
Abstract
Purpose:
To assess the prevalence of perceived barriers to accessing health care services, self-efficacy, and health-promoting behaviors among Franco-Americans as a higher-risk group for familial hypercholesterolemia (FH), stratified by cardiovascular risk factors.
Design:
Cross-sectional survey based on components of the Health Belief Model
Setting:
Administered in-person at a Franco-American cultural center and online through mailing lists and social media platforms in the Northeastern United States
Sample:
Franco-Americans and French Canadians (n = 170)
Measures:
Demographic and clinical characteristics (i.e. high cholesterol, prior heart attack or stroke, family history of atherosclerotic cardiovascular disease (ASCVD), diagnosis of FH), perceived barriers to accessing health care services, self-efficacy, and health-promoting behaviors (i.e. taking lipid-lowering medications, seeing a cardiovascular specialist).
Results:
In a cohort of Franco-Americans, 42 (25%) had both high cholesterol and family history of ASCVD. Among Franco-Americans with both cardiovascular risk factors, 22% had low self-efficacy and only 16% had discussed FH with their physician. Individuals with both risk factors were significantly more likely to report a concern over a future diagnosis as a barrier to accessing health care services when compared with those with neither risk factor (36% vs. 15%, p = 0.014). Overall, other prominent barriers to care included knowledge of when to seek help (27%) and a distrust in medicine (26%).
Conclusion:
Franco-Americans report significant barriers to accessing health care services. Our findings strengthen the case for developing focused public health strategies to raise awareness for FH, particularly among high-risk subpopulations with unmet cardiovascular needs.
Keywords
Purpose
Familial hypercholesterolemia (FH) is an inherited disorder characterized by lifelong elevated low-density lipoprotein (LDL) cholesterol levels and an increased risk of premature atherosclerotic cardiovascular disease (ASCVD). 1 If left untreated, patients with FH have 20 times the risk of developing ASCVD compared with the general population. 1,2 Among the nearly 1.3 million individuals in the United States with FH, approximately 90% remain undiagnosed. 2 Though FH affects all racial and ethnic groups, FH is more prevalent among certain founder populations, including French-Canadians and Franco-Americans. 3 Prior research has evaluated the genetic predisposition of FH in French-Canadians living in the Province of Quebec, yet little is known about Franco-Americans as direct descendants of this demographic along with their unique cardiovascular risk profile, perceptions of disease, and barriers to care. 3,4
Given the increased risk of FH among Franco-Americans and general gaps in the diagnosis and management of FH, there is an urgent need to characterize the perceptions of and barriers to early diagnosis and treatment in this higher-risk population. With its longstanding application of predicting health-related behaviors and uptake of health services through integrating individuals’ beliefs and perceptions, cues to action, and self-efficacy, the Health Belief Model (HBM) represents a key model for evaluating current gaps in care for Franco-Americans and identifying potential opportunities to promote health and prevent disease. Using a questionnaire incorporating components of the HBM, we aimed to describe the prevalence of perceived barriers to accessing health care services, cues to health action, self-efficacy, and health-promoting behaviors among Franco-Americans and French-Canadian descendants. We also assessed variations in these measures across cardiovascular risk factor profiles such as those with high cholesterol and/or a family history of ASCVD.
Methods
Design
We developed a conceptual model to assess factors contributing to health-promoting behaviors in Franco-Americans. 4 This adapted model was designed based on components of the HBM and served as the basis for our survey instrument investigating demographic and clinical characteristics, perceived barriers to accessing health care services, cues to health action, self-efficacy, and health-promoting behaviors.
Measures
Our study variables included demographic characteristics (i.e. age, sex, annual household income, and highest level of completed education) and clinical characteristics (i.e. high cholesterol, prior heart attack or stroke, family history of ASCVD, and FH diagnosis). Perceived barriers to accessing health care services are listed in Table 1 and include knowledge of when to seek help, distrust in medicine, and a concern over a future diagnosis, among others. Self-efficacy was analyzed by asking respondents, on a 4-point Likert scale (strongly disagree to strongly agree), their levelof agreement with the following statement: “There is nothing I can do to prevent myself from getting heart disease.” Self-efficacy was categorized in a dichotomous manner classifying those who selected “strongly agree” or “agree” to the above question as having lower relative self-efficacy when compared with participants who selected “strongly disagree” or “disagree.” Participants were also asked the following question indicating an affirmative (yes) for cues to health action: “My doctor has talked to me about familial hypercholesterolemia (FH).” Lastly, health-promoting behaviors included participants’ utilization of 1 or more lipid-lowering medications and whether they see a cardiologist or other cardiovascular specialist.
Perceived Barriers to Accessing Health Care Services Among Franco-Americans Stratified by High-Risk Cardiovascular Characteristics Including the Presence of High Cholesterol or a Family History of ASCVD, Both Risk Factors Concurrently, and Those Who Have Received an FH Diagnosis.
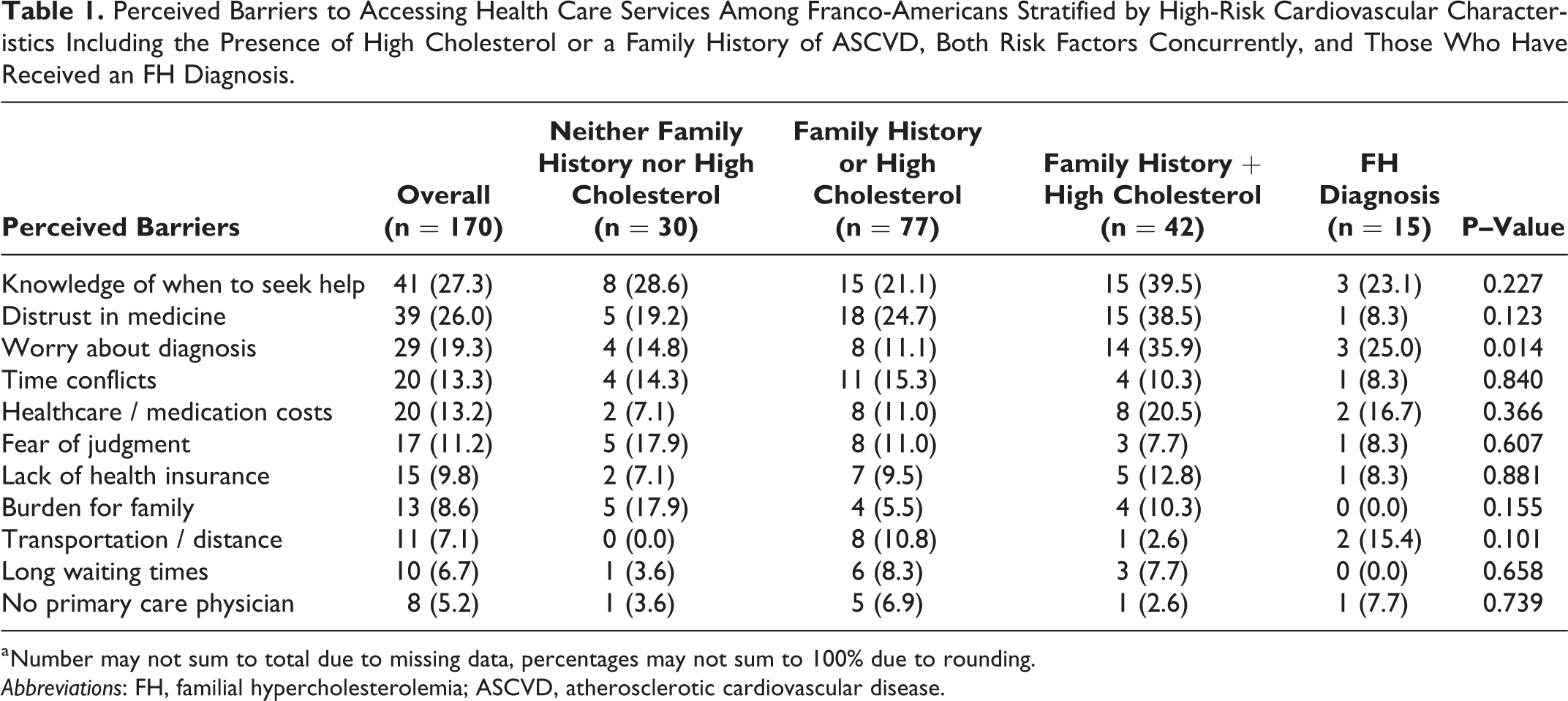
a Number may not sum to total due to missing data, percentages may not sum to 100% due to rounding.
Abbreviations: FH, familial hypercholesterolemia; ASCVD, atherosclerotic cardiovascular disease.
Sample
Printed surveys were administered in-person to participants attending regular programming at a Franco-American historical and cultural center in Lewiston, Maine, a city with one of the highest demographic representations of Franco-Americans and French Canadians per capita in the United States. 5 We also administered an electronic version of our survey through the online mailing lists of the cultural center and through social media platforms of affiliated organizations to maximize the participation of Franco-Americans. Both the printed and electronic versions of the survey were available in English and French depending on the participants’ language preferences. Participants were included if they were 18 years of age or older, self-identified as Franco-American or of French-Canadian descent, and proficient in either English or French.
Analysis
We analyzed differences in categorical and binary descriptive data across stratified cardiovascular risk subgroups using chi-squared analysis or Fisher’s exact test. These stratified subgroups across cardiovascular risk factor profile subgroups included individuals with either high cholesterol or a family history of ASCVD, those with high cholesterol and a family history of ASCVD concurrently, and those who have received an FH diagnosis. Due to a small proportion of individuals in our sample who indicated receiving an FH diagnosis, our chi-square analysis consisted of comparisons between participants affected by a single cardiovascular risk factor alone, those affected by both risk factors, and participants with neither condition. A p-value <0.05 was considered statistically significant a priori and all statistical tests were two-tailed. Analyses were conducted with SAS, version 9.4 (SAS Inc., Cary, North Carolina).
Results
We received 229 completed paper-based and electronic surveys between February and April 2018. After excluding incomplete surveys and responses from individuals who were not Franco-American or of French-Canadian descent, the final sample included 170 self-identified Franco-American and French-Canadian participants.
Overall and stratified distributions of demographic and clinical characteristics and other HBM-derived study variables are presented in Table 2. When stratified by cardiovascular risk factors, 77 (45.3%) individuals had either high cholesterol or a family history of ASCVD, 42 (24.7%) had both risk factors, 30 (17.6%) had neither risk factor, and 15 (8.8%) reported receiving an FH diagnosis. Among those with both risk factors, 9 (22.0%) individuals reported lower self-efficacy, and 6 (15.8%) reported discussing FH with their physician. In this higher-risk subgroup without an FH diagnosis, 31 (73.8%) and 14 (33.3%) individuals indicated taking 1 or more lipid-lowering medications and seeing a cardiologist as relevant health-promoting behaviors, respectively (Table 2).
Study Variables Among Franco-Americans Stratified by High-Risk Cardiovascular Characteristics Including the Presence of High Cholesterol or a Family History of ASCVD, Both Risk Factors Concurrently, and Those Who Have Received an FH Diagnosis.
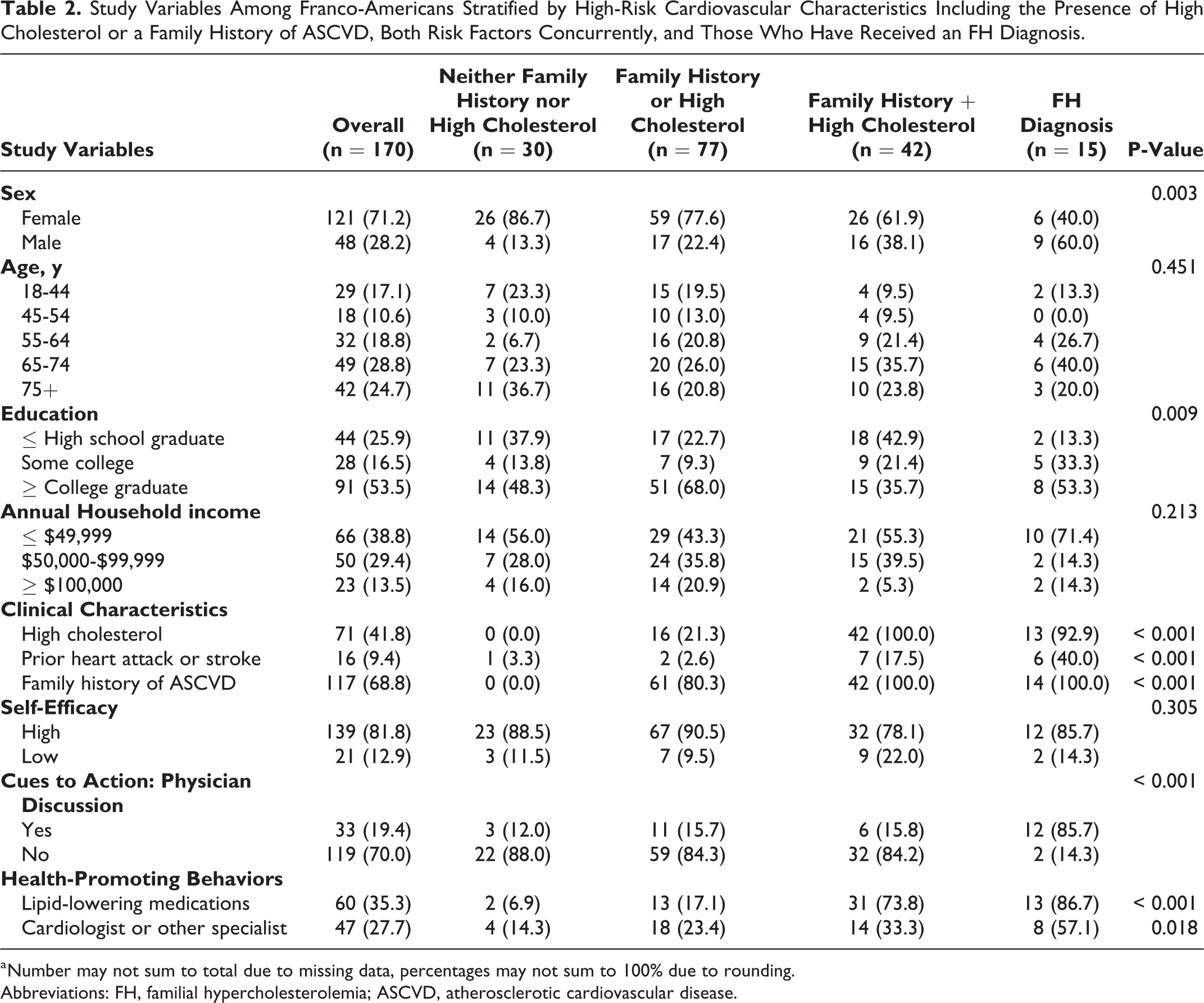
a Number may not sum to total due to missing data, percentages may not sum to 100% due to rounding.
Abbreviations: FH, familial hypercholesterolemia; ASCVD, atherosclerotic cardiovascular disease.
Among Franco-Americans with both cardiovascular risk factors, the most frequently reported barriers to accessing health care services included knowledge of when to seek help (n = 15, 39.5%), distrust in medicine (n = 15, 38.5%), and a concern over a future diagnosis (n = 14, 35.9%) (Table 1). Moreover, when compared with participants with neither risk factor, those with both cardiovascular risk factors were significantly more likely to express a concern over a future diagnosis as a barrier to care (35.9% vs. 14.8%, p = 0.014).
Lastly, among the 15 Franco-Americans with an FH diagnosis, we found that 40.0% (n = 6) reported having previously experienced a heart attack or stroke. Additionally, 13 (86.7%) and 8 (57.1%) individuals with FH were taking 1 or more lipid-lowering medications and seeing a cardiologist, respectively.
Discussion
In our cohort of 170 Franco-Americans, an understudied population with a high genetic risk for FH and premature ASCVD, we found that 1 in 4 had both high cholesterol and a family history of ASCVD. Among those in this higher-risk subgroup without an FH diagnosis, 1 in 5 had low self-efficacy and even fewer had discussed FH with their physician. Commonly reported barriers to accessing health care services included knowledge of when to seek help and adistrust in medicine. Participants with both cardiovascular risk factors were significantly more likely to report a concern over a future diagnosis (36%) as a barrier to care when compared with individuals with ≤1 risk factor.
While prior applications of the HBM have been used to gain insight into individual perceptions and health actions regarding ASCVD, few studies have applied components of these behavior change models to FH patients specifically. 6 -8 Of note, Hagger and colleagues found that attitudes and perceived control predicted intentions to engage in self-management behaviors including taking cholesterol-lowering medications. 8 Furthermore, while individuals with FH recognize that untreated FH increases risk of ASCVD, many dismissed the severity of FH. 7,8
Stratified analyses describing HBM components by cardiovascular risk factors underscore the importance of assessing these factors in advancing routine clinical practice. Qureshi et al., for instance, reported that engaging in a systematic approach to collecting a comprehensive family history increases the proportion of individuals identified as having high cardiovascular risk and candidates for targeted prevention. 9 Considering that nearly 40% of Franco-Americans with both high cholesterol and a family history of ASCVD reported barriers to care including knowledge of when to seek help, distrust in medicine, and a concern over their diagnosis, there is an urgent need for physicians to address patients’ concerns and perceived barriers, acknowledge the implications of a potential founder effect when applicable, and integrate a systematic approach to gathering patients’ family history in managing cholesterol levels and lowering future cardiovascular risk. Integrated shared decision making and patient-centered care into routine clinical practice along with providing clear information about available therapeutic options may aid in alleviating individuals’ concerns about a potential diagnosis and their risk of a future cardiac event.
Our findings can also be interpreted alongside prior research pertaining to the general lack of FH awareness among patients and physicians. 10 Despite being descendants of a well-studied FH founder population in which 1 in 4 study participants had both high cholesterol and a family history of ASCVD, only 19% of individuals overall and fewer than 16% among the higher-risk subgroup without an FH diagnosis reported discussing FH with their physician.
Limitations
These findings should be interpreted in light of several limitations. First, our survey administration strategy occurred in a targeted manner, aimed to maximize the participation of Franco-American respondents, therefore introducing the possibility of selection bias. The inclusion of response and recall bias in participants’ responses also cannot be discounted, particularly with regard to our assessment of individuals’ self-efficacy. Second, the relatively small sample size of respondents limited the statistical power of our stratified analyses. Lastly, the external validity of our findings is limited to self-reported Franco-Americans from the Northeastern United States in which participants were predominantly female and ≥65 years of age. Moreover, given our utilization of electronic mailing lists and social media platforms for the dissemination of the online version of our survey, we could not accurately produce estimates of the total number of eligible study participants. Future studies should aim to gain greater insight into this founder population through random recruitment, a larger sample size, and comprehensive analyses of all HBM components.
Conclusion
Franco-Americans with high cholesterol and a family history of ASCVD had low self-efficacy and reported significant barriers to accessing health care services, with few having discussions about FH with their physician. Together these factors may contribute to the underdiagnosis and delayed treatment of FH in this understudied and high-risk founder population. Our findings strengthen the case for focused public health interventions and education campaigns raising awareness for FH, particularly among individuals and families with unmet cardiovascular needs.
So What?
What is Already Known on this Topic?
Franco-Americans and French Canadians represent high-risk founder populations for familial hypercholesterolemia, a genetic disorder of lipid metabolism that increases cardiovascular disease risk. However, little is known regarding the prevalence of factors influencing health-promoting behaviors including self-efficacy, perceived barriers to accessing health care services, and cues to health action in Franco-Americans, specifically.
What Does this Article Add?
A large proportion of Franco-Americans report significant barriers to accessing care including knowing when to seek help, distrust in medicine, and a concern over a future diagnosis, with few having discussions about FH with their physician despite having an increased cardiovascular risk.
What are the Implications for Health Promotion Practice or Research?
There is a fundamental need to continue increasing awareness for FH through focused public health interventions and awareness campaigns. Physicians who care for patients of French-Canadian descent who present with cardiovascular risk factors should be cognizant of the increased risk of FH among certain founder populations.
Footnotes
Acknowledgments
The authors gratefully acknowledge the Gendron Franco Center, Bates College, and other community stakeholders for their partnership toward this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.