Family Life, Activity, Sun, Health, and Eating study.
Sample:
Parent–adolescent dyads (N = 1555).
Measures:
The outcome was adolescent SSB intake. Exposure variables were parent SSB intake, sociodemographics, and parent and adolescent attitudes about SSB/JF intake (responses: agree, neither, or disagree).
Analysis:
Multinomial logistic regressions estimated adjusted odds ratios (aOR) and 95% confidence intervals (CIs).
Results:
Half (49.5%) of adolescents and 33.7% of parents consumed SSB ≥1 time/day. Parent daily SSB intake was associated with adolescent daily SSB intake (aOR = 8.9; CI = 4.6-17.3) [referent: no consumption]. Adolescents who disagreed on having confidence to limit SSB/JF intake had higher odds of daily SSB intake (aOR = 3.5; CI = 1.8-6.8), as did those who disagreed they felt bad about themselves if they did not limit SSB/JF intake (aOR = 1.9; CI=1.1-3.3), compared to adolescents who agreed with these attitudes. No parental attitudes were significant.
Conclusion:
Higher odds of daily SSB intake among adolescents was associated with parent SSB intake and adolescent attitudes about confidence in, and feeling bad about, limiting SSB/JF intake. Parent attitudes were not associated with daily adolescent SSB intake. Efforts to reduce adolescent SSB intake could consider strategies geared toward improving adolescent attitudes and dietary behaviors and parental SSB intake.
Purpose
Frequent intake of sugar-sweetened beverages (SSB), drinks sweetened with added sugars, is associated with adverse health consequences in children including obesity, insulin resistance, and dental caries. 1 Compared to other youth age-groups, adolescents aged 12 to 19 years have the highest SSB intake. 2 Behavior change interventions may significantly reduce adolescent SSB intake. 3 Understanding factors associated with SSB intake is important to develop and implement interventions to decrease adolescent SSB intake.
Self-determination theory (SDT) explores motivational mechanisms of health behaviors and could help design such interventions. A component of SDT is the motivational continuum, which ranges from controlled (motivated by primarily external factors) to autonomous (motivated primarily by internal factors of personal choice, interest, or values). 4,5 Among adolescents, autonomous motivation has been associated with determinants of obesity, including predicting fruits and vegetables intake. 6 Compared to younger children, adolescents often have more autonomy over food and drink choices but might still be influenced by parent attitudes or behaviors. 7 There is a growing body of literature about how adolescent autonomous motivation and attitudes, and parent attitudes, affect adolescent SSB intake. 8 -10 For example, perception of high behavioral control among adolescents and their parents has been associated with decreased SSB consumption. 9,10 This study simultaneously examined associations of adolescent SSB intake with parent SSB intake within adolescent–parent dyads, as well as adolescent SSB intake, filling a gap in the adolescent–parent dyad literature specific to dietary patterns.
Methods
Design and Sample
This cross-sectional study used data from parent–adolescent dyads in the 2014 Family Life, Activity, Sun, Health, and Eating (FLASHE) study. The FLASHE study assessed physical activity and diet behaviors among a national sample of adolescent children (aged 12-17 years) and their parents. 11 The FLASHE study was reviewed and approved by National Cancer Institute’s special studies institutional review board and the US Government’s Office of Management and Budget. Of the 5027 dyads invited to participate using balanced sampling from the Ipsos Consumer Opinion Panel, 1945 enrolled, 1646 completed parent and adolescent diet online surveys, and 1555 met this study’s inclusion criteria of having adolescent SSB intake data.
Measures
The outcome variable was self-reported adolescent SSB intake during the past 7 days determined by 4 questions: “DURING THE PAST 7 DAYS, how many times did you drink:” (1) “SWEETENED FRUIT DRINKS and TEAS like Capri Sun, Sunny D, Arizona Tea, etc.? DON’T COUNT 100% pure fruit juice or artificially sweetened or diet drinks,” (2) “regular SODA or pop like Coke, Pepsi, Sprite, Dr. Pepper, etc.? DON’T COUNT diet or zero calorie,” (3) “ENERGY DRINKS like Rockstar, Red Bull, etc.? These drinks usually have caffeine,” and (4) “SPORTS DRINKS like Gatorade, Powerade, etc.? DON’T COUNT low-calorie sports drinks like G2, Powerade Zero, etc.” Not all possible SSBs were ascertained by these questions; for instance, sugar-sweetened coffee drinks were not specified. Response options were “I did not drink [SSB] in past week, 1-3 times in past week, 4-6 times in past week, 1 time/day, 2 times/day, and ≥3 times/day.” To calculate daily SSB intake, 1 to 3 times/week was changed to 0.3 times/day (2 times divided by 7 d/wk), 4 to 6 times/week changed to 0.7 times/day (5 times divided by 7 d/wk), and ≥3 times/day changed to 3 times/day. To calculate the frequency of total daily SSB intake, responses from the 4 questions were summed and categorized as 0, >0 to <1, or ≥1 time/day.
The main exposure variables were parent SSB intake (measured and defined in an identical manner as adolescents) and parent and adolescent attitudes/reasons for limiting SSB/junk food. Adolescents rated 2 statements, the first related to self-efficacy: “I feel confident in my ability to limit the amount of junk food and sugary drinks I eat and drink,” and the second related to social norm: “My friends eat junk food or sugary drinks on most days of the week.” Adolescents and parents both rated 4 reasons for limiting SSB/junk food intake, which were modified from the Treatment Self-Regulation Questionnaire (TSRQ). 12 These included responses to “I would try to limit how much junk food and sugary drinks I have because:” (1) “I would feel bad about myself if I didn’t”; (2) “I have thought about it and decided that I want to limit junk food and sugary drinks”; (3) “Others would be upset with me if I didn’t”; and (4) “It’s an important thing for me to do.” The attitudes represented in items 2 and 4 are on the autonomous motivation subscale of the TSRQ. Item 1 represents introjected regulation (ie, internally controlled but not self-determined), while item 3 indicates external regulation (environmentally controlled). Both concepts are components of SDT measured by the TSRQ. 12 All questions had 5 response options: strongly disagree, somewhat disagree, neither disagree nor agree, somewhat agree, or strongly agree; these were subsequently categorized as disagree, neither disagree nor agree, or agree.
Covariates included self-reported sex, age (12-14 and 15-17 years), race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanic, and other), weight status (underweight/normal weight, overweight, and obesity), parental education level (≤high school/GED, some college, ≥4 year college degree), and annual household income (<$100 000, ≥$100 000). For weight status, self-reported height and weight were used to calculate body mass index (weight [kg]/height [m2]).
Analysis
To determine differences across categories, χ2 tests were used (significant at P < .05). Separate multinomial logistic regression models were performed for each attitude variable to calculate adjusted odds ratios (aORs) and 95% confidence intervals (CIs) for adolescent SSB intake (>0 to <1 time/day and ≥1 time/day; reference: 0 times/day), controlling for parent and adolescent sociodemographics. Statistical analyses were performed in SAS version 9.4, using survey procedures and sample weights.
Results
Overall, 49.5% of adolescents reported consuming SSB ≥1 time/day. Adolescent and parent race/ethnicity and parent age were associated with adolescent SSB intake (Table 1). About 34% of parents consumed SSB ≥1 time/day (Table 2). Adolescent agreement with the 6 attitudes about limiting SSB/junk food ranged from a low of 41.6% who agreed others would be upset if they did not limit SSB/junk food intake, to a high of 79.6% who agreed it was important for them to limit SSB/junk food intake.
Characteristics of Study Participants and Adolescent Sugar-Sweetened Beverage (SSB) Intake During the Past 7 Days, Family Life, Activity, Sun, Health, and Eating (FLASHE) Study, 2014.
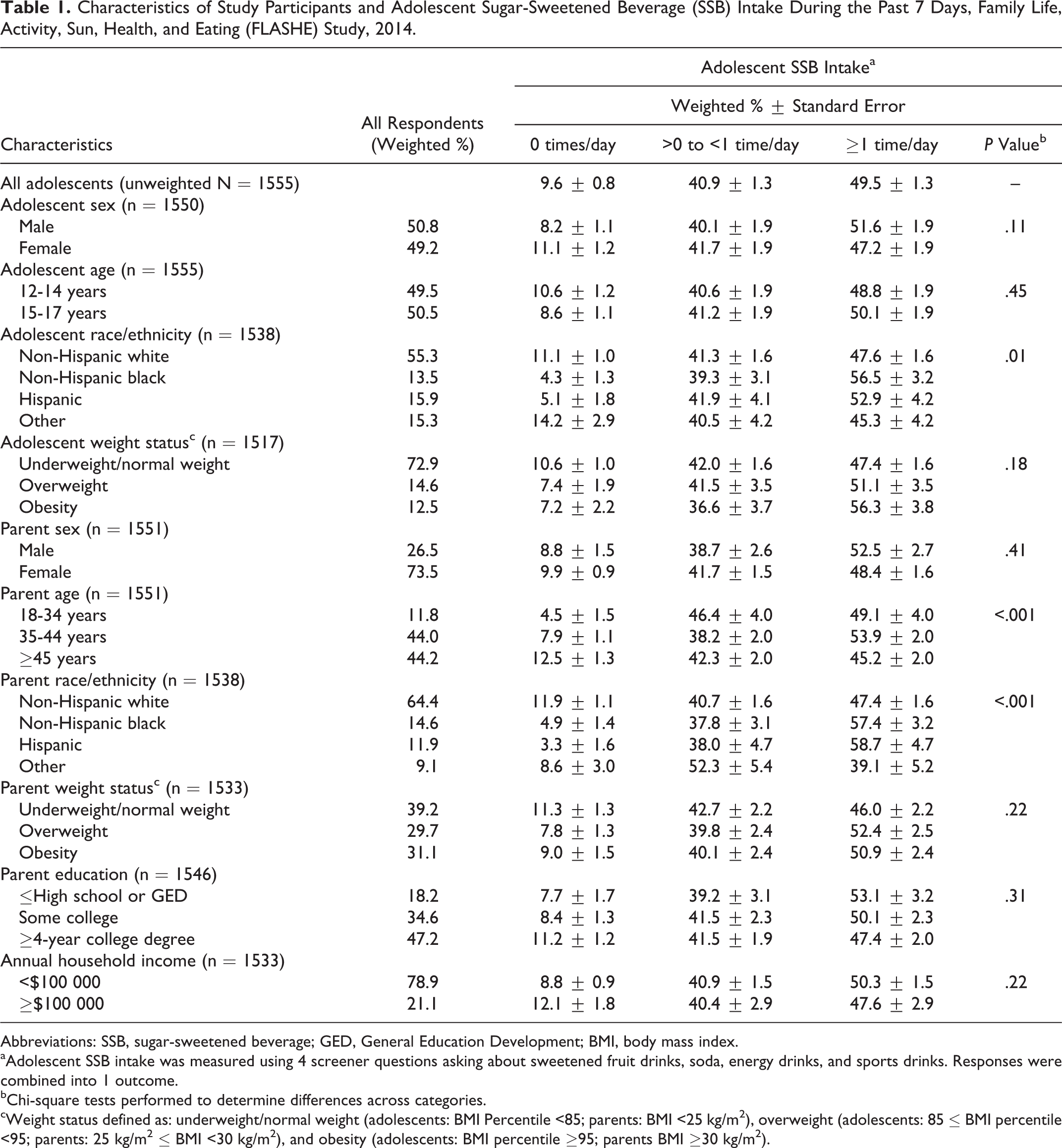
Abbreviations: SSB, sugar-sweetened beverage; GED, General Education Development; BMI, body mass index.
aAdolescent SSB intake was measured using 4 screener questions asking about sweetened fruit drinks, soda, energy drinks, and sports drinks. Responses were combined into 1 outcome.
bChi-square tests performed to determine differences across categories.
cWeight status defined as: underweight/normal weight (adolescents: BMI Percentile <85; parents: BMI <25 kg/m2), overweight (adolescents: 85 ≤ BMI percentile <95; parents: 25 kg/m2 ≤ BMI <30 kg/m2), and obesity (adolescents: BMI percentile ≥95; parents BMI ≥30 kg/m2).
Unadjusteda and Adjusted Analysis Between Adolescent Sugar-Sweetened Beverage (SSB) Intake During Past 7 Days, Parent SSB Intake, and Parent and Adolescent Attitudes About Limiting SSB Intake; Family Life, Activity, Sun, Health, and Eating (FLASHE) Study, 2014.
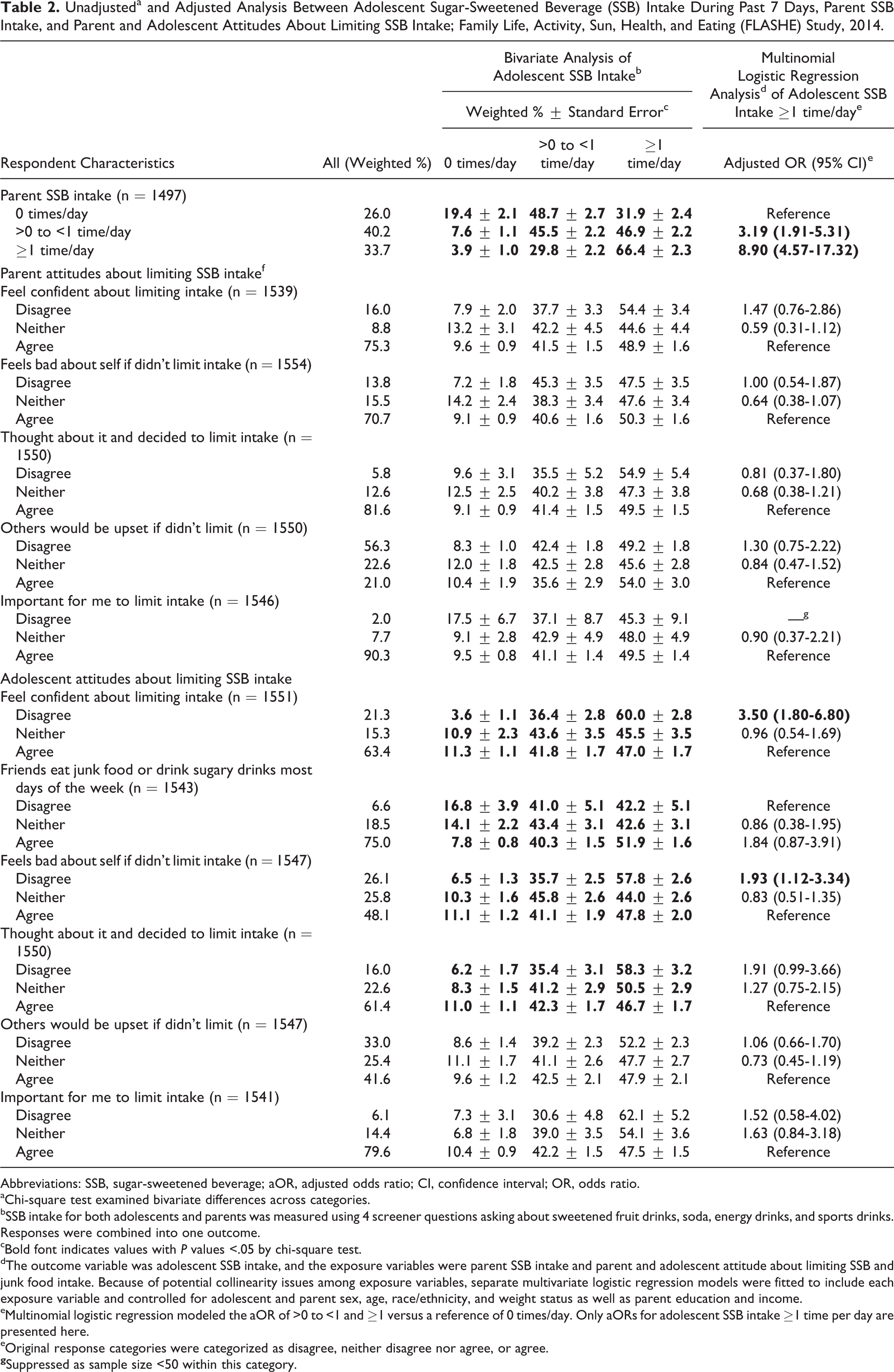
Abbreviations: SSB, sugar-sweetened beverage; aOR, adjusted odds ratio; CI, confidence interval; OR, odds ratio.
aChi-square test examined bivariate differences across categories.
bSSB intake for both adolescents and parents was measured using 4 screener questions asking about sweetened fruit drinks, soda, energy drinks, and sports drinks. Responses were combined into one outcome.
cBold font indicates values with P values <.05 by chi-square test.
dThe outcome variable was adolescent SSB intake, and the exposure variables were parent SSB intake and parent and adolescent attitude about limiting SSB and junk food intake. Because of potential collinearity issues among exposure variables, separate multivariate logistic regression models were fitted to include each exposure variable and controlled for adolescent and parent sex, age, race/ethnicity, and weight status as well as parent education and income.
eMultinomial logistic regression modeled the aOR of >0 to <1 and ≥1 versus a reference of 0 times/day. Only aORs for adolescent SSB intake ≥1 time per day are presented here.
eOriginal response categories were categorized as disagree, neither disagree nor agree, or agree.
In adjusted models, adolescent SSB intake ≥1 time/day was associated with parent SSB intake ≥1 time/day (aOR = 8.9; 95% CI = 4.6-17.3; vs nonconsumers). Higher odds of adolescent SSB intake ≥1 time/day were found for those who disagreed on feeling confident about limiting SSB/junk food intake (aOR = 3.5; 95% CI = 1.8-6.8) and for those who disagreed that they felt bad about themselves if they did not limit SSB/junk food intake (aOR = 1.9; 95% CI = 1.1-3.3), compared to adolescents who agreed with these attitudes. There were no significant associations with parental attitudes.
Discussion
In this study, daily adolescent SSB intake was associated with parent SSB intake and select adolescent attitudes regarding limiting SSB/junk food intake, but not parent attitudes. Parent daily SSB intake had the highest odds of adolescent daily SSB intake, consistent with a previous study. 13 Odds of adolescent SSB intake ≥1 time/day were higher among adolescents who disagree with feeling confident (a proxy for the SDT construct of self-efficacy) about limiting SSB/junk food intake and who disagree about feeling bad about themselves (reflecting introjected regulation) if SSB/junk food intake was not limited, compared to adolescents who agreed. Similar to our study findings, positive attitudes to decrease SSB intake have been significantly associated with decreasing SSB consumption among adolescents. 9 Another study also found that adolescent attitude was significantly associated with SSB consumption, although intention to limit SSB intake was a stronger predictor. 10 The association between daily parent SSB intake, although not parent attitudes, could be due to a mediating factor such as the presence of SSB at home. Parents may purchase SSB for the household where the adolescent lives. 14 Interventions to decrease adolescent SSB intake could focus on limiting parent intake and purchase of SSB. Given this predominantly female parent sample, similar to another study, 10 such interventions could focus on mothers. In a prior study, mothers influenced adolescent SSB intake more than fathers. 8
About two-thirds of adolescents agreed they felt confident (had self-efficacy) about their ability to limit SSB/junk food intake, and three quarters agreed with the perceived peer behavior that their friends consumed SSB/junk food most days of the week. Adolescent agreement with attitudes about limiting SSB/JF intake were highest among the 2 questionnaire items that are associated with autonomous motivation 12 : important for them to do (4 in 5 adolescents) and thought and decided to limit SSB/junk food intake (3 in 5 adolescents). However, less than half of adolescents agreed that they experienced introjected regulation about limiting SSB/junk food or agreed others would be upset if they did not limit SSB/junk food intake in the present study. The demonstration of autonomous motivation regarding limiting SSB/junk food intake and the associations of adolescent attitudes with adolescent SSB intake suggest that future behavioral interventions could be directed specifically toward adolescents’ attitudes—including improving self-efficacy to increase confidence—in limiting of SSB/junk food intake. Indeed, adolescent autonomous motivation has been associated with adolescent SSB consumption. 8 In one behavioral intervention, reported SSB intake decreased among adolescents after being provided information on SSB health risks, as well as a water bottle. 15 This could reflect self-determining attitudes within these adolescents.
This study is subject to limitations. Self-reported data were used, which may be subject to social desirability bias. In addition, FLASHE findings may not be generalizable throughout the population. Finally, SSB intake was reported by frequency instead of by volume. Despite these, results of this study provide an important contribution to the literature. This is the first study to our knowledge that both assesses the SSB intake of adolescents and their parents within dyads, as well as examines their attitudes and beliefs regarding limitation of SSB/junk food.
In conclusion, this study showed that adolescent SSB intake was significantly associated with parent intake and indicates that some adolescent attitudes regarding the limitation of SSB/junk food—but not parental attitudes—were associated with adolescent daily SSB intake. Given the strong association between daily adolescent and daily parent SSB intake, interventions that address parental SSB intake could be tested. Behavioral interventions that improve adolescent confidence in limiting SSB limiting intake, perhaps using SDT, could also be tested for decreasing adolescent SSB intake.
SO WHAT? Implications for Health Promotion Practitioners and Researchers
What is already known on this topic?
Prior studies have demonstrated an association between parental SSB intake and adolescent SSB intake.
What does this article add?
Daily parent SSB intake was associated with daily adolescent (12-17 years) SSB intake (aOR = 8.9; 95% CI = 4.6-17.3) [referent no consumption]. Additionally, adolescents who disagreed on feeling confident about limiting SSB/junk food intake had higher odds of SSB intake ≥1 time/day (aOR = 3.5; 95% CI = 1.8-6.8) as did those who disagreed that they felt bad about themselves if they did not limit SSB/junk food intake (aOR = 1.9; 95% CI = 1.1-3.3) compared to adolescents who agreed with these attitudes. However, parental attitudes were not associated with adolescent daily SSB intake.
What are the implications for health promotion practice or research?
Dietary interventions targeted toward adolescents limiting SSB intake could be developed to intervene on adolescent attitudes and practices. Given the strong association between daily adolescent and daily parent SSB intake, parental SSB intake could also targeted for change.
Footnotes
Authors’ Note
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Acknowledgments
We appreciate the contributions of Dr. Linda Nebeling to this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.