
Abstract
Purpose:
Previous DPP translations in African American women have been suboptimal. This trial evaluated a community-based participatory research developed faith-based diabetes prevention program (DPP) to improve weight loss in African American women.
Design:
This cluster randomized trial allocated churches to faith-based (FDPP) or standard (SDPP) DPP interventions. Setting. African American churches. Subjects. Eleven churches with 221 African American women (aged 48.8 ± 11.2 years, BMI = 36.7 ± 8.4) received the FDPP (n = 6) or SDPP (n = 5) intervention.
Intervention:
FDPP incorporated 5 faith-based components, including pastor involvement, into the standard DPP curriculum. The SDPP used the standard DPP curriculum. Lay health leaders facilitated interventions at church sites.
Measures:
Weight and biometrics were collected by blinded staff at baseline, 4- and 10-months.
Analysis:
A multilevel hierarchical regression model compared the FDPP and SDPP groups on outcomes.
Results:
FDPP and SDPP churches significantly lost weight at 10-months (overall −2.6%, p < .01). Women in FDPP churches who attended at least 15 sessions lost an additional 6.1 pounds at 4-months compared to SDPP corresponding to a 5.8% reduction at 10-months (p < .05). Both groups had significant improvements in health behaviors and biometrics.
Conclusions:
Faith-based and standard DPP interventions led by lay health leaders successfully improved weight, health behaviors, and chronic disease risk. However, the faith-based DPP when fully implemented met the CDC’s recommendation for weight loss for diabetes prevention in African American women.
Keywords
Purpose
There is a continued need to develop effective translational programs to reduce disparities related to obesity and chronic disease in African American women. 1 African American women have disproportionately higher rates of obesity, prediabetes, type 2 diabetes, and cardiovascular disease compared to White women. 2 Despite research, health care, and policy changes, health disparities continue to exist. 3 As shown in the Diabetes Prevention Program (DPP), improving diet, increasing physical activity, and modest weight reduction substantially improves chronic disease risk. 4 However, African American women tend to have less success than others in lifestyle interventions, 5 -9 and to date, DPP translations in African Americans have been suboptimal. 1
Interventions delivered in faith-based organizations (FBO), such as churches, have been a pillar of health promotion in the African American community for decades. 10 -12 Health promotion programs have integrated faith-based adaptions, such as prayer and scripture, which is considered “faith-based.” 13 Others implement secular programs in the FBO without faith-based adaptions, which is termed “faith-placed.” 14,15 Interestingly, a large review found that faith-placed programs have better weight loss outcomes than faith-based programs, 16 which is inconsistent with research indicating deep structural tailoring, such as faith, can improve outcomes. 17 Further, this review noted that due to heterogeneity across program components and methodological weaknesses, they were unable to directly compare the impact of faith-based versus faith-placed interventions on weight loss outcomes. Although many studies have evaluated faith adaptions to the DPP, 13,18 only 1 directly compared faith-based versus faith-placed approaches and findings were inconclusive. 19 Rigorous randomized trials are needed to determine which approach is more effective to guide DPP translations in African American communities.
Community-based participatory research (CBPR) is an approach to reduce health disparities used to develop faith-based weight loss interventions. 13,20 To date, there has been limited robust randomized trials using CBPR for weight loss. 11,21 Further, although pastors have significant influence and may empower individuals to change health behaviors, 12,22 -24 they have not been included in individual level health promotion program delivery likely due to time demands. 23 Pastor involvement in previous studies has consisted of promotion, encouragement, and discussion of health from the pulpit, commitment to changing a church health related policy, and participating in church level events, advisory boards, and recruitment. 13,19,25 -28 As agents of change, incorporating the pastor specifically in program implementation while considering time demands could strengthen outcomes of faith-based approaches. The Better Me Within (BMW) trial used CBPR to develop a faith-based curriculum and included pastors in program delivery as strategies to develop a more effective faith-based DPP adaption. 29
The primary aim of the BMW church-based randomized trial was to compare a faith-based tailored DPP (FDPP) to a non-tailored secular DPP (SDPP) in African American women who were overweight. This study hypothesized that women in the FDPP group would have greater weight loss and associated improvements in chronic disease than women in the SDPP group at 4 and 10-months follow-up.
Methods
Design
The BMW trial was a community-based prospective cluster randomized trial to evaluate a faith-based DPP (FDPP) compared to a standard DPP (SDPP) on reducing body weight and chronic disease risk. CBPR was used to design, implement and evaluate BMW in partnership with a Community Advisory Board (CAB) of local pastors and first ladies. The BMW CAB developed the faith-based adaptions with feedback from study staff. A total of 12 churches were selected from January 2014 to February 2016 in Dallas, TX and surrounding areas, and randomized to the SDPP or FDPP interventions using a random digit number table with a 1:1 ratio. Participants completed baseline measures, a 4-month intervention and post-intervention measurement, and an additional 6-month maintenance intervention followed by 10-month follow-up measures. Detailed information on the BMW trial has been reported previously. 29 The Institutional Review Board at The University of North Texas Health Science Center approved the study.
Sample
Churches were recruited in cohorts of 4 over 3 years in October-December prior to the intervention starting the following year. The recruitment process was led primarily by the CAB who contacted churches from their community networks and worked with research staff to meet with local pastors. Churches were required to have a minimum of 100 members and matched by size prior to randomization (small ≤ 200 members, large > 200 members). In addition, churches had to accept the randomization process, identify health coaches (1-2 female church members), and support BMW study activities.
Recruitment of participants included announcements during church services and events, flyers, health coach or pastor communications, or in-person recruitment. Eligibility requirements included: 1) African-American female (≥ 18 years), 2) non-diabetic, 3) body mass index (BMI) ≥ 25, 4) not attending a weight loss program currently or during the previous 6 months, 5) not having a medical condition that interfered with physical activity or dietary changes, 6) not intending to move in the next year, 7) church member or amenable to receiving church services, and 8) willingness to participate in a 10-month weight-loss study. Initial phone or in-person screening evaluated eligibility and self-reported height and weight. Participants who screened eligible were invited to an in-person orientation at their church to collect informed consent and complete baseline measures including objective measures of height and weight. Details on church and participant recruitment can be found in Kitzman et al. 29
Measures
A total of 3 measurement events: baseline, 4-month (post-intervention), and 10-month follow-up (post-maintenance phase) were held at each church. Participants were instructed to be fasting and to take any prescribed morning medications. Objective measures were collected by trained and blinded research staff. A detailed description of measures was previously reported. 29
Primary measures. Weight was collected with a digital scale (Doran DS610) and height was measured with a stadiometer (SECA 213). Waist circumference was taken at the top of the pelvis with a measuring tape. 30 Weight, height, and waist circumference were measured twice with the average recorded.
Secondary measures. Hemoglobin A1c (HbA1c), fasting glucose, low-density lipoprotein cholesterol (LDL), high-density lipoprotein cholesterol (HDL), total cholesterol, and triglycerides were measured with a fasting finger stick blood sample using a point of care machine. Blood pressure was measured twice following the Eighth Joint National Committee guidelines. 31 Saliva samples were collected and assayed for morning salivary cortisol (ng/mL) and estradiol (E2, pg/mL) levels. Diet was collected with the Delta NIRI food frequency questionnaire and analyzed for average daily intake of calories, fat, sodium, carbohydrates, protein, and other dietary components. 32 Physical activity and sedentary behavior were measured with a valid self-report survey. 33 Metabolic syndrome was defined based on the National Cholesterol Education Program Adult Treatment Panel III. 34
Process evaluations. Process evaluations were implemented by trained staff regularly (4 times over the core intervention) to monitor dose (e.g., whether a program activity was done) and fidelity (e.g., how well a program activity was done) in the SDPP and FDPP churches following published guidelines 35 and detailed in Kitzman et al. 29 Fidelity was measured using a Likert scale (1-4 for the highest level of fidelity), with an a-priori goal of 3.0. Dose of program delivery was measured with a YES/NO scale, with an a-priori goal of 75%.
Interventions
FDPP and SDPP churches used the DPP, an evidence-based lifestyle intervention that emphasizes 2 primary goals: 7% weight loss and 150 minutes of weekly physical activity. 4,36,37 Additionally, the DPP emphasizes behavioral skills for healthy eating and physical activity such as self-monitoring, social support, and goal setting. The DPP is structured with a 16-week core program followed by a 6-month maintenance phase. Female congregation members facilitated the DPP after completing an 8-hour training conducted by a National DPP trained research staff member. Participants received a DPP curriculum binder, and health coaches received facilitator guides and DPP curriculum. Health coaches received support from the DPP trained research staff member through weekly or bi-weekly phone meetings or email.
For FDPP churches, 5 additional faith components tied to weekly learning objectives were incorporated into the standard DPP curriculum and facilitator materials for each session including: 1) a 15-minute mini sermon delivered by a pastor or pastor associate, 2) a memory verse, 3) in-class or take-home faith activity, 4) promises to remember, and 5) scripture and prayer. Detailed information on development of the FDPP curriculum was previously published. 29
After the core program, participants received 6 DPP maintenance sessions according to their intervention group. During this period, health coaches continued to meet with participants in a group setting on a monthly or bi-monthly basis.
Statistical Analyses
Intent-to-treat analyses were conducted for the entire sample and within-group changes from baseline to 4-months, baseline to 10-months, and 4-months to 10-months. A fully conditional specification (FCS) method was used to estimate a set of 20 multiple imputed datasets for intent-to-treat analyses. Biometrics and health behaviors were evaluated using 2-level mixed effect models. Due to the study design, randomization of treatment conditions at the cluster (church) level, a multilevel (2 levels: cluster level and individual level) hierarchical regression model was used to estimate the adjusted effect of the intervention (see equation 1 and 2). The impact of FDPP compared to SDPP was evaluated at 2 assessment periods: 1) at 4-months (post-intervention phase) and 2) at 10-months (maintenance phase). Each of the differential characteristics by intervention conditions found at baseline were included in the adjusted models to account for individual-level baseline differences. PROC MIXED followed by PROC MIANALYZE in SAS 9.4 (SAS institute Inc.) were employed in the adjusted analysis to account for the cluster level effects (estimated intracluster correlation coefficient (ICC) was 0.06) and to estimate the standard error accurately for multiple imputed data.
A classification and regression tree (CART) method was used to dichotomize the optimum number of intervention sessions as high or low attendance corresponding to a 5% weight reduction. Type I error rate was set to 5% in drawing statistical significance in each null hypothesis significance test. The following multilevel models were used to estimate the treatment effects at 4-months and 10-months separately on weight loss.
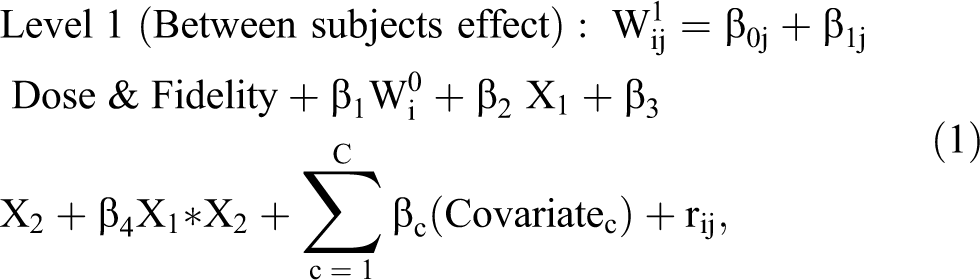
where,

where, indicator j represents the clusters (churches) (j = 1, 2,…, 11). The parameter
Several similar multilevel models were fitted to estimate the effect of intervention on chronic disease (blood pressure, HDL and LDL cholesterol, and metabolic syndrome, hemoglobin A1C) at 4-months for those with elevated risk at baseline.
A-priori power analyses were conducted with an effect size of 0.50 for weight loss between 2 intervention groups as reported by Wu et al. 38 Intra-cluster correlation coefficient (ICC) was used as 0.03 as reported in a similar study (GoodNEWS trial) 26 and type I error rate was 5%. To observe 80% power, the estimated number of required clusters (churches) was 12 with approximately 20 participants in each cluster (N = 240). In this study, 1 church was dropped due to low participation and resulted to the final sample size of 221 in 11 churches.
Results
Recruitment and Attrition
The CONSORT diagram (Figure 1) shows church recruitment, screening, and attrition. A total of 333 adult African American women from 12 churches were screened for eligibility. Of 289 screened eligible participants, 263 attended baseline measures and 221 enrolled in the study. Six churches with 119 participants were randomized to the FDPP group and 5 churches with 102 participants were randomized to the SDPP group. One church randomized to SDPP dropped due to inability to recruit participants. About 37 participants (17%) were lost to follow-up at the 10-month measurement. Missing data were found missing completely at random with no monotonic pattern of missingness. 39 There were no significant differential characteristics for baseline weight, age, educational status, health behavior and biometric measures between those lost to follow-up and those who completed the intervention.
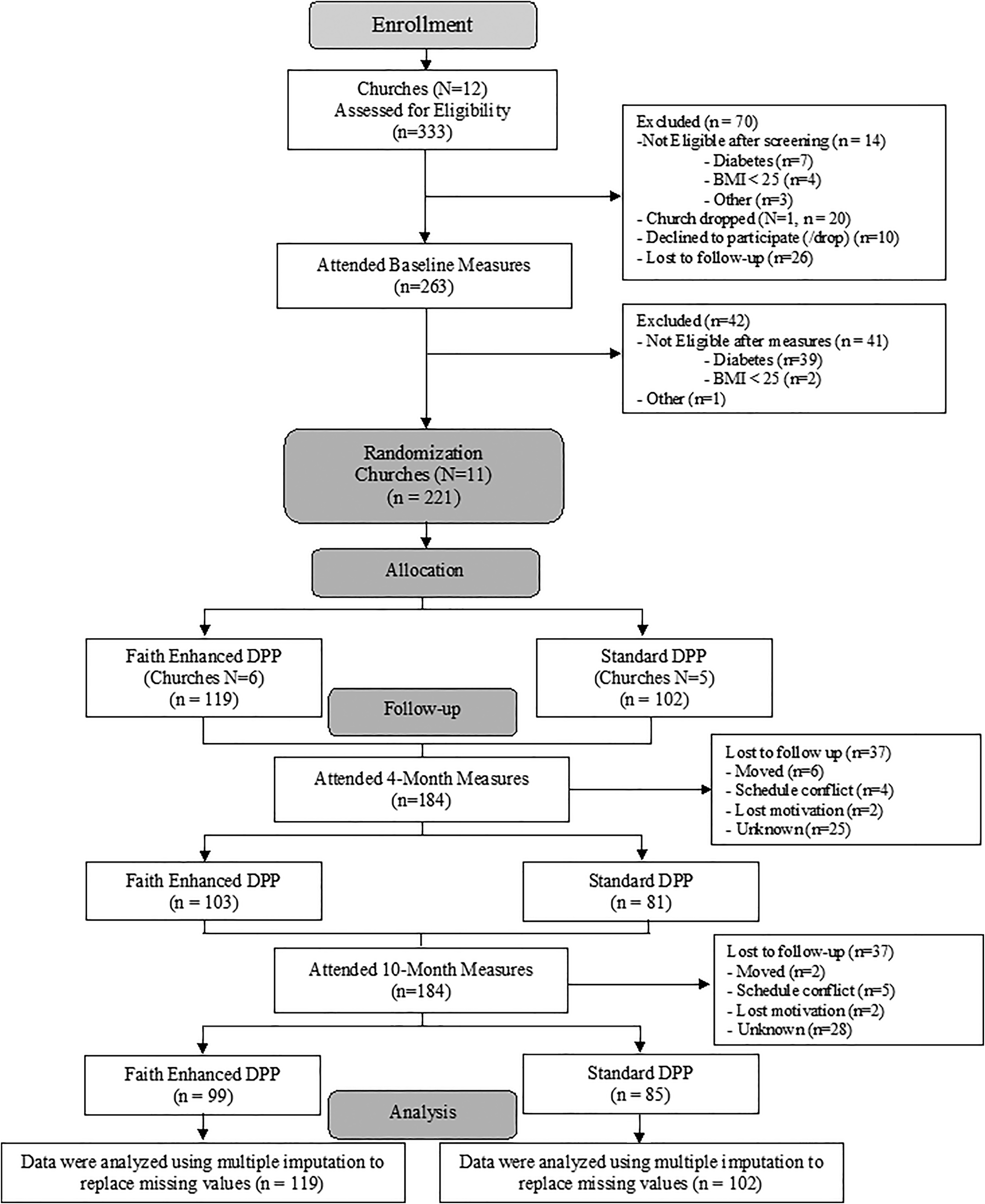
Better Me Within CONSORT diagram.
Participant Characteristics: Demographics, Health Behaviors, and Biometric Measures
Table 1 summarizes the baseline demographic, health behaviors, and biometric measures for the entire sample and by groups. On average, participants (n = 221) were aged 48.8 years (SD = 11.2) and 48% had a college degree or more. More than 80% of the participants were obese (BMI ≥ 30) with mean BMI = 36.7 kg/m2 (SD = 8.4). More than two-thirds (n = 150) of the participants were pre-diabetic (HbA1c ≥ 5.7) at baseline and the mean HbA1c was slightly higher among the SDPP than the FDPP participants (p < 0.05). About 75% of the participants were pre-hypertensive (SBP ≥ 120 or DBP ≥80) and one-third were hypertensive (SBP ≥140 or DBP ≥90).
Baseline Demographic, Health Behavior, and Biometric Characteristics of BMW Participants.
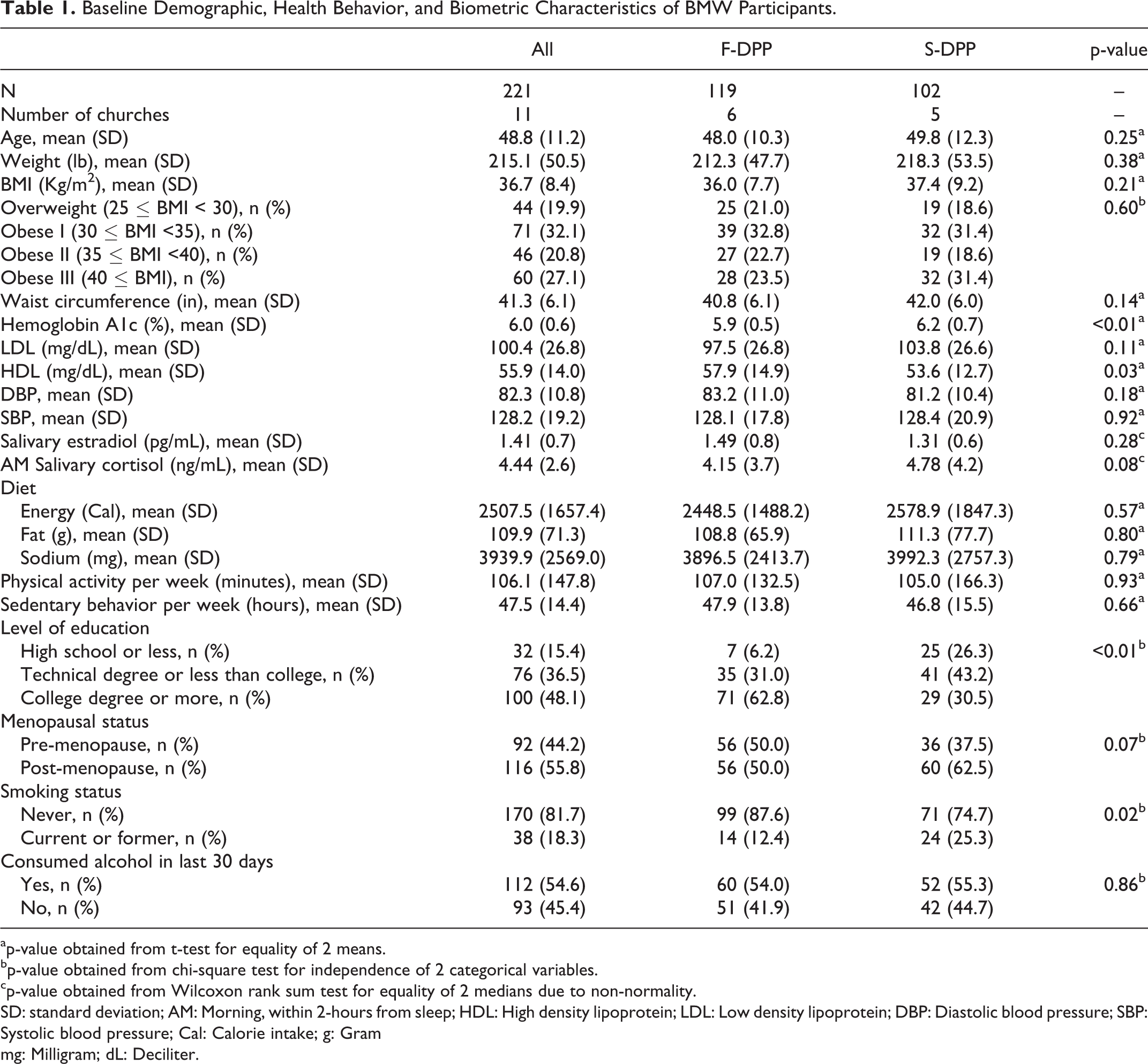
ap-value obtained from t-test for equality of 2 means.
bp-value obtained from chi-square test for independence of 2 categorical variables.
cp-value obtained from Wilcoxon rank sum test for equality of 2 medians due to non-normality.
SD: standard deviation; AM: Morning, within 2-hours from sleep; HDL: High density lipoprotein; LDL: Low density lipoprotein; DBP: Diastolic blood pressure; SBP: Systolic blood pressure; Cal: Calorie intake; g: Gram
mg: Milligram; dL: Deciliter.
Process Evaluation
Table 2 displays the process evaluation summary measuring dose and fidelity to program implementation. Dose was 79% and mean fidelity score was 3.3 out of 4.0 across intervention groups. There were no significant differences in dose and fidelity between FDPP and SDPP churches (p > 0.05). Four churches did not meet dose and/or fidelity goals, which was adjusted for in regression models comparing intervention effects. Participants in churches that met dose and fidelity lost on average 1.25 lbs. more than those whose church did not; however, the effect was not significant (p = 0.31). Participants attended 11 out of 16 total classes during the core intervention (69%). Based on the CART analysis, the optimum number of classes was identified as 15 or more (high attenders) to achieve CDC recommendation for weight loss of 5% to 7%. 40
Program Implementation at 4-Month by Lay Health Leaders in BMW Study.
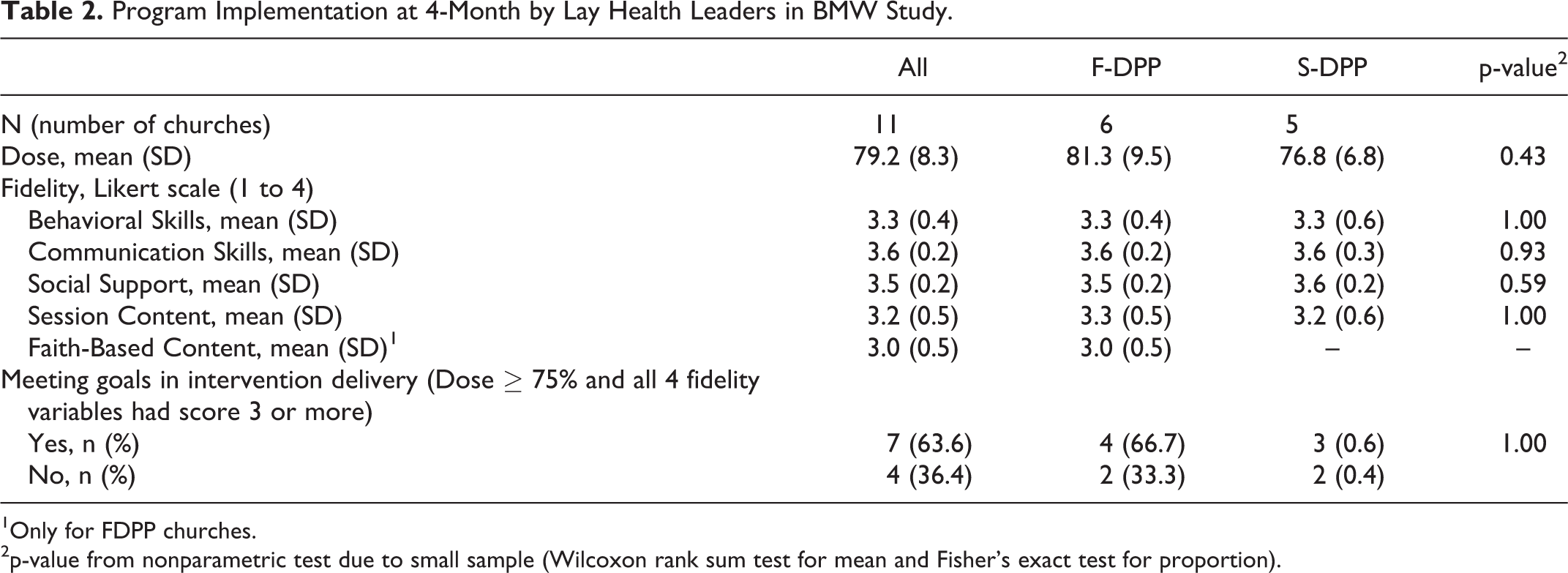
1Only for FDPP churches.
2p-value from nonparametric test due to small sample (Wilcoxon rank sum test for mean and Fisher’s exact test for proportion).
Overall Changes in Body Weight
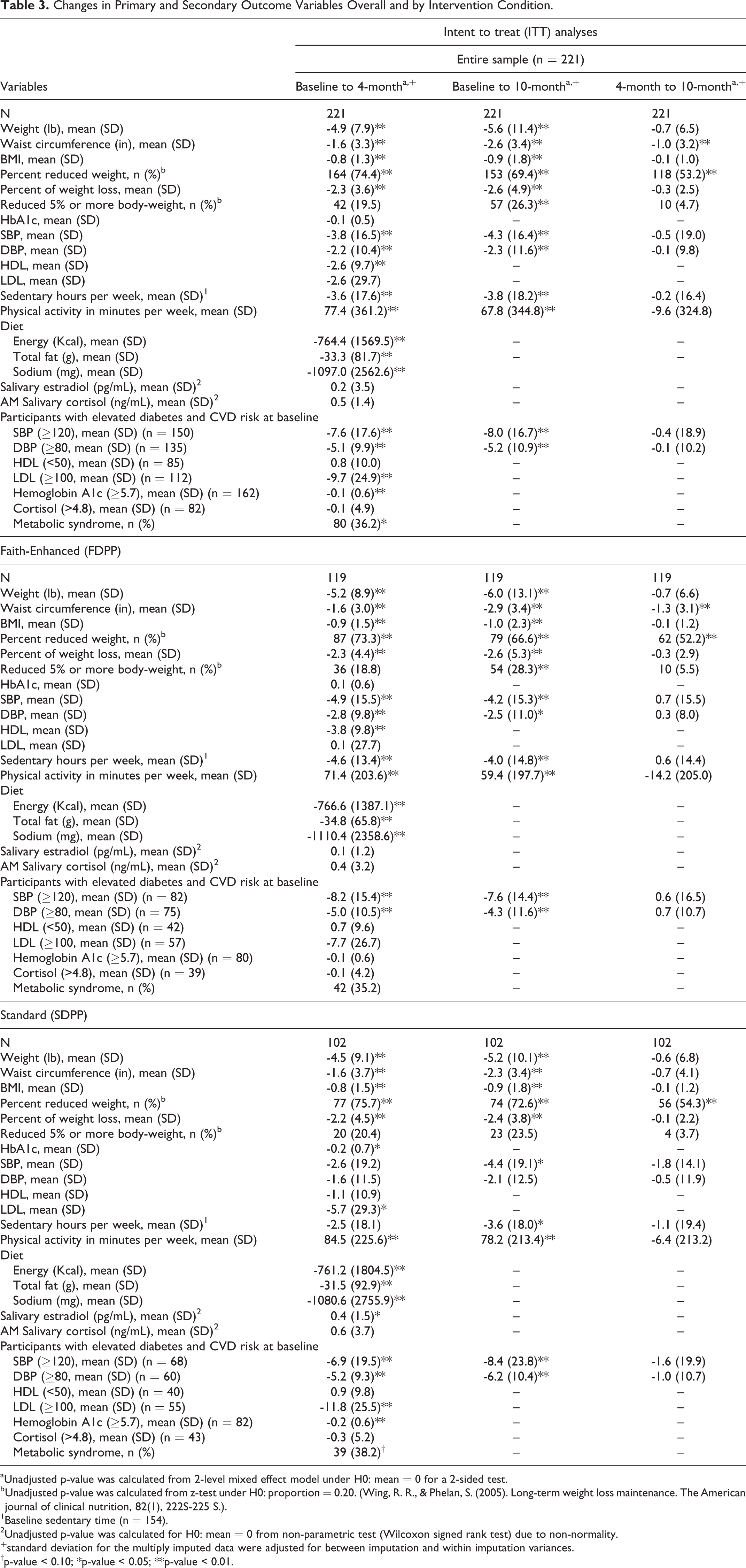
Based on the intent-to-treat analyses, ∼ 75% of the participants lost weight by the end of the intervention at 4-months, and many of them (53%) continued to lose weight during the maintenance phase (Table 3). On average, participants lost 4.9 lb (SD = 7.9) at 4-months and 5.6 lb (SD = 11.4) at 10-months. About 2.6% of total body weight was reduced at 10-months and 26% of participants lost 5% or more of their total body weight. At 4-months, ∼ 14% moved to a lower BMI category, and at 10-months, ∼ 20% moved to a lower BMI category (p < 0.01).
Changes in Primary and Secondary Outcome Variables Overall and by Intervention Condition.
a Unadjusted p-value was calculated from 2-level mixed effect model under H0: mean = 0 for a 2-sided test.
b Unadjusted p-value was calculated from z-test under H0: proportion = 0.20. (Wing, R. R., & Phelan, S. (2005). Long-term weight loss maintenance. The American journal of clinical nutrition, 82(1), 222S-225 S.).
1Baseline sedentary time (n = 154).
2Unadjusted p-value was calculated for H0: mean = 0 from non-parametric test (Wilcoxon signed rank test) due to non-normality.
+standard deviation for the multiply imputed data were adjusted for between imputation and within imputation variances.
†p-value < 0.10; *p-value < 0.05; **p-value < 0.01.
Intervention Effects on Weight Reduction at 4-Months and at 10-Months: Adjusted Analysis
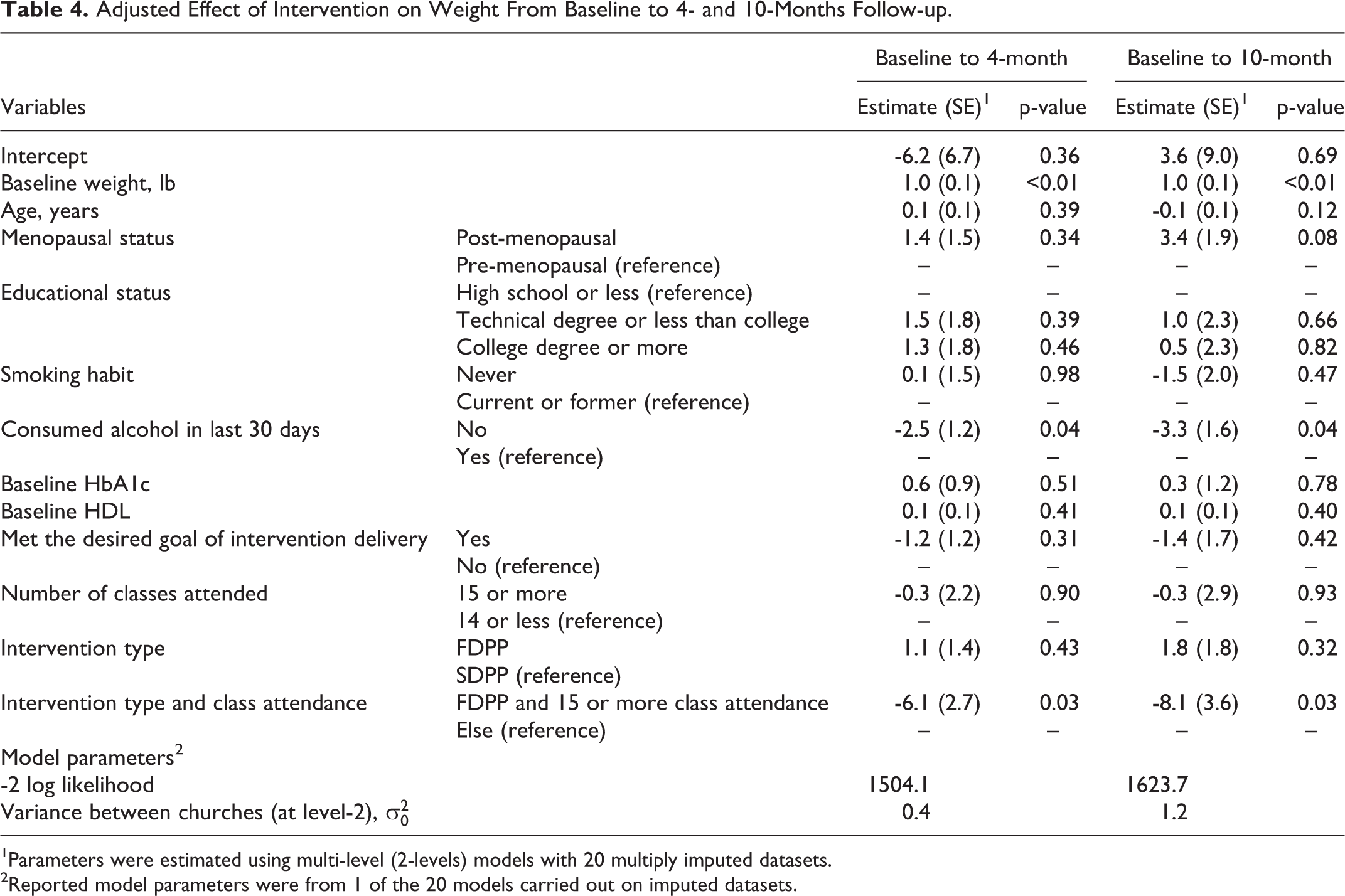
Table 4 presents the adjusted effects of the intervention conditions on weight at 4-months. Participants who attended 15 or more classes (high attenders) and randomized to FDPP lost significantly more weight than those randomized to SDPP or were low attenders in the FDPP (attended 14 or less classes) (adjusted mean = 6.1 lbs, p = 0.03; reduced 4.8% body weight at 4-months, 5.8% at 10-months). The adjusted mean weight loss was 10.0 lbs at 4-months and 12.4 lbs at 10-months for high attenders (15 or more class attended) randomized to FDPP churches compared to low attenders and/or SDPP participants (Figure 2). In contrast, weight loss at 4- and 10-months varied between 3.3 lbs to 5.0 lbs for those randomized to SDPP or categorized as low attenders (14 or less FDPP class attended). Without considering attendance, there were no significant differences between groups with both demonstrating significant weight loss.
Adjusted Effect of Intervention on Weight From Baseline to 4- and 10-Months Follow-up.
1Parameters were estimated using multi-level (2-levels) models with 20 multiply imputed datasets.
2Reported model parameters were from 1 of the 20 models carried out on imputed datasets.
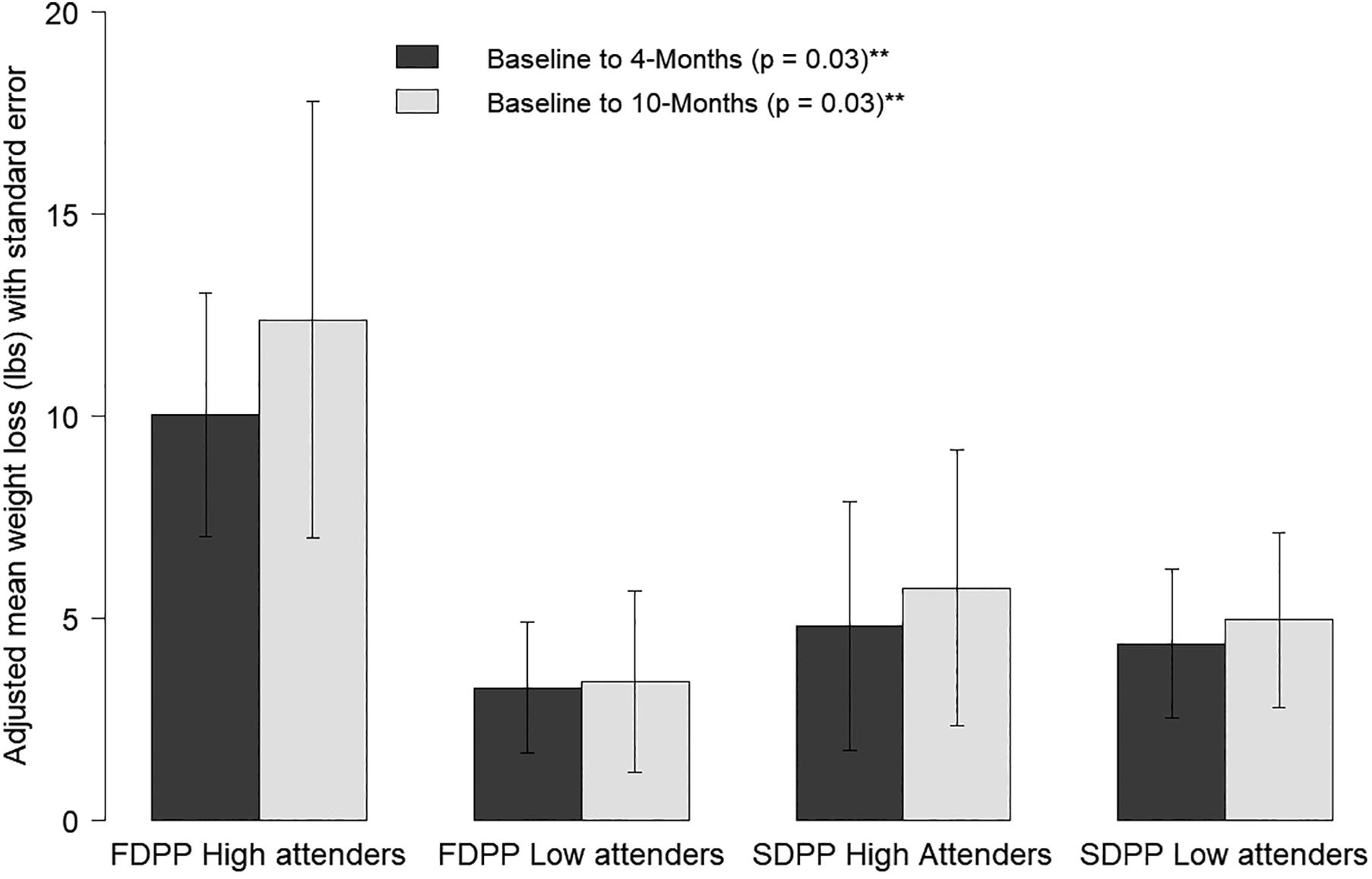
Adjusted mean weight loss by intervention conditions and attendance.
Participants who reported no alcohol use in the past month had a significant decrease in their body weight as opposed to their counterparts (p = 0.04). Pre-menopausal women had a reduction of 3.4 lbs. on average more than post-menopausal women at 10-months (p = 0.08). Estradiol and cortisol levels were not significantly related to weight loss. Findings at 10-months were similar to the adjusted model for weight loss at 4-months.
Intervention Effects on Diet and Physical Activity
FDPP and SDPP had significant improvements in diet and physical activity with no significant treatment effects. Overall, participants reduced their kcals by 764.4, fat grams by 33.3, and sodium by 1097.0 mg at 4-months follow-up. Participants increased their average weekly physical activity by 77.4 minutes at 4-months, and 67.8 minutes at 10-months.
Intervention Effects on Reducing Diabetes and CVD Risk
Table 3 presents diabetes and CVD outcomes along with a subgroup analyses on participants with elevated markers. Participants with elevated blood pressure (SBP ≥120 or DBP ≥80) at baseline experienced a 7.6 mmHg (SD = 17.6) and 8.0 mmHg (SD = 16.7) reduction in SBP and 5.1 mmHg (SD = 9.9) and 5.2 mmHg (SD = 10.9) reduction in DBP at 4 and at 10-months, respectively. Participants (37%) with suboptimal HDL (<50 mg/dL) at baseline observed an increase of 0.8 mg/dL (SD = 10.0) at 4-months. Participants (53%) who had LDL above the desired level (>100 mg/dL), experienced a reduction of 9.7 mg/dL (SD = 24.9). Participants with an elevated level of HbA1c (≥5.7) at baseline had a mean reduction of 0.12 (SD = 0.6). About half of the participants (44.8%) were diagnosed with metabolic syndrome at baseline which reduced to 36.2% at 4-months (p < 0.01). At baseline, metabolic syndrome was more prevalent among the participants randomized to SDPP than those in FDPP (51.1% and 37.8%, respectively). FDPP and SDPP participants had similar changes in blood pressure, HDL, LDL, HbA1c, cortisol level, and metabolic syndrome at 4-months.
Discussion
The BMW trial evaluated a faith-enhanced DPP compared to a standard DPP facilitated by congregation members that included the pastor in program delivery on weight loss in African American women. The primary finding was that both the FDPP and SDPP had significant reductions in weight; however, those with optimal attendance in the FDPP condition lost significantly more weight than those in the SDPP group, or low attenders in the FDPP group. Further, both the FDPP and SDPP interventions demonstrated significant improvements in diet and physical activity, and reductions in chronic disease risk factors.
In the original DPP efficacy trial, African American women lost 9.7 (SD = 13.2) lbs at 12-months corresponding to a 5% weight loss. 8 Whereas DPP translation studies in African Americans have reached half of that goal on average (2.6%-3.2%) including both genders and studies of varying quality and duration. 1 Further, most of these translational studies were facilitated by health professionals with 1 using trained community health workers. 1 The BMW trial overall resulted in a 5.6 (11.4) lb weight loss corresponding to a 2.6% reduction at 10-months. For those in the FDPP intervention that had optimal attendance, 4-month weight loss was 10.0 lbs or 4.8%, and at 10-months was 12.4 lbs or 5.8%. In the Fit Body and Soul study, high attenders in the faith-based DPP had an 8 lb reduction at 12-months. 13 To our knowledge, the BMW faith-based DPP translational trial has produced the largest weight loss percent in urban African American women to date. The success of the BMW trial compared to other adaptions is encouraging considering its intervention was conducted by congregation members with limited training. Sustainability and high-cost of training and implementation have been cited as barriers to expanding the reach of the DPP to help address health disparities, particularly in lower resourced environments. 41
Other translations of the DPP, including faith-based adaptions, have not resulted in reaching the DPP’s goal of 7% weight loss. 1,13,18 This goal was nearly reached for high attenders in the BMW’s FDPP group. The faith-based adaption included several novel components that may have contributed to this finding. First, it was developed primarily by faith leaders from the local community using CBPR principles with feedback from researchers. Past studies have mentioned collaborative approaches to curriculum development, but descriptions are often vague, and it is unclear how much community partners guided the process. Secondly, faith-based adaptions and pastor mini-sermons were specifically connected to DPP weekly learning objectives to reinforce the theoretical underpinnings of the DPP with religious constructs meaningful to participants. Third, pastors were included in the delivery of the BMW faith-based DPP by delivering mini-sermons at the beginning of each class. This allowed influential pastors to be involved in health promotion delivery while being respectful of time constraints. 42 One study found that higher levels of pastor support during health promotion programs improved participant retention. 25 Due to their influence and importance, pastor involvement in weekly sessions may have improved participant motivation leading to higher attendance and subsequently greater weight loss. 22,24,25,42
There are several limitations of this study. The BMW trial had a moderate attrition rate of 17%, which is higher than the original DPP, but consistent with other DPP translational studies. 1 Participants in the BMW trial attended 69% of intervention sessions, while not optimal, is similar to other DPP translational studies. 1 Further, due to cluster randomization, some individual level baseline differences were found between intervention groups, however, these factors were included as covariates in outcome models. Lastly, the population included in the BMW trial may not be representative of African American women throughout the country but does provide generalizable findings for church-going African American women.
Overall, participants in the faith-based adaption who received at least 15 sessions nearly reached the DPP’s original goal of 7% weight loss and met the CDC’s goal of 5% weight loss. BMW’s faith-based DPP has the potential to help African American women reach 5% weight loss in a church-based community setting. Further, the BMW trial demonstrated that congregation members can successfully deliver the DPP providing a potential pathway for increasing reach and adoption. Both the standard DPP and the enhanced faith-based DPP led to significant improvements in weight, lifestyle behaviors and chronic disease risk, highlighting that churches with limited resources can still significantly improve the health of African American women using non-tailored secular approaches.
So What? (Implications for Health Promotion Practitioners and Researchers)
What is already known on this topic?
African American women tend to have less success than others in lifestyle interventions and DPP translations in African Americans have resulted in suboptimal results.
What does this article add?
This study found that faith-based components, when fully implemented, can improve the effectiveness of DPP translations in African American women. It also highlights the influential role of the pastor in health promotion delivery.
What are the implications for health promotion practice or research?
This study indicates that DPP programs facilitated by church congregation members with limited training are effective and can improve the reach and adoption in lower resourced communities. Faith-based programs should consider integrating the pastor into health promotion delivery in time effective ways.
Footnotes
Author Contributions
Heather Kitzman, PhD - designed and implemented study, collected and analyzed data, interpreted data, drafted manuscript and edited. Abdullah Mamun, PhD - collected and analyzed data, interpreted data, drafted manuscript and edited. Leilani Dodgen, MPH - implemented study, collected and analyzed data, interpreted data, drafted manuscript and edited. Donna Slater - designed study, collected data, edited manuscript. George King, MDiv - designed and implemented study, collected data, edited manuscript. Alene King, BA - designed and implemented study, collected data, edited manuscript. Lee Slater, BS - designed and implemented study, collected data, edited manuscript. Mark DeHaven, PhD - designed study, drafted and edited manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.